-
8/6/2019 Reactions to Cold
1/52
Cutaneous reactions to cold
Dr geetika paul
-
8/6/2019 Reactions to Cold
2/52
Physiological reactions to cold
Cutaneous changes depend upon:
Actual temperature achieved
Duration of chilling Rate of chilling
Rate of rewarming
-
8/6/2019 Reactions to Cold
3/52
Effect on vascular system
Constriction of arterioles and veins
Increase viscosity of blood
Changes in platelet adhesiveness Decrease conduction velocity in
cutaneous
nerves
-
8/6/2019 Reactions to Cold
4/52
Direct effect of cold : veins> arteries
Rewarming and local metabolites
Greater dilator effect on arteries
Resumption of arterial flow
Oedema
-
8/6/2019 Reactions to Cold
5/52
-
8/6/2019 Reactions to Cold
6/52
-
8/6/2019 Reactions to Cold
7/52
Physiological reactions to cold
Diseases of cold exposure
Frostbite
Trench foot
Diseases of abnormal sensitivity to cold
Perniosis
Acrocyanosis
Livedo reticularis Raynauds phenomenon
Cryoglobulinaemia
-
8/6/2019 Reactions to Cold
8/52
Diseases of cold exposure
Frost bite
Trench foot
-
8/6/2019 Reactions to Cold
9/52
Frost bite
Etiology
Acute freezing of tissues onexposure to extreme degrees
ofcold
Exposure of only a few seconds
duration may be sufficient tocause it
GREATER SEVERITY OF INJURY
Factors which increase rate ofloss ofheat ie contact with a
cold metal Wind chills
Prior cold injury
-
8/6/2019 Reactions to Cold
10/52
PATHOLOGY
Duration
Severity
Mild perivascular inflammatory change
Severe bulla formation & tissue necrosis
-
8/6/2019 Reactions to Cold
11/52
CLINICAL FEATURES
SITES
Toes, feet, fingers, ears, nose,
cheeks
Initial pain or feeling ofburning
Waxy and white affected skin
Muscles and nerves may bedamaged ; severe cases
arteries , bone and
subcutaneous tissue affected
-
8/6/2019 Reactions to Cold
12/52
Extent & severity of tissue damagebecomes apparent on
rewarming Mild : Erythema, mild pain,
soreness
Severe: Blistering and destruction ofepidermis, dermis and
deepertissues gangrene
Nerves & blood vessels persistentparaesthesia, abnormal
sensitivityto cold, compromised nutrition to
tissue Muscles, subcutaneous tissue or
even bone may be injured
-
8/6/2019 Reactions to Cold
13/52
TREATMENT
Rapid rewarming : Water at 40- 42 C for 20 mins
Early administration of Heparin and LMW dextran
Vasodilator and thrombolytic agents
Surgical removal of gangrenous tissue
-
8/6/2019 Reactions to Cold
14/52
Trench foot
FACTORS
Prolonged exposure to cold
Damp and windy conditions Prolonged immobility
Dependency of the limbs
Vascular disease and smoking
-
8/6/2019 Reactions to Cold
15/52
PATHOLOGY
Dependent oedema and stasis
Perivascular inflammation
Actual occlusion of vessels with ischaemic necrosis Both
myelinated and demyelinated nerve fibres
are damaged
-
8/6/2019 Reactions to Cold
16/52
CLINICAL FEATURES:
Cold anaesthetic limb
On rewarming Oedema
Hyperaemia
Painful paraesthesias
Cold sensitivity, vasomotorinstability, hyperhidrosis may
persist
-
8/6/2019 Reactions to Cold
17/52
TREATMENT
Analgesics
Antibiotics Bed rest
Adjuvant vasodilator therapy
-
8/6/2019 Reactions to Cold
18/52
Diseases of abnormal sensitivity to
cold
Perniosis/ chill blains
Acrocyanosis
Livedo reticularis
Raynauds phenomenon
Cryoglobulinaemia
Cold urticaria
-
8/6/2019 Reactions to Cold
19/52
Perniosis/ chill blains
Localized, usually tender,inflammatory, erythematous, oftenitchy
lesions which may blister orulcerate
ETIOLOGY
Genetic factors
Nutrition
Focal sepsis
Systemic diseases
Dysproteinemias
Myelodysplastic disease
Anorexia
-
8/6/2019 Reactions to Cold
20/52
PATHOLOGY
Idiopathic perniosis is primarily a disease of the
microvasculature
Persistent cold induced constriction of large
cutaneous arterioles
Persistent dilatation of the smaller, more
superficial vessels
-
8/6/2019 Reactions to Cold
21/52
HISTOPATHOLOGY
SUPERFICIAL/ ACRAL Epidermis: Necrotic keratinocytes ,
Spongiosis
Dermis : Intense oedema of papillary dermis
Marked perivascular mononuclear
cell infilterate of upper dermis
Fluffy oedema of blood vessel wall
DEEP/ THIGH:
Intense mononuclear infilterate throughout the dermis
and subcutaneous fat
Fluffy oedema of blood vessel wall
-
8/6/2019 Reactions to Cold
22/52
CLINICAL FEATURES ONSET
Early winters when humidity is
increased
Lesions are tender, pruritic, red orpurple lesions which may
blister or
ulcerate
Sites
Fingers, toes, heels, lower legs,thighs, nose, ears
Individual lesions usually run a self
limiting course over about 3 weeks
-
8/6/2019 Reactions to Cold
23/52
TREATMENT
Prophylactic wearing of warm clothing
Calcium channel inhibitors
Nicotinic acid derivatives
Minoxidil application topically
Phototherapy
-
8/6/2019 Reactions to Cold
24/52
Acrocyanosis
Persistent cyanotic orerythrocyanoticdiscoloration of skin
usuallywith a mottled pattern
Chiefly affects the hands
Peripheral arterioles are saidto react unduly to cold
Smaller vessels, especiallythose of the subpapillaryvenous
plexus, are dilated
No neuronal deficit seen
-
8/6/2019 Reactions to Cold
25/52
ETIOLOGY
1. Idiopathic
2.
Autoimmune Connective tissue disease
Antiphospholipid Ab syndrome
3. Neoplastic Paraproteinemias
Paraneoplastic syndrome
4. Cryoglobulinemia
5. Eating disorders Anorexia nervosa
Bulimia nervosa
6. Orthostatic disorders
7. Neurological disorders Brachial plexus neuropathy
8. Chronic arsenic poisoning
9. Drugs Butyl nitrate
INF alfa
10. Psychiatric Mental retardation
Schizophrenia
11. Essential thrombocythaemia
-
8/6/2019 Reactions to Cold
26/52
CLINICAL FEATURES
Often a familyhistory present ; genetic basis
Starts in adolescence and persists into adult life
Hands, face involved
Perniosis, erythrocyanosis, livedo reticularis may occur
simultaneously
DIAGNOSIS
Persistent cyanotic discoloration
Normal peripheral pulses
Absence of venous occlusion
TREATMENT
Vasodilators
Topical application: Nicotinic acid derivatives, minoxidil
-
8/6/2019 Reactions to Cold
27/52
Livedo reticularis
Mottled cyanoticdiscoloration of the skin witha characteristic
network
pattern which is accentuatedby cold
Dark area of the networkcorresponds to the area ofanastomosis
between 2cones, each supplied by anarteriole
-
8/6/2019 Reactions to Cold
28/52
CLINICAL FEATURES:
Mottled cyanotic discolorationoccurs commonly on legs,
arms,trunk
Tingling and numbness of skin onexposure to cold
Mottling taking the form ofcomplete network or
branchingconfiguration (LIVEDORACEMOSA)
Changes are initially reversible butafter a time vessels
becomepermanently dilated andtelangiectatic
-
8/6/2019 Reactions to Cold
29/52
CLASSIFICATION
1. Physiological
Cutis marmorata
2. Idiopathic/ Primary
Congenital
Cutis marmorata telangiectatica congenita
Acquired Uncomplicated
With winter ulceration
With summer ulceration
With systemic vascular involvement
3. Secondary Intravascular obstruction
Vessel wall disease
-
8/6/2019 Reactions to Cold
30/52
Intravascular obstruction Stasis
Paralysis Cardiac failure
Occlusive disease Emboli
Compressed air
NSAIDs, minocycline
Thrombocythaemia
Cryoglobulins
Vessel wall disease Arteriosclerosis
Arteritis : PAN, SLE, RA, Dermatomyositis, lymphoma,
pancreatitis
Infections TB, syphilis, hepatitis C, brucellosis, coxiella
Hyperparathyroidism and hypercalcemia
-
8/6/2019 Reactions to Cold
31/52
Treatment
Prophylactic
Cases with ulceration
Anticoagulants
Antithrombotic therapy
Prostacyclin
Treatment of underlying condition
-
8/6/2019 Reactions to Cold
32/52
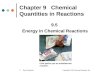
Raynauds phenomenon
Raynauds phenomenon isdescribed as episodic digital
ischemic vasospasm
triggered by cold oremotional stress leading to a
pale and cyanotic skin with a
postischemic phase of
hyperemia; the typical
tricolore phenomenon
-
8/6/2019 Reactions to Cold
33/52
Characterized by sequentialcolour changes
Pallor cyanosis rubor
Pallor is essential for diagnosis
Causes of Raynaudsphenomenon
Primary Raynauds Phenomenon(Raynauds disease)
Secondary Raynauds phenomenon
-
8/6/2019 Reactions to Cold
34/52
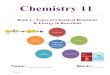
Imbalance of vasoconstriction and vasodilation in Raynauds
disease
-
8/6/2019 Reactions to Cold
35/52
Primary Raynauds Phenomenon
Primary Raynauds disease is common, with a
prevalence of 3% to 5% in the general population,
and remains uncomplicated without permanent
injury
Secondary Raynauds phenomenon
Occurs in patients with connective tissue disease,and might have
a more severe progression with
digital necrosis and ulceration leading to disability
-
8/6/2019 Reactions to Cold
36/52
-
8/6/2019 Reactions to Cold
37/52
Secondary Raynauds Phenomenon
Causes1. Trauma or vibration
2. Connective tissue diseaseand vasculitis
SS, SLE, RA, Sjogrenssyndrome,MCTD,Dermatomyositis
3. Obstructive arterialdisease
Arteriosclerosis
Buergers disease
4. Neurologicaldisease Thoracic outlet syndrome
Carpel tunnel syndrome
5. Haematological disease Cryoglobulinemia
Paroxysmal hemoglobinuria
Waldenstromsmacroglobulinaemia
6. Drugs and toxins Ergot
Imipramine
blockers
Bromocriptine
Heavy metals OCPs
Clonidine
Bleomycin
Cyclosporin
Amphetamines
7. Miscellaneous Paraneoplastic syndrome
CRF
Hypothyroidism
Anorexia nervosa
-
8/6/2019 Reactions to Cold
38/52
CRITERIA FOR THE DIAGNOSIS OF PRIMARY
RAYNAUDS PHE
NOME
NON1. Intermittent attacks of discoloration of extremeties
2. Absence of evidence of organic peripheral arterial
occlusion
3. Symmetrical or bilateral distribution4. Exclusion of any
disease, occupation, trauma or drug
ingestion
5. Absence of immunological abnormality
6. Female sex, age < 25 years
7. H/O cold intolerance since childhood
8. Normal nail fold capillaries
-
8/6/2019 Reactions to Cold
39/52
Secondary Raynaud's Syndrome
Periodic vasospastic attacks of pallor and
cyanosis Abnormal nailfold capillary pattern
Positive antinuclear antibody test
Abnormal erythrocyte sedimentation rate Presence of pitting
scars or ulcers of the skin,
or gangrene in the fingers or toes
-
8/6/2019 Reactions to Cold
40/52
CLINICAL FEATURES:
Typical attack: Sudden pallor of1 or more digits cyanosis and
erythema
Precipitated by cold, pressure or psychological stimuli
Raynauds disease:
F:M = 5:1
Age of onset < 40 years
Condition is usually symmetrical and affects several digits
Severe cases:
Telangiectasia of the nail fold Thinning and ridging of the
nail
Atrophy or sclerosis of fingers (sclerodactyly)
Gangrene rarely
-
8/6/2019 Reactions to Cold
41/52
TREATMENT
-
8/6/2019 Reactions to Cold
42/52
Cryoglobulinaemia
Cryoglobulins are globulins precipitated from
plasma/ serum on cooling
Cryoglobulinemia is characterized by thepresence of
cryoglobulins in the serum.
This may result in a clinical syndrome of systemic
inflammation (most commonly affecting thekidneys and skin)
caused by cryoglobulin-
containing immune complexes.
-
8/6/2019 Reactions to Cold
43/52
Causes1. Infections
Glandular fever
Hepatitis B/ C Syphilis
Borreliosis
SABE
Leprosy
Kala azar
HIV
2. Autoimmune diseases SLE
RA
Sjogrens syndrome
Vasculitis
3. Lymphoproliferative disease Myeloma
Lymphoma
4. Liver disease
5. Sarcoidosis
-
8/6/2019 Reactions to Cold
44/52
Clinical features:
Intravascular precipitation of cryoglobulins occur
Purpura on exposed parts after cooling
Patchy livedo reticularis
Cold urticaria
Raynauds phenomenon
Atypical ulceration of legs Haemorrhages
Ischemic necrosis
Acrocyanosis
Nailfold capillary abnormalities
Treatment Anticoagulants
Corticosteroids
Plasmapharesis
-
8/6/2019 Reactions to Cold
45/52
Cold urticarias
Cold urticaria is a relatively uncommon
physical urticaria
There are two forms of cold urticaria, a rare
familial (hereditary) form and a more common
acquired form.
With both forms an urticarial rash develops
after being exposed to cold, cold water, and
cold objects.
-
8/6/2019 Reactions to Cold
46/52
Clinical features
The onset of rash after exposure to cold differsbetween the
acquired and hereditary forms.
In the acquiredform, symptoms become
obvious in 2-5 minutes after exposure and lastfor 1-2 hours.
In the hereditary form, symptoms may not
become obvious until 9 to 48hours afterexposure and may last for
up to 24-48hours
-
8/6/2019 Reactions to Cold
47/52
Signs and symptoms of cold urticaria include:
Itchy weals and angioedema that may belocalised (affecting
certain parts of thebody) or generalised (rash over the
wholebody).
In some cases systemic symptoms may
develop Shortness of breath, wheezing
Abdominal pain, gastrointestinalulcers
Rapid and irregular heartbeat
In very severe cases hypotension, shock,collapse and even death
may occur
-
8/6/2019 Reactions to Cold
48/52
How is the diagnosis made?
Ice-cube test
-
8/6/2019 Reactions to Cold
49/52
Treatment
Patients with cold urticaria should learn to protect
themselvesfrom a rapid drop in body temperature.
Any aquatic activities (e.
g.
swimming, surfing) should be doneunder supervision at all
times.
Regular doses of antihistamines have generally proven to
beineffective, but high doses may be helpful (e.g., four times
theusual dose).
Some related medications that have been found to be
usefulinclude cyproheptadine and doxepin
There have been reports of successful treatment withleucotriene
antagonists, ciclosporin , systemic corticosteroidsand oral
antibiotics
-
8/6/2019 Reactions to Cold
50/52
Departmental Studies
-
8/6/2019 Reactions to Cold
51/52
Role ofPentoxifylline in various Dermatoses
with special reference to Leg ulcersDr Shikha Sood -1994
Role ofPentoxifylline in treatment of chronic leg
ulcers of various etiologies was evaluated
Pentoxifylline in a dose of 400 mg tds was given to a
group of18 patients with chronic leg ulcers with
Raynauds phenomenon
88.
8% patients had moderate to markedimprovement after 6 weeks of
therapy in the form of
decrease in the frequency and duration of attacks ,
decrease in the associated dysaesthesia and with
faster healing of ulcers
-
8/6/2019 Reactions to Cold
52/52
Thank you