Embed Size (px)
Citation preview

Rational Use of Antibiotics in Respiratory Tract Infections
nzbpacbetter edicin m e

bpacnz Development Team: RachaelClarke
SoniaRoss
DrTrevorWalker
DavidWoods
Acknowledgement:
bpacnzwouldliketothankProfessorBruceArroll,DrRosemaryIkram,ProfessorJimReid,DrDavidReithandDrNeilWhittakerfortheir
helpandguidanceonthedevelopmentofthisresource.
Developedbybpacnz
Level8,10GeorgeStreet
POBox6032
Dunedin
Phone034775418
Fax0800bpacnz(0800272269)
Contact:[email protected]
www.bpac.org.nz
©bpacnzAugust2006
Allinformationisintendedforusebycompetenthealthcareprofessionalsandshouldbeutilisedinconjunctionwithpertinentclinical
data.
www.bpac.org.nz

Key Points Rational use of Antibiotics in Respiratory Tract Infections
Generalprinciplesofrationalantibioticuse 2
Part 1 Rational use of Antibiotics in Upper Respiratory Tract Infections
1a. Commoncold(viralrhinosinusitis) 3
1b.AcuteSinusitis 4
1c.Acutesorethroat 5
1d.Influenza-likeillness 7
1e.OtitisMediainchildren 9
1f.Croupandepiglottitis 12
1g. Pertussis 13
Part 2 Rational use of Antibiotics in Lower Respiratory Tract Infections in Adults
2a. Acutebronchitis 14
2b.Communityacquiredpneumonia 15
2c. COPD 16
Part 3 Rational use of Antibiotics in Lower Respiratory Tract Infections in Children
3a.Pneumonia 18
3b. Bronchiolitis 20
Appendices SoreThroatScore 21
SummarySheet 22
References 24
Contents

New Zealand general practitioners have done well in moving
toward more rational antibiotic use. Rational use of antibiotics
reducesresistanceratesforthecommunityasawhole(Molstad,
1999,Hefferman,2002).Italsoimportantlyreducesthelikelihood
of individuals developing resistant bacteria. People who take
antibioticshaveincreasedriskofdevelopingresistantstrainsof
bacteria,forexamplearesistantstrainofpneumococcusintheir
nasopharynx(Dowell,1998).
Thesituationhere inNewZealand isunlikeanAmericanstudy,
which reported that 46% of patients presenting to doctors
with thecommoncoldwereprescribedantibiotics for thisviral
infection.Worse,51%oftheantibioticsusedwerebroad-spectrum
(Steinman,2003).Neverthe less,therewerethreequartersof
amillionprescriptionsforamoxicillin-clavulanate(Augmentin®)in
NewZealandin2005(Pharmhousedata).
Evenwhenantibioticsare indicated,theuseofbroad-spectrum
antibiotics such as amoxicillin-clavulanate, second generation
macrolides,cephalosporinsandquinolonesasfirst line therapy
for respiratory tract infections encourages the development of
resistantstrainsandsubstantiallyaddstocosts.
Whenapersontakesanantibiotictotreatanillness,thedrugkillssusceptiblebacteria.Thisleavesbacteriathatcanresist
it-resistantbacteria.Withthereducedcompetition,resistantbacteriacanincreasetheirnumbersexponentially,tobecome
predominant. Broad-spectrum antibiotics kill a wide-range of bacteria allowing resistant strains which were previously an
insignificantminoritytopredominate.
General principles of rational antibiotic use
Avoidprescribingantibioticsforviralinfections.
When antibiotics are indicated, choose the
appropriate dose and duration of an effective
agentwiththenarrowestspectrum,fewestside
effectsandlowestcost.
Application of these principles to the treatment of
respiratorytractinfectionswouldresultinnoprescribing
of antibiotics for viral infections such as the common
cold and a selection between penicillin V, amoxicillin
orerythromycinasfirst line therapy formostbacterial
respiratoryinfections.Thiswouldreducethedevelopment
of organisms resistant to second line agents, reduce
nationalprescribingcosts,and reduceadverseeffects
toantibioticswithoutcompromisingpatientcare.
•
•
Rational Use of Antibiotics in Respiratory Tract Infections
Key Points
“Theprevalenceofantibioticresistanceinacountryreflectsthelocalconsumptionofantibiotics.Themajorityofantibioticsareprescribed
ingeneralpracticeandmostprescriptionsareattributabletotreatmentofrespiratorytractinfections.”(Bjerrum,2004).
2 IbpacnzInfections

Rational Use of Antibiotics in Upper Respiratory Tract
InfectionsAnoverviewofCochranereviewsontheuseofantibioticsforupperrespiratoryinfectionsrevealsalimitedroleforantibiotics
inacuteotitismedia,sorethroatandstreptococcaltonsillitis,commoncoldandacutepurulentsinusitis(Arroll,2005).
Part 1
Principles for rational antibiotic use
for the common cold
Antibiotics are not beneficial for the
commoncold.
Mucopurulent discharge frequently
accompanies the common cold.
It is not an indication for antibiotic
treatmentunless itpersistsfor10to
14days.
1.
2.
1a. Common cold (viral rhinosinusitis)
Mostchildrenwillhave3to8coldsperyear;however10%-15%
will have 12 or more per year. Higher incidences seem to be
related to starting school or day care. The incidence is much
reducedinadultlife.
Commoncold is usually accompanied bymild fever and some
degreeofsinuscongestion.Itfrequentlyresultsinmucopurulent
nasaldischargeorcoughandoftenlastsforupto10days.
Antibioticshavenoeffecton thedurationorseverityofanyof
thesecomponentsofthecommoncoldnordotheydecreasethe
likelihood of progression to bacterial infection. Short term use
oforalor topicalnasaldecongestants ismore likely toprovide
symptomaticrelief.
bpacnzInfectionsI3

1b. Acute Sinusitis
Identifying people who will benefit from antibiotic use
Sinus congestion related to viral rhinosinusitis is approximately 20 to 200
timesmorecommonthanbacterialsinusitis.Rationalantibioticuserequires
prescriberstocorrectlyidentifypatientswhoaremorelikelytohavebacterial
sinusitis.
Theseare:peoplewith:
Severeclassicalsymptomsoffacialpainandswelling,
Temperature>390C,
Toothpainnotofdentalorigin,or
Knownanatomicalblockage.
Orpeoplewith:
Rhinosinusitisandcoughnotimprovingafter10days.
Choice and duration of antibiotic for bacterial sinusitis
Acutebacterialsinusitis isusuallycausedby thesamebacterialpathogens
that cause acute otitis media (Streptococcus pneumoniae, Haemophilus
influenzae,andMoraxella catarrhalis).Nasopharyngealculturesarenotuseful
topredictthesinuspathogen.
Amoxicillin issuccessful for the initial treatmentofmostepisodesofacute
bacterial sinusitis, despite beta-lactamase production by some isolates
ofH. influenzae andM. catarrhalis. For the fewpatientswhoget recurrent
infectionsordonotrespondtoamoxicillinin48to72hours,abeta-lactamase-
stable agent, such as amoxicillin-clavulanate is appropriate. Doxycycline,
cotrimoxazoleorcefaclorareappropriatealternativesforpeopleallergicto
penicillin.
Theusualcourseoftreatmentisatleast10daysandthereisnoadvantage
in prolonging treatment more than 7 days beyond the point of substantial
improvementinsignsandsymptoms.
•
•
•
•
•
Principles of rational antibiotic use
for acute sinusitis
Sinuscongestionaccompanyingthe
commoncoldisthemostfrequent
causeofafeelingofpressureinthe
sinuses.
Analgesia and short-term nasal
decongestants usually provide
symptomaticrelief.
Bacterial sinusitis is diagnosed
whentherearespecificsymptoms
whichsuggestbacterialsinusitisor
when rhinosinusitis and cough are
notimprovingafter10days.
Routineradiographsarenotuseful
indeterminingabacterialaetiology
ofsinusitis.
Initial antibiotic treatmentofacute
bacterial sinusitis should be with
the narrowest spectrum agent
that is effective against the likely
pathogens(amoxicillin).
Antibiotics are usually prescribed
foratleast10days.
1.
2.
3.
4.
5.
6.
Further reading:
Acutesinusitisinadults.InstituteofClinical
SystemsImprovement.(2004)
Availablethroughhttp://snipurl.com/temk
4 IbpacnzInfections

1c. Acute sore throat
Clinical signs and symptoms are not reliable in differentiating viral from bacterial sore throats.
Viralandbacterialsorethroatscannotbereliablydifferentiatedbyclinical
signsorsymptoms,severityordurationof illness.Scoringsystemscan
helpdeterminetheprobabilityofapositivethroatswabforGroupAbeta
haemolyticstreptococcus(GABHS)(Appendixone).GABHSpharyngitis is
uncommoninchildrenunderthreeyears.
People with a past history of rheumatic fever or who are at high risk of rheumatic fever with positive throat swab for GABHS are likely to benefit from penicillin.
In countries with low incidences of rheumatic fever (most developed
countries)therisksofantibioticuseoutweightheirbenefitsinpreventing
rheumatic fever. However in New Zealand there are higher rates of
rheumatic fever especially among Pacific peoples and Māori. Professor
Diana Lennon points out that Cochrane reviews often include studies
predominantly performed in developed countries. In some communities
in thenorthernNorth Islandwecontinue to havea high risk thirdworld
type infectiousdiseaseprofileformanythings includingrheumaticfever,
but also suppurative complications of pharyngitis such as otitis media,
mastoiditisandquinsy.
Thecorrectstrategyfordealingwiththisproblemisnotyetdetermined,
andtheNewZealandHeartFoundationiscurrentlypreparingguidelinesfor
sorethroatmanagementwithintheNewZealandcontext.
Asthepreventionofrheumaticfeverisnotcompromisedbydelaysofup
toninedaysinstartingantibiotictreatment,apragmaticstrategymaybe
totakethroatswabsfrompeoplewhoaredeemedtobeathigherriskof
rheumatic fever and give them back-pocket prescriptions to get filled if
swabresultsreturnaspositive.Peopleathighriskinclude:
Māoripeople
Pacificpeople
People with lower socioeconomic status living in overcrowded
accommodation
People living in communities with high prevalence of rheumatic
fever.
•
•
•
•
Principles of rational antibiotic use
for acute sore throat
Most sore throats are viral and
will not benefit from antibiotic
treatment.
Theprincipalindicationforantibiotic
treatment in acute sore throat in
New Zealand is for primary and
secondarypreventionofrheumatic
feverforthoseatincreasedrisk.
People with severe systemic
symptoms may benefit from
antibiotics.
When antibiotics are indicated,
penicillinV(phenoxymethlpenicillin)
isthefirstchoicewitherythromycin
forpeoplewhoareallergictothis.
1.
2.
3.
4.
Pamphlets for patients about back-pocket
prescriptionscanbeorderedordown-loaded
fromwww.bpac.org.nz
bpacnzInfectionsI5

People with severe systemic symptoms or people at risk because of other medical conditions such as immunosupression may benefit from antibiotics.
Peoplewithseveresystemicsymptomsareusuallyexcludedfromclinicaltrialsoftheeffectiveness
ofantibioticsanditisprobablyappropriatetoofferantibioticstothesepeople.
People with severe local symptoms may benefit from penicillin.
Peoplewhohaveatleastthreeofthefollowingcriteriamayhavetheirsymptomdurationreducedby
abouteighthoursbytreatmentwithpenicillin.
Fever
Purulenttonsils
Cervicaladenopathy
Absenceofcough
Penicillin V is first choice when antibiotics are indicated for sore throat
Phenoxymethylpenicillin (penicillin V) is first choice because it remains effective againstGABHS.
Itistheonlyantibioticthathasbeenshowntoeffectivelypreventprimaryandsecondaryattacks
of rheumatic fever.Twoor threedailydosesareaseffectiveas fourdailydosesbut,when the
indicationfortreatmentistoeradicateGABHSforrheumaticfeverprevention,a10-daycourseis
required.Itmustbetakenonanemptystomach.
Broad-spectrum antibiotics are no more effective and increase the risk of developing resistant
organisms.Inadditionthesyntheticpenicillinssuchasamoxicillinoramoxicillin-clavulanatearelikely
toproducearashifthepersonhasglandularfever;resultinginthemistakenassumptionthatthe
personisallergictopenicillin.
Erythromycinissuitableforpeoplewhoareallergictopenicillin.
Antibiotics do not prevent glomerulonephritis, local respiratory tract complications or progression to pneumonia.
AntibioticsdonotsignificantlyreducetheincidenceofglomerulonephritissecondarytoGABHS.
Thenumberneededtotreat(NNT)topreventprogressiontootitismedia,sinusitis,quinsyorother
suppurativecomplications ishigh.Forexampleantibioticsneedtobegiventoabout150adults
withsorethroatstopreventoneprogressingtootitismedia.TheNNTforchildrenisabout30and
thereforeitmaybeworthwhilegivingpenicillintochildrenwithahistoryofotitismediaorthosewith
ahigherriskofprogressiontosuppurativecomplicationsbecauseofdemographicfactors.
Antibioticsdonotpreventprogressionofupperrespiratorytractinfectionstopneumonia.
•
•
•
•
6 IbpacnzInfections

1d. Influenza-like illness
TheNewZealandcasedefinitionforaninfluenza-likeillness
is“anacuterespiratorytractinfectioncharacterisedby
an abrupt onset of two of the following: fever, chills,
headache and myalgia”. It is a significant health issue
with10to20%ofNewZealandersaffectedeachyear.
Influenzaisdifficulttodistinguishclinicallyfromthewide
range of other viruses and bacteria that cause similar
symptoms. Diagnostic testing is not usually indicated
exceptforsurveillancepurposes.
Principles of rational antibiotic use in
influenza-like illness
Immunisation is the best protection against
influenza.
Antibiotics are not beneficial in influenza-
like illnesseswhen bacterial causes such as
pneumoniahavebeenclinicallyexcluded.
Peoplewithinfluenza-likeillnessesneedwritten
informationaboutwarningsignsandactionsto
takeforseriousillnesssuchasmeningococcal
disease.
1.
2.
3.
A–Allpeople65yearsofageandolder
B–Peopleunder65yearsofage,includingchildrenwith:
cardiovasculardisease(ischaemicheartdisease,congestiveheartfailure,rheumaticheart
disease,congenitalheartdisease,cerebrovasculardisease)
chronic respiratory disease (asthma if on regular preventive therapy; other chronic
respiratorydiseasewithimpairedlungfunction)
diabetes
chronicrenaldisease
anycancer,excludingbasalandsquamousskincancersifnotinvasive
other conditions (autoimmune disease, immune suppression, human immunodeficiency
virus (HIV), transplant recipients, neuromuscular and central nervous system diseases,
haemoglobinopathies,childrenonlongtermaspirin).
•
•
•
•
•
•
Immunisation is the best protection against influenza
AnnualimmunisationisfreeinNewZealandforthefollowinggroupsofpeople:
bpacnzInfectionsI7

Meningococcal disease may present as a flu-like illness
Meningococcal meningitis often presents with a headache but
meningococcalsepticaemiaoftendoesnotand ismuchmoredifficult to
diagnose.MeningococcaldiseasecanaffectanyonebutratesamongMāori
andPacificpeoplesarehigh.Onaverage,Māoricontractmeningococcal
diseaseatdoubletherateofEuropeans;andPacificpeoplesatfourtimes
therateofEuropeans.Approximately80%ofcasesoccurinpeopleaged
0-19years.
Forallethnicgroups,therateofdiseaseisparticularlyhighamongchildren
underfive-yearsold.Abouthalfofallmeningococcaldiseasecasesoccur
inthisagegroup.Oneinevery117Māorichildrenwillgetmeningococcal
diseasebythetimetheyreachfiveyears.Oneinevery66Pacificchildren
andone inevery438childrenofotherethnicitieswillgetmeningococcal
diseasebythetimetheyturnfive.
Theoccurrenceofmeningococcal disease is expected to drop following
theintroductionoftheMeNZBvaccineprogramme,andtheearlysignslook
encouraging.Inthemeantime,peoplewithflu-likeillness,especiallythose
undertheageof20yearsshouldbegivenwritteninformationaboutlooking
forsignsofmeningococcaldiseaseandwhattodoshouldtheyoccur.
Order pamphlets
YoucanorderordownloadMinistryofHealthpamphlets.Availablethrough:
http://snipurl.com/sgg8
Further reading:
MeningococcalDisease.MinistryofHealth.MeningococcaldiseaseinNew
Zealand.Factsheetone.
Availablethrough:http://snipurl.com/sgfp
8 IbpacnzInfections

1e. Otitis Media in children
Differentiating between AOM and OME
Acute otitis media isapurulentmiddleear infection.Earache
usually occurs in association with systemic upset such as
irritability,restlesssleepandfever.
Typicalchangesofthetympanicmembraneinclude:
Bulgingwithlossofnormallandmarks,
Changeincolour(usuallyredoryellow),and
Reducedmobility.
These symptoms and signs may have resolved because of
perforationofthetympanicmembraneanddischargeofpus.
When acute symptoms have settled AOM frequently leaves a
persistentmiddleeareffusion.
Otitis media with effusionismiddleeareffusionwithnosigns
ofacuteinflammation.Themainsymptomishearingloss.
Examinationrevealsreducedmobilityofthetympanicmembrane
on pneumo-otoscopy or tympanometry; and several of the
followingfeaturesonvisualisationofthetympanicmembrane:
Abnormalcoloursuchasyellow,amber,orbluish;
Opacificationotherthanduetoscarring;
Retraction;and
Airbubblesoranair/fluidlevel.
Table 1: Diagnostic features of AOM and OME
•
•
•
•
•
•
•
Principles for rational antibiotic use in otitis
media
Episodesof otitismedia need tobeclassified
asacuteotitismedia(AOM)orotitismediawith
effusion(OME).
Acute Otitis Media
MostchildrenwithAOMcanbetreated
withappropriateanalgesia
Antibioticuseisreservedfor:
Childrenwithsystemicsymptoms,
Children under three years with
severeorbilateralAOM,and
Childrenundersixmonths.
A five-day course of high dose
amoxicillin is appropriate for most
childrenwhenantibioticsareindicated.
Otitis Media with Effusion
Persistent middle ear effusion (OME)
after AOM is expected and does not
requiretreatment.
Antibiotic treatment is not usually
recommended.
•
•
•
•
•
Earache
Fever
Irritability
Middle
ear
effusion
Opaque
drum
Bulging
drum
Impaired
drum
mobility
Hearing
loss
AOM Present Present Present Maybepresent Present Present
OME Usuallyabsent Present Maybeabsent Usuallyabsent Present Usuallypresent
bpacnzInfectionsI9

Most children with AOM do not benefit from antibiotics.
Most episodes of AOM settle spontaneously without
ongoingproblems.Antibioticshavelimitedbenefits;about
17 children with AOM need to be treated with a broad-
spectrumantibioticforonechildtobenefit,andtheiruse
isassociatedwithaneardoublingoftheriskofvomiting,
diarrhoeaorrashes(Glasziouu,2002).
Anappropriatestrategyistotargettheminorityofchildren
athigherriskofpooroutcomebyreservingantibioticsfor:
Childrenwithsystemicfeatures(hightemperatureor
vomiting)(Little,2002),
Children under three years with severe or bilateral
AOM,and
Childrenundersixmonths(Kaleida,1991).
Anotherusefulstrategyistogiveabackpocketprescription
for antibiotics, to be collected at the parents’ discretion
after72hoursifthechildhasnotimproved.Mostparents
arecomfortablewiththisapproachanditreducesantibiotic
use(Little,2001;Arroll,2003).
Five days of high dose amoxicillin is appropriate when antibiotics indicated in AOM.
Streptococcus pneumoniae and Haemophilus influenzae
areusually implicated inbacterialAOM.Amoxicillin is the
drugofchoice ifanantibiotic istobeused.HIghdoses
are used to combat non-susceptible S.pneumoniae. The
recommended dose is 15mg/kg (up to 500mg) TDS or
30mg/kg(upto1000mg)BD,forfivedays.Cotrimoxazole
andcefaclorareeffectivealternatives.
Decongestants and antihistamines are not useful in AOM.
Giventhelackofbenefitandincreasedriskofsideeffects,
theuseofdecongestant,antihistamine,ortheircombination
isnotusefulforchildrenwithAOM(Flynn,2002).
•
•
•
Paracetamol is the best option for analgesia in AOM.
Paracetamolatadoseof15mg/kgfourtimesperdayis
themostappropriateoptionforpainreliefinAOM.However
parentsshouldbewarnedofthedangersofoverdosage.
Although non-steroidal anti-inflammatory drugs such as
ibuprofenareeffective,cautionshouldbeexerciseddueto
thesideeffectprofileofthisclassofdrugs.
Two randomised controlled trials show no benefit of
insertingoilsinreducingpaininAOM.
Referral for AOM
Thereareno trialsofwhenreferral is indicated forAOM.
This is usually appropriate and urgent when there are
seriouscomplications,suchasmastoiditis;anditmaybe
requiredwhenapatienthasseveralrecurrencesinashort
timespan;oraperforationisslowinhealing.
Management of OME
OME is a very common condition that usually resolves
spontaneouslyanddespitecommonbelieftheevidencefor
itsimpactonlearningdifficultiesislimited.
Antibiotics are not usually helpful for children with OME.
Thereissomeshort-termbenefitfromtheuseofantibiotics.
Howevertheyhave little influenceon long-termoutcomes
andtheincidenceofsideeffectsincludingdiarrhoea,skin
rashes,allergydevelopment,anaphylaxisanddevelopment
ofresistantstrainsoforganismisconsiderable.
10 IbpacnzInfections

There is no evidence to support the routine use of antihistamines, decongestants or mucolytics in the management of OME.
Studies considering interventions with antihistamines, decongestants
ormucolyticsshownoconvincingbenefitsontheclearanceofmiddle
eareffusions.
Topical or systemic steroid therapy is not recommended in OME.
Reviewoftheliteratureconcludedthattheuseofsteroidscouldnotbe
recommendedforOME(Butler,2002).
Referral
ForchildrenunderthreeyearswithOMEandmildtomoderatehearing
loss(<25dB)andnootherproblems,thereisconsistentevidencethat
watchfulwaitingisasgoodasearlysurgery(Paradise,2000,Rovers,
2000). It should be noted that children in these trials all underwent
audiometrytoexcludeamoreseriousdegreeofhearingloss.
Some trials,which includedchildrenover threeyearsand thosewith
behavioural or language problems have shown some benefit (Maw,
1999,Wilks,2000).
Further reading:
Scottish Intercollegiate Guidelines Network. (2003) Diagnosis and
managementofchildhoodotitismedia.Guideline66.Availablefrom:
http://www.sign.ac.uk/guidelines/fulltext/66/index.html
bpacnzInfectionsI11

1f. Croup and epiglottitis
Croup can be clinically diagnosed in children with typical barking cough, stridor,
hoarsevoice,othersignsofrespiratorydistressandrelativelymildsystemicupset.
It may be confused with epiglottitis, inhaled foreign body, bacterial tracheitis or
retropharyngealabscess.
Most children with croup can be treated at home
Childrenwithcroupwiththefollowingfeaturesmaybesuitableformanagementat
home:
Minimalstridoratrest,
Nosternalretraction,
Nosignsofhypoxia,and
Notsignificantlydistressed.
Forchildrenmanagedathomeoralsteroidsstartedondayonemayhelpprevent
deteriorationondaytwoorthree.Prednisolone(Redipred®)atadoseof1to2mg/
kgperdayisgivenfor3to4days.
There is no evidence that inhaled mist or steam is helpful but some children do
improvewithachangeinairtemperature.Reviewwillbenecessaryiftherearesigns
ofdeteriorationsuchassternalretraction,restlessnessorlethargy.
When epiglottitis is suspected parenteral antibiotics may be indicated
Epiglottitis is rarenowthanks to theuseofHib immunisation.The following table
from the Starship Children’s Health Clinical Guideline helps distinguish epiglottitis
fromseverecroup.
Table 2: Guidance to help distinguish epiglottitis from severe Croup
•
•
•
•
Croup Epiglottitis
Onset Days Hours
Fever ++ +++
Cough +++ -
Drooling + ++
Activity Upset Lethargic
Signs of
obstruction+++ +
Stridor Inspiratory,highpitched Softexpiratorysnore
Principles of rational antibiotic use
in croup and epiglottits
Antibioticsarenotindicatedinthe
treatmentofcroup.
Epiglottitis is rare but may be
confusedwithseverecroup.
Parenteralantibioticsareindicated
whenepiglottitisissuspected.
1.
2.
3.
Further reading:
Croup.StarshipChildren’sHealth
ClinicalGuideline.Availablethrough:
http://snipurl.com/se8o
Although epiglottitis is rare,
practitioners, especially those in
rural areas, need to be ready if
theyencounter it.Localitiesvary
inthesystemstheyhaveinplace
for dealing with this emergency
and practitioners need to know
whatthelocalsystemisandhow
toinitiateit.
12 IbpacnzInfections

1g. Pertussis
PertussiscontinuestocauseproblemsinNewZealandprimarilybecausewedonot
immuniseourchildrenadequately.
Pertussis has an incubation period of 7 to 20 days. The clinical case definition in
NewZealandiscoughformorethan14dayswithoneormoreofwhoop,cyanosis,
post-tussivevomitingorapnoeaforwhichthereisnootherknowncause.Thepeakof
severityusuallydoesnotoccuruntilthecoughhasbeenpresentforthreeweeks.
Pertussisshouldbesuspectedbeforethe14dayswhenthesesymptomsarepresent
particularly if there are no signs of tachypnoea, wheeze or crackles because it is
highlycommunicableintheearlystages.Thecommunicableperiodcontinuesforthree
weeksinpersonsnottreatedwithantibiotics,oruntil5daysofa14-daycourseof
erythromycin.
Diagnosis of Pertussis is usually confirmed by pernasal swab.
Confirmationofthediagnosisisusuallybyapernasalswab,whichispassedgently
along the base of the nasal cavity to reach the posterior nares. Cultures are only
positiveinthecatarrhalphaseandthefirstweekofparoxysmalcoughing.Serology
canalsobedonebuttheinterpretationoftheresultscanbeproblematic.
Erythromycin is recommended for treatment and prophylaxis
Erythromycin is the recommended treatment for cases andprophylaxis for certain
contacts.Theinitiationoferythromycinisnotdelayeduntiltheresultsoftheswabare
available.Thedoseis40-50mg/kgperday(maximum2gperday)individeddoses
for14days.Cotrimoxazoleisanalternativebutitisnotaseffective.
Treatallhouseholdmemberswitha14-daycourseoferythromycinifthehousehold
includeseither:
Achildunderoneyearotherthanthecase,or
Awomanlateinthethirdtrimester.
Reducing the spread of infection
Excludeallpre-schoolersfrompre-schooliftheyhavehadpertussisandexclude
childrenunder10-yearswhoarenotfullyimmunisedfromschool,untilthey:
havehadfivedaysofa14-daycourseoferythromycin,or
for14daysaftertheirlastexposuretoinfection.
Considerswabbingothersymptomaticsiblings.
NotifycasestotheMedicalOfficerofHealth.
•
•
•
•
•
Principles of rational
antibiotic use for pertussis
Theevidenceofbenefitfor
erythromycinonthecourse
of the illness is relatively
poor.
Erythromycin reduces the
length of time that people
with pertussis are culture
positive.
1.
2.
Further reading:
Pertussis.StarshipChildren’sHealthClinical
Guideline.
Availablethrough:http://snipurl.com/se8j
Petussis: GP flowchart, Immunisation
AdvisoryCentre.Availablethrough:
http://snipurl.com/oez4
bpacnzInfectionsI13

2a. Acute bronchitis
Acutebronchitisisdiagnosedclinicallywhenapreviouslywellperson
presentswithcoughwithsputumproduction,dyspnoeaorwidespread
wheeze. Localised, focal chest signs or severe systemic upset are
absent.Itisusuallyamild,self-limitingvirusinfection.Thereissome
doubt whether the condition actually exists. Most cases are in fact
either the common cold, asthma, pneumonia or an exacerbation of
COPD(Arroll,2001).
Previouslyhealthypeoplewithacutebronchitisdonotgetsignificant
benefit from antibiotic use. Patient understanding of this may be
improvedifthetermviralbronchitisisused.
Coughmaylastforfourweeksbutdurationorseverityofsymptoms
is not significantly changed by antibiotics, beta-agonist or cough
medicines.Smokeavoidance isbeneficialandparacetamolandhigh
fluidintakemaybehelpfulifthepatienthasahighfever.
Ifapatienthasasignificantcomorbidity,lookssickorisover55years
empiricaltreatmentwithamoxicillin,erythromycinordoxycyclinemay
beappropriate.Amoxicillin-clavulanate isbetter reserved for the few
occasionswherefirstlineagentshavenotbeeneffective.
Principles for rational antibiotic
use for acute bronchitis
Antibioticsarenotindicatedfor
previously healthy peoplewith
acutebronchitis.
Thepresenceofmucopurulent
sputumisnotanindicationfor
antibioticuse.
Antibiotics may be useful for
people over the age of 55
yearswholooksick.
1.
2.
3.
Rational Use of Antibiotics in Lower Respiratory Tract
Infections in Adults
Part 2
14 IbpacnzInfections

2b. Community acquired pneumonia
Communityacquiredpneumoniacanbediagnosedclinically,
without the need for microbiological and radiological
investigations,whenapatientacquiresalowerrespiratory
tractinfectioninthecommunityandhas:
Newfocalchestsigns,
Systemicillnesssuchassweating,achesandpains
ortemperature>380C,and
Nootherexplanationfortheillness.
Many adults with CAP can be treated safely at home
AdultswithCAPwhoarelessthan50yearsofageandhave
nosignificantcomorbiditiesandnopsychosocialbarriersto
homecarecanbemanagedathomeasnon-severeCAPas
longastheyhaveallofthefollowingfeatures:
Nonewmentalconfusion,
Respiratoryrate<30/min,
SystolicBP>90anddiastolic>60,and
pO2(ifavailable)of>85.
Peoplewhodonotmeetthesecriteriaforhomecareare
likelytobenefitfromhospitalassessmentoradmission.
Amoxicillin remains the first line agent for CAP in the community
ThepreferredantibioticforCAPtreatedinthecommunityis
amoxicillin500mg–1.0gthreetimesdaily.Erythromycin
500mgfourtimesdailyisasuitablealternativeforthose
peoplewhoareallergictopenicillin.
•
•
•
•
•
•
•
Principles for antibiotic use in
community acquired pneumonia (CAP)
Only a small range of pathogens cause
CAP,thecommonestisS. pneumoniae.
People with non-severe community
acquired pneumonia can be given
empirical antibiotic treatment at home
withouttheneedformicrobiologicaland
radiologicalinvestigations.
People with severe CAP need hospital
admission and empirical antibiotics may
bestartedifadelaytoadmissionofmore
thantwohourswilloccur.
Amoxicillin at higher doses remains the
preferredagentforcommunitymanaged
CAPwitherythromycinforthosewhoare
allergictopenicillin.
Acombinationof these twoagentsmay
be appropriate in localities with high
prevalenceoflegionella.
1.
2.
3.
4.
5.
bpacnzInfectionsI15

TheseantibioticsarealsoappropriateforpatientswithsevereCAPwhowillexperiencesomedelayinreceivinghospital
treatment.PatientswhocannottakeoralmedicationmaybegivenpenicillinGorerythromycinparentally.
ThisrecommendationoftheBritishThoracicSocietytakesintoaccounttherarityoffailuresofpenicillintreatmenteven
amongpenicillinresistantpneumococcalpneumonia,theuncommonoccurrenceofbeta-lactamaseproducingstrainsof
H. influenzaeorM. catarrhalisascausesofCAP,andconcernsaboutthesafetyofneweragentsandthedevelopment
ofresistantstrainstothem.
When there is higher prevalence of legionella in the local community it is appropriate to combine amoxicillin and
erythromycinasfirstlinetherapy.
Aviewthatspecificpathogensareassociatedwithothercomorbidities,suchasCOPDorinfluenza,isnotsupported
bytheliterature.
Patientswhoaremanagedathomewhonolongerfitthecriteriaforhomecareordonotimprovein48hoursrequire
hospitalassessmentandprobableadmission.
Further reading
Guidelinesforthemanagementofcommunityacquiredpneumoniainadults.BritishThoracicSociety.2001updated
2004.Availablethroughhttp://snipurl.com/sccm
Principles of rational antibiotic use
in COPD
Prophylacticantibiotictherapyisnot
recommended in the management
ofstableCOPD.
People with exacerbations but
without more purulent sputum or
signs of pneumonia do not need
antibiotictherapy.
People with exacerbations
accompaniedbyincreaseinpurulent
sputumproductionmaybenefitfrom
amoxicillinordoxycycline.
1.
2.
3.
2c. COPD
Studiesontheroleofantibioticsinthemanagementofexacerbationsof
COPDaredifficulttointerpretowingtohighratesofbacterialcolonisation
in the sputum of people with COPD. There is increasing evidence that
manyexacerbationsarecausedbyvirusesandotherunidentifiedcauses.
Itappearsthatbacterialinfectionplayseitheraprimaryorsecondaryrole
inapproximately50%ofexacerbationsofCOPD.
16 IbpacnzInfections

Antibiotics are only indicated in COPD exacerbations with more purulent sputum or clinical signs of infection.
Exacerbations with clinical signs of infection (increased
volume and change in colour of sputum and/or fever,
leucocytosis)maybenefitfromantibiotictherapy.Theearlier
this is commenced the better and patients benefit from
havingahomesupplyofantibioticssothattheycaninitiate
treatmentthemselves.
When antibiotics are indicated either amoxicillin or
doxycycline for 7 to 10 days is appropriate as first line
therapy.Aresponseisusuallyseenwithinthreetofivedays.
Ifthereisnotasatisfactoryresponsebythenachangeto
amoxicillin–clavulanatecanbemade.
Signsofpneumoniashouldbesoughtand if found treated
appropriately.
Systemicglucocorticoidsreducetheseverityofandshorten
recoveryfromacuteexacerbations.
Influenza vaccination is beneficial for people with COPD
In people with COPD annual influenza vaccination reduces
the risk of exacerbations, hospitalisation and death from
respiratorydiseaseandallcauses.
Thevaccineusuallycontainsthreestrainswhichareadjusted
annually according to epidemiological data. The vaccine
shouldbegiveninearlyautumntoallpatientswithmoderate
tosevereCOPD.Asecondvaccination inwinter increases
antibody levels and should be considered for severely
immunocompromisedpatients.
Influenza vaccine is available fully subsidised on the
Pharmaceutical schedule between 1 March and 30 June
eachyearforpatientswithchronicrespiratorydisease.
Pneumococcal vaccination prevents pneumococcal pneumonia
Pneumococcal vaccination is very effective in preventing
invasivebacteraemicpneumococcalpneumonia,butmaybe
lesseffectiveinelderlyorimmunosuppressedpatients.There
isnofirmevidencethatthevaccineiseffectiveinpreventing
pneumococcal exacerbations of COPD but there are over-
ridingbenefitsinpreventingpneumoniainpatientswithalready
reduced respiratory reserve. Pneumococcal vaccination
(polyvalent covering 23 virulent serotypes – Penumovax-23)
is recommended but not currently funded for patients with
chronic pulmonary disease. Vaccination should be avoided
in patients with severely compromised cardiovascular or
pulmonaryfunction inwhomasystemicreactionwouldpose
agreaterrisk.
No evidence that Haemophilus influenzae vaccination beneficial in COPD
There is no evidence that currently available vaccines for
Haemophilus influenzae in New Zealand are effective in
reducingtheincidenceorseverityofbronchiticepisodes.
Further reading
TheCOPD-XPlan:AustralianandNewZealandGuidelinesfor
themanagementofChronicObstructivePulmonaryDisease,
2006.Availablethrough:
http://snipurl.com/sfuz
COPDPOEM.bpacnz.April2005.Availablethrough:
www.bpac.org.nz
bpacnzInfectionsI17

Pneumonia,bronchiolitisandasthmaareallcommoninchildren.Childrenwithpneumoniaarelikelyto
benefitfromantibiotictreatmentbutchildrenwithbronchiolitisorasthmaarenot.
Principles of rational antibiotic use in LRTI
in children
The diagnosis of pneumonia needs to be
considered.
Many children with pneumonia and no
significantco-morbiditiescanbetreatedat
home.
Theprincipalguidetoantibioticchoicefor
community management of pneumonia is
theageofthechild.
Antibiotics are not indicated in the
managementofbronchiolitisorasthma.
Antibiotics do not prevent pneumonia
in children with upper respiratory tract
infections.
1.
2.
3.
4.
5.
Rational Use of Antibiotics in Lower Respiratory Tract
Infections in children
Part 3
3a. Pneumonia
Tachypnoea Indrawing*
Wheezeandahistoryofwheeze
Childdoesnothavepneumonia
Childhaspneumonia
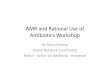
Figure 1: Child presents with cough or breathing difficulty
18 IbpacnzInfections
*Indrawingindicatesseverepneumonia.Achildwithindrawingwithafirstepisodeofwheezingshouldbetreatedasifthisillness
isseverepneumoniaeventhoughthediagnosismaybeprovedincorrectinthesubsequent24-48hours.
AdaptedfromWHOalgorithmfordiagnosingpneumonia.

Tachypnoea, chest indrawing and absence of wheeze are the principle signs for the diagnosis of pneumonia in pre-school children
A pre-school child can be assumed to have pneumonia if they have
tachypnoeaorchestindrawinganddonothaveacurrentwheezewitha
pasthistoryofwheeze.Nasalflaring,gruntingorcrepitationsincrease
theprobabilityofpneumonia.Atypicalpresentationsincludeabdominal
painandmeningismus.
The absence of tachypnoea reduces the likelihood of pneumonia. If
there is no respiratory distress, tachypnoea, crackles or decreased
breathsoundsthereisnopneumonia.
Thepresenceorabsenceoffeverisnotausefulsigninthediagnosisof
pneumoniainyoungchildren.
Many children with pneumonia can be treated at home
Children with pneumonia and no significant co-morbidities with the
followingfeaturesmaybesuitablefortreatmentathome.
Over6months
Donotlooktoxic
Mildrespiratorysymptoms
Drinkingwell
Abletotakeoralmedication
Noskinabscesses
Pneumonia is not a consequence of chickenpox, influenza or
measles.*
*Thepresenceofskinabscessesorrecentchickenpox,influenzaor
measlesmaybeassociatedwithstaphylococcalpneumoniawhichisa
paediatricemergency.
•
•
•
•
•
•
•
Age
Tachypnoea
Respiratoryrate
countedover60
seconds
<2monthsold>60breathsper
minute
2-12months>50breathsper
minute
12monthsto5years>40breathsper
minute
Table 3: The WHO definition of tachypnoea is
age dependent
bpacnzInfectionsI19

Age of the child is the best guide to antibiotic use in community management of childhood pneumonia
Sputumsamples,swabs,CBC,CRPorCXRdonotusuallydetermine
ifpneumoniaisviralorbacterialorwhichantibioticwouldbemost
appropriate. Age is the best guide to the causative agent and
thereforeantibioticchoice.
For children with pneumonia suitable for treatment at home the
followingantibioticsarerecommendedinTable4.
3b. Bronchiolitis
Bronchiolitis can be diagnosed clinically when a child up to the
ageof12monthsdoesnotmeet thecriteria for adiagnosisof
pneumoniaandhascough,tachypnoeaorhyperinflationofthechest
andexaminationrevealswidespreadcrepitationsandwheeze.Itis
oftendifficulttodifferentiatebetweenbronchiolitisandanepisode
ofacuteasthma.Thepresenceofatopy,previouswheezeorstrong
familyhistoryofatopyincreasesthelikelihoodofasthma.
Antibiotics are not indicated for bronchiolitis
Bronchiolitisisaviral infection(usuallyrespiratorysyncytialvirus)
anddoesnotrespondtoantibiotics.Thesymptomspeakat2to
3daysandresolveover7to10daysbutcoughmaypersistfor
severalweeks.
Many children with bronchiolitis can be managed at home
Childrenwithbronchiolitiswhoarefeedingandbehavingnormally
maybesuitableforcommunitymanagementiftheyhave:
Onlymildwheeze,
Noormildchestindrawing,
Nocyanosis,
Heartrate<160,and
Respiratoryrate<60.
Steroids or beta-agonists are not indicated in the community
managementofbronchiolitis.
•
•
•
•
•
Further reading:
Acute pneumonia in infants and children. Starship
Children’sHealthClinicalGuideline.Availablethrough:
http://snipurl.com/se3q
Bronchiolitis. Starship Children’s Health Clinical
Guideline.Availablethrough:http://snipurl.com/scii
Ageunder5years
Amoxicillin50mg/kgperday
(max500mgperdose)in
threedivideddosesfor7to
10days
Ageover5years
Erythromycin40mg/kgper
day(max500mgperdose)in
fourdivideddailydoses
Table 4: Age guide for antibiotic use
20 IbpacnzInfections

Appendix one
Table 5: A clinical score to reduce unnecessary antibiotic use in patients with sore throat
Criteria Point Score
Temp>38oC 1
Nocough 1
Tenderanteriorcervicaladenopathy 1
TonsilllarySwellingorexudates 1
Age3-14yr 1
Age15-44yr 0
Age≥45yr -1
Total score =
Ifyouscore4thenyouhaveahighlikelihoodofgrowingGABHSonthroatswab.
McIssacWJetalAclinicalscoretoreduceunnecessaryantibioticuseinpatientswithsorethroat.CanMedAssocJ1998;158:75-83.
Appendices
bpacnzInfectionsI21

Appendix two Summary table
Upper respiratory Tract Infections
Illness Comments Antibiotic (if indicated)
Consider delayed antibiotic prescriptions for upper respiratory tract infections
Influenza Annual vaccination is essential for all those at risk of influenza.
Pharyngitis,
sore throat &
tonsillitis
The majority of sore throats are viral; most patients do not benefit from antibiotics.
Main indications is rheumatic fever prophylaxis to those at high risk.
PatientswithseveresymptomsorchildrenwithhistoryofotitismediamaybenefitfromantibioticsA-.Antibioticsonlyshorten
durationofsymptomsby8hoursA+.Youneedtotreat30childrenor145adultstopreventonecaseofotitismedia.A+
Twice daily higher dose can be used.A- QDS
maybemoreappropriateifsevere.D
1st linephenoxymethylpenicillin500mgBD-QDSfor10days
if allergic to penicillin
erythromycin500mgBDor250mgQDS(lesssideeffects)for10days
Otitis media
(child doses)
Many are viral. Resolves in 80% without antibiotics.A+
Pooroutcomeunlikelyifnovomitingortemp<38.5oC.A-Useparacetamol.A-forpainrelief.
Antibioticsindicatedforchildrenundersixmonths,youngchildrenwithseverelocalsymptomsorchildrenwithsystemic
symptoms.
Antibioticsdonotreducepaininfirst24hours,
subsequent attacks or deafness.A+ Need to
treat20children>2yrsandseven6-24mold
togetpainreliefinoneat2-7days.A+B+
Haemophilusisanextracellularpathogen,thus
macrolides, which concentrate intracellularly,
arelesseffectivetreatment.
1stlineamoxicillin15mg/kg(upto500mg)TDS,or
30mg/kg(upto1000mg)BD
if allergic to penicillin cotrimoxazole8/40mg/kg/dayfor5days
dividedinto12hourlydoses
2nd line
amoxicillin-clavulanate1 - 6 yrs156mgTDSfor5days
6 - 12 yrs312mgTDSfor5days
Rhinosinusitis
acute or
chronicManyareviral.ReserveantibioticforsevereB+
orsymptoms>10days.
If failure to respond use another first line
antibiotic
amoxicillinA+500mgTDSfor7daysor,
doxycycline200mgstat/100mgODfor7days or,
erythromycin250mgQDS/500mgBDfor7daysor,
phenoxymethylpenicillinA+500mgTDSfor7days
22 IbpacnzInfections

Lower Respiratory Tract Infections
Illness Comments Antibiotic (if indicated)
Note: Avoid tetracyclines in pregnancy. Low doses of penicillins are more likely to select out resistance.
Acute bronchitis
Systematicreviewsindicateantibioticshave
marginalbenefitsinotherwisehealthyadults.A+
Reserveantibioticsforolderpeoplewholook
sick.Patientleafletscanreduceantibioticuse.B+
amoxicillin500mgTDSfor5daysor,
doxycycline200mgstat/100mgODfor5days
Acute
exacerbation of
COPD
Approximately50%bacterial.
Antibioticsnotindicatedinabsenceofpurulent/
mucopurulentsputum.B+
Mostvaluableifincreaseddyspnoeaand
increasedpurulentsputum.B+Inpenicillinallergy
useerythromyciniftetracyclinecontraindicated.
amoxicillin500mgTDSfor5daysor,
doxycycline200mgstat/100mgODfor5days
erythromycin250-500mgQDSfor5days
2nd line
amoxicillin-clavulanate625mgTDSfor5days
Community-
acquired
pneumonia -
treatment in the
community
Start antibiotics immediately.B- If no response in
48 hours or local high prevalence of legionella
consideramoxicillinpluserythromycinC
Inseverelyillgiveparenteralbenzylpenicillinbefore
admissionCandseekriskfactorsforLegionella.
amoxicillin500mg-1gTDSforupto10days or,
erythromycin500mgQDSforupto10days
Meningitis
Suspected
meningococcal
disease
Transferallpatientstohospitalimmediately.
Administerbenzylpenicillinpriortoadmission,
unlesshistoryofanaphylaxis,B-NOTallergy.
IdeallyIVbutIMifaveincannotbefound.
IVorIMbenzylpenicillinChildren< 1 yr300mg
Children1 - 9 yr600mg
Children10 yr and over1200mg
Note:Dosesareoralandforadultsunlessotherwisestated.PleaserefertoBNFforfurtherinformation.
AdaptedfromHealthProtectionAgency,UK.Originaltableavailablethroughhttp://snipurl.com/sqi4
Lettersindicatestrengthofevidence:A+=systematicreview:D=informalopinion
Produced2001-ReviewedApril2006-AmendedMay2006.
bpacnzInfectionsI23

References
Arroll,B.andKenealy,T.(2001).Antibioticsforacutebronchitis.
Fourreviewsandstillnoanswers.BMJ,322,939-940.
Arroll,B.(2005).Antibioticsforupperrespiratorytractinfections:
an overview of Cochrane reviews. Respiratory Medicine, 99,
255-261.
Arroll, B., Kenealy, T., and Kerse, N. (2003). Do delayed
prescriptionsreduceantibioticuseinrespiratorytractinfections?
A systematic review. British Journal of General Practice. 53,
871-7.
Arroll,B.(2005).Antibioticsforupperrespiratorytractinfections:
an overview of Cochrane reviews. Respiratory Medicine, 99,
255–261.
Bjerrum,L.,Boada,A.,Cots,J.,LlorC.,ForesGarciaD.,Gahrn-
Hansen,BandMunck,A.(2004).Respiratorytractinfectionsin
generalpractice:considerabledifferences inprescribinghabits
betweengeneralpractitionersinDenmarkandSpain.EurJClin
Pharmacol,60,23-8.
Butler, C. and van der Voort, J. (2002). Oral or topical nasal
steroidsforhearinglossassociatedwithotitismediawitheffusion
inchildren(CochraneReview).In:TheCochraneLibrary,Issue2.
Oxford:UpdateSoftware.
EBMReviews-CochraneDatabaseofSystematicReviews
Accession Number 00075320-100000000-00197. Author
Kozyrskyj, AL; Hildes-Ripstein, GE; Longstaffe, SEA; Wincott,
JL;Sitar,DS;Klassen,TP;Moffatt,MEK.GroupNameCochrane
AcuteRespiratoryInfectionsGroup.TitleShortcourseantibiotics
foracuteotitismedia.SourceCochraneDatabaseofSystematic
Reviews.1,2006.DateofMostRecentAmendment02-17-2005
DateofMostRecentSubstantiveAmendment02-18-2000.
Flynn,C.,Griffin,G.andTudiver,F. (2002).Decongestantsand
antihistaminesforacuteotitismediainchildren(CochraneReview).
In:TheCochraneLibrary,Issue2,Oxford:UpdateSoftware.
Glasziou, P., Del Mar, C., Sanders, S. and Hayem, M. (2002).
Antibioticsforacuteotitismediainchildren(CochraneReview).In:
TheCochraneLibrary,Issue2,Oxford:UpdateSoftware.
Hefferman, H. (2002). Annual summaries bacteriology. Lablink
10,9.
Kaleida,P.,Casselbrant,M.,Rockette,H.,Paradise,J.,Bluestone,
C.andReisingerK,etal.(1991).Amoxicillinormyringotomyor
bothforacuteotitismedia:resultsofarandomizedclinicaltrial.
Pediatrics,87,466-74.
Little, P., Gould, C., Moore, M., Warner, G., Dunleavey, J. and
Williamson, I. (2002).Predictorsofpooroutcomeandbenefits
from antibiotics in children with acute otitis media: pragmatic
randomisedtrial.BMJ,325,22.
Little, P., Gould, C., Williamson, I., Moore, M., Warner, G. and
Dunleavey, J. (2001). Pragmatic randomised controlled trial of
twoprescribingstrategiesforchildhoodacuteotitismedia.BMJ,
322,336-42.
Marcy, M., Takata, G., Shekelle, P., Mason, W., Wachsman, L.
andErnst, R. et al. (2001)Management of acuteotitismedia.
Rockville (MD): Agency for Healthcare Research and Quality;
Evidence Report/Technology Assessment No. 15. AHRQ
Publication No. 01-E010. [cited 16 Jul 2004]. Available from
url: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?call=bv.View..
ShowSection&rid=hstat1.chapter.21026
Maw,R.,Wilks,J.,Harvey,I.,Peters,T.andGolding,J.(1999).
Early surgery compared with watchful waiting for glue ear
and effect on language development in preschool children: a
randomisedtrial.Lancet,353,960-3.
24 IbpacnzInfections

Molstad,S. andCars,O. (1999).Major changes in the useof
antibiotics Following a national programme: Swedish Strategic
Programme for the Rational Use of Antimicrobial agents and
surveillanceofresistance.ScandJInfectDis,31,191–5.
Paradise,J.,Feldman,H.,Campbell,T.,Dollaghan,C.,Colborn,
D. and Bernard, B. et al. (2000). Effect of early or delayed
insertionof tympanostomy tubes forpersistentotitismediaon
developmentaloutcomesattheageofthreeyears.NEnglJMed,
344,1179-87.
Reidpath,D.,Glasziou,P.,DelMar,C.(1999).Systematicreview
ofautoinflationfortreatmentofglueear inchildren.BMJ,318,
1177.
Rovers,M.,Straatman,H., Ingels,K.,vanderWilt,G.,vanden
Broek,P.andZielhuis,G.(2000).Theeffectofventilationtubes
onlanguagedevelopmentininfantswithotitismediawitheffusion:
arandomizedtrial.Pediatrics.106,E42.
Steinman,M.,Landefeld,C.andGonzales,R.(2003).Predictors
of Broad-Spectrum Antibiotic Prescribing for Acute Respiratory
TractInfectionsinAdultPrimaryCare.JAMA,289,719-725.
Scott,F.,Dowell,S.,MarcyDagger,M.,William,P.,Gerberparallel,
M and Schwartz, B. (1998). Principles of Judicious Use of
Antimicrobial Agents for Pediatric Upper Respiratory Tract
Infections.PEDIATRICSVol.101No.1Supplement,163-165.
Wilks,J.,Maw,R.,Peters,T.,Harvey,I.andGolding,J.(2000).
Randomised controlled trial of early surgery versus watchful
waiting forglueear: theeffectonbehaviouralproblems inpre-
schoolchildren.ClinOtolaryngol,25,209-14.

nzbpacbetter edicin m e
www.bpac.org.nz








![Rational Antibiotic Use in the Management of … Antibiotic...Rational Antibiotic Use in the Management of Respiratory Tract [RTI] and Urinary Tract [UTI] Infections Noe B. Mateo,](https://img.pdfslide.net/doc/110x75/5ae2540a7f8b9ad47c8cf9fb/rational-antibiotic-use-in-the-management-of-antibioticrational-antibiotic.jpg)