Embed Size (px)
Citation preview

Br. J. Surg. Vol. .@I (1981) 825-826 Printed in Great Britain
Correspondence Suction drainage compUcntion Sir I write to describe a hitherto unreported complication of suction drainage whereby the small bowel was traumatized in a manner which could have resulted in perforation.
At emergency laparotomy, a nulliparous woman was found to have an ectopic pregnancy aborting from the fimbrial end of her only remaining fallopian tube. Hoping to save her fertility, the pregnancy was ‘milked‘ out of the tube and apparent haemostasis achieved with the diathermy. The abdomen was closed with a 6 mm Redi-vac drain in the pouch of Douglas.
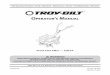
After 2 days, however, she was still bleeding copiously from the drain and salpingectomy had to be performed. An inci- dental finding was that part of the small bowel which had fallen into the pouch of Douglas bore a series of punctate haematomas each surrounded by a small halo of indented serosa (Fig. I). These can only have been caused by the holes in the drain. Thereafter the patient made an uncomplicated recovery.
Fig. 1. Small bowel trauma caused by perforations in Redi- Vac suction drainage catheter.
Suction drainage via a catheter with multiple perforations was first described by Murphey ( I ) , who used a syringe intermittently to evacuate the haemoserous fluid under mastectomy flaps. Raffle (2) used a continuous suction system instead of the syringe and the patient’s postoperative mobility was facilitated by the portable evacuated glass bottle advocated by Redon (3). whose basic system has remained unchanged.
Although .originally intended to drain spaces it was hoped to obliterate, such as block dissection flaps and amputation stumps, this kind of suction drainage has also been used for the subhepatic area after cholecystectomy (4) and the pelvis after rectal or naecological surgery. No case of Xmage to neighbouring structures has been
reported, and indeed Sutton and Scanlon (9, deliberately placing a suction catheter next to major veins in human cadavers and dogs, were unable to inflict any damage using the maximum vacuum available from the collection bottles.
In this case it was considered that the small bowel might well have perforated had the suction drainage been continued much longer, especially if an ileus had developed.
Bristol Maternity Hospital Southwell Street Bristol BS2 8EG
1. WOODFORDE SCOTT
I . MURPHEY D. R.: The use of atmospheric pressure in obliter- ating axillary dead space following radical mastectomy. South. Surg. 1947; 1 3 372-5.
2. RAFFLE A. B.: The use of negative pressure under skin flaps atter radical mastectomy. Ann. Surg. 1952; 136: 1048.
3. REWN H.: La fermeture sans dtpression des plaies ttendues. Mem. Acad. Chirurg. 1954; 80: 394-6.
4. CLEMEPJTE c. and MANNO 8.: Suction drainage of the sub- hepatic area after cholecystectomy. Am. J. Surg. 1967;
5. SUITON w. I . and SCANLON E. F.: Suction for postoperative wounds. Arch. Surg. 1961; 82: 569-75.
Rnmstedt’s operation Sir The report of Ramstedt’s operation from a district hospital was of great interest and such a series is long overdue (Br. J. Surg. 1981; 68: 590-2). It seems both impractical and un- necessary to refer all cases of congenital hypertrophic pyloric stenosis to regional centres. Until now there has been little information on its safety in the district hospital.
I have recently reviewed the experience of a district hospital in Hampshire over a 10-year period. Ten surgeons (6 con- sultants, 4 trainee surgeons) operated on 47 patients. The mean delay from admission to diagnosis and operation was 2.3 days and a tumour was palpated only in 76 per cent. Twenty-three infants had X-rays of which 13 were useful or confirmatory, showin that radiology does have a place when the diagnosis is in foubt. Unlike the series cited, all the operations were carried out under general anaesthesia through a transverse rectus cutting incision. The duodenal mucosa was punctured in 21 per cent which is a higher fi w e than in the series quoted. There were 3 severe wound infections (6.3 per cent), 3 incisional hernias and 2 wound dehiscences (4.2 per cent). One infant required reoperation at a regional centre for recurrent symptoms. Two consultants performed the bulk of the surgery (18 and 13 cases), but their rate of perforation and other complications was similar to the occasional operators. The infants that had a mucosal perforation had a higher incidence of wound infection and incisional hernia.
As in the series from Bath, there was a high incidence of postoperative vomiting (79 per cent mean 3.5 days) and there IS now some evidence that the standard early feeding regmen employed widely in Britain might be contributing to this ( I ) . Series from large specialist centres do vary greatly in their admitted complication rates from almost no morbidity (2) to a similar rate as ours.
It Seems reasonable, therefore, that district hospital surgeons can continue to treat these children safely with local paediatric assistance without the inconvenience, disruption and expense of travelling to a distant regional centre.
Research Senior Registrar University of Southampton Southampton
113 853-5.
PETER MCWNALD
1. LEAHY A. L. and FI’IZGERALD R. J. Posto rative vomiting in hypertrophic pyloric stenosis: is deGed feeding the answer? Br. J. Surg. 1981, 68: 805.
2. BELL M. 1.: Infantile yloric stenosis: experience with 305 cases at Louisville Chdren’s Hospital. Surgery 1968; 64: 983-9.
Stripping the long saphenous vein Sir As a footnote to their discussion on the merits of stripping the long saphenous vein Munn et al. (Br. J. Surg. 1981; 68: 426-8) quote the work of Rivlin (I). They suggest, I believe with ample justification, that their patients with sensory disturbance might have been spared this complication had their veins not been stripped from ankle level, but from upper






![[MS-WSPOL]: Web Services: Policy Assertions and WSDL ...... · [WSDL]. processing operation: A WSDL operation that is not a terminating operation. terminating operation: A WSDL operation](https://img.pdfslide.net/doc/110x75/5fee0a69f9c7494e656bdefe/ms-wspol-web-services-policy-assertions-and-wsdl-wsdl-processing.jpg)