Embed Size (px)
Citation preview

British Journal oJ‘Plastic Surgery (1986) 39, 114-l 11 tQ 1986 The Trustees of British Association of Plastic Surgeons
Reanimation of lower lip reconstructed by flaps
C. P. SAWHNEY
Department of Plastic Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh
Summary-This paper describes a technique of reanimating the reconstructed lower lip. For this the complete masseter on both sides has been used in order to obviate the danger of damaging the motor nerve supply to the muscle. The technique has been suitably modified to use the remaining musculature of the lips (i.e. orbicularis and the levators of the angle and upper lip) to improve the overall efficiency of the remaining upper lip function.
Reconstruction following total loss of the lower lip, using distant flaps, leaves much to be desired with regard to the restoration of normal function to the lower lip and efficient functioning of the upper lip. There will usually be (a) constant drooling of saliva, (b) spillage of fluids during swallowing because of inability of the lips to form a seal, (c) drooping of the lower lip with exposure of the teeth due to lack of support to the reconstructed lip, (d) defective articulation due to the inability to control movements of the lower lip resulting in difficulty in pronouncing certain consonants and vowels (i.e. P, M, B, V, F, 0, U and Y), (e) accumulation of solids and liquids in the gingivolabial sulcus and the vesti- bule. In addition, the loss of continuity of the oral sphincter and the unopposed action of the levators affect the efficiency of the upper lip.
Attempts to overcome these defects and restore a semblance of function to the lower lip have only
partly solved the problem. They include the provi- sion of static support to the lower lip using naso- labial flaps (Parson and Thering, 1972), fascia lata slings (Arem, 1975) and reanimating it through a fascia lata sling powered by the anterior half of the masseter (Sawhney, 1977) or temporalis (Perko, 1965). De Castro Correia and Zani (1973) showed on the basis of anatomical dissections that splitting the masseter may damage the nerve supply to its anterior half and we have therefore modified our technique to use the entire masseter to reanimate the lower lip. We have used this modified technique in four patients.
Operative technique
Through a submandibular approach the masseter is elevated subperiosteally from the mandibular ramus, starting from the lower border and extend-
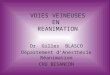
r7LE”AToR ANGULl ORIS
ZVGOMATICUS MAJOR
LEVATOR ANGULI ORlS
MASSETER
ZVGOMATICUS MAJOR
MASSETER
FASCIA LATA STRIP
ORBICULARIS ORIS
FASCIA LATA STRIP
Fig. 1
Figure I-_(A and B) The technique of using masseter muscle as a motor for reanimating the lower lip reconstructed by distant flaps.
114

REANIMATION OF LOWER LIP RECONSTRUCTED BY FLAPS 115
Fig. 2
Figure 2-_(A and B) Front and side view of a patient with total loss of lower lip. (C) Drooping lower lip reconstructed by distant Raps. (D. E and F) Opening and closing of the mouth after reanimation of the lower lip.
ing as far up as possible but stopping below the blunt and sharp dissection a pocket is created in the mandibular notch. An oblique incision is then subcutaneous tissue of the cheek extending as far made parallel to the nasolabial furrow, 1 cm from back as the masseter. It is made sufficiently wide to the angle of the mouth, and by a combination of accommodate the masseter without distortion

116 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 3
Figure 3%-(A) A patient with loss of lower lip, upper lip and adjacent cheek. (B and C) Drooping of the lower lip with exposure of the teeth after reconstruction. using distant flaps. (D, E and F) Function of the lower lip after reanimation.
when it is rerouted to traverse a straight downward Next, a tendon graft from the long extensor of and forward course towards the angle of the the second toe or a 1 cm wide fascia lata strip is tun- mouth. A similar procedure is carried out on the nelled through the reconstructed lower lip from other side. one end to the other and brought out through the

REANIMATION OF LOWER LIP RECONSTRUCTED BY FLAPS 117
obhque incisions near the angle. The tendon or the of the broad sheet of masseter, which is now obli- fascia lata graft traverses the lower lip in the subcu- que across the cheek, is advantageous because it re- taneous plane and 1 cm below the free border. The produces some of the action of the buccinator and graft is first anchored to the anterior fibres of the thereby prevents accumulation of food particles in masseter on the one side and then it is pulled tight the vestibule and also helps in swallowing. The nor- from the other side so as to raise the lower lip to its mal tone of the masseter supports the recon- proper position in apposition to the upper lip structed lower lip at rest and prevents its drooping before it is anchored to the masseter on the other and consequent exposure of the lower teeth. This side. The hbres of the zygomaticus major, levator also stops constant drooling of saliva. The ability anguli oris and orbicularis oris lying free in the to raise the lower lip voluntarily and press it tightly upper lip and in the cheek are then dissected free against the upper lip by upward and backward and pulled downwards as a bundle to be securely movement of the masseter helps in swallowing and anchored to the masseter and the graft close to the articulation. The advancement of the fibres of the angle (Fig. I). The posterior part of the masseter is orbicularis oris from the upper lip, the zygomaticus left undisturbed and this becomes adherent to the major and levator anguli superior from the adjoin- ramus in its new position. The skin wounds are ing cheek and their fixation to the masseter and the closed and a moderate pressure dressing is applied. tendon or fascial graft restores continuity of the The dressing is maintained for 3 weeks followed by oral sphincter and the function of the upper lip. graduated exercises to train the patient and restore The combined effect is to restore oral function to a function. All four patients have had good results great extent and bring back the confidence of the and are very pleased. Two illustrative cases are patient who can now look forward to a useful role shown in Figs 2 and 3. in society.
Discussion References
The lower lip is an important aesthetic and func- tional unit of the face and when completely lost produces a devastating functional and cosmetic disability. In addition, the function of the upper lip is secondarily affected because of the disruption of the continuity of the oral sphincter. Reconstruction of the whole of the lower lip with or without the adjoining cheek by distant flaps can be done satis- factorily but it is difficult to restore full function which combines a number of complicated move- ments. The use of the entire masseter to reanimate the lower lip in the manner described obviates any risk of injury to its motor nerve. The masseter is a powerful muscle and consequently only a few of its anterior fibres are used to reanimate the lower lip. The posterior part of the muscle becomes re- anchored to the ramus and its fibres can consis- tently be felt as a contracting bundle when the teeth are clenched. No patients have complained of any weakness of jaw closing. The change in the course
Arem, A. J. (1975). Fascia lata sling to correct oral incompe- tence. British Journal ofPlastic Surgqv, 28. 103.
de Castro Correia, P. and Zani, R. (1973). Masseter muscle rotation in the treatment of inferior facial paralysis, Anatomi- cal and clinical observations. Plasric and Reconstructive Sur- gery, 52, 370.
Parson, R. W. and Thering, H. R. (1972). An approach to recon- struction of complex lower face injuries. Brirish Juurnd q/ Plastic Surgery, 25. 23.
Perko, M. (1965). An interesting case of lower lip reconstruc- tion. Briiish Journal qf‘Plastic Surgery, 18,285.
Sawhney. C. P. (1977). Restoration of function to the lower lip reconstructed by flaps. Ptmfic und Rwonstruc~ive Surgery. 60. 17.
The Author
Chander P. Sawhney, MS, FAMS, Professor and Head of De- partment of Plastic Surgery, Postgraduate Institute of Medi- cal Education and Research, Chandigarh. India.
Requests for reprints to: Dr C. P. Sawhney. House No. 1030, Sector 249, Chandigarh 160023. India.