Embed Size (px)
Citation preview

Reducing Mortality and Infections After CongenitalHeart Surgery in the Developing World
abstractBACKGROUND: There is little information about congenital heart surgeryoutcomes in developing countries. The International Quality Improve-ment Collaborative for Congenital Heart Surgery in Developing WorldCountries uses a registry and quality improvement strategies with non-governmental organization reinforcement to reduce mortality. Registrydata were used to evaluate impact.
METHODS: Twenty-eight sites in 17 developing world countries submittedcongenital heart surgery data to a registry, received annual benchmarkingreports, and created quality improvement teams. Webinars targeted 3key drivers: safe perioperative practice, infection reduction, and team-based practice. Registry data were audited annually; only verified datawere included in analyses. Risk-adjusted standardized mortality ratios(SMRs) and standardized infection ratios among participating siteswere calculated.
RESULTS: Twenty-seven sites had verified data in at least 1 year, and 1site withdrew. Among 15 049 cases of pediatric congenital heart surgery,unadjusted mortality was 6.3% and any major infection was 7.0%. SMRsfor the overall International Quality Improvement Collaborative forCongenital Heart Surgery in Developing World Countries were 0.71(95% confidence interval [CI] 0.62–0.81) in 2011 and 0.76 (95% CI0.69–0.83) in 2012, compared with 2010 baseline. SMRs among 7 sitesparticipating in all 3 years were 0.85 (95% CI 0.71–1.00) in 2011 and 0.80(95% CI 0.66–0.96) in 2012; among 14 sites participating in 2011 and2012, the SMR was 0.80 (95% CI 0.70–0.91) in 2012. Standardizedinfection ratios were similarly reduced.
CONCLUSIONS: Congenital heart surgery risk-adjusted mortality andinfections were reduced in developing world programs participatingin the collaborative quality improvement project and registry. Similarstrategies might allow rapid reduction in global health care disparities.Pediatrics 2014;134:e1422–e1430
AUTHORS: Kathy J. Jenkins, MD, MPH,a Aldo R. Castañeda,MD, PhD,b K.M. Cherian, MD,c Chris A. Couser, MHA,a EmilyK. Dale, MPH, CHES,d Kimberlee Gauvreau, ScD,a Patricia A.Hickey, PhD, MBA, RN, FAAN,a Jennifer Koch Kupiec, MPH,a
Debra Forbes Morrow, RN,a William M. Novick, MD,e,f
Shawn J. Rangel, MD, MSCE,a Bistra Zheleva, MBA,d andJan T. Christenson, MD, PhDg
aBoston Children’s Hospital, Boston, Massachusetts; bUnidad deCirugía Cardiovascular Pediátrica de Guatemala, Guatemala City,Guatemala; cFrontier Lifeline Hospital, Chennai, India; dChildren’sHeartLink, Minneapolis, Minnesota; eInternational Children’sHeart Foundation, Memphis, Tennessee; fUniversity of TennesseeHealth Sciences Center, Memphis, Tennessee; and gUniversityHospital Geneva, Geneva, Switzerland
KEY WORDScongenital heart surgery, mortality, hospital-acquired infection,quality improvement
ABBREVIATIONSCI—confidence intervalIQIC—International Quality Improvement Collaborative forCongenital Heart Surgery in Developing World CountriesNGO—nongovernmental organizationRACHS-1—Risk Adjustment for Congenital Heart SurgerySIR—standardized infection ratioSMR—standardized mortality ratio
Dr Jenkins conceptualized and designed this study, interpretedthe data, and drafted and critically revised the initial manuscript;Drs Castañeda, Cherian, Novick, and Christenson and BistraZheleva conceptualized and designed this study, and reviewed andcritically revised the manuscript; Chris A. Couser managed thestudy, oversaw data collection and acquisition at sites, anddrafted and critically revised the manuscript; Ms Dale supporteddata collection and acquisition at several sites, and reviewed andcritically revised the manuscript; Dr Gauvreau conducted allstatistical analyses, interpreted the data, contributed to the initialdraft, and critically revised the manuscript; Dr Hickeyconceptualized and designed this study, contributed to the initialdraft, and critically revised the manuscript; Ms Koch Kupieccontributed to data interpretation, and drafted and criticallyrevised the initial manuscript; Ms Morrow and Dr Rangelcontributed to study concept and design, contributed to the initialdraft, and critically revised the manuscript; and all authorsapproved the final manuscript as submitted. All authors agree tobe accountable for all aspects of the work in ensuring thatquestions related to the accuracy or integrity of any part of thework are appropriately investigated and resolved.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-0356
doi:10.1542/peds.2014-0356
Accepted for publication May 16, 2014
(Continued on last page)
e1422 JENKINS et al at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

Only 7% of the population has accessto life-saving congenital heart surgeryin the developing world,1 where con-genital anomalies are the eighth leadingcause of death in children.2 Approxi-mately 90% of births worldwide occurin developing countries that havelimited resources and high expectedmorbidity and mortality due to con-genital heart disease.3,4 The establish-ment of surgical programs allows anincreasing number of children accessto life-saving surgery. Congenital heartsurgery carries considerable risk fordeath, even in programs in the de-veloped world. Congenital heart sur-gery has the potential to offer repair orpalliation for children who would oth-erwise die, but requires a highly skilledmultidisciplinary team and a reliable in-stitutional framework. These factors areoften limited in resource-poor envi-ronments, where survival also may belimited by late identification of poornutrition and other morbidities.5 Trans-lation of quality improvement activi-ties, now common in developed worldsurgical programs, can catalyze rapidimprovement in surgical outcomes.
Onecornerstoneofquality improvementis the need tomonitor clinical outcomesand benchmark performance. A majorproblem faced by health care pro-fessionals in thedevelopingworld is thelack of benchmarking data for pur-poses of evaluating performance oftheir congenital heart surgery pro-grams and guiding efforts to makeimprovements. The Global Forum onHumanitarian Medicine in Cardiologyand Cardiac Surgery was establishedfor nongovernmental organizations(NGOs) to discuss opportunities to helpaddress challenges for cardiac surgeryprograms in the developing world. Theneed for improved data collection andclinical outcomes was identified dur-ing the Global Forum by developingcountry practitioners and NGOs sup-porting capacity-building in developing
world pediatric cardiac surgery pro-grams. To address these gaps andstrengthen health care systems, theInternational Quality Improvement Col-laborative for Congenital Heart Surgeryin Developing World Countries (IQIC) wasconceived in 2007 by Boston Children’sHospital representatives and NGOs atthe Global Forum in Geneva, Switzerland.The IQIC aims to (1) collect informationabout site-specific outcomes, includingin-hospital mortality, major infection,and 30-day mortality, after congenitalheart surgeries performed in the de-veloping world; (2) determine patientand procedural predictors of site-specificoutcomes; and (3) use quality improve-ment methodology and collaborationbetween programs in developed anddeveloping countries to reduce mortalityin the developing world. Initial sites hadattended Global Forum meetings or hadaffiliations with NGOs. Later, participationwas opened to other interested, similarprograms that were self-identified asperforming congenital heart surgery inresource-constrained environmentsbasedon the amount of gross domestic productavailable to health care. Between 2010 and2012, 28 sites in 17 countries participatedin the IQIC and submitted data (Table 1).
METHODS
Database Creation and DataCollection
A Web-based data entry tool was de-velopedwith thegoalofcollectingdatatoassess in-hospital and 30-day mortality,as well as surgical site infections andbacterial sepsis. Data elements col-lected include patient characteristics,preoperative status, and variablesnecessary to use the Risk Adjustmentfor Congenital Heart Surgery (RACHS-1)methodology.6,7 Physician-nurse teamsfrom each site oversee data collectionand project management, and sites sub-mit diagnostic, procedural, and clini-cal information for all congenital heartsurgeries in patients,18 years of age
into the Web-based entry tool. Sitesreport de-identified patient data only.The Boston Children’s Hospital insti-tutional review board approved thisproject. Participating sites obtainedlocal institutional review board or otherapprovals if necessary.
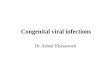
Development of Key Driver Diagram
Discussions at Global Forum meetingsoutlinedkeychallengesfacingdevelopingworld programs. Using this informa-tion, along with current quality improve-ment priorities in the developed world, 3“key drivers” to reduce mortality associ-ated with congenital heart surgery wereselected: safe perioperative practice, re-duction of surgical site infections andbacterial sepsis, and team-based prac-tice through nurse empowerment (Fig 1).
Learning Modules
The quality improvement component ofthe collaborative began in 2010, usinga targeted educational program to ad-dress each of the 3 key drivers. Sitesbegan participating inmonthly webinars,with training to develop targeted qualityimprovement strategies at their respec-tive institutions. The learning modulesinclude educational videos and Webcontent related to each key driver. In2011, additional curriculawithadvancednursing content were incorporated, andsite-led webinars were introduced in2012. A total of 44 webinars were con-ducted between 2010 and 2012, in whichparticipating sites were highly engaged.Webinars included topics on surgicalsafety checklist implementation, healthcare–associated infectionprevention, handhygiene, clear communication, effectiveteamwork, nursing postoperative care,postoperative respiratorymanagement,pain management, nutrition, emergencysituations, crisis resource management,surgical repairs of common congenitalheart defects, arrhythmias, fetal circula-tion and physiology, cardiac embryology,endotracheal tube suctioning, data entry,
QUALITY REPORT
PEDIATRICS Volume 134, Number 5, November 2014 e1423 at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

and annual benchmarking report in-terpretation. All webinars are archivedon the IQIC Web site for participants’future reference and are translatedfrom English locally by sites as needed.In addition, NGOs actively supportedadoption of key IQIC activities to facili-tate implementation. In June 2013, anin-person learning session reinforcingoutcomes and interventions was heldat the ninth Global Forum meeting inGeneva, Switzerland; 66 participants from23 sites attended.
Safe Perioperative Practice
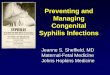
Using design principles outlined by theWorld Health Organization’s Safe Sur-gery Saves Lives campaign and a pre-viously published pediatric surgicalsafety checklist as a conceptual frame-work,8,9 a checklist designed specificallyto meet the needs of pediatric congen-ital heart surgery was created (Fig 2).The checklist was disseminated to allinstitutions, which were encouraged tomake any necessary modifications tomeet unique needs of their institutions.
Perioperative care team members atsites were trained on effective checklistutilization through interactive webinarsand one-on-one site mentoring.
Infection Reduction
Learning modules were developed tointroduce the concept of evidence-based “practice bundles” and teachspecific components of infection re-duction. A bundle is defined as a set ofevidence-based practices that improvepatient outcomes when implementedby every member of the health careteam.10 An initial module focused ondeveloping a hand hygiene programand included strategies to improvehand-washing compliance, recognizingthat health care workers’ hands areresponsible for the transmission ofmost pathogens in hospitals.11 Addi-tional modules focused on practicebundles to improve sterility for centralvenous catheter insertions, central lineaccess, and central line dressings; toreduce surgical site infections, empha-sizing correct antibiotic timing, hair re-moval with clippers, preoperative skindisinfection, and postoperative woundmanagement; and to reduce urinarytract infections and ventilator-associatedpneumonia. The importance of stan-dardizing care, auditing practice, andthe feedback of practice audit resultsand infection rateswere common themesacross modules.
Team-Based Practice Through NurseEmpowerment
To achieve the goal of team-basedpractice through nurse empowerment,numerous tools were provided for em-powering nurses, including high-fidelitycase-based teaching videos, standard-ized scripts for nurses to give compre-hensivepatientreports in ICUsandwards,aswell as techniques of assertion, closedloop communication, and a structuredsituation briefing framework with 4components: Situation, Background, As-sessment, and Recommendation. This
TABLE 1 Participating Sites and Locations
Name of Institution Location Included in Aggregate Data
2010 2011 2012
Amrita Institute of Medical Sciences Kochi, India Yes Yes YesArmed Forces Institute of Cardiology,National Institute of Heart Disease
Rawalpindi, Pakistan Yes No Yes
Care Hospital Hyderabad, India N/A N/A YesClinica Infantil Colsubsidio Bogota, Colombia Yes Yes YesFederal State Budgetary Institution“Research Institute for ComplexProblems of Cardiovascular Diseases,”Siberian Branch of the RussianAcademy of Medical Sciences
Kemerovo, Russia N/A N/A Yes
First Hospital of Lanzhou University Lanzhou, Gansu Province, China N/A Yes YesFrontier Lifeline Hospital Chennai, India Yes Yes YesFundacion Cardioinfantil de Bogota Bogota, Colombia N/A Yes YesFundacion Cardiovascular Adulto-Pediatrica Clinica San Rafael
Bogota, Colombia Yes Yes Yes
Hospital Arturo Grullon Santiago de los Caballeros,Dominican Republic
Yes No No
Hospital de Base Sao Jose do Rio Preto, Brazil Yes Yes YesHospital de Ninos Cordoba, Argentina N/A N/A YesHospital Garrahan Buenos Aires, Argentina N/A Yes YesHospital Nacional de Ninos BenjaminBloom
San Salvador, El Salvador N/A No No
Innova Children’s Heart Hospital Hyderabad, India Yes Yes YesInstitute of General and Urgent Surgery,Academy of Medical Sciences
Kharkov, Ukraine No Yes Yes
Instituto do Coracao (InCor) Sao Paulo, Brazil N/A N/A YesInstituto Nacional Cardiovascular (INCOR) Lima, Peru N/A N/A YesKardias A.C. (Instituto Nacional dePediatria & Centro Medico ABC)
Mexico City, Mexico N/A N/A Yes
KJ Hospital Chennai, India N/A Yes YesKokilaben Dhirubhai Ambani Hospital &Medical Research Center (KDA Hospital& MRC)
Mumbai, India N/A No Yes
National Children’s Cardiac SurgicalCenter
Minsk, Belarus Yes Withdrawn Withdrawn
Nhi Dong 1 (Children’s Hospital #1) Ho-Chi Minh City, Vietnam Yes Yes YesShanghai Children’s Medical Center Shanghai, China No Yes YesStar Hospital Hyderabad, India Yes No YesUganda Heart Institute, Mulago Hospital Kampala, Uganda Yes No YesUnidad de Cirugía CardiovascularPediátrica (UNICARP) de Guatemala
Guatemala City, Guatemala Yes No No
United Hospital Dhaka, Bangladesh N/A Yes Yes
N/A, not yet participating in International Quality Improvement Collaborative.
e1424 JENKINS et al at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

framework of Situation, Background,Assessment, and Recommendation, acommunication model adopted fromthe US Nuclear Navy,12 has been foundto be beneficial in health care settings.An example of assertion training thatreinforces infection reduction strategiesincludes empowering nurses to speakup in a professionalmannerwhen sterilityis compromised or when practice bun-dles are not followed. Detailed demon-strations of fundamental and advancedcompetencies for pediatric cardiovas-cular nurses were also presented.
Outcomes
The following outcome variables werecollected: in-hospital mortality, 30-daymortality, surgical site infection, andbacterialsepsis.Anymajor infectionwasdefined as surgical site infection and/orbacterial sepsis. Surgical site infectionwas defined according to Centers forDiseaseControlandPrevention/NationalHealthcare Safety Network definitions.13
Bacterial sepsis was defined as knownor presumed bacterial sepsis with feveror hypothermia, tachycardia, hypo-tension, tachypnea, leukocytosis, orleukopenia.
Auditing and Analysis
Multidisciplinary teams from BostonChildren’s Hospital, as well as NGO rep-resentatives and volunteers, conductedsite visits consisting of hospital tours,round table discussions, and formalpresentations to reinforce collaborativegoals. In addition, data source verificationwas performed by using a minimum 10%sample of all cases entered into the IQICdatabase. Key variables audited includedtype of procedure, RACHS-1 risk cate-gory, age, prematurity, major noncardiacstructural anomaly, postoperative out-comes, and 30-day follow-up. Auditresults determined whether dataweresufficiently complete and accurate forinclusion in aggregate results. Annualbenchmarking reports were providedto each site and discussed in detailduring designated webinars; sites re-ceived aggregate collaborative data forthe calendar year as well as data specificto their institution. Site-specific outcomeswere compared with the aggregate, andtrends over time were examined.
For the current analysis, patient char-acteristics, procedural information, andsurgical outcomeswere summarized for
15 049 cases of congenital heart surgeryin patients,18 years of age from sitesparticipating in the IQIC at any time be-tween 2010 and 2012, and for which datawere verified by audit (13 sites in 2010,14 sites in 2011, 24 sites in 2012). Toevaluate the effectiveness of the IQIC inreducing mortality and infections, risk-adjusted outcomes for 2011 and 2012were compared to the appropriate ref-erence population. The previously vali-dated RACHS-1 method was used torisk adjust in-hospital mortality; pa-tient risk factors included in the modelare surgical risk category (categories1 through 6), age group, prematurity,major noncardiac structural anomaly,andmultiple congenital heart proceduresduring the admission. A risk adjustmentmodel for occurrence of major infec-tion was derived based on 2010 aggre-gate data; logistic regression analysiswas used, and only patient risk factorssignificant at the 0.05 level of significancewere retained in the final model. Fac-tors included were RACHS-1 risk cate-gory, age group, major medical illness,malnourished or emaciated nutritionalappearance, and oxygen saturation,90%. For bothmodels, congenital heart
FIGURE 1Implementation of quality improvement methodology to reduce mortality.
QUALITY REPORT
PEDIATRICS Volume 134, Number 5, November 2014 e1425 at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

surgery cases either ineligible forRACHS-1risk adjustment (such as premature in-fants or neonates undergoing patentductus arteriosus ligation only) or unableto be assigned to a risk category wereexcluded. The c statistic, a measure ofdiscrimination, was provided for eachmodel; a c statistic of 0.5 indicates thatthe model is no better than chance atpredicting who will experience the out-come of interest and who will not,whereas a value of 1.0 indicates that themodel predicts the outcome perfectlyevery time. Standardized mortality ratios(SMRs), standardized infection ratios(SIRs), and their 95%confidence intervals(CIs) were calculated for aggregate datafrom 2011 and 2012, using 2010 as thereference population. An SMR is defined
as the observed mortality rate in a cal-endar year divided by the mortality rateexpected in that year based on patientcase mix; an SMR .1.0 suggests higherthan expected in-hospital mortality rela-tive to the reference population, whereasan SMR ,1.0 indicates lower thanexpected mortality. If a 95% CI for theSMR does not contain the value 1.0, thenrisk-adjusted mortality is significantlydifferent from the reference population(P, .05). SIRs are similarly interpreted.Because different institutions contrib-uted data in different years, SMRs andSIRs for 2011 and 2012 relative to 2010were also generated for the 7 sites con-tributing data for the entire time period,using these 7 sites’ 2010 data as thereference population rather than the
entire collaborative. Similarly, SMRs andSIRs for 2012 relative to 2011 were gen-erated for the 14 sites contributingdata in both 2011 and 2012. Statisticalanalyses were conducted by using SASversion 9.2 (SAS Institute, Inc, Cary, NC).
RESULTS
Among 28 sites, 15 joined by 2010, 7joined in 2011, and 6 joined in 2012. Onesite officially withdrew after 2010. Allsites except one met data audit re-quirements in at least 1 calendar year. Atotal of 16 979 cases of congenital heartsurgery were entered into the IQIC da-tabase between 2010 and 2012. Of these,15 049 cases in patients ,18 years ofage at the time of surgery, representing27 sites in 16 countries, were verified by
FIGURE 2Congenital heart surgery check list.
e1426 JENKINS et al at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

data audit. Patient demographics, pa-tient preoperative status and RACHS-1classification, and postsurgery patientoutcomes are shown in Tables 2, 3, and 4.
The unadjusted in-hospital mortalityratewas 6.3%. The 30-daymortality ratewas 7.4% among sites reporting 30-daymortality data for at least 90% of sur-gical cases (7 sites in 2010, 12 sites in2011, 19sites in2012); siteswereunableto capture 30-day mortality data for24.4% of cases. The surgical site in-fection rate was 2.1%, the bacterialsepsis ratewas5.5%, and the rateof anymajor infection was 7.0%. In-hospitalmortality was 1.5% in RACHS-1 riskcategory 1, 3.8% in category 2, 10.6% incategory 3, 17.7% in category 4, and51.1% in categories 5 and 6 combined.
TheRACHS-1 risk adjustmentmodel for in-hospital mortality applied to the 2010–2012 combined aggregate data is dis-played in Table 5, with a c statistic formodel discrimination of 0.740. SMRs forthe aggregate data from 2011 and 2012,using 2010 as the reference population,are shown in Table 6. The SMR was 0.71(95%CI 0.62–0.81) in 2011 and 0.76 (95%CI0.69–0.83) in 2012. Therefore, risk-adjustedin-hospital mortality was significantlylower inboth2011and2012relative to2010.
Table 6 also shows SMRs for 2011 and2012 for the 7 sites contributing datafrom 2010 to 2012, using 2010 data fromthese 7 sites as the reference population,as well as the SMR for 2012 for the 14sites contributing data in 2011 to 2012,using 2011 data from these 14 sites asthe reference. The SMRs for the 7 sites
were 0.85 (95% CI 0.71–1.00) in 2011 and0.80 (95% CI 0.66–0.96) in 2012, and forthe 14 siteswas 0.80 (95%CI 0.70–0.91) in2012. Thus, among sites participating inall 3 years, or both 2011 and 2012, risk-adjusted in-hospital mortality decreasedsignificantly.
When applied to the aggregate datafrom 2010 to 2012, the risk adjustmentmodel for major infection yielded a cstatistic of 0.747. SIRs for the aggregate
data from 2011 and 2012, using 2010 asthe reference population, are shown inTable 6. The SIR was 0.65 (95% CI 0.58–0.73) in 2011 and 0.53 (95% CI 0.48–0.58) in 2012. Therefore, risk-adjustedmajor infection decreased significantlyin both 2011 and 2012 relative to 2010.
Table 6 also shows SIRs for 2011 and2012 for the 7 sites contributing datafrom 2010 to 2012, using 2010 datafrom these 7 sites as the reference
TABLE 2 Patient Demographics
Number Percent
Total cases 15 049 100.0Age at surgery#30 d 969 6.431 d to ,1 y 5942 39.51 to 17 y 8138 54.1
GenderFemale 6661 44.3Male 8378 55.7Not reported 10 —
TABLE 3 Patient Preoperative Status and RACHS-1 Risk Classification
Number or Median Percent or Range
Nutritional appearanceNormal 9282 61.9%Malnourished 3839 25.6%Emaciated 1797 12.0%Overweight 86 0.6%Not reported 45 —
WHO weight for age percentile (if age at surgery ,10 y),5th percentile 3965 52.3%$5th, ,15th percentile 1003 13.2%$15th percentile 2617 34.5%Not reporteda 7364 —
Preoperative proceduresBalloon atrioseptostomy 121 0.8%Resuscitation 46 0.3%Inotrope therapy 126 0.8%Ventilation preoperatively 524 3.5%No preoperative procedure reported 14 232 94.6%
PrematurityYes 808 5.4%No 14 097 94.6%Not reported 144 —
Major noncardiac structural anomalyYes 433 2.9%No 14 595 97.1%Not reported 21 —
Major chromosomal abnormalityYes 848 5.7%No 14 058 94.3%Not reported 143 —
Major medical illnessYes 835 5.6%No 14 175 94.4%Not reported 39 —
Weight, kg 8.2 0.1–139Height, cm 74 10–198Hematocrit 37 1.3–99Oxygen saturation, % 95 4–100RACHS-1 risk category1 2724 18.1%2 7254 48.2%3 3347 22.2%4 750 5.0%5 9 0.1%6 78 0.5%Unassigned 436 2.9%Not eligible 451 3.0%
a Available for cases enrolled in 2012 only.
QUALITY REPORT
PEDIATRICS Volume 134, Number 5, November 2014 e1427 at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

population, as well as the SIR for2012 for the 14 sites contributing datain 2011 to 2012, using 2011 data fromthese 14 sites as the reference. TheSIR for the 7 siteswas 0.64 (95% CI 0.56–0.74) in 2011 and 0.53 (95% CI 0.43–0.62)in 2012, and for the 14 sites was 0.77(95% CI 0.68–0.87) in 2012. Thus, amongsites participating in all 3 years, or both
2011 and 2012, risk-adjusted major in-fection decreased significantly.
DISCUSSION
The IQIC was officially launched in2008 to provide benchmarking datafor congenital heart surgery in thedevelopingworld,with theoverall goalofguiding quality improvement efforts andreducing mortality for congenital heartdisease. Outcomes were reported for15 049 surgeries in patients,18 yearsof age from27 sites in 16 countries self-identified as developing world. Col-laborative learning focused on 3 keyareas: safe perioperative practice usinga surgical safety checklist, reduction ofsurgical site infections and bacterialsepsis, and team-based practice throughnurse empowerment and effectivecommunication. Overall unadjusted in-hospital mortality was 6.3%; mortalityrates within RACHS-1 risk categorieslook similar to those reported in theUnited States in 1994 to 1996.6 Risk-adjusted mortality and infections weresignificantly lower in 2011 and 2012,compared to the appropriate referencepopulation, for the collaborative over-all and for institutions participating inthe IQIC during consecutive years. Al-though these reductions cannot be at-tributed to the IQIC with certitude, therapid improvements in both mortalityand infections are highly suggestive ofsuccess.
Key driver diagrams create a usefulframework for collaborative quality im-provement.14 The 3 key drivers chosen forthe IQIC were identified by developingworld cardiac surgeons and were com-mon across diverse geographic loca-tions. Increasing evidence has shown thatuse of surgical safety checklists in peri-operative settings can reduce mortalityand prevent complications by improvingteamwork, communication, and overallquality of care,15–18 and the World HealthOrganization strongly recommendsworldwide adoption of surgical safetychecklists.19 The potential benefit ofthis intervention may be even greaterfor surgical procedures that are com-plex and involve high-risk patient pop-ulations.20 Children with congenitalheart disease represent a particularlyhigh-risk population that could greatlybenefit from the coordination of team-based care, and thus implementationof a surgical safety checklist was in-cluded as a key driver.
Strategies for preventing hospital-acquired infections are significantlyless robust in the developing world.21,22
Hospital-acquired infections are associ-ated with increased morbidity, mortality,and hospital costs.23 The occurrence ofthese infections in countries with lim-ited resources imposes a significantburden on the health care system, andresults in resources being directedaway from care of additional pa-tients.24 In recent years, hospitalsthat have introduced evidence-basedpractice bundles to prevent occurrenceof device-associated and surgical siteinfections have successfully decreasedoccurrence of these infections.10,23,25,26
Hand hygiene is the cornerstone ofevery bundle to reduce device-associatedand surgical site infections. Theseand other practices were incorporatedinto learning modules to reducehospital-acquired infections, and in-fections also were included as sec-ondary outcomes.
TABLE 4 Postsurgery Patient Outcomes
Number Percent
In-hospital mortalityYes 926 6.3No 13 882 93.7Not reported 241 —
Surgical siteinfectionYes 312 2.1No 14 711 97.9Not reported 26 —
Bacterial sepsisYes 822 5.5No 14 175 94.5Not reported 52 —
Any major infectionYes 1043 7.0No 13 953 93.0Not reported 53 —
MortalityRate, %
95% CI
RACHS-1 riskcategorya
1 1.5 (1.0–2.0)2 3.8 (3.4–4.3)3 10.6 (9.6–11.7)4 17.7 (15.0–20.7)5+6 51.1 (40.1–62.1)Unassigned 9.7 (7.0–13.0)Not eligible 11.4 (8.6–14.8)
a The 241 cases where in-hospital mortality was notreported are excluded.
TABLE 5 RACHS-1 Risk Adjustment Model for In-Hospital Mortality (2010–2012 Aggregate Data)
Odds Ratio 95% CI P Value
RACHS-1 risk category1 1.0 — —
2 2.4 (1.7–3.4) ,.0013 6.7 (4.8–9.3) ,.0014 9.1 (6.2–13.2) ,.0015+6 36.8 (21.4–63.0) ,.001
Age at surgery#30 d 3.0 (2.4–3.8) ,.00131 d to ,1 y 1.7 (1.4–2.0) ,.0011 to 17 y 1.0 — —
Prematurity 1.5 (1.1–2.0) .007Major noncardiac structural anomaly 2.1 (1.5–2.8) ,.001Multiple cardiac procedures 1.0 (0.8–1.1) .52
The c statistic for this model is 0.740.
e1428 JENKINS et al at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

It is widely recognized that effectivecommunication and teamwork are es-sential for the delivery of high-quality andsafe patient care. Ineffective communi-cation has been linked to inadvertentpatient harm.27 Nurses must feelempowered to confidently communicatepatient concerns. Educational and cul-tural barriers that preclude nurses fromspeaking freely are prevalent amongdeveloping world countries.28 Thus,team-based practice through nurse em-powerment and effective communicationwas included as a major key driver forreducing mortality.
Collaborations between programs incountries of the developed and develop-ing world and NGO capacity-buildingpartnerships provide an invaluable op-portunity to build sustainable quality-driven cardiac surgery programsworldwide.The IQIChas,withthesupportand targetedtechnicalassistanceofNGOpartners to facilitate implementa-tion, fulfilled critical needs in moni-toring clinical outcomes and providingbenchmarking data, as well as edu-cating developing programs with re-spect to key determinants of mortality,data collection, data analysis, andquality improvement techniques. The
IQIC reports significant, reliable, pre-viously unavailable outcome data froma substantial number of developingworld surgical programs. Risk-adjustedmortality and infections were signifi-cantly lower in2011and2012, comparedto the appropriate reference pop-ulation, for the collaborative overalland for institutions participating in theIQIC during consecutive years. Thus, inamere 3 years, the IQIC appears to havesuccessfully reduced both infectionsand mortality after congenital heartsurgery among participating sites.Despite some limitations in our formalanalysis, such as lack of standardizeddefinitions for several infection variables,missing data, and, importantly, lack ofa nonparticipating comparison group,audited results suggest substantial sta-tistically significant improvements, andthe focus and time frame are highlysuggestive of success due to qualityimprovement efforts by teams throughIQIC learning and NGO-supported imple-mentation. These successes may bereplicable in other medical conditions,thereby allowing rapid translation ofknowledge and practice throughout de-veloping world settings to reduce globalhealth care disparities.
This collaborative effort also has yieldedcritical data on congenital heart sur-gery in low-resource environments,with audited results from more than15 000 cases. Although data are pooledfrom sites self-identified as operating inlow-resource settings without other in-clusion criteria, this is neverthelessa rich source of useful, previously un-available information. The data col-lected will allow further researchregarding the outcomes of and riskfactors for various types of congenitalheart disease in these settings, as wellas the development of improved riskadjustment methods, if required. Simi-larly, it will be possible to addressimportant questions regarding the suc-cess of quality improvement activities invarious low-resource settings, such aschildren’s versus nonchildren’s hospi-tals, free-standing heart centers versusfull-service hospitals, sites differing inannual clinical volume, and sites sup-ported by NGOs in different ways, as wellas to gain an understanding of specificprocesses that led to improvement.Efforts are currently under way to in-crease this critical body of information,which should further enhance the rapidspread of access to successful congen-ital heart surgery.
ACKNOWLEDGMENTSWe recognize the following individualswho have helpedmake this project suc-cessful: Dorothy M. Beke, RN, MS, CPNP-PC/AC, David Dennis, BA, Patricia Galvin,RN, Vlad Gankin, BS, Matthew Glynn, BA,Rebecca Hehn, MA, Annette Imprescia,BSN, RN, CCRN, David Roberson, MD,Beverly Small, RN, Ravi Thiagarajan,MD, Jason Thornton, RN, MSN, CCRN,and Traci Wolbrink, MD, MPH.
REFERENCES
1. Pezzella AT. International cardiac surgery:a global perspective. Semin Thorac CardiovascSurg. 2002;14(4):298–320
2. Jamison DT, Breman JG, Measham AR,et al. Disease Control Priorities in Develop-ing Countries. 2nd ed. Washington, DC:
The International Bank for Reconstruc-tion and Development/The World BankGroup; 2006
TABLE 6 Risk-Adjusted Standardized In-Hospital Mortality and Infection Ratios
SMRs
2010 2011 2012
Aggregate data 1.00 0.71 (0.62–0.81) 0.76 (0.69–0.83)7 sites contributing data 2010–2012 1.00 0.85 (0.71–1.00) 0.80 (0.66–0.96)14 sites contributing data 2011–2012 — 1.00 0.80 (0.70–0.91)
SIRs
2010 2011 2012
Aggregate data 1.00 0.65 (0.58–0.73) 0.53 (0.48–0.58)7 sites contributing data 2010–2012 1.00 0.64 (0.56–0.74) 0.53 (0.43–0.62)14 sites contributing data 2011–2012 — 1.00 0.77 (0.68–0.87)
Standardized ratios are shown with 95% CIs.
QUALITY REPORT
PEDIATRICS Volume 134, Number 5, November 2014 e1429 at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

3. Saxena A. Strategies for the improvementof cardiac care services in developingcountries: what does the future hold?Future Cardiol. 2012;8(1):29–38
4. Tchervenkov CI, Jacobs JP, Bernier PL, et al.The improvement of care for paediatricand congenital cardiac disease across theworld: a challenge for the World Society forPediatric and Congenital Heart Surgery.Cardiol Young. 2008;18(suppl 2):63–69
5. Saxena A. Congenital cardiac surgery in theless privileged regions of the world. ExpertRev Cardiovasc Ther. 2009;7(12):1621–1629
6. Jenkins KJ, Gauvreau K, Newburger JW,Spray TL, Moller JH, Iezzoni LI. Consensus-based method for risk adjustment for sur-gery for congenital heart disease. J ThoracCardiovasc Surg. 2002;123(1):110–118
7. Larrazabal LA, Jenkins KJ, Gauvreau K, et al.Improvement in congenital heart surgeryin a developing country: the Guatemalan ex-perience. Circulation. 2007;116(17):1882–1887
8. Weiser TG, Haynes AB, Lashoher A, et al.Perspectives in quality: designing the WHOsurgical safety checklist. Int J Qual HealthCare. 2010;22(5):365–370
9. Norton EK, Rangel SJ. Implementing apediatric surgical safety checklist in the ORand beyond. AORN J. 2010;92(1):61–71
10. Institute for Healthcare Improvement. Pro-tecting 5 million lives from harm. Availableat: http://ihi.org/IHI/Programs/Campaign.Accessed May 14, 2013
11. Boyce JM, Pittet D; Healthcare InfectionControl Practices Advisory Committee;HICPAC/SHEA/APIC/IDSA Hand Hygiene TaskForce; Society for Healthcare Epidemiologyof America/Association for Professionals inInfection Control/Infectious Diseases Soci-ety of America. Guideline for hand hygienein health-care settings. Recommendationsof the Healthcare Infection Control PracticesAdvisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force.
MMWR Recomm Rep. 2002;51(RR-16):1–45,quiz CE1–CE4
12. Kosnik LK, Brown J, Maund T. Patient safety:learning from the aviation industry. NursManage. 2007;38(1):25–30, quiz 31
13. Horan TC, Andrus M, Dudeck MA. CDC/NHSNsurveillance definition of health care-associated infection and criteria for spe-cific types of infections in the acute caresetting. Am J Infect Control. 2008;36(5):309–332
14. Crawford B, Skeath M, Whippy A. Multifocalclinical performance improvement across21 hospitals [published online ahead ofprint August 27, 2013]. J Healthc Qual. doi:doi:10.1111/jhq.12039
15. Haynes AB, Weiser TG, Berry WR, et al; SafeSurgery Saves Lives Study Group. A sur-gical safety checklist to reduce morbidityand mortality in a global population. N EnglJ Med. 2009;360(5):491–499
16. de Vries EN, Prins HA, Crolla RM, et al;SURPASS Collaborative Group. Effect ofa comprehensive surgical safety system onpatient outcomes. N Engl J Med. 2010;363(20):1928–1937
17. Neily J, Mills PD, Young-Xu Y, et al. Associ-ation between implementation of a medicalteam training program and surgical mor-tality. JAMA. 2010;304(15):1693–1700
18. Semel ME, Resch S, Haynes AB, et al.Adopting a surgical safety checklist couldsave money and improve the quality of carein U.S. hospitals. Health Aff (Millwood).2010;29(9):1593–1599
19. World Health Organization. New scientificevidence supports WHO findings: a sur-gical safety checklist could save hun-dreds of thousands of lives. Available at:www.who.int/patientsafety/safesurgery/checklist_saves_lives/en/index.html. AccessedSeptember 9, 2013
20. Weiser TG, Haynes AB, Dziekan G, Berry WR,Lipsitz SR, Gawande AA; Safe Surgery Saves
Lives Investigators and Study Group. Effectof a 19-item surgical safety checklist dur-ing urgent operations in a global patientpopulation. Ann Surg. 2010;251(5):976–980
21. Allegranzi B, Bagheri Nejad S, Combescure C,et al. Burden of endemic health-care-associatedinfection in developing countries: systematicreview and meta-analysis. Lancet. 2011;377(9761):228–241
22. World Health Organization. Health care-associated infections (fact sheet). Avail-able at: www.who.int/gpsc/country_work/gpsc_ccisc_fact_sheet_en.pdf. AccessedSeptember 9, 2013
23. Costello JM, Morrow DF, Graham DA, Potter-Bynoe G, Sandora TJ, Laussen PC. Systematicintervention to reduce central line-associatedbloodstream infection rates in a pediatriccardiac intensive care unit. Pediatrics. 2008;121(5):915–923
24. World Health Organization. Global patientsafety challenge. Available at: www.who.int/gpsc/en/index.html. Accessed September 9,2009
25. Bratzler DW, Hunt DR. The surgical infectionprevention and surgical care improvementprojects: national initiatives to improveoutcomes for patients having surgery. ClinInfect Dis. 2006;43(3):322–330
26. Jeffries HE, Mason W, Brewer M, et al.Prevention of central venous catheter-associated bloodstream infections in pediatricintensive care units: a performance improve-ment collaborative. Infect Control HospEpidemiol. 2009;30(7):645–651
27. Leonard M, Graham S, Bonacum D. Thehuman factor: the critical importance ofeffective teamwork and communication inproviding safe care. Qual Saf Health Care.2004;13(suppl 1):i85–i90
28. Giger JN. Transcultural Nursing: Assess-ment and Intervention. 6th ed. St. Louis,MO: Elsevier/Mosby; 2013
(Continued from first page)
Address correspondence to Kathy J. Jenkins, MD, MPH, Department of Cardiology, Boston Children’s Hospital, 300 Longwood Ave, Farley 135, Boston, MA 02115.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
e1430 JENKINS et al at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-0356; originally published online October 13, 2014; 2014;134;e1422Pediatrics
Morrow, William M. Novick, Shawn J. Rangel, Bistra Zheleva and Jan T. ChristensonKimberlee Gauvreau, Patricia A. Hickey, Jennifer Koch Kupiec, Debra Forbes
Kathy J. Jenkins, Aldo R. Castañeda, K.M. Cherian, Chris A. Couser, Emily K. Dale,Developing World
Reducing Mortality and Infections After Congenital Heart Surgery in the
ServicesUpdated Information &
htmlhttp://pediatrics.aappublications.org/content/134/5/e1422.full.including high resolution figures, can be found at:
References
html#ref-list-1http://pediatrics.aappublications.org/content/134/5/e1422.full.at:This article cites 22 articles, 6 of which can be accessed free
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-0356; originally published online October 13, 2014; 2014;134;e1422Pediatrics
Morrow, William M. Novick, Shawn J. Rangel, Bistra Zheleva and Jan T. ChristensonKimberlee Gauvreau, Patricia A. Hickey, Jennifer Koch Kupiec, Debra Forbes
Kathy J. Jenkins, Aldo R. Castañeda, K.M. Cherian, Chris A. Couser, Emily K. Dale,Developing World
Reducing Mortality and Infections After Congenital Heart Surgery in the
http://pediatrics.aappublications.org/content/134/5/e1422.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Vanderbilt Univ on January 13, 2015pediatrics.aappublications.orgDownloaded from