Embed Size (px)
Citation preview

1
For educational purposes only
The Content of this Presentation is only intended for registered healthcare professionals.The medical information in this Presentation is provided as an information resource only, and is not to be used or relied on for any diagnostic or treatment purpose. Pfizer (including its parent, subsidiary and affiliate entities) makes no representation or warranties of any kind, expressed or implied; as to the content used in the Presentation and/or the accuracy, completeness of its content.
Rational use of antibiotics in bacterial infection of CAP

2
For educational purposes only
Table of Contents
Introduction and Overview
Epidemiology of CAP
Management of Disease
Guidelines
123
4Conclusion5

3
For educational purposes only
Introduction

4
Lower Respiratory Tract Infections
WHO The top 10 causes of death Fact sheet N°310. Updated May 2014. Accessed thru http://www.who.int/mediacentre/factsheets/fs310/en/ on 26 Aug 2016.

5
Community-acquired pneumonia (CAP)
• Major respiratory disease with a high prevalence in the general population, clinical heterogeneity and variable severity.
• Usually causes symptoms for 3–4 weeks, and daily activities may be impaired for a further 3 weeks on average.
• Reported incidence of pneumonia varies considerably from country to country and study to study, with a consistently higher incidence in very young children and elderly adults.
ERS European Lung White Book, Chapter 18 - Acute lower respiratory infections. Accessed thru http://www.erswhitebook.org/chapters/acute-lower-respiratory-infections/ on 26 August 2016.

6
Most common etiologies
Mandell, LA. Postgrad Med 2015; 127(6): 607–615.

7
Host Risk Factors for CAP Infection
Risk of infection
Advanced age
Smoking
AlcoholismImmune dysfunction
Poor nutrition
InstitutionalizationDefective phagocytosis
Co-morbidityAsthmaCOPDCVD
Baik I, Curhan GC, Rimm EB, Bendich A, Willett WC, Fawzi WW. A prospective study of age and lifestyle factors in relation to community-acquired pneumonia in US men and women. Archives of Internal Medicine. 2000;160(20):3082-8.Koivula I, Sten M, Makela PH. Risk factors for pneumonia in the elderly. The American journal of medicine. 1994;96(4):313-20.

8
CAP in Asia
• In Asia, CAP is estimated to cause almost one million adult deaths per year.1,2
• Many of these deaths occur in the elderly, but a large number occur in those with good life expectancy
• Systematic review of all adult CAP etiology studies publish in English from Jan 1990- Mar 2012 (incl. China, India, Indonesia, Japan, Malaysia, Philippines, Singapore, South Korea, Taiwan, Thailand and Vietnam) 2
1. World Health Organization. Global burden of disease (GBD). Geneva: World Health Organization; 2008. http://www.who.int/healthinfo/ global_burden_disease/gbd/en/ [accessed 1 August 2012].
2. Peto, L., et al. Trans R Soc Trop Med Hyg 2014; 108: 326–337.
• Streptococcus pneumoniae was the most commonly identified pathogen (13.3%). 2
• Overall rate of Haemophilus influenzae for Asia was 6.9%; Legionella spp. was low at 3.0%2
• Gram negative bacilli (GNB) were identified in 13.0% of hospitalised patients (averaging all Asian studies) 2

9
For educational purposes only
Epidemiology of CAP

10
For educational purposes only
Epidemiology
•CAP is a common and potentially serious disease, globally ranked as the
5th leading cause of mortality•It is the most common cause of disability-adjusted life-years among all respiratory diseases (more common than chronic obstructive pulmonary disease human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) 1
•Majority of patients with CAP are treated as outpatients, the greatest proportion of pneumonia-related mortality and healthcare expenditure occurs among persons who are hospitalized 2
1. Niederman MS, Luna CM. Community-Acquired Pneumonia Guidelines : A Global Perspective. Semin Respir Crit Care Med. 2012;33(212):298–310. 2. Ramirez JA, Anzueto AR. Changing needs of community-acquired pneumonia. J Antimicrob Chemother. 2011;66 Suppl 3(Suppl 3):iii3-9.
Bacteria are the most common etiological pathogens of CAP and have traditionally been divided into two groups designated ‘typical’ and ‘atypical’ 2
• The most common typical pathogens include Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, group A streptococci and Moraxella catarrhalis 2
• The most common atypical pathogens include Legionella spp., Mycoplasma pneumoniae and Chlamydophila pneumoniae

11
For educational purposes only
Mortality due to CAP
In the past two decades, patients aged 65–84 years have experienced a 20% increase in pneumonia-related hospitalizations
For individuals >65 years of age, the rates of hospitalization and death caused by pneumonia continue to increase even though rates are decreasing for all other age groups
1. Ramirez JA, Anzueto AR. Changing needs of community-acquired pneumonia. J Antimicrob Chemother. 2011;66 Suppl 3(Suppl 3):iii3-9.
World Health Organization (WHO) global burden of disease study estimated that lower respiratory tract infections (LRTIs), which include CAP, were 429.2 million episodes of illness worldwide and accounts for 94.5 million disability adjusted life years (DALYs)

12
For educational purposes only
Management of Disease

13
For educational purposes onlyBritish Thoracic Society :
CURB 65 severity score
1. Lim WA, et al. Thorax 2009;64 Suppl3:iii1-55.

14
For educational purposes only
BTS : Hospital management of CAP in the first 4 hours
2Moderate severity
0-1Low severity
3-5High severity
Other reasons for admission (unstable comorbidity, social)
Hospital Supportive care Microbiological
investigations Antibiotics given
Hospital Supportive care Microbiological
investigations Antibiotics given Urgent senior review Decision regarding
transfer to critical care unit (especially if CURB65 = 4 or 5)• Home
• Antibiotics• Hospital• Antibiotics
Yes No
Patient meets criteria for CAP: Treat according to clinical judgement and CURB65 severity score
1. Lim WA, et al. Thorax 2009;64 Suppl3:iii1-55.

15
For educational purposes onlyTreatment Options
• Treatment regimens vary for CAP for patients with or without co-morbidities and ICU or non-ICU patients
• In non-ICU patients, levofloxacin, moxifloxacin and a combination of beta-lactam with azithromycin may be considered
• ICU patients with gram-negative pseudomonas spp. suspected, piperacillin-tazobactam, cefepime, aminoglycoside, etc. may be considered
• In those with risk of aspiration pneumonia, clindamycin, piperacillin-tazobactam, ceftriaxone, vancomycin, etc. may be considered
Donovan F 2015. Community-Acquired Pneumonia Empiric Therapy: Empiric Therapy Regimens [Internet]. Emedicine.medscape.com. 2016 [cited 9 December 2016]. Available from: http://emedicine.medscape.com/article/2011819-overview

16
For educational purposes only
Condition Likely organisms
Recommendation Alternative Comments
Community acquired Pneumonia
S. pneumoniae, H.influenzae, Legionella, E.coli, Klebsiella sp.,S.aureus
Mild to moderate cases Amoxycillin- 500mg-1 g TDS oral. If IV indicated, amoxycillin-clavulanate 1.2 g IV TDS or Ceftriaxone 2g IV OD Severe cases Amoxycillin-clavulanate 1.2 g IV TDS OrCeftriaxone 2g IV OD Duration 5-8 days
Piperacillin-Tazobactam 4.5gm IV 6 hourly ORImipenem 1g IV 6hourly ORCefoperazone-Sulbactam 3gm IV 12 hourly
If MRSA is a concern, add Linezolid 600mg IV/Oral BD
If atypical pneumonia suspected, Doxycycline 100mg bd OR Azithromycin 500 mg oral/IV OD
Available at http://www.ncdc.gov.in/writereaddata/linkimages/AMR_guideline7001495889.pdf last accessed on 14th March 2016
National Treatment Guidelines for CAP

17
For educational purposes onlyNational Treatment Guidelines for CAP
•Macrolide antibiotics should be considered in following clinical scenarios where the likelihood of mycoplasma pneumonia is high:
•In the first two conditions macrolide antibiotics can be used along with the first line therapy for CAP
a.• Children with a subacute presentation with prolonged low grade fever, persistent cough, chest
signs out of proportion to the radiographic abnormality (usually showing perihilar streaky infiltrates).
b.• Children with CAP (acute pneumonia like presentation with radiological evidence of patchy or
lobar consolidation) who also have or develop extrapulmonary manifestations like myocarditis, hemolytic anemias, glomeruonephritis, aseptic arthritis, CNS problems (aseptic meningitis, encephalitis, ataxia), etc.
c.• Non response to first line antibiotics in children who are immunized with Hib/PCV and have no
suppurative complications of CAP
Available at http://www.ncdc.gov.in/writereaddata/linkimages/AMR_guideline7001495889.pdf last accessed on 14th March 2016

18
For educational purposes only
GUIDELINES

19
For educational purposes only
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

20
For educational purposes only
Introduction
• This guideline focuses on adults with CAP who do not have an immunocompromising condition
• Antibiotic recommendations for the empiric treatment of CAP are based on selecting agents effective against the major treatable bacterial causes of CAP.
• Traditionally, these bacterial pathogens include Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, Staphylococcus aureus, Legionella species, Chlamydia pneumoniae, and Moraxella catarrhalis.
• The microbial etiology of CAP is changing, particularly with the widespread introduction of the pneumococcal conjugate vaccine, and there is increased recognition of the role of viral pathogens.
• Recommendations are to initially treat empirically for possible bacterial infection or coinfection.
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

21
For educational purposes onlyShould Gram Stain and Culture of Lower Respiratory
Secretions Be Obtained at the Time of Diagnosis?
•This guideline recommend not obtaining sputum Gram stain and culture routinely in adults with CAP managed in the outpatient setting (strong recommendation, very low quality of evidence).
•This guideline recommend obtaining pretreatment Gram stain and culture of respiratory secretions in adults with CAP managed in the hospital setting who:
1. are classified as severe CAP* especially if they are intubated (strong recommendation, very low quality of evidence); or2. a. are being empirically treated for MRSA or P. aeruginosa (strong recommendation, very low quality of evidence); or b. were previously infected with MRSA or P. aeruginosa, especially those with prior respiratory tract infection (conditional recommendation, very low quality of evidence); or c. were hospitalized and received parenteral antibiotics, whether during the hospitalization event or not, in the last 90 days (conditional recommendation, very low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

22
For educational purposes only
Should Blood Cultures Be Obtained at the Time of Diagnosis?
•This guideline recommend not obtaining blood cultures in adults with CAP managed in the outpatient setting (strong recommendation, very low quality of evidence).
•This guideline suggest not routinely obtaining blood cultures in adults with CAP managed in the hospital setting.•This guidelines recommend obtaining pretreatment blood cultures in adults with CAP managed in the hospital setting who:
1. are classified as severe CAP* (strong recommendation, very low quality of evidence); or2. a. are being empirically treated for MRSA or P. aeruginosa (strong recommendation, very low quality of evidence); or b. were previously infected with MRSA or P. aeruginosa, especially those with prior respiratory tract infection (conditional recommendation, very low quality of evidence); or c. were hospitalized and received parenteral antibiotics, whether during the hospitalization event or not, in the last 90 days (conditional recommendation, very low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

23
For educational purposes only
*Defining Severe CAP
• Validated definition includes either 1 major criterion OR three or more minor criteria
• MINOR CRITERIAoRespiratory rate>30 breaths/minoPaO2/FIO2 ratio<250oMultilobar infiltratesoConfusion/disorientationoUremia (blood urea nitrogen level>20 mg/dl)o Leukopenia* (white blood cell count,4,000 cells/ml)o Thrombocytopenia (platelet count,100,000/ml)oHypothermia (core temperature,368C)oHypotension requiring aggressive fluid resuscitation
• MAJOR CRITERIAoSeptic shock with
need for vasopressors
oRespiratory failure requiring mechanical ventilation
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

24
For educational purposes onlyDifferences between 2019 and 2007 ATS/IDSA
Community-Acquired Pneumonia Guidelines
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

25
For educational purposes onlyShould Legionella and Pneumococcal Urinary Antigen
Testing Be Performed at the Time of Diagnosis?
•This guideline suggest not routinely testing urine for pneumococcal antigen in adults with CAP (conditional recommendation, low quality of evidence), except in adults with severe CAP (conditional recommendation, low quality of evidence).
•This guideline suggest not routinely testing urine for Legionella antigen in adults with CAP (conditional recommendation, low quality of evidence), except
1. in cases where indicated by epidemiological factors, such as association with a Legionella outbreak or recent travel (conditional recommendation, low quality of evidence); or2. in adults with severe CAP* (conditional recommendation, low quality of evidence).
•This guideline suggest testing for Legionella urinary antigen and collecting lower respiratory tract secretions for Legionella culture on selective media or Legionella nucleic acid amplification testing in adults with severe CAP (conditional recommendation, low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

26
For educational purposes onlyInitial Treatment Strategies for Outpatients with
Community-acquired Pneumonia
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

27
For educational purposes onlyShould a Respiratory Sample Be Tested for
Influenza Virus at the Time of Diagnosis?
• When influenza viruses are circulating in the community, this guideline recommend testing for influenza with a rapid influenza molecular assay (i.e., influenza nucleic acid amplification test), which is preferred over a rapid influenza diagnostic test (i.e., antigen test) (strong recommendation, moderate quality of evidence).
Should Serum Procalcitonin plus Clinical Judgment versus Clinical Judgment Alone Be Used to Withhold Initiation of Antibiotic Treatment?
• This guideline recommend that empiric antibiotic therapy should be initiated in adults with clinically suspected and radiographically confirmed CAP regardless of initial serum procalcitonin level (strong recommendation, moderate quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67
28
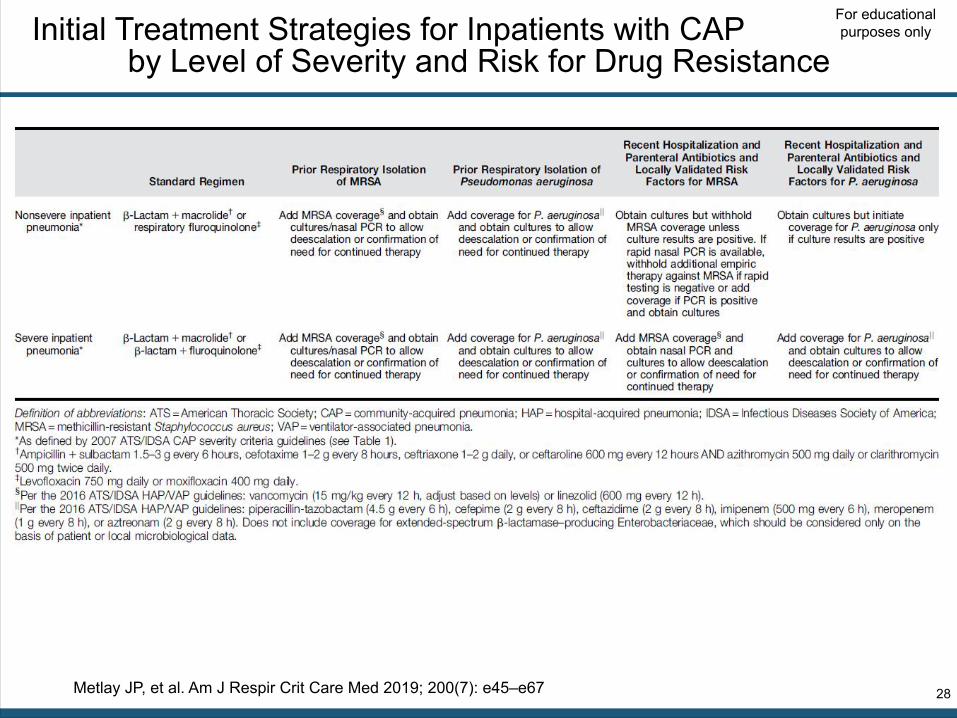
For educational purposes onlyInitial Treatment Strategies for Inpatients with CAP
by Level of Severity and Risk for Drug Resistance
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

29
For educational purposes only
Should a Clinical Prediction Rule for Prognosis plus Clinical Judgment versus Clinical Judgment Alone Be Used to Determine Inpatient versusOutpatient Treatment Location for Adults with CAP?
• In addition to clinical judgement, this guideline recommend that clinicians use a validated clinical prediction rule for prognosis, preferentially the Pneumonia Severity Index (PSI) (strong recommendation, moderate quality of evidence) over the CURB-65 (tool based on confusion, urea level, respiratory rate, blood pressure, and age >65) (conditional recommendation, low quality of evidence), to determine the need for hospitalization in adults diagnosed with CAP.
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

30
For educational purposes only
Should a Clinical Prediction Rule for Prognosis plus Clinical Judgment versus Clinical Judgment Alone Be Used to Determine Inpatient General Medical versus Higher Levels of Inpatient Treatment Intensity (ICU, Step-Down, or Telemetry Unit) for Adults with CAP?
• This guideline recommend direct admission to an ICU for patients with hypotension requiring vasopressors or respiratory failure requiring mechanical ventilation (strong recommendation, low quality of evidence).
• For patients not requiring vasopressors or mechanical ventilator support, we suggest using the IDSA/ATS 2007 minor severity criteria* together with clinical judgment to guide the need for higher levels of treatment intensity (conditional recommendation, low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

31
For educational purposes onlyAntibiotics which Are Recommended for Empiric
Treatment of CAP in Adults In the Outpatient Setting (1)
For healthy outpatient adults without comorbidities listed below or risk factors for antibiotic resistant pathogens, this guideline recommend:
•amoxicillin 1 g three times daily (strong recommendation, moderate quality of evidence), or•doxycycline 100 mg twice daily (conditional recommendation, low quality of evidence), or•a macrolide (azithromycin 500 mg on first day then 250 mg daily or•clarithromycin 500 mg twice daily or clarithromycin extended release 1,000 mg daily) only in areas with pneumococcal resistance to macrolides <25% (conditional recommendation, moderate quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

32
For educational purposes onlyAntibiotics which Are Recommended for Empiric
Treatment of CAP in Adults In the Outpatient Setting (2)
For outpatient adults with comorbidities or asplenia this guideline recommend (in no particular order or preference) :•Combination therapy:
o amoxicillin/clavulanate 500 mg/125 mg three times daily, or amoxicillin/ clavulanate 875 mg/125 mg twice daily, or 2,000 mg/125 mg twice daily, or a cephalosporin (cefpodoxime 200 mg twice daily or cefuroxime 500 mg twice daily); AND
omacrolide (azithromycin 500 mg on first day then 250 mg daily, clarithromycin [500 mg twice daily or extended release 1,000 mg once daily]) (strong recommendation, moderate quality of evidence for combination therapy), or doxycycline 100 mg twice daily (conditional recommendation, low quality of evidence for combination therapy); OR
•Monotherapy:o respiratory fluoroquinolone (levofloxacin 750 mg daily, moxifloxacin 400 mg
daily, or gemifloxacin 320 mg daily) (strong recommendation, moderate quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

33
For educational purposes only
Antibiotic Regimens Which Are Recommended forEmpiric Treatment of CAP in Adults without Risk Factorsfor MRSA and P. aeruginosa In the Inpatient Setting
In inpatient adults with non-severe CAP without risk factors for MRSA or P. aeruginosa, this guideline recommend the following empiric treatment regimens (in no order of preference):•combination therapy with a β-lactam (ampicillin1sulbactam 1.5–3 g every 6 h, cefotaxime 1–2 g every 8 h, ceftriaxone 1–2 g daily, or ceftaroline 600 mg every 12 h) and a macrolide (azithromycin 500 mg daily or clarithromycin 500 mg twice daily) (strong recommendation, high quality of evidence), or•monotherapy with a respiratory fluoroquinolone (levofloxacin 750 mg daily, moxifloxacin 400 mg daily) (strong recommendation, high quality of evidence).
A third option for adults with CAP who have contraindications to both macrolides and fluoroquinolones is:•combination therapy with a b-lactam (ampicillin1sulbactam, cefotaxime, ceftaroline, or ceftriaxone, doses as above) and doxycycline 100 mg twice daily (conditional recommendation, low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

34
For educational purposes onlyShould Patients with Suspected Aspiration Pneumonia Receive
Additional Anaerobic Coverage beyond Standard Empiric Treatment for CAP In the Inpatient Setting?
• This guideline suggest not routinely adding anaerobic coverage for suspected aspiration pneumonia unless lung abscess or empyema is suspected (conditional recommendation, very low quality of evidence)
What Is the Appropriate Duration of Antibiotic Treatment In Outpatient and Inpatient Adults with CAP Who Are Improving?
• This guideline recommend that the duration of antibiotic therapy should be guided by a validated measure of clinical stability (resolution of vital sign abnormalities [heart rate, respiratory rate, blood pressure, oxygen saturation, and temperature], ability to eat, and normal mentation), and antibiotic therapy should be continued until the patient achieves stability and for no less than a total of 5 days (strong recommendation, moderate quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

35
For educational purposes onlyShould Adults with CAP and Risk Factors for MRSA or
P. aeruginosa Be Treated with Extended-SpectrumAntibiotic Therapy Instead of Standard CAP Regimens In the Inpatient Setting,?
•This guideline recommend abandoning use of the prior categorization of healthcare-associated pneumonia (HCAP) to guide selection of extended antibiotic coverage in adults with CAP (strong recommendation, moderate quality of evidence).
•This guideline recommend clinicians only cover empirically for MRSA or P. aeruginosa in adults with CAP if locally validated risk factors for either pathogen are present (strong recommendation, moderate quality of evidence).
•Empiric treatment options for MRSA include vancomycin (15 mg/kg every 12 h, adjust based on levels) or linezolid (600 mg every 12h).
•Empiric treatment options for P. aeruginosa include: piperacillin-tazobactam (4.5 g every 6h), cefepime (2 g every 8h), ceftazidime (2 g every 8h), aztreonam (2 g every 8h), meropenem (1 g every 8h), or imipenem (500 mg every 6h).
•If clinicians are currently covering empirically for MRSA or P. aeruginosa in adults with CAP on the basis of published risk factors but do not have local etiological data, we recommend continuing empiric coverage while obtaining culture data to establish if these pathogens are present to justify continued treatment for these pathogens after the first few days of empiric treatment (strong recommendation, low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

36
For educational purposes onlyShould Adults with CAP Be Treated
with Corticosteroids In the Inpatient Setting?
• This guideline recommend not routinely using corticosteroids in adults with nonsevere CAP (strong recommendation, high quality of evidence).
• This guideline suggest not routinely using corticosteroids in adults with severe CAP (conditional recommendation, moderate quality of evidence).
• This guideline suggest not routinely using corticosteroids in adults with severe influenza pneumonia (conditional recommendation, low quality of evidence).
• This guideline endorse the Surviving Sepsis Campaign recommendations on the use of corticosteroids in patients with CAP and refractory septic shock
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

37
For educational purposes onlyShould the Treatment Regimen Include Antiviral Therapy
In Adults with CAP Who Test Positive for Influenza?
• This guideline recommend that antiinfluenza treatment, such as oseltamivir, be prescribed for adults with CAP who test positive for influenza in the inpatient setting, independent of duration of illness before diagnosis (strong recommendation, moderate quality of evidence).
• This guideline suggest that antiinfluenza treatment be prescribed for adults with CAP who test positive for influenza in the outpatient setting, independent of duration of illness before diagnosis (conditional recommendation, low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

38
For educational purposes only
Should the Treatment Regimen Include Antibacterial Therapy In Adults with CAP Who Test Positive for Influenza?
• This guideline recommend that standard antibacterial treatment be initially prescribed for adults with clinical and radiographic evidence of CAP who test positive for influenza in the inpatient and outpatient settings (strong recommendation, low quality of evidence).
Should Follow-up Chest Imaging Be Obtained In Adults with CAP Who Are Improving?
• In adults with CAP whose symptoms have resolved within 5 to 7 days, we suggest not routinely obtaining follow-up chest imaging (conditional recommendation, low quality of evidence).
Metlay JP, et al. Am J Respir Crit Care Med 2019; 200(7): e45–e67

39
For educational purposes only
CONCLUSION

40
For educational purposes only
Conclusion
• CAP is major respiratory disease with a high prevalence in the general population, clinical heterogeneity and variable severity1
• In Asia CAP estimated to cause almost one million adult deaths per year with Streptococcus pneumoniae was the most commonly identified pathogen (13.3%) 2 while in Indonesia ICU P. aeruginosa was the predominant pathogen3
• Hospitalized patients with CAP should receive the first antibiotic dose in the ED. 4
• Non ICU patient:• β-lactams + macrolide or• Respiratory fluoroquinolone
• ICU Patient routinely need antibiotic cover the 3 most common severe CAP pathogens, all the atypical pathogens, and most of the relevant Enterobacteriaceae spp includes the following:• Beta-lactam + macrolide or respiratory fluoroquinolone
• If Pseudomonas is suspected, therapy is as follows:• Anti-pneumococcal and anti-pseudomonal beta-lactam (piperacillin/tazobactam, cefepime,
carbapenem [imipenem, meropenem, or doripenem]) + ciprofloxacin or levofloxacin or• Beta-lactam (as above) + aminoglycoside and azithromycin or aminoglycoside and
fluoroquinolone• Patients with CAP should be treated for a minimum of 5 days (level I evidence), afebrile for 48–72 h,
and should have no more than 1 CAP-associated sign of Clinical instability before discontinuation of therapy. 4
1. ERS European Lung White Book, Chapter 18 - Acute lower respiratory infections. Accessed thru http://www.erswhitebook.org/chapters/acute-lower-respiratory-infections/ on 26 August 2016
2. Peto, L., et al. Trans R Soc Trop Med Hyg 2014; 108: 326–337.3. Radji, et al. Asian Pac J Trop Biomed 2011;1:39-424. Mandell, LA, et al. Clinical Infectious Diseases 2007; 44:S27–72.