Embed Size (px)
Citation preview

Randomized Phase III trial comparing immediate versus deferred nephrectomy in patients with synchronous metastatic renal
cell carcinoma.
EORTC study 30073: SURgery TIME
24 Nov 2011
Investigators & site staff training

Overview of presentation
Scientific background and protocol for EORTC study 30073
Tips for organizing the randomization timeline
Operational aspects (translational research logistics, site authorization, interactions with centers)

Participating European sites
Up to 50 sites in Europe
Italy (4)
706 – Brausi 796 – Sternberg
720 – Gontero 797 – Berruti
…
Belgium (6)
101 – Van Velthoven
104 – Rottey
130 – D’Hondt 1217 – Van Renterghem
150 – Carpentier 1257 – Debruyne
…
The Netherlands (9)22 – Oddens 335 – De Jong
301 – Bex 324 – Soetekouw
304 – Mulders 342 – Laguna
306 – Boeken Kruger …
308 – Van Moorselaar
310 – Osanto
UK (16)601 – Sim 848 – Savage xxx - Fife
606 – Mead xxx – Mc Laren
610 – Hawkins xxx – Boleti
651 – Kynaston xxx – Farrugia
664 – Bahl xxx – Lydon
669 – Wagstaff xxx – Sheehan
671 – Maraveyas xxx – Newman
7120 – Sundaram …

Participating non-European sites
7 sites outside Europe
Canada (7)754 – Jewett
876 – Reaume
9373 – Wood
181 – Tanguay
9374 –Black
1785 - Lattouf

Scientific background and protocol for EORTC study 30073

Background (1)
• The effective therapy with a high probability of cure is surgical removal of the primary tumor
• Unfortunately, up to 30 % of all patients with renal cell carcinoma have metastatic disease at the time of diagnosis with the primary tumor in situ
Renal Cell Carcinoma (RCC) disease confined to the
kidney
• In exceptional cases pats will benefit from surgery multimodality management that comprises systemic therapy
• In highly selected patients, a combined analysis of both trials demonstrated a survival advantage for cytoreductive nephrectomy (CN) followed by interferon with a median survival of 13.6 months versus 7.8 months for interferon therapy alone.
Patients with primary
metastatic RCC and multiple non-
resectable metastases
Renal cell cancer is the 7th most frequent cancer and accounts for 2-3 % of all new cancer cases worldwide.

Background (2)
• Criteria for CN: candidate for systemic therapy, significant tumor burden of the primary tumor, absence of significant comorbidity, absence of central nervous system metastasis and low risk of surgical morbidity, performance status and early progressive disease .
• Sunitinib was registered in the US and Europe in 2007 for the treatment of metastatic RCC and became the approved first-line therapy.
• Due to its pharmacodynamics and safety profile sunitinib can be administered in close timing with surgery and is therefore the first-line drug of choice for a combination with surgery
Patients with primary
metastatic RCC and multiple
non-resectable metastases
(con’t)

Objectives and End-points
Principal objective
•To investigate whether the sequence of the nephrectomy in patients who receive sunitinib has an effect on patient outcome.
Secondary endpoin
ts
• Overall survival • Morbidity • Overall response to treatment in the deferred nephrectomy arm including the proportion
of patients who become unresectable• Effect of nephrectomy on early progression in both arms
Primary endpoin
t
• Overall progression free survival. Progression will be defined according to the "RECIST" 1.1 criteria.

Eligibility Criteria (1)
Histologically confirmed metastatic Renal Cell Cancer of clear-cell subtype (tru-cut biopsy) with a resectable asymptomatic in situ primary.
Metastatic RCC: multiple distant lesions at one site mean that patient will not be eligible Resectable: primary tumor must be resectable and resectability not be doubtful at entry
Measurable disease according to RECIST 1.1 criteria.
Prior therapies Prior systemic therapies for mRCC
Local radiotherapy for bone lesions
Concomitant medications investigational/systemic therapies for mRCC
Systemic corticosteroids and/or other immunotherapies
Sunitinib as background therapy
Disease Status

Eligibility Criteria (2)
Age ≥ 18 years
Life expectancy > 3 months
WHO PS 0 or 1
Adequate bone marrow, coagulation, hepatic & renal function
No more than 3 surgical risk factors
Normal cardiac function (LVEF, ECG).
No serious cardiac illness within the past 12 months (myocardial infarction and/or (un)treatable angina pectoris not responding to treatment)
Uncontrolled HTA Clinical signs of CNS
Pulmonary disease
Patient Status

Eligibility Criteria (3)
Surgical risk factors :
serum albumin CTCAE v4.0 grade 2 or worse (< 3.0 g/dl)
serum LDH > 1.5 x UNL
liver metastases
symptoms at presentation due to mestastases
retroperitoneal lymph node involvement
supra-diaphragmatic lymph node involvement
clinical stage T3 or T4
Patients with active or uncontrolled infections or with serious illnesses, malabsorption syndrome or medical conditions (chronic alcohol abuse, hepatitis, HIV and/or cirrhosis…)
Patient Status (con’t)

Eligibility Criteria (4)
Other malignancies history of malignancies other than RCC within the past five years (except: basal or squamous cell carcinoma of the
skin, in situ carcinoma of the cervix, resected incidental prostate cancer staged pT2 with Gleason Score 6 and postoperative PSA < 0.5 ng/ml).
Patients with any history of malignancies who are disease-free for more than 5 years
Contraception Women must be post-menopausal with a total cessation of menses of >1 year Women of childbearing potential must not be pregnant (negative serum pregnancy test at entry) or lactating; and
must agree to use effective contraceptive methods (with a documented failure rate < 1% e.g.; vasectomized partner sterile prior to trial entry and sole sexual partner or double-barrier contraception) from 2 weeks before to enrollment. The duration of the contraception will depend on the treatment that patient will receive
Written informed consent
Participation in the translational research program Patients will be eligible for the translational research program if they are eligible for the clinical trial and have given
their written informed consent to participate in this program. If patient refuses to take part in the translational research project, patient remains eligible for the clinical trial.
Informed consent

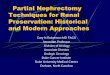
Trial Design
458 eligible patients
Immediate Nephrectomy
Nephrectomy Sunitinib
Deferred nephrectomySunitinib Nephrectomy Sunitinib
R

Treatment Schedule (1)
Immediate nephrectomy arm
Cycle 1 (6 wk) Cycle 2 (6 wk)
4 weeks of sunitinib
2 weeks break
Progression status at week 16
Progression status every 12 weeks
Cycle 3 (6 wk) Cycle 4 (6 wk)
Progression status at week 28
NE
PH
RE
CT
OM
Y
4 weeks rest after nephrectomy
Sunitinib until withdrawal criterion
In both arms, the interval between the randomization and the start of treatment should not exceed 48 hours.

Treatment Schedule (2)
Deferred nephrectomy arm
Sunitinib until withdrawal criterion
NE
PH
RE
CT
OM
Y
4 weeks of sunitinib
2 weeks break
Cycle 1 (6 wk) Cycle 2 (6 wk) Cycle 3 (4 wk)
Progression status at week 28
Cycle 4 (6 wk) Cycle 5 (6 wk)
4 weeks rest after nephrectomy
Progression status every 12 weeks
Progression status at week 16
Sunitinib will stop the day before surgery (# end week 4)
Criteria for surgery ■ Non systemic progressive disease (RECIST 1.1 criteria).
■ Recovery from toxicity due to sunitinib specifically interfering with surgery.
■ Patients must not have more than 3 surgical risk factors.

Tips for organizing the randomization timeline for centres with a waiting list (1)
Based on experience from the NKI
• At the first contact with the patient crudely check general eligibility, inform about the trial and possible inclusion
• place patient on the waiting list for surgery at the time of first contact, except if patient definitely refuses to participate
• once the potential date for surgery is known, randomization can be planned 48 hours in advance
• instruct planning staff not to communicate the potential date for surgery directly to the patient as this may cause misunderstanding.It should be used for internal communication and planning of the randomization date.

Tips for organizing the randomization timeline for centres with a waiting list (2)
• Inform the patient as early as possible about the date of randomization. Explain, that admission for surgery or start of medical treatment will take place within 48 hours of randomization. This will allow the patient to prepare well in advance for the two options depending on randomization. Don’t wait with this information until randomization as an admission within 48 hours may completely surprise the patient.
• perform new CT scans, tru-cut biopsies and other eligibility checks if required in the waiting time. Don’t do this first and plan the patient subsequently if your centre has a long waiting time for surgery. If the patient turns out not to be eligible, it is easier to cancel the planning

Tips for organizing the randomization timeline for centres with a waiting list (3)
• Nevertheless, if at all possible, the waiting time should not be too long as we discovered that patients experience it as a waste of time if they randomize for sunitinib first. In their view they could have started right away in retrospect if only it would have been known earlier. Again, good communication is essential: Patients should be informed that metastatic RCC is not an emergency

Tips for organizing the randomization timeline for centres with a waiting list (4)
Regarding the 50 % chance of loosing surgery time there are several options to follow:
• At the NKI we have a pool of planned alternative patients. There are patients who do not mind to be informed at short notice in exchange for a chance to shorten the waiting time.
• Use of ‘trial slots’.
• Performing surgery after the regular program as an ‘emergency’

Treatment and Schedule modifications (1)
1. PRE-SURGICAL PERIOD
Dose and schedule modifications of sunitinib will follow the standard recommendations of the drug and the decision will be based on the investigator's judgment.
2. SURGICAL PERIOD
Immediate nephrectomy arm
Given the primary endpoint, if the interval from baseline disease assessment to surgery date exceeds 4 weeks, re-staging of the disease should be performed again.

Treatment and Schedule modifications (1)
Deferred nephrectomy arm
If during the course of cycle 3, a patient has to interrupt sunitinib due to a side effect, the disease assessment must be performed after recovery as close as possible to surgery.
If the recovery period leads to a delay in surgery for > 2 weeks compared to the initially scheduled date, the patient will be taken off protocol treatment but should continue to be followed for protocol endpoints (progression and survival).
In case of severe hematuria necessitating intervention during the three pre-surgical courses, sunitinib must be stopped temporarily.
In case of an overdose of sunitinib, surgery should be delayed by 3 days according to the half life of the active metabolite.
3. POST-SURGICAL PERIOD
In both arms
If the delay > 4 wk recovery period the patient will not be eligible for evaluation of the primary endpoint, but will be followed for evaluation of secondary endpoints.

Treatment Withdrawal Criteria
Withdrawal criteria are defined as:
Disease progression
Occurrence of second malignancy
Unacceptable toxicity based on the investigator's judgment.
Patient decision.
In case of withdraw due to other reason than disease progression:
■ Pats should not receive any other cancer treatment before their disease progresses, unless
this is clearly not in the best interest of the patient.
■ Follow up must be continued for progression and survival as per protocol

Clinical Evaluation (1)
• Biopsy: if the histological diagnosis of “clear-cell” subtype is not established patients need to undergo a transcutaneous tru-cut needle biopsy of the primary tumor.
Before randomization
• Radiological assessment includes the primary tumor and the metastases according to RECIST 1.1 criteria
Within 4 wks prior to random.
• Medical history• WHO PS, blood pressure, pulse rate, body weight and height• Cancer signs and symptoms• Assessment of adverse events (CTCAE 4.0)• LVEF, 12-lead ECG • Serum pregnancy test• Complete blood counts & Serum chemistry
Within 2 wks prior to random

Clinical Evaluation (2)
Before random.
Post surgical period Fol.up weekly if discontinue
due tox.
Fol. up until PD
after PDQ 12 weeks for survival4 wks post
surg.week 16 Week 28 After week
28
Q 12 wks
Medical history
WHO PS, BP, PR, W, H
Cancer signs and symptoms
Adverse events
Cardiac function
Serum pregnancy test
Hematology (2)
Serum chemistry (3)
Radiological assessment (RECIST 1.1)
(4 wks)
(Re-staging)
(Q 12 wk)
Survival status
Immediate nephrectomy arm

Clinical Evaluation (3)
Deferred nephrectomy arm
Before random.
Pre-surgical period Post surgical period Fol.up weekly if discontinue
due tox.
Fol. up until PD
after PDQ 12
weeks for survival
Week 4 Week 16 Week 20 Week 28 Week 32 After week 28,
Q 12 wks
Medical history
WHO PS, BP, PR, W, H
Cancer signs and symptoms
Adverse events
Cardiac function
Serum pregnancy test
Hematology (2),
Serum chemistry(3)
Radiological assessment (RECIST 1.1)
(4 wks)
(Re-staging)
(Q 12 wk)
Survival status

Clinical Evaluation (4)
Follow ups must still be provided for the study endpoints (progression free survival and overall survival).
In addition, for patients that withdraw due to adverse event, follow up for adverse event will continue on a weekly basis until any associated adverse event has resolved or clinical judgment deems necessary. It will consist of:
Medical examination
Assessment of adverse events
Complete blood counts, if needed
Serum chemistry, if needed
Cardiac function, if needed
Other tests, if needed
In both arms, for the patients who discontinue treatment in absence of progression:

Criteria for Evaluation (1)RECIST 1.1
Measurable disease: presence of at least one measurable lesion. If the measurable disease is restricted to a solitary lesion, its neoplastic nature should be confirmed by cytology/histology

Criteria for Evaluation (2)RECIST 1.1
Measurable lesionTumor lesions: that can be accurately measured in at least one dimension (longest diameter to be recorded) as ≥ 20 mm with chest x-ray, and as ≥ 10 mm with CT scan or clinical examination [using calipers].
Bone lesions: are considered measurable only if assessed by CT scan and have an identifiable soft tissue component that meets these requirements (soft tissue component > 10 mm by CT scan).
Malignant lymph nodes: must be ≥ 15 mm in the short axis to be considered measurable; only the short axis will be measured and followed. All tumor measurements must be recorded in millimeters (or decimal fractions of centimeters) by use of a ruler or calipers
Tumor lesions situated in a previously irradiated area, or in an area subjected to other loco-regional therapy: are usually not considered measurable unless there has been demonstrated progression in the lesion.

Criteria for Evaluation (3)RECIST 1.1
All other lesions (or sites of disease), including small lesions
Bone lesions without a measurable soft tissue component
leptomeningeal disease, ascites, pleural/pericardial effusions, lymphangitis cutis/pulmonis, inflammatory breast disease, lymphangitic involvement of lung or skin and abdominal masses followed by clinical examination.
Nodes that have a short axis <10 mm at baseline are considered non-pathological and should not be recorded or followed.
Non Measurable lesions

Criteria for Evaluation (4)RECIST 1.1
Target and non target lesions
Target lesion (TL)
• Up to a maximum of 5 lesions (maximum of 2 lesions per organ) • size (lesions with the longest diameter), representative of all involved organs, reproducible for repeated measurements. • Pathological nodes: short axis of ≥ 15 mm by CT scan (baseline sum). •Baseline Sum of TL= longest diameter of tumor lesions + short axis of lymph nodes
Non target lesion (NTL)
• All non-measurable lesions (or sites of disease) including :pathological nodes (those with short axis ≥ 10 mm but < 15 mm)• Any measurable lesions over and above those listed as target lesions are considered non-target lesions.• These lesions should be noted at baseline and should be followed as “present” or “absent”.

Criteria for Evaluation (5)RECIST 1.1
Evaluation of Response
Complete Response (CR)
•Disappearance of all target and non-target lesions and normalization of tumor markers. •Pathological lymph nodes must have short axis measures < 10mm•Tumor markers must have normalized .•Residual lesions (other than nodes < 10 mm) thought to be non-malignant should be further investigated (by cytology or PET scans) before CR can be accepted.
Partial Response (PR) • At least a 30% decrease in the sum of measures (longest diameter for tumor lesions and short axis measure for nodes) of target lesions, taking as reference the baseline sum of diameters. • Non target lesions must be non-PD.
Stable Disease (SD) Neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD taking as reference the smallest sum of diameters on study.

Criteria for Evaluation (6)RECIST 1.1
Evaluation of ResponseProgressive Disease (PD)
at least a 20% increase in the sum of diameters of measured lesions taking as references the smallest sum of diameters recorded on study (including baseline) AND an absolute increase of ≥ 5 mm.
Appearance of new lesions will also constitute PD (including lesions in previously unassessed areas).
In exceptional circumstances, unequivocal progression of non-target disease may be accepted as evidence of disease progression
If the evidence of PD is equivocal (target or non-target), treatment may continue until the next assessment, but on further documentation, the earlier date must be used

Criteria for Evaluation (7)RECIST 1.1
Evaluation of response to take into account:
Response of target lesions
Response of non target lesions
Presence of new lesions

Disease Evaluation criteria (8) RECIST 1.1
Best Overall Response Evaluation
Target Lesions
Non-Target Lesions
New Lesions
Overall Response
CR CR No CR
CR SD No PR
PR Not PD No PR
SD Not PD No SD
PD Any Yes or No PD
Any PD Yes or No PD
Any Any Yes PD

Translational research: patient eligibility
Eligible patient
Objectives TR:1. Identify possible molecular markers that correlate with
response, prognosis and overall survival
Written consent for TRNo consent for TR
Eligible for study Eligible for study and TR

Translational Research
Before random.
During treatment
Week 16 Surgery 6 mo. After random
Paraffin embedded tumor block
♦1
(Tru-cut biopsy)
♦2
(specimen from surgery)
Fresh frozen tissue
♦1
(Tru-cut biopsy)
♦2
(specimen from surgery)
Blood sample 10 ml
♦ ♦ ♦
1. In the immediate nephrectomy arm: native tumor tissue will be obtained from nephrectomy specimen.
2. In deferred surgery arm: for those patients who will not undergo surgery, it’s strongly recommended to perform a transcutaneous tru-cut needle biopsy of the primary tumor

Preparation and storage TR samples (1)
1) Blood samples
Centrifugation at 2000 g; 10 minT = Room temperature
3 storage tubes1 ml serum/tube
Label: Protocol 30073Subject seqidSample date; Serum
10 mlblood
At baselineAt surgeryAt 6 months
Freeze and
store at -80°C
30-60 min
Room temp

Preparation and storage TR samples (2)
3 biopsies
2) Tissue samplesBiopsy samples
Room temp 30 minutes max
Pathology department
Biopsies 1/tube in storage tube (3ml)
Label: Protocol 30073Subject seqidSample date; paraffin/frozen tissueLocal inventory code
1 formaldehyde fixed paraffinTumor biopsy (at least)
Freeze and store at -80°C
Store at Room temp

Preparation and storage TR samples (3)
2) Tissue samples
Blocks or punch biopsies8/tube in storage tubes (3ml)
Label: Protocol 30073Subject seqidSample date; paraffin/frozen tissueLocal inventory code
Nephrectomy samplesStore at Room temp
1 formaldehyde fixed paraffinTumor block (at least)
Room temp 30 minutes max
Freeze and store at -80°C
Pathology department