Embed Size (px)
Citation preview

REDUCING CENTRAL LINE BLOODSTREAM INFECTIONS
Going beyond the checklist
Richard T. Ellison III, MDJune 2009

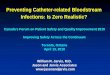
UMMMC Intensive Care Unit Central Line-Bloodstream Infections
FY 2003 to FY 2009
98
87
60 58
46
25
11
0
1
2
3
4
5
6
7
8
9
10
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Rat
e pe
r 1,0
00 C
L D
ays
0
20
40
60
80
100
120
Num
ber o
f CL-
BSI
Rate CL-BSI/1000 CL days No. CL-BSI

Improvement Strategy FY 2004 – Creation of Critical
Care Operations Committee FY 2005 – Creation of
Centerwide CL-BSI taskforce created: Use of a checklist, central line
cart, full barrier precautions, and physician and staff education was implemented.
FY2006 - use of Chlorhexidine impregnated dressings on all central lines
FY2006 - monthly report on CL-BSI rates in each ICU to full CCOC
FY2006 – educational presentations and discussions with front line staff in each ICU on CL-BSI in rotation with other CCOC quality initiatives
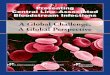
UMMMC Intensive Care Unit Central Line-Bloodstream Infections
FY 2003 to FY 2009
98
87
60 58
46
25
11
0
2
4
6
8
10
FY03 FY04 FY05 FY06 FY07 FY08 FY09R
ate
per
1,0
00 C
L D
ays
0
20
40
60
80
100
120
Nu
mb
er o
f CL
-BS
I
Rate CL-BSI/1000 CL days No. CL-BSI

Improvement Strategy FY 2007 - on line education
of all ICU physicians and staff on presenting central line infections
FY2007 – routine use of antimicrobial impregnated central line catheters begun for catheters placed in ICU
FY2007 – “High risk” lines identified through ICU electronic medical record with notification of ICU directors (those placed in emergency department and at femoral site)
UMMMC Intensive Care Unit Central Line-Bloodstream Infections
FY 2003 to FY 2009
98
87
60 58
46
25
11
0
2
4
6
8
10
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Ra
te p
er 1
,000
CL
Da
ys
0
20
40
60
80
100
120
Nu
mb
er o
f CL
-BS
I
Rate CL-BSI/1000 CL days No. CL-BSI

Improvement Strategy FY2008 - a reduction in CL-BSI rates in
the ICUs became a hospital goal with financial implications for hospital senior administration as well as CCOC director and ICU directors
FY2008 – education on proper blood culture collection technique provided to all ICU staff
FY2008 – each CL-BSI treated as a “critical” event with a follow up review meeting held with ICU unit director, ICU nurse manager, infection control department staff, and CCOC leadership
FY2008 – an atlas of dressing options for central line catheters placed at internal jugular site was created for situations where individual patient’s anatomy made it difficult to maintain an intact dressing
FY2009 – the rate of contaminated blood cultures collected in individual ICUs is reported back to individual ICUs
UMMMC Intensive Care Unit Central Line-Bloodstream Infections
FY 2003 to FY 2009
98
87
60 58
46
25
11
0
2
4
6
8
10
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Ra
te p
er 1
,000
CL
Da
ys
0
20
40
60
80
100
120
Nu
mb
er o
f CL
-BS
I
Rate CL-BSI/1000 CL days No. CL-BSI

SUMMARY A sustained reduction in CL-BSIs achieved
across 7 ICUs has been achieved with over 80% reduction from baseline
Key factors to improvement have included: A commitment by Senior management to change
approach to ICU care Ongoing feedback Interactive staff education
Best practices from one unit shared with all others
Adoption of new technologies Ongoing review of factors that contribute to each
CL-BSI