Embed Size (px)
Citation preview

Raman Spectroscopy Detects Cardiac Allograft Rejection with Molecular Specificity
A Thesis
Submitted to the Faculty
of
Drexel University
by
Qiang Tu
in partial fulfillment of the
requirements for the degree
of
Doctor of Philosophy
June 2012

© Copyright 2012
Qiang Tu. All Rights Reserved.

ii
Acknowledgement
First and foremost I would like to express my deepest gratitude to my advisor, Dr.
Chang Chang, who has unreservedly support me with his patience and knowledge. I
would not have completed the thesis without his encouragement and excellent guidance.
He is a great mentor and my best friend, from whom I have learnt a lot not only with
respect to research skills but also with regard to life experience.
I would like to thank Dr. Pourrezaei, who showed great support for my defense and
gave me valuable advice and suggestions to my thesis with his wealth of knowledge. And
I had a great time working with him.
I would like to thank Dr. Kurzweg, who was willing to participate in my defense
committee even though he had a very tight schedule. And he has offered valuable advice
to my thesis.
I would like to thank Dr. Taskin who was willing to be on my defense committee and
has offered much advice and insight to my research and thesis.
Special thanks go to Dr. Zhong who was willing to participate in my defense
committee at the last moment.
I would like to thank Dr. Harada for teaching me pathology knowledge and training
me with skills of cryosection and H&E with patience.

iii
I would like to thank Natalia, Lisa and Danielle in Biomed office, who were always
willing to help and made my school life easier.
Finally I thank my parents and my wife for supporting me throughout my study and
work. I would also like to thank my friends in Drexel, Leko, Jingjia, especially Fu-han,
for their support and help.
This research is supported by Wallace H. Coulter Foundation Translational Research
Grant.

iv
Table of Contents
List of Tables ..................................................................................................................... vi
List of Figures ................................................................................................................... vii
Abstract ............................................................................................................................... x
CHAPTER 1. INTRODUCTION ....................................................................................... 1
CHAPTER 2. BACKGROUND ......................................................................................... 3
2.1 Raman Spectroscopy ................................................................................................. 3
2.2 Surface Enhanced Raman Spectroscopy ................................................................... 7
2.3 Analysis Methods in Raman Spectroscopy............................................................... 8
2.3.1 Fluorescence background removal ................................................................... 8
2.3.2 Multivariate data analysis .................................................................................. 9
2.3.2.1 Hierarchical clustering ................................................................................ 9
2.3.2.2 Principle component analysis ................................................................... 10
2.3.2.3 Linear discriminant analysis ..................................................................... 11
2.3.2.4 Artificial neural network ........................................................................... 12
2.3.2.5 Ordinary least squares regression ............................................................. 13
CHAPTER 3. CURRENT RELATED RESEARCH ....................................................... 15
3.1 Current Research Using Raman Spectroscopy ....................................................... 15
3.1.1 Cancer detection............................................................................................... 15
3.1.1.1 Breast Cancer ............................................................................................ 15
3.1.1.2 Cervical Cancer ......................................................................................... 19
3.1.1.3 Colorectal Cancer ...................................................................................... 22
3.1.2 Allograft rejection ............................................................................................ 23

v
3.2 Current research using SERS .................................................................................. 24
3.2.1 SERS for biomarkers ....................................................................................... 24
3.2.2 SERS for in vivo detection .............................................................................. 26
3.3 Emerging techniques of Raman spectroscopy ........................................................ 29
3.3.1 Single-walled carbon nanotube ........................................................................ 29
3.3.2 Multiplexed SERS imaging ............................................................................. 30
3.3.3 Photothermal effect .......................................................................................... 31
3.3.4 Core-Shell nanoparticle structure for improved SERS reproducibility ........... 31
CHAPTER 4. DETECTION OF CARDIAC TRANSPLANT REJECTION USING
RAMAN SPECTROSCOPY ............................................................................................ 35
4.1 Materials and Methods ............................................................................................ 35
4.1.1 Endomyocardial Biopsy ................................................................................... 35
4.1.2 Raman Spectroscopy Setup.............................................................................. 35
4.2 Results and Analysis ............................................................................................... 36
CHAPTER 5. SERS STUDY OF INDOLIC MOLECULES ADSORBED ON GOLD
COLLOIDS ....................................................................................................................... 49
5.1 Materials and Methods ............................................................................................ 49
5.2 Results and Analysis ............................................................................................... 49
CHAPTER 6. CONCLUTION AND FUTURE WORK .................................................. 60
CHAPTER 7. CONTRIBUTION ..................................................................................... 62
BIBLIOGRAPHY ............................................................................................................. 64
VITA ................................................................................................................................. 78

vi
List of Tables
Table 1. Diagnostic applications of Raman spectroscopy. Adapted from reference 12
. ... 33
Table 2. Summary of the histopathological readings of the biopsy samples and the results
of their Raman spectroscopy studies. A biopsy is defined as “rejected” by Raman
spectroscopy if more than 35% of its Raman spectra are abnormal, i.e. I758/I718 > 1. Using
this definition, eleven out of the twelve Grade-1R biopsies are classified as rejected by
Raman spectroscopy, while only 1 out of 17 Grade-0 biopsies display such property.
Adapted from reference 67
. ................................................................................................ 41
Table 3. Band assignments for the Raman and SERS spectra of serotonin, tryptophan,
melatonin and 5-HIAA. Adapted from reference 145
. ....................................................... 54

vii
List of Figures
Figure 1. Energy diagram for Rayleigh and Raman scattering processes. Rayleigh
scattering is the most intense scattering process, and Stokes scattering predominates over
anti-Stokes scattering at room temperature. Thickness of the arrows indicates the relative
intensity of the three processes (not to scale). Adapted from reference 12
. ........................ 5
Figure 2. A typical laboratory Raman spectroscopy system. Adapted from reference 12
. .. 6
Figure 3. Visual (A) and Raman imaging (B, C) of single control and senescent MCF-
7/NeuT cells. Raman images (B) were composed specifically from CH- stretching, and
were analyzed using unsupervised hierarchical cluster analysis (C). Adapted from
reference 59
. ....................................................................................................................... 18
Figure 4.The as-recorded Raman spectra of normal cervical squamous cells and invasive
cervical cancer cells are shown in (A). Details of these Raman spectra in the fingerprint
region of 700 to 1800 cm-1
and the high wavenumber region of 2800 to 3100 cm-1
are
enlarged in (B) and (C), respectively, for display. Adapted from reference 60
. ................ 21
Figure 5. SERS-based molecular sentinel (MS) nanoprobes. The MS nanoprobe shown
on the left of the figure is in the closed state and generates a strong SERS signal due to
the proximity between the Raman label and the silver nanoparticle. In the presence of the
complementary target DNA, the MS nanoprobe switches to the open state as shown on
the right of the figure, and the SERS signal is significantly reduced due to the separation
of the Raman label from the silver nanoparticle. Adapted from reference 76
. .................. 25
Figure 6. In vivo glucose detection using SERS. A rat with a surgically implanted sensor
and optical window was examined by a conventional laboratory Raman spectroscopy
system (A). The SERS-based sensor was fabricated using silver films over nanosphere
(AgFON) (B). The resultant nano-structure (C) is shown using an atomic force
microscope. After functionalization, a reflectance spectrum (D) was collected to
determine the position of the localized surface plasmon resonance (LSPR). Adapted from
reference 84
. ....................................................................................................................... 27
Figure 7. In vivo SERS detection of tumor biomarker EGFR using ScFv-antibody
conjugated gold nanoparticles. The bottom panels show the experimental setup. The top
panels show spectra obtained from the tumor (red) and the liver (blue) by using targeted
(A) and non-targeted (B) nanoparticles. In vivo SERS spectra were clearly observed from
the tumor site using targeted nanoparticles, but not with non-targeted nanoparticles.
Adapted from reference 88
. ................................................................................................ 28

viii
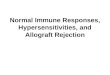
Figure 8. shows a typical Grade-1R (mild rejection) endomyocardial biopsy examined by
(a, b, c) Raman spectroscopy and (d) histopathology with haematoxylin & eosin (H&E)
stain. Raman spectra and the locations at which they are obtained are numbered
accordingly in Figure 8(a) and (c), with rejected Raman spectra (I758 > I718) and their
corresponding locations marked in red. Rejection-specific spectral regions of the 10th
and
11th
Raman spectra are shaded in Figure 8(a) and enlarged in Figure 8(b) for better
visualization. The H&E stained picture of an adjacent tissue section is shown in Figure
8(c). The distribution of rejected Raman spectra matches that of lymphocytes, and the
distribution of normal Raman spectra (I758 > I718) matches that of normal cardiac muscle.
Scale bars are 100 m. Adapted from reference 67
. .......................................................... 38
Figure 9. A Grade-1R (mild rejection) endomyocardial biopsy is examined by (a)
histopathology with haematoxylin & eosin (H&E) stain and (b, c, d) Raman
spectroscopy. Raman spectra and the locations at which they are obtained are numbered
in Figure 9(c) and (b), with rejected Raman spectra (I758 > I718) and their corresponding
locations (Number 1~11) marked in red. Rejection-specific spectral regions of the 11th
and 12th
Raman spectra are shaded in Figure 9(c) and enlarged in Figure 9(d) for display.
Locations of moderate lymphocyte infiltration and cardiac myocyte necrosis observed in
the H&E image (a) are seen to conform with those of rejected Raman spectra (b, c). Scale
bars are 100 m. Adapted from reference 122
. .................................................................. 39
Figure 10. Rejection-specific Raman spectral features are clearly observed at 758 cm-1
and 678 cm-1
where the average of rejected Raman spectra (1) shows elevated intensities
when compared to averaged normal Raman spectrum (2). Spectral comparison with
naturally occurring indoles, including serotonin (3), 5-methoxytryptophan (4), 5-
hydroxyindoleacetic acid (5), melatonin (6), 5-hydroxytryptophan (7), and tryptophan (8)
reveals that Raman bands of serotonin coincide with the spectral differences observed
between normal and rejected heart biopsies. Adapted from reference 67
. ........................ 43
Figure 11. Multivariate statistical analysis PCA also confirms the separation of rejected
Raman spectra from normal ones. Separation achieved by this statistical method is
consistent with that obtained by the intensity ratio test where normal (I758 ≤ I718) and
rejected (I758 > I718) Raman spectra are marked in blue and red, respectively. Adapted
from reference 67
. .............................................................................................................. 46
Figure 12. SERS spectra of serotonin and its solutions mixed with gold colloids (a, d) are
shown at (1) pH=1.6, (2) pH=2.2, (3) pH=3.0, (4) pH=4.1, (5) pH=5.0, (6) pH=6.1, (7)
pH=7.1. SERS spectra of tryptophan and its solutions mixed with gold colloids (b, e) are
shown at (1) pH=1.6, (2) pH=2.1, (3) pH=3.0, (4) pH=4.1, (5) pH=5.0, (6) pH=6.0, (7)
pH=7.1. (c) Averaged AEFs of serotonin (red) and tryptophan (blue) at various pH levels
are obtained from 8 measurements and presented with their respective pK1. Adapted from
reference 25
. ....................................................................................................................... 50
Figure 13. SERS intensity of serotonin is a reversible function of the pH values. The top
panel shows the intensities at 816 cm-1 at varying pH levels. HCl was added first to

ix
decrease the pH values from 5 to 1 (red), and then NaOH was added to bring the pH
values back to 1.5, 3 and 5 for comparison (blue). Corresponding spectra are shown in the
lower panel. ....................................................................................................................... 53
Figure 14. (a) SERS spectrum of serotonin at 5×10-6
mol/L (1), and ordinary Raman
spectrum at 0.1mol/L (2). (b) SERS spectrum of tryptophan at 5×10-6
mol/L (1), and
ordinary Raman spectrum at 5×10-2
mol /L (2). Adapted from reference 25
. .................... 55
Figure 15. The SERS spectra (a) of serotonin (1), tryptophan (2), melatonin (3) and 5-
HIAA (4) are shown, all at concentration 5×10-6
mol/L. SERS spectra of four different
mixtures containing various indolic components, all at 5×10-6
mol/L, are marked in blue,
with their respective NNLS fit in red and fitting residuals in grey. The compositions in
the four mixtures are serotonin and tryptophan (5), serotonin, tryptophan, melatonin and
5-HIAA (6), serotonin and 5-HIAA (7), serotonin, tryptophan and 5-HIAA (8),
respectively. Relative concentrations of the indolic components in the four mixtures are
normalized with respect to serotonin (b). Serotonin, tryptophan, melatonin and 5-HIAA
are marked with circles (○, red), squares (□, blue), diamonds(◊, green) and triangles(△,
brown), respectively. Adapted from reference 25
. ............................................................. 58

x
Abstract
Raman Spectroscopy Detects Cardiac Allograft Rejection with Molecular Specificity
Qiang Tu
Advisor: Chang Chang, PhD
Optical techniques capable of in vivo and molecularly specific detection of disease
markers are continuously being sought after with the goal of replacing invasive biopsy
procedures that incur tissue incision and morbidity. Raman spectroscopy, with its
chemical and molecular specificity as well as its intrinsic detection capability without the
need for exogenous labeling and fixation, presents an attractive opportunity for minimally
invasive in vivo diagnostics. However, medical applications of Raman spectroscopy have
been largely limited by the complexity of tissue constituents. As a result, complicated
post-experiment data processing is required and the attainable information is limited to a
set of given a priori sample constituents, such as collagen, cholesterol and phospholipids.
This work overcame such limitation by directly detecting a specific biomarker of cardiac
allograft rejection and showed that spatially resolved Raman spectroscopy is capable of
making molecular specific detection at the tissue level without exogenous labeling. This
molecular specificity is achieved by detecting the strong and characteristic Raman
spectral signature of serotonin, whose selective existence in rejected heart transplants
serves as the molecular marker. By combining both medical and physical sciences, this
work demonstrates the potential use of Raman spectroscopy in replacing the
endomyocardial biopsy as the standard for post-transplantation rejection surveillance and
presents a new paradigm in advancing clinical care.

xi
The particular indole implicated in this study, serotonin, corroborates the increasingly
recognized role of serotonin receptors in various immune responses including cardiac
allograft rejection. Serotonin is both a ubiquitous neurotransmitter in the central nervous
system and an important immunomodulator involved in various immune responses. The
ability to unambiguously detect serotonin is therefore imperative in biomedical research.
However, detection of serotonin and related indoles using immunohistochemistry has
been largely limited by their small molecule size and the resultant uncertainty in antibody
specificity. Here Surface-enhanced Raman spectroscopy (SERS) is showed to be capable
of detecting and distinguishing serotonin from its various closely related precursors and
metabolites. Comparing with traditional antibody-based methods, SERS is highly specific
and capable of real-time detection. We expect this optical detection method to directly
benefit a variety of immune and nervous systems studies involving serotonin.


1
CHAPTER 1. INTRODUCTION
Heart transplantation is the therapy of last resort for patients with end-stage heart
failure and its efficacy relies on the successful management of the recipient immune
response1. Endomyocardial biopsy is the current standard of care for post-transplantation
rejection surveillance of cardiac allografts2. Tissue samples are retrieved from the
endocardium of the right ventricle and the severity of allograft rejection is graded
histopathologically3,4
. Like other biopsy procedures, endomyocardial biopsy is invasive,
subject to sampling errors, and causes morbidity and rarely mortality. Its finite
turnaround time also incurs unwanted patient anxiety. A less invasive and potentially
real-time in vivo diagnostic method is therefore desired.
Minimally invasive optical techniques capable of differentiating between diseased
and normal tissues are attractive alternatives to invasive biopsy procedures. By probing
the intrinsic molecular vibrations, Raman spectroscopy is capable of chemical and
molecular specific detections without the need for exogenous labeling. In addition, no
tissue removal or sectioning is required. The wavelengths of a typical probing laser and
the Raman scattered light are both in the non-ionizing infrared region, further facilitating
its use for in vivo biomedical applications. Minimally invasive optical fiber-based
insertion devices such as catheters and endoscopes are also readily available5,6
. More
recently, Raman spectroscopy has been used to classify regions of diseased and normal
tissues, and the underlying compositional differences can be determined given a priori
knowledge of the tissues’ constituents, such as fat, collagen, cell nucleus, cell cytoplasm,
and -carotene7,8
. However, wider adoption of Raman spectroscopy in clinical settings

2
has yet to be seen primarily due to the complicated post-experiment data processing and
the resultant difficulty in obtaining molecular specificity. Here we utilize the strong and
characteristic Raman spectral features of an aromatic amino acid derivative, serotonin, to
directly identify rejected cardiac allografts. The potential use of Raman spectroscopy in
detecting ring-structured endogenous molecular markers for clinical applications is
demonstrated.
This work is the first approach to use Raman spectroscopy to detect heart transplant
rejection. An optical biomarker was discovered and used for the effective detection by
Raman spectroscopy. It is the first SERS analysis on serotonin and its related molecules
including melatonin and 5-HIAA to my best knowledge. This work successfully qualifies
the relative concentrations of indole molecules in mixed solution.

3
CHAPTER 2. BACKGROUND
2.1 Raman Spectroscopy
Raman spectroscopy is a powerful technique which detects molecules vibrations by
Raman scattering. It is widely used to obtain molecular structure information,
qualitatively identify the substances, and quantitatively or semi-quantitatively determine
the amounts of substances in a sample, which can be solid, liquid, or vapor. Raman
spectroscopy typically uses a non-ionizing laser as the excitation source. The incident
photons can be absorbed, scattered, and/or pass through the material without interaction.
If the energy of the incident photon matches the energy gap between the ground state and
an excited state of a molecule, the photon will most likely be absorbed and the molecule
is promoted to the excited state. Fluorescence occurs when the excited molecule
subsequently relaxes to the ground state by emission. Scattering takes place on the other
hand as the incident photon distorts the electron clouds. Two types of scattering typically
exist in the visible-light and near infrared (NIR) spectral range, Rayleigh and Raman
scattering. The more intense form, Rayleigh scattering, happens when only the electron
clouds are distorted. This is considered an elastic process as no appreciable energy
exchange occurs. However, if the vibrational state of the molecule is altered, energy
transfer occurs, either from the photon to the molecule or vice versa. The process
becomes inelastic and is named Raman scattering. This is in general a weak process
involving approximately one in every 106~10
8 scattered photons.
9-11
Depending on the direction of energy transfer between the molecule and the photon,
Raman scattering can be further categorized into two subtypes: Stokes and anti-Stokes.
Stokes scattering takes place when the molecule absorbs energy from the incident photon

4
and elevates itself from a lower energy state to an excited vibrational state. On the other
hand, due to thermal perturbation or prior external excitation, the molecule may already
be in an excited vibrational state before interacting with the incident photon. In this case
anti-Stokes scattering may result such that the molecule releases energy upon interacting
with the incident photon and subsequently returns to a lower energy state. The scattered
photons in an anti-Stokes process therefore are of higher energy than the incident photons.
Since at room temperature most molecules are in the ground state, Stokes scattering
typically dominates. Stokes scattering is therefore commonly recorded for Raman
spectroscopy unless special experimental conditions are arranged. Raman band shifts, i.e.
the energy difference between the incident and scattered photons, are typically described
in wavenumber. The most commonly used unit to denote wavenumber is cm-1
, and it is
equivalent to joule by a conversion factor (hc), where h is the Planck constant and c is the
speed of light. Figure 1 illustrates the Rayleigh, Stokes and anti-Stokes scattering
processes.

5
Figure 1. Energy diagram for Rayleigh and Raman scattering processes. Rayleigh
scattering is the most intense scattering process, and Stokes scattering predominates
over anti-Stokes scattering at room temperature. Thickness of the arrows indicates
the relative intensity of the three processes (not to scale). Adapted from reference 12
.
A typical laboratory Raman spectroscopy system is shown in Figure 2. The incident
laser irradiates the sample via an optical microscope, and the Raman scattered photons
are collected into a spectrometer following appropriate filtering. Lasers at various visible-
light and NIR wavelengths can be used as the excitation source. For example, a HeNe
laser has a wavelength of 633 nm, and a Ti: sapphire laser is tunable from 650 nm to
1100 nm. When examining biological samples, longer wavelength excitations typically
produce less fluorescence background and are therefore preferred.

6
Figure 2. A typical laboratory Raman spectroscopy system. Adapted from reference 12
.

7
2.2 Surface Enhanced Raman Spectroscopy
Surface-enhanced Raman spectroscopy (SERS) increases the Raman signal level by
exploiting the interaction between the molecule and a nano-scale metal surface. Raman
signals thus emitted are strongly enhanced by a factor of 103 – 10
14, depending on the
definition of the enhancement factor.13,14
For substrate-based SERS experiments, the
most widely used definition for average SERS enhancement factor is SERS Surf
RS Vol
I NEF
I N ,
where SERSI and RSI are the SERS and regular Raman intensity, respectively. VolN is the
average number of molecules in the scattering volume for regular Raman, and SurfN is
the average number of adsorbed molecules in the scattering volume for SERS. For SERS
in colloidal solutions, the analytical enhancement factor or apparent enhancement factors
(AEF) are calculated by SERS SERS
RS RS
I CAEF
I C , where SERSI and RSI are SERS and regular
Raman intensities of normalized Raman spectra at the selected band, respectively. SERSC
and RSC are concentrations of the target molecule in colloidal and aqueous solutions,
respectively. SERS is capable of detecting molecules in extremely low concentrations,
making it an attractive technique for biomedical applications.
Although the exact theoretical foundation of SERS is still illusive, it is generally
agreed that SERS consists of two major underlying physical mechanisms: the
electromagnetic field effect and the chemical charge transfer effect.15,16
The
electromagnetic effect is a result of the excitation of surface plasmon by the incident laser,
while the charge transfer effect is caused by the electron exchange between the molecule

8
and the metal colloid.17
Surface plasmon is the resonant oscillation of conduction
electrons on a metal surface induced by an electromagnetic field. It is well known that the
exposure of surface plasmon to laser irradiation increases the lattice temperature,18,19
and
this surface plasmon induced heat generation has been identified as the potential cause of
SERS signal reduction seen in prolonged irradiation of nanoparticles.20
Note that since
SERS results from the interaction between the molecule under test and the nano-scale
metal surface, the band shifts, relative peak intensity, and peak bandwidths in the SERS
spectra are different from those in the Raman spectra of the same molecule.
2.3 Analysis Methods in Raman Spectroscopy
Raman spectra obtained from biological samples often contain significant amounts of
fluorescence background. Since Raman spectral differences between normal and diseased
tissues are generally subtle, effective data processing algorithms are often required for
data analysis and interpretation.
2.3.1 Fluorescence background removal
As mentioned above, Raman spectra collected from tissues are composed mainly of
Raman scattering and intrinsic tissue fluorescence. To eliminate the fluorescence
background, a polynomial function that fits to the fluorescence profile is usually
subtracted from the Raman spectra.21-24
While there is no consensus on the optimal order
of the polynomial function, fourth- and fifth-order polynomials are most commonly
employed.24-28

9
2.3.2 Multivariate data analysis
Raman spectra contain various overlapping Raman bands. As a result, it is difficult to
visually inspect and interpret the spectral data. Multivariate spectral analysis methods are
often used to process the Raman spectra and facilitate data interpretation. Spectral
analysis methods are generally categorized as either supervised or unsupervised. For
unsupervised analyses, such as cluster analysis (CA) and principle component analysis
(PCA), no a priori knowledge of class characteristics is required but to be determined
from the analysis itself. In contrast, in a supervised analysis, the number of classes and
representative samples of each class are known a priori, as is the case in linear
discriminant analysis (LDA), regression analysis and artificial neural networks (ANN).29
Several commonly used analysis methods are introduced below.
2.3.2.1 Hierarchical clustering
Hierarchical clustering is a cluster analysis method in which Raman spectra are
grouped according to their similarities defined by the distance matrices. A distance
matrix measures dissimilarity among a group of objects, i.e. Raman spectra in this case.
For example, the most commonly used distance metric is the Euclidean distance where a
Raman spectrum with p wavenumbers is expressed as 1 2[ , , ]px x xx , and the
distance between two Raman spectra ix and jx is defined as
1
22
1
( ) ( )p
ij i j ik jk
k
d x x
x x . The clustering process is repeated at different levels
to produce a tree structure, called the dendrogram, and the spectra from normal and

10
diseased samples are discriminated at the end of the process. Hierarchical clustering is
widely used in analytical Raman spectroscopy.30,31
2.3.2.2 Principle component analysis
Principle component analysis (PCA) is one of the most commonly used unsupervised
classification method in Raman spectroscopy. Raman spectra contain intensity
information obtained at a large number of different wavenumbers. Each of these
wavenumbers can be regarded as an independent dimension, on which the Raman
spectral data is measured. PCA reduces the dimensionality of the original Raman data set
with most of its variance retained in the selected principle components.21,26,32-36
PCA has
been successfully used in multivariate Raman spectral analysis and is widely accepted for
data interpretation. A brief overview of PCA is provided below for a typical diagnostic
Raman spectral data classification process.
The set of Raman spectra obtained from a diagnostic experiment can be expressed as
an m by n matrix X,
11 12 13 1
21 22 23 2
31 32 33 3 1 2 3
1 2 3
n
n
n n
m m m mn
x x x x
x x x x
x x x x
x x x x
X x x x x ,
where n is the number of Raman spectra taken in the experiment, m is the total number of
spectral wavenumbers, and ix is a column vector of length m representing the i
th Raman
spectrum. The covariance matrix CX of the original Raman data set X can then be

11
determined, as well as the eigenvectors of CX. The resulting eigenvector matrix W is
given by
1 2 3 mW w w w w ,
where iw is a column vector of length m representing the i
th eigenvector of CX. Note that
the eigenvectors are arranged with descending eigenvalues, i.e. decreasing contributions
to the overall variance of the Raman data set.
The principle component scores P is obtained by projecting the original Raman data
set X onto the new basis spanned by the eigenvectors, i.e.
T
1 2 3 m P W X p p p p ,
where pi is a column vector of length n representing the scores of the ith
principle
component for each of the n measurements in the Raman data set. Since the principle
components corresponding to the largest eigenvalues account for most of the variations in
the data set, classification of Raman spectra in most cases can be achieved with these first
few principle components. PCA is therefore a powerful analytic tool for dimensionality
reduction in Raman spectroscopy.
2.3.2.3 Linear discriminant analysis
Linear discriminant analysis (LDA) is another commonly used spectral data
classification method. Since the projection axes produced by PCA do not always provide
clear boundaries for between-class discrimination, LDA is often used to improve the
class separation following PCA. One of the most common LDA approaches is Fisher’s
criterion. It is a supervised analysis that maximizes the between-class variance while

12
minimizing the within-class variance in a set of Raman spectra. Effective class separation
is achieved by projecting the Raman data into a new eigenvector set.26,37-40
This method
applied to a two-class problem is briefly described below.
Within-class and between-class scatter matrices are used to formulate the criterion.
The within-class scatter matrix is defined as
T
1,2 i
W i i
i C
x
S = (x -m )(x -m ) ,
where x is a column vector representing an individual Raman spectrum in class iC , and
im is the mean of the Raman spectra in class iC , i =1,2. The between-class scatter
matrix is given by
T
1 2 1 2( )( )B S = m m m m ,
where 1m and 2m are defined above. The Fisher’s criterion function, T
T( ) B
W
J w S w
ww S w
is
used to evaluate the classification. A vector w that maximizes the function ( )J w is the
solution to the generalized eigenvalue problem B WS w S w . The eigenvector w is then
used as the new basis vector. Once the data set is transformed onto this vector, Euclidean
distance can be used for data classification. However, some data located in the middle of
the two classes might not be easily categorized.
2.3.2.4 Artificial neural network
While LDA can only discriminate classes that are linearly separable, artificial neural
network (ANN) is a nonlinear method capable of multi-dimensional bounding problems.

13
ANN emulates the process of human mind by employing artificial neuron functions in
which each neuron provides an output value based on multiple inputs. Typically, an ANN
consists of multiple layers, including the input layer, the hidden layer and the output layer.
Neurons on the input layer take the Raman spectral data as inputs and the classifications
are made at the output layer. Each neuron in the hidden layers sums up the inputs from
neurons in preceding layers with certain weights. These “middle” neurons then send out
their outputs after some nonlinear operations, such as hyperbolic tangents, step functions,
and sigmoid functions. The weights are computed using a set of known data during the
training process. The number of hidden layers, the neuron functions, and the form of the
data are crucial parameters for an effective ANN design.41
Note that which Raman
spectral features to be used as inputs should be carefully chosen for optimal classification.
One example of Raman spectral analysis using ANN is the single-cell diagnosis of
colorectal cancer.42
2.3.2.5 Ordinary least squares regression
Ordinary least squares (OLS) is a commonly used linear regression method that
minimizes the sum of squared distances between experimental data and the
corresponding fitted curve. OLS is often used to determine the compositional
concentrations of a tissue sample, where the sample spectrum is fitted to the individual
composition’s Raman spectra and a weighted sum is obtained from the fitting
coefficients.31,43
Briefly, the Raman spectrum of a tissue sample (or solution mixture) can
be expressed as an m × 1 column vector T
1 2 3 my y y yy , where m is the
number of wave numbers at which Raman shifts are recorded. Similarly, Raman spectra

14
of its component chemicals can be expressed as column vectors and put together as an m
× n matrix Z,
11 12 13 1
21 22 23 2
31 32 44 3
1 2 3
n
n
n
m m m mn
z z z z
z z z z
z z z z
z z z z
Z ,
where n is the number of component chemicals, and m is the same set of wavenumbers as
defined above. The OLS coefficient T
1 2 3 n β needs to satisfy
y Zβ u , where u is an m × 1 error vector. OLS minimizes the residual sum
of squares 2 T( ) ( )SSR y - Zβ y - Zβ y - Zβ by setting the derivative of SSR with
respect to β equal to 0. The OLS estimator β̂ is then calculated to be T 1 Tˆ ( )β Z Z Z y .44
Considering that the weights of components are positive, a nonnegativity constraint is
applied in this case to avoid negative fitting coefficients and this variant of OLS is called
nonnegative least squares (NNLS).

15
CHAPTER 3. CURRENT RELATED RESEARCH
3.1 Current Research Using Raman Spectroscopy
3.1.1 Cancer detection
Cancer is the second most common cause of death in the United States.45
Efficacious
cancer treatments rely on early detection and accurate diagnosis. Various Raman
spectroscopic studies on cancers have been reported,31,36,46-49
and here we review its use
on three most commonly seen carcinomas, i.e. breast, colorectal and cervical cancers.
3.1.1.1 Breast Cancer
Breast cancer has the highest rate of occurrence in the United States among the
female population in 2010.45
Numerous studies have investigated the application of
Raman spectroscopy on the detection of normal, precancerous and cancerous breast
tissues.22,34,43,50,51
For instance, Haka and colleagues have demonstrated the ability of
Raman spectroscopy to distinguish between normal, benign, and malignant lesions of
breast ex vivo, with a sensitivity of 94% and a specificity of 96%.43
Tissues in four
pathological conditions were examined and classified, including normal, fibrocystic
change, fibroadenoma, and infiltrating carcinoma. Raman spectra of breast tissues were
fitted to those of individual breast tissue components including fat, collagen, cell nucleus,
epithelial cell cytoplasm, calcium oxalate, calcium hydroxyapatite, cholesterol-like lipid
deposits, and -carotene. This approach is based on the assumption that the Raman
spectrum of a mixture is a linear combination of the spectra of its components. Variations
in the fitting coefficients reflected the chemical and morphologic changes of the breast
tissue due to carcinogenesis. Fitting coefficients of fat and collagen have been identified
as the key parameters used for diagnostic differentiation. Normal breast tissues are

16
composed of fat predominately, and all abnormal breast tissues show increased
percentage of collagen, due to the formation of fibrosis. Fibroadenoma can then be
further separated from infiltrating carcinoma by its lower fat content, since fibroadenoma
grows by pushing the fat aside while infiltrating carcinoma infiltrates between fat cells
and retained the fat in situ. These results were consistent with known breast pathology
and therefore validate the use of Raman spectroscopy for breast cancer detection ex vivo.
The clinical potential of Raman spectroscopy was also demonstrated by the same authors
with the use of an optical fiber probe for in vivo Raman studies.50
The spectral data were
analyzed in real time and the diagnosis results were displayed intraoperatively.
Rehman and co-workers quantitatively examined the Raman spectral differences
between different grades of invasive ductal carcinoma (IDC) and ductal carcinoma in situ
(DCIS).52
For both IDC and DCIS, the spectral intensity of selected Raman peaks
increased with advancing grades, indicating Raman spectroscopy’s potential for
quantitative carcinoma grading.
Instead of examining breast tissues directly, Pichardo-Molina’s group studied serum
samples from breast cancer patients and demonstrated the use of Raman spectroscopy for
minimally invasive diagnostics.40
Seven Raman band ratios were used for classification
and spectral differences were observed between serum samples of breast cancer patients
and normal healthy subjects. Using principle component analysis (PCA) and linear
discriminant analysis (LDA), the sensitivity and specificity were reported to be 97% and

17
78%, respectively. However, the underlying molecular mechanism of these differences
was not reported.
Raman spectroscopic imaging technique has gained popularity recently in cancer
research.30,53-56
Comparing with other standard imaging methods such as
immunofluorescence and immunohistochemisty, Raman spectroscopic imaging is capable
of visualizing the samples without extrinsic labeling, thus minimizing sample
perturbation. In addition, the much needed chemical and structural information of the
sample are provided by Raman spectral analysis.57,58
Mariani and co-workers have
applied Raman imaging to the detection of nuclear membrane lipid fluctuations in
senescent epithelial breast cancer cells.59
In this study, Raman images were composed
based on the Raman peak intensity of CH- stretching [Figure 3(B)]. Subcellular localities
such as the nucleus were accurately imaged, and differences in lipid and glycoprotein
components were detected.

18
Figure 3. Visual (A) and Raman imaging (B, C) of single control and senescent
MCF-7/NeuT cells. Raman images (B) were composed specifically from CH-
stretching, and were analyzed using unsupervised hierarchical cluster analysis (C).
Adapted from reference 59
.

19
3.1.1.2 Cervical Cancer
Cervical cancer is the second most common malignancy in women worldwide, with
more than half a million cases diagnosed and approximately 288,000 related death each
year.60
Currently Papanicolaou smear is the most commonly used screening method for
cervical cancer with a detection specificity of 96.8%, but a sensitivity of only 55.4%.61
Raman research in this area has focused on achieving comparable or better specificity
and sensitivity numbers than the Papanicolaou smear.
Algorithms were designed to discriminate between normal and diseased cervical
tissues. Using a logistic regression algorithm Robichaux-Viehoever, et al. were able to
distinguish high-grade dysplasia from benign tissues with a sensitivity of 89% and a
specificity of 81%.62
The spectra were collected in vivo using a fiber-optic probe.5
Employing non-linear algorithms, Kanter and colleagues achieved a sensitivity of 98%
and a specificity of 96%.63
They have also reported that by incorporating into their
algorithm the patient’s hormonal status, particularly the menstrual cycle and the
menopausal state, the classification accuracy can be further improved.64
New experimental techniques have also been used to improve detection accuracy in
cervical cancer. While most Raman studies are performed in the “fingerprint” spectral
region with wavenumbers below 1500 cm-1
,9 Mo and colleagues have investigated the
high wavenumber region (2800 ~ 3700 cm-1
) for cervical cancer diagnosis, and achieved
a diagnostic specificity and sensitivity of 97.8% and 93.5%, respectively.38
Kamemoto’s
group compared the use of both fingerprint (775 ~ 975 cm-1
) and high wavenumber
regions (2800 ~ 3100 cm-1
) for in vitro cervical cancer detection, and found that Raman

20
bands at the low wavenumber region [Figure 4(B)] provide more information on specific
molecular and chemical changes in the tissue, while Raman spectra at the high
wavenumber region [Figure 4(C)] have higher detection sensitivity due to stronger
Raman signals and significantly less fluorescence background from the optical fibers.38,60
Molecular etiology of the observed Raman spectral differences between normal and
diseased cervical tissues was also studied.32,60
Comparison between normal and
malignant cervical tissues showed that Raman spectra from normal cervical tissues
feature characteristics of structural proteins such as collagen. For malignant cervical
tissues, sharper amide I, minor red shift in CH2 and sharper amide III indicated the
presence of DNA, lipids and non-collagen proteins.

21
Figure 4.The as-recorded Raman spectra of normal cervical squamous cells and
invasive cervical cancer cells are shown in (A). Details of these Raman spectra in the
fingerprint region of 700 to 1800 cm-1
and the high wavenumber region of 2800 to
3100 cm-1
are enlarged in (B) and (C), respectively, for display. Adapted from
reference 60
.

22
3.1.1.3 Colorectal Cancer
Colorectal cancer is the third most common malignancy in the United States.45
An
estimated 142,570 new cases and 51,370 related deaths are expected for 2010. Current
standard of practice utilizes a white-light endoscope to screen and excise biopsies on
suspected sites. Difficulty exists in that early neoplasia and subtle lesions might evade the
endoscopic survey, and biopsies are impractical for patients with multiple suspicious
lesions.65
Optical biopsy using Raman spectroscopy is therefore an attractive alternative.
Several groups have thus investigated and developed effective detection/classification
algorithms. Widjaja and colleagues, for instance, combined PCA and support vector
machines (SVM) to classify different types of pathologic colonic tissues, including
normal, polyps and cancers. Sensitivity and specificity greater than 98% have been
reported.65
Beljebbar, et al. investigated the spatial distribution of molecular changes on
the adenocarcinoma ex vivo.30
Pseudo-color maps of normal and cancerous colonic
tissues were generated using Raman spectra of individual tissue constituents, including
proteins, lipids, collagen, nucleic acid and mucus. These Raman maps were shown to
correlate with hematoxylin and eosin (H&E) stains, demonstrating the use of proteins and
nucleic acids as potential spectroscopic biomarkers for the differentiation of
adenocarcinomatous tissues.
Laser Tweezers Raman spectroscopy (LTRS) has also been investigated for single-
cell colorectal cancer diagnosis.66
At the early stages of colon cancer development, the
epithelium layer on the luminal surface carries diagnostic information while the
underlying bulk tissues are mostly irrelevant. In order to minimize the fluorescence
background from the bulk tissues, laser tweezers are used to trap single cells from the

23
epithelium and inspect them in isolation using Raman spectroscopy. Sensitivity of 86.3%
and specificity of 86.3% have been reported with LTRS.42
3.1.2 Allograft rejection
Allograft transplantation is the last resort therapy for patients with failed organs. Its
efficacy relies on the successful management of the recipient’s immune responses.
Several studies using Raman spectroscopy to detect acute allograft rejection after
transplantation have shown promising results.67-69
Raman spectroscopy has been used to
detect acute rejection after renal transplantation. Acute rejection typically occurs in 15% -
20% of the patients within the first year of renal transplant, and currently the most
commonly used diagnostic indicator is serum creatinine elevation (SCE). However, this
method has been shown to have low sensitivity and specificity, since serum creatinine
level can be affected by other disease conditions. In addition, serum creatinine level
elevates only after significant histological damages have already taken place.68
. Using
Raman spectroscopy, Brown, et al. observed significant spectral differences between
activated and naive T lymphocytes, and reported a sensitivity and specificity of 95.7%
and 100%, respectively.69
This result demonstrates the potential of Raman spectroscopy
as a minimally invasive screening tool for acute renal transplantation rejection.

24
3.2 Current research using SERS
3.2.1 SERS for biomarkers
SERS has been used to detect various biomolecules and proteins, such as glucose,
hemoglobins, RNAs and pathogens.70-73
Detection using SERS is especially
advantageous for small signaling molecules that often lack recognizable epitopes for
antibody-based immunohistochemistry. For instance, Huang and co-workers conjugated
gold nanorods to anti-epidermal growth factor receptor (anti-EGFR) antibodies and
demonstrated its use as a potential cancer diagnostic tool.74
Due to its large curvatures,
gold nanorod in theory has the strongest surface electromagnetic field compared with
other colloid shapes.75
In this study, gold nanorods were coated with poly(styrene
sulfonate) to stabilize the colloids and to reverse the surface charge polarity from
negative to positive for antibody conjugation. Minimal Raman signals were observed on
normal cells, while significantly stronger Raman signals were detected on cancer cells,
demonstrating specific antibody binding. The detection specificity was provided by the
antibody and the SERS signal served simply as the readout. Other novel SERS based
techniques such as the nanoprobe technology were also developed.76-78
As an example,
the molecular sentinel (MS) nanoprobe consisted of a DNA hairpin probe with one end
binding to a silver nanoparticle, and the other tagged with a SERS signal reporter. In the
absence of the target DNA, significant SERS signals were observed since the SERS
signal reporter was close enough to the silver nanoparticle on the other end of the folded
stem-loop structure [Figure 5 (left)]. While in the presence of the complementary target
DNA, the SERS signal was significantly reduced due to the semi-loop unfolding and
separation of the SERS signal reporter from the silver nanoparticle [Figure 5 (right)].
Multiplexing was achieved by mixing two MS nanoprobes specific to the breast cancer

25
biomarker genes, erbB-2 and ki-67, to simultaneously detect both target DNAs present in
the sample.
Figure 5. SERS-based molecular sentinel (MS) nanoprobes. The MS nanoprobe
shown on the left of the figure is in the closed state and generates a strong SERS
signal due to the proximity between the Raman label and the silver nanoparticle. In
the presence of the complementary target DNA, the MS nanoprobe switches to the
open state as shown on the right of the figure, and the SERS signal is significantly
reduced due to the separation of the Raman label from the silver nanoparticle.
Adapted from reference 76
.

26
3.2.2 SERS for in vivo detection
The application of SERS for in vivo diagnostics in complex living systems is a
challenging task. Surface of the nanoparticle must be biocompatible and placed in vivo
without causing damage to the living system. In addition, the in vivo environments are
awash with a variety of molecules and contaminants that may deactivate the SERS
surface or interfere with the interested Raman signals. Moreover, the concentrations of all
molecules, both targets and contaminants, are constantly changing. Recently several
successful in vivo SERS experiments have been demonstrated.79-83
Stuart and colleagues
performed in vivo SERS on rats and quantitatively determined glucose concentration in
the interstitial fluid.84
The SERS-based sensor was fabricated using silver films over
nanosphere (AgFON) [Figure 6(B)]. Hydrophilic pockets were formed around the sensor
and partitioned glucose to the SERS-active surface, while excluding other molecules in
the interstitial fluid such as plasma proteins. A glass window was surgically placed on the
rat, allowing the sensor to be in contact with interstitial fluid and optically accessible for
Raman spectroscopy [Figure 6(A)]. In their more recent work,85
the window was
removed and SERS spectra were collected transcutaneously. In order to obtain Raman
signals deeper in the tissues, spatially offset Raman spectroscopy (SORS) was applied, in
which the Raman scattered light was collected with a spatial offset from the point of laser
incidence.86,87
In another recent study, Qian and co-workers demonstrated in vivo tumor
detection using SERS with PEGylated gold nanoparticles.88
The SERS sensor was
prepared by binding the reporter molecule diethylthiatri-carbocyanine (DTTC) to the gold
colloids. A mixture of thiol-PEG and a heterofunctional PEG (SH–PEG–COOH) was
then coated to stabilize the gold colloid-DTTC complex. Cancer cell-specific single-chain
variable fragment (ScFv) B10 antibodies were conjugated at the last step. As shown in

27
Figure 7(C), the sensor was injected through tail vein into the mice bearing human head
and neck tumors. Highly resolved SERS signals were observed specifically at the tumor
site [Figure 7(A, B)]. Keren’s group demonstrated in vivo Raman imaging in a similar
study using single-walled carbon nanotubes (SWNT).89
Since SWNTs inherently exhibit
a strong Raman peak at 1593 cm-1
, Raman imaging using SWNTs does not rely on SERS
reporter molecules and therefore requires fewer conjugation processes.
Figure 6. In vivo glucose detection using SERS. A rat with a surgically implanted
sensor and optical window was examined by a conventional laboratory Raman
spectroscopy system (A). The SERS-based sensor was fabricated using silver films
over nanosphere (AgFON) (B). The resultant nano-structure (C) is shown using an
atomic force microscope. After functionalization, a reflectance spectrum (D) was
collected to determine the position of the localized surface plasmon resonance
(LSPR). Adapted from reference 84
.

28
Figure 7. In vivo SERS detection of tumor biomarker EGFR using ScFv-antibody
conjugated gold nanoparticles. The bottom panels show the experimental setup. The
top panels show spectra obtained from the tumor (red) and the liver (blue) by using
targeted (A) and non-targeted (B) nanoparticles. In vivo SERS spectra were clearly
observed from the tumor site using targeted nanoparticles, but not with non-
targeted nanoparticles. Adapted from reference 88
.

29
3.3 Emerging techniques of Raman spectroscopy
3.3.1 Single-walled carbon nanotube
Single-walled carbon nanotube (SWNTs) is an useful diagnostic tool in
nanomedicine.90-94
It has been shown that conjugation to SWNT improves the
permeability, as well as enhances the retention, of various functional moieties in the
tumor tissues.95,96
This enhanced permeability and retention (EPR) effect of SWNT has
been explored for drug delivery where various biomolecules such as chemotherapeutic
agents, proteins and DNA were conjugated to SWNT and delivered to tumor sites.97-100
SWNT’s intrinsic Raman peak at 1593 cm-1
(G-band) is typically used as the
unambiguous marker to detect SWNT conjugates in drug delivery and Raman imaging
studies.101-104
In an in vivo cancer drug delivery study, paclitaxel (PTX), a chemotherapy
drug was conjugated to SWNTs and injected into mice.99
Raman spectroscopy was used
to quantify the pharmacokinetics and biodistribution of this SWNT-PTX conjugate
without any radio or fluorescent label. Raman imaging is another area where SWNT finds
important applications.89,102
Zavaleta and co-workers have shown noninvasive Raman
imaging of tumors on mice in vivo using SWNTs.102
The SWNTs were linked to
arginine-glycine-asparatic acid (RGD) peptides, which specifically target integrin v3,
an integrin overexpressed in angiogenic vessels and various tumor cells. After
subcutaneous injection of this SWNT-RGD conjugate, in vivo Raman images of tumor
were obtained using SWNT’s G-band intensity. In a more recent study, Liu et al.
successfully performed multicolor Raman imaging of living cells by multiplexing
different isotope compositions.105
SWNTs made of carbon-12 (12
C), carbon-13 (13
C), and
12C/
13C mix were used and each presented different G-band peak positions at 1590, 1528,
and 1544 cm-1
, respectively. These three types of SWNTs were conjugated to Herceptin

30
(anti-Her2), Erbitux (anti-Her1), and arginine-glycine-aspartic acid (RGD) peptides,
recognizing Her2/neu, Her1/EGFR, and integrin v3 cell-surface receptors, respectively.
These SWNT conjugates are then administered in vitro and after incubation, multiplexed
three-color Raman images were obtained, clearly identifying the existence of the three
targeted cell receptors. Note that G-band spectral positions are key to distinguishing the
three multiplexed colors in Raman imaging and it was recently shown that up to five
different colors could be achieved by varying the 12
C/13
C ratios in SWNTs.106
3.3.2 Multiplexed SERS imaging
Multiplexed Raman imaging is capable of detecting multiple targets simultaneously
and it has attracted great interests recently.107-110
Gold nanoparticles are typically used as
the tag in multiplexed SERS imaging for their narrow and strong SERS bands. In
addition, silica coated gold nanoparticles are biocompatible and nontoxic. In a recent
work, Zavaleta et al. achieved five color multiplexed Raman imaging in vivo using five
SERS nanotags adsorbed on gold nanoparticles.111
Each nanotag generated a unique
Raman signal, which is used as a multiplexed channel and assigned an arbitrary color in
the resultant image. These five types of nanotagged gold nanoparticles were
simultaneously injected through the tail vein and accumulated in the liver where a
multiplexed five color Raman image was obtained.
Using functionalized silver nanoparticles, Kennedy and co-workers demonstrated
multiplexed SERS imaging of cell surface proteins in vitro.112
SERS signals from four
differently functionalized nanoparticles were separated using least square fitting and the
spatial co-localization between the targeted proteins were visualized in the multiplexed

31
SERS image. Other in vitro multiplexed SERS imaging works include cancer cell line
identification where specific nanotags were used to recognize their respective biomarkers
found on cancer cells.113
3.3.3 Photothermal effect
Photothermal effect is an important feature of metal nanoparticles. The exposure of
metal nanoparticles to laser induces an increase in temperature.18
Application of this
laser-induced thermal effect in Raman spectroscopy has recently been demonstrated
where plasmon heating was used to produce SERS-active micro spots on colloidal
crystals.114
Polystyrene (PS) colloidal nanospheres were first coated with a 10nm layer of
gold nanoparticles and then with a 50 nm layer of amorphous TiO2 deposited by atomic
layer deposition (ALD). The resulting PS/Au/TiO2 core/shell nanospheres are assembled
as colloidal crystals. When irradiated by a laser beam, the gold interlayer was strongly
absorbing and the heat generated decomposed the polymeric spheres. A bowl-like pit was
formed as a result, and the SERS effect of Methylene Blue adsorbed on these spots was
demonstrated.
3.3.4 Core-Shell nanoparticle structure for improved SERS reproducibility
Strong signal enhancement, high reproducibility and stability are critical for effective
SERS phenomenon.115
SERS studies using metal nanoparticles typically suffer from the
desorption of Raman labels or target molecules from the metal surface, and the
interference from the environment such as non-target molecules and other surrounding
metal nanoparticles. A core-shell structure offers an effective solution to those stochastic
interventions, in that the shell capsulates the Raman labels or target molecules around the

32
metal core and prevents the adsorption of other molecules as well as the aggregation of
nanoparticles themselves. Various shell materials have been investigated, including
polymers, silica and metal.88,116-119
Among them, the stability and biocompatibility of
silica makes it an attractive choice in medical research. Li and co-workers have
developed ultra-thin silica-coated gold nanoparticles with strong SERS signal and
minimal gold aggregations.116
Using etching technology, Roca’s group developed silica-
void-gold nanoparticles to prevent aggregations while allowing molecules to diffuse
through the porous silica membranes and interact with the entrapped gold core.120
In a
more recent study Lim et al. have demonstrated gold core–shell nanoparticles with highly
uniform and reproducible SERS signals.121
The Raman labels trapped within the gap
generated strong and highly quantitative SERS signals with 633 nm laser excitation. The
development of new nanoparticles continues to expand the application of Raman
spectroscopy in biology and medicine.
Table 1 summarizes the applications of Raman spectroscopy reviewed above,
including the types of analysis, experimental apparatus, and analysis methods.

33
Table 1. Diagnostic applications of Raman spectroscopy. Adapted from reference 12
.
Raman application
Experimental setup
Analysis method Reference Wavelength
(nm) Power (mW)
Exposure time (s) Other
Cancer detection
Breast cancer
830 100~150 10~30 Nonnagative least square (NNLS) 43
830 82~125 1 Probe NNLS 50
786 N/A 4 Raman shifts 52
830 65 10 PCA-LDA 40
514.5 8 N/A Hierarchical cluster 59
Cervical cancer
785 80 5~15 Probe Logistic regression 62
785 80 5 Probe Maximum representation and discrimination feature (MRDF) 63
Sparse multinomial logistic regression (SMLR)
785 15 60 Probe PCA-LDA 38
785 10 60 Raman shifts 60
785 100 30 PCA 32
Colorectal cancer
785 300 5 Probe PCA-Support vector machines (SVM) 65
785 70 N/A
PCA 30
Hierarchical cluster
Multiple least squares (MLS)
782.5 11.5 60 LTRS PCA-Logistic regression 66
782.5 11.5 60 LTRS PCA-Artificial neural network (ANN) 42
Allograft rejection
Cardiac rejection
785 100 10 PCA 67
Renal rejection
785/514.5 8~12 10 PCA-Discriminant function analysis (DFA) 69
SERS for Biomarker
785 100 20 NNLS 25
785 25 10 Raman shifts 74
633 N/A N/A Raman shifts 76
SERS for in 785 50 120 Partial least squares 84

34
vivo 785 20 2 Raman shifts 88
SWNT
N/A 100 2 Raman imaging using G-band 99
785 100 3/10 Raman imaging using G-band 102
785 80 0.5 Raman imaging using G-band 105
SERS imaging
785 60 N/A Raman imaging using SERS peaks 111
633 N/A N/A Raman imaging using SERS peaks 112
Core-shell nanoparticle
633 0.5/4 30/60 Raman shifts 116
633 2 50 Raman shifts 120
633 0.3 10 Raman shifts 121

35
CHAPTER 4. DETECTION OF CARDIAC TRANSPLANT REJECTION USING
RAMAN SPECTROSCOPY
4.1 Materials and Methods
4.1.1 Endomyocardial Biopsy
Endomyocardial biopsies are obtained from heart transplant patients during regular
surveillance biopsy procedures. The biopsy sample is stored at -80 °C until use, at which
time the sample is cryo-sectioned to 4 m thickness and examined by histopathology
using haematoxylin & eosin (H&E). The remaining biopsy section adjacent to the 4 m
slice is examined by Raman spectroscopy. The pathological results are withheld until the
end of the study period, after which time the comparison with Raman spectra was made.
A number of Raman spectra are obtained at different randomly selected locations within
each biopsy specimen depending on the sample size. This procedure emulates the in vivo
clinical environment where an optical fiber is inserted through the cardiac catheter and
samples randomly selected endocardium sites. Patient selection criteria follow the
guideline set by United Network for Organ Sharing (UNOS). Briefly, the patient will be
excluded if the patient is pregnant, or if the patient develops systemic diseases that will
affect the heart at anytime after the transplant, such as malignancy, amyloidosis,
sarcoidosis, HIV, sepsis from infections of virus, bacteria, and fungus. The patient is also
not eligible if refuse to sign consent for this study. A total of 17 patients are included in
this study.
4.1.2 Raman Spectroscopy Setup
Endomyocardial biopsies are passively thawed at room temperature and put between
two calcium fluoride slides (Buck Scientific, East Norwalk, CT) for Raman spectroscopy

36
experiment. The edges of the calcium fluoride slides are sealed by petrolatum to prevent
the biopsy samples from dehydration. The Raman spectroscopy experiments are
conducted using a confocal Raman microscope, equipped with a 100mW 785nm
wavelength single-line diode laser (LabRAM HR800, HoribaJobinYvon, Edison, NJ). All
data are acquired using a 10X objective (NA=0.25) with a spot size of 100 m at the
sample. Shutter setting is fixed at 10 sec exposure time with 180 accumulations
throughout the experiment. A 600 lines/mm grating is used and the range of wavenumber
recorded is between 522 cm-1
and 1253 cm-1
. The intensity of the obtained Raman spectra
is peak-normalized at 718 cm-1
, which is associated with membrane phospholipids and
relatively stable. Intensity exhibit is offset vertically for display. No background
subtraction is performed in order to preserve the integrity of the original data. The study
was approved by the Institutional Review Board of Drexel University College of
Medicine and all subjects gave informed consent.
4.2 Results and Analysis
To establish the validity of Raman spectroscopy in detecting cardiac allograft
rejection, comparative studies are performed on endomyocardial biopsies using both
Raman spectroscopy and standard histopathology. Spatially resolved Raman spectra are
obtained from the biopsy at randomly selected locations and the result is compared with
an adjacent tissue section stained by H&E. “Rejected” Raman spectra is defined
quantitatively as the intensity at 758 cm-1
surpasses that of the adjacent Raman band at
718 cm-1
, i.e. when I758 > I718. Comparison is then made between the locations at which
rejected Raman spectra are observed and the distribution of lymphocytes in the H&E

37
stained image. Figure 8 shows a typical Grade-1R (mild rejection) endomyocardial
biopsy examined by Raman spectroscopy (a, b, c) and histopathology (d). Rejected
Raman spectra and their corresponding positions are marked in red in Figure 8(a, b, c).
Agreement between Raman and histopathological results are clearly observed as the
distribution of rejected Raman spectra overlap with lymphocyte aggregation. This result
confirms the ability of Raman spectroscopy to detect cardiac allograft rejection.

38
Figure 8. shows a typical Grade-1R (mild rejection) endomyocardial biopsy
examined by (a, b, c) Raman spectroscopy and (d) histopathology with haematoxylin
& eosin (H&E) stain. Raman spectra and the locations at which they are obtained
are numbered accordingly in Figure 8(a) and (c), with rejected Raman spectra
(I758 > I718) and their corresponding locations marked in red. Rejection-specific
spectral regions of the 10th
and 11th
Raman spectra are shaded in Figure 8(a) and
enlarged in Figure 8(b) for better visualization. The H&E stained picture of an
adjacent tissue section is shown in Figure 8(c). The distribution of rejected Raman

39
spectra matches that of lymphocytes, and the distribution of normal Raman spectra
(I758 > I718) matches that of normal cardiac muscle. Scale bars are 100 m. Adapted
from reference 67
.
Figure 9. A Grade-1R (mild rejection) endomyocardial biopsy is examined by (a)
histopathology with haematoxylin & eosin (H&E) stain and (b, c, d) Raman
spectroscopy. Raman spectra and the locations at which they are obtained are
numbered in Figure 9(c) and (b), with rejected Raman spectra (I758 > I718) and their
corresponding locations (Number 1~11) marked in red. Rejection-specific spectral
regions of the 11th
and 12th
Raman spectra are shaded in Figure 9(c) and enlarged in
Figure 9(d) for display. Locations of moderate lymphocyte infiltration and cardiac
myocyte necrosis observed in the H&E image (a) are seen to conform with those of
rejected Raman spectra (b, c). Scale bars are 100 m. Adapted from reference 122
.

40
To evaluate the feasibility of Raman spectroscopy for clinical applications, each
individual endomyocardial biopsy is classified by Raman spectroscopy as either normal
or rejected according to the percentage of rejected Raman spectra found on the biopsy.
This classification is then compared with the histopathological reading. It is found that
Raman spectroscopy indeed consistently identifies Grade-1R biopsies by detecting the
abnormal intensity increase at 758 cm-1
. For 11 out of the 12 Grade-1R biopsies
examined, rejected Raman spectra consistently account for more than 35% of the spectra
obtained while only 1 out of 17 Grade-0 biopsies exhibits such property (Table 2).
Results here show that increased frequency of occurrence of rejected Raman spectra
obtained at randomly selected locations on a biopsy correlates with elevated immune
response, suggesting that cardiac allograft rejection can be identified by the relative
occurrence of rejection specific Raman spectra.

41
Table 2. Summary of the histopathological readings of the biopsy samples and the
results of their Raman spectroscopy studies. A biopsy is defined as “rejected” by
Raman spectroscopy if more than 35% of its Raman spectra are abnormal, i.e.
I758/I718 > 1. Using this definition, eleven out of the twelve Grade-1R biopsies are
classified as rejected by Raman spectroscopy, while only 1 out of 17 Grade-0
biopsies display such property. Adapted from reference 67
.
Sample Grade Total Spectra
number
Abnormal
I758/I718 > 1
Normal
I758/I718 ≤ 1
Abnormal
Percentage
1
Grade 0
12 0 12 0%
2 15 0 15 0%
3 13 0 13 0%
4 15 0 15 0%
5 7 4 3 57%
6 17 1 16 6%
7 6 1 5 17%
8 19 2 17 11%
9 17 0 17 0%
10 5 0 5 0%
11 15 3 12 20%
12 15 0 15 0%
13 15 0 15 0%
14 14 1 13 7%
15 16 1 15 6%
16 6 0 6 0%
17 14 0 14 0%
Subtotal 221 13 208 6%
18
Grade 1R
2 2 0 100%
19 14 5 9 36%
20 22 11 11 50%
21 24 22 2 92%
22 5 5 0 100%
23 24 14 10 58%
24 23 2 21 8%
25 12 5 7 42%
26 19 11 8 58%
27 22 10 12 45%
28 22 9 13 41%
29 16 6 10 38%
Subtotal 205 102 103 50%

42
The observed Raman spectral difference between normal and rejected biopsies at 758
cm-1
is a well-known characteristic of indole ring vibration123
and comparison with
various indole derivatives’ Raman spectra implicates a particular indole, serotonin, as the
underlying molecular marker instigating the observed spectral difference. The abnormal
intensity increase at 758 cm-1
has been quantitatively defined above as I758 > I718, and is
consistently observed in all of the 12 Grade-1R biopsies examined. Since this 758 cm-1
Raman band is a well-known characteristic of indole ring vibration,123
Raman spectra of
several naturally occurring indoles are examined for comparison with normal and
rejected Raman spectra. Averages of 311 normal and 115 rejected Raman spectra are
obtained, together with the Raman spectra of serotonin, tryptophan, melatonin, 5-
hydroxyindoleacetic acid, 5-hydroxytryptophan, and 5-methoxytryptophan. As seen in
Figure 10, in addition to the 758 cm-1
band which is common to all indoles, rejected
Raman spectra contain an additional band at 678 cm-1
which is unique to serotonin. The
Raman spectral difference observed between rejected and normal heart biopsies is
therefore attributed to serotonin, a known immunomodulator.124
By detecting the
selective existence of indoles in rejected cardiac allografts, Raman spectroscopy’s
molecular specific detection capability for clinical applications is demonstrated.

43
Figure 10. Rejection-specific Raman spectral features are clearly observed at 758
cm-1
and 678 cm-1
where the average of rejected Raman spectra (1) shows elevated
intensities when compared to averaged normal Raman spectrum (2). Spectral
comparison with naturally occurring indoles, including serotonin (3), 5-
methoxytryptophan (4), 5-hydroxyindoleacetic acid (5), melatonin (6), 5-
hydroxytryptophan (7), and tryptophan (8) reveals that Raman bands of serotonin
coincide with the spectral differences observed between normal and rejected heart
biopsies. Adapted from reference 67
.

44
Minimally invasive optical techniques capable of differentiating between diseased
and normal tissues are attractive alternatives to invasive biopsy procedures. By probing
the intrinsic molecular vibrations, Raman spectroscopy is capable of chemical and
molecular specific detections without the need for exogenous labeling. In addition, no
tissue removal or sectioning is required. The wavelengths of a typical probing laser and
the Raman scattered light are both in the non-ionizing infrared region, further facilitating
its use for in vivo biomedical applications. Minimally invasive optical fiber-based
insertion devices such as catheters and endoscopes are also available.5,125
More recently,
Raman spectroscopy has been used to classify regions of diseased and normal tissues,126
and the underlying compositional differences can be determined given a priori
knowledge of the tissues’ constituents, such as fat, collagen, cell nucleus, cell cytoplasm,
and -carotene.7,8
However, wider adoption of Raman spectroscopy in clinical settings
has yet to be seen primarily due to the lack of specific biomarkers with strong and
characteristic Raman scattering signals. Here distinct Raman spectral features of an
indole ring are consistently identified in rejected endomyocardial biopsies and used to
detect cardiac allograft rejections. In addition, these Raman spectral signatures of rejected
biopsies are attributed to a particular indole derivative, serotonin, which is known to
mediate various immune responses.124,127
The detection of cardiac allograft rejection by
Raman spectroscopy is shown to agree with histopathological results and the potential
use of Raman spectroscopy in detecting ring-structured endogenous molecular markers
for clinical applications is demonstrated.

45
A particular indole derivative, serotonin, is implicated here as the biomarker for
cardiac allograft rejection. Serotonin is a well-known neurotransmitter whose immune
modulation effects have gained increasing recognition recently.128-130
Serotonin is
released by platelets at the sites of tissue injury131
and has been shown to regulate various
immune responses such as delayed-type hypersensitivity,132
phagocytosis,133
and mast
cell chemotaxis.134
Serotonin is also implicated in the pathogenesis of a variety of
inflammatory disorders, such as asthma, inflammatory bowel syndrome, and chronic
eczema. Recently serotonin has been shown to promote T-cell activation and
proliferation,135
the primary immune mechanism responsible for allograft rejection.136
For
cardiac allograft rejection in particular, the role of serotonin has recently been suggested
as a serotonin receptor antagonist prolongs the life span of heart transplants in mice.127
Given the diverse arrays of serotonin receptor isoforms expressed differentially by
various immune cells,124
we expect serotonin to involve in a wider range of immune
responses.137
Such expectation, if realized, will further broaden the clinical utility of
Raman spectroscopy.
A multivariate statistical method, principle component analysis (PCA), is employed
here to confirm the validity of the intensity ratio test (I758 > I718) used above. PCA is an
unsupervised statistical method typically used in spectral chemometrics. Such statistical
methods are also useful for larger amounts of data often encountered in clinical settings.
Here PCA is used to confirm the spectral separation observed by the intensity ratio test
between normal and rejected Raman spectra. Comparison of PCA with intensity ratio test
yields consistent results where separation between rejected (I758 > I718, red) and normal

46
(I758 < I718, blue) Raman spectra is clearly observed (Figure 11). In addition, PCA enables
the visualization of data clustering and as a result will be useful for future clinical
deployment of Raman spectroscopy.
Figure 11. Multivariate statistical analysis PCA also confirms the separation of
rejected Raman spectra from normal ones. Separation achieved by this statistical
method is consistent with that obtained by the intensity ratio test where normal (I758
≤ I718) and rejected (I758 > I718) Raman spectra are marked in blue and red,
respectively. Adapted from reference 67
.

47
The characteristic Raman band of indole rings at 758 cm-1
, together with an adjacent
and relatively stable membrane phospholipids band at 718 cm-1
, permits the use of
intensity ratio test as the quantitative measure for detecting heart transplant rejection with
Raman spectroscopy. In addition, the consistent emergence of serotonin’s unique Raman
band at 678 cm-1
in rejected biopsy specimens essentially enables direct spectral
identification. Results obtained with this method, which utilizes characteristic Raman
signatures of the disease biomarker serotonin, are confirmed by PCA. Note that
serotonin’s other Raman bands at 824 cm-1
and 938 cm-1
overlap with those of collagen
as well as other commonly seen molecules in the tissue, and as a result can not be used
for rejection identification. Fluorescent noises existed in the Raman spectra can also
cause variations between the classification results obtained with intensity ratio test and
PCA. To achieve improved signal quality, we therefore intend to examine spectral
regions with wavenumbers greater 1500 cm-1
, where interference from fluorescence is
expected to be minimal.
Sophisticated data processing, namely background subtraction, is specifically avoided
here in order to preserve data integrity. While commonly employed for qualitative
display of spectra, it is well known that background subtraction causes subsequent
statistical analysis such as PCA to fail. It is primarily due to the artificial variance
introduced into the spectra when one subjectively fits and removes higher-order
polynomials as the background.138-140
Despite this fact, use of background subtraction
continues to exist in clinical Raman applications where data interpretation depends on
complicated spectral data processing. We would like to point out that, to the best of our

48
knowledge, it presents the first experimental result where differentiability between
normal and diseased states is clearly observable in original Raman spectra without the
need for data processing. Such observation is also verified by PCA, an objective
multivariate statistical analysis.

49
CHAPTER 5. SERS STUDY OF INDOLIC MOLECULES ADSORBED ON GOLD
COLLOIDS
5.1 Materials and Methods
Serotonin, tryptophan, melatonin, and 5-HIAA (≥98% purity) are purchased from
Sigma-Aldrich Co. (St. Louis, MO). Gold colloids are purchased from Structure Probe,
Inc. (West Chester, PA), with a size of 20nm, and a concentration of ~ 7.0×1011
per ml.
The mixed solutions are then excited by a near infrared (NIR) integrated Raman system
(LabRam800HR, Horiba Jobin Yvon, Edison, NJ) with 100mW 785 nm wavelength
single-line diode laser. The exposure time is 20 seconds.
Apparent enhancement factor (AEF) is calculated following the standard in the
literature.13
An averaged AEF is calculated using ten Raman bands within the spectral
range (Fig. 2). A linear regression method, nonnegative least squares (NNLS),141
is used
to quantify the relative concentration of indolic molecules mixed in the gold colloidal
solution. By fitting the SERS spectrum of the mixture as a weighted sum of those of
individual indoles, the NNLS coefficients are proportional to the product of indole
concentration and its AEF.
5.2 Results and Analysis
SERS intensities observed correlate strongly with varying pH value (Figure 12). Both
serotonin and tryptophan are ampholytes in aqueous solutions, with serotonin having a
hydroxyl and an amine group, and tryptophan a carboxyl and an amine group. Since the
electrostatic status of serotonin and tryptophan changes with pH, their electrostatic

50
interaction with the negatively charged gold colloid surface also changes with the pH
level. SERS spectra of the solutions were taken at various pH levels, all at a
concentration of 5×10-6
mol/L.
Figure 12. SERS spectra of serotonin and its solutions mixed with gold colloids (a, d)
are shown at (1) pH=1.6, (2) pH=2.2, (3) pH=3.0, (4) pH=4.1, (5) pH=5.0, (6) pH=6.1,
(7) pH=7.1. SERS spectra of tryptophan and its solutions mixed with gold colloids (b,
e) are shown at (1) pH=1.6, (2) pH=2.1, (3) pH=3.0, (4) pH=4.1, (5) pH=5.0, (6)
pH=6.0, (7) pH=7.1. (c) Averaged AEFs of serotonin (red) and tryptophan (blue) at
various pH levels are obtained from 8 measurements and presented with their
respective pK1. Adapted from reference 25
.

51
The onset of SERS is observed as the pH value drops below pI and approaches pK1,
at which levels the molecules begin to be positively charged. The electrostatic interaction
between the negatively-charged gold colloids and the positively-charged molecules
contributes to the SERS phenomenon. The pK1, pK2, and pI of serotonin are 4.9, 9.8, and
7.35 respectively. For tryptophan, pK1 and pK2 are 2.38 and 9.34 respectively, and its pI
is 5.86.142
Indeed as seen in Figure 12(a, b, c) SERS effects are observed at pH level
lower than 6.1 for serotonin, and lower than 5.0 for tryptophan. As the pH value
continues to decrease toward pK1, more amine groups are protonated and stronger SERS
signal is observed.
At pH levels below their respective pK1, serotonin and tryptophan molecules are fully
protonated in solution and strong SERS effects are observed. As shown in Figure 12(a, c),
serotonin’s SERS spectra become significantly stronger as the pH values approach and
decrease beyond its pK1. Likewise for tryptophan as shown in Figure 12(b, c), strong
SERS effects are observed at pH=1.6, 2.1 and 3.0. Additionally in Figure 12(c), one also
observes that SERS spectral intensity continues to increase as pH level drops below pK1.
It is likely a result of gold nanoparticles aggregating with the positively-charged
ampholytes, forming 3D complexes.143
These 3D nanostructures induce greater SERS
enhancement than 1D or 2D nanostructures.144

52
The emergence of SERS is also seen to be accompanied by color changes in the
solution. As described above, the pH dependence of SERS is attributed to the protonation
of ampholytes and the aggregation of gold nanoparticles. Similarly the observed color
change at low pH values is a result of colloid aggregation. This is because the
accumulation of gold colloids alters the surface plasmon characteristics and light
absorption by the surface plasmon determines the color of the solution. At pH levels
where strong SERS signals are observed, i.e. below pH 5.1 for serotonin and below pH
3.0 for tryptophan, the solutions [Figure 12(d) and (e)] are light blue. At higher pH levels
where SERS phenomenon disappears, the solution is pink in color. In addition, for pure
gold colloid solutions with neither serotonin nor tryptophan present, this color change
phenomenon was also observed although at a much lower pH level (pH = 2.0). These
observations suggest that the existence of highly protonated molecules such as serotonin
and tryptophan in this case facilitates gold colloid aggregation, which in turn enhances
the SERS phenomenon.
A reversible correlation in SERS intensity with respect to pH levels is also observed.
As described above, serotonin is an ampholyte in aqueous solutions, with a hydroxyl and
an amine group. Since the electrostatic status of serotonin changes with pH, their
electrostatic interaction with the negatively charged gold colloid surface also changes
with the pH level, which in turn results in changes in SERS intensity. Figure 13 shows
SERS intensity changes as a function of serotonin solution’s pH level. SERS intensity of
the serotonin/gold colloid solution increases as the pH level decreases from 5.0 to 1.0 by
adding HCl. NaOH is subsequently added to the solution to raise the pH level back to 5.0.

53
At pH=1.5, 3.0 and 5.0, SERS intensity reduces back to the same level as before NaOH
was added, which indicates that the electrostatic interaction between serotonin and gold
colloid surface is reversible. The result demonstrated that SERS is a reliable and
repeatable technique for the detection of serotonin.
Figure 13. SERS intensity of serotonin is a reversible function of the pH values. The
top panel shows the intensities at 816 cm-1 at varying pH levels. HCl was added first
to decrease the pH values from 5 to 1 (red), and then NaOH was added to bring the
pH values back to 1.5, 3 and 5 for comparison (blue). Corresponding spectra are
shown in the lower panel.
Specific Raman vibrational modes of an indole ring are examined for serotonin,
tryptophan, melatonin and 5-HIAA (Table 3). Substantially downward band shifts are
observed in SERS spectra of the four indolic molecules, comparing with their ordinary
Raman spectra, which indicate the interaction between the indole ring and the gold
colloidal surface. The two strong Raman bands at 757 and 937 cm-1
for serotonin are

54
assigned to the indole ring in-phase and out-of-phase breathing modes, respectively
(Figure 14). These two bands are downward shifted to 750 and 918 cm-1
in SERS
spectrum of serotonin. In addition, the band at 826 cm-1
in ordinary Raman spectrum of
serotonin is attributed to indole ring NH bending, which shifts to 816 cm-1
in the SERS
spectrum. Serotonin’s other indole Raman bands present these shifts as well, i.e. 460, 678,
1133, 1235, 1433 and 1549 cm-1
. Likewise, these clearly observable downward shifts of
indole Raman bands happen for tryptophan, melatonin and 5-HIAA, as shown in Table 3.
Table 3. Band assignments for the Raman and SERS spectra of serotonin,
tryptophan, melatonin and 5-HIAA. Adapted from reference 145
.
Assignment146-149
Serotonin Tryptophan Melatonin 5-HIAA
Raman
(cm-1
)
SERS
(cm-1
)
Raman
(cm-1
)
SERS
(cm-1
)
Raman
(cm-1
)
SERS
(cm-1
)
Raman
(cm-1
)
SERS
(cm-1
)
Indole ring stretching 460 450 460 421 458 429 457 451
Indole ring NH bending 678 632 575 565 663 634 679 624
Indole ring in-phase
breathing 757 750 757 749 751 745 751 744
Indole ring NH bending 826 816 877 868 819 813 841 826
Indole ring out-of-phase
breathing 937 918 1010 990 922 907 924 914
Benzene H scissoring 1133 1112 1132 1109 1133 1085 1130 1114
Benzene H scissoring
Pyrrole H rocking 1235 1221 1256 1226 1235 1219 1247 1215
Indole ring stretching 1433 1425 1430 1413 1428 1410 1432 1423
Indole ring stretching 1549 1518 1551 1521 1549 1513 1552 1519

55
Figure 14. (a) SERS spectrum of serotonin at 5×10-6
mol/L (1), and ordinary Raman
spectrum at 0.1mol/L (2). (b) SERS spectrum of tryptophan at 5×10-6
mol/L (1), and
ordinary Raman spectrum at 5×10-2
mol /L (2). Adapted from reference 25
.
The spectral shifts described above are consistent with previous studies in which the
indole NH band shifts downward following the formation of a hydrogen bond.150
The
indole NH group is a well-known proton donor, which tends to form hydrogen bonds
with negatively charged gold colloids. As a result, indole rings interact strongly with
colloidal gold, causing the indole NH band as well as other Raman bands of indole to
shift downward. These substantial downward shifts observed in our study suggest strong
interaction between the indole ring and the gold colloids. These observations are also
consistent with previous SERS studies of tryptophan using positively charged silver
colloids, where no significant Raman band shifts are recorded.146
The positively charged

56
silver colloidal surface prevents the formation of hydrogen bonds and as a result shuns
interaction with the ring structure of indole. In this study, we showed that using gold
colloids instead of silver enables one to exploit the strong Raman signals associated with
the indole ring structure.
SERS spectra are also obtained from solutions containing multiple indolic molecules,
all at concentrations of 5×10-6
mol/L, and NNLS fits are performed to determine their
relative concentration. In the first experiment, a solution containing both serotonin and
tryptophan is examined. SERS spectrum of this mixture (line 5 in Figure 15) is fitted with
those of serotonin (line 1 in Figure 15) and tryptophan (line 2 in Figure 15). The NNLS
coefficients for serotonin and tryptophan are 0.730 and 0.216, respectively. Taking into
consideration their respective averaged AEFs at 5×10-6
mol/L, which are 4.69×104 and
1.35×104 respectively, the NNLS fitting result gives a concentration ratio of serotonin to
tryptophan at (0.730/4.69×104) : (0.216/1.35×10
4) = 1.00 : 1.03, which is in good
agreement with the administered concentrations in the mixture. Similarly, a second
experiment is conducted where we obtain the SERS spectrum (line 6 in Figure 15) of a
solution containing serotonin, tryptophan, melatonin and 5-HIAA. NNLS fitting is
performed again with SERS spectra of these four individual indoles (line 1-4 in Figure
15). The NNLS fitted composition ratios are (0.503/4.69×104) : (0.147/1.35×10
4) :
(0.287/2.46×104) : (0.115/1.12×10
4) = 1.00 : 1.02 : 1.09 : 0.957 for serotonin, tryptophan,
melatonin and 5-HIAA respectively. This result is again in good agreement with
administered concentrations of serotonin, tryptophan, melatonin and 5-HIAA. Note that
the AEFs of melatonin and 5-HIAA are 2.46×104 and 1.12×10
4, respectively. A third and

57
a fourth experiment are performed using the same method. SERS spectra of the third
mixture containing serotonin and 5-HIAA (line 7 in Figure 15), and the forth mixture
containing serotonin, tryptophan and 5-HIAA (line 8 in Figure 15) are fitted using spectra
of their respective compositions. The relative concentration ratios are (0.830/4.69×104) :
(0.183/1.12×104) = 1.00 : 0.923 for serotonin and 5-HIAA in the third experiment, and
(0.627/4.69×104) : (0.181/1.35×10
4) : (0.146/1.12×10
4) = 1.00 : 1.00 : 0.975 for serotonin,
tryptophan and 5-HIAA in the fourth experiment. The relative concentration ratios for
these four mixtures are presented in Figure 15(b). These experiments demonstrate that the
relative concentration of serotonin with respect to other closely related indoles in a mixed
solution can be quantitatively determine from its SERS spectrum.

58
Figure 15. The SERS spectra (a) of serotonin (1), tryptophan (2), melatonin (3) and
5-HIAA (4) are shown, all at concentration 5×10-6
mol/L. SERS spectra of four
different mixtures containing various indolic components, all at 5×10-6
mol/L, are
marked in blue, with their respective NNLS fit in red and fitting residuals in grey.
The compositions in the four mixtures are serotonin and tryptophan (5), serotonin,
tryptophan, melatonin and 5-HIAA (6), serotonin and 5-HIAA (7), serotonin,
tryptophan and 5-HIAA (8), respectively. Relative concentrations of the indolic
components in the four mixtures are normalized with respect to serotonin (b).
Serotonin, tryptophan, melatonin and 5-HIAA are marked with circles (○, red),

59
squares (□, blue), diamonds(◊, green) and triangles(△, brown), respectively.
Adapted from reference 25
.

60
CHAPTER 6. CONCLUTION AND FUTURE WORK
Unlike prior Raman clinical applications, the need for complicated data processing is
overcome by employing the concept of a Raman biomarker, serotonin. Utilizing the
strong and specific Raman spectral characteristics of this indole biomarker, disease
differentiability is directly observable in the original Raman spectra. Furthermore, this
work has demonstrated the molecular specific detection capability of Raman
spectroscopy beyond the limitation of a set of a priori common tissue constituents. We
anticipate this new paradigm of disease specific “Raman optical biomarker” to stimulate
searches of other ring-structured biomolecules specific to disease models, and as a result
open up a wider application of Raman spectroscopy in clinical settings.
The direct optical detection of specific biomolecules that distinguish a diseased state
using Raman spectroscopy demonstrates its potential for in vivo molecular diagnostics.
Without the need for exogenous labeling, Raman spectroscopy complements
immunohistochemical methods for it is especially sensitive to small ring-structured
signaling molecules which are difficult to detect with conventional
immunohistochemistry. With the demonstrated new paradigm in utilizing Raman
spectroscopy and the advancements in biomarker discovery, Raman spectroscopy can
potentially become a clinically viable tool for minimally invasive, molecular specific, in
vivo diagnostics.
As the roles and functions of the 14 serotonin receptor subtypes in the immune
system continue to be discovered and defined,137,151,152
definitive detection techniques for
their common signaling molecule, serotonin, are critically needed. In addition, such

61
techniques need to be able to distinguish serotonin from its closely related precursors and
metabolites. Here we demonstrated the capability of SERS for such a task and we
envision increasing SERS applications in the study of immune responses.

62
CHAPTER 7. CONTRIBUTION
This work is the first approach to use Raman spectroscopy to detect heart transplant
rejection. Allograft transplantation is the last-resort therapy for patients with failed organs.
Its efficacy relies on the successful management of the recipient's immune responses. The
current standard surveillance method using endomyocardial biopsy is subject to sampling
errors, since only 4 samples are examined each time, the rejected site may be missed. It is
invasive and causes morbidity and rarely mortality, because of the open wounds left in
the heart. And it is subjective because the severity is determined by a pathologist. Here
the capability of Raman spectroscopy to detect cardiac rejection is demonstrated in this
work. To our best knowledge, this is the first approach to detect cardiac rejection using
Raman spectroscopy.
An optical biomarker was discovered and used for the effective detection by Raman
spectroscopy. Unlike prior Raman clinical applications, the need for complicated data
processing is overcome by employing the concept of a Raman biomarker, serotonin.
Utilizing the strong and specific Raman spectral characteristics of this indole biomarker,
disease differentiability is directly observable in the original Raman spectra. Furthermore,
this work has demonstrated the molecular specific detection capability of Raman
spectroscopy beyond the limitation of a set of a priori common tissue constituents. We
anticipate this new paradigm of disease specific “Raman optical biomarker” to stimulate
searches of other ring-structured biomolecules specific to disease models, and as a result
open up a wider application of Raman spectroscopy in clinical settings.

63
It is the first SERS analysis on serotonin and its related molecules including
melatonin and 5-HIAA to my best knowledge. Electrostatic interaction between the
positively charged amine on the serotonergic molecules and the negatively charged gold
colloidal surface plays a significant role in Raman surface enhancement phenomenon.
The detectable concentration is as low as 1×10-7
mol/L for serotonin and 3×10-7
mol/L
for tryptophan. The regular Raman peaks and SERS peaks in spectra of serotonin,
tryptophan, melatonin and 5-HIAA are also assigned in this work
This work successfully qualifies the relative concentrations of indole molecules in
mixed solution. It is shown that the relative concentration of serotonin, tryptophan,
melatonin and 5-HIAA in mixed solutions can be quantitatively determine from a SERS
spectrum, demonstrating the potential use of SERS for in vitro diagnostics. Further
optimization of the AEF is needed to allow in vivo diagnostics under physiological
conditions.

64
BIBLIOGRAPHY
1. Eisen HJ, Tuzcu EM, Dorent R, Kobashigawa J, Mancini D, Valantine-von
Kaeppler HA, et al. Everolimus for the prevention of allograft rejection and
vasculopathy in cardiac-transplant recipients. N Engl J Med 2003;349:847-58.
2. Al-khaldi A, Robbins RC. New directions in cardiac transplantation. Annu Rev
Med 2006;57:455-71.
3. Stewart S, Winters GL, Fishbein MC, Tazelaar HD, Kobashigawa J, Abrams J, et
al. Revision of the 1990 working formulation for the standardization of
nomenclature in the diagnosis of heart rejection. J Heart Lung Transplant
2005;24:1710-20.
4. Cunningham KS, Veinot JP, Butany J. An approach to endomyocardial biopsy
interpretation. J Clin Pathol 2006;59:121-9.
5. Utzinger U, Richards-Kortum RR. Fiber optic probes for biomedical optical
spectroscopy. J Biomed Opt 2003;8:121-47.
6. Mahadevan-Jansen A, Mitchell WF, Ramanujam N, Utzinger U, Richards-
Kortum R. Development of a fiber optic probe to measure NIR Raman spectra of
cervical tissue in vivo. Photochemistry and Photobiology 1998;68:427-431.
7. de Jong BW, Schut TC, Maquelin K, van der Kwast T, Bangma CH, Kok DJ, et al.
Discrimination between nontumor bladder tissue and tumor by Raman
spectroscopy. Anal Chem 2006;78:7761-9.
8. Haka AS, Shafer-Peltier KE, Fitzmaurice M, Crowe J, Dasari RR, Feld MS.
Diagnosing breast cancer by using Raman spectroscopy. Proc Natl Acad Sci USA
2005;102:12371-6.
9. Smith E, Dent G. Introduction, basic theory and principles. Modern Raman
spectroscopy : a practical approach. Hoboken, NJ: J. Wiley, 2005:1-5, 71-73.
10. Mansour HM, Hickey AJ. Raman characterization and chemical imaging of
biocolloidal self-assemblies, drug delivery systems, and pulmonary inhalation
aerosols: a review. AAPS PharmSciTech 2007;8:E99.

65
11. Gremlich H-U, Yan B. Infrared and raman spectroscopy of biological materials.
New York: M. Dekker, 2001.
12. Tu Q, Chang C. Diagnostic applications of Raman spectroscopy. Nanomedicine
2011;8:545-58.
13. Le Ru EC, Blackie E, Meyer M, Etchegoin PG. Surface enhanced Raman
scattering enhancement factors: a comprehensive study. J Phys Chem C
2007;111:13794-803.
14. Park WH, Kim ZH. Charge transfer enhancement in the SERS of a single
molecule. Nano Lett 2010;10:4040-8.
15. Fang Y, Seong NH, Dlott DD. Measurement of the distribution of site
enhancements in surface-enhanced Raman scattering. Science 2008;321:388-92.
16. Stiles PL, Dieringer JA, Shah NC, Van Duyne RP. Surface-enhanced Raman
spectroscopy. Annu Rev Anal Chem (Palo Alto Calif) 2008;1:601-26.
17. Campion A, Kambhampati P. Surface-enhanced Raman scattering. Chem Soc Rev
1998;27:241-50.
18. Lu X, Rycenga M, Skrabalak SE, Wiley B, Xia Y. Chemical synthesis of novel
plasmonic nanoparticles. Annu Rev Phys Chem 2009;60:167-92.
19. Link S, El-Sayed MA. Optical properties and ultrafast dynamics of metallic
nanocrystals. Annu Rev Phys Chem 2003;54:331-66.
20. Kho KW, Shen ZX, Lei Z, Watt F, Soo KC, Olivo M. Investigation into a surface
plasmon related heating effect in surface enhanced Raman spectroscopy. Anal
Chem 2007;79:8870-82.
21. Vidyasagar MS, Maheedhar K, Vadhiraja BM, Fernendes DJ, Kartha VB, Krishna
CM. Prediction of radiotherapy response in cervix cancer by Raman spectroscopy:
a pilot study. Biopolymers 2008;89:530-7.
22. Matousek P, Stone N. Prospects for the diagnosis of breast cancer by noninvasive
probing of calcifications using transmission Raman spectroscopy. J Biomed Opt
2007;12:024008.
23. Chan JW, Taylor DS, Zwerdling T, Lane SM, Ihara K, Huser T. Micro-Raman
spectroscopy detects individual neoplastic and normal hematopoietic cells.
Biophys J 2006;90:648-56.

66
24. Short KW, Carpenter S, Freyer JP, Mourant JR. Raman spectroscopy detects
biochemical changes due to proliferation in mammalian cell cultures. Biophys J
2005;88:4274-88.
25. Tu Q, Eisen J, Chang C. Surface-enhanced Raman spectroscopy study of indolic
molecules adsorbed on gold colloids. J Biomed Opt 2010;15:020512.
26. Teh SK, Zheng W, Ho KY, Teh M, Yeoh KG, Huang Z. Diagnostic potential of
near-infrared Raman spectroscopy in the stomach: differentiating dysplasia from
normal tissue. Br J Cancer 2008;98:457-65.
27. Lau DP, Huang Z, Lui H, Anderson DW, Berean K, Morrison MD, et al. Raman
spectroscopy for optical diagnosis in the larynx: preliminary findings. Lasers Surg
Med 2005;37:192-200.
28. Crow P, Molckovsky A, Stone N, Uff J, Wilson B, WongKeeSong LM.
Assessment of fiberoptic near-infrared raman spectroscopy for diagnosis of
bladder and prostate cancer. Urology 2005;65:1126-30.
29. Adams MJ, Royal Society of Chemistry (Great Britain). Chemometrics in
analytical spectroscopy. 2nd ed. Cambridge: Royal Society of Chemistry, 2004.
30. Beljebbar A, Bouche O, Diebold MD, Guillou PJ, Palot JP, Eudes D, et al.
Identification of Raman spectroscopic markers for the characterization of normal
and adenocarcinomatous colonic tissues. Crit Rev Oncol Hematol 2009;72:255-64.
31. de Jong BWD, Bakker TC, Maquelin K, van der Kwast T, Bangma CH, Kok DJ,
et al. Discrimination between nontumor bladder tissue and tumor by Raman
spectroscopy. Anal Chem 2006;78:7761-9.
32. Krishna CM, Prathima NB, Malini R, Vadhiraja BM, Bhatt RA, Fernandes DJ, et
al. Raman spectroscopy studies for diagnosis of cancers in human uterine cervix.
Vib Spectrosc 2006;41:136-41.
33. Jess PR, Smith DD, Mazilu M, Dholakia K, Riches AC, Herrington CS. Early
detection of cervical neoplasia by Raman spectroscopy. Int J Cancer
2007;121:2723-8.
34. Chowdary MV, Kumar KK, Kurien J, Mathew S, Krishna CM. Discrimination of
normal, benign, and malignant breast tissues by Raman spectroscopy.
Biopolymers 2006;83:556-69.

67
35. Schlücker S, Kustner B, Punge A, Bonfig R, Marx A, Strobel P. Immuno-Raman
microspectroscopy: In situ detection of antigens in tissue specimens by surface-
enhanced Raman scattering. J Raman Spectrosc 2006;37:719-21.
36. Crow P, Barrass B, Kendall C, Hart-Prieto M, Wright M, Persad R, et al. The use
of Raman spectroscopy to differentiate between different prostatic
adenocarcinoma cell lines. Br J Cancer 2005;92:2166-70.
37. Das K, Stone N, Kendall C, Fowler C, Christie-Brown J. Raman spectroscopy of
parathyroid tissue pathology. Lasers Med Sci 2006;21:192-7.
38. Mo J, Zheng W, Low JJ, Ng J, Ilancheran A, Huang Z. High wavenumber Raman
spectroscopy for in vivo detection of cervical dysplasia. Anal Chem
2009;81:8908-15.
39. Teh SK, Zheng W, Ho KY, Teh M, Yeoh KG, Huang Z. Diagnosis of gastric
cancer using near-infrared Raman spectroscopy and classification and regression
tree techniques. J Biomed Opt 2008;13:034013.
40. Pichardo-Molina JL, Frausto-Reyes C, Barbosa-Garcia O, Huerta-Franco R,
Gonzalez-Trujillo JL, Ramirez-Alvarado CA, et al. Raman spectroscopy and
multivariate analysis of serum samples from breast cancer patients. Lasers Med
Sci 2007;22:229-36.
41. Lewis IR, Edwards HGM. Handbook of Raman spectroscopy : from the research
laboratory to the process line. New York: Marcel Dekker, 2001.
42. Zheng F, Qin Y, Chen K. Sensitivity map of laser tweezers Raman spectroscopy
for single-cell analysis of colorectal cancer. J Biomed Opt 2007;12:034002.
43. Haka AS, Shafer-Peltier KE, Fitzmaurice M, Crowe J, Dasari RR, Feld MS.
Diagnosing breast cancer by using Raman spectroscopy. Proc Natl Acad Sci U S
A 2005;102:12371-6.
44. Hanlon EB, Manoharan R, Koo TW, Shafer KE, Motz JT, Fitzmaurice M, et al.
Prospects for in vivo Raman spectroscopy. Phys Med Biol 2000;45:R1-59.
45. American Cancer Society. Cancer Facts & Figures 2010. Atlanta: American
Cancer Society, 2010.
46. Haka AS, Volynskaya Z, Gardecki JA, Nazemi J, Shenk R, Wang N, et al.
Diagnosing breast cancer using Raman spectroscopy: prospective analysis. J
Biomed Opt 2009;14:054023.

68
47. Ghanate AD, Kothiwale S, Singh SP, Bertrand D, Krishna CM. Comparative
evaluation of spectroscopic models using different multivariate statistical tools in
a multicancer scenario. J Biomed Opt 2011;16:025003.
48. Oshima Y, Shinzawa H, Takenaka T, Furihata C, Sato H. Discrimination analysis
of human lung cancer cells associated with histological type and malignancy
using Raman spectroscopy. J Biomed Opt 2010;15:017009.
49. Teh SK, Zheng W, Ho KY, Teh M, Yeoh KG, Huang Z. Near-infrared Raman
spectroscopy for early diagnosis and typing of adenocarcinoma in the stomach. Br
J Surg 2011;97:550-7.
50. Haka AS, Volynskaya Z, Gardecki JA, Nazemi J, Lyons J, Hicks D, et al. In vivo
margin assessment during partial mastectomy breast surgery using raman
spectroscopy. Cancer Res 2006;66:3317-22.
51. Keller MD, Vargis E, Granja NdM, Wilson RH, Mycek M-A, Kelley MC, et al.
Development of a spatially offset Raman spectroscopy probe for breast tumor
surgical margin evaluation. J Biomed Opt 2011;16.
52. Rehman S, Movasaghi Z, Tucker AT, Joel SP, Darr JA, Ruban AV, et al. Raman
spectroscopic analysis of breast cancer tissues: identifying differences between
normal, invasive ductal carcinoma and ductal carcinoma in situ of the breast
tissue. J Raman Spectrosc 2007;38:1345-51.
53. Kirsch M, Schackert G, Salzer R, Krafft C. Raman spectroscopic imaging for in
vivo detection of cerebral brain metastases. Anal Bioanal Chem 2010;398:1707-
13.
54. Draux F, Gobinet C, Sule-Suso J, Trussardi A, Manfait M, Jeannesson P, et al.
Raman spectral imaging of single cancer cells: probing the impact of sample
fixation methods. Anal Bioanal Chem 2010;397:2727-37.
55. Bonnier F, Knief P, Lim B, Meade AD, Dorney J, Bhattacharya K, et al. Imaging
live cells grown on a three dimensional collagen matrix using Raman
microspectroscopy. Analyst 2010;135:3169-77.
56. Neugebauer U, Clement JH, Bocklitz T, Krafft C, Popp J. Identification and
differentiation of single cells from peripheral blood by Raman spectroscopic
imaging. J Biophotonics 2010;3:579-87.
57. Wu Y, McEwen GD, Harihar S, Baker SM, DeWald DB, Zhou A. BRMS1
expression alters the ultrastructural, biomechanical and biochemical properties of

69
MDA-MB-435 human breast carcinoma cells: an AFM and Raman
microspectroscopy study. Cancer Lett 2010;293:82-91.
58. Hartsuiker L, Zeijen NJ, Terstappen LW, Otto C. A comparison of breast cancer
tumor cells with varying expression of the Her2/neu receptor by Raman
microspectroscopic imaging. Analyst 2010;135:3220-6.
59. Mariani MM, Maccoux LJ, Matthaus C, Diem M, Hengstler JG, Deckert V.
Micro-Raman detection of nuclear membrane lipid fluctuations in senescent
epithelial breast cancer cells. Anal Chem 2010;82:4259-63.
60. Kamemoto LE, Misra AK, Sharma SK, Goodman MT, Luk H, Dykes AC, et al.
Near-infrared micro-Raman spectroscopy for in vitro detection of cervical cancer.
Appl Spectrosc 2010;64:255-61.
61. Mayrand MH, Duarte-Franco E, Rodrigues I, Walter SD, Hanley J, Ferenczy A, et
al. Human papillomavirus DNA versus Papanicolaou screening tests for cervical
cancer. N Engl J Med 2007;357:1579-88.
62. Robichaux-Viehoever A, Kanter E, Shappell H, Billheimer D, Jones H, 3rd,
Mahadevan-Jansen A. Characterization of Raman spectra measured in vivo for
the detection of cervical dysplasia. Appl Spectrosc 2007;61:986-93.
63. Kanter EM, Majumder S, Vargis E, Robichaux-Viehoever A, Kanter GJ, Shappell
H, et al. Multiclass discrimination of cervical precancers using Raman
spectroscopy. J Raman Spectrosc 2009;40:205-211.
64. Kanter EM, Vargis E, Majumder S, Keller MD, Woeste E, Rao GG, et al.
Application of Raman spectroscopy for cervical dysplasia diagnosis. J
Biophotonics 2009;2:81-90.
65. Widjaja E, Zheng W, Huang Z. Classification of colonic tissues using near-
infrared Raman spectroscopy and support vector machines. Int J Oncol
2008;32:653-62.
66. Chen K, Qin Y, Zheng F, Sun M, Shi DR. Diagnosis of colorectal cancer using
Raman spectroscopy of laser-trapped single living epithelial cells. Opt Lett
2006;31:2015-7.
67. Chung YG, Tu Q, Cao D, Harada S, Eisen HJ, Chang C. Raman spectroscopy
detects cardiac allograft rejection with molecular specificity. Clin Transl Sci
2009;2:206-10.

70
68. Brown KL, Palyvoda OY, Thakur JS, Nehlsen-Cannarella SL, Fagoaga OR,
Gruber SA, et al. Differentiation of Alloreactive Versus CD3/CD28 Stimulated T-
Lymphocytes Using Raman Spectroscopy: A Greater Specificity for Noninvasive
Acute Renal Allograft Rejection Detection. Cytometry A 2009;75:917-23.
69. Brown KL, Palyvoda OY, Thakur JS, Nehlsen-Cannarella SL, Fagoaga OR,
Gruber SA, et al. Raman spectroscopic differentiation of activated versus non-
activated T lymphocytes: an in vitro study of an acute allograft rejection model. J
Immunol Methods 2009;340:48-54.
70. Han XX, Huang GG, Zhao B, Ozaki Y. Label-free highly sensitive detection of
proteins in aqueous solutions using surface-enhanced Raman scattering. Anal
Chem 2009;81:3329-33.
71. Qian XM, Nie SM. Single-molecule and single-nanoparticle SERS: from
fundamental mechanisms to biomedical applications. Chem Soc Rev
2008;37:912-20.
72. Kang T, Yoo SM, Yoon I, Lee SY, Kim B. Patterned multiplex pathogen DNA
detection by Au particle-on-wire SERS sensor. Nano Lett;10:1189-93.
73. Driskell JD, Seto AG, Jones LP, Jokela S, Dluhy RA, Zhao YP, et al. Rapid
microRNA (miRNA) detection and classification via surface-enhanced Raman
spectroscopy (SERS). Biosens Bioelectron 2008;24:923-8.
74. Huang X, El-Sayed IH, Qian W, El-Sayed MA. Cancer cells assemble and align
gold nanorods conjugated to antibodies to produce highly enhanced, sharp, and
polarized surface Raman spectra: a potential cancer diagnostic marker. Nano Lett
2007;7:1591-7.
75. Hao E, Schatz GC. Electromagnetic fields around silver nanoparticles and dimers.
J Chem Phys 2004;120:357-66.
76. Wang HN, Vo-Dinh T. Multiplex detection of breast cancer biomarkers using
plasmonic molecular sentinel nanoprobes. Nanotechnology 2009;20:065101.
77. Kneipp J, Kneipp H, Wittig B, Kneipp K. Novel optical nanosensors for probing
and imaging live cells. Nanomedicine 2009;6:214-26.
78. Gregas MK, Yan F, Scaffidi J, Wang HN, Vo-Dinh T. Characterization of
nanoprobe uptake in single cells: spatial and temporal tracking via SERS labeling
and modulation of surface charge. Nanomedicine;7:115-22.

71
79. Samanta A, Maiti KK, Soh KS, Liao X, Vendrell M, Dinish US, et al.
Ultrasensitive Near-Infrared Raman Reporters for SERS-Based In Vivo Cancer
Detection. Angew Chem Int Ed Engl;50:6089-92.
80. Bergholt MS, Zheng W, Lin K, Ho KY, Teh M, Yeoh KG, et al. Characterizing
variability in in vivo Raman spectra of different anatomical locations in the upper
gastrointestinal tract toward cancer detection. J Biomed Opt;16:037003.
81. Mohs AM, Mancini MC, Singhal S, Provenzale JM, Leyland-Jones B, Wang MD,
et al. Hand-held Spectroscopic Device for In Vivo and Intraoperative Tumor
Detection: Contrast Enhancement, Detection Sensitivity, and Tissue Penetration.
Anal Chem 2010.
82. Maiti KK, Dinish US, Fu CY, Lee JJ, Soh KS, Yun SW, et al. Development of
biocompatible SERS nanotag with increased stability by chemisorption of
reporter molecule for in vivo cancer detection. Biosens Bioelectron 2010;26:398-
403.
83. Qian J, Jiang L, Cai F, Wang D, He S. Fluorescence-surface enhanced Raman
scattering co-functionalized gold nanorods as near-infrared probes for purely
optical in vivo imaging. Biomaterials 2011;32:1601-10.
84. Stuart DA, Yuen JM, Shah N, Lyandres O, Yonzon CR, Glucksberg MR, et al. In
vivo glucose measurement by surface-enhanced Raman spectroscopy. Anal Chem
2006;78:7211-5.
85. Yuen JM, Shah NC, Walsh JT, Jr., Glucksberg MR, Van Duyne RP.
Transcutaneous glucose sensing by surface-enhanced spatially offset Raman
spectroscopy in a rat model. Anal Chem 2010;82:8382-5.
86. Matousek P, Clark IP, Draper ER, Morris MD, Goodship AE, Everall N, et al.
Subsurface probing in diffusely scattering media using spatially offset Raman
spectroscopy. Appl Spectrosc 2005;59:393-400.
87. Matousek P. Deep non-invasive Raman spectroscopy of living tissue and powders.
Chem Soc Rev 2007;36:1292-304.
88. Qian X, Peng XH, Ansari DO, Yin-Goen Q, Chen GZ, Shin DM, et al. In vivo
tumor targeting and spectroscopic detection with surface-enhanced Raman
nanoparticle tags. Nat Biotechnol 2008;26:83-90.

72
89. Keren S, Zavaleta C, Cheng Z, de la Zerda A, Gheysens O, Gambhir SS.
Noninvasive molecular imaging of small living subjects using Raman
spectroscopy. Proc Natl Acad Sci U S A 2008;105:5844-9.
90. Bhirde AA, Patel V, Gavard J, Zhang G, Sousa AA, Masedunskas A, et al.
Targeted killing of cancer cells in vivo and in vitro with EGF-directed carbon
nanotube-based drug delivery. ACS Nano 2009;3:307-16.
91. Liu Z, Tabakman S, Welsher K, Dai H. Carbon Nanotubes in Biology and
Medicine: In vitro and in vivo Detection, Imaging and Drug Delivery. Nano Res
2009;2:85-120.
92. Biris AS, Galanzha EI, Li Z, Mahmood M, Xu Y, Zharov VP. In vivo Raman
flow cytometry for real-time detection of carbon nanotube kinetics in lymph,
blood, and tissues. J Biomed Opt 2009;14:021006.
93. Kostarelos K, Bianco A, Prato M. Promises, facts and challenges for carbon
nanotubes in imaging and therapeutics. Nat Nanotechnol 2009;4:627-33.
94. De la Zerda A, Zavaleta C, Keren S, Vaithilingam S, Bodapati S, Liu Z, et al.
Carbon nanotubes as photoacoustic molecular imaging agents in living mice. Nat
Nanotechnol 2008;3:557-62.
95. Maeda H. The enhanced permeability and retention (EPR) effect in tumor
vasculature: the key role of tumor-selective macromolecular drug targeting. Adv
Enzyme Regul 2001;41:189-207.
96. Maeda H. Tumor-selective delivery of macromolecular drugs via the EPR effect:
background and future prospects. Bioconjug Chem 2010;21:797-802.
97. Liu Z, Fan AC, Rakhra K, Sherlock S, Goodwin A, Chen X, et al. Supramolecular
stacking of doxorubicin on carbon nanotubes for in vivo cancer therapy. Angew
Chem Int Ed Engl 2009;48:7668-72.
98. Feazell RP, Nakayama-Ratchford N, Dai H, Lippard SJ. Soluble single-walled
carbon nanotubes as longboat delivery systems for platinum(IV) anticancer drug
design. J Am Chem Soc 2007;129:8438-9.
99. Liu Z, Chen K, Davis C, Sherlock S, Cao Q, Chen X, et al. Drug delivery with
carbon nanotubes for in vivo cancer treatment. Cancer Res 2008;68:6652-60.

73
100. Kam NW, Liu Z, Dai H. Carbon nanotubes as intracellular transporters for
proteins and DNA: an investigation of the uptake mechanism and pathway.
Angew Chem Int Ed Engl 2006;45:577-81.
101. Xiao Y, Gao X, Taratula O, Treado S, Urbas A, Holbrook RD, et al. Anti-HER2
IgY antibody-functionalized single-walled carbon nanotubes for detection and
selective destruction of breast cancer cells. BMC Cancer 2009;9:351.
102. Zavaleta C, de la Zerda A, Liu Z, Keren S, Cheng Z, Schipper M, et al.
Noninvasive Raman spectroscopy in living mice for evaluation of tumor targeting
with carbon nanotubes. Nano Lett 2008;8:2800-5.
103. Shi X, Wang SH, Shen M, Antwerp ME, Chen X, Li C, et al. Multifunctional
dendrimer-modified multiwalled carbon nanotubes: synthesis, characterization,
and in vitro cancer cell targeting and imaging. Biomacromolecules 2009;10:1744-
50.
104. Welsher K, Liu Z, Sherlock SP, Robinson JT, Chen Z, Daranciang D, et al. A
route to brightly fluorescent carbon nanotubes for near-infrared imaging in mice.
Nat Nanotechnol 2009;4:773-80.
105. Liu Z, Li X, Tabakman SM, Jiang K, Fan S, Dai H. Multiplexed multicolor
Raman imaging of live cells with isotopically modified single walled carbon
nanotubes. J Am Chem Soc 2008;130:13540-1.
106. Liu Z, Tabakman S, Sherlock S, Li X, Chen Z, Jiang K, et al. Multiplexed Five-
Color Molecular Imaging of Cancer Cells and Tumor Tissues with Carbon
Nanotube Raman Tags in the Near-Infrared. Nano Res;3:222-233.
107. Kneipp J, Kneipp H, Rice WL, Kneipp K. Optical probes for biological
applications based on surface-enhanced Raman scattering from indocyanine green
on gold nanoparticles. Anal Chem 2005;77:2381-5.
108. Hu Q, Tay LL, Noestheden M, Pezacki JP. Mammalian cell surface imaging with
nitrile-functionalized nanoprobes: biophysical characterization of aggregation and
polarization anisotropy in SERS imaging. J Am Chem Soc 2007;129:14-5.
109. Matschulat A, Drescher D, Kneipp J. Surface-enhanced Raman scattering hybrid
nanoprobe multiplexing and imaging in biological systems. ACS Nano
2010;4:3259-69.

74
110. Kneipp J, Wittig B, Bohr H, Kneipp K. Surface-enhanced Raman scattering: a
new optical probe in molecular biophysics and biomedicine. Theor Chem Acc
2010;125:319-27.
111. Zavaleta CL, Smith BR, Walton I, Doering W, Davis G, Shojaei B, et al.
Multiplexed imaging of surface enhanced Raman scattering nanotags in living
mice using noninvasive Raman spectroscopy. Proc Natl Acad Sci U S A
2009;106:13511-6.
112. Kennedy DC, Hoop KA, Tay LL, Pezacki JP. Development of nanoparticle
probes for multiplex SERS imaging of cell surface proteins. Nanoscale
2010;2:1413-6.
113. Maiti KK, Samanta A, Vendrell M, Soh KS, Olivo M, Chang YT. Multiplex
cancer cell detection by SERS nanotags with cyanine and triphenylmethine
Raman reporters. Chem Commun (Camb) 2011;47:3514-6.
114. Alessandri I, Ferroni M, Depero LE. In situ plasmon-heating-induced generation
of Au/TiO2 "hot spots" on colloidal crystals. Chemphyschem 2009;10:1017-22.
115. Li W, Camargo PH, Lu X, Xia Y. Dimers of silver nanospheres: facile synthesis
and their use as hot spots for surface-enhanced Raman scattering. Nano Lett
2009;9:485-90.
116. Li JF, Huang YF, Ding Y, Yang ZL, Li SB, Zhou XS, et al. Shell-isolated
nanoparticle-enhanced Raman spectroscopy. Nature 2010;464:392-5.
117. Küstner B, Gellner M, Schutz M, Schoppler F, Marx A, Strobel P, et al. SERS
labels for red laser excitation: silica-encapsulated SAMs on tunable gold/silver
nanoshells. Angew Chem Int Ed Engl 2009;48:1950-3.
118. Brown LO, Doorn SK. A controlled and reproducible pathway to dye-tagged,
encapsulated silver nanoparticles as substrates for SERS multiplexing. Langmuir
2008;24:2277-80.
119. Bao F, Yao JL, Gu RA. Synthesis of magnetic Fe2O3/Au core/shell nanoparticles
for bioseparation and immunoassay based on surface-enhanced Raman
spectroscopy. Langmuir 2009;25:10782-7.
120. Roca M, Haes AJ. Silica-void-gold nanoparticles: temporally stable surface-
enhanced Raman scattering substrates. J Am Chem Soc 2008;130:14273-9.

75
121. Lim DK, Jeon KS, Hwang JH, Kim H, Kwon S, Suh YD, et al. Highly uniform
and reproducible surface-enhanced Raman scattering from DNA-tailorable
nanoparticles with 1-nm interior gap. Nat Nanotechnol 2011;6:452-60.
122. Tu Q, Chung Y, Cao D, Harada S, Cheng C, Eisen H, et al. Biomarker Enables
Molecular Specific Optical Detection of Transplant Rejection. World Congress on
Medical Physics and Biomedical Engineering, September 7 - 12, 2009, . Munich,
Germany: Springer Berlin Heidelberg, 2009:740-743.
123. Thomas G, Jr., Murphy P. Structure of coat proteins in Pf1 and fd virions by laser
Raman spectroscopy. Science 1975;188:1205-7.
124. Gordon J, Barnes NM. Serotonin: a real blast for T cells. Blood 2007;109:3130-1.
125. Short MA, Lam S, McWilliams A, Zhao J, Lui H, Zeng H. Development and
preliminary results of an endoscopic Raman probe for potential in vivo diagnosis
of lung cancers. Opt Lett 2008;33:711-3.
126. Shetty G, Kendall C, Shepherd N, Stone N, Barr H. Raman spectroscopy:
elucidation of biochemical changes in carcinogenesis of oesophagus. Br J Cancer
2006;94:1460-4.
127. Akiyoshi T, Zhang Q, Inoue F, Aramaki O, Hatano M, Shimazu M, et al.
Induction of indefinite survival of fully mismatched cardiac allografts and
generation of regulatory cells by sarpogrelate hydrochloride. Transplantation
2006;82:1051-9.
128. Cloëz-Tayarani I, Changeux JP. Nicotine and serotonin in immune regulation and
inflammatory processes: a perspective. J Leukoc Biol 2007;81:599-606.
129. O'Connell PJ, Wang X, Leon-Ponte M, Griffiths C, Pingle SC, Ahern GP. A
novel form of immune signaling revealed by transmission of the inflammatory
mediator serotonin between dendritic cells and T cells. Blood 2006;107:1010-7.
130. Idzko M, Panther E, Stratz C, Muller T, Bayer H, Zissel G, et al. The
serotoninergic receptors of human dendritic cells: identification and coupling to
cytokine release. J Immunol 2004;172:6011-9.
131. Lesurtel M, Graf R, Aleil B, Walther DJ, Tian Y, Jochum W, et al. Platelet-
derived serotonin mediates liver regeneration. Science 2006;312:104-7.
132. Mössner R, Lesch KP. Role of serotonin in the immune system and in
neuroimmune interactions. Brain Behav Immun 1998;12:249-71.

76
133. Freire-Garabal M, Nunez MJ, Balboa J, Lopez-Delgado P, Gallego R, Garcia-
Caballero T, et al. Serotonin upregulates the activity of phagocytosis through 5-
HT1A receptors. Br J Pharmacol 2003;139:457-63.
134. Kushnir-Sukhov NM, Gilfillan AM, Coleman JW, Brown JM, Bruening S, Toth
M, et al. 5-hydroxytryptamine induces mast cell adhesion and migration. J
Immunol 2006;177:6422-32.
135. León-Ponte M, Ahern GP, O'Connell P J. Serotonin provides an accessory signal
to enhance T-cell activation by signaling through the 5-HT7 receptor. Blood
2007;109:3139-46.
136. Morrell CN, Sun H, Swaim AM, Baldwin WM, 3rd. Platelets an inflammatory
force in transplantation. Am J Transplant 2007;7:2447-54.
137. Platten M, Ho PP, Youssef S, Fontoura P, Garren H, Hur EM, et al. Treatment of
autoimmune neuroinflammation with a synthetic tryptophan metabolite. Science
2005;310:850-5.
138. Shaver JM. Chemometrics for Raman Spectroscopy. In: Lewis IR, Edwards HGM,
eds. Handbook of Raman Spectroscopy. New York: Marcel Dekker, 2001:275 -
306.
139. Smith BC. Quantitative spectroscopy: theory and practice. Amsterdam: Academic
Press, 2002.
140. Enejder AM, Scecina TG, Oh J, Hunter M, Shih WC, Sasic S, et al. Raman
spectroscopy for noninvasive glucose measurements. J Biomed Opt
2005;10:031114.
141. Lawson CL, Hanson RJ. Linear least squares with linear inequality constraints.
Solving least squares problems. Englewood Cliffs, N.J.,: Prentice-Hall, 1974:158-
65.
142. Ayano E, Suzuki Y, Kanezawa M, Sakamoto C, Morita-Murase Y, Nagata Y, et
al. Analysis of melatonin using a pH- and temperature-responsive aqueous
chromatography system. J Chromatogr A 2007;1156:213-9.
143. Si S, Mandal TK. pH-controlled reversible assembly of peptide-functionalized
gold nanoparticles. Langmuir 2007;23:190-5.
144. Sztainbuch IW. The effects of Au aggregate morphology on surface-enhanced
Raman scattering enhancement. J Chem Phys 2006;125:124707.

77
145. Tu Q, Eisen J, Chang C. Band shifts in surface enhanced raman spectra of indolic
molecules adsorbed on gold colloids. AIP Conference Proceedings. Boston (MA):
American Institute of Physics, 2010:1097-1098.
146. Chuang CH, Chen YT. Raman scattering of L-tryptophan enhanced by surface
plasmon of silver nanoparticles: vibrational assignment and structural
determination. J Raman Spectrosc 2009;40:150-6.
147. Razmute-Razme I, Kuodis Z, Olegas EL, Niaura G. In-situ surface-enhanced
Raman spectroscopic investigation of NH site of indole ring-terminated self-
assembled monolayer on gold electrode. Chemija 2007;18:16-20.
148. Lee HI, Suh SW, Kim MS. Raman-Spectroscopy of L-Tryptophan-Containing
Peptides Adsorbed on a Silver Surface. J Raman Spectrosc 1988;19:491-5.
149. Rava RP, Spiro TG. Resonance Enhancement in the Ultraviolet Raman-Spectra of
Aromatic Amino-Acids. J Phys Chem 1985;89:1856-61.
150. Takeuchi H. Raman structural markers of tryptophan and histidine side chains in
proteins. Biopolymers 2003;72:305-17.
151. Mellor AL, Munn DH. Creating immune privilege: active local suppression that
benefits friends, but protects foes. Nat Rev Immunol 2008;8:74-80.
152. Gordon J, Barnes NM. Serotonin: a real blast for T cells. Blood 2007;109:3130-
3131.

78
VITA
Qiang Tu
Education
Master of Science, Drexel University, Philadelphia, PA
Bachelor of Engineering, Tsinghua University, Beijing, China
Teaching Experience
Biomeasurements
Biomedical Electronics
Principles of Systems Analysis I
Principles of Systems Analysis II
First Author Publications
Qiang Tu, Chang Chang, Diagnostic Applications of Raman Spectroscopy,
Nanomedicine: Nanotechnology, Biology and Medicine, 8(5), 545-558, 2012.
Qiang Tu, Jonathan Eisen, Chang Chang, Surface-enhanced Raman Spectroscopy
Study of Indolic Molecules Adsorbed on Gold Colloids, Journal of Biomedical Optics
(Letters), 15(2), 020512, 2010
Qiang Tu, Jonathan Eisen, Chang Chang, Band Shifts in Surface Enhanced Raman
Spectra of Indolic Molecules Adsorbed on Gold Colloids, AIP Conference Proceedings
(Proceedings of the XXII International Conference on Raman Spectroscopy), 1267, 1097-
1098, 2010
Qiang Tu, Yoon-Gi Chung, Dianjun Cao, Shuko Harada, Christine S. Cheng,
Howard J. Eisen, Chang Chang, Biomarker Enables Molecular Specific Optical
Detection of Transplant Rejection, IFMBE Proceedings (World Congress on Medical
Physics and Biomedical Engineering 2009), 25(7), 740-743, 2010
Yoon-Gi Chung*, Qiang Tu*, Dianjun Cao, Shuko Harada, Howard J. Eisen, Chang
Chang, Raman Spectroscopy Detects Cardiac Allograft Rejection with Molecular
Specificity, Clinical and Translational Science, 2(3), 206-210, 2009
(* CO-FIRST AUTHORS)