Embed Size (px)
Citation preview
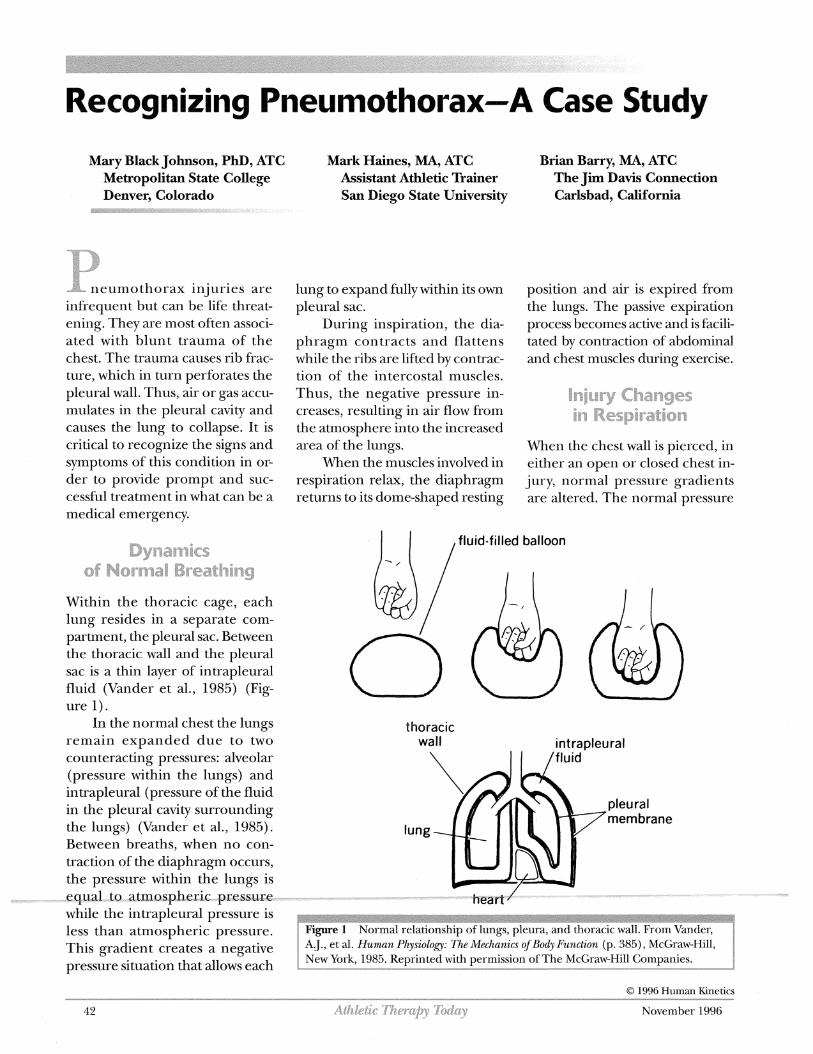
Recognizing Pneumothorax-A Case Study
Mary Black Johnson, PhD, ATC Mark Haines, MA, ATC Brian Barry, MA, ATC Metropolitan State College Assistant Athletic Trainer The Jim Davis Connection Denver, Colorado San Diego State University Carlsbad, California
9%- neumothorax injuries are infrequent but can be life threat- ening. They are most often associ- ated with blunt trauma of the chest. The trauma causes rib frac- ture, which in turn perforates the pleural wall. Thus, air or gas accu- mulates in the pleural cavity and causes the lung to collapse. It is critical to recognize the signs and symptoms of this condition in or- der to provide prompt and suc- cessful treatment in what can be a medical emergency.
Dynamics of Normal Breathing
Within the thoracic cage, each lung resides in a separate com- partment, the pleural sac. Between the thoracic wall and the pleural sac is a thin layer of intrapleural fluid (Vander et al., 1985) (Fig-
lung to expand fully within its own pleural sac.
During inspiration, the dia- phragm contracts and flattens while the ribs are lifted by contrac- tion of the intercostal muscles. Thus, the negative pressure in- creases, resulting in air flow from the atmosphere into the increased area of the lungs.
When the muscles involved in respiration relax, the diaphragm returns to its dome-shaped resting
position and air is expired from the lungs. The passive expiration process becomes active and is facili- tated by contraction of abdominal and chest muscles during exercise.
9njuw Changes in Respiration
When the chest wall is pierced, in either an open or closed chest in- jury, normal pressure gradients are altered. The normal pressure
, 1 , fluid-filled balloon
ure 1). In the normal chest the lungs thoracic
remain expanded due to two wall intrapleural counteracting pressures: alveolar (pressure within the lungs) and intrapleural (pressure of the fluid in the pleural cavity surrounding the lungs) (Vander et al., 1985). Between breaths, when no con- traction of the diaphragm occurs, the pressure within the lungs is
.-- ,, ,-,,"* e q d t ~ ~ a t m ~ s p h e ~ ~ i ~ - ~ - e s ~ ~ r e - ~ ~ - ~ ~ ~ ~ - while the intrapleural pressure is less than atmospheric pressure. This gradient creates a negative pressure situation that allows each
O 1996 Human Kinetics
42 AthZeEie DZWCCB Today November 1996
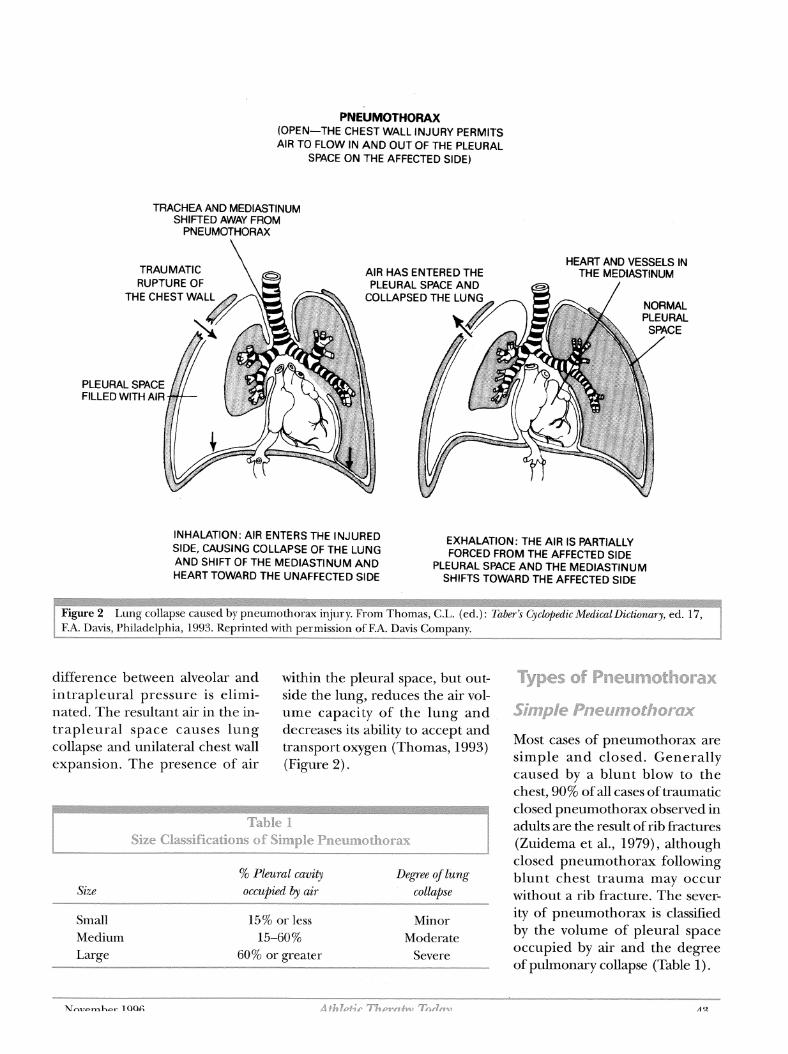
PNEUMOTHORAX (OPEN-THE CHEST WALL INJURY PERMITS AIR TO FLOW IN AND OUT OF THE PLEURAL
SPACE ON THE AFFECTED SIDE)
TRACHEA AND MEDIASTINUM SHIFTED AWAY FROM
PNEUMOTHORAX
TRAUMATIC AIR HAS ENTERE HEART AND VESSELS IN RUPTURE OF PLEURAL SPACE
THE CHEST WA COLLAPSED THE
PLEURAL SPACE FILLED WITH AIR
INHALATION: AIR ENTERS THE INJURED EXHALATION: THE AIR IS PARTIALLY SIDE, CAUSING COLLAPSE OF THE LUNG FORCED FROM THE AFFECTED SIDE AND SHIFT OF THE MEDIASTINUM AND PLEURAL SPACE AND THE MEDlASTlNUM HEART TOWARD THE UNAFFECTED SIDE SHIFTS TOWARD THE AFFECTED SIDE
difference between alveolar and within the pleural space, but out- intrapleural pressure is elimi- side the lung, reduces the air vol- nated. The resultant air in the in- ume capacity of the lung and trapleural space causes lung decreases its ability to accept and collapse and unilateral chest wall transport oxygen (Thomas, 1993) expansion. The presence of air (Figure 2).
Size % Pleural cavity Degree of lung occupied by air collapse
Small Medium Large
- -
15% or less Minor 15-60 % Moderate
60% or greater Severe
Types a$f P n e ~ m s t h o r a
Most cases of pneumothorax are simple and closed. Generally caused by a blunt blow to the chest, 90% of all cases of traumatic closed pneumothorax observed in adults are the result of rib fractures (Zuidema et al., 1979), although closed pneumothorax following blunt chest trauma may occur without a rib fracture. The sever- ity of pneumothorax is classified by the volume of pleural space occupied by air and the degree of pulmonary collapse (Table I).

The increase in intrapleural pressure can cause a mediastinal shift toward the uninvolved side of the chest, adversely affecting car- diac output. The hypovolemic condition created by the decrease in cardiac output results in periph- eral hypoxia and metabolic acido- sis. Ifthese conditions persist for any length of time, they can be fatal.
,r the prl i fluid. T ;pita1 for nt.
e hospital a CT scan was perrormed, confir 111111~ LIIC ICL
of pleur; ,f both t
3 pain in ysical sig
chest as on the fi
well as d eld inch
in breat nt tende < . .*
3ver the horax iq
d fractu suspecti
11-.
re sites c :d.
l ne i minatio~ ax, physi . .
pecting : s. The X
Occasionally pneumothorax oc- curs without an associated injury. This spontaneous accumulation of gas within the pleural space with- out a portal of entry through the chest wall (Simoneaux et al., 1990) is most common in young people between the ages of 15 and 30 and is reported more often in men than in women (Booher & Thibodeau, 1994).
Spontaneous pneumothorax is often associated with pulmo- nary disease (asthma, emphy- sema, chronic bronchitis) that results in rupture of the alveoli in the lungs (Griffith, 1986). How- ever, it has also been associated with heavy exertion in healthy in- dividuals. Diving, scuba diving, high altitude flying, or other ac- tivities that unduly stretch the chest and rib cage (e.g., track and field or throwing sports) can all cause spontaneous pneumothorax.
ponent c ) the hoa
esence o further
f pleural ion com ushed tc
horax w ithout el qealed fr . .
vidence 1 a1 effusic he 8th a1
>n (Figu nd 9th ri actures (
he anter Trea
he area 1
lor-lateral thorar tment in of the pi
- -
:ural dra Linage h lung re- 3mplete
[he tube's inserti :urred w Whe
.eaccumi
ithin 8 h n the ch ulation c
ours of 1
lest tube >f pneur
was a was rerr loved at K of moc ie left
,- nothora:
-- side. A tu t
[be was r The ch
loved wi
e-insertr est tube th no fu
h d , allow remaine rther prc
ing immediate re-expansion of hd in place for 75 oblems and the :
It was vas re-
! hours. athlete v
he lung. hen rerr
ost-injur :ventfull lgress w;
eased frt Reh:
lospital
3m the l- ibilitatio release. '
lospital : n procet The athl
1 week p :ded unt jete's prc
eeks foll owing ored by .. .-- ---"
physi- 3s monit clans and athletic trainin tions and X-rays. His sol! tenderness over the fract
cly foll01 ing this swelling
g staff M e compl ure sites
iith wee1 aint dur . Minor r
~mina- was of lent at
N-Up CXd
period was pres
post-injury showed heal11 tne atn ana ym lerr nus. The athlete was cleared fc
,he injur X-ra
7 n .
y site. ys taken
T n . 1 1
ng fract~ ,r full acl
3 weeks r. . L - 1
Ires of tivi ty 4
: Therea t further
fter he e injury t~
mployec o the rib
X protect 1s (Figurt
ive padd e 4).
Hemothorax, a condition in which In simple pneumothorax, affect the cardiorespiratory SYS- blood but no air is present in the
-"--- lung-capacitymay-notbe_signifl---*- t e m , . I n c r e a s i n g - i n t r a p I e u r a l - p r e ~ - ~ ~ ~ 1 ~ ~ 1 ~ - - s f ~ ~ ~ ~ ~ ~ ~ -* -* --- cantly altered. However, for cases sure can compress the vena cavae, with blunt chest trauma. The in& in which pneumothorax is sig- interfering with diastolic filling of dence of hemothorax in patients nificant or complications arise, the heart. This will decrease car- with nonpenetrating ,-hest wounds changes in normal respiration can diac output. varies between 25 and 75% (Kirsh
44 November 1996
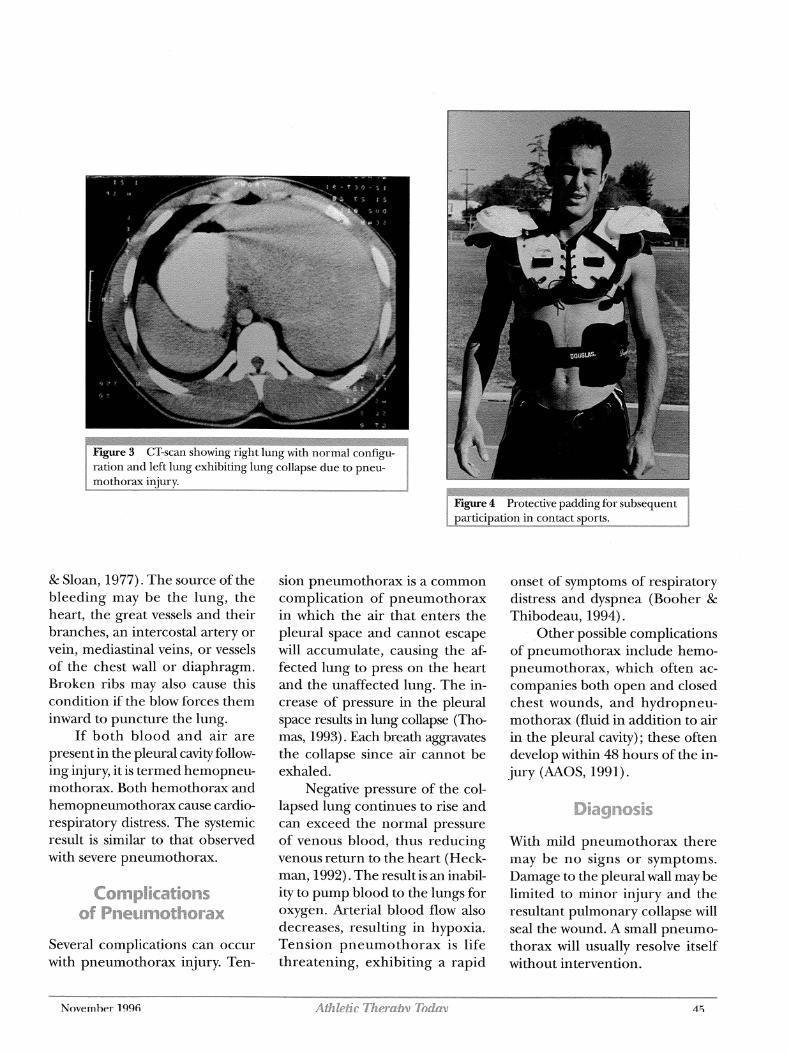
ation and left lung exhibiting lung collapse due to pneu- othorax iniurv.
& Sloan, 19'73). The source of the bleeding may be the lung, the heart, the great vessels and their branches, an intercostal artery or vein, mediastinal veins, or vessels of the chest wall or diaphragm. Broken ribs may also cause this condition if the blow forces them inward to puncture the lung.
If both blood and air are present in the pleural cavity follow- ing injury, it is termed hemopneu- mothorax. Both hemothorax and hemopneumothorax cause cardio- respiratory distress. The systemic result is similar to that observed with severe pneumothorax.
Several complications can occur with pneumothorax injury. Ten-
November 1996
sion pneumothorax is a common complication of pneumothorax in which the air that enters the pleural space and cannot escape will accumulate, causing the af- fected lung to press on the heart and the unaffected lung. The in- crease of pressure in the pleural space results in lung collapse (Tho- mas, 1993). Each breath aggravates the collapse since air cannot be exhaled.
Negative pressure of the col- lapsed lung continues to rise and can exceed the normal pressure of venous blood, thus reducing venous return to the heart (Heck- man, 1992). The result is an inabil- ity to pump blood to the lungs for oxygen. Arterial blood flow also decreases, resulting in hypoxia. Tension pneumothorax is life threatening, exhibiting a rapid
onset of symptoms of respiratory distress and dyspnea (Booher & Thibodeau, 1994).
,Other possible complications of pneumothorax include hemo- pneumothorax, which often ac- companies both open and closed chest wounds, and hydropneu- mothorax (fluid in addition to air in the pleural cavity) ; these often develop within 48 hours of the in- jury (AAOS, 1991).
Diagnosis
With mild pneumothorax there may be no signs or symptoms. Damage to the pleural wall may be limited to minor injury and the resultant pulmonary collapse will seal the wound. A small pneumo- thorax will usually resolve itself without intervention.

Only in moderate and severe pneumothorax injury will symp- toms usually present, the most common ones being marked chest pain and shortness of breath. These symptoms are seen in about half of all cases (Kirsh & Sloan, 1977).
The chest pain may extend to a shoulder or across the chest and abdomen, and breathing may be rapid and shallow. The athlete may have a dry, hacking cough, occa- sionally coughing blood. These symptoms usually appear soon after injury.
If the pneumothorax has a tension component, respiratory distress progresses rapidly. The pulse is weak and rapid and blood pressure decreases rapidly. In moderate and severe cases, there is a mediastinal and tracheal shift to the uninjured side and a bulg- ing of the tissues of the chest wall between the ribs and above the clavicle (Vinger & Hoerner, 1986). There is visible distention of the neck veins and cyanosis.
Physical examination reveals tympanitic hyperresonance to per- cussion. Distant or absent breath sounds occur on the involved side. These sounds may be difficult to interpret since the patient cannot breathe normally.
The definitive diagnosis of pneumothorax is made from the physical findings and chest X-rays, which will show a separation of the two layers of pleura by an accumu- lation of air (or fluid in the case of hemothorax or hemopneu- mothorax) in the pleural cavity. A small pneumothorax may be dif-
-.--fi~ult-to-dete~h&-&ay- --
Immediate attention to suspected pneumothorax injuries involves making the athlete comfortable and monitoring vital signs: pulse, blood pressure, and respiration. The athlete will usually breathe more easily if he or she lays on the affected side, as this may seal the pleural perforation.
Emergency treatment of the athlete with pneumothorax re- quires immediate administration of oxygen and transport to a hos- pital. Moderate and severe trau- matic pneumothorax will be drained by intercostal intubation (tube thoracostomy) (Hughes, 1983). Some advocate needle as- piration and/or observation of "minor" pneumothorax, particu- larly spontaneous pneumothorax. If the condition is caused by trauma, however, Zuidema et al. state, 'This so-called conservative approach is associated with a much lower success rate than when used for spontaneous pneu- mothorax" (1979, pp. 394395).
American Academy of Orthopedic Surgeons. (1991). Athletic training and sports medicine (2nd ed.). Park Ridge, IL: AAOS.
Booher, J.M., & Thibodeau G.A. (1994). Ath- letic injury assessmat (3rd ed.). St. Louis: Mosby.
Griffith, H.W. (1986). Complete guide to sports injuries. New York: Putnam Publ.
Heckman, J.D. (Ed.) (1992). Emergency careand transportation of the sick and injured (4th ed). Park Ridge, IL: American Academy of Orthopaedic Surgeons.
Hughes, S. (1983). The basis and practice oftrau- matology. London: William Heinemann Medical Books Ltd.
Kirsh, M.M., & Sloan, H. (1977). Blunt chest trauma-Generalpinciples of management. Boston: Little, Brown & Co.
Simoneaux, F., Murphy, B.J., & Tehranzadeh, J. (1990). Spontaneous pneumothorax in a weightlifter: A case report. American Journal of Sports Medicine, 18,647-648.
Thomas, C.L. (Ed.) (1993). Tuber's cyclopedic medical dictionary (17th ed.) . Philadel- phia: F.A. Davis.
Vander, A.J., Sherman, J.H., & Luciano, D.S. (1985). Human physiology: The mechanics of body function (4th ed.). New York: McGraw-Hill.
Vinger, P.F., & Hoerner, E.F. (1986). Sports in- juries-The unthwarted epidemic (2nd ed.) . Littleton, MA: PSG Publ. Co.
Zuidema, G.D., Rutherford, R.B., & Ballinger, W.F. (1979). The managmnt of trauma (3rd ed.). Philadelphia: Saunders.
Pneumothorax can be life threat- ening. Trauma-induced pneu- mothorax may be overlooked in blunt trauma, such as that result- ing in rib fracture. Successful treat- ment includes close monitoring of symptoms and medical interven- tion. With careful and consistent monitoring, adequate recupera- tion time, rehabilitation, and proper postinjury protection, the patient can expect full recovery -fr~m-pn.eum~thu~~inj~ry.----~~~~-
Mary Black Johnson is a curriculum specialist in athletic training and an assistant professor in the Dept. of Human Performance, Sport and Leisure at Metropolitan State College in Den- ver. She was formerly an assistant professor of athletic training at San Diego State University.
Mark Haines is the assistant athletic trainer at San Diego State University. His primary respon- sibilities are with the football and men's bas- ketball programs. He has a master's in exercise physiology from Michigan State University.
Brian Barry is president of The Jim Davis Connection, a research and education facility that designs rehab and therapeutic exercise equipment. He has a master's in cellular and exercise physiology from Central Michigan University:--- --- - y - * - - * "*
46 Aflz le~c mc~.@ji Todo)] November 1996












![CASE REPORT Open Access Tension pneumothorax … proven in a retrospective study with diaphragmatic ... presentation of a tension pneumothorax [3,7]. In this case the tension pneumothorax](https://img.pdfslide.net/doc/110x75/5ae6a4b67f8b9ae1578df685/case-report-open-access-tension-pneumothorax-proven-in-a-retrospective-study.jpg)