Embed Size (px)
Citation preview

HematologyRBC disorders
Dr. Mehzabin Ahmed

Anemia
Def: Reduction in the circulating red cell mass is called anemia.
Thus there is a reduced oxygen carrying capacity of the RBCs
Compensatory changes: Decreased affinity of hemoglobin for the oxygen Increased cardiac output Attempted increase in the RBC production.

Symptoms
Easy fatiguibility
Dyspnoea on exertion
Faintness vertigo
Common features of anemias
Signs
Pallor
Rapid bounding pulse
Systolic murmurs
Dependent edema

Erythroid hyperplasia seen in the bone marrow in anemia

Reduced production Deficiency of hematinics
Iron deficiency Folate & B12 deficiency
Dyserythropoiesis Anemia of chronic disorders Myelodysplasia Sideroblastic anemia
Marrow infiltration Failure of production
Aplastic anemia Pure red cell aplasia
Increased destruction Hemolytic anemia
Intrinsic causes Membrane defects Enzyme deficiencies Hemoglobinopathy
Extrinsic causes Immune reactions Microangiopathic Parasitic
Hypersplenism Bleeding
Classification of anemia

Anemia due to deficiency of hematinics- Iron deficiency
Iron deficiency is the most common cause of anemia & is due to chronic
blood loss, deficient intake, and increased demand (pregnancy &
lactation)
Chronic blood loss is the most common cause of iron deficiency in
adults (peptic ulcers, cancers of the stomach & colon, menorrhagia,
urinary tract lesions)
Microcytic hypochromic anemia with a low serum total iron, increased
iron binding capacity, and decreased serum ferritin indicating reduced
iron stores
Clinical features: Angular cheilits, atrophic glossitis, esophageal webs,
koilonychia and brittle nails, fatigue, dyspnoea on exertion, tachycardia

Koilonychia- Spoon shaped nails
Microcytes- small RBCs
Hypochromic- RBCs with a large central pallor

Causes megaloblastic anemia
Synthesis of DNA in the marrow precursors is impaired
Pernicious anemia due to deficiency of intrinsic factor expressed on the
gastric parietal cells which results in malabsorption of vitamin B12
Autoimmune atrophic gastritis (resulting in the destruction of the gastric
parietal cells) &
Partial gastrectomy result in Disease/ surgical removal of terminal ileum
Folic acid deficiency may be due to deficient intake / increased demand
Pancytopenia with megaloblastic erythropoiesis is seen
Vitamin B12 deficiency is associated with neurological disease & impaired
cardiac function
Anemia due to deficiency of hematinics- Vitamin B12 & folic acid

Large oval RBCs

Anemia due to Dyserythropoiesis Anemia of chronic disorders is the second most common cause of
anemia. Disorders associated with anemia:
Autoimmune disorders like rheumatoid arthritis; Chronic infections like TB, malaria, schistosomiasis; Neoplasms like lymphoma and some carcinomas
Myelodysplastic syndromes: Production of abnormal clones of marrow stem cells which form
defective blood cells that are destroyed prematurely. Results in refractory anemias & pancytopenias. It progress to leukemia
Sideroblastic anemia :defective heme synthesis in the RBC precursors. Causes include- Toxins- lead, alcohol, Drug- isoniazid, Associated
with neoplasm, Due to myelodysplasia

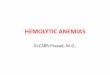
Anemia due to failure of production Aplastic anemia: there is a failure of the marrow stem cells.
The marrow is replaced by fat. Patients develop pancytopenia and have a life threatening disease. Many are idiopathic
Causes of secondary aplastic anemia: Radiation Chemotherapeutic agents Drugs like chloramphenicol, gold, NSAIDs Toxins like benzene Viruses like papovavirus, HIV-1 Fanconi’s anemia- Autosomal recessive disease

Aplastic anemia: hypocellular bone marrow is largely devoid of hematopoietic cells; often only fat cells, fibrous stroma,
Aplastic anemia

Anemia due to hemolysisIncreased destruction/ reduced red cell survival in the blood.
Causes:
1) Intravascular hemolysis occurs in: Hemolytic anemia
Intrinsic causes Membrane defects- hereditary spherocytosis Enzyme deficiencies- glucose 6 phosphate dehydrogenase deficiency Hemoglobinopathies- thalassemia, sickle cells anemia
Extrinsic causes Immune reactions- autoimmune hemolytic anemia Microangiopathic- DIC Parasitic
2) Extravascular hemolysis Hypersplenism Bleeding- trauma and accidents

Hereditary spherocytosis Spherocytes

G6PD deficiency
Heinz bodies Bite cells- schistocytes

Sickle cell Anemia Sickle cells

General clinical features of Hemolytic Anemias
Anemia
Jaundice: excessive breakdown of RBCs results in the
release of Hb, which is converted in the liver to bilirubin
& this, gives the yellowish discoloration to the tissues.
Pigment gall stone formation
Hepatosplenomegaly is seen due to extramedullary
hemopoiesis

Thalassemia Inherited defect in the synthesis of globin chains of the hemoglobin.
Common in the Mediterranean, Middle and Far East and South East Asia.
Mutations in the genes coding for the synthesis of & globin chains (normal adult
Hb- 2 & 2 chains).
Two types: depending on the chain affected (reduced or absent)
Thalassemia
Thalassemia
Thalassemia is of 2 types
major (microcytic hypochromic anemia with severe hemolysis, hepatosplenomegaly,
skeletal deformities and iron overload) and
minor (mild disease with microcytic hypochromic anemia).

Clinical features of Thalassemia Microcytic hypochromic anemia Hemosiderosis: the deposition of iron in the tissues like
The endocrine glands results in the development of diabetes mellitus, failure of sexual development.
Deposition in the heart and liver results in their failure. It is treated by iron chelation using desferroxamine.
Facial deformities: like frontal bossing and prominent maxillae resulting from the extramedullary hemopoieis in the
flat bones (like the skull bones, the ribs, etc) due to the hemolysis & severe anemia. Expansion of the bone marrow results in the cortical thinning and new bone is formed which
is deposited in the outer aspect of the bone. Cortical thinning predisposes to fractures. Hepatosplenomegaly is seen due to extramedullary hemopoiesis Hydrops fetalis: In extreme cases were all 4 chains are absent and in utero death of the fetus
occurs.

Thalassemia
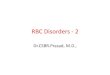
Hair on end appearance of the skull on X-ray- due to extramedullary hematopoiesis
Microcytic hypochromic RBCs
Puffy cheeks & frontal bossing
Pencil shaped RBCs
Target cells

Sickle cell anemia
Point mutation in the gene coding for globin chain resulting in an
abnormal type of hemoglobin, HbS. This HbS polymerizes when
exposed to low oxygen tension making the RBC rigid and becomes
sickle shaped.
The abnormal forms undergo lysis and anemia results.
Microvasculature (capillaries) get occluded (blocked) and infarction
(ischemic necrosis) of the tissues ( as in the spleen and bone marrow)
can occur

Sickle cell crises
Patterns of acute deterioration
Sequestration crises: sudden pooling of the RBCs in the spleen causes a
rapid fall in the Hb which can result in death
Infarctive crises: obstruction of the small blood vessels leads to
infarcts, especially in the bone (femoral head), spleen (resulting in
atrophy), skin ( ulcer formation) and in the bowel (acute abdominal
pain)
Aplastic crises: splenic atrophy due to repeated infarction predisposes
to infections which depresses the RBC production further reducing the
Hb

Hemolysis due to defects outside the RBCs- Extrinsic causes of hemolysis
These include the acquired causes of the hemolytic anemias:
Immune mediated hemolytic anemias: these may be autoimmune or may
be due to mismatched blood transfusion or hemolytic disease of the
newborn ( Rh incompatibility of the mother’s blood and the fetal RBC).
Physical trauma: as in burns and in artificial heart valves
Microangiopathic anemia: in DIC
Infections like malaria and rarely clostridia
Toxicity due to chemicals like lead, snake venom, and spider bites.
Extravascular hemolysis
Hyperslenism: Causes anemia due to increased functioning of the spleen in
the sequestering of the RBCs. Platelets & WBCs may also be decreased.

Direction ofblood flow
Fibrin
SchistocyteMicroangiopathic Trauma Seen in DIC were the fibrin
strands formed intravascularly results in the tearing up of the RBCs
Malarial parasite with in the RBCs

Polycythemia
It is the increase in the RBC mass above the normal levels.
The Hb concentration & the packed cell volume/ hematocrit are raised.
The blood is viscous (thick) and does not flow easily, predisposing to
thrombosis and thereafter infarction of organs like the brain, heart and
spleen.

Classification of polycythemias Primary: It is due to increased proliferation of the precursors of the RBCs,
WBCs and the platelets in the bone marrow (myeloproliferative disease). This
is known as Polycythemia rubra vera.
Secondary to increased erythropoietin levels: erythropoietin is a hormone
secreted by the kidney and it acts on the bone marrow simulating the RBC
production (erythropoiesis). It may be raised in
Hypoxic conditions like smoking, high altitude, lung diseases (like severe
chronic bronchitis, emphysema), congenital heart diseases
Tumors of the kidney, liver or brain resulting in increased production of
the erythropoietin.
Relative: it is seen when the plasma volume is depleted as in dehydration &
stress.

At the end of the lesson on RBC Disorders, the student should be able to:
1. Define anemias and classify them based on the mechanisms of their
production
2. Enumerate the clinical features of anemias in general
3. Enumerate the hemolytic Anemias
4. Describe briefly pathogenesis thalassemias and sickle cell Anemia
5. Enumerate the skeletal changes and complications in the thalassemia
and sickle cell anemia
6. Define polycythemia and classify it.







![FIS for the RBC/RBC Handover...4.2.1.1 The RBC/RBC communication shall be established according to the rules of the underlying RBC-RBC Safe Communication Interface [Subset-098]. Further](https://img.pdfslide.net/doc/110x75/5e331307d520b57b5677b3fa/fis-for-the-rbcrbc-handover-4211-the-rbcrbc-communication-shall-be-established.jpg)