Embed Size (px)
Citation preview

16.10.2019
1
SPINAL CORD ISCHEMIA
ECNR Rovinj, Oct 16th 2019
Alessandro CianfoniNeuroradiology – diagnostic & interventional
Neurocenter of Southern Switzerland – Lugano
University of Bern, Inselspital
References• “Diagnostic Imaging: Spine” – Ross J, Moore K. Editors. Elsevier (2015)
• “Spinal Cord Infarction and Differential Diagnosis” – Boddu S, Cianfoni A, Kim K, Banihashemi M, Pravatà E, Gobin YP, Patsalides Ain «Neurovascular Imaging» Saba L, Raz E, Editors. Springer (2016)
• “Vascular anatomy of the spinal cord” - Santillan et al, J Neurointerv Surg(2012)
Saliou G, Krings T
Thanks to Dr. Marco Pileggi (Lugano-CH) for help and advise
• 1% of all strokes
• embolic vs. hemodynamic (hypoperfusion)
• 90% anterior spinal artery (in embolic)
• 70% lower thoracic-lumbar regions
ARTERIAL ANATOMY 1Longitudinal arterial trunks (ASA, PSA)
• Not a single straight artery, but rather a consecutive series of anastomotic vascular loops
ARTERIAL ANATOMY 2Segmental arteries
• 1 pair of supreme intercostal arteries (above T3)
• 9 pairs of posterior intercostal arteries (T3–T11)
• 1 pair of subcostal arteries (T12)
• 4 pairs of lumbar arteries (L1–L4)
• In the cervical and upper thoracic regions (T1-T2), theyoriginate from vertebral artery, deep cervical artery and ascending cervical artery
• In lower lumbar and sacral region (L5, sacrum), theyoriginate from median sacral artery and branches of the internal iliac arteries
From: “Vascular anatomy of the spinal cord”, Santillan et al. (2012)
Saliou G, Krings T

16.10.2019
2
ARTERIAL ANATOMY 3Radiculomedullary arteries
• Only at some nerve root levels
• On average:• 6 anterior radiculomedullary arteries (2–14), including:
• Artery of Adamkiewicz
• Artery of the cervical enlargment (usually C6)
• 11-16 posterior radiculomedullary arteries
From: “Spine”,Ross J, Moore K From: “Atlas of Human Anatomy”, Netter F.
ARTERIAL ANATOMY 4Radiculomedullary arteries
• The artery of Adamkiewicz (arteria radicularis magna, artery of the lumbarenlargement) is the largestradiculomedullary artery
• Hairpin with ascending branch
• 75% between T8 and L2, but can be identified as superiorly as T5 and asinferiorly as L4
• 80% on the left side
SPINAL BLOOD SUPPLYWatershed “paradox”
• Cervical and upper thoracic cord (up to T2/T3) usually supplied by vertebral arteries and 2–3 anterior radiculomedullary arteries
• The intermediate cord segment involving the mid-thoracic cord (T4–T8) is a poorly vascularized segment
• Lower thoracic and lumbar cord usually supplied by 2–3 anteriorradiculomedullary arteries
WATERSHED PARADOX
>95% of cardiac arrest and hypotensive patients with associated ischemic myelopathy had predominant involvementof the lumbosacral level followed by cervical level, with relative
sparing of thoracic levels (selective vulnerability?)
VENOUS ANATOMY
• The variability of the spinal cord venous drainageis even greater than that of the arterial system
• The anterior spinal vein accompanies the ASA
• Along the posterior surface there is high variability, as up to three posterior longitudinalveins may be present (two accompanies the PSAs and one in median position)
• The great anterior radiculomedullary vein may be mistaken for the artery of Adamkiewicz due to the similar location and course
From: “Vascular anatomy of the spinal cord”, Santillan et al. (2012)
ETIOLOGY – CLASSIFICATION
• Ischemic– Hypoperfusion related
• Aortic surgery
• Aortic Dissection
• Atherosclerosis (relative sparing spinal arteries)
• Systemic Hypotension
• Surfer’s Myelopathy
– Embolism Related 654
• Thromboembolic Infarction
• Fibrocartilaginous Embolism
• Infection
• Iatrogenic Embolization (Spinal Angiography)
• Venous
• Haemorrhagic
ETIOLOGYAortic surgery / Aortic dissection
• Most common etiology for
spinal cord infarction
mechanism:
– hypoperfusion due to prolonged clamping
– “declamping synd” and SC tamponade
– increased CSF pressure during clamping
– false lumen

16.10.2019
3
ETIOLOGYAtherosclerosis
• Spinal arterial network undergo minimalalterations compared to other arteries
• ASA is the most affected
• Good collateral circulation prevents infarction
ETIOLOGYSystemic hypoperfusion
• Commonly lower SC (“Watershed paradox”)
ETIOLOGYEmbolic infarction
Most common sources:
1. Emboligenous cardiac pathology
2. Fibrocartilagineous embolism after trauma (women, young age)
– Fragments of intervertebral disks
3. Infection– Prior to introduction of penicillin, syphilis was a common
cause
– Today is usually as late complication of aortic surgery
4. Iatrogenic embolization– Rare etiology with modern equipment
ETIOLOGYSurfer’s myelopathy
• Acute non-traumatic myelopathy
• Prolonged spinal hyperextension in prone posture and repetitive flexion and extensionresulting in watershed ischemia
• Proposed pathophysiology:– avulsion of perforating vessels
– vasospasm of the a. of Adamkiewicz
– inferior vena cava obstruction
• Complete or near-complete recovery in mostpatients, but residual paraplegia has beenreported
Mixed ETIOLOGYin surfer’s myelopathy
….surfer’s heart attack!
CLINICAL PRESENTATION
– Back pain at onset (ddx sign in non-compressive myelopathies)
– Bilateral weakness/paralysis
– Sensory loss (pain-temperature/vibration-proprioception)
– Urinary retention

16.10.2019
4
CLINICAL PRESENTATION
• Spinal cord syndromes in SCI:
1) Anterior spinal artery syndrome
2) Complete spinal cord syndrome
3) Brown-Sequard syndrome
4) Posterior spinal artery syndrome
IMAGING
• Modality of choice in acute phase: MRI
• underlying etiology (?)
• differential diagnosis and
RULE OUT COMPRESSIVE ETIOLOGIES
STANDARD PROTOCOL
• 1.5-3.0 T• Multiplanar T2WI (sagittal, axial)• At least one T1WI sequence (sagittal)• DWI• +/- Contrast-enhanced MRA• Multiplanar CE T1 Fat sat
• MRI may be normal in hyperacute (T2 normal up to 8-72h) (T2 positive in 50% @24h)
IMAGING FINDINGS
E Pravata’, C Cereda, A Gabutti, D Distefano, A Cianfoni. Spine J 2014
IMAGING FINDINGS
• Longitudinal T2 signal >2 vertebral levels
• Central lesion in SC on axial T2-W
• T2 findings non-specific
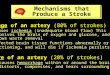
Stages of spinal cord ischemia
1) Anterior horn(Owl’s eyes sign)
2) Central gray matter ischemia
Stages of spinal cord ischemia
3) Gray and white matter ischemia
4) Cross section ischemia

16.10.2019
5
2/3 ant cord syndrome IMAGING FINDINGS
• Bone infarct in hemivertebra (30%) (strong sign in ddx non-compressive myelopathies)
IMAGING FINDINGS
• Contrast-enhancement in subacute (SC and rarely cauda equina)
E Pravata’, C Cereda, A Gabutti, D Distefano, A Cianfoni. Spine J 2014
• DWI and ADC evolve similarly to brain ischemia
• …but more false negatives
• technical challenges (size SC, SNR, motion, breathing, heart, CSF pulsation, susceptibility, b500-700)
IMAGING FINDINGS
DWI b 600 ADC

16.10.2019
6
• DWI axial vs sagittal
• Axial has less artifacts
• No normal SC background signal on axial plane
???
Sick patients: motion artefacts

16.10.2019
7
A B C
D
Luigetti M, Cianfoni A, Conte A, Colosimo C, Tonali PA, Sabatelli M. Posteriorischaemic myelopathy associated with cocaine abuse. Intern Med J. 2010
A B C D
Follow-up
Luigetti M, Cianfoni A, Conte A, Colosimo C, Tonali PA, Sabatelli M. Posteriorischaemic myelopathy associated with cocaine abuse. Intern Med J. 2010
Multi-embolic etiology-diver’s decompression sickness-
Mixed etiology-delayed post-traumatic SC infarct-
Chronic sequelae:myelomalacia
IMAGING – MRA / CTA
• Do we need to demonstrate the vessel occlusion?
• Screening tool before DSA when a SVM is suspected
• May serve as guide for DSA, to reduce the number of catheterized vessels
MRA technique• TOF-MRA and PCA-MRA unable to depict
normal spinal cord vessels• CE-MRA is performed with strong bolus
injection to provide separation of intraduralarteries and veinsNijenhuis R. AJNR 2006

16.10.2019
8
IMAGING – MRA / CTA
LIMITS:• Limited spatial resolution (CT 0.4 mm,
MR 1.0 mm) for the vessels involved:– Artery of Adamkiewicz: 0.5-1.0 mm
– ASA: 0.2-0.8 mm
– PSA: <0.5 mm
• Unable to identify arterialized veins in SVMs due to low temporal resolution
• Arteries and veins are oftenundistinguishable on MRA-CTA
At present no valid treatment of SC infarct based on vascular imaging
IMAGING – DSA
• Differentiation of embolic from non-embolic etiology
• Higher spatial (0.2 mm) and temporal resolution (0.25 s)
• Mandatory if SVMs is suspected
(AKA identified in almost 100%)
• Time consuming, radiation, contrast load• Small risk of complication (invasive procedure)• Clinical relevance?
Systemic hypoperfusion(non-embolic)
• Commonly lumbar region, up to 70% (“Watershed paradox”)
Embolic infarction
IMAGING - MRIAdvanced techniques
• diffusion tensor imaging (DTI) and fiber tractography (FT) are increasingly investigated
• Fractional anisotropy (FA) of DTI showed better correlation with motor function and clinical findings compared to the conventional MRI
• currently only a research tool, it holds considerable promise in predicting the severity of spinal cord injury (at day 9-10; Theaudin et al 2013)
DIFFERENTIAL DIAGNOSIS
• MULTIPLE SCLEROSIS– Asymmetric, peripheral lesions
– Less than 2 segments
– Cervical region (and brain!)
– “Relapsing-remitting” course

16.10.2019
9
DIFFERENTIAL DIAGNOSIS
• IDIOPATHIC TRANSVERSE MYELITIS– Challenging to differentiate with imaging
– Extension beyond vascular territories
– History of recent viral infection or vaccination
– Pleiocytosis and elevated IgG in CSF
DIFFERENTIAL DIAGNOSIS
• TRANSVERSE MYELITIS (mycoplasma)
DIFFERENTIAL DIAGNOSIS
• ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)– Thoracic and cervical cord most commonly affected
– Cerebral involvement in all patients (basal ganglia, thalamus, brain stem, brain cortex)
DIFFERENTIAL DIAGNOSIS
• SPINAL CORD ARTERIOVENOUS SHUNT (SDAVFs, AVMs)– Spinal cord edema may mimic a cord infarction (cord swelling and CE
in subacute stage, atrophy in chronic stage)
– DAVFs usually present with tortuous, dilated perimedullary vessels with “flow void” artifacts
TREATMENT
• Antiplatelet agents
• Systemic high arterial pressure (MAP >90 mm Hg)
• CSF lumbar shunt and aggressive control of hypotensionduring aortic surgery
• Electrophysiology check during aortic surgery
• Prevention of secondary complications and physical therapy
• Embolic
• Hypoperfusion
• Aortic pathology and surgery
• T2 signal in grey matter or anterior 2/3, longitud > 2 levels
• May have CE in subacute phase
• T2 and CE changes non-specific
• MRI in emergency might be normal (DWI?) but mandatory to rule out treatable conditions
• Clues to diagnosis: acute onset back pain, osseous infarct
• Vascular spinal studies at the moment have no impact on treatment
Summary