Embed Size (px)
Citation preview

Rehabilitation for PoTSPoTS UK Masterclass
Dr Jane Simmonds MCSP MACP SFHEAD Prof, MA, PGDip, B App(Sc), BPEProgramme Lead: MSc Paediatric PhysiotherapyPhysiotherapy Lead Hypermobility Unit, Hospital of St John and St Elizabeth

Plan
• Share an approach to rehabilitating people with PoTS• Integrating key PoTS exercise related research• Anecdotal experience
• Case studies.

AcknowledgmentsPatientsDr Nelly NinisProfessor Christopher MathiasProfessor Rodney GrahameDr Alan HakimDr Hanadi KazkazDr Inge de WandeleDr David Low Professor Peter Rowe.

Interest started with complex referrals• Joint laxity/ hypermobility / joint instability (hEDS/ HSD)• Persistent widespread pain• Persistent fatigue• Pre syncope and sometimes fainting• Temperature dysregulation• Gastrointestinal symptoms - reflux, slow transit• Bladder symptoms – irritable bladder, incontinence• Allergies - rashes

Onset

GImanifesta,ons
CardiacDysautonomia
Musculoskeletal
Allergy/MAC
Pain
Fa,gue
Bladder
systemicseverityscaleNinis,deWandele&Simmonds2013
MentalHealth

GImanifesta,ons
CardiacDysautonomia
Musculoskeletal
Allergy/MAC
Pain
Fa,gue
Bladder
systemicseverityscaleNinis,deWandele&Simmonds2013
MentalHealth

GImanifesta,ons
CardiacDysautonomia
Musculoskeletal
Allergy/MAC
Pain
Fa,gue
Bladder
systemicseverityscaleNinis,deWandele&Simmonds2015
MentalHealth

GImanifesta,ons
CardiacDysautonomia
Musculoskeletal
Allergy/MAC
Pain
Fa,gue
Bladder
systemicseverityscaleNinis,deWandele&Simmonds2013
MentalHealth

Problembasedapproach-Exploreexpecta7ons-Choice

Rehabilitation PrinciplesEducation: Reassurance Pacing – fatigue and pain managementAgree and set realistic goals
Anxiety management • Cognitive Behavioural Therapy, Relaxation, Mindfulness, Hypnosis• Hyperventilation - Breathing ExercisesSleep management• Sleep routine • Timing of food and exercise• Screen time• Sleepio App

Monitor medications: often complex cocktailAdvise on non pharmacological treatments• Compression garments – aid venous return• Fluids and salt – maintain blood volume• Dietary advice – small meals, low carbohydrate, FODMAPS
Design and implement exercise reconditioning programme* Evidence suggests that orthostatic intolerance and PoTS
are related to deconditioning (Fu et al., 2010; Parsaik et al., 2012; Sheldon et al., 2016)
Cause or Effect?

Monitor medications: often complex cocktailAdvise on non pharmacological treatments• Compression garments – aid venous return• Fluids and salt – maintain blood volume• Dietary advice – small meals, low carbohydrate, FODMAPS
Design and implement exercise reconditioning programme* Evidence suggests that orthostatic intolerance and PoTS
are related to deconditioning (Fu et al., 2010; Parsaik et al., 2012; Sheldon et al., 2016)
Cause or Effect?Regardless of the relationship – deconditioning negatively influences cardiovascular function

Premise: Long term benefits of improved physical fitness counteract orthostatic intolerance• Increased blood volume• Increased cardiac output• Enhanced vascular compression due to increased muscle
mass and tone• Improved endothelial function• Improved baro-reflex function

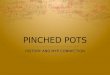
CaseControlStudy:19casesofPoTSand16healthycontrols3monthgraduatedexerciseinterven7onResults• 10/19casesnolongermetthediagnosisofPoTS• Significantreduc,oninuprightheartrate• Allimprovedqualityoflife(SF36)

Growing evidence for exercise as alternative to medication
Side effects of medication – lead to cessation• Beta blockers – fatigue• Fludrocortizone – hypokalemia• Alpha adrenergic agonists - hypertension
Galbreath et al., 2016 Clin Auton Res, 21, 73-80

Exercise Reconditioning ProgrammeAims : improve cardiovascular fitness and lower limb strength
Cardiovascular exerciseStart with chair peddles, reclining bicycle, rowing and swimmingProgress to upright position
During exercise, people with PoTS have a low stroke volume response to exercise – leads to light headedness, dizziness, dyspnoea and weakness

Resistance / Strength Training• Body weight• Weights • Elastic bands
Resistance training is more demanding on the circulatory system. Lead to changes in blood pressure. Avoid Static exercise and Valsalva hold breath – increase in BP, followed by a fall in BP

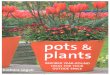
How Often and How Hard? Frequency and Intensity of ExerciseFirstmonth3-4perweek:RecliningexerciseCVtraining(20-40min)1xperweek:Resistancetrainingperweek(15–20mins)RPE6-16
Secondmonth3-4perweek:UprightbikeCVtraining(25-34mins)2xperweek:Resistancetrainingperweek(20-25mins)RPE6-18
Thirdmonth3-4perweek:UprightCVtraining(35-40mins)Crosstrainer/walking2xperweek:Resistancetraining(30mins)RPE8-18
Georgeetal.,2016HeartRhythm,13,943-50
RateofPerceivedExer7ons

My Reality - Frequency and Intensity of Exercise
FirstMonth4-5perweek:RecliningexerciseCVtraining(2-10mins)4-5xperweek:Resistance&propriocep,ontrainingperweek(2-10mins)RPE6–9:Graduateby10%perweekSecond–ThirdMonth4-5perweek:Uprightbike/WalkingCVtraining(10–30mins)4-5perweek:Resistance&func,onaltrainingperweek(10–20mins)RPE6-13Fourth–SixMonth3-4perweek:Uprightbike,Walking,Crosstrainer(30-40mins)2-3xperweek:Resistance&func,onaltraining(20mins)RPE9-18
Georgeetal.,2016HeartRhythm,13,943-50

GImanifesta,ons
CardiacDysautonomia
Musculoskeletal
Allergy/MAC
Pain
Fa,gue
Bladder
systemicseverityscaleNinis,deWandele&Simmonds2015
MentalHealth

Case Two
ManagementComplexpharmacologicalmanagementforPoTSandMastCellAc,va,on• Fluidsandsalt• Dietaryadvice• SchoolingplanFunc7onalrestora7onprogrammeNormalisemovementGaitreeduca,onHydrotherapyGraduatedcardiovascularandresistancetrainingBike,crosstrainer,squats,weightsarmsandlegs,legpressGoalsCompleteGCSE’sBeabletogoshoppingonthehighstreetStayoverwithfriendsandholiday

Tips for Rehabilitation
GivehopeHolis,cviewProblemsolvingFindthebaselineProgresssteadypaceDrinkbefore,duringandaberPsychologyGraduateslowlyUnderlyingHSD–likelytobeveryweakanddecondi,onedwithporrpropriocep,on.Needtoincorporatestabilitytraining.