Embed Size (px)
Citation preview

RED BLOOD CELL DESTRUCTION


A, 1,3,5,8

ALA, protoporphinogen, mito
Oroporphinogen, coproporphinogen
cytoplasm׀׀׀
Mitochanemia

-4CO2
copropotphinogen
׀׀׀
׀
vinyl
copropophynogenase
Protoporphynogen
׀׀׀
Color,purfirine
,4M(1,3,5,8),v
)2,4,(2p(6,7)
Non-color
mitot
Protoporphyn
-only- ׀׀׀Copro
oxidase
Oxidase, decarboxylase

Protoporphyn ׀׀׀
hemeferrochel
atase
Fe
Pb inhibits ferrochelatase, ALA dehydratase


yellow

porphinogen
Bili diglucoReduction, intestine
orobillinogen
intestine orobillin
liver





Uncon,
therapy phenobar
bital,phototherapy

•Uncon-billi;
• hemolytic anemia
•Neonatal physilogical jaundice, most common•Crigler najjar syndrom (Phenobarbital has not effect)׀
•Billi more than 20mg/dl•Crigler najjar syndrom glucoronidase active׀ ׀
•Billi not more than 20mg/dl•Gilbert glucoronidase active 30%, harmless
•Toxic hyperbilli liver•Damage liver parenchym
•Con billi;
•Obstruction of billiary no excretion of con-billi appear in serum, urine•Dubin johnson no secretion Con billi to bile
•Rotor syndrom normal liver, abnormality in liver storage

Degradation of HaemglobinAfter approximately 120 days, red blood cells
aredegraded by reticuloendothelial (RE) system,
particularlyin the liver and spleen.
1 )First haemoglobin is dissociated into haem and globin.
2 )Globin is degraded to its constituent amino acids,whichare reused.
3 )The catabolism of haem is carried out in the
microsomal fraction of cells by a complex enzyme
system called haem oxygenase, in presence of NADPH,O2

Pathway for conversion of Hb to bilirubin
Red Blood CellsHaemoglobin
120 days dissociationGlobin Haem
O2, NADPH + H+Fe Haem Oxygenase
Amino Acids NADP+ , COBiliverdin
NADPH + H+Biliverdin reductase
Reutilized NADP+Bilirubin

Metabolism and excretion of bilirubin occurs in the liver
and intestine. It can be divided into four processes-:
1 -Uptake of bilirubin by liver parenchymal cells.
2 -Conjugation of bilirubin in the smooth endoplasmic
reticulum in liver. 3 -Secretion of conjugated bilirubin into the
bile. 4 -Excretion of bilirubin in the form of
urobilinogenthrough faeces and urine.

1 -Uptake of bilirubin by liver parenchymal cells
a- Bilirubin formed in peripheral tissues is transported to
the liver by binding to plasma albumin. b- In the liver bilirubin is removed from
albumin and takenup by hepatocyte where it binds to
intracellular proteinscalled ligandin.
2 -Conjugation of Bilirubina- Hepatocytes convert soluble bilirubin to a
more solubleform by conjugation of two molecules of
glucuronic acid.-This reaction is catalyzed by bilirubin
glucuronyltransferase using UDP-glucuronate as a
source ofglucuronic acid.

b- Bilirubin monoglucuronide is an intermediate and is converted
to the bilirubin diglucuronide as shown in figure (2).Bilirubin
Bilirubin glucuronyl UDP-Glucuronatetransferees
UDPBilirubin monoglucuronide
UDP-GlucuronateBilirubin glucuronyl
transferase UDPBilirubin diglucuronide
Figure(2):- Conjugation of bilirubin with glucuronic acid in the liver.

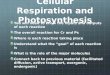
Overview of heme degradation. Heme is degraded to bilirubin, carried in the blood by
albumin, conjugated to form the diglucuronide in the liver, and excreted in the
bile. Theiron is returned to the body’s iron stores. RES
= reticuloendothelial system: RBC = redblood cells.

3 -Secreation of Bilirubin into Bile-:Most of the bilirubin secreted in the bile is in
the form ofbilirubin diglucuronide (conjugated form of
bilirubin),Unconjugated bilirubin is not secreted into
bile. 4 -Excretion of Bilirubin in the form of
Urobilinogen throughFaeces and Urine-:
a- After secretion into bile, the conjugated bilirubin passes
through the hepatic and common bile ducts into the
intestinal lumen. b- Bilirubin diglucuronide is hydrolyzed in the
intestine bybacterial enzymes β-glucuronidase and the
bilirubinportion is reduced by the faecal flora to
colourlessurobilinogens and excreted through faeces.

GlobinReticuloendothelial Hb HaemSystemFe+3Bilirubin
(1 )UptakeBlood Bilirubin-albumin Urobilinogen Kidney
(2 )ConjugationUrobilin UrinebilirubinLiver 2UDP-Glucuronate Conjugation ExcretedBilirubin-diglucuronideBile (3) Secretion EnterohepaticBilirubin-diglucuronide Urobilinogen cycle
(4 )ExcretionBilirubin-diglucuronideIntestine Glucuronide GlucuronidaseUrobilinogenFaeces UrobilinogenUrobilinExcretedFigure ( ):- Schematic representation of

The normal concentration of serum bilirubin is-:
Total bilirubin = 0.1-1.0 mg/dl. Conjugated bilirubin = 0.1-0.4 mg/dl.
Unconjugated bilirubin = 0.2-0.7 mg/dl. Hyperbilirubinemia exists when bilirubin in
the bloodexceeds 1mg/dl.
Hyperbilirubinemia may be due to-:1 .Increased bilirubin production.
2 .Decreased hepatic uptake.3 .Decreased hepatic conjugation
4 .Decreased excretion of bilirubin into bile

In all these situations bilirubin accumulates in the bloodand when it reaches a certain concentration (2.2 - 5mg/dl), it diffuses into the tissues. The skin and thesclera appear yellowish due to the deposition ofbilirubin in the tissues. The condition is calledJaundice.Jaundice can be divided into four types-:
1 .Haemolytic anemia un-billi or prehepatic jaundice.
2 .Hepatocellular or intrahepatic jaundice.3 .Obstructive or posthepatic jaundice.
4 .Neonatal or physiological jaundice.Hyperbiliubinemia may be acquired or inherited

cquried hyperbilirubinemia-:1 .Haemolytic Jaundice.
2 .Hepatic Jaundice.3 .Obstructive Jaundice.
4 .Neonatal Jaundice.1 .Haemolytic Jaundice-:
In haemolytic jaundice, there is an increased inbreakdown of haemoglobin to bilirubin at a rate inexcess of the ability of the liver cell to conjugate andexcrete it.
Excess haemolysis may be due to-:a- Sickle haemoglobin.b- Deficiency of G-6-P dehydrogenase.c- Incompatible blood transfusion.

The main biochemical features of the haemolytic jaundice are:
1 -Inreased plasma concentration of unconjugated bilirubin.
2 -Increased amount of urobilinogen in urine and faeces.
3 -Absence of bilirubin in the urine.2 -Hepatic jaundice-:
In hepatic jaundice, there is some disorder of the liver cells
or the bile passages within the liver. The hepatic parenchymal cell damage impairs conjugation ofbilirubin and results in unconjugated hyperbilirubinemia.
Hepatocellular damage is caused by-: a- Infections ( Viral Hepatitis).b-Toxic chemicals ( Alcohol,Chloroform,CCl4).c- Drugs.d- Cirrhosis.

Patients with hepatic jaundice have obstruction of thebiliary tree within the liver that results in the presence ofsome conjugated hyperbilirubinemia.
The main biochemical features of the hepatic jaundice-:
1 -Increased plasma concentration of conjugated andunconjugated bilirubin.
2 -Decreased amount of urobilinogen in urine andfaeces
3 -Presence of bilirubin in the urine.4 -Increased level of alanine transaminase
(hepatic celldamageallows intracellular enzymes to leak
into theblood.)

3 -Obstructive Jaundice-: This occurs when there is an obstruction in
thepassage of conjugated bilirubin from the liver cells tothe intestine.
This condition is also called Cholestasis, (theobstruction of biliary flow.)
The obstruction may be intrahepatic or extrahepatic.
Extrahepatic cholestasis occurs due to-: 1 -Blockage of the common bile duct by
gallstones.2 -Carcinoma of the head of the pancrease.
3 -Carcinoma of the bile duct.

The liver is deficient in UDP-glucuronyl transferasewhich is necessary for conjugation.
The enzyme deficiency is more serious with increasingdegree of prematurity.
The increased in unconjugated bilirubin above 20-
25mg/dl can cause mental retardation