Embed Size (px)
Citation preview
REFORMATION inSURGICAL EDUCATION &TRAINING
Stephen Tobin
DEAN of EDUCATION
Royal Australasian College of Surgeons
IMELF Calgary 2013

REFORMATION
● ‘… the action or process of reforming an institution or practice …’
● From ‘reformare’ = shape again
● The Reformation (the Church 1517)● Re-formation = the action or process of
forming again • * NEW OXFORD DICTIONARY OF ENGLISH

SURGICAL EDUCATION & TRAINING
● RACS commenced 1927-1930● ‘Excellence in surgical education &
practice’● Training in hospitals (employers)● Framework of SET principles● Collaboration with Speciality Societies● Fellowship exam (SET5-6)● Professional development role as well
The structure of the RACS program
● The College is accredited as the training provider
● The College provides curriculum resources, particularly for the non-technical competencies
● Each of the nine surgical specialties develop and deliver much of their curriculum in the regions and hospitals, and at specialty meetings

SET 2007…..
● Structured program from PGY 3-4● Effectively PGY3-6+● 5-year programs (5-7)● Absence of official surgical framework for
clinical years before SET program
● Workforce issues ● IMGs

The structure of the RACS program
● RACS as an organisation – diversity & number
Figures at the end of December 2012 Australia and New Zealand
Specialty Trainees Fellows
Cardiothoracic Surgery 34 182
General Surgery 419 1731
Neurosurgery 53 229
Otolaryngology Head and Neck Surgery 81 497
Orthopaedic Surgery 236 1419
Plastic and Reconstructive Surgery 83 440
Paediatric Surgery 22 104
Urology 111 410
Vascular Surgery 42 191
Totals 1081 5203
The structure of the RACS program
● RACS as an organisation – size and distribution

Issues with SET – reform?
● Medical students: surgical societies● Numbers of graduates● Lack of structure PGYs● Selection● Supervision – feedback, assessment● Fellowship exam success % less● Competent not confident Fellows

MEDICAL STUDENTS
● Well-developed ‘surgical societies’■ All 22 medical schools
● Articulate● Connections – locally, College● Up to 25% interest
● Courses, evenings, draft agreements….
GRADUATE NUMBERS
● 22 MEDICAL SCHOOLS● 55% graduate-entry● Nomenclature MD increasing● Numbers 1800 (2005) >> 3800 (2017)*● Vocational stream jobs less (est 2800 now)*
● Urban v. regional & rural● IMGs
• *MTRP 16TH REPORT , JULY 2013• Australian figures; NZ better match
J-Doc : New for early years
● Suite of resources / e-portfolio● Assist with pathway to surgery (SET)● Mapped to AustralianCurriculumFramework*
■ For young doctors in PGY1-2
● Develop to novice-intermediate levels of the 9 RACS Competencies
● Provide well-developed doctors for SET■ Or other (procedural) specialties
• *3RD EDITION, 2012, www.curriculum.cpmec.org.au

Bringing this together : First profile
12

Education across the continuum
● Developing expectations of behaviour and performance
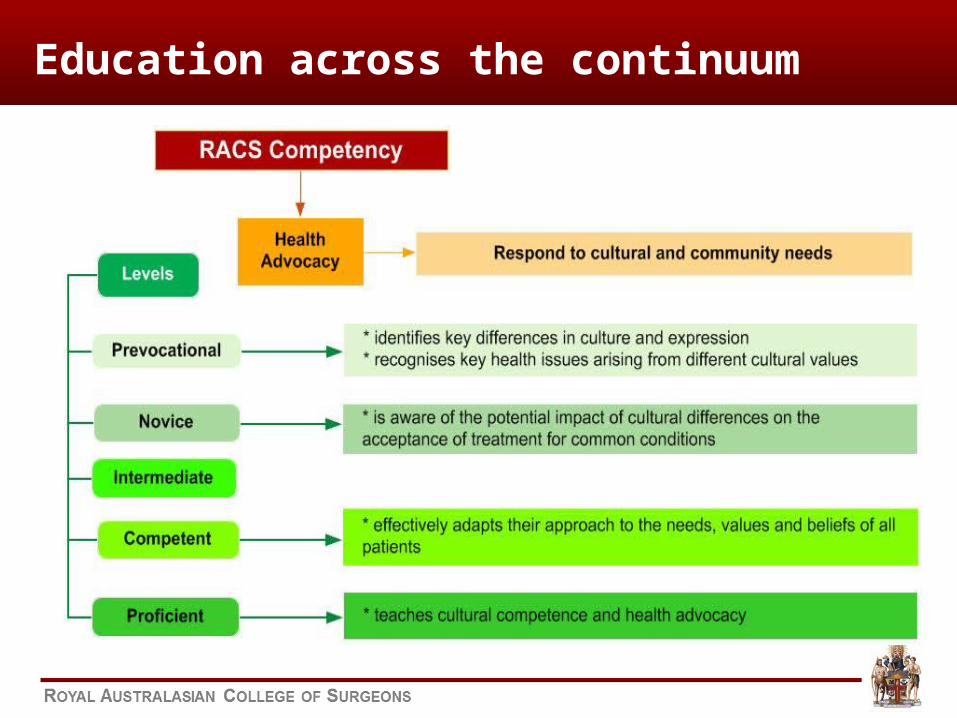
Education across the continuum

Bringing it all together
Social tools/APPS
Web Linked Resources
• The PGY Curriculum• Passing the GSSE
Examination• Register for the GSSE
examination• Links to College
documents (policies/competencies)
• Self Assessment• Surgical SkillsBox• Practice Bank MCQs• Clinical Decision
Making• Goal Setting
e-Learning
PRE-VOCATIONAL LANDING PAGE
Presentations
External Web Links
• Register for Skills Training Courses
• Apply to SET
• How to pass the GSSE examinaton
• Video tips
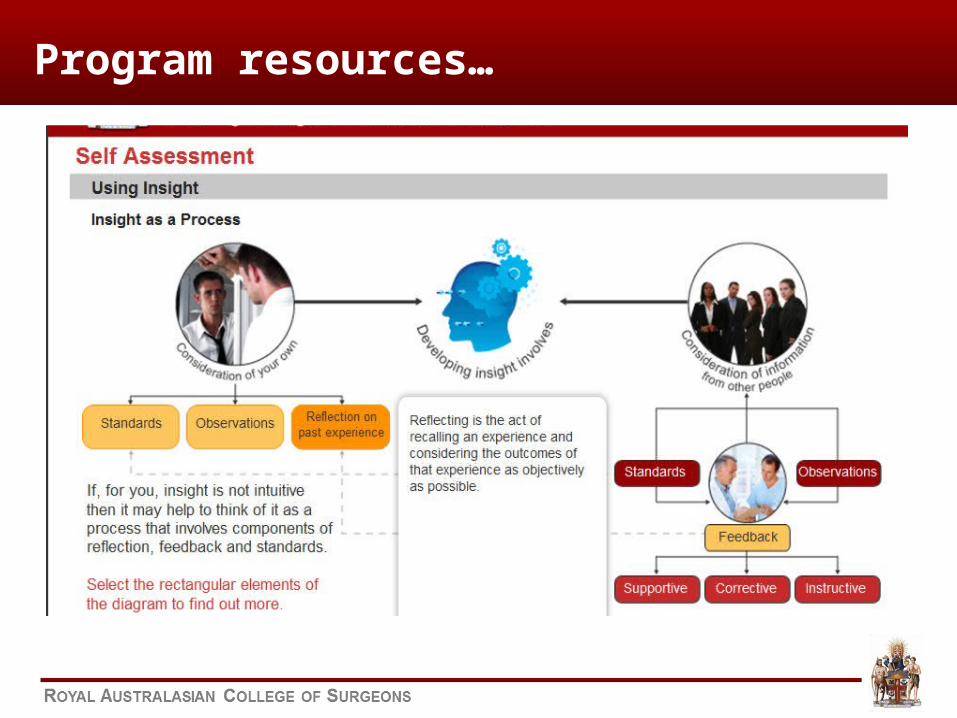
Program resources…

Digital College Vision
Welcome John CitizenHome > My Page
Update My Details
Welcome John CitizenHome > My Page
Update My Details
News ePortfolio Self Assessment Progress
News feed, any upcoming events..
15%5%
30%
50% Courses completedThe Morbidity Audit and Logbook Tool(MALS)
My Learning Modules
Course Name Description Cost
Goal Setting
Clinical decision making
Examination Module
Surgical Skills tool box N/A
N/A
50
100
Text
Text
Text
Text
My Tools and Resources
Description Resource/Tool Description
Description
Text
Text
Text
Skills Training
External Anatomy Course
College Standard Documentation
Free Apps Text
View
View
View
My Subscriptions
Description Resource/Tool Description
Text
Text
Text
Text
Fax Mentis and Surgical News
Social Tools Yes No
Yes No
Yes No
Buy
Re-Attempt
Complete
Buy
Buy
ePortfolio
SET selection
● Curriculum vitae (15-30% weighting)■ Points■ Prerequisite jobs*
● References: 2 or more…6-8 (27-60%)■ Some closer to work-based assessment■ Features of MSF-360
● Interview (25-45%)■ Use of the above to rank for interview
• *some year of application (to come)• *others must have been completed

Summary of significant selection-assessment relationships
Examinations DOPS MiniCEX End of Term Assessments
SSE Gen-eric
SSE Spec-ialty
Spec-ific
Clin-ical
DOPS1
DOPS
2
DOPS
3
DOPS
4
DOPS Mean
Mini-CEX
1
Mini-CEX
2
Mini-CEX
3
Mini-CEX
4
Mini-CEX
Mean
ETA1
ETA2
ETA3
ETA4
ETA Mean
n 339 292 337 252 204 88 42 253 254 199 82 33 256 277 297 148 139 312
CV Neg Neg Neg
RR
Inter-view
Total Sel-
ection
P < 0.05 P < 0.01 P < 0.05

What about selection?
● British study compared 1990 cf late 90s● Compared regional vs.hospital/surgeon selection
● No difference between ‘performance’● Dropping-out; length of time; GMC
● Review BJS 2012*■ No discriminators■ Psychometric testing some role
● Not statistically significant• *Note Leading Articles series 2013 (100th)
SET PROGRAM - assessment
● Evaluation forms● LogBooks● MiniCEX used by 6 (usually early years)● DOPS used by 7 (as above)● MSF – 360 noted, not used● Purpose of assessment● Signing off for FEX exam.
Collins JP, ANZ J Surg June 2013

SUPERVISION
● “Good supervision is difficult”
● Need to improve quality, numbers
● Academy of Surgical Educators■ ‘professional development of educators’
● Foundation course for educators/supervisors
● Authentic ‘signing-off’● EPAs

What about the program?
● Academic enhancement (<10%)● RESEARCH – before or during SET● Masters programs – Australia-NZ, Uni Edinburgh
● Personal leave (2-5%)● Probation (2-5%)● Dismissal (1%)
RACS data 2009-2012
Comparable
● Time-expired may increase● As Fellowship pass rate has declined

Fellowship (FEX) examination
● Signing-off is vitally important● FEX tests :
■ Medical and technical expertise■ Decision-making and judgement
● Recent close-marking■ Documentation
● Recent decline in success rates■ 81% - 2010 : 63% - May 2013 ■ Variation across states & NZ■ Variation between specialties
Evaluation of SET – current survey
● Entry level varies● Need to develop WBA approach● Working hours● Presence of ‘Fellows’● Signing off?● FEX approach
■ Surveys of trainees, supervisors, new Fellows
New Fellows
● Competent level across competencies● What done this mean?● Need for support at transition
● Matching to positions● Overseas work● Post FRACS ‘Fellowships’● Work in hospital unit or (private) practice

Reformation…
● SET is grounded in the community● Hospitals, Specialty societies, College, Urban& Rural
● Excellence >> befit community needs● DISTRIBUTION OF FELLOWS
● College covers trainees and Fellows● EDUCATION & PROFESSIONAL DEVELOPMENT
● NEW J-Doc program starts the approach● RACS COMPETENCIES
Reformation could mean…
● Better quality applicants● Better selection● Better supervision & WBA● Appropriate “signing-off”
● For some, this could be earlier
● FEX matches competent practice● Support in workplace to start● Lifelong learning – e-portfolio/CPD (WBA)
Reformation needs…
● Evidence –base & evaluation● Good supervision● Recognition-support of supervisors● Motivated trainees● Competency assessment with meaning
■ EPAs , training to match profession (work)
● Leadership & awareness of surgical education■ International influences■ THANK-YOU