Embed Size (px)
Citation preview

STATISTICS IN MEDICINEStatist. Med. 2007; 26:2074–2087Published online 13 September 2006 in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/sim.2671
Random changepoint modelling of HIV immunologic responses
Pulak Ghosh1,∗,† and Florin Vaida2,‡
1Department of Mathematics and Statistics, Georgia State University, Atlanta, GA, 30303-3083, U.S.A.2Department of Family and Preventive Medicine, University of California at San Diego,
La Jolla, CA 92093-0645, U.S.A.
SUMMARY
We propose a changepoint model for the analysis of longitudinal CD4 T-cell counts for HIV infectedsubjects following highly active antiretroviral treatment. The profile of CD4 counts for each subjectfollows a simple, ‘broken stick’ changepoint model, with random subject-specific parameters, includingthe changepoint. The model accounts for baseline covariates. The longitudinal CD4 records are censoredat the time of the subject going off-study-treatment. This is a potentially informative drop-out mechanism,which we address by modelling it jointly with the CD4 count outcome. The drop-out model incorporatesterms from the CD4 model, including the changepoint. The estimation is done in a Bayesian framework,with implementation via Markov chain Monte Carlo methods in the WinBUGS software. Model selectionusing DIC indicates that the data support the complex random changepoint and informative censoringmodel. Copyright q 2006 John Wiley & Sons, Ltd.
KEY WORDS: CD4 count; changepoint; Markov chain Monte Carlo; informative censoring; DIC
1. INTRODUCTION
Current treatment guidelines for HIV recommend a highly active antiretroviral treatment (HAART),consisting of three or more active drugs (National Institute of Health Panel on Clinical Practices forTreatment of HIV infection, 2004). HAART has achieved good success in restoring the immunesystem by suppressing the replication of HIV-1, in reducing the viral burden, and in extending theAIDS-free survival and quality of life. The status and progression of the HIV infection are usuallymeasured by the viral load (number of copies of HIV-1 RNA per millilitre of plasma), and by theCD4 count (numbers of cells per microlitre of plasma). These virologic and immunologic markershave been shown to predict progression to AIDS and death [1]. Since the CD4 cell counts are
∗Correspondence to: Pulak Ghosh, Department of Mathematics and Statistics, Georgia State University, Atlanta,GA, 30303-3083, U.S.A.
†E-mail: [email protected]‡E-mail: [email protected]
Received 15 August 2005Copyright q 2006 John Wiley & Sons, Ltd. Accepted 27 June 2006

RANDOM CHANGEPOINT MODELLING OF HIV IMMUNOLOGIC RESPONSES 2075
variable even from day to day within an individual, the general pattern over time is a more reliableindicator of immunological health.
In acute HIV infection the CD4 count has a fast increase in the first 2–4 weeks followed by agradual decline; a third stage of steep decline precludes and predicts progression to AIDS, about1 year prior to diagnostic [2, 3]. In subjects starting antiretroviral treatment (ART), the CD4 countbegins to recover [4]. The exact mechanism and dynamic between the HIV-1 and the CD4 is notwell understood, and having an accurate estimate of the rate of decline or rebound of CD4 countsis an important step in addressing this key question. The rise in CD4 count after initiation of ARTtypically has two stages, a steeper increase in first stage, followed by a more gradual increase in thesecond stage [4, 5]. The duration of the first stage was estimated in subjects with viral suppressionat 12 weeks [5]. However, patient-to-patient variability is to be expected, since the CD4 profilesmay be very different for different individuals, and having a fixed changepoint between phasesfor all subjects is a model constraint that may not reflect the biological reality. In this paper wepropose a set of statistical models that address this issue. We model the CD4 counts for subjectswith advanced HIV infection who achieve and maintain viral suppression on a new HAART,using mixed-effects models. These models allow subject-to-subject variability in their CD4 levelsand changepoint times. This feature cannot usually be addressed by the standard mixed-effectsmodels. We employ a fully Bayesian approach, based on Markov chain Monte Carlo sampling.The longitudinal CD4 profiles are censored at the time of the subject going off-study-treatment.This is a potentially informative drop-out mechanism, which we address by modelling it jointlywith the CD4 count outcome. The parameters of the drop-out time distribution include the timeof changepoint and the random effects of the CD4 model.
Prior to HAART the analysis of CD4 data focused on non-treated subjects, see References[3, 6–8] and the citations within. Several of these studies found significant evidence for a changepoint model for CD4 counts prior to AIDS in untreated patients, in the pre-HAART era [3].Recently, Guo and Carlin [8] fit a joint model for CD4 outcome and informative censoring mech-anism to data from an HIV clinical trial, taking into account the effect of treatment and of othercovariates, and fitting a linear mixed-effects model to the CD4 counts. In this article we pro-pose a joint model which combines a piecewise linear mixed model with a random changepointfor the longitudinal CD4 responses and a exponential survival model depending on the randomchangepoint for the time to drop-out. Explicitly, our analysis supports the inclusion of the randomchangepoints in the drop-out time parameter. The scientific question addressed here focuses onsubjects who are successful on HAART; however, the methodology may be applied to CD4 de-creases closer to the time of immune system failure for untreated subjects or subjects with advanceddisease.
2. ACTG 398 CLINICAL TRIAL
ACTG 398 was a large randomized, double-blind, placebo-controlled study comparing fourdifferent HAART regimens for 481 subjects with advanced stage of infection. All regimensincluded the following ART drugs: abacavir—a nucleoside reverse transcriptase inhibitors (NRTI),adefovir dipivoxil—a nucleotide reverse transcriptase inhibitor, efavirenz—a non-NRTI (NNRTI),and amprenavir—a protease inhibitor (PI). In addition, three of the four arms included a secondPI: saquinavir, indinavir, or nelfinavir, respectively, whereas the fourth arm received a matchedplacebo. The primary objective of the study was to compare the proportion of subjects who had
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

2076 P. GHOSH AND F. VAIDA
virologic failure after 24 weeks on study between the double-PI arms and the single-PI arm.The results of the primary analysis were reported by Hammer et al. [9]. Vaida et al. [10] furtherstudied the predictors of virologic failure. The analyses showed that the endpoint was mainlyassociated with the NNRTI component of the regimen, efavirenz. The subjects in the trial wereeither NNRTI naive, i.e. they had not previously received drugs from the NNRTI class, or NNRTIexperienced, i.e. they had previously received NNRTI’s as part of their treatment. Due to cross-resistance within the NNRTI class of drugs, the NNRTI experienced subjects developed resistanceto efavirenz faster and had a higher rate of virologic failure. In the first 48 weeks of the study, 317subjects had virologic failure, while 164 maintained a good virologic response. Since researchersoften aim to understand better the ‘successful’ population in a study, in this analysis we studythe CD4 cells recovery for the 164 subjects with good virologic response. The CD4 counts weremeasured at weeks 0 (baseline), 2, 4, 8, 16, 24, 32, 40, and 48 for all subjects. There are 985 CD4observations, 3–8 per subject. The median CD4 count is 290 cells/�l. The covariates of interestincluded here are: treatment (binary covariate, the three dual PI arms combined versus placebo),NNRTI experience, and baseline log10 viral load.
ACTG 398 had high toxicity rates, due to the high drug burden and to the advanced stage ofinfection in the study population; 46 per cent of the subjects went off-study-treatment (stopping atleast one drug) due to toxicity by week 48. When a subject goes off-study-treatment this affectsimmediately their viral load and CD4 cell count. In our analysis the interest is in modelling theeffect of the actual ARV treatment on CD4 for subjects which sustain control of viral infection,so the CD4 values were censored at the time of off-study-treatment. Based on the main analysisresults [9] we only consider two treatment groups, the combination of the three dual-PI arms versusthe PI-placebo arm.
As one of the reviewers pointed out, in this analysis the patients were excluded if they failedto maintain virologic success after going ‘off-study-treatment’. It should also be noted that manypatients switched to other treatments, which was the only way they maintained virologic successfor 48 weeks and qualified for this study. Thus, the subpopulation of interest is that of virologicsuccesses. This includes some subjects who went off-study-treatment prior to week 48. Theoret-ically, some of those would have failed virologically, had they stayed on treatment. However, inthis population practically no treatment options are left after failing the current regimen, and goingoff-study-treatment is virologically detrimental.
3. STATISTICAL METHODS
3.1. Changepoint model
Let yi = (yi1, . . . , yini )� be the response vector for individual i , and ti = (ti1, . . . , tini )
� the corre-sponding vector of observation times, i = 1, . . . , n. The CD4 counts were analysed on the square-root scale. This transformation has been typically used for CD4 counts [8, 11] for stabilizing thevariance, improving normality of errors and linearity of the mean, and we found that for our dataas well it is preferable to the natural scale or logarithmic transformation. To focus the discussionon modelling of changepoints, we consider the model
yi j = �1 + �2(ti j − Ki )− + �3(ti j − Ki )+ + bi + ei j (1)
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

RANDOM CHANGEPOINT MODELLING OF HIV IMMUNOLOGIC RESPONSES 2077
where Ki is the changepoint for subject i , � = (�1, �2, �3)� is the vector of fixed effects, bi is the
random effects for subject i , and ei j is the error. We assume that
bi ∼N(0, �2b), ei j ∼N(0, �2) (2)
independently of each other. In (1) we used the notation x− = min(x, 0), x+ = max(x, 0). Thecoefficients �2, �3 are the overall slope before and after changepoint Ki . It should be noted thatmodel (1) can be viewed as a normal linear spline mixed-effects model [12, 13] with the maindifference in the standard formulation being the incorporation of random knots. A more generalset-up with additional random effects can be easily accommodated in model (1) and is consideredin Section 4.
Conditionally on the changepoints Ki , (1) follows a mixed-effects model, which can be writtenin general as
yi = Xi� + Zibi + ei (3)
where Xi and Zi are ni×p and ni×q matrices of covariates for subject i , corresponding tothe fixed and random effects, respectively. Xi includes baseline covariates, possibly time-varyingcovariates, such as treatment adherence, and the before-changepoint and after-changepoint vectors(t − Ki )− and (t − Ki )+; in general, Zi is a submatrix of Xi . The random effects are givenby (2), and the errors are assumed normal, ei ∼N(0, �2 Ini ), independently of each other.
The changepoints are assumed random,
Ki ∼ F(·; �) (4)
independently of each other; F(·; �) is a parametric family of distributions (e.g. exponential orWeibull).
Equations (3) and (4) define a general class of mixed effects random changepoint models forCD4 cell counts. In addition to (1) we considered models with more complex random effectsstructure—e.g. including random slopes—models including covariates, and models with fixedcommon changepoint. We discuss the modelling strategy in more detail in Section 4.
3.2. Incorporating informative censoring
AIDS data sets are often unbalanced due to differential treatment follow-up, staggered entryof patients, missing visits and loss to study follow-up. When the data will not be missing atrandom then the probability of an individual terminating the study early is related to that subject’sunderlying rate of change. This is called informative censoring [14, 15]. In our case, it is possiblethat lower gain in CD4 counts post-treatment may be associated with earlier treatment drop-out. Tocorrectly account for possibly informative censoring we jointly model the longitudinal marker andthe survival censoring process [16–18]. The basic idea is to incorporate censoring as a survivalvariable, which gives another dimension of the outcome. Explicit modelling of the survival isrequired, rather than a semi-parametric Cox model [19, 20]. In this paper we use an exponentialand piecewise-exponential survival model for the drop-out process, whose intensity is related tothe longitudinal process by sharing the individual parameters of (1).
Specifically, Let T si denote the drop-out time for subject i , in our analysis the time to going
off-treatment; let Ci denote the ‘censoring time’ for T si , here 48 weeks. The observed survival
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

2078 P. GHOSH AND F. VAIDA
data consists of Ti =min(T si ,Ci ) and the event indicator variable �i taking the value 1 if Ti = T s
i
and 0 otherwise. We assume that T si has an exponential distribution with mean �−1
i where
�i = exp{�0 + �1 log(Ki ) + �2bi } (5)
Note that the roles of T si and Ci seem at first counterintuitive, since when Ti = T s
i the longitudinalvector yi is censored due to subject drop-out, whereas when Ti =Ci , the vector yi is complete.
The association between the longitudinal and the survival processes arises in (5) in two ways.One is through the changepoint and the other is through the sharing of the random effect bi . Thestrength and significance of the association is measured by �1 and �2, with values of 0 indicatingno association with log Ki and bi , respectively. Other forms for �i are possible. We arrived at (5)through a model selection process, described in Section 4.
3.3. Model fitting and prior specification
The parameter inference is based on joint estimation of models (1), (2), (4) and (5). Technically,the joint likelihood for the model is f (y, T |�) = ∏n
i=1 fi (y, T |�), where � includes all the fixedeffects parameters, � = (�, �, �2, �2b, �)
�, and � = (�0, �1, �2)�. The individual contribution forsubject i , conditional on Ki and bi is
fi (yi , Ti |Ki , bi ) = f (Ti , �i |�, Ki , bi ) f (yi |�, bi ) (6)
where the first factor on the right-hand side is the pdf for the censored data Ti , and the secondfactor corresponds to (1). Finally, the random components are integrated out
fi (yi , Ti |�) =∫ ∫
fi (yi , Ti |Ki , bi ) f (bi |�2b) dbi dF(Ki |�) (7)
We assumed for (4) that Ki follow an exponential distribution with mean �.We fit the model using a fully Bayesian approach. The full model specification includes prior
distributions for the parameter �,
f (y, T, �) = f (y, T |�) f (�) (8)
We assume the unknown parameters �, �, �2b, �2, and � to be mutually independent in the prior.The hyperparameters in the prior distributions were chosen so that the priors are uninformative.
We took
� j ∼N(0, 1000), independently (9)
� j ∼N(0, 1000), independently (10)
�2 ∼ IG(0.001, 0.001) (11)
�2b ∼ IG(0.001, 0.001) (12)
� ∼ G(0.1, 0.1) (13)
x ∼ IG(a, b) means that 1/x has the Gamma distribution with mean a/b and variance a/b2, andG(a, b) denotes a Gamma distribution with parameter a, b, see Reference [21].
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

RANDOM CHANGEPOINT MODELLING OF HIV IMMUNOLOGIC RESPONSES 2079
We implemented the model in WinBugs, using Markov chain Monte Carlo sampling from theposterior distribution [22]. Care needs to be taken in determining the number of iterations to achieveconvergence to the stationary distribution. Using the convergence diagnostic tool of Gelman andRubin [23] and the quantile plots, we concluded that 10 000 iterations were sufficient for theburn-in-period.
3.4. Model selection using deviance information criterion
In Bayesian data analysis, model comparison and selection is needed for at least two reasons:finding the ‘best’ model, or subset of models, which describe the data, and studying the sensitivityof the results to prior specification, which in practice, in the absence of prior information, meansmaking sure that the specified prior distribution is reasonably uninformative. The choice of modelusually entails model prediction, rather than simple fit of the existing data.
We use here the deviance information criterion (DIC) [24]. This criterion is a Bayesian equivalentof the AIC [25]. DIC is also related to cAIC proposed by Vaida and Blanchard [26], particularlysuitable for hierarchical models. DIC has been recently increasingly used as a model selectioncriteria [27–30]. DIC consists of two components, a term that measures goodness-of-fit and apenalty term for increasing model complexity: DIC= D + pD . The first term, D, is defined asthe posterior expectation of the deviance: D = E�|y[D(�)]= E�|y[−2 ln f (y|�)]. The better themodel fits the data, the smaller is the value of D. The second component, pD , measures thecomplexity of the model by the effective number of parameters and is defined as the differencebetween the posterior mean of the deviance and the deviance evaluated at the posterior mean � ofthe parameters:
pD = D − D(�) = E�|y[D(�)] − D(E�|y[�]) = E�|y[−2 ln f (y|�)] + 2 ln f (y|�) (14)
The above expression (14) shows that pD can be regarded as the expected excess of the true overthe estimated residual information in data y conditional on �. Hence, we can interpret pD as theexpected reduction in uncertainty due to estimation. Rearranging (14) gives D = D(�) + pD. Asa result, DIC can be represented as DIC= D(�) + 2pD .
Alternatively, one can use the Bayes factor for model comparison. We do not pursue this here.Bayes factor is highly sensitive to the assumed prior distribution and it can be difficult both tocompute and interpret for hierarchical models [28, 29]. In striking contrast to calculating Bayesfactor, computing DIC via MCMC is almost trivial, and is reported automatically by WinBugs.The interpretation of DIC is similar to that of the AIC, as a single-number summary of the relativefit between the model and the ‘true model’ generating the data, from the perspective of prediction,conditional on the clusters in the hierarchy, e.g. the subjects in the study. The smaller the DIC thebetter the fit, and, in analogy with AIC, a difference larger than 10 is overwhelming evidence infavour of the better model [27]. The effective number of parameters pD counts the random effectsas a fraction, and comparing them between different models gives a sense of how strongly they are‘shrunk’ by the hierarchical distribution assumption. Because it is based on model prediction, DICseeks to balance model complexity with the information available in the data, i.e. a simpler modelwill be preferable for a smaller data set, whereas a larger data set will support a more complexmodel.
DIC is not fool-proof, and some of the discussants in Reference [26] point out possible difficultiesin its use and interpretation. DIC takes from the AIC the asymptotic justification; when the log-likelihood is not log-concave, due to sub-asymptotic sample sizes or due to weak parameter
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

2080 P. GHOSH AND F. VAIDA
identifiability, DIC may not be meaningful—in particular, pD may be negative, e.g. in mixturemodels [31]. In our setting DIC offered credible values.
The model focus dictates the exact form of the DIC [24, 32]. However, the easily computable DIC(reported by WinBUGS) corresponds to a single model focus, which includes all the parameters,or ‘nodes’ in the model. If a model implementation needs additional nodes, or data augmentation,then its reported DIC will not be comparable with models implemented without the additionalnodes. The following section will provide an interesting such example.
4. RESULTS
We arrived at models (1) and (5) via a two-step process. In the first step, the model for theCD4 responses was chosen. The models considered included simpler models than (1), e.g. fixedchangepoint Ki , no random effects, and also more complex models, e.g. including random slopes.We also included different distributions for Ki in (4), including truncated normal and scaled betafamily. The inclusion of covariates gives
yi j = �1 + �2(ti j − Ki )− + �3(ti j − Ki )+ + �4x4i + �5x5i + �6x6i + bi + ei j (15)
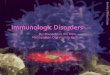
where x4i , x5i , x6i are baseline log10 HIV-1 RNA, treatment (dual PI versus PI-placebo), and NNRTIexperience, respectively. The model fits using (1) were in general similar to thoseusing (15). Figure 1 shows the longitudinal CD4 profiles for the 164 subjects.
In the second step, which we describe in more detail, we included the drop-out model. Of the164 drop-off times, 50 (30 per cent) were censored at week 48. In separate fits for the drop-offdata only, an exponential model fit better than a log-normal model. Figure 2 shows the drop-outcurve using the Kaplan–Meier estimate and using the fits from the final joint model. We considered
0 10
35
30
25
20
15
10
5
20 30 40
Week
Squ
are
root
CD
4 co
unt
Figure 1. CD4 profiles for the 164 subjects in the study (thin lines). The solid lines mark themedian and quartiles of the observed data at each time point. The dashed line is the median
predicted CD4 for all subjects based on Model 6.
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

RANDOM CHANGEPOINT MODELLING OF HIV IMMUNOLOGIC RESPONSES 2081
0
1.0
0.8
0.6
0.4
0.2
0.0
10 20 30 40 50Weeks
Sur
viva
l
Figure 2. Drop-out times for the 164 subjects in the study: Kaplan–Meier curves and model fits from themarginal drop-out distribution of Model 6.
several joint models for yi j and for the exponential parameter of T si , �i , as follows:
Model 1: Independent models for survival and longitudinal measures, i.e. (1) and �i = �.Model 2: Longitudinal model given by equation (1) and �i (t) = exp(�0 + �1Ki ).Model 3: Longitudinal model given by equation (1) and �i (t) = exp(�0 + bi ).Model 4: Longitudinal model given by equation (1) and
�i (t) = exp{�0 + �1 log(Ki )} (16)
Model 5: Fixed changepoint model, i.e. longitudinal model given by equation (1) with Ki = K ,and survival model (5).
Model 6: Longitudinal model given by equation (1) (random changepoint), and survivalmodel (5).
Model 7: Same as Model 6, but with the three covariates included, i.e. equations (15) and (5).Model 8: Same as Model 6 but with log10 HIV-1 RNA as covariate.Model 9: A random intercept and slopes model for yi j ,
yi j = �1 + �2(ti j − Ki )− + �3(ti j − Ki )+ + b0i + b1i ti j + ei j
and survival model (5).Model 10: Longitudinal model given by equation (1), and survival model
�i (t) = exp{�0 + �1 I (t>Ki )} (17)
Model 5 has a fixed changepoint for the (square root) CD4, whereas all other models haverandom changepoint. Models 1–6 share the same mean function for the CD4; Models 7 and 8include also baseline covariates. Model 8 includes only log10 HIV-1 RNA, which is the onlycovariate statistically significant in Model 7. Model 9 includes a random slope for the squarerood CD4. Models 1–6 and 8 have an increasingly complex model for the drop-off time. Model 1assumes uninformative censoring mechanism for the CD4. In Model 3 the correlation is induced
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

2082 P. GHOSH AND F. VAIDA
Table I. Model comparison: DIC values for Models 1–10; pD is the effectivedegrees of freedom, and K is the average (and standard deviation) of the
posterior mean changepoint for the 164 subjects, in weeks.
DIC pD K (SD)
Model 1 4482.7 201.4 3.6 (1)Model 2 4481.3 199.5 3.8 (1.3)Model 3 4481.1 202.6 3.3 (0.9)Model 4 4470 191.7 3.406 (0.9)Model 5 4593.2 165.3 6.8 (1.1)Model 6 4457.4 200.6 3.6 (1.2)Model 7 4463 190.8 3.5 (1.2)Model 8 4464.2 191 3.4 (1.2)Model 9 4481.2 198.6 3.5 (1)Model 6∗ 7137.4 238.7Model 10∗ 7755.9 201.3
DICs for models marked with * include additional parameters and are onlycomparable with each other.
by bi , whereas in Models 2 and 4 the correlation is given by Ki and log(Ki ), respectively,linearly on the log(�i ) scale. Finally, in Models 5–9 the correlation is given by both bi , log(Ki ),as in (5). Model 10 has piecewise-constant hazard for each subject, prior to and after the CD4changepoint Ki .
Table I describes the model comparison for these models, and includes the DIC and the effectivenumber of parameters pD . Model 5 (fixed changepoint) has least support, DIC= 4593.2, at least100 larger than all other models. Model 1 (uninformative censoring) is next least supported,DIC= 4482.7. Including bi , Ki or log(Ki ) in log(�i ) (Models 2–4) slightly reduces the DIC.Including random slope (Model 9) does not improve the DIC. A large improvement is achievedby Model 6, DIC= 4457.4 where both bi and log(Ki ) are included, as in (5). Adding covariatesto the CD4 in Models 7 and 8 does not improve the DIC over Model 6 (the difference in DIC ismoderately large, 7.4 and 9.2, respectively).
Model 10 is a special case, because its implementation (with piecewise constant hazard of drop-out) requires additional ‘nodes’, or parameters in the model. We used the ‘zero trick’, or the pointprocess representation of the survival process, as suggested in Reference [22]. As mentioned in theprevious section, the DIC in this case includes these additional nodes ‘in focus’, and therefore itis not directly comparable with the DIC of the other models. The computation of the relevant DICis non-trivial, it requires integration of the additional nodes, and is an open area of research. Forcomparison with Model 6 we also ran Model 6 using the equivalent ‘zero trick’ implementationas for Model 10, and we compared the DIC values from this implementation (Table I). In thiscomparison the more parsimonious Model 6 has the lower DIC value.
Thus, Model 6 is the favoured model. The number of effective degrees of freedom pD is smallestfor the fixed changepoint model, pD = 165.3. Interestingly, the 164 random effects bi in this modelare counted almost as full parameters. The ‘full status’ of the bi indicates that the random effectsmodel fit will be similar to one in which the random parameters are treated as fixed. Vaida andBlanchard [26] show an example of a linear mixed-effects model where such a random effectsmodel has a better fit than the corresponding model with the random parameters treated as fixed
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

RANDOM CHANGEPOINT MODELLING OF HIV IMMUNOLOGIC RESPONSES 2083
Changepoints
Fre
quen
cy
0 5 10 15 20
50
40
30
20
10
0
Figure 3. Histogram of the posterior mean values of the changepoints Ki .
Table II. Parameter estimates: posterior means (and 95 per cent posteriorintervals) for Models 6 and 7.
Model 6 Model 7
�1 16.89 (16.1, 17.8) 24.6 (19.0, 29.0)�2 0.40 (0.399, 0.481) 0.436 (0.404, 0.503)�3 0.017 (0.002, 0.027) 0.018 (0.008, 0.028)�4 — — −1.90 (−2.84,−0.77)�5 — — 1.23 (−0.28, 2.85)�6 — — 0.90 (−0.64, 2.54)�b 5.06 (4.40, 5.58) 4.73 (4.20, 5.33)� 1.59 (1.50, 1.68) 1.59 (1.50, 1.68)�0 −3.475 (−4.01,−3.19) −3.71 (−4.07,−3.27)�1 −0.035 (−0.456, 0.352) −0.030 (−0.127, 0.055)�2 −0.066 (−0.107,−0.019) −0.060 (−0.109,−0.014)
effects, and much better than a model where the random effects are completely ignored and discussthe issue of counting the random effects. The random changepoint accounts for an additional 27–35degrees of freedom, pD = 190.8–202.6 for the other models. The fixed changepoint model placesK at 6.8 weeks (standard deviation, SD= 1.1 weeks). The other seven models have very similarposterior means of the changepoint values, which is placed, on average, at 3.6 weeks. However,the credible interval for K in the fixed changepoint model overlaps with that for the average Kin the random changepoint models. Figure 3 shows the histogram of the posterior means for thechangepoints Ki .
The parameter estimates for Model 6 are in Table II. Although Model 7 has a higher DIC, sincethe influence of the covariates may be of interest nonetheless, we report in Table II the parameterestimates from this model as well. Except for the intercept, the two models give similar parametervalues. For Model 6, the initial slope is of about 0.40 (in square root CD4 concentrations per week),which translates in a first-week increase of about 13.7 cells/�l, and a first-month increase of about
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

2084 P. GHOSH AND F. VAIDA
43 cells/�l. The subsequent increase, following the changepoint, is much smaller, of 0.017, whichtranslates into a first-month increase following the changepoint of less than 1 cells/�l. Both slopes,�2 and �3, are significantly positive, i.e. the 95 per cent posterior credible interval of each ofthese parameters does not include zero. The residual and between-subject standard deviations are1.54 and 4.96, respectively, which indicates that 8.3 per cent of the variability is due to randomerror, and 86.4 per cent is due to between-subjects variation. The remaining 5.2 per cent of thevariability is accounted by the random Ki .
For Model 7, the covariates parameters show that the square-root CD4 counts are significantlyassociated with baseline log10 HIV-1 viral load, with a −1.90 reduction in response, or about−68 cells/�l, per one log10 increase in viral load, but it is not significantly associated with studytreatment or with NNRTI experience.
Turning to the parameters of the drop-off times, we note that none of �1 or �2 is zero, indicatinga correlation between longitudinal and drop-out model. However, while �1 is not statisticallysignificant, �2 is significantly different from 0. The point estimates for both are negative, suggestingthat lower baseline CD4 values and earlier changepoint values are associated with earlier drop-off times.
A visual inspection of various model parameters showed that the posterior densities are smoothand unimodal. The trace plots indicated good mixing and convergence (not included). DIC gavecredible values with positive and meaningful pD values.
5. DISCUSSION
In this paper we introduced a flexible random changepoint model for CD4 data, which incorpo-rates informative censoring via sharing of the random effects and changepoints with the drop-offtime model. Bayesian model fitting in WinBUGS allows flexibility in model specification. Non-informative priors may be chosen for the mean model parameters and for the variance components.However, the modelling of the changepoint needs more care, since even with a moderately largesample, as in our study, the information in the data about the changepoint is limited, and theanalysis tends to be more sensitive to the specification of the prior distribution and its parameters.In both the issues of prior selection and in balancing the model complexity with the informa-tion available in the data set we were guided in model selection by DIC. The DIC howeverhas its own limitations, and needs careful handling. Recently, there has been some work on thealternative prior distribution for various parameters [33, 34]. However, no consensus has yet beenreached.
Our analysis confirms previous findings that in subjects with viral suppression the CD4 shows atwo-stage rebound. Allowing the changepoint of the rebound to vary from subject to subject makesfor more flexible estimation and improved prediction. The results suggest that the changepointfrom steep to modest rebound in CD4 occurs earlier than was previously thought, on average atabout 4 weeks from the start of successful treatment. This further suggests that the CD4 reboundprocess may follow closer the viral load process, in which the steep decline lasts for the first2 weeks since start of treatment [10]. One possible explanation for the earlier changepointis that in this salvage population the therapy has a reduced benefit on the immune system,acting mainly in the first 4 weeks, than in a healthier population. More work is needed forthe joint modelling of the CD4 and HIV-1 RNA processes in order to illuminate thisassociation.
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

RANDOM CHANGEPOINT MODELLING OF HIV IMMUNOLOGIC RESPONSES 2085
APPENDIX A: CONDITIONAL DISTRIBUTIONS
Here we give a brief conceptual explanation of the conditional distributions used in the MCMCsimulation of the posterior distribution.
Conditional distributions of �, �2b, �2 are conjugate and have normal and inverse gamma distri-
butions, respectively. For the parameters bi and Ki , which appears in both submodels, their fullconditional distributions are a product of a normal distribution from the longitudinal model, a termfrom the hazard model, and the corresponding prior. Thus, the conditional distribution of bi isgiven by
log p(bi ) ∝ −0.5�−2e
∑j
[yi j − {�1 + �2(ti j − Ki )− + �3(ti j − Ki )+ + bi }]2
− 0.5�−2b b2i + �2�i bi + log Si (si )
where for subject i the survival probability at survival time si is Si (si ) = exp(− ∫ si0 �i (t) dt), �i is
the indicator of disease status and si is the time for last follow-up if a subject is censored.Similarly, the conditional distribution of Ki is
log p(Ki ) ∝ −0.5�−2e
∑j
[yi j − {�1 + �2(ti j − Ki )− + �3(ti j − Ki )+ + bi }]2
+ Ki + �1�i log Ki + log Si (si )
The conditional distributions for bi and for Ki are not in standard form. WinBUGS samplesfrom continuous conjugate full conditionals using standard algorithms. For non-standard but log-concave full conditionals, derivative-free adaptive rejection sampling is used. For non-log-concavedistributions WinBUGS uses either slice-sampling or Metropolis–Hastings algorithms. For detailssee Reference [35].
APPENDIX B: IMPLEMENTATION USING WinBUGS
We describe the WinBUGS code to implement the methods described in this paper.
model{ for ( i in 1:N) {
for ( j in 1:M){Y[i,j]∼ dnorm(mu[i,j],tauY)mu[i,j]<-beta[1]+beta[2]*(t[j]-K[i])*step(K[i]-t[j])+beta[3]*(t[j]-K[i])*step(t[j]-K[i])+b[i]
}
*Survival Modelsurt[i]∼ dexp(mus[i])I(surt.cens[i],)
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

2086 P. GHOSH AND F. VAIDA
mus[i]<-exp(logmus[i])logmus[i]<-alpha[1]+alpha[2]*log(K[i])+alpha[3]*b[i]b[i] ∼ dnorm (0, invSigma)K[i] ∼ dexp(lambda)pi[i]<-step(K[i]-cens[i])}
*Prior distributionlambda ∼ dgamma(0.1,0.1)beta[1:3] ∼ dmnorm(zero[], invSigmabeta[,])tauY ∼ dgamma(0.001,0.001)alpha[1] ∼ dnorm(0,0.001)alpha[2] ∼ dnorm(0,0.001)alpha[3] ∼ dnorm(0,0.001)}
REFERENCES
1. Mellors JW, Munoz A, Giorgi JV, Margolick JB, Tassoni CJ, Gupta P, Kingsley LA, Todd JA, Saah AJ, Detels R,Phair JP, Rinaldo Jr CR. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection.Annals of Internal Medicine 1997; 126:946–954.
2. Burcham J, Marmor M, Durbin N, Tindall B, Cooper DA, Berry G, Penny R. CD4-percent is the best predictorof development of AIDS in a cohort of HIV-infected homosexual men. AIDS 1991; 5:365–372.
3. Kiuchi AS, Hartigan JA, Holford TR, Rubinstein P, Stevens CE. Change points in the series of T4 counts priorto AIDS. Biometrics 1995; 51:236–248.
4. Deeks S, Kitchen CMR, Liu L, Guo H, Gascon R, Narvaez AB, Hunt P, Martin JN, Kahn JO, Levy J,McGrath MS, Hecht FM. Immune activation set point during early HIV infection predicts subsequent CD4+T-cell changes independent of viral load. Blood 2004; 104:942–947.
5. Hunt PW, Deeks SG, Rodriguez B, Valdez H, Shade SB, Abrams DI, Kitahata MM, Krone M, Neilands TB,Brand RJ, Lederman MM, Martin JN. Continued CD4 cell count increases in HIV-infected adults experiencing4 years of viral suppression on antiretroviral therapy. AIDS 2003; 17:1907–1915.
6. Lang W, Perkins H, Anderson RE, Royce R, Jewell N, Winkelstein Jr W. Patterns of T lymphocyte changes withhuman immunodeficiency virus infection: from seroconversion to the development of AIDS. Journal of AcquiredImmune Deficiency Syndrome 1989; 2:63–69.
7. DeGruttola V, Lange N, Dafni U. Modeling the progression of HIV infection. Journal of the American StatisticalAssociation 1991; 74:829–836.
8. Guo X, Carlin BP. Separate and joint modeling of longitudinal and event time data using standard computerpackages. The American Statistician 2004; 58:16–24.
9. Hammer SM, Vaida F, Bennett KK, Holohoan MK, Sheiner L, Eron JJ, Wheat LJ, Mitsuyasu RT, Gulick RM,Valentine FT, Aberg JA, Rogers MD, Karol CN, Saah AJ, Lewis RH, Bessen LJ, Brosgart C, DeGruttola V,Mellors JW. Dual vs single protease inhibitor therapy following antiretroviral treatment failure. Journal of theAmerican Medical Association 2002; 288:169–180.
10. Vaida F, Hammer S, Bennett KK, Bates M, DeGruttola V, Mellors J. Comparative analysis of predictors ofvirologic response to multidrug salvage regimens in ACTG 398, submitted.
11. Carlin B. Hierarchical longitudinal modelling. In Markov Chain Monte Carlo in Practice, Gilks WR, Richardson S,Spiegelhalter DJ (eds). Chapman & Hall: London, 1996; 303–320.
12. Paris H, Wand MP, Ruppert D, Ryan L. Incorporation of historical controls using semiparametric mixed model.Journal of Royal Statistical Society, Series C 2001; 50:31–42.
13. Anderson SJ, Jones RH. Smoothing spline for longitudinal data. Statistics in Medicine 1995; 14:1235–1248.14. Little RJA, Rubin DB. Statistical Analysis with Missing Data (2nd edn). Wiley: New York.15. Wu MC, Carroll RJ. Estimation and comparison of changes in the presence of informative right censoring by
modelling the censoring process. Biometrics 1988; 44:175–188.
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim

RANDOM CHANGEPOINT MODELLING OF HIV IMMUNOLOGIC RESPONSES 2087
16. Touloumi G, Pocock SJ, Babiker AG, Darbyshire JH. Estimation and comparison of rates of change in longitudinalstudies with informative drop-outs. Statistics in Medicine 1999; 18:1215–1233.
17. Faucett CL, Thomas DC. Simultaneously modelling censored survival data and repeatedly measured covariates:a Gibbs sampling approach. Statistics in Medicine 1996; 15:1663–1685.
18. Lyles RH, Lyles CM, Taylor DJ. Random regression models for human immunodeficiency virus ribonucleic aciddata subject to left censoring and informative drop-outs. Journal of the Royal Statistical Society, Series C 2000;49:485–497.
19. Schluchter MD. Methods for the analysis of informatively censored longitudinal data. Statistics in Medicine1992; 11:1861–1870.
20. Raab GM, Parpia T. Random effects models for HIV marker data: practical approaches with currently availablesoftware. Statistical Methods in Medical Research 2001; 10:101–116.
21. Gelman A, Carlin JB, Stern HS, Rubin DB. Bayesian Data Analysis (2nd edn). CRC Press: London, 2003.22. Spiegelhalter D, Thomas A, Best N, Lunn D. WinBUGS User Manual, version 1.4. MRC Biostatistics Unit,
Institute of Public Health and Department of Epidemiology and Public Health, Imperial College School ofMedicine, 2003, available at http://www.mrc-bsu.cam.ac.uk/bugs
23. Gelman A, Rubin D. Inference from alternative simulation using multiple sequences. Statistical Science 1992;457–472.
24. Spiegelhalter DJ, Best NG, Carlin BP, Van der Linde A. Bayesian measures of model complexity and fit (withdiscussion). Journal of the Royal Statistical Society, Series B 2002; 64:583–639.
25. Akaike H. Information theory and an extension of the maximum likelihood principle. In International Symposiumon Information Theory, Petov BN, Csaki F (eds). Akademia Kiado: Budapest; 267–281.
26. Vaida F, Blanchard S. Conditional akaike information for mixed-effects models. Biometrika 2005; 351–370.27. Burnham KP, Anderson DR. Model Selection Multimodel Inference: A Practical Information—Theoretic Approach
(2nd edn). Springer: New York, 2002.28. Zhu L, Carlin B. Comparing hierarchical models for spatio-temporally misaligned data using the deviance
information criterion. Statistics in Medicine 2000; 19:2265–2278.29. Berg A, Meyer R, Yu J. Deviance information criterion for comparing stochastic volatility models. Journal of
Business and Economic Statistics 2004; 24:107–120.30. Ghosh P, Branco MD, Chakraborty H. Bivariate random effect model using skew-normal distribution with
application to HIV-RNA, accepted.31. Celeux G, Forbes CP, Robert CP, Titterington DM. Deviance information criteria for missing data models.
Bayesian Analysis 2005, in press.32. Meng X-L, Vaida F. What is missing in DIC for missing data? (Discussion of article by Celeux et al.). Bayesian
Analysis 2006, in press.33. Gelman A. Prior distribution for variance parameters in hierarchical models. Bayesian Analysis 2005; 1:1–19.34. Lambert P, Sutton A, Burton P, Abrams K, Jones D. How vague is vague! A simulation study of the impact of
the use of vague prior distributions in MCMC using WinBUGS. Statistics in Medicine 2005; 24:2401–2428.35. Cowles K. Review of WinBUGS 1.4. American Statistician 2004; 330–336.
Copyright q 2006 John Wiley & Sons, Ltd. Statist. Med. 2007; 26:2074–2087DOI: 10.1002/sim