Embed Size (px)
Citation preview

Neuropsychology2001, Vo l . 15 , No. l , 80-100
Reflective and ReflexiveWith Frontal
Anselika LensfelderUiiversität Mü"nchen
Patients with frontal lobe damage are often unable tocope with everyday life despite their unaffected perfor-mance in tests of intelligence, language, memory, and per-ception (Grattan & Eslinger, l99l). This discrepancy hasstimulated various models describing the planning and ac-tion control deficits in patients with frontal brain lesions.
For a long time, the frontal lobes have been considered tobe involved in regulating and programming behavior (e.9.,Harlow, 1896/1993:'Luna,1962, 1973; Pribram, 1987; Pri-bram & Tubbs, 1967). Hierarchical models of brain func-tioning (Stuss & Benson, 1986; Tranel, Anderson, & Ben-ton, 1994) assume that executive functions (including an-ticipation, goal selection, planning, monitoring, and use offeedback), located in the prefrontal cortex, control the lowerlevel fixed functional systems (e.g., attention, memory).Other models make a distinction between explicit and im-
Angelika Lengfelder, Institut für Pädagogische Psychologie undEmpirische Pädagogik, Universität München, München, Germany;Peter M. Gollwitzer, Fachgruppe Psychologie, Universität Kon-stanz, Konstanz, Germany, and Department of Psychology, NewYork University.
This research was supported by the Max-Planck ResearchAward of the Max-Planck-Society and the Humbold Society toPeter M. Gollwitzer, as well as the Max-Planck-Institute for Psy-chological Research. We greatly appreciate the help of Gabi Mat-thes-von Cramon in collecting the data of the neurological patients.We are particularly indebted to Detlef von Cramon, who was thechair of the Unit of Neuropsychological Rehabilitation at theKrankenhaus München Bogenhausen at the time of the study, forproviding access to the patients panicipating in the present study.Thanks are due to Irmina Quenzel and Maya Böhm, who assistedin collecting and analyzing the data.
Correspondence conceming this article should be addressed toAngelika Lengfelder, Institut für Pädagogische Psychologie undEmpirische Pädagogik, LMU München, Leopoldstr. 13, D-80802München, Germany. Electronic mail may be sent to [email protected].
Copyright 2001 by the American Psychological Association, Inc.0894-4 I 05/01/$5.00 DOI: I 0. 1037//089+4 I 05. I 5. 1.80
Action Control in PatientsBrain Lesions
Peter M. GollwitzerUniversität Konstanz and New York University
plicit control of action. Processes of the frontal lobes areassumed to be involved whenever a new activity is beinglearned. However, when an activity has become routine,other brain regions-especially subcortical ones-are saidto determine action. For instance, Norman and Shallice(1986) suggested that two processes operate in the selectionand control of action: contention scheduling (CS) and thesupervisory attentional system (SAS). CS acts through lat-eral activation and inhibition of action schemas dependingon their activation value, and, thus, behavior is triggeredautomatically. The SAS, in contrast, provides the consciousattentional control of action selection by modulating theactivation and inhibition values of action schemas, and thusis assumed to be responsible for planning, decision making,and monitoring behavior. Whereas the SAS is thought to belocated in the frontal lobes, CS is assumed to take place inother regions of the brain (possibly the basal ganglia). Tosuppon their model, Norman and Shallice (1986) referred toslips of action (Reason, 1987) that occur when action istriggered by CS unmonitored by the SAS.
Indeed, in patients with frontal lesions, heightened fre-quencies of action slips have been documented in researchon utilization behavior (Fukui, Hasegawa, Sugita, & Tsuka-goshi, 1993; Lhermitte, 1983; Shallice, Burgess, Schon, &Baxter, 1989), imitation behavior (Lhermitte, Pillon, & Ser-daru, 1986; Luria, 1973), environmental dependency (Lher-mitte, 1986), novelty preference (D. S. Levine, Leven, &Prueitt, 1992), and capture errors in sequencing (DellaMalva, Stuss, D'Alton, & Willmer, 1993).In other words,the intentional goal-directed behaviors of patients with fron-tal brain lesions are easily disrupted and replaced by rou-tinized and habitual behaviors when the current situationentails the respective triggering stimuli.
Even though defective planning and action control afterfrontal lobe lesions are well documented in the neuropsy-chological literature (case studies: e.g., Cockbum, 1995;von Cramon & Matthes-von Cramon. 1994: Damasio. 1985:Konow & Pribram, 1970; overviews: e.9., Fuster, 1989;
Two types of action control derived from the model of action phases (H. Heckhausen & P. M.Gollwitzer, 1987) were analyzed in patients with frontal lesions, patients with nonfrontallesions, and university students. In Study l, reflective action control in terms of goal selectionwas assessed, and impaired deliberation was found in patients with frontal lesions. Study 2assessed reflexive action control in terms of automatic action initiation as a result of formingimplementation intentions (P. M. Gollwitzer, 1999). All participants sped up their responsesto critical stimuli by forming implementation intentions. Moreover, lesion patients with weakperformances on the Tower of Hanoi (TOH) task did worse than patients with strong TOHperformances in Study 1 but better than control participants in Study 2. Findings areinterpreted as a functional dissociation between conscious reflective action control andautomatic reflexive action control.
80
ACTION CONTROL 8 l
Shallice, 1988; Stuss & Benson, 1986), the concepts ofaction control and planning are used inconsistently and areonly vaguely defined. The neuropsychological assessmentof planning also suffers from conceptual vagueness. Forexample, Tower puzzles are commonly used to assess tion-tal functions, even though these tasks do not always suc-cessfully identify patients with fiontal lobe dysf'unctions(Levin, Goldstein, Will iams, & Eisenberg, 1991; Shall ice &Burgess, l99l). Still, there is evidence of impaired perlbr'-mance on Tower puzzles after fiontal lobe lesions (e.g.,Owen, Downes, Sahakian, Polkey, & Robbins, 1990). Inpositron emission tomography (PET) and single photonemission computed tomography (SPECT) studies with nor-mal participants, dorsolateral frontal involvement wasfound during Towel of London petformance (Moris,Ahmed, Syed, & Toone, 1993: Rezai et al., 1993).
Accordingly, Tower puzzles seem to assess frontal func-tions, but it is not clear which functions are assessed. Fordiagnostic pu{poses, Tower puzzles are often used to assessthe ability to look ahead in planning (e.g., Morris et al.,1993), but they are also used to assess procedural leaming(Saint-Cyr, Taylor, & Lang, 1988), which leads to basalganglia activation in addition to activation in frontal areas(Owen, Doyon, Dagher, Sadikot, & Evans, 1998). Goel andGrafman (1995) recently analyzed the task demands ofTower of Hanoi type problems and argued that it is neitherplanning nor sequencing that is assessed in these problemsbut rather the ability to solve goal-subgoal conflicts. Fi-nally, findings fi'om cognitive psychology suggest thatTower puzzles indeed measure different cognitive processesthat relate to various stages of strategy acquisition: con-scious deliberation (participants use reasoned strategieswhen first confronted with the task), sequencing, and pro-cedural learning (Simon, 1975;Kotovsky, Hayes, & Simon,1 985).
Jeannerod (1997) recently suggested that planning is "a
broad process which can be analyzed and decomposed intomore elementary operations" (p. 133). We share this viewand maintain that it is impoftant to explicate the concept ofplanning because it is likely that not all aspects of planningare affected to the same degree by frontal brain lesions. Inthe present article, we put this hypothesis to the test byexploiting recent advances in action control theorizing. Intheir model of action phases, Heckhausen and Gollwitzer( 1 987; Gollwttzer, 1990; Heckhausen, 1 99 1 ) suggested thatintentional control ofaction necessitates the successful solv-ing of four different tasks. First, people need to set prefer-ences between their wishes and desires by engaging inintensive deliberation of the feasibility and desirability ofthe potential goals and then turn the most preferred desiresinto binding goals. Second, once such goal decisions havebeen made, the next task is to make plans for when, where,and how one intends to implement the chosen goal and toinitiate the implementation of goal-directed actions. Third,ongoing goal-directed actions need to be monitored andbrought to a successful ending. Fourth, to be able to decideon further goal striving, one needs to evaluate whether theattained outcomes match the originally desired outcomes.
Gollwitzer (1993, 1999) expanded the theorizing on the
second task of the action phases model (i.e., planning the
initiation of goal-directed actions) by suggesting a distinc-tion between so-called goal intentions ("I intend to achieve
xl") and implementation intentions ("And if I encounter the
situation -r', I will perform the goal-directed behavior z!").Goal intentions turn desires into binding goals, whereasimplementation intentions plan how the goal is going to beattained. Implementation intentions are thus formed in the
service of goal intentions and belong to the planning phase
of goal attainment. It is assumed that implementation inten-tions delegate the control of one's actions to the specified
anticipated future situations, which, once encountered, ini-tiate the intended goal-directed behaviors automatically.Research has demonstrated that behavior specified in im-plementation intentions is initiated immediately, effi ciently,and without conscious intent (Gollwitzer, 1993,1999; Goll-witzer & Brandstätter, 1997: Gollwitzer & Schaal, 1998),
all of which are characteristic features of automatic action
control (Bargh, 1997).The selection of new goals (i.e., the formation of new
goal intentions) would certainly demand conscious reflec-tion, however. Assuming that frontal lobe injuries impairconscious action control processes, patients with a frontallobe lesion should evidence less deliberation when makinggoal decisions compared with people without a frontal lobeinjury.In Study 1, we tested this hypothesis by confrontingpatients with frontal lobe lesions, patients with nonfrontallobe lesions, and university students with numerous differ-ent behavioral choice situations that demanded a goaldecision.
In contrast, because automatic control of habitualizedbehavior remains intact after frontal lobe damage, patientswith frontal lobe lesions should benefit as much from hav-ing formed implementation intentions as control partici-pants. Even though the formation of implementation inten-tions involves conscious reflection, the initiation of thegoal-directed behaviors specified in implementation inten-tions may solely rely on automatic process. ln Study 2, wetherefore helped patients with frontal brain lesions, patientswith nonfrontal brain lesions, and university students toform implementation intentions and then observed whetherthe intended goal-directed behavior became automaticallycontrolled to the same degree in all groups.
In both studies, we analyzed complex processes of actioncontrol in heterogeneous samples. Therefore, we used re-peated measures designs (i.e., within designs) becäuse theymost effectively control for relevant premorbid interindi-vidual differences (e.g., education, life experiences, cogni-tive abilities, sex, age, handedness) and interindividual neu-rological and neuropsychological differences (e.g., lesionlocation, deficiencies in cognitive processing, effects ofrehabilitation). Accordingly, both studies use mixed be-tween-within factorial experimental designs that allow forcomparisons of individual patterns of behavior betweenpatients with frontal brain lesions, other brain-injured pa-tients, and noninjured college students. Within these groups,we compared performances on different types of tasks (i.e',

82 LENGFELDER AND GOLLWITZER
decision problems of various difficulty in Study 1 anddifferent types of preparing a critical response in Study 2).
Study 1: Reflective Action Control
Defective decision making is considered to be a typicalfrontal lobe dysfunction. Problems in decision making havebeen documented in case studies (e.g., Damasio, Tranel, &Damasio, l99l; Eslinger & Damasio, 1985; Saver &Damasio, l99l), whereas experimental studies directly ad-dressing decision making are rare (Bechara, Damasio,Damasio, & Anderson, 1994; Coolidge & Griego, 1995:Decary & Richer, 1995). Still, experimental studies onproblem solving imply that deliberation is hampered inpatients with frontal lobe lesions. Moreover, deficiencies intasks of subject-ordered pointing and recency discrimina-tion not only may indicate def'ective temporal organization(McAndrews & Milner, l99l; Milner, Petrides, & Smith,1985; Petrides & Milner, 1982) but also may hint at im-paired conscious deliberation (Wiegersma, van der Scheer,& Hijman, 1990). Finally, an inferior petformance in theTower of Hanoi can be interpreted as a deficiency in makinggoal-subgoal decisions (Goel & Grafman, 1995).
The present experiment directly addresses the issue ofdeliberating a decision. Participants were confronted withbehavioral choice situations that varied in terms of thenumber and complexity of aspects that needed to be takeninto account to arrive at a reasoned decision. The ability todeliberate adequately was thought to be reflected in a closelink between the perceived difficulty of the problem and thetime spent deliberating on the problem. If this ability islacking, no positive relation between the perceived diffi-culty of the problem and the time spent deliberating shouldprevail. Moreover, the classic result that intensive deliber-ation increases uncerlainty (Mann & Taylor, 1970) shouldfail to emerge.
We ran four groups of participants: patients with frontallobe lesions, patients with nonfrontal lobe lesions, and twocontrol groups consisting of university students. In patlici-pants with intact frontal lobe functioning, the deliberationtime was expected to correlate positively with the perceiveddifficulty of the presented choice problems and negativelywith the rated certainty of the decisions made, whereas nosystematic relations were predicted for patients with frontallobe lesions.
Method
Participants
The clinical sample consisted of 30 brain-injured patients of theKrankenhaus Bogenhausen, München, Germany. Eighteen pa-tients had a frontal brain lesion (7 women, I I men) and 12 had anonfrontal brain lesion (2 women, l0 men). In the liontal lobe (FL)group, the mean age was 32.50 years (SD : 12.N), and in thenonfrontal lobe (NFL) group, the mean age was 42.92 years(SD = 13.93). As nonclinical controls for the frontal lobe (CFL)group, 7 female and 1l male university students were randomlyselected from the participant pool of the Max-Planck-Institute forPsychological Research in Munich, Germany; the same procedure
was applied to create a control group for the nonfrontal lobe(CNFL) group as well. The mean age of the two control groups
was 25.33 years (SD = 2.97) and 24.67 years (SD : 1.83),respectively.
Patients' lesions (see Appendix A for single case information) in
the FL group were due to head injury (r : I I ) and cerebrovascular
disease (n : 7). In the NFL group, head injury (n : 4), cerebro-vascular disease (n -- 6), and hypoxia (n : 2) were considered tobe responsible for the brain lesions. Clinical data about lesionlocation, etiology, handedness, symptoms of paralysis, and mea-
sures of cognitive and motor functions were available in thehospital's files. Patients were selected on the criteria that theywould have no reading difficulties (e.g., alexia, aphasia, or fixationproblems), would possess an intact understanding of instruction,
and would be able to use a pencil with one hand. All patients hadmore than 40 days of recovery. Twenty-five participants had
experienced more than 6 months of recovery and thus qualified aschronic patients (Karnath, Wallesch, & Zimmermann, l99l).
Procedure and Materials
As depressive states are known to increase decision times (Pi-
etromonaco & Rook, 1987), we asked participants at the outset ofthe experiment to fill out two reliable depression scales: the BeckDepression Inventory @DI; Beck, Rush, Shaw, & Emery, 1986;Beck & Steer, 1987) and the Center for Epidemiological StudiesDepression scale (CES-D; Radlofi 1977). Participants then re-
ceived a booklet that contained 20 decision problems of equal
length (15 lines of text each) concerning various aspects of life(including professional and social issues, shopping, eating, finan-
cial investments, transportation or moving; see Appendix B forexamples). In constructing the decision problems, we took steps toavoid issues that are gender biased or too far removed from thepatients' everyday life. To produce enough variance in perceived
difficulty of the decision problems, we constructed problems atdifferent levels of complexity. This was achieved by varying the
number of aspects requiring deliberation (e.g., uncertainty of con-
sequences, questionable attractiveness of these consequences, orquestionable reversibility of these consequences).
Each problem was embedded in a short story (of equal length)and presented on a different page. Participants were instructed toread each problem and to imagine that they were experiencing it inperson. They were told to think about the decision alternativespresented after having read the text and to take as much time as
necessary to make a decision. For each decision problem, twodecision alternatives were listed, and participants were asked topick their choice. Immediately after each decision, participants hadto answer questions that assessed the perceived difficulty of thedecision problem at hand as well as the cenainty of having madethe correct decision using l0-point rating scales (0 = not at all
dfficult, 9 : very difficult; and 0 = not at all certain, 9 : ver!-certain, respectively). The decision time for each problem was
defined as the time from turning the page to marking the chosenalternative. Participants did not know that their decision timeswere recorded while they worked on the decision problems.
Design
A mixed-factorial design was used, with group (FL, NFL, CFL,CNFL) as the between factor and decision problem (Problems
1-20) as the within factor.
ACTION CONTROL 83
Results
Equivalence ofGroups
Before analyzing the individual patterns of behavior (us-ing individual correlation coefficients), we compared groupmeans to explore the differences between groups.
Depression. To assure a valid assessment ofdepression,we computed a correlation coefficient for the two scales(r : .65). The four groups (FL, NFL, CFL, and CNFL) didnot differ in terms of their depression levels as assessed bythe two scales, F"o,(3,56) : 1.68, rs; F.r._o(3,56) :
1.22, ns. BDI scores in the patient group (Mrt : 12.50,SD : 11.72; M*rt: 11.92, SD : 9.58) were slightlyabove normal (normal scores are < I 1: Beck & Steer,1987), which may be a reaction to the lesion or the expe-rienced abrupt life changes. However, these scores are farbelow clinical relevance (clinically relevant scores are >18: Beck & Steer. 1987).
Problem dfficuln, and certairu.y* of decisiort. To assessthe validity of our measures of problem difficulty and cer-tainty of decision, we correlated the perceived difficultywith the rated certainty. The classic finding of a negativerelation between cer-tainty and task difficulty (in the sensethat easier decisions lead to higher certainty ratings; e.g.,Peterson &Pitz, 1988) was confirmed in all groups (rr.r_ :- .73; r*o, : - .71; rcpL: - .81; r i *o,_ : - .46) .
We used the students' ratings of the difficulty of thedecision problems to classify the 20 problems into threedifficulty groups: low, medium, and high. The reliability ofthis grouping was checked by computing Cronbach's alphacoefficients of internal consistency. The reliability of thescores of perceived difficulty (FL Mdn: .66; NFL Mdn :
.14;CFL Mdn : .51; CNFL Mdn : .72) and rated certainty(FL Mdn : .74; NFL Mdn : .72; CFL Mdn : .52; CNFLMdn = .55) tumed out to be satisfactory. When we com-puted a 4 (groups: FL, NFL, CFL, CNFL) x 3 (level ofdifficulty: low, medium, high) analysis of variance(ANOVA) on the mean perceived difficulty of the decisionproblems, a highly significant main effect of level of per-ceived diffic-ulty was observed, Flin,u. t."na(1, 56) : 108.00,p < .001, T' = .66, which was not qualified by an interac-tion with group of participants, Frin.u,,."na(3, 56) : 1.2r, nt.
This pattem of data suggests that the lesion patients per-ceived the increase in difficulty of the 20 decision problemsjust as clearly as the university students did. An analogousanalysis conducted on the dependent variable of ratedcertainty yielded very similar results: efl-ect of prob^lemdiff iculty, Frin"u, t,".0(1,56) : 55.90, p < .001, r1'�=.50; interaction with the group factor, F,,n.o. t...d(3, 56): 1.08, ns.
Decision tintes. We also computed a 4 (groups: FL,NFL, CFL, CNFL) X 3 (level of difficulty: low, medium,high) ANOVA on decision times. It yielded a highly sig-nificant main effect for the level of difficulty, Frin.". ,..nd(1,561 : 4.1n, p < .05, accounting for only 8% of variance(l' : .08), which was not qualified by an interaction effectwith the group fäctor, Fri,"-,,"na(3,561 : 1.tt, rrs. Thistime, however, there was a significant main effect of group,F(3,56) : 5.71, p < .0l.To understand the nature of thegroup differences, we compared the clinical groups withtheir respective student control groups. Whereas bothgroups of lesion patients responded more slowly than therespective control groups (all ts > 2.70, ps < .01), nodift-erence was found between the two lesion groups,(28) < 0.35, ns. This pattern of data suggests that all lesionpatients needed more time to make decisions than universitystudents, which may be due not only to differences in agebut also to a general slowing of information processing insome patients. In the central analyses (see below), we there-fore focused on the relation between dependent variableswithin each individual participant. These individual patternsof data stay unafTected from potential biases rooted ininterindividual diff'erences in speed of processing, age, sex,IQ, and so forth.
Amount of Deliberation
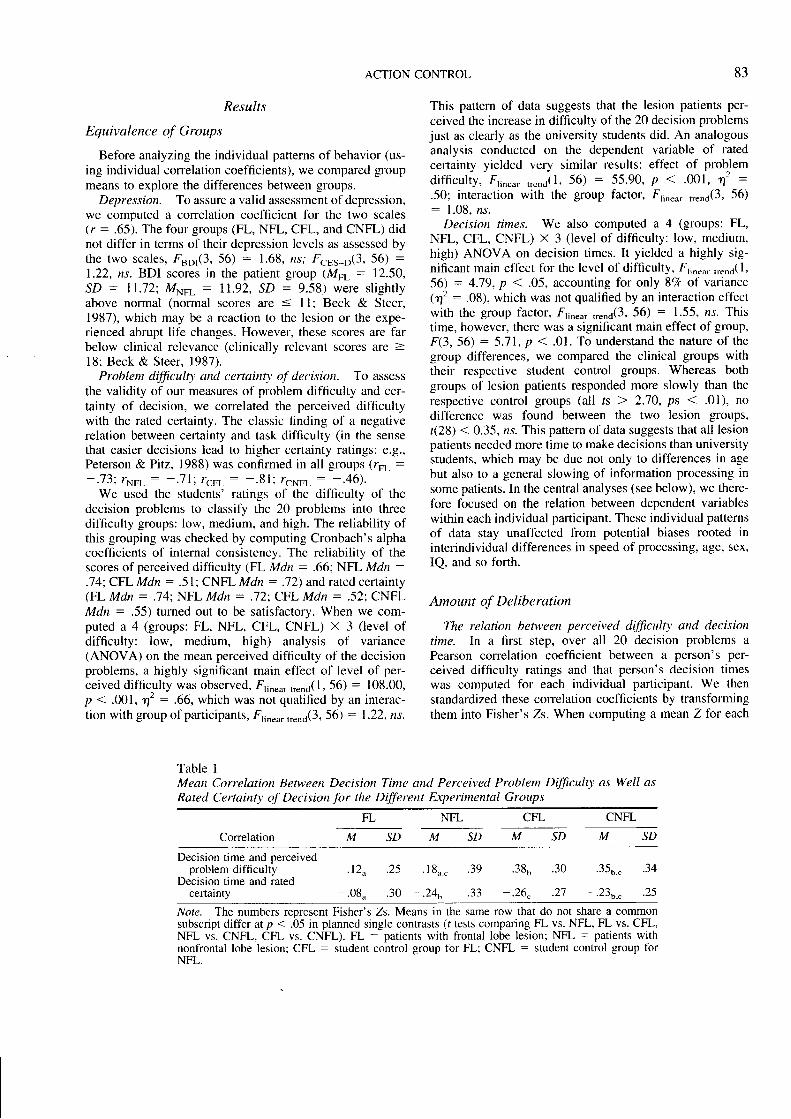
The relation between perceived dfficuln' and decisiontime. In a first step, over all 20 decision problems aPearson correlation coefficient between a person's per-ceived difficulty ratings and that person's decision timeswas computed for each individual participant. We thenstandardized these correlation coefficients by transformingthem into Fisher's Zs. When computing a mean Z for each
Table IMean Correlation Between Decision Time and Perceived Problem Dfficuhl as Well asRated Certainty oY prrrtton for the Dffirent Experimental Groups
NFL CFL CNFL
Correlation
FL
SDMSDMSDMSDM
Decision time and perceivedproblem difficulty
Decision time and ratedcertainty
'12u
-'o8u
' I 8o."
a ^
.38o
- ) A
' " " b . c - J.+
.25
.30
.27
.39
. J J
.25
.30
Note. The numbers represent Fisher's Zs. Means in the same row that do not share a commonsubscript differ at p < .05 in planned single contrasts (r tests comparing FL vs. NFL, FL vs. CFL,NFL vs. CNFL, CFL vs. CNFL). FL = patients with liontal lobe lesion; NFL = patients withnonfrontal lobe lesion; CFL : student control group for FL; CNFL : student control group forNFL.
84 LENGFELDER AND GOLLWITZER
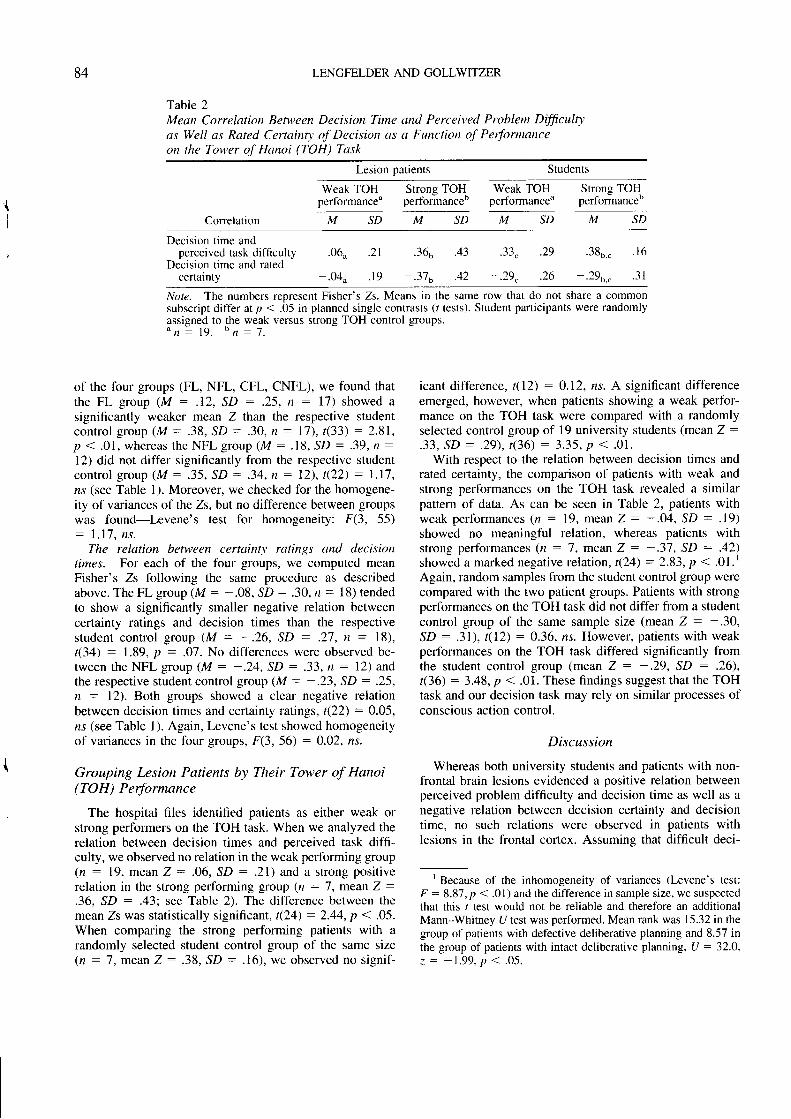
Table 2Mean Correlation Between Decision Time and Perceived Problem Dfficult1,as Well as Rated Certain1' of Decision as a Function of Performanceon the Tower of Hanoi (TOH) Task
Lesion patients Students
Weak TOH Strong TOHperformanceu performanceo
Weak TOHperformanceu
Strong TOHperformance"
Correlation M SD M S D M S D M SD
Decision time andperceived task difficulty
Decision time and ratedcenainty
'06o
-'04u
.Jor
- t q
'38o."
* r o' " b . c
. t 6
- - l I
. 21
. 1 9
.29
.26
.4J
^.\
Note. The numbers reDresent Fisher's Zs. Means in the same row that do not share a commonsubscript differ at p < .05 in planned single contrasts (r tests). Student participants were randomlyassigned to the weak versus suong TOH control groups." n : 1 9 . " n : 7 .
of the four groups (FL, NFL, CFL, CNFL), we found thatthe FL group (M - .12, SD : .25, n : 17) showed asignificantly weaker mean Z than the respective studentcontro l group (M: .38, SD: .30, r r : 1 l ) , t (33) :2.91,p < .O1 , whereas the NFL group (M : .18, SD : .39, n :
l2) did not differ significantly from the respective studentcon t ro l g roup (M : . 35 , SD : . 34 ,n :12 ) , t ( 22 ) :1 .17 ,ns (see Table 1). Moreover, we checked for the homogene-ity of variances of the Zs,but no difference between groupswas found-Levene's test for homogeneity: f(3, 55): 1 .17 , ns .
The relation between certainQ ratings and decisiontimes. For each of the four groups, we computed meanFisher's Zs following the same procedure as describedabove. The FL group (M : -.08, SD : .30, n = 18) tendedto show a significantly smaller negative relation betweencertainty ratings and decision times than the respectivestudent control group (M: -.26, SD: .21 , n : l8),t(34) : 1.89, p : .O1 . No differences were observed be-tween the NFL group (M : -.24, SD : .33, n: 12) andthe respective student control group (M : -.23, SD : .25,n : l2). Both groups showed a clear negative relationbetween decision times and certainty ratings, t(22) : 9.95,ns (see Table l). Again, Levene's test showed homogeneityof variances in the four groups, F(3, 56) : 0.02, ns.
Grouping Lesion Patients by Their Tower of Hanoi(TOH) Performance
The hospital files identified patients as either weak orstrong performers on the TOH task. When we analyzed therelation between decision times and perceived task diffi-culty, we observed no relation in the weak performing group(n : 19, mean Z : .06, SD : .21) and a strong positiverelation in the strong performing group (n : 7, mean Z :
.36, SD : .43: sec Tablc 2). Thc differcnce between thcmean Zs was statistically significant, t(24) : 2.44, p < .05.When comparing the strong performing patients with arandomly selected student control group of the same size(n:7,meanZ: .38, SD : .16) , we observed no s igni f -
icant difference, t(12) : 0.12, ns. A significant differenceemerged, however, when patients showing a weak perfbr-mance on the TOH task were compared with a randomlyselected control group of 19 university students (mean Z :
.33, SD : .29), t(36) : 3.35, p < .o1.With respect to the relation between decision times and
rated certainty, the comparison of patients with weak andstrong pedormances on the TOH task revealed a similarpattern of data. As can be seen in Table 2, patients withweak performances (rr : 19, mean Z: -.04, SD : .19)showed no meaningful relation, whereas patients withstrong performances (n : 7, mean Z : - .37, SD : .42)showed a marked negative relation, t(24) : 2.83, p < .01.'Again, random samples from the student control group werecompared with the two patient groups. Patients with strongperformances on the TOH task did not differ from a studentcontrol group of the same sample size (mean Z : -.30,
SD : .31), t(12) : 0.36, ns. However, patients with weakperformances on the TOH task differed significantly fromthe student control group (mean Z: -.29, SD: .26),t(36) : 3.48, p < .01. These findings suggest that the TOHtask and our decision task may rely on similar processes ofconscious action control.
Discussion
Whereas both university students and patients with non-frontal brain lesions evidenced a positive relation betweenperceived problem difficulty and decision time as well as anegative relation between decision certainty and decisiontime, no such rclations were observed in paticnts withlesions in the frontal cortex. Assumine that difficult deci-
t Because of the inhomogeneity of variances (Levene's test:p : 8.87, p < .01) and the difference in sample size, we suspectedthat this t test would not be reliable and therefore an additionalMann-Whitney U test was performed. Mean rank was 15.32 in thegroup of patients with defective deliberative planning and 8.57 inthe group of patients with intact deliberative planning, U : 32.0,z = - 1 . 9 9 , p < . 0 5 .
ACTION CONTROL 85
sions are commonly associated with more intensive delib-eration than are easy decisions, the lack of a relation be-tween decision time and perceived problem difficulty aswell as between decision time and lated certainty as ob-
served in the FL group suggests that these patients failed to
engage in intensive deliberation.This conclusion is supported by the lack of a relation
between perceived problem difficulty and decision time aswell as between decision certainty and decision time, par-
ticularly in those lesion patients with weak TOH perfor-mances. Patients with strong TOH performances produced apattern of results similar to a random sample of universitystudents. These findings also suggest that the mental pro-
cesses required to successfully perform the TOH task (at
least those at the early stages of performance) are similar tothe processes of conscious deliberation that precede behav-ioral choices in everyday life.
Any form of deliberation starts with the encoding ofrelevant information, and, because there is evidence fbr
encoding and retrieval deficiencies in patients with frontal
brain lesions (e.g., concerning source memory [Janowsky,Shimamura, & Squire, 19891, temporal organization ofmemory lFuster, 1989; Johnson, O'Connor' & Cantor,19911, and monitoring of encoding and retrieval [Stuss &Benson, l936l), encoding of the relevant infbrmation itselfrather than deliberation may have been impaired in thepresent study. The pattern of data, however, speaks againstthis view because patients with frontal brain lesions did notdiffer from the other groups of participants in terms of theperceived difficulty of the decision problems. Althoughpatients with frontal lesions were sensitive to the difficultylevels of the decision problems, they failed to adjust theamount of deliberation. In line with our interpretation of thepresent data, Saver and Damasio (199 l) observed that in
tasks of decision making, frontal lobe patients are not de-
ficient in the encoding and retrieval of information. Furthersupport comes from the classic findings of a dissociationbetween cognition and action in some patients with frontalbrain lesions who successfully repeat received instructionsand provide the correct verbal response but fail to produce
the respective behavior (Milner, 1963; Stuss, Alexander, &
Benson, 1997).Even though other deficiencies, such as an impaitment
in affective evaluation (Bechara, Damasio, Tranel' &Damasio, 1997;Damasio, 1995, 1997; Mesulam' 1998) andthe failure to energize oneself to form a goal commitment(Al-Adawi, Powell, & Greenwood, 1998), may contribute topoor deliberation in patients with frontal brain lesions, in-
sufficient cognitive weighing of the decision alternatives athand may be most detrimental. As Knight, Grabowecky,and Scabini (1995) have pointed out, the capability to gen-erate and evaluate counterfactuals is strongly hampered inpatients with frontal lobe lesions. Accordingly, patients withfrontal brain lesions in our study failed to become moreintensively involved with weighing pros and cons in relationto an increase in perceived difficulty of the decision prob-
lem at hand. Our data thus confirm that lesions in areas ofthe frontal lobes lead to defective deliberation. Reflectiveaction control in the sense of effbrtful goal selection seems
to rely on processes that are subsumed in the frontal lobes'
executive functions of control.
Study 2: Reflexive Action Control
Gollwitzer (1993, 1999) described how people can autom-
atize the initiation of goal-directed actions by tbrming imple-
mentation intentions. Automatic action initiation is commonly
found with habitual behaviors in which the same behavior has
repeatedly and consistently been performed in the vety same
situation. Forming implementation intentions shortcuts this
leaming process (Gollwitzer & Brandsüiner. 1997: Gollwitzer
& Schaal, 1993) by simply linking critical anticipated situa-
tional cues to the intended goaldirected behavior ("If situation
,r, arises, I will perform the goaldirected behavior :."). By
forming a decisive plan ahead of time, action control becomes
reflexive and does not require conscious deliberation once the
critical situation is encountered.Because patients with frontal brain lesions are easily
distracted by environmental cues that trigger the execution
of routine behaviors (Karnath et al., 1991)' they should
benefit from having formed implementation intentions. Fur-
thermore, not only do frontal lobe lesions seem to spare the
automatic initiation of behavior, but new habits can still be
established through classical conditioning procedures (e.g''
Daum, Channon, Polkey, & Gray, l99l; Doyon et al', 1998)
as long as the task does not require deliberative thinking or
decision making (B. Levine, Stuss, & Milberg, 1991;Pet-
rides, 1997). Thus, when patients with fiontal lobe lesions
are helped to fotm implementation intentions, the positive
.onsequences in terms of automatic action initiation shouldprevail. In other words, implementation intentions once
fbrmed should effectively control their behavior.We used a dual-task paradigm that allowed us [o assess
the immediacy and efficiency of action initiation-two vital
features of the automatic, reflexive control of action (Bargh'
1997). Immediacy was tested in a Go-NoGo task by mea-
suring the speed of a button-press response. To assess
effici-ncy, we manipulated the difficulty of the primary task(a motor tracking task), which also allowed us to observe
the speed of responses under low versus high mental load
conditions.We predicted that when implementation intentions are
formed, the initiation of the intended response should be
facilitated in all groups of participants (patients with frontal
lobe lesions, patients with nonfrontal lobe lesions, and uni-
versity students) to the same degree. Moreover, we expected
this effect to be independent of the difficulty of the com-
peting task. According to classic findings from dual-task
iesearch (Heuer, 1996), there should be less interference
between the button-press responses in the Go-NoGo task
and the competing tracking task if the button-press re-
sponses are automatically controlled by implementationintentions.
Method
Participants
Of the 34 brain-injured participants, 20 had frontal lobe lesions(8 women. 12 men) and 14 had nonfrontal lobe lesions (8

86 LENGFELDER AND COLLWITZER
women,6 men). The mean age in the FL group was 31.30 years(SD : 8.45), whereas in the NFL group, the mean age was 41.21years (SD : 14.13). For the nonclinical control group (CFL andCNFL), 33 (16 temale and 17 male) university students (meanage = 24.85 years, SD : 3.15) were randomly selected from theMax-Planck-Institute's pool of research participants.
In the FL group, lesions were due to head injury (n : 15) or tocerebrovascular disease (n = 5). Head injury (n = 4), cerebrovas-cular disease (n :7), hypoxia (n : 1), and encephali t is (n : 2)were considered to be responsible for lesions in the NFL group(see Appendix C for single case information). Again, clinical dataabout lesion location, etiology, handedness, symptoms of paraly-sis, and different measures of cognitive functioning were availablethrough the hospital's files. Patients were selected on the criteriathat eye fixation and the movement of one arm as well as therespective hand were unimpaired; the foveal visual field containedan angle of at least 8o. Furthermore, patients had to have no visualneglect and had to display intact understanding ofthe instructions.The sample contained no acute cases; 3l patients were in a chroniccondit ion.
Procedures, Equipment, and Materials
We developed a dual task that allowed for interference andtransfer. In dual-task research, interference is thought to depend onthe nature ofthe tasks involved and on the extent to which the twotasks rely on the same resources. Transfer, in contrast, occurs whenautomatic control of performance in one task frees resources thatcan then be used to improve performance in the other task (Heuer,1996; Heuer & Schmidtke, 1996). Therefore, we used structurallysimilar tasks that used the same input channel (visual perception)and the same output channel (motor reaction). Task difficulty wasvaried systematically by increasing difficulty in the primary task.Furthermore, panicipants were forced to work on both tasks si-multaneously. For this purpose, we used the same target for bothtasks. This precaution was taken because we wanted to control forpossible deficits in sustained attention (Rueckert & Grafman,1996) and to respect the fact that the ability of patients with frontalbrain lesions to perform parallel tasks is still a controversial issue(Alderman, 1996; Baddeley, Della-Sala, Papagno, & Spinnler,1997; Vilkki, Virtanen, Surma-Aho, & Servo, 1996),
Participants had to perform a dual task that combined a primarytask of tracking with a secondary Go-NoGo task. The dual taskwas presented on a computer screen. A headrest was used to keepa distance of 50 cm between the participants' eyes and the screen.The target stimulus of both tasks-a circle 1.7 cm in diameter,corresponding with the foveal visual angle of 1-2', thus providingmaximal visual acuity (Nelson & Loftus, 1980)-moved with aspeed of 3 cm/s within a delineated area (18 X 24.5 cm2) on rhescreen in randomly designed curves.
Cover story. The purpose of the study was said to be toanalyze the speed of encoding of information depicted on trafficsigns. The experimenter was allegedly interested in how fastpeople process the number "3" under distracting circumstances.
Manipulation of task dfficultv. The tracking task demandedcontinuous attention and was thus described to the participants asthe primary task. The participants had to enclose the wanderingcircle in a square (tracking field) that could be moved by perform-ing the equivalent movement with the mouse on a 52 x 65-cm:mouse pad. Before each trial (to be explained below), rhe mousehad to be retumed to a starting line. To vary the difficulty of theprimary task, the size of the tracking field was set either to 4 x 4cm' llow difficulty) or to 2.2 x 2.2 cml (high difficulty). Both ofthese squares are placed within the visual angle of 4-6'(i.e., thearea of parafoveal perception, according to Nelson & Loftus,
1980). The dependent variable in the tracking task was percentageof overlap between square and circle. It was measured at discretel-s intervals and additionally whenever the mouse button waspressed (see below).
Manipulation of intplementation intentions. The Go-NoGotask demanded only temporary attention and was thus described tothe participants as the secondary task. Participants were asked topress the mouse button immediately if a number appeared in thecircle and to forego pressing if a letter appeared (Go-NoGoparadigm). Participants were told to respond quickly and accu-rately. They were instructed to press the mouse button particularlyfäst if the number "3" appeared. This way, we established criticaltargets (i.e., the number "3"), noncritical targets (i.e., the numbers"1", "5," "7," "9"), and distractor targets (i.e., the leuers a, e, n, \x). All targets appeared three times per phase and were presentedfbr 1 s in varying intervals (2-7 s) in fixed prerandomized order(each phase consisted of three randomized sequences containingthe set of targets). Dependent variables were speed of button-pressresponses (accuracy in the range of l0 ms) and correctness of theseresponses.
Two different instructions were given to all participants tocreate implementation intention trials versus control trials; theorder of instructions was varied. Both instructions informed par-ticipants that they could accelerate their button-press responses tothe number "3" by applying cenain mental strategies. The imple-mentation intention strategy implied the following mental exercisewhile looking at the number "3" presented on a card: "Start withthe mental exercise now. Tell yourself: If the number '3' appears,I will press the button particularly fast! Tell yourself this sentencesilently a couple of times, thus fully commining yourself to thisplan." For the familiarization strategy (control instructions), par-ticipants received a sheet of paper carrying several lines of thenumber "3." At various places, the number "3" was missing, andparticipants were asked to fill in the missing "3"s in the gaps. Thefamiliarization instruction was meant to control for both effects ofpriming the number "3" and effects of experimenter demand.
Design
The participants of the four groups (FL, NFL, CFL, CNFL) wereassigned to two task conditions. In one task condition. participantsbegan to work under implementation intention instructions fol-lowed by familiarization instructions (Condition I-F). In the othertask condition, participants began to work on the dual task underfamiliarization instructions followed by implementation intenrioninstructions (Condition F-I). The two lesion groups in the two taskconditions were balanced for gender, age, handedness, IQ, prob-lem solving, Wisconsin Card Sorting Test (Grant & Berg, 1993),and TOH scores. The student control groups (CFL, CNFL)matched the clinical groups with respect to gender.
Three blocks of trials were presented. The first block consistedof practice trials in which the Go-NoGo task and the tracking taskhad to be performed separately and in combination at both levelsof difficulty. The second block contained four phases of dual-taskperformance. Each phase represented a different level of difficultyin an easy-difficult-difficult-easy (E-D-D-E) order (each phaselasted 150 s). The second block oftrials had to be performed eitherunder implementation intention instructions or familiarization in-structions. The third block again presented four phases of dual-taskperformance in an E-D-D-E order. All participants were told thatthey should now use a new strategy to speed up their responses tothe number "3." Thus, when the second block was performedunder familiarization instructions, the third block of trials wasperformed under implementation intention instructions, and viceversa.
ACTION CONTROL 87
The design used in this study was a mixed-factorial design that
consisted of two between fäctors and four within fäctors. The
between factors were group (FL, NFL, CFL, CNFL) and order of
instructions ß-I, I-F). The within factors were type of instructions(F, I), response type (critical: "3," noncritical: "1," "5," "7'" "9"),
difficulty of tracking task (E, D), and phases (E-D-D-E). As
dependent variables, we used participants' speed of button-pressresponse in the discrimination task and the percentage of overlap
in the tracking task.
Results
Performance on the Go-NoGo Task (Secondary
Task)
Overall response tintes. The speed of button-press re-
sponses of the FL group (M: 0.68 s, SD: 0.11) and theNFL group (M : 0.67 s, SD : 0.10) did not diff-er,
t(32) : 0.26, ns. The mean l'esponse times were faster in thestudentcontrol group (M : O.52 s, SD :0.05) than in the
patient group (M : 0.6'7 s, SD = 0.10), (46) : 8'10, P <
.001. Again, this difference is not surprising because thepatient group was significantly older than the student group
and may have included patients with slowed informationprocessing.
Accuracl' of discrimination. We used Rae's (1976) dis-crimination index A', ranging tiom 0 to 1.00 (from random
to accurate discrimination), to compare the hit rate and the
false-alarm rate. The discrimination index was close to 1.00
in all groups (A'",- : .97; A'*"t : .91: A'"ot : '99;A'c*"t : .99): thus discrimination can be considered to bevery accurate in all grouPs.
Speed-up effects with respect to the critical number "3-"
To assess the strength of the speed-up effects, we computeddifference scores (mean response time of the 12 noncriticalresponses minus mean response time of the 3 critical re-
sponses per phase) because such scores control for interin-dividual variance (e.g., information-processing speed). Pos-itive scores point to a faster response to the critical number"3" as compared with the noncritical numbers.
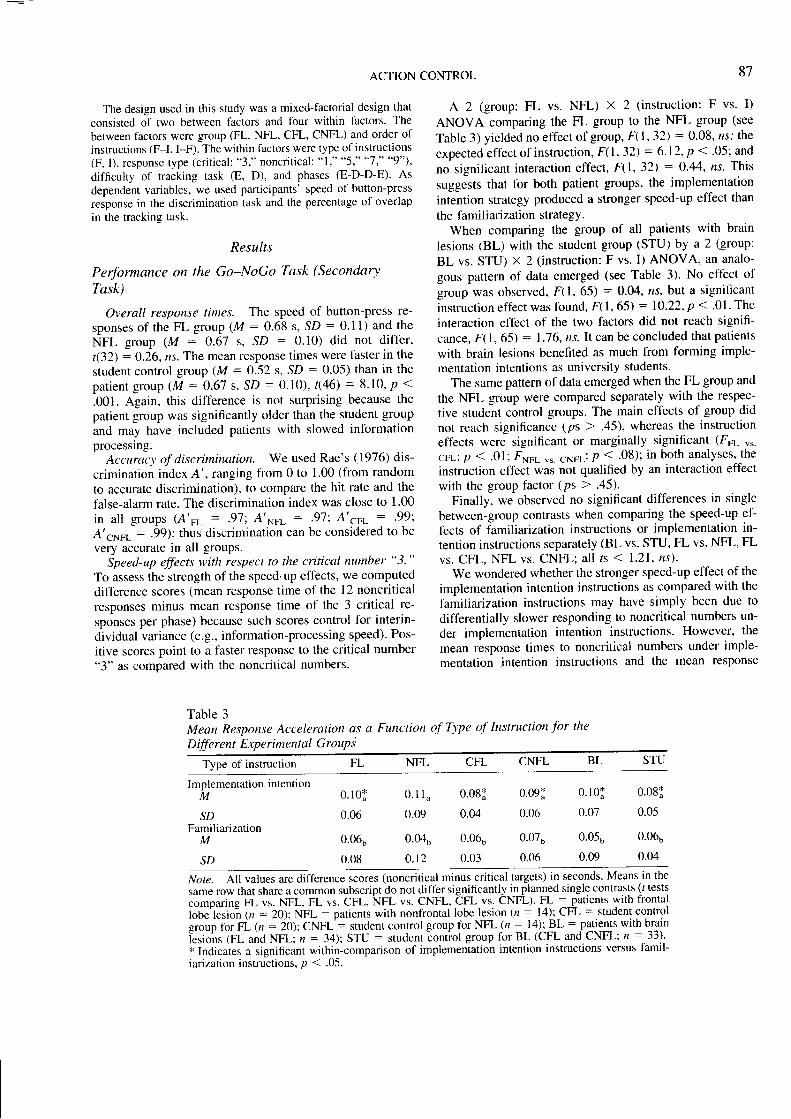
A 2 (group: FL vs. NFL) x 2 (instruction: F vs. I)
ANOVA comparing the FL group to the NFL group (see
Table 3) yielded no effect ofgroup, F(l '32) : 0.08' ns; the
expected effect of instruction, F( l. 32\ : 6'12, p < .05; and
no significant interaction effect, F(1, 32\ : 0.44' ns. This
suggests that for both patient groups, the implementation
intention strategy produced a stronger speed-up effect than
the fämiliarization strategy.When comparing the group of all patients with brain
lesions (BL) with the student group (STU) by a 2 (group:
BL vs. STU) x 2 (instruction: F vs. I) ANOVA' an analo-
gous pattern of data emerged (see Table 3). No eff'ect of
group was observed, F(1, 65) : 0.04, rts, but a significant
instruction effect was found, F( l, 65) : 10.22' p < .01' The
interaction effect of the two factors did not reach signifi-
cance, F( l, 651 : 1.76, rts. It can be concluded that patients
with brain lesions benefited as much from forming imple-mentation intentions as university students.
The same pattern of data emerged when the FL group and
the NFL group were compared separately with the respec-
tive student control groups. The main effects of group did
not reach significance (ps > .45), whereas the instruction
effects were significant or marginally significant (FFL 's.cFL'. p <.01; F*o, vs. CNFL: p < .08); in both analyses, the
instruction effect was not qualified by an interaction effect
with the group factor (Ps > .45).Finally, we observed no significant differences in single
between-group contrasts when comparing the speed-up ef-
f'ects of familiarization instructions or implementation in-
tention instructions separately (BL vs. STU, FL vs. NFL, FL
vs. CFL, NFL vs. CNFL; all rs ( l-21, ns)-We wondered whether the stronger speed-up effect of the
implementation intention instructions as compared with the
lämiliarization instructions may have simply been due to
differentially slower responding to noncritical numbers un-
der implementation intention instructions' However, the
mean response times to noncritical numbers under imple-
mentation intention instructions and the mean response
Table 3Mean Response Acceleration as a Function of T-v-pe of Instruction for the
Dffi rent Experirnental GrouP i
Type of instruction FL CFL CNFL BL STUNFL
Implementation intentionM 0.10i 0.11" 0.08* 0.09ä 0. l0 i 0 .081
SDFamiliarization
M
SD
0.06
0.06b
0.08
0.09 0.04 0.06
0.ßo 0.06b 0.07b
o.r2 0.03 0.06
0.07 0.05
0.05b 0.06b
0.09 0.04
Note. All values are difference scores (noncritical minus critical targets) in seconds. Means in the
same row that share a common subscript do not difl'er significantly in planned single conuasts (/ tests;;;p;;g FL vs. NFL, FL vs. CFL, NFL ur. CNFL, eFL vs. CNFL). FL : patients yitlt floltlllobe'lesio"n (n = 20); NFL : patients with nonfrontal lobe lesion (n : l4); CFL = student controlgioup for i t, - iö); CNFL'= srudent control group for NFL (n : la); EL
: P{igIJt with brain
iesions (FL and NFL; n = 34); STU = student iontiol group for BL (CFL and CNFL; n : 33).ilndi"ui"r a significant within-comparison of implemeniatioh intention instructions versus famil-iarization instructions, p < .05.

88 LENGFELDER AND GOLLWITZER
times to noncritical numbers under familiarization instruc-tions did not differ: STU, (32) = 1.57, ns; BL, r(33): 0.39, ns. Therefore, the stronger speed-up eff-ects inresponding to the critical numbers under implementationintention instructions cannot be attributed to less effectiveresponding to the noncritical numbers.
Order effects of instructions. Correlations between theorder of instructions 11 : Condition I-F, 2 : ConditionF-I) and the difference scores of responding to noncriticalversus critical numbers were computed to assess whetherthe implementation intention instructions would producestronger effects when they were given first or second. How-ever, the order of instructions was not critical for the dif-ference scores under implementation intention instructions(rsru : *.14, ns; rsy : -.12, ns). It can be concluded,therefore, that implementation intentions produced their ef-f-ects no matter whether they were given prior to or after thefamiliarization instructions.
Performance on the Tracking Task (Primary Task)
As expected, an increase in task difficulty led to a sig-nificant decrease in average tracking performance. The av-erage overlap of mouse field and target field in difficultphases of tracking (Msru : 82Vo, SD : 4.59; Msy : 53Vo,SD : 13.78) was significantly lower than in easy phases oftracking (Mrr,, 9l%o, SD l.M; M", 82Vo,SD : 10.77): STU, (32) : 25.84, p < .001; BL,t ( 3 3 ) : 2 8 . 4 6 , p < . 0 0 1 .
The perfbrmance measures in the tracking task couldhave been affected by the use of the dominant or thenondominant hand. However, we found no significant cor-relation between the hand used (nondominant : 0 anddominant : 1) and the amount of overlap (r : .25).
Interference Between Primary and Secondary TaskPerformance
General effects of the secondary task on the primary task.We analyzed whether the two different instructions (F vs. I)on how to perform the Go-NoGo task would affect overalltracking performance. The percentage of average overlapachieved in the tracking task was the same under both typesof instructions (all ts < | .1 1 , ns), indicating that implemen-tation intentions' stronger speed-up effects in the Go-NoGotask are neither produced at the cost of shifting attentionaway from the tracking task nor a result of a general rise invigilance.
Specific effects of the secondary task on the pimary task.The assumption that implementation intentions automatizeaction initiation implies that this process demands littlecapacity and that free capacities can be transferred to theparallel task. Whenever participants perform a critical re-sponse under implementation intention instructions, track-ing performance should be better as compared with famil-iarization instructions, particularly when the mental load ishigh (difficult tracking performance). Accordingly, we an-alyzed participants' tracking performance in the difficulttracking phases exactly at those points in time when critical
responses were performed in the secondary task. We pre-dicted better tracking performances in the difficult trackingphases when participants operated under implementationintention instructions as compared with familiarization in-structions. Indeed, we observed the expected diff-erenceswhenever critical responses were perfbrmed in phases ofdifficult tracking with lesion patients (Mt 63Vo,SD: 16 .58 ; Mp : 55Va , SD : 19 .15 ) , r ( 33 ) = 2 .21 ,p <.05, but not with university students (M1 : 85Vo, SD : 8.58;Mp:837o, SD : 11.66) , t (32) : 0.51, r ts . Because thetracking task was easier for university students-producingless mental load than in the patient group-it makes sensethat their tracking performance benefited less liom the au-tomatic action initiation in the secondary task. Finally, weobserrred that when noncritical responses had to be per-formed, no differences occurred between tracking perfbr-mances under implementation intention instructions as com-pared with familiarization instructions fbr lesion patientsand university students (all rs < 0.67, all ps > .51).
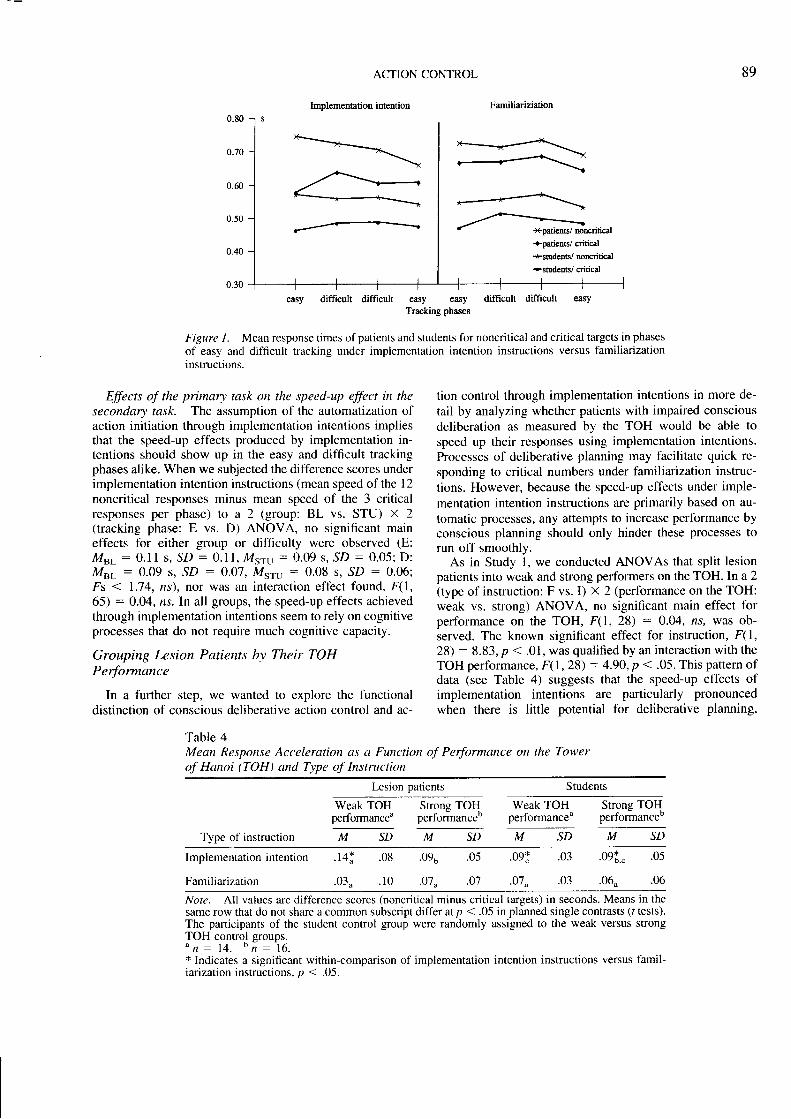
Effects of the pimary task on the secondary task. Tomake sure that the inter{erence intended by the dual-taskparadigm had actually taken place, critical and noncriticalresponses (see Figure l) were analyzed separately fbr fa-miliarization instructions and implementation intention in-structions in four 2 (group: BL vs. STU) X 4 (phase:Phase 1 to Phase 4) ANOVAs, including trend analyses forthe within-factor phase (note that the E-D-D-E order oftracking phases would lead one to expect a quadratic trendrather than a linear or other trend). Slowing effects in phasesof difficult tracking as compared with phases of easy track-ing were observed for critical and noncritical responsesunder familianzation instructions as well as for criticalresponses under implementation intention instructions(Fouuas > 5.30, ps < .05, accounting for 8-157o of vari-anCe). There were significant group differences in overallresponse times (Fs > 54.31 ,ps < .001), but no interactioneffects (Fri..-. ouuo ( 0.71, ns).
For noncriticäl responses under implementation intentioninstructions, we observed with all groups of parlicipants alinear improvement over time, F,,n"u.(1, 65) : 15.O2, p <.001, 4' : .19. Because this effect was stronger in thepat ientgroup, f i inear( I ,33) : 10.35.p < .01,4t : .24, thanin the student group, Fri..u.(I, 321 :7.46, p < .Ol. q2 :
.19, a significant interaction eff'ect was observed, Frin"u.(1,65 ) : 4 .61 .p < . 05 . n2 : .O7 .
Even though we found task interference (of the trackingtask on the Go-NoGo task) in the form of a slowing ofcritical responses after both kinds of instructions and aslowing of noncritical responses after familiarization in-structions in phases of difficult tracking, we observed thatunder implementation intention instructions, noncritical re-sponses were not affected by the difficulty of the trackingtask. The initiation of the critical responses under imple-mentation intention instructions apparently frees cognitivecapacities that can be used not only for perforrning thetracking task (see above) but also for responding to thenoncritical numbers. This present pattern of data stronglyspeaks for efficient action initiation by implementationintentions.
ACTION CONTROL
Implementation intention
89
Femiliariziation
tion control through implementation intentions in more de-tail by analyzing whether patients with impaired consciousdeliberation as measured by the TOH would be able tospeed up theil responses using implementation intentions.Processes of deliberative planning may facilitate quick re-sponding to critical numbers under familiarization instruc-tions. However, because the speed-up effects under imple-mentation intention instructions are primarily based on au-tomatic processes, any attempts to increase performance byconscious planning should only hinder these processes torun off smoothly.
As in Study 1, we conducted ANOVAs that split lesionpatients into weak and strong performers on the TOH. In a 2(type of instruction: F vs. I) x 2 (performance on the TOH:weak vs. strong) ANOVA, no significant main effect forperformance on the TOH, f(1,28) : 0.04, ns, was ob-served. The known significant effect for instruction, F(1,28) : 8.83, p < .01, was qualified by an interaction with theTOH performance, F(1, 28) : 4.99, p < .05. This pattern ofdata (see Table 4) suggests that the speed-up effects ofimplementation intentions are particularly pronouncedwhen there is little potential fbr deliberative planning,
+----- *patien6/ mrcriticäl
+patieDts/ critical
+surdilts/ rcrcritical
+students/ critical
easy difficult difficult easy easy difFtcult difficult easyTracking phases
Figure l. Mean response times ofpatients and students for noncritical and critical targets in phasesof easy and difficult tracking under implementation intention instructions versus familiarizationinstructions.
Effects of the primaD, task on the speed-up effect in thesecondary task. The assumption of the automatization ofaction initiation through implementation intentions impliesthat the speed-up eft'ects produced by implementation in-tentions should show up in the easy and difficult trackingphases alike. When we subjected the difference scores underimplementation intention instructions (mean speed of the l2noncritical responses minus mean speed of the 3 criticalresponses per phase) to a 2 (group: BL vs. STU) x 2(tracking phase: E vs. D) ANOVA, no significant maineffects for either group or difficulty were observed (E:Mer : 0.11 s, SD : 0.11, Msru : 0.09 s, SD : 0.05: D:Mst : 0.09 s, SD : 0.07, Msru : 0.08 s, SD : 0.06;Fs < 1.74, ns), nor was an interaction eft-ect found, F(1,65) : 0.04, ns. In all groups, the speed-up effects achievedthrough implementation intentions seem to rely on cognitiveprocesses that do not require much cognitive capacity.
Grouping Lesion Patients by Their TOHPerformance
In a furlher step, we wanted to explore the functionaldistinction of conscious deliberative action control and ac-
Table 4Mean Response Acceleration as a Function of Performance on the Towerof Hanoi (TOH) and Type of Instntction
Lesion patients Students
Weak TOHperformanceu
Strong TOHperformanceo
Weak TOH Strong TOHperformanceu performanceo
Type of instruction M S D SD SDMSDMM
Implementation intention
Familiarization
t A *
.03.
'o9o
.07..
.09:
.07 ^
oqr
'06u
.08
. 1 0
.03
.03
. ( , J
.o'l
.05
.06
Note. All values are difference scores (noncritical minus critical targets) in seconds. Means in thesame row that do not share a common subscript differ at p < .05 in planned single contrasts (l tests).The participants of the student control group were randomly assigned to the weak versus strongTOH control groups." n : 7 4 . " n : 1 6 .* Indicates a significant within-comparison of implementation intention instructions versus famil-iarization instructions, p < .05.

90 LENGFELDER AND GOLLWITZER
whereas the reverse is true for the speed-up effects achievedunder familiarization instructions.
Additionally, a random student sample of the respectivesize (n : 16; see Table 4) was taken and compzu'ed withpatients who had a strong performance on the TOH. Therespective 2 (type of instruction; F vs. I) X 2 (group:patients vs. students) ANOVA revealed no group maineffect, F(1, 30) : 0.18, ns,'the expected eff'ect of instruc-tion, F(I, 30) : 4.18, p < .05; and no significant interactioneffect, F(1, 30):0.27, ns, indicating that patients with astrong performance on the TOH task showed the samepattern of data as university students. A final 2 (type ofinstruction: F vs. I) X 2 (group: patients vs. students)ANOVA comparing the patients performing weakly on theTOH task to a second randomly selected student sample(n : 141' see Table 4) yielded no effect of group, F(1,26) : 9.10, ns,' a significant effect of instruction, F(1,26): lO.4O, p < .01; and a significant interaction effect,F(1,26) : 4.23, p < .05. It appears, then, that lesionpatients with weak perfbrmances on the TOH task benefitmore fiom the implementation intention instructions thaneither the university students ol those patients with strongperformances on the TOH.
Discussion
Although patients with frontal and nonfrontal brain le-sions responded slower to the target stimuli than universitystudents, all participants managed to speed up their re-sponses to critical stimuli as compared with noncriticalstimuli more by fbrming implementation intentions than byusing the familiarization strategy. Forming implementationintentions had no effect on attention or efforl in general butenhanced performance selectively whenever the critical sit-uational cue was encountered. These efl'ects of.'implemen-tation intentions cannot be explained in terms of experi-menter demand because participants showed positive differ-ence scores (i.e., faster critical than noncritical responses)under both implementation intention instructions and famil-iarization instructions.
When participants were encouraged to form implemen-tation intentions, the speed-up effect in the group ofpatientswith frontal lobe lesions was at least as strong as in all of theother groups. Apparently, the notorious stimulus depen-dence of patients with frontal brain lesions (Lhermitte,1983) appears to be of good use when it comes to quicklyinitiating responses to anticipated stimuli. When taking thelesion patients' performance on the TOH task into account,we found that patients with defective deliberation (i.e., aweak performance on the TOH) performed better underimplementation intention instructions than patients with in-tact deliberation (i.e., a strong performance on the TOH) oreven university students. Moreover, lesion patients withweak TOH performance did not show an acceleration ofbutton pressing under fämiliarization instructions. The latterobservation suggests that under lämiliarization instructions,
participants had to deliberately and reflectively build anduse strategies on their own-a function known to be im-paired in cases of tiontal lobe lesions (Burgess & Shallice,1996).
The observation that the effect of implementation inten-tions is reduced in university students and lesion patientswho are able to exert conscious behavioral control (i.e..
strong TOH performance) suggests that normal brain func-tioning provides a kind of continuous conscious metacontrolthat may, at times, interfere with automatic processes. Ob-viously, the inability to exeft conscious control is advan-tageous in tasks of leflexive action initiation, becauseconscious processing to deliberately control automaticprocesses decreases accuracy and slows pedormance(Delacour, 1995; Norman & Shall ice, 1986).
Two features of automatic processes are immediacy andefficiency (Bargh, 1997; Logan, 1992). With respect toimmediacy, implementation intentions helped to speed upcritical button-press responses. With respect to efficiency,implementation intentions reduced mental load during taskperformance in two ways: First, tracking performance wasimproved whenever a critical button-press response wasperformed in phases of difficult tracking, and second, ef-fects of practice were achieved over the four phases withrespect to noncritical responses. These findings providefurther evidence that implementation intentions create au-tomatic action control and can therefore be considered as ashortcut to establishing automatic responses that otherwiserequire extensive training. Once formed, implementationintentions seem to produce their effect on behavior inde-pendent of conscious control processes and independent ofintact frontal lobe functionine.
General Discussion
Only some aspects of planning and action control seem todepend on intact frontal lobe functioning. There is no doubtof frontal lobe participation in those aspects of action con-trol that relate to deliberating decisions. However, otheraspects of action control-namely, the automatic contlol ofintended behavior-seem independent of frontal lobefunctions.
In our two experiments, two entirely different kinds ofmental processes in action control (Gollwitzer, 1999) weretested. In Study l, we focused on conscious deliberation andtheretbre on aspects of reflective action control, whereas inStudy 2, we tried to assess processes of automatic actioninitiation and thus reflexive processes of action control. Inpatients with various frontal lesions (see Appendixes A andC), reflective action control (in terms of choosing betweenaction goals) was found to be severely hampered, whereasreflexive action control processes (i.e., action control guidedby implementation intentions) were intact.
The quality of mental processing in the experimentaltasks was, in both studies, compared with the performanceon the TOH task, as this task does (at an early stage of taskperformance) assess conscious deliberation. Splitting thepatient groups according to their performance on the TOH
ACTION CONTROL 9r
task produced inspiring results that are all the more impor-tant because some patients from the nonfrontal lobe grouphad lesions in brain areas that are considered to play a partin the dorsolateral prefrontal-subcortical circuit that pro-
vides reciprocal connections between the dorsolateral pre-
frontal cortex, the "dorsolateral portion of the caudate nu-cleus, distinct areas of the globus pallidus and substantianigra, and ventral anterior and medial nuclei of the thala-mus" (Cummings, 1995, p.2), and is claimed to be involvedin executive functions.
In Study l, patients with difliculties solving the TOH taskshowed inadequate relations of perceived difficulty andrated certainty to decision times, whereas patients withintact deliberative planning (i.e., a strong performance onthe TOH) showed a pattern similar to the student controlgroup. However, in Study 2, patients with weak TOH per-formances achieved stl'onger speed-up effects than bothpatients with strong pedbrmances and university students.We conclude that the cognitive processes underlying imple-
mentation intentions and those underlying performances onthe TOH task must be contrary in nature.
Deliberation depends on reflective conscious processesthat are involved in working memory (Baddeley, 1986;Goldman-Rakic, 1993) and related to frontal lobe function-ing (Carter et al., 1998; Saint-Cyr, Taylor, Trdpanier, &Lang, 1992). However, patients with frontal lesions are stillcapable of reflexive action control. Their behavior can be-come stimulus bound and inflexible because of an inabilityto perform acts of mental stimulation and rcality checking(Knight et al., 1995). Accordingly, the results of both of ourstudies taken together suggest that the inability to deliberatedecision outcomes is complemented with an extreme stim-ulus dependence that helps to reap the benefits of imple-mentation intentions. This pattern of dissociation was alsoobserved with the only fiontal lesion patient who, per
chance, participated in both studies. This patient performedweakly on the TOH, showed an impairment in reflectivedeliberation (Study l), but successfully managed to speedup critical responses under implementation intention in-structions (Study 2). Although the two studies presented donot allow us to determine a double dissociation of brainareas, we still observed a double dissociation of brainfunctioning.
From our data, we can determine neither which parts ofthe frontal lobes are particularly related to deliberation norwhich parts of the nonfrontal brain are related to actioncontrol on the basis of implementation intentions. However,in post hoc analyses, we focused on the perfbrmance ofthose patients with frontal brain lesions who had lesions inthe dorsolateral frontal lobes, which are considered to becentral for processes related to executive functioning (Cum-mings, 1995; Petrides, 1995; Stuss & Benson, 1986).Study I contained 7 patients with dorsolateral liontal lobedamage (see Appendix A). According to the argument de-veloped above, they should show deficits in deliberation.Indeed, all of them showed weak positive corelations be-tween problem difficulty and decision time as well as weaknegative conelations between tated decision cerlainty anddecision time. In Study 2, 4 of the 5 patients with dorsolat-
eral frontal lesions (see Appendix C) could improve their
performance under implementation intention instructions as
compared with familiarization instructions, whereas the 5thpatient, who had additional damage to areas in the parietal
cofiex, was unable to speed up his responses. Again, these
observations would support the above cited notion that
dorsolateral frontal functioning is essential in consciousprocesses ofaction control but is not a necessary component
of action initiation through implementation intentions.
Our data cannot resolve the issue of the location or
pathways of the functional systems in the brain that are
responsible for the effects of implementation intentions. To
answer this question, neuroimaging studies with healthy
volunteers need to be conducted as well as lesion studies
that focus exactly on those parts of the brain kaown to be
related to automatic behaviors. The basal ganglia' especially
the striatum and the head of the nucleus caudatus, seem to
be involved with the execution of routine behavioral pro-
grams (Knopman & Nissen, 1991: Partiot et al., 1996) and
with associative habit leaming (Knowlton, Mangels, &
Squire, 1996). Moreover, cerebellar functions are basic fea-tures of classical conditioning (Daum et al., 1993), and inparietal brain areas, sensoric input and automatic output arethought to be closely related (Brody & Pribram, 1978;Snyder, Batista, & Andersen, 1997).
Finally, our findings have important implications for re-
habilitation and therapy in patients with frontal lobe lesions.Commonly, new routines are developed in patients withfrontal lobe lesions through extensive practice (Schmitter-
Edgecombe & Rogers, 1997). According to the results ofour second study, such routines could also be establishedsimply by forming implementation intentions' This way ofshoftcutting the otherwise lengthy process of habit fbrma-tion is an economical and very effective self-regulatory toolfor organizing one's everyday conduct (Gollwitzer, 1999).Therefore, next to classic instruments of behavior therapy(e.g., Becker & Vakil, 1993; Hux, Reid, & Lugen, 1994;Sohlberg, Mateer, & Stuss, 1993), the strategy of formingimplementation intentions could be offered to patients with
frontal brain lesions to help them organize their dailyactivities.
References
Al-Adawi. S.. Powell. J. H., & Greenwood, R. J. (1998). Motiva-tional deficits after brain injury: A neuropsychological approachusing new assessment techniques. Neuropstchologt' 12, ll5-124.
Alderman, N. (1996). Central executive deficit and response tooperant conditioning methods. Neuropstchological Rehabilita-tion.6. 161-186.
Baddeley, A. (1986). Working memory. Oxford, England: OxfordUniversity Press.
Baddeley, A., Della-Sala, S., Papagno, C., & Spinnler' H. (1997).Dual-task performance in dysexecutive and nondysexecutivepatients with a frontal lesion. Neurops,-cholog,-, I l' l8'7-194.
Bargh, J. A. (1997). The automaticity of everyday life. In R' S.Wyer (Ed.), Advances in social cognition (Vol. 10, pp. l-48).Mahwah. NJ: Erlbaum.
92 LENGFELDER AND GOLLWITZER
Bechara, A., Damasio, A. R., Damasio, H., & Anderson, S. W.(1994). Insensitivity to future consequences following damageto human prefrontal cortex. Cognition, 50, 7-15.
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997,
February 28). Deciding advantageously before knowing theadvantageous strategy. Science, 275, 1293-1295.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1986).Kognitive therapie der depression [Cognitive therapy ofdepres-sion]. München, Germany: PVU/Urban und Schwarzenberg.
Beck, A. T., & Steer, R. A. (1987). Beck Depression Inventory,-manual. San Antonio, TX: Psychological Corporation.
Becker, M. E., & Vakil, E. (1993). Behavioural psychotherapy ofthe frontal-lobe-injured patient in an outpatienr setting. BrainInjury, 7,515-523.
Brody, B. A., & Pribram, K. H. (1978). The role of frontal andparietal cortex in cognitive processing. Tests of spatial andsequence functions. Brain, I 01, 60'l-633.
Burgess, P. W., & Shallice, T. (1996). Response suppression.initiation and strategy use following frontal lobe lesion. Neuro-p s -,-c ho I o gia, 3 4, 263-27 3.
Carter, C. S., Braver, T. S., Barch, D. M., Botvinick, M. M., Noll,D., & Cohen, J. D. (1998, May 1). Anterior cingulate cortex,error detection, and the online monitoring of performance. ,Scl-ence. 280.747-749.
Cockburn, J. (1995). Task intemrption in prospective memory: Afrontal lobe function? Correx. 31.87-97.
Coolidge, F. L., & Griego, J. A. (1995). Executive functions of thefrontal lobes: Psychometric properties of a self-rating scale.P s _,- c ho lo gic a I Report s, 77, 24 -26.
Cummings, J. L. (1995). Anatomic and behavioral aspects offrontal-subcortical circuits. In J. Grafman, K.-J. Holyoak, & F.Boller (Eds.), Structure and functions of the human prefrontalcortex (pp. 1-13). New York: New York Academy of Sciences.
Damasio, A. R. (1985). The frontal lobes. In K. M. Heilmann & E.Valenstein (Eds.), Clinical neurops,-cholo$ (pp. 339 -375).
New York: Oxford University Press.Damasio, A. R. (1995). On some functions of the human prefrontal
cortex. In J. Grafman, K.-J. Holyoak, & F. Boller (Eds.), Slruc-ture and functions of the human prefrontal cortex (pp. 24I-251). New York: New York Academy of Sciences.
Damasio, A. R. (1997, Apil 24). Towards a neuropathology ofemotion and mood. Nature, 386, 769-770.
Damasio, A. R., Tranel, D., & Damasio, H. C. (1991). Somaticmarkers and the guidance of behavior: Theory and preliminarytesting. In H. S. Levin, H. M. Eisenberg, & A. L. Benton (Eds.),Frontal lobe function and d,-sfunction (pp. 218-229). NewYork: Oxford University Press.
Daum, I., Ackermann, H., Schugens, M. M., Reimold, C., Dich-gans, J., & Birbaumer, N. ( 1993). The cerebellum and cognitivefunctions in humans. Behavioral Neuroscience, 107, 4ll-419.
Daum, I. , Channon, S., Polkey, C. 8., & Gray, J. A. (1991).Classical conditioning after temporal lobe lesions in man: Im-pairment in conditional discrimination. Behavioral Neuro-science. 105.396-408.
Decary, A., & Richer, F. (1995). Response selection deficits infrontal excisions. Neurop st chologia, 3 3, 1243-1253.
Delacour, J. (1995). An introduction to the biology of conscious-ness. Neurops-vcholo gia, 3 3, 1061 -10'7 4.
Della Malva, C. L., Stuss, D. T., D'Alton, J., & Wil lmer, J. (1993).Capture errors and sequencing after liontal brain lesions. Nea-ropstchologia, 3 1, 363-372.
Doyon, J., Laforce, R., Jr., Bouchard, G., Gaudreau, D., Roy, J.,Poirier, M., B6dard, P. J., B6dard, F., & Bouchard, J.-P. (1998).Role of the striatum, cerebellum and frontal lobes in the autom-
atization of a repeated visuomotor sequence of movements.Nettropstchologia, 36, 625-641.
Eslinger, P. J., & Damasio, A. R. (1985). Severe disturbance ofhigher cognition after bilateral frontal lobe ablation: PatientEYR. Neurolog,", 35, 1731-1741.
Fukui, T., Hasegawa, Y., Sugita, K., & Tsukagoshi, H. (1993).
Utilization behavior and concomitant motor neglect by bilateralfrontal lobe damage. European Neurolog:,,, 33, 325-330.
Fuster, J. M. (1989). The prefrontal cortex. Anatonn, phlsiologtand nettropsycltolog,- of the frontal /oäe. New York: RavenPress.
Goel, V., & Grafman, J. (1995). Are the frontal lobes implicated in"planning" functions? Interpreting data from the Tower ofHanoi. Neuropsrchologia, 3 3, 623- 642.
Goldman-Rakic, P. S. (1993). Specification of higher conicalfunctions. Journal of Head Trauma Rehabilitation, 8, 13-23.
Gollwitzer, P. M. (1990). Action phases and mind-sets. In E. T.Higgins & R. M. Sorrentino (Eds.), Handbook of motivation andsocial cognition: Foundations of social behavior (Vol. 2, pp.53-9D. New York: Guilford Press.
Gollwitzer. P. M. (1993). Goal achievement: The role of inten-tions. In W. Stroebe & M. Hewstone (Eds.), European review ofsocial psycholoS.r (Vol. 4, pp. l4l-185). London: Wiley.
Gollwitzer, P. M. (1999). Implementation intentions and effectivegoal pursuit: Strong effects of simple plans. American Pstchol-ogist, 54, 493-503.
Gollwitzer, P. M., & Brandstätter, V. (1997). Implementationintentions and effective goal pursuit. Journal of Personalit-"\ andSocial Ps,-chologt, 73, 186-199.
Gollwitzer, P. M., & Schaal, B. (1998). Metacognition in action:The importance of implementation intentions. Personalih' andSocial Psychologr Review, 2, 124-136.
Grant, D. A., & Berg, E. A. (1993). Wisconsin Card Sorting Test(WCST). Göttingen, Germany: Hogrefe.
Grattan, L. M., & Eslinger, P. J. (1991). Frontal lobe damage inchildren and adults: A comparative review. Developmental Neu-rop st c ho lo gt, 7, 283 -326.
Harlow, J. M. (1993). Recovery from the passage of an iron barthrough the head. History of Ps1:chiatn, 4, 271-281. (Originalwork published 1896)
Heckhausen, H. (1991). Motivation and volition. Heidelberg, Ger-many: Springer-Verlag.
Heckhausen, H., & Gollwitzer, P. M. (1987). Thought contents andcognitive functioning in motivational versus volitional states ofmind. Motivation and Emotion. I 1. 101-120.
Heuer, H. (1996). Dual-task performance. In O. Neumann & A. F.Sanders (Eds.), Handbook of perception and action, Vol. 3:Attention (pp. 113-153). London: Academic Press.
Heuer, H., & Schmidtke, V. (1996). Secondary-task effects onsequence learning. P st:cltological Re search, 59, 1 19 -133.
Hux, K., Reid, R., & Lugert, M. (1994). Self-instruction trainingfolfowing neurological injury. Applied Cognitive Pstchologt, 8,259-271.
Janowsky, J. S., Shimamura, A. P., & Squire, L. R. (1989). Sourcememory impairment. Neurops -vc hologia, 27, I 043-1056.
Jeannerod, M. (1997). The cognitive neuroscience of action. Cam-bridge, MA: Blackwell Publishers.
Johnson, M. K., O'Connor, M., & Cantor, J. (1997). Confabula-tion, memory deficits, and frontal dysfunction. Brain and Cog-nit ion. 34.189-206.
Kamath, H.-O., Wallesch, C. W., & Zimmermann, P. (1991).Mental planning and anticipatory processes with acute and
93ACTION CONTROL
chronic frontal lobe lesions: A comparison of maze performance
in routine and non-routine situations. Neuropsychologia, 29'
271-290.Knight, R. T., Grabowecky, M. F., & Scabini, D. (1995). Role of
human prefrontal cortex in attention control. In H. H. Jasper, S'
Riggio, & P. S. Goldman-Rakic (Eds.)' Epilepsy and the Jünc-tional anatonn of the frontal lobe (pp. 2l-36). New York:
Raven Press.Knopman, D., & Nissen, M. J. (1991). Procedural learning is
impaired in Huntington's disease: Evidence from the serial
reaction time task. Ne uropst chologia, 29, 245-254.
Knowlton, B. J., Mangels, J' A., & Squire, L. R. (1996' September
6). A neosriatal learning system in humans. Science, 273,
1399-1402.Konow, A., & Pribram, K. H. (1970). Error recognition and
utilization produced by injury to the frontal cortex in man'
Neuropstchologia, 8, 489 -49I.
Kotovsky, K., Hayes, J. R., & Simon, H. A' (1985). Why are some
problems hard? Evidence from Tower of Hanoi. Cognitive Ps.r�''
cholog,-, 17, 248-294.Levin, H. S., Goldstein, F. C., Wil l iams, D. H., & Eisenberg'
H. M. (1991). The contr ibution of frontal lobe lesions to the
neurobehavioral outcome of closed head injury. In H' S'
Levin, H. M. Eisenberg, & A. L. Benton (Eds.), Frontal lobe
function and dtsfunction (pp.318-338). New York: Oxford
University Press.Levine. B., Stuss, D. T., & Milberg, W. P. ( 1997). Effects of aging
on conditional associative learning: Process analyses and com-
parison with focal frontal lesions. Neuropst:chologt, l,1,367-
3 8 1 .Levine, D. S., Leven, S. J., & Prueitt, P' S. (1992). lntegration,
disintegration and the frontal lobes. In D. S. Levine & S' J'
Leven (Eds.), Motivation, emotion, and goal directiott in neural
networks (pp. 301-335). Hillsdale, NJ: Erlbaum.
Lhermitte, F. (1983). "Utilization behaviour" and its relation to
lesions of the frontal lobes. Brain, 106,23'l-255.
Lhermitte. F. (1986). Human autonomy and the frontal lobes. Part
II: Patient behavior in complex and social situations: The "en-
vironmental dependency syndrome." Annals of Neurolog,-, 19,
33s-343.Lhermitte. F., Pillon, 8., & Serdaru, M. (1986). Human autonomy
and the frontal lobes. Part I: Imitation and utilization behavior:
A neuropsychological study of 75 patients. Annals of Neurol-
ogy, 19,326-334.Logan, G. D. (1992). Attention and preattention in theories of
automaticity. The American Journal of Psychologt' 105' 3l'7-
339.Luria, A. R. (1962). Higher cortical functions in man' New York:
Basic Books.Luria. A. R. (1973). The frontal lobes and the regulation of
behavior. In K. H. Pribram & A. R. Luria (Eds.), Ps,-chophts-
iolog, of the frontal lobes (pp. 3-26). New York: Academic
Press.Mann, L., & Taylor, V. A. (1970). The effects of commitment and
choice difficulty on predecision processes. The Journal ofSocial
P stcholo 91,, 82, 221 -230.
McAndrews. M. P., & Milner, B. (1991). The frontal cortex and
memory for temporal order. Neurop st:cholo gia' 29, 849 -859'
Mesulam. M.-M. (1998). From sensation to cognition. Brain, 12l'
l 013-1052.Milner. B. (1963). Effects of different brain lesions on card sort-
ing. Archives of Neurolog'-, q 100-ll0'
Milner, 8., Petrides, M., & Smith, M. L. (1985)' Frontal lobes and
the temporal organization of memory. Human Neurobiolog" 4'
137-142.Morris, R. G., Ahmed, S., Syed, G. M., & Toone, B' K' (1993)'
Neural correlates of planning ability: Frontal lobe activation
during the Tower ofLondon test' Neuropstchologia, 31,1367-
I 378.Nelson, W. W., & Loftus, G. R. (1980). The functional visual field
during picture viewing. Journal of Experinental Pstchologt':
Human Learning and Memory, 6,391-399'
Norman, D. A., & Shallice, T. (1986). Attention to action' Willed
and automatic control of behavior. In R. J' Davidson' G' E'
Schwartz, & D. Shapiro (Eds.), Consciousness and self'regula'
tion. Arlvances in research and theory (Vol' 4, pp' l-18)' New
York: Plenum Press.Owen, A. M., Downes, J. J., Sahakian, B. J', Polkey, C' E" &
Robbins, T. W. (1990). Planning and spatial working memory
following frontal lobe lesions in man- Neuropst'chologia' 28'
102r-1034.Owen, A. M., Doyon, J., Dagher, J.' Sadikot, A', & Evans, A' C'
(1998). Abnormal basal ganglia outflow in Parkinson's disease
identified with PET. Implications for higher cortical functions'
Brain, 121,949-965.Partiot. A.. Vdrin, M., Pillon,8., Teixeira-Ferreira, C" Agid' Y'' &
Dubois, B. (1996). Delayed response tasks in basal ganglia
lesions in man: Further evidence for a striatofrontal cooperation
in behavioural adaptation. N europsvcholo gia, 34, 7 09 -7 2l'
Peterson, D. K., & Piiz, G. F. (1988). Confidence, uncertainty, and
the use of information - Journal of Experimental Psychologt:
Learning, Memor,', and Cognition' 14' 85-92'
Petrides. V. ttSSSl. Functional organization of the human frontal
cortex for mnemonic processing. Evidence from neuroimaging
studies. In J. Grafman, K'-J' Holyoak, & F' Boller (Eds')'
Structure and functions of the human prefrontal cortex (pp'
35-96). New York: New York Academy of Sciences'
Petrides, M. (1997). Visuo-motor conditional associative leaming
after frontal and temporal lesions in the human bratn' Neuro-
pstchologia, 3 5, 989 -997 -
Peirides. M., & Milne., B. (1932). Deficits on subject-ordered
tasks after frontal- and temporal-lobe lesions in man' Neuropst''
chologia, 20. 249-262.Pietromönaco, P., & Rook, K' (1987). Decision style in depres-
sion: The contribution of perceived risks versus benelits' Joar-
nal of Personalin* and Social Psychologt, 52, 399-408'
Pribram, K. H. (1937). The subdivisions of the frontal cortex
revisited. In E. Perecman (Ed.), The frontal lobes revisited (pp'
1l-39). New York: IRBN Press.Pribram, K. H., & Tubbs, W. E. (1967, June 30)' Short-term
memory, parsing, and the primate frontal cortex' Science, 156,
1765-1767.Radloff, L. S. (1977). The CES-D scale: A self-report depression
scale for research in the general population' Applied Psvcholog-
ical Measurement, 1, 385-401.Rae. G. (1976). Table of A'. Perceptual and Motor Skills, 42' 98'
Reason, J. (1987). The psychology of mistakes: A brief review of
planning failures. In J. Rasmussen, K. Duncan, & J' Leplat
iear.), lr"t rcchnolotu- and human error (pp.45-52)' Chiches-
ter, England: Wiley.Rezai, K.lAndreasen, N. C., Alliger, R.' Cohen, G', Swayze, V', &
O'Leary, D. S. (1993). The neuropsychology of the prefrontal
coftex. Archives of Neurologt, 50, 636-642'
Rueckert. L., & Grafman, J. (1996). Sustained attention deficits in
patients with right frontal lesions ' Neuropstchologia, 34' 953-
963.

94 LENGFELDER AND GOLLWITZER
SainrCyr, J. A., Taylor, A. 8., & Lang, A. E. (1988). Procedurallearning and neostriatal dysfunction in man. Brain, I I l, 941-959.
Saint-Cyr, J. A., Taylor, A. E., Trdpanier, L. L., & Lang, A. E.(1992). The caudate nucleus: Head ganglion on the habitsystem. In G. Val lar, S. F. Cappa, & C.-W. Wallesch (Eds.),Neuropsttchological disorders associated v,itlt subcorticallesions (pp. 204-226). Oxford, England: Oxford UniversityPress.
Saver, J. L., & Damasio, A. R. (1991). Preserved access andprocessing of social knowledge in a patient with acquired soci-opathy due to ventromedial frontal damage. Neuropst'cholo-gia,29, 1241-1249.
Schmitter-Edgecombe, M., & Rogers, W. A. (1997). Automaticprocess devefopment following closed head injury. Neuropst,-chologt', I 1,296-308.
Shallice, T. (1988). From neuropst:chologl'to mental stucture.New York: Cambridge University Press.
Shallice, T., & Burgess, P. W. (1991). Higher-order cognitiveimpairments and frontal lobe lesions in man. In H. S. Levin,H. M. Eisenberg, & A. L. Benton (Eds.), Frontal lobe functionand dtsfunction (pp. 125-138). New York: Oxford UniversityPress.
Shallice, T., Burgess, P. W., Schon, F., & Baxter, D. M. (1989).The origins of utilization behaviour. Brain, I 12, 1587-1598.
Simon, H. A. (19'75). The functional equivalence of problemsolving skills. Cognitive Ps,-chologt,, 7, 268-288.
Snyder, L. H., Batista, A. P., & Andersen, R. A. (1997, March l3).Coding ofintention in the posterior parietal conex. Nature, 386,t6' t-170.
Sohlberg, M. M., Mateer, C. 4., & Stuss, D. T. (1993). Contem-porary approaches to the management of executive controldysfunction. Journal of Heatl Trauma Rehabilitation, 8, 45-58.
Stuss, D. T., Alexander, M. P., & Benson, D. F. (1997). Frontallobe functions. In M. R. Trimble & J. L. Cummings (Eds.),Contemporan behavioral neurologl, (pp. 169-187). Boston:Butterworth-Heinemann.
Stuss, D. T., & Benson, D. F. ( 1986). Tlte frontal /obes. New York:Raven Press.
Tranel, D., Anderson, S. W., & Benton, A. (1994). Developmentof the concept of "executive function" and its relationship to thefrontal lobes. In F. Boller & J. Grafman (Eds.), Handbook ofnettropst'cholog.r (Vol. 9, pp. 125-148). Amsterdam: ElsevierScience.
Vilkki, J., Virtanen, S., Surma-Aho, O., & Servo, A. (1996). Dualtask performance after focal cerebral lesions and closed headinjuries. Neuropstchologia, 34, l05l-1056.
von Cramon, D. Y., & Matthes-von Cramon, G. (1994). Back towork with a chronic dysexecutive syndrome? (A case report).Neurops n-chological Rehabilitation, 4, 399 -417 .
Wiegersma, S., van der Scheer, 8., & Hijman, R. (1990). Subjec-tive ordering, short-term memory, and the frontal lobes. Neuro-pst'chologi<t. 28, 95-98.
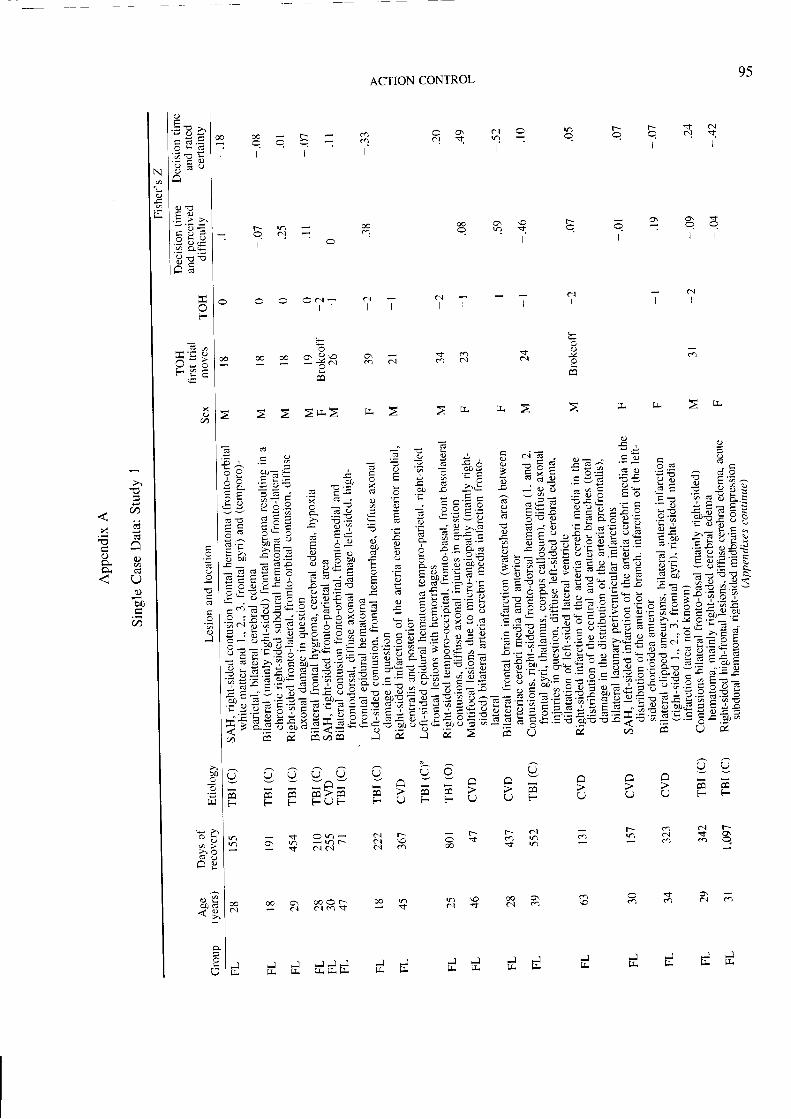
95
q ? € E ä { }r l l
@ o 9 t r = 5 2 XE n i q q - q
l l l l
ACTION CONTROL
a.t v
t c a6 0.1
o o 9 = F = 2--:l l l l
r n c .' : a c l - : c 1t -
c.lI
ö.1 c.)
Jl a
I(\{I
F.
0
I
va l
t!
T T T i
o o t
O Oc ' . | -l 1
f
ü o, !?\o- z c \
*! äEä äiäi* älEt,eiftEE Eg trigl€äEE,€;iE,Ej"=,?t*'l:ä212fli{!!!tE,ff'Efi FzZitf'l:EEEi:+zZ?tlZZEEEzEziEiliE*******************************************************************************************ä?EraeTi;z1E:E1=,aElz=EEZ*=r*ZiEZtEEiETiZlTlE;:äi:fä:€sjä:€F?#;,ä,,i4,!zT;2iEit!ä,äE'ceeEiEeEe€3EE.E
d
v x= F
o - -
t r >o a
F
O :
- Y Oc =
- 4 0 . ,
l ' ! 3l < .t v )
U UA N
; ' ' F FFv v
r-- o qt F'; V . d $ o= : i ö m o .
- v Ä Cg Y Y ^ ^ =
F 7 E E - ' PF l , / F - v
r r r q tä ' ' c a t m v 'ä ö & $ n
U O U U- a -
t r F F ' ,FF F F V -
O
F
dl
* O n -g S F K -
v) \oa.r S
@ o \a] o
JrJ.
@al
O
J JlL q.J - l
lL trJ Jlr tLd d d d d d d
(). = ! >
a - Q \ :':: tr :'/o - -
. = > > r
'; äts
F
! L y^ - a
€
Xo
a
I
J
- o
> oA H
0 0 6
N
C)
l f
x i 5= c d
o " ,o. Y,6 =
c)b0
ö
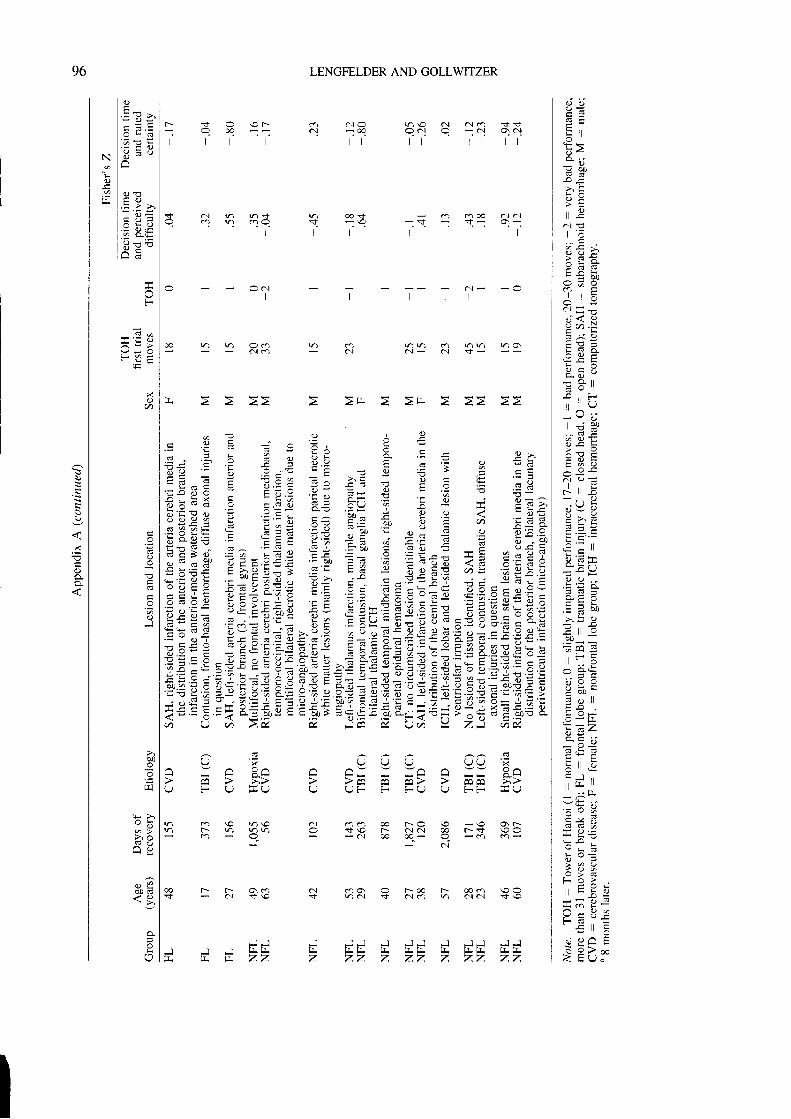
LENGFELDER AND GOLLWITZER
o o
E >9 i l
ä :> , E> E. O
a l E
r + > .> q 5 ;
= a Y
a ] | r -. i ? üo 7 ) . :
E v =l = =ä ö =
ä t o
! ii F-'i l \ J
_ - o
a C J E- o s !
6 q Et d q
a . l e =
- , , I
O - : iI > - t= ! L
o ' - t l
9 F T E* = r )
x : i
. - d - "
> . ! E
. : : J - -
z c a E, . ' . :
^ o €. - = =! ? Y :
: 9 r l
o ö
6 , F 6
F l l . ö
l l E '- ; I r
E : 3F O . -: * F -o
- v -
'^ ..) q
L - >L = ^ . '
r r r X E- - ; cI 6 i -o - y , 2F - A - =
o" ' o A t r
5 F > ;( t r L r c
ca c l o n \O 6 l ö . l ca tSc . l - : oq qc l q - c l q . l
l r t t r r l l
t--- * O \Ot-r
t t t t l
I c . l n nd n oo$ o ooo ö .1 a iO c a n m C $ - \ o - S < ' - o \ -
l r r r l
C d ^ c 3
O ' I U U U U U ' i^ A c ^ A - - - A A o ^=- =-U F U E U U U F F F U U F F E U
v) 6 \o r)\o ö] 60 00 tr-o \or) F- r) r)r) O sf,\O F- C!C'n @c . 3 - . r o o 3 - 3
c i - - O
caal
r )v ) c i r ) r ) r )o \C i - a n < - -
> E
- \ O O . F -t = s \ o o- c a c a -
o O \ O t ' - o o F @ m \ O Or ) a j $ ö . 1 6 v ) o n ö l $ \ o
- ^ l
I
n r) Oc'ro.l o
F- t.- O\ dlöl .tr \o
F I J
t r E Z ZJ J J J J
z z z z z. ] J J J
z z z z
I
; , . ä E E ; E c F ; € , € ?i i , E ' ' E E i " E : E E i E i = E * ,zE+: E E7'z ää iä F .E E t ;:Esäs ; E , : :E € : äs g FE_5 = 'E ,9 rä:=€€ iz,EiE=: *; 1c f iEEi ' , i i :g€i€EgE iEEägE ;E Eg=EI;;::=EIEE{EE€€ :$ E:E :äi": g i ! ! ; :EE;; ä!: iE iäEIEEE t ; ; t E E rä i a= c; € i E i EIEigää! E €: : ! = + : zE != "=ü ! : i ax i ; I E ? :EeE l j zä : iE i= E = = s i Z Z f ' s E E ä ; E + E = ä 8 4 + € j e : + ä E ä € 8 -ö ü ö >'&, t, i i fr E, uü Y Zi ä&,
J
z
Ns
J
z
I c.>
l . = 9 > '
l @ - O !l ' ; 1 c ! ?
N l ö s "j " l -o l
r l . E 9 *l - - q =t a Y -
t ; E ü
F
=^ - >V o O
xV)
o
r-
oJ
ooEr r l
- o
> r öq o
n o
c ; 9ö o d
O
96
€
g
x
q.)
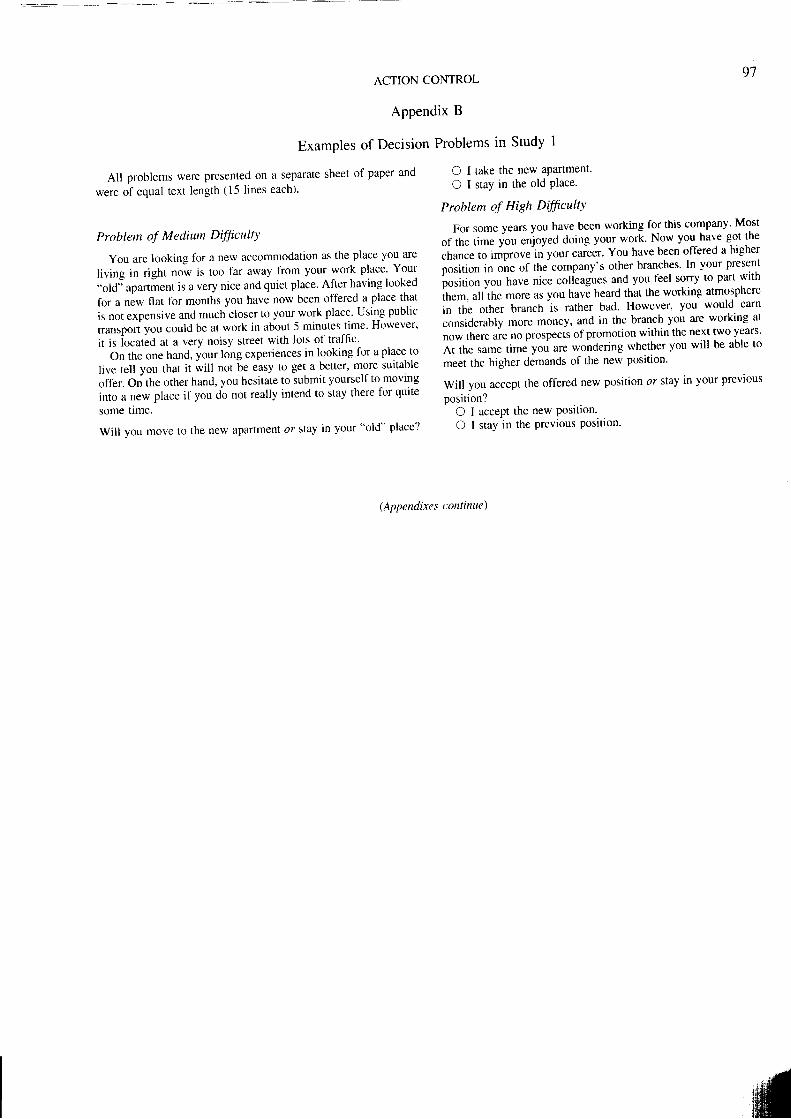
9'�7ACTION CONTROL
APPendix B
Examples of Decision Problems in Study I
All problems were presented on a separate sheet of paper and
were of equal text length (15 lines each)'
Problem of Mediutn Dfficul4'
You are looking fbr a new accommodation as the place you are
living in right now is too far away from your work place' Your"old'; apartÄent is a very nice and quiet place' Af'ter having looked
for a new flat for months you have now been offered a place that
is not expensive and much closer to your work place' Using public
t.unrpoi you could be at work in about 5 minutes time' However'
it is iocatäd at a very noisy sffeet with lots of traffic'
On the one hand, your long experiences in looking for a place to
live tetl you that it will not be easy to get a better' more suitable
offe.. On ttte other hand, you hesitate to submit yourself to moving
into u n.* place if you do not really intend to stay there for quite
some time.
Will you move to the new apartment or stay in your "old" place?
O I take the new apartment.
O I stay in the old Place.
Problem of High Dfficult"t
For some years you have been working for this company' Most
"f ;; ;;. ;", enjoyed doing your work' Now you ha'e got the
chance to improve-in yout ca.ei.. You have been offered a higher
oosition in one of the company's other branches' In vour present
;;;i;;; uoo ttuu. nice colieagues and you feel sorry to part with
ih.* urrirt. more as you have heard that the working atmosphere
in tfre otirer branch is rather bad' However, you would eam
considerably more money, and in the branch you are working at
now there aie no prospects of promotion within the next two years'
At the same time you are wondering whether you will be able to
meet the higher demands of the new posit ion'
Will you accept the off'ered new position or stay in your previous
posit ion?O I accePt the new Posltlon.O I stay in the Previous Posit ion'
(Appendixes continue)
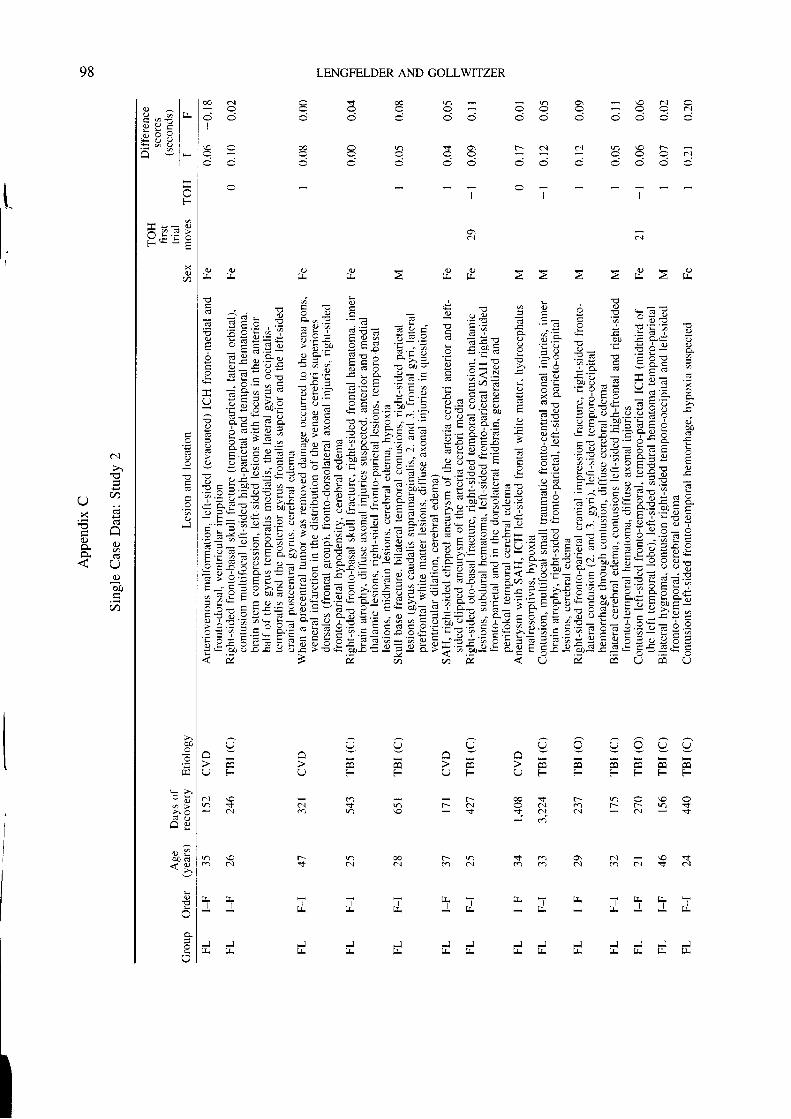
r ) o \ \ O a . l C
; - i
t-- c'.1 al Vl \O f-
o d o o v l
@ o r ) t o \
LENGFELDER AND GOLLWITZER
cl
O O
T , lJ IJ.
J JIL IJ.
00 a.l
I
I
&
C ) ! ( )z t l z l l
t T ' i ltt ,..r. + lr
I J J J
ot l
t EEE=E?ziEurciz; El- ä i=-E-7EEEäE =E3:ä i !+ i
i ää!iä Et=EE{,Ia:Ei,Eää iäi äc,ä Eää EEEZZzEu*iErlTzz|+ü.;:s€:;;'jäi:il{iE--ü e ä F e E i = ä ; i E ! ?E€+Izi i;;=titt Ei ;1_T Ei=zel ==iz;;i,zEiz5| 7;g ; I ; T;ig;E;=|!| =EE .E;? E E Ei ;= zE i ; ; ; g ä ä P : äE ; + s sv Eä E= FF: IZ;:=EEi?1EIä= äi i€ Ei ä€iEtitii;E= äii g ;eE;g;äE ä ä;iiuu= E E= EEälE E;fei +aa;: _ ä : = E c € ä g E ; E ! g r = i 9 = i : F ; ; F ; : F : g 3 ; t g U E : : ä E ;0 : € ' ; ; ' r X = o = !
E E ä E E ; ä E :r = EäF! ; ! ääE ;' a' gä ä€ E : ä äE E g E E i E E E
2 2 ,
$ . iM O
' i l,t tL
J J
c ) c )t r E
l+ t+t t
J J
U U O O O U O U Q^ A ^
U F F U F ( J F F F F F F
c i F - c o < . F - r ) O \ o Oa.l sf v) r- c.l c c.l ca t-- F- v) t6 h \ o v n q . i ö i $
-
C)
U F
cl \on v
ci
O \ ö l \ o dö l o a l $ c ' l
@ F - r )d o N
r ) \ oo ö l
J
- lu. Itr
r ^ lO o I L L
E ü : It ö 9 1E 3 ü lx q l'-.,t
-F
* = = v
0a
I
(.)J
äo
p
h ä- o
> öA : . i
ö 0 ( €< 9 ,
!
(,
98
ö.1
>l
(t
x g
tr l-.'l(,)o ö
ooo
a
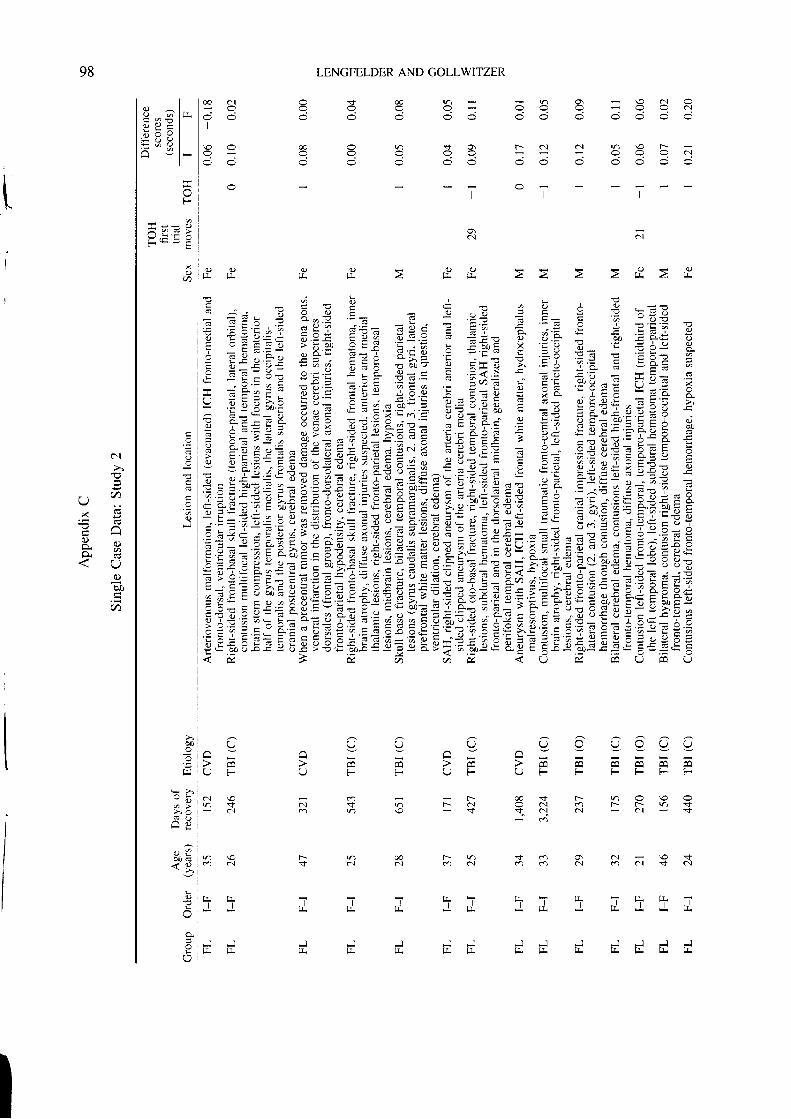
r ) O , \ O ( . . I O
F- c..t Cj r) \O t--O O O ( - . I
O S @ n
c p C r ) < 1 - 3C O O O O
@ c]
I
LENGFELDER AND COLLWITZER
ö]
f - r )ca c.l
- tJ I J .
J J
I
F
r C ) e O2 lJ- 2. IL
ö i \ o do ö . 1 * c n
OI
E ;:EeE E=iaila ääg E ;ii ä gs i* ä ili tIE:EIEItgi'j'ääiä 'eziä= ;ä 9ä€ääE! I ii=?gg+alEE;ls=?cl1i4aäEäiE,Ei=i,iE+äzEl€iviji.zEilz.iir;=E=i:+Ei'Ez;E;iliEa=.äEEEäE\Ei=*EErIE=Ee;!.l+{!9:Eä+EE;g=AEieElff EiEEeEE ; € : äft gäE :äE äi;€ ä: : I ä* äg? Eiäl€ E äE äi äEFiQ i € ; ; : 5 = q 6 ü f € = - ' s l Z = E . 9 ' o , ,
EEäEiE äEt r€EgE€i€€äEäsäiEääi EEiäEEgE EIEE E
s oo o
o ot! tJ.
rt \oca öl
t l
J JIJ. IL
A f ,v v v v v v
A
U F F F F F F
@ $ t t - V ) O \ O OO a-.1 m F- r-- v) tq .l c.r ö.r s
U U ( JA A
r ) L L T ) L
ce F-a . l $ r ) r - a {c e v f \ o *
U
r ) sN
t i i [ 1 1 [I
r<+
JE d d d d-l ".1
t r E,tIL
r ^ io o | J .c ? - l
9 E F I. o 9 x lE ; ö l
v r lH - t r
I
T
F
?* - = vY , F ' T OF - - E
0a
€
oJ
b0
H
- o
> ' o
H Y
0 0 6
o
r l
98
l.
ö.1
r \ ( t
X Ü
o* 6 3
C)
öo
(n
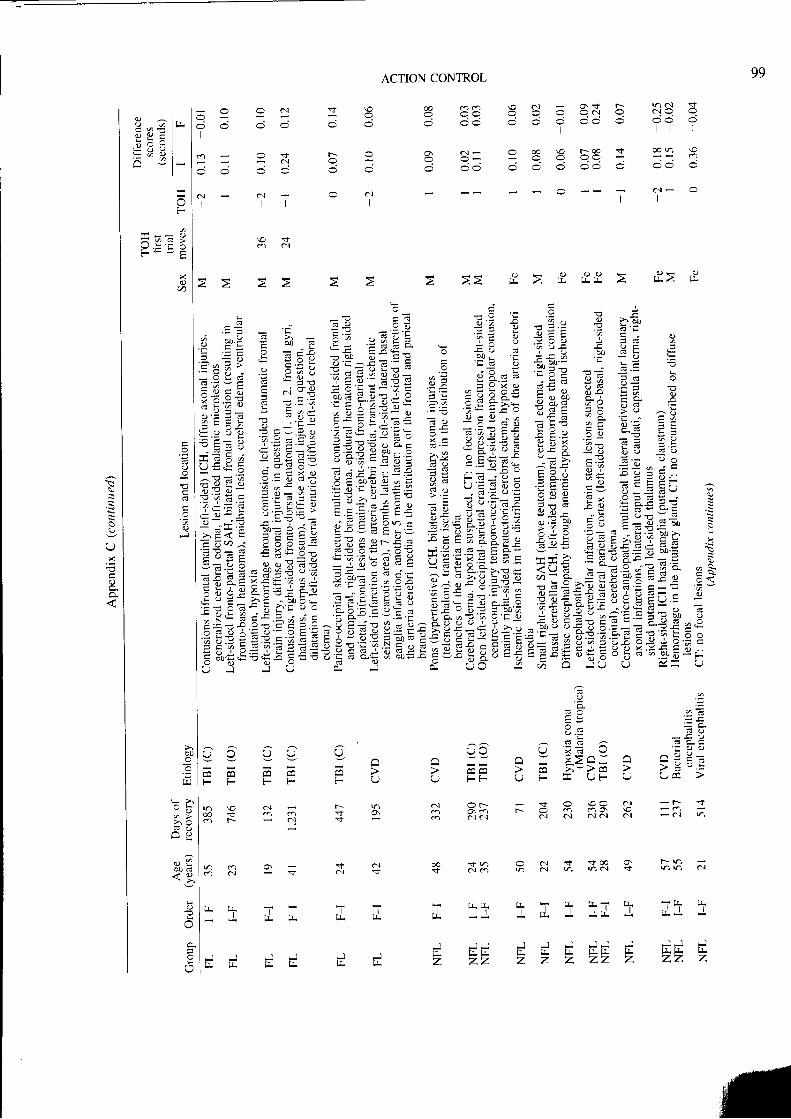
99ACTION CONTROL
n a l s
: - i - i - i
t l l
+ @ ! n \ oo
- l - i - i Ä
8 8 5-i -i /.i
I
o 9 a 9- i ^ Ä
ca co
a { - F- 0c
@
C l - CI
OIc.t a.l o cl
l l l l
o c n
: : s: . - O - =
= e F E , ! z = t 3 r EtEZ E ä: i lzi a:s E2-42 { iZ e Qg : = .= * 7= ; ! b
EEi ZE äiää; !Eä TE E1 Cär : ä ; E t ; ; E H € 5 E ; g E E$+iE 3i €+E:: :ä5 EIEE,ETEilZlu= ZEllz EEi ä1 ==rEÄi :;tZ giezllrllu':'?i "==i: ää iä Z E F ; E g = E + i : : = ; € E € € .'EEzEäiä! iä; 'Eäet*IgEEts '5y EE aE y E äi u;4- äg I äi€ g; E lEg ;ii äeE=sEggs E3e=uä Hü5 sg 8#alr I
A o
F T . g= . - !
e = c
6 0 . YE t a
i : F d
o d -
Ä = ,= - , !
F A Oi ' i L
i > L
c . E . )
' Ö a a
'q ' - " . r
öh= 7
O ' F E
i € . -I e ;
: . e . := x f ,
oE
oI
o
6
o
I
Eo
. F
I
aöl)
Eo
,'J
L
E6
E
d
o
o
6
€
01)
I
d
a
, F
-)<
I
0
c
q
. =E Ir O
3 o
2 ' 6
9 ö
= E
o -x o
9 ' Et - o
C O
i \ :
o . o
6 L 5
= E
d)
ö ä- 3
n t r2 -. ' -
; -
E ;E c.:
? : *
= h
- a
. F
c.i
--i
? . s '
h g
9 E3 ?
t :
. i l>''-
- öU
I
6 -
-!
o x
I a ) ,
O . E t .
a oöl) 4
i c e
i. a\
- ' Fo) .-
. - 7 - ,
c ' 2 d >- ä 9 a
5 ö = öx o . : : . 1c 3 1 , 2 -^ , . =
J =
A F E '
,€ o 32,- o t r d x
I 6 ^ O
^ E = ' A
E g : i s
h : . :
> . E < t sE öra , - r
- c . F l l -- h = 6 . : :6 l : x c xE H I ö Ry u : s x- u . t 2 :: =t r = € + . 99 f r € e ;- c o : a
F ä o ' ; r ! -O O
U J
- d
ü . ?
9 ? . 2 7c = . = €
9 . : = Y! _ ä J
d a - n C - =
\ J x = v L : 'I C = : n - . 1 a ' 9 . . l -
I J ; 2 - - - - - ; -
- F F- - r 7 , aä ' " t9 F I V F V
öl
ör
U
a{
O
r
r , (v v v
m m
F F F F F
rr \O an r-0 o $ c n c a sc ) r - c \ v
ceF F
a.l ö{F - o - - , 3
c.l öl Öt ar
- r \ - f ,
- a l V '
t\ r,vt vf cl
I T Tl J . i l
J J J
z z z
o c J + s c c qn ö l r ) mN v
(r - lÄ E-- tJ-J d . J J d J
J J # t # #kz z z z z z
& sv ' )$ a { oo, .+ qr
+ d s
d.t 1 T T
I J
r+l+t l
J JtJ. tr.z z
J
J J
I3 a l oc ? P lo y J c lL = ^ l
, o y i tE ; ö lx a l
I
F
* - = Y
F - - C
o
'o
Cd
OJ
öO
E
: b- o
> . cA HH t s
. t o
o
O
h
-
UX
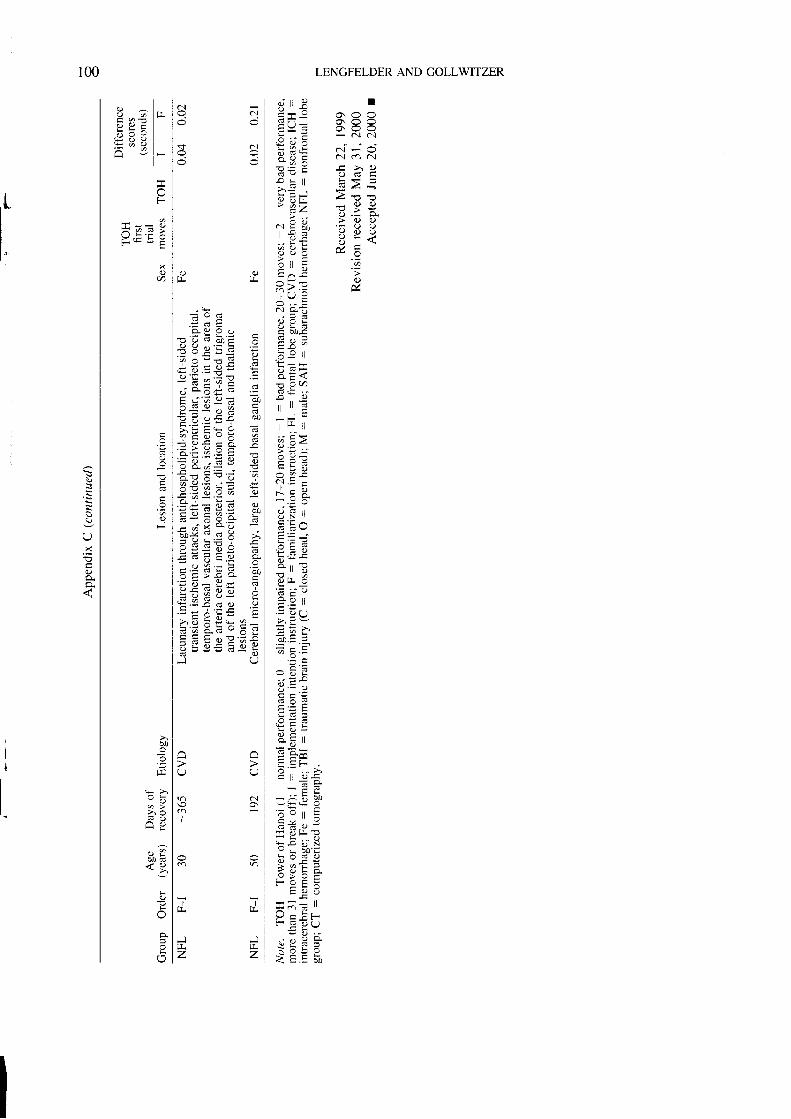
LENGFELDER AND GOLLWITZER
o i l l I I) - - oE * - X = =c9 ; > ( . ; < ; <L = - N a J
| = ' L ö l - OX ö c c ' l r , N
;.e ? -c >, cr- e - ( J ( i ca . r r L * <
; = " - j a gb i # Z : o r
a L Y > XI > . - : a ' - -
N E ; , . a < ) ' Jr 3 ä Y ( l !' 9 c H - <ä ö k J c9 a aA , t E
' ä
; , ' C J . -
= ^ c 2^ ! _ o; P X &N C ;
" t I l t
E ö .
8.: <= ? q6 ( E . .
i l =l l r r t J
' [ l t t
. - : j :a ^ 2 .
t r L : ' i
(.J .! c
J . Q
O € I L! N ' ,
Q i V
c - - i
: . E äF i :ö * *- l r o: , , rt - i :
x : , .= v t l
'- : \.,/> / v
= E >
äo.= =
E F . =
- g :o L _ .
= : x: . v ;
a - b t l; = -F c | !o . . >
' = E " E- - � E ' 9 :q E o i K
; - e : : g; @ t =< o ! o
_ v > U C
C 7 , ?r - ; "+ - - l l
t - = t > ,' : v ve o . -
n ! i : :N : ; i< l . = ä I )
c.l
c.l
c\|
s
I I
i ä a
. + I 9 uf ? I 6 öoF öT Y E E E ' Z
d ^ - - ! J F
: > a ' 6 e ' -
C : f = . : : lQ : v ^ , 2 >
i 3 - . F ! l Ä ' n
ä : : ä ! s- i o s - X : l. : > e . =O - - o . = = i
= q : ä s ö- q g
b E ö ?? Y ; i E , E= Y 6 i a 6 a )
. = , ! = C r G O
= 9 E 3 ä 5! w e : . F
- . ; x g o -- * . J d - o - -r y z , . : Q aä c 3 6 9 Ä =i = - - ! l ; ß
€ 6 d t . 9 *- u 9 - ä - =! = t " : Ä a 0a E - - ^ - C' i q = F c IE ! E u e IE ' - + . P I . :' - E o h = Ei " . q 5 : h E =d o O G - ^ : '
E E E o e ' ä Er l ü o E : u 9 /t - - - * - EJ U
O
al
r;.
U
oI
d.
Jr r
z
, ' Iö 6 lr:-E ? = le x E lo 9 Y l
E 3 ü lÄ E t -
I
F
?t J . == : '
(t
6
d
.l
E
: r- o
> , oA 9H Y
ä o d. l A
^
r l
100
I '
-
Ox
II