Embed Size (px)
Citation preview
Renu
Eli
Dep
� Pmcan� Jo
m
International Journal of Nursing Studies 51 (2014) 761–767
A R
Artic
Rece
Rece
Acce
Keyw
Elde
Focu
Long
Prof
Regi
*
002
http
gistered nurses’ perceptions of their professional work inrsing homes and home-based care: A focus group study
sabeth Carlson *, Margareta Ramgard, Ingrid Bolmsjo, Mariette Bengtsson
artment of Care Science, Faculty of Health and Society, Malmo University, Jan Waldenstroms Gata 25, SE-20506 Malmo, Sweden
What is already known about the topic?
revious research has described elderly care as unde-anding and depressing, not usually considered as areer choice by student nurses and newly graduated
urses.b satisfaction is a strong predictor for nurse recruit-ent and retention.
� Professional identity can be conceptualised in terms ofwhat it means to be and act as a nurse in everydaynursing practice.
What this paper adds
� Professional work in elderly care is complex, requiringadvanced nursing skills and several years of previousexperience in acute-care settings.� Three key aspects of registered nurses’ perception of
their professional work emerged: establishing long-termrelationships, nursing beyond technical skills, and
T I C L E I N F O
le history:
ived 19 April 2013
ived in revised form 1 October 2013
pted 2 October 2013
ords:
rly care
s groups
term relationship
essional work
stered nurses
A B S T R A C T
Background: In Sweden, as well as in most industrialised countries, an increasing older
population is expected to create a growing demand for health care staff. Previous studies
have pointed to lack of proficient medical and nursing staff specialised in geriatric care,
which poses serious threats to the care of a vulnerable population. At the same time, there
are studies describing elderly care as a low-status career choice, attracting neither nurses
nor student nurses. Judging from previous research it was deemed important to explore
how nurses in elderly care perceive their work, thus possibly provide vital knowledge that
can guide nurse educators and unit managers as a means to promote a career in elderly
care.
Objective: The aim of the present study was to illuminate how nurses, working in nursing
homes and home-based care, perceived their professional work.
Method: This was a qualitative study using focus groups. 30 registered nurses in seven
focus groups were interviewed. The participants worked in nursing homes and home-
based care for the elderly in rural areas and in a larger city in southern Sweden. The
interviews were analysed in line with the tradition of naturalistic inquiry.
Results: Our findings illustrate how nurses working in elderly care perceived their
professional work as holistic and respectful nursing. Three categories of professional work
emerged during analysis: (1) establishing long-term relationships, (2) nursing beyond
technical skills, and (3) balancing independence and a sense of loneliness.
Conclusions: The findings are important as they represent positive alternatives to the
somewhat prevailing view on elderly care as depressing and undemanding. Nurse
educators might use the key aspects as good examples, thus influencing student nurses’
attitudes towards elderly care in a positive way. Elderly care agencies might find them
helpful when recruiting and retaining nurses to a much needed area.
� 2013 Elsevier Ltd. All rights reserved.
Corresponding author. Tel.: +46 406657451.
E-mail address: [email protected] (E. Carlson).
Contents lists available at ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
0-7489/$ – see front matter � 2013 Elsevier Ltd. All rights reserved.
://dx.doi.org/10.1016/j.ijnurstu.2013.10.002

E. Carlson et al. / International Journal of Nursing Studies 51 (2014) 761–767762
balancing independence with a sense of loneliness,indicating a strong professional identity.� The findings provide nurse educators and unit managers
with positive examples when attracting and recruiting toan area in need of qualified and engaged registerednurses.
1. Introduction
In Sweden, as well as in most industrialised countries,an ageing population is expected to create a growingdemand for health care staff, in particular specialist nursesin geriatric care. It is not unusual that high age is followedby the risk to develop a number of different chronicdiseases leading to an increased group of patients withlong-term caring needs. Hence, it is most likely that amajor part of nursing and medical care for this populationwill be redirected from hospitals to home-health careteams or assisted living, intensifying the need for highlyqualified geriatric care. It is therefore alarming whenstudent nurses and newly graduated nurses describeelderly care as boring, undemanding and depressing,and not an option for a future career (Kloster et al.,2007; Stevens, 2011). The reported findings are in partcontradicted by findings in a recent study by Carlson(2013). Student nurses valued the independent andperson-centred nature of nursing they had experiencedduring clinical placements in elderly care. This was putforward by the students as a reason to consider a career inelderly care. On the other hand, some students describedelderly care as hopeless in a stressful and depressing workenvironment, and explained that elderly care was not acareer choice they would consider after graduation. InSweden, recent reports (Statistics Sweden, 2011; NationalBoard of Health and Welfare, 2012) point to the risk thatlack of proficient medical and nursing staff specialised ingeriatric care and gerontology poses serious threats to careand patient safety for a vulnerable population. Adding tothis picture is the anticipated worldwide shortage of healthand social care staff (WHO, 2006). Conclusively, with thecurrent global demographic change, an increased demandfor nurses working in geriatric care will be imminent.
1.1. Job satisfaction
Job satisfaction, including intrinsic factors such as:autonomy, freedom to use personal knowledge andjudgement, and relationships with patients, as well asextrinsic factors i.e. working conditions, benefits andsalaries, is a strong predictor for nurse retention (Ellen-becker, 2004; Karsh et al., 2005). Vlachos (2012) reportedthat continuous relationships with patients and families,and being able to make a difference were rewardingcomponents significant for positive job satisfaction innursing homes. On a similar note, Prentice and Black(2007) concluded that sufficient resources allowing nursesto care for, and make a difference to the residents’ liveswere important factors for nurse retention. In a survey byEllenbecker (2001), professional autonomy, relationshipswith peers and patients and sensing that the work isimportant and worthwhile were indicators positively
related to job satisfaction. Factors influencing job satisfac-tion negatively were related to relationship to adminis-tration and the power to change organisational policies. Ina later study by Ellenbecker et al. (2008), job satisfactionand tenure were presented as the strongest predictors ofnurse retention. However, job satisfaction is probably notonly of vital importance to nurses. Ellenbecker andCushman (2012) proposed in an extended theoreticalmodel, including patient outcomes that the qualities ofpatient care will be affected by how satisfied nurses are intheir jobs. Cowin et al. (2008) investigated the relation-ships between nurses’ professional identity or self-concept, job satisfaction and retention plans. Their findingssuggested that nurses’ self-concept had a strongerrelationship to retention than to job satisfaction. However,the study did not focus exclusively on nurses in elderlycare. Therefore, to facilitate the recruitment and retentionof nurses it is important to further explore nurses’perceptions of their professional work in nursing homesand home based care.
1.2. Professional identity
Professional identity as a concept is not well described innursing literature, and has been addressed in terms ofsimilar and related concepts, for example, professionalismor professional self. Johnson et al. (2012) explained thatformation of professional identity involves a sense of values,practices and purposes associated with the nursing role,acquired through socialisation, commencing at the start ofnursing education and extending during a life-long career. Inan earlier study by Fagermoen (1997) professional identitycould be conceptualised in terms of what it meant to be andact as a nurse directly linked to everyday nursing practice.Skar (2009) conceptualised professional autonomy on asimilar note by illustrating how experienced registerednurses defined autonomy in terms of being knowledgeable,confident, and having the personal courage to act. Ellen-becker (2001) discussed nurses’ professional autonomy interms of meeting professional standards and providing carebeneficial to patients. However, formation of professionalidentity does not take place in a void. It is sociallyconstructed and evolves in interaction with significantand generalised others (Shaffir and Pawluch, 2003), in aprocess of actively gaining skills and knowledge, values andattitudes of a group that the individual seeks to become amember of. Professional identity evolves through education(Levett-Jones et al., 2007), and through professionalexperience gained over time in interaction with colleaguesand patients (Fagermoen, 1997).
In the light of the expected nursing shortage in elderlycare, it was deemed important to explore how elderly carenurses perceived their work, and thereby contribute to theexisting knowledge of factors for attracting and retainingnurses to a much needed area.
1.3. Aim of the study
The aim of the present study was to illuminate hownurses, working in nursing homes and home based care,perceived their professional work.

2. M
datidewhbelwathedes
2.1.
peoorghomtermmecurfouThecarmeaffimadesfirsnuruniwriwhat lhomfor
to tfocgrosenmalarginfotheaut
2.2.
Helthe
Tab
Focu
Ge
Ag
Ye
Sp
Ye
a
care
care
E. Carlson et al. / International Journal of Nursing Studies 51 (2014) 761–767 763
ethods
A qualitative design, utilising focus group interviews asa collection method was employed. Focus groups areal in capturing the interaction between participantso share experience and perspectives, and in exploringiefs and attitudes (Freeman, 2006). The chosen methods therefore deemed relevant as a means to illuminate
social reality of being a nurse in elderly care ascribed by the participants.
Participants and setting
In Sweden, social welfare and health care for olderple is the responsibility of local municipalities, usuallyanised as home-based care or long-term care in nursing
es. For this paper, we use elderly care as the common. The needs of the patients range from complex
dical conditions to dementia and end of life care. For therent study the researchers contacted unit managers inr different municipalities in the southwest of Sweden.
nursing homes and the organisation for home-basede within these municipalities provide clinical place-nts for the undergraduate nursing programme at theliated university where the researcher work. The unitnagers were provided with written informationcribing the study, the inclusion criteria, and for thet author. During a regular weekly meeting, eligibleses were informed about the study by their respectivet manager. They had the opportunity to read thetten information in order to make an informed decisionether to participate or not. Registered nurses (RNs) witheast one year of work experience in nursing homes or
e-based care for the elderly met the inclusion criteriathis study. 30 nurses volunteered by sending an e-mailhe first author (Table 1). It was possible to form sevenus groups, with three to seven participants in eachup (5 + 4 + 3 + 4 + 3 + 7 + 4). Five of the groups repre-ted RNs working in rural areas, and two groups werede up of RNs representing six out of ten boroughs in aer city. Correspondence with participants included anrmation letter briefly describing the aim of the study,
interview process, telephone number and to the firsthor as well as ethical considerations.
Ethical considerations
The study was conducted in accordance with thesinki Declaration (WMA, 2008) and approved by
local Ethical Advisory Board at the university where
the authors hold their positions. It was assured, by the firstauthor prior to the interviews, that participants fullyunderstood the issue of confidentiality, and that they hadthe right to withdraw from the study at any time withoutfurther explanation. Informed consent was obtained, andnone of the nurses declined or terminated participation inthe focus group interviews.
2.3. Data collection
The interviews were held during spring 2012, either atthe different workplaces or at the university where theauthors work, subject to participant convenience. Inter-views were conducted by using a digital voice-recorderand lasted between 57 and 96 min (mean 75 min). Duringinterviews, participants were encouraged to elaborate ontheir thoughts of being a nurse in elderly care, and thediscussions started with the first author asking ‘How would
you like to describe nursing in elderly care?’. The researcherallowed the discussion to evolve, and only interruptedwhen the discussions raised any questions that neededclarification. Such follow-up questions were typicallyphrased as: Can you please explain what you mean or can
you please tell me a bit more? Seven interviews wereconsidered sufficient with this specific population (McLaff-erty, 2004), even though the groups comprising threeparticipants each are small (Kitzinger, 1994). However, asemerging data were continuously compared it wasdeemed reasonable to include the smaller groups.
2.4. Data analysis and rigour
The interviews were transcribed verbatim and readrepeatedly by the first author (EC). No software for codingof data was used, but hand coded as a means to gain adeeper understanding of the data (Polit and Beck, 2006).The first author started the inductive process of analysing(Lincoln and Guba, 1985) by identifying meaning unitsillustrating patterns of how nurses perceived their work inelderly care. Meaning units were then sorted into codedsubcategories, and the meaning of each subcategory wasexplained and clarified. Hence, a model for continuinganalysis as well as the transcripts was presented to thethree co-authors who independently critically reviewedthe material. The next step involved peer review (Creswelland Miller, 2000) when the emerging findings werediscussed with a group of fellow researchers at theuniversity where the authors work. This process providedthe researchers with valuable feedback for the continuedanalysis. The final abstractions of meaning units andsubcategories into categories were discussed and agreedby all four authors (Table 2). The authors are experiencedqualitative researchers as well as lecturers in researchmethodology.
In an effort to obtain credibility, data are presented byverbatim quotes and explained by the authors’ interpreta-tion. The quotes represent discussions from all seven focusgroups to illustrate the richness of the data. Moreover, asdiscussed by Malterud (2001) and Tong et al. (2007) theresearchers’ background and personal experience willaffect not only what to investigate or how to analyse, but
le 1
s Group participants (n = 30).
nder (female/male) 25/5
e, mean (range) 46 (25–64)
ars of professional experience mean (range) 20 (1½–42)
ecialist nursea
s/no/missing
17/11/2
Midwifery = 1; Primary health care = 10; Palliative care = 1; Elderly
= 1; Anaesthesiology and intensive care = 2; Surgical and medical
= 2.
E. Carlson et al. / International Journal of Nursing Studies 51 (2014) 761–767764
also the interaction with participants during data collec-tion. The researchers in the presented study hold positionsas either senior lecturers (EC, MR, MB) or professor (IB) atthe affiliated university. However, at the time of the studythe researchers were neither involved in clinical work norcollaborative initiatives between the university and thestudied settings. Thus, none of the researchers had anypersonal or professional knowledge of the participants.
3. Findings
Registered nurses working in elderly care perceivedtheir professional work as holistic and respectful nursing.We illustrate this by elaborating the following categories:establishing long-term relationships, nursing beyondtechnical skills, and balancing independence and a senseof loneliness. Our findings are illustrated by excerpts fromthe focus groups.
P ¼ Participant; Fg ¼ Focus group
3.1. Establishing long-term relationships
All nursed described how they valued the possibility toestablish long-term relationships with patients and theirfamilies, contrary to the short and superficial relationshipsthey had experienced in acute-care settings. One of thenurses told the focus group of some of her patients that shehad taken care of for more than ten years, and this wassomething she appreciated:
‘‘Well, you know your relationship with the patients iscompletely different when you see them for years, andthat is something that has become more and moreimportant to me’’ (P 17, Fg 5).
Long-term relationships with patients were describedas entirely positive, and a major reason why the nursesperceived elderly care as a preferred field of nursing. It wasinteresting to note how the nurses often compared theircurrent work situation to previous work experience,favouring the former:
You don’t meet the same patients from one shift toanother working in acute-care; you don’t have thecontinuity and get to know the people you care for. I thinkit is worth a lot when you are able to follow up all thenursing interventions you actually start’’ (P 23, Fg 6).
The nurses experienced professional pride when theywere able to follow the recovery processes of their patientsand described continuity of nursing care as a professionalbenefit:
‘‘It is such a great feeling when you have struggled witha problem for several months, trying to heal a venousulcer and then suddenly you actually get to see theresult’’ (P 1, Fg 1).
Further, several of the nurses valued the individualisedand person-centred care they were able to provide. Thiswas something they considered much harder to achieve in
‘‘There are so many things I like with home-based care;you get a totally different view on your patients as youare the guest in their homes.’’ When you meet thepatients and their families, you get to see the full picture,not only a single symptom or a diagnosis’’. (P 8, Fg 2) ‘‘Yes,and I appreciate all my home visits, meeting them [thepatients] in their own environment, on their terms, andwith families and pets around them.’’ (P 9, Fg 2).
3.2. Nursing beyond technical skills
The nurses argued that their choice of elderly care as apreferred field of nursing was choosing a nursing careerstretching beyond technical skills. They considered theirwork to be more complex than in acute-care settings asthey worked closer together with patients and families.They emphasised the necessity of a holistic approach tonursing care, acknowledging all aspects of their patients’needs. This was explained as:
‘‘Nothing is ever black or white, what we do is muchharder, more assessments to be done, and you needsome experience to see the full picture. I mean you haveto see your patient in a holistic way.’’ (P 7, Fg 2).
Therefore, the decision to practice in elderly care hadusually been taken by the nurses after they had workedsome years in acute-care settings. The nurses agreed thatover time as you gained professional experience, yourthoughts on the nature of nursing changed. As expressedby one of the participants:
‘‘I remember as a new grad I absolutely loved being busyadministrating i.v. drips, cannulas and meds, but in thelong run, it doesn’t give you any real satisfaction.However, meeting an old person though, who will tellyou all about his life and who you get to meet day afterday is something I have come to appreciate.’’ (P 28, Fg 7).
Furthermore, the nurses shared the experience of beingpreceptors to undergraduate student nurses. Although,acutely aware of the need for qualified nursing staff, thenurses usually recommended their students to gain someexperience in acute-care settings before commencing acareer in elderly care. The reason, given by the nurses, wasthat caring for older people was an advanced and complexnursing skill requiring experience from a variety of nursingspecialities:
‘‘I think that you need some years under your belt, youneed all sorts of skills which I think you learn byworking in different hospital wards, especially sinceyou have more colleagues around you to turn to forsupport’’ (P 19, Fg 5).
The nurses also pointed to the multi-facetted aspects oftheir work when they accounted for elderly care as beingnot only of a palliative, but also curative and preventivenature. One nurse explained:
’’We do a lot of preventive work trying to preventpressure ulcers or malnutrition, but prevention is
probably not what you think of at first’’ (P 13, Fg 3). acute-care settings: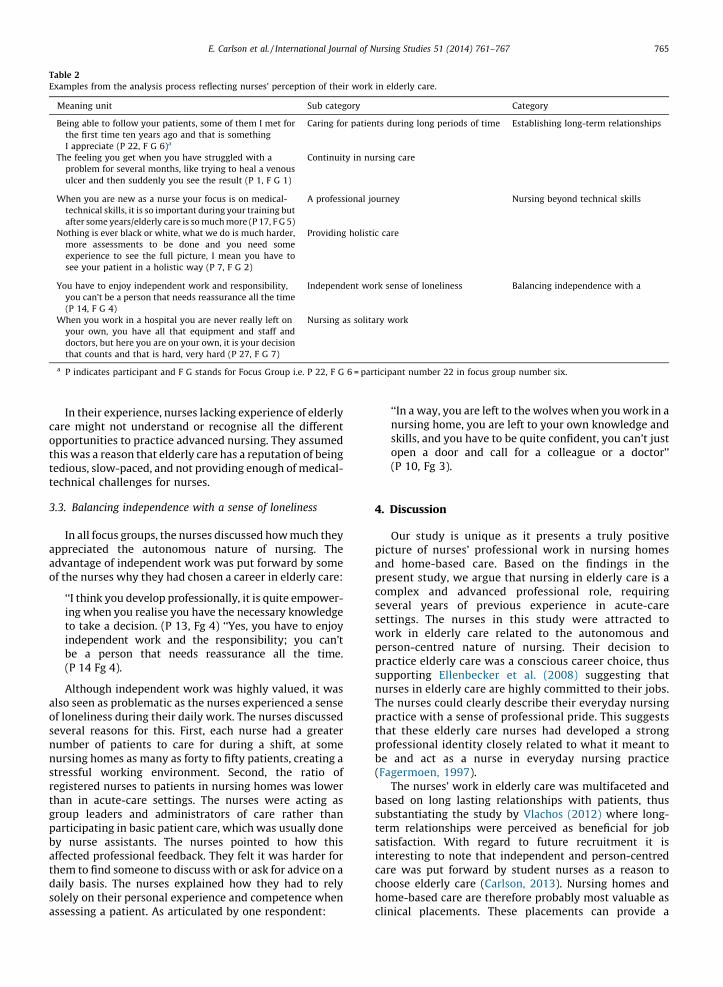
caroppthistedtec
3.3.
appadvof t
alsoof lsevnumnurstreregthagroparby
affethedaisoleass
Tab
Exam
M
Be
Th
W
No
Yo
W
a
E. Carlson et al. / International Journal of Nursing Studies 51 (2014) 761–767 765
In their experience, nurses lacking experience of elderlye might not understand or recognise all the differentortunities to practice advanced nursing. They assumed
was a reason that elderly care has a reputation of beingious, slow-paced, and not providing enough of medical-hnical challenges for nurses.
Balancing independence with a sense of loneliness
In all focus groups, the nurses discussed how much theyreciated the autonomous nature of nursing. Theantage of independent work was put forward by somehe nurses why they had chosen a career in elderly care:
‘‘I think you develop professionally, it is quite empower-ing when you realise you have the necessary knowledgeto take a decision. (P 13, Fg 4) ‘‘Yes, you have to enjoyindependent work and the responsibility; you can’tbe a person that needs reassurance all the time.(P 14 Fg 4).
Although independent work was highly valued, it was seen as problematic as the nurses experienced a sense
oneliness during their daily work. The nurses discussederal reasons for this. First, each nurse had a greater
ber of patients to care for during a shift, at somesing homes as many as forty to fifty patients, creating assful working environment. Second, the ratio of
istered nurses to patients in nursing homes was lowern in acute-care settings. The nurses were acting asup leaders and administrators of care rather thanticipating in basic patient care, which was usually donenurse assistants. The nurses pointed to how thiscted professional feedback. They felt it was harder form to find someone to discuss with or ask for advice on aly basis. The nurses explained how they had to relyly on their personal experience and competence when
essing a patient. As articulated by one respondent:
‘‘In a way, you are left to the wolves when you work in anursing home, you are left to your own knowledge andskills, and you have to be quite confident, you can’t justopen a door and call for a colleague or a doctor’’(P 10, Fg 3).
4. Discussion
Our study is unique as it presents a truly positivepicture of nurses’ professional work in nursing homesand home-based care. Based on the findings in thepresent study, we argue that nursing in elderly care is acomplex and advanced professional role, requiringseveral years of previous experience in acute-caresettings. The nurses in this study were attracted towork in elderly care related to the autonomous andperson-centred nature of nursing. Their decision topractice elderly care was a conscious career choice, thussupporting Ellenbecker et al. (2008) suggesting thatnurses in elderly care are highly committed to their jobs.The nurses could clearly describe their everyday nursingpractice with a sense of professional pride. This suggeststhat these elderly care nurses had developed a strongprofessional identity closely related to what it meant tobe and act as a nurse in everyday nursing practice(Fagermoen, 1997).
The nurses’ work in elderly care was multifaceted andbased on long lasting relationships with patients, thussubstantiating the study by Vlachos (2012) where long-term relationships were perceived as beneficial for jobsatisfaction. With regard to future recruitment it isinteresting to note that independent and person-centredcare was put forward by student nurses as a reason tochoose elderly care (Carlson, 2013). Nursing homes andhome-based care are therefore probably most valuable asclinical placements. These placements can provide a
le 2
ples from the analysis process reflecting nurses’ perception of their work in elderly care.
eaning unit Sub category Category
ing able to follow your patients, some of them I met for
the first time ten years ago and that is something
I appreciate (P 22, F G 6)a
Caring for patients during long periods of time Establishing long-term relationships
e feeling you get when you have struggled with a
problem for several months, like trying to heal a venous
ulcer and then suddenly you see the result (P 1, F G 1)
Continuity in nursing care
hen you are new as a nurse your focus is on medical-
technical skills, it is so important during your training but
after some years/elderly care is so much more (P 17, F G 5)
A professional journey Nursing beyond technical skills
thing is ever black or white, what we do is much harder,
more assessments to be done and you need some
experience to see the full picture, I mean you have to
see your patient in a holistic way (P 7, F G 2)
Providing holistic care
u have to enjoy independent work and responsibility,
you can’t be a person that needs reassurance all the time
(P 14, F G 4)
Independent work sense of loneliness Balancing independence with a
hen you work in a hospital you are never really left on
your own, you have all that equipment and staff and
doctors, but here you are on your own, it is your decision
that counts and that is hard, very hard (P 27, F G 7)
Nursing as solitary work
P indicates participant and F G stands for Focus Group i.e. P 22, F G 6 = participant number 22 in focus group number six.

E. Carlson et al. / International Journal of Nursing Studies 51 (2014) 761–767766
learning environment where the essence of caring andnursing can be explicit helping student nurses shaping anddeveloping professional identity (Carlson and Bengtsson,2013). The nurses’ desire to establish long-term relation-ships can be seen as a reaction to what has been discussedby Heaslip and Boarde (2012) as a strategy among nursesto focus on the technological aspects of care to protectthem from feeling vulnerable. They concluded that nursinginvolves emotional, intellectual and physical commitmentto patients. This is concordant with our findings whennurses pointed to the relational aspect of their work, andthe continuity of the nursing care they provided incollaboration with patients and families. The significanceof meaningful relationships with patients and families isfurther substantiated in a phenomenological study by deGuzman et al. (2009). They proposed that nurses ingeriatric care develop a special kind of relationships withelderly patients based on holistic care that is caring for thephysical, mental, emotional and spiritual wellbeing of theolder person. Dewar and Nolan (2013) presented apromising model to promote what is referred to as‘appreciative caring conversation’ (p.4) required to realiserelationship centred care in practice. This is a model wefind interesting to test and implement in the Swedishcontext where our study took place as a means ofilluminating the meaning of holistic and relational nursingin elderly care.
Balancing independence and loneliness is a uniquefeature of elderly care. The ability to handle that balancerequires several years of experience, and is one part ofbeing professional. Professional identity is reshaped andevolves throughout a nurse’s professional life (Johnsonet al., 2012). In the current study, the evolution ofprofessional identity can be exemplified by nursesdescribing how their thoughts on nursing had changedfrom a technical to a relational and holistic aspect, or in thewords of Ohlen and Segesten (1998) from working as anurse to being a nurse. Nurses in our study described howconfident and knowledgeable they felt in relation to thedecisions they had to make without the immediate supportfrom physicians. This suggests that elderly care nurses, dueto maturity and tenure, have developed a strong sense ofprofessional autonomy encompassing confidence, knowl-edge and personal courage to act as conceptualised by Skar(2009). However, it needs to be noted that nurses in thecurrent study expressed a sense of loneliness in daily workdespite their appreciation of having professional auton-omy. This implies that collaboration with peers and co-workers might be as important as building relationshipswith patients. Ellenbecker (2001) as well as Prentice andBlack (2007) pointed to how respectful professionalrelationships between nursing colleagues and physiciansinfluenced positively on job satisfaction and retention. Onthe other hand, Choi et al. (2011) reported that therelationship between nurse and physician was notsignificantly associated to higher RN job satisfaction, andit was suggested that the collaboration with physicianswas a less critical issue in nursing homes than in acute-caresettings. Why this should be the case is not explained,rather based on our findings, we would argue thatcollaboration with physicians and being able to share
the burden of complex decisions are as important innursing homes as in acute-care settings.
Therefore, building on the current study, the aspect of asense of loneliness needs to be elaborated upon. We proposefurther research on emotional stress and the psychosocialaspects of lonely work, and how these factors mightinfluence job satisfaction. In addition, we recommend thatmodels for clinical supervision (CS) are discussed andpossibly implemented in elderly care practice. Begat et al.(2005) described CS as a structured model for reflection andproblem solving where nurses can become clear about whythey think and act in certain ways. Improved patient care,stress reduction, and enhanced job satisfaction werepresented as perceived benefits of CS. We suggest that CSmost likely hold the potential to support not only personalbut also professional development thus strengthening theprofessional identity.
4.1. Limitations
Our study was situated in Southern Sweden, and theorganisation of elderly care which might have impacted thefindings is thus restricted to a Swedish context, and cannotbe widely generalised. Another limitation is the possibilitythat participants might have withheld vital information toavoid conflict or voicing critical views. However, the firstauthor (EC) started the interviews by explaining that no datacould be traced to any individual and that participantswould remain anonymous. In addition, the focus groupswere characterised by lively discussions, and participantsseemed comfortable and open when sharing their thoughts.Moreover, the interviews started with informal small talk inan effort to create a respectful and friendly atmosphere.However, it can be argued that we present an overly positiveview on nurses’ professional work in elderly care. This can beattributed to the question of purposive sampling andrespondent bias. One reason might be that the participantswho volunteered were those who had made a conscious andrational career choice, and thus developed a strongprofessional identity as nurses in elderly care. Note thatthe mean age of the participants was 46 years and most ofthem had worked for more than 20 years. This implies agroup of confident and autonomous nurses with nointention to leave. Age and tenure have previously beendescribed as variables related to intention to stay and jobsatisfaction (Ellenbecker, 2004; Ellenbecker et al., 2008). Inaddition, as we did not find any differences according todemographic variables or type of care settings no compar-isons were conducted. On the contrary, the participantsdiscussed professional work in terms related to theirrelationships to patients and their relatives, not in termsof how that work was organised or whether it took place inrural or urban settings. We would therefore interpret this asstrength of the study contributing to the unique character ofthe positive picture of elderly care we have presented. Wealso need to acknowledge the fact that no formal memberchecking was performed as we did not want to add to thenurses’ work load. However, we achieved what Sandelowski(1993) refers to as informal member checking, by raisingfollow-up questions during the interviews as a means toseek clarification or elaboration of meaning and intention.

5. C
termproproimpsomandaspatticarreta
dec
Eth
EthholFun
graDevSw
Ack
regthe
Ref
Bega
Carl
Carl
Cho
Cow
Cres
de G
Dew
Elle
E. Carlson et al. / International Journal of Nursing Studies 51 (2014) 761–767 767
onclusion
Our study shows that the opportunity to develop long- relationships, execute professional autonomy, and
vide holistic care are all central to registered nurses’fessional work in elderly care. The findings areortant as they represent positive alternatives to theewhat prevailing view on elderly care as depressing
undemanding. Nurse educators might use the keyects as good examples, thus influencing student nurses’tudes towards elderly care in a positive way. Elderlye agencies might find them helpful when recruiting andining nurses to a much needed area.
Conflict of interest: No conflict of interest has beenlared by the authors.
ical approval: The study was approved by the localical Advisory Board at the university where the authorsd their positions.ding: This research was made possible by generousnts funded by the Postdoctoral Programme for Qualityelopment in Higher Education at Malmo University,
eden.
nowledgements
The authors also wish to extend their gratitude to all theistered nurses participating in the study for sharingir time and experience.
erences
t, I., Ellefsen, B., Severinsson, E., 2005. Nurses’ satisfaction with theirwork environment and the outcomes of clinical nursing supervisionon nurses’ experiences of well-being—a Norwegian study. Journal ofNursing Management 13, 221–230.son, E., 2013. Meaningful and enjoyable or boring and depressing?The reasons student nurses give for and against a career in aged care.Journal of Clinical Nursing (in press).son, E., Bengtsson, M., 2013. The uniqueness of elderly care: regis-tered nurses’ experience as preceptors during clinical practice innursing homes and home-based care. Nurse Education Today,http://dx.doi.org/10.1016/j.nedt.2013.07.017.i, J.S., Flynn, L., Aiken, L.H., 2011. Nursing practice environment andregistered nurses’ job satisfaction in nursing homes. Gerontologist 52(4) 484–492.in, L.S., Johnson, M., Craven, R.G., Marsh, H.W., 2008. Casual modelingof self-concept, job satisfaction and retention of nurses. InternationalJournal of Nursing Studies 45, 1449–1459.well, J.W., Miller, D.L., 2000. Determining validity in qualitativeinquiry. Theory into Practice 39 (3) 124–130.uzman, A.B., Dangoy, R-J., David, K.C., de Claro, K.A., de Guzman, G., deJesus, G.I., 2009. How many sides does a coin have? A phenomenologyof Filipino nurses’ motivation and attitudes toward geriatric care.Educational Gerontology 35, 260–276.ar, B., Nolan, M., 2013. Caring about caring: developing a model to
implement compassionate relationship centered care in an olderpeople care setting. International Journal of Nursing Studies, http://dx.doi.org/10.1016/j-ijnurstu.2013.01.008.nbecker, C.H., 2001. Home health care nurses’ job satisfaction: asystem indicator. Home Health Care Management & Practice 13 (6)462–467.
Ellenbecker, C.H., 2004. A theoretical model of job retention forhome health care nurses. Journal of Advanced Nursing 47 (3)303–310.
Ellenbecker, C.H., Porell, F.W., Samia, L., Byleckie, J.J., Milburn, M., 2008.Predictors of home healthcare nurse retention. Journal of NursingScholarship 40 (2) 151–160.
Ellenbecker, C.H., Cushman, M., 2012. Home health care nurse retentionand patient outcome model: discussion and development model.Journal of Advanced Nursing 68 (8) 1881–1893.
Fagermoen, M.S., 1997. Professional identity: values embedded in ameaningful nursing practice. Journal of Advanced Nursing 25,434–441.
Freeman, T., 2006. ‘Best practice’ in focus groups: making sense ofdifferent views. Journal of Advanced Nursing 56 (5) 491–497.
Heaslip, V., Boarde, M., 2012. Does nurses’ vulnerability affect their abilityto care? British Journal of Nursing 21 (15) 912–916.
Johnson, M., Cowin, L.S., Wilson, I., Young, H., 2012. Professional identityand nursing: contemporary theoretical developments andfuture research challenges. International Nursing Review 59, 562–569.
Karsh, B., Booske, B.C., Sainfort, F., 2005. Job and organizational determi-nants of nursing home employee commitment, job satisfaction andintent to turnover. Ergonomics 48 (10) 1260–1281.
Kitzinger, J., 1994. The methodology of focus groups: the importance ofinteraction between research participants. Sociology of Health andIllness 16, 103–121.
Kloster, T., Høie, M., Skar, R., 2007. Nursing students’ career preferences: aNorwegian study. Journal of Advanced Nursing 59, 155–162.
Levett-Jones, T., Lethlean, J., McMillan, M., Higgins, I., 2007. Belonging-ness: a montage of nursing students’ stories of their clinical place-ment experiences. Contemporary Nurse 24, 162–174.
Lincoln, Y.S., Guba, E.G., 1985. Naturalistic Inquiry. SAGE Publications,Beverley Hills, CA, pp. 332–356.
Malterud, K., 2001. Qualitative research: standards, challenges and guide-lines. Lancet 358, 483–488.
McLafferty, I., 2004. Focus group interviews as a data collecting strategy.Journal of Advanced Nursing 48 (2) 187–194.
National Board of Health and Welfare, 2012. Competence in Geriatricsand Gerontology-suggestions for design and implementation of edu-cational resources.(Okad kompetens inom geriatrik och gerontologiforslag till utformning och genomforande av satsning). (In Swedish).
Polit, D.F., Beck, C.T., 2006. Essentials of nursing research: methods,appraisal, and utilization, 6th ed. Lippincott, Williams and Wilkins,Philadelphia.
Prentice, D., Black, M., 2007. Coming and staying: a qualitative explora-tion of registered nurses’ experiences working in nursing homes.International Journal of Older People Nursing 2, 198–203.
Sandelowski, M., 1993. Rigor or rigor mortis: the problem of rigor inqualitative research revisited. Advances in Nursing Science 16 (2) 1–8.
Shaffir, W., Pawluch, D., 2003. Occupations and professions. In: Reynolds,L., Herman-Kinney, N. (Eds.), Handbook of Symbolic Interactionism.AltaMira Press, Walnut Creek, CA, pp. 893–913.
Skar, R., 2009. The meaning of autonomy in nursing practice. Journal ofClinical Nursing 19, 2226–2234.
Statistics Sweden, 2011. Trends and forecast for education and labourmarket—revised 2012-11-09.(Trender och prognoser om utbildningoch arbetsmarknad). (In Swedish)http://www.scb.se/2013-02-01.
Stevens, J.A., 2011. Student nurses’ career preferences for working witholder people: a replicated longitudinal survey. International Journalof Nursing Studies 48, 944–951.
Tong, A., Sainsbury, P., Craig, J., 2007. Consolidated criteria for reportingqualitative research (COREQ): a 32-item checklist for interviews andfocus groups. International Journal for Quality in Health Care 19 (6)349–357.
Vlachos, S., 2012. Nurse Satisfaction in Caring for Elders. Paper 20.(Honors Theses)http://scholars.unh.edu/honors/20.
World Health Organization, 2006. World Health Report 2006: WorkingTogether for Health. World Health Organization, Geneva.
WMA. 2008. www.wma.net/en/30publications/10policies/b3/index.html(01.10.13).
Ohlen, J., Segesten, K., 1998. The professional identity of the nurse:concept analysis and development. Journal of Advanced Nursing 28(4) 720–727.