Embed Size (px)
Citation preview

President Obama Bench Bedside
Release Criteria for Hematopoietic Stem Cell Therapies
Curt Civin, Nancy Hardy, Tami KingsburyUniversity of Maryland School of Medicine
CASSS Feb 9, 2017

Financial disclosure Drs. Civin and Kingsbury own
shares and serve on the board of 3DBioWorks Inc, a small privately-held biotechnology company which develops stem cell expansion and bioreactor technology.
The University of Maryland holds patents on bioreactor technologyand related inventions.
These arrangements are being managed by the University in accordance with its conflict of interest policies.
Dr. Hardy has nothing to disclose.

Release Criteria for Hematopoietic Stem Cell Therapies
Overview: HSCs and HSCT Curt Civin MD
Conceptual basis for standards and quality control
Genetic Engineering of HSCs for Blood Diseases Tami Kingsbury PhD
Considerations for which new standards and QC needed
Clinical Use of HSCT Nancy Hardy MD
Current standards and QC (i.e. “Release Criteria” for HSCT Grafts)

Overview: HSCs and HSCT
Curt I. Civin, MDAssociate Dean for Research, University of Maryland School of Medicine
Director, Center for Stem Cell Biology & Regenerative MedicineProfessor of Pediatrics and Physiology

Hematopoiesis is essential to human life
~200x109 cells produced per day
HSPCs are the cells most sensitive to radiation and most antineoplastic
chemotherapy
Homeostatic and reactive production of all cells of the
blood and immune system for over a lifetime

Functions of HSCT preparative radiochemotherapy regimens
Create hematopoietic space in the recipient Reduce numbers of endogenous HSCs that compete with
the donor graft Esp, delete endogenous HSCs occupying the hematopoietic
nicheImmunosuppress the recipient Prevent grant rejection (host vs graft)
Note: Radiochemotherapy may benefit the cancer patient, but does only harm to the patient w/ non-malignant disorder Reduced intensity (non-myeloblative) regimens

Important features of HSCT graftsVolume: with respect to recipient cardiac/renal functionCryoprotectant: limit DMSO cardiac/renal toxicitiesHematopoietic Capacity: engraft and support full donor-derived lympho-hematopoiesis in the recipient for lifetime
Leukocytes Colony-forming cells CD34+ cells CD34+ cell subsets
Immunologic potential: graft vs leukemia, graft vs host disease (biggest toxicity of HSCT)
T, B, NK lymphocyteso Graft vs tumor potentialo Alloreactive potential
Cancer potential Contaminating cancer cells in autologous HSCT for cancer Leukemogenicity of unintended genetic modifications in HSCT gene therapy

Purified CD34+ HSPCs for research and clinical transplantation
Civin, J Immunol 1984

CD34+ cell subsetsHSC
CD34+/CD38-/Lin-
Mature Blood & Immune Cells
CLP CMP EP
CD34+/[CD38/Lin]++
Human CD34+/CD38-/Lin- HSC cell subset:
contains most of the primitive in vivo-engrafting HSCs includes few of the less primitive hematopoietic single-lineage-committed progenitor cells
CD34+/[Lineage/CD38]++ subset: enriched in later hematopoietic progenitors depleted of HSCs
HPC

Hematopoiesis in the nicheSelf-renewal
ProliferationTrumpp 2010
Kaplan, The Biomedical Engineering Handbook 2010

HSPC transplant
The CD34 antibody is widely, but not always, used to purify HSPCs for HSCT
Civin, J Clin Oncol 1996

Stem cells
Multipotentprogenitors
Committedprogenitors
Mature cells
Regulators:
IL-1 IL-6 G-CSFIL-3 IL-11 GM-CSFG-CSF IL-4 M-CSFIL-2 IL-6 Epo IL-7
HSC self-renewal is limited, in vitroSCF TPO FL
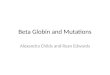
The ultimate stem cells: Pluripotent embryonic stem cells can self-renew indefinitely and generate all types cells of a mouse in vitro and contribute to all of the tissues and organs of a mouse in vivo
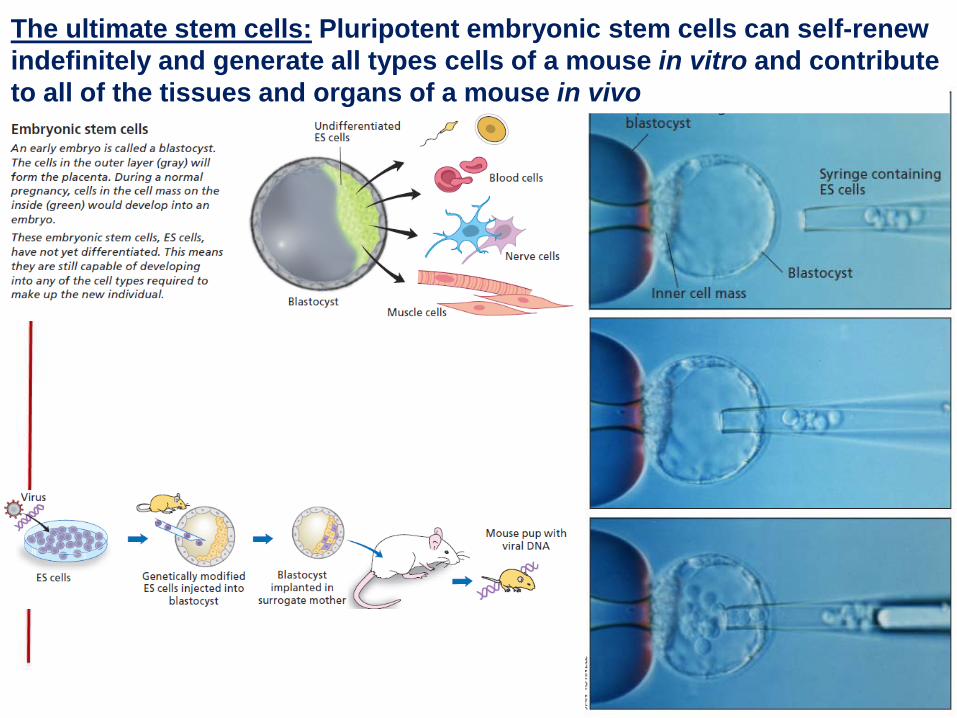
We had thought and taught that differentiation could be only a one-way trip in mammals

Differentiation of human ES cells (or iPSCs) into blood cells
Day 2: Differentiating
human embryonicstem cell
aggregates called “embryoid bodies” 1-2 weeks later:
Many differentiating human embryoid
bodies
Zambidis, Blood 2005
2 weeks later: Coloniesof functional blood cells
But lots of work and ES cells generate only a few mature blood cells, and no HSCs.
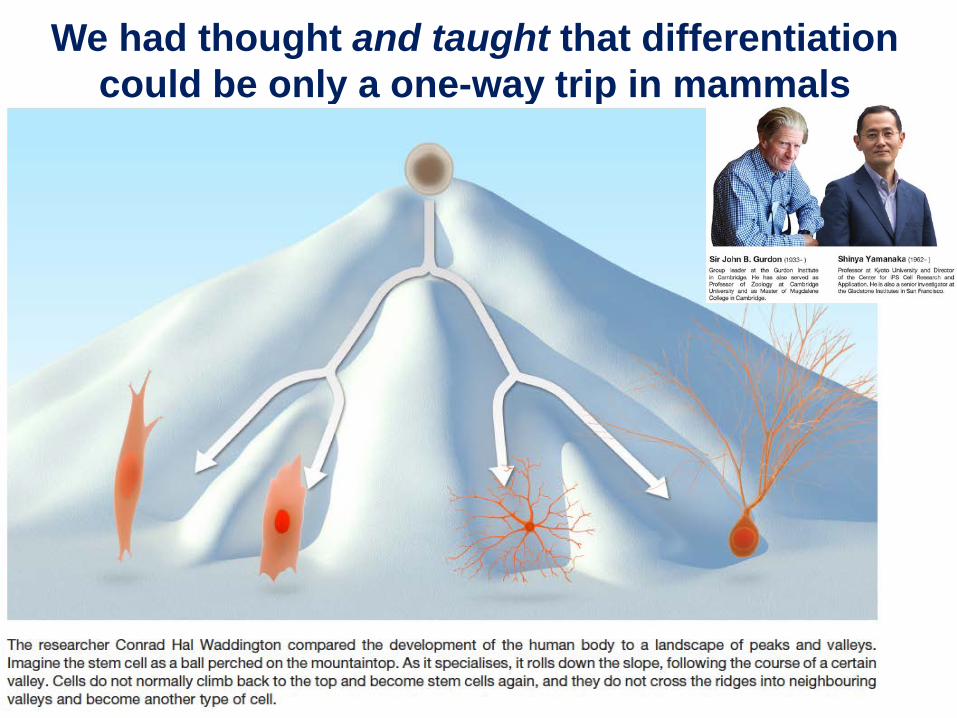
Reprogramming procedures are being enhanced: more efficient and safer iPSCs

Leukemias can originate in HSPCsTheir longevity and (self-)renewal capacity make stem(-progenitor) cells susceptible to the acquisition of both initiating and secondary oncogenic mutations (in the same cell): Theory: Stem(-progenitor) cells persist long enough to accumulate
the multiple oncogenic hits necessary for cancer development Theory: Stem(-progenitor) cells are already programmed to
generate huge clones of identical or similar progeny cells Fact: Gammaretroviral vector-mediated IL2RG gene transfer into
autologous human CD34+ HSPCs and subsequent transplantation resulted in activation of LMO2 and other proto-oncogenes, and T-cell leukemias developed in 4 of the 9 patients

Donor-Derived Brain Tumor Following Neural Stem Cell Transplantation in an Ataxia Telangiectasia Patient
First case of tumor development in a human following (fetal = “adult”) stem cell therapy, though similar findings have been made when embryonic stem cells were injected into rats.
The immunologic deficits of the boy’s A-T may itself have allowed the allogeneic tumors to develop.
Amariglio et al, PLOS Med, Feb 2009
QuickTime™ and a decompressor
are needed to see this picture.

Genetic Engineering of HSCs for Blood Diseases
Tami Kingsbury PhDAsst Professor of Physiology
Center for Stem Cell Biology & Regenerative MedicineUniversity of Maryland School of Medicine

Gene Editing
What determines off-target site binding and cleavage despite mismatches in sgRNA?What dictate INDEL biases for a given sgRNA? How can we improve HDR efficiency and increase conversion track length?
Nucleases generate DSBs at target site (and off-target sites)
Ran Nature Protocols, 2013

MSCRF project: Genetic Modification of Sickle Cell Disease in Hematopoietic Stem Cells
Disrupt the DNA encoding an erythroid-specific enhancer that regulates levels of BCL11A via CRISPR/Cas9 genome editing
technology of human HSCsCurt Civin, Wen-Chih Cheng, MinJung Kim, Tami Kingsbury
HbS(α2βs
2)http://www.nhlbi.nih.gov/health/health-topics/topics/sca
Gene Editing to Treat Disease

BCL11A enhancer SNPs reduce SCD phenotypes via increasing g-globin production in adult erythrocytes
BCL11A (transcriptional repressor)
γ-globin
fetal hemoglobin, HbF, α2γ2
Patients with HPFH have reduced severity of SCD because HbS polymerization is inhibited by HbF
HPFH patients have rare SNPs in the enhancer of BCL11A that specifically disrupt BCL11A expression in erythroidcells
Bauer, D.E. et al. Science 342, 253-257 (2013).

Individuals with hereditary persistence of fetal hemoglobin syndrome (HPFH) contain SNPs in their genomes that reduce
sickling and complications of Sickle Cell Disease SCD HPFH Modify BCL11A in SCD
Hardison & Blobel, Science 341:206, 2013

sgRNA sites near critical GATA binding site
sgRNA sites are limited by PAM sequences

Sequencing INDELS

- + - + - +
K562 HSPCs
C.Cas9
Cas9 +sgRNA
Cas9 +sgRNA
CRISPR/Cas9 editing of K562 leukemia cell line vsprimary CD34+ HSPCs
50-60% <10%
Gene editing requires an efficient method to deliver editing reagents to cells of interest
Low yield of edited cells may impact safety, although in some cases, selective advantage conferred by editing may provide benefit even if editing was not efficiente.g. SCID-X1 mouse models: 1% not enough, but 10% is sufficient

Optimize CRISPR/Cas9 delivery to HSCs using Maxcyte flow electroporation
HSCs are very difficult to transfect, ~1% efficiency with high toxicity Maxcyte flow electroporation instrument is cGMP compliant, and is
already being used in clinical trials
57% viable
97% GFP+
Collaboration with Maxcyte: Madhusudan Peshwa, PhD and Linhong Li, PhD

Gene editing reagent formatsReagent format impacts editing efficiency, cell toxicity and genotoxicity
Cas9 can be delivered using:DNAmRNARNPvirus based strategies, (IDLV, Adeno)
Modified sgRNAs direct more efficient gene editing
For HR, repair templates are also required
www.mirusbio.com

Clinical Gene EditingMaximize specificity of editing nuclease
Develop new toolsSplit Cas9Chimeric nucleases
Zetsche, Nature 2015
Corrigan-Curay, Mol Therapy 2015
Optimize protocol

Clinical Gene Editing cont.Unbiased and global identification of off-target sites
SequencingGuide-seqDefine “rules” for off-target binding and cleavage
Develop appropriate cell-type specific assays to detect cell transformation
Assess impact of gene editing risks in context of background levels of DSBs and chromosome translocations (or generate alternative strategies-hit & run)

Clinical HSCT
Nancy Hardy MDAssociate Professor of Medicine, UMSOM
Director, Cellular Therapy LaboratoriesDirector, Allogeneic Stem Cell Transplantation
Medical Director, Cancer Center Quality and SafetyMarlene and Stewart Greenebaum Comprehensive Cancer Center

CELL THERAPY & TRANSPLANTATION

PRODUCT RELEASE
Autologous or Related-Donor Hematopoietic Stem Cells (HSC)• Current Good Tissue Practice:
prevent the introduction or transmission of communicable diseases
Unrelated HSC, Umbilical Cord Blood, T Cell Therapy, Gene Therapy• Current Good Manufacturing
Practice: specific requirements for identity, strength, quality, and purity
CHALLENGES➳Patient-directed products➳Customization
Red Cells, Plasma, CD34 ➳Clinical realities require
Exceptional Release

REGULATION OF HUMAN CELLS, TISSUES, AND CELLULARAND TISSUE-BASED PRODUCTS (HCT/PS)
361 ProductsNot subject to premarket clearance or approval• Minimally manipulated• Homologous use• Not combined• No systemic effect, function is not
dependent upon the activity of living cells, or it is intended for autologous use or allogeneic use in close relatives …
Minimally Manipulated: Processing that does not alter the relevant biological characteristics of cells or tissues:Density-gradient separation, cell selection, centrifugation, cryopreservation
351: HCT/P that are not 361Adulterated drugs and devicesUnrelated allogeneic HSC, Lymphocytes• Lymphocyte Immune Therapy• Gene Therapy Products

STANDARD
• Communicable disease testing (allogeneic)• HLA typing (allogeneic)• ABO group and Rh typing on 2 separate samples• Microbial testing after processing• Post-processing nucleated cell count and viability• Assay of target cell population for products that have been
enriched or depleted
The Processing Facility Director shall define tests and procedures for measuring and assaying cellular therapy products to:
- assure their safety, viability and integrity - document that products meet predetermined release specifications

PRODUCT RELEASE

HSC Release Criteria
Identity
Purity
Potency
Donor Screening

HSC Potency: Engraftment, Chimerism & Immunity
Allogeneic: Donor Chimerism
Engraftment: cell dose, viability, “stemness”• Hematopoietic recovery
• Confounders• Conditioning intensity• Histocompatibility, rejection• Disease, e.g., infection, damaged
marrow stroma, hypersplenism
Immune Reconstitution: CD34, T cell dose; viability• Therapeutic: Graft-versus-Leukemia
• Functional: Immunity• Confounders:
• Histocompatibility, Graft-vs-Host Disease
• Donor, recipient age, gender
PLT
ANC
TRM
OS
CD34 & Engraftment, Outcomes:Autologous vs Allogeneic

Alloreactive Potency: Graft-vs-Leukemia
Monitor: Graft-vs-Host Disease
Horowitz, M. M. et al. Blood 75:555, 1990
Relapse after Hematopoietic Stem Cell Transplantation: Syngeneic vs. T-cell Depleted vs. T-cell Replete
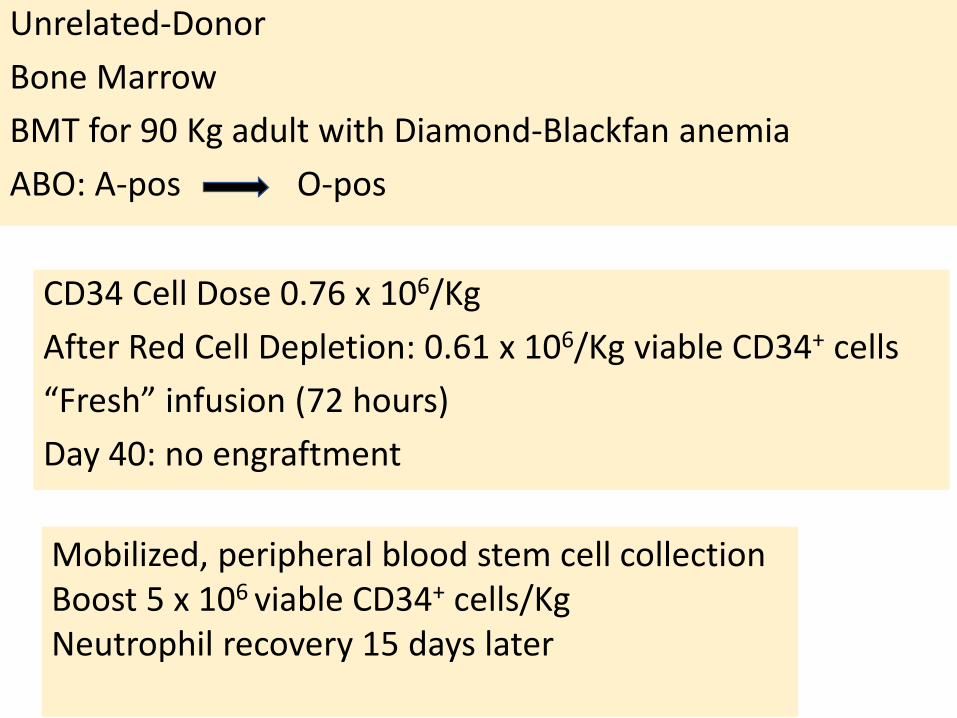
Unrelated-DonorBone Marrow BMT for 90 Kg adult with Diamond-Blackfan anemiaABO: A-pos O-pos
CD34 Cell Dose 0.76 x 106/KgAfter Red Cell Depletion: 0.61 x 106/Kg viable CD34+ cells“Fresh” infusion (72 hours)Day 40: no engraftment
Mobilized, peripheral blood stem cell collectionBoost 5 x 106 viable CD34+ cells/KgNeutrophil recovery 15 days later

Autologous PBSC 60 year-old “super-mobilizer” with MMCD34 Cell Dose: 4.8 x 106/Kg viable CD34+ cells
CD34 Boost: 2.4 x 106/Kg on ~ Day 14
CD34 Boost: 2.4 x 106/Kg on ~ Day 21
Neutrophil Engraftment: Day 29Engraftment Monitoring on All Products• Failures trigger investigation
• Neutrophils• Platelets• Donor Cells
• Potency• Fresh viable CD34+ cell dose• Fresh CFU dose

Effect of Overnight Storage Prior to Cryopreservation on Hematopoietic Engraftment after Autologous HPCT
ANC PLT 20K PLT 50K ANC PLT 20K PLT 50K ANC PLT 20K PLT 50K

Potency Assays
STEMCELL Technologies Inc. WHITE PAPER, 09/2012: “Potency” Assays for Measuring the Engraftment Potential of Hematopoietic Stem and Progenitor Cells.

Potency Assays for Release• Enumeration of viable CD34 cell dose and CFU dose
prior to cryopreservation correlate with engraftment
• Late engraftment may reflect viable cell loss with freeze/thaw
• Post-thaw enumeration of viable progenitors is limited
• DMSO effects on membrane integrity• Cell loss with washing; clumping, filtering• Rapid cell loss GM-CFC stability testing of thawed PBSC
products @ RT. The mean GM-CFC yield from the fresh harvests tested on immediate thaw was 68 ± 27%. British Journal of Haematology, 175, 5, 17 OCT 2016.
Biology of Blood and Marrow Transplantation 2010; 16, 500-508.
Flow cytometric evaluation of thawed Cord units. Modified gating more accurately measures viability.

• Tolerant: Transplant across HLA barriers• Progenitor cells have high “stemness” but marginal numbers• Quality and outcomes vary: collection, processing and
storage: sites; practices, procedures• Leukemic Clones in cord blood units???
Umbilical cord blood, 4/6 HLA match; Adult, GATA-2 deficiency and MDS CD34 Cell Dose: 0.787x106/KgCD3 Cell Dose: 3.48 x 106/KgNeutrophil Engraftment Day 76Donor Cell Leukemia ~ 16M after transplant
Umbilical Cord Blood• Collected at L&D• Processing @ CBB• Cryoshipped• Transplant Center Thaw, Infusion

TNC Dose Neutrophils
Platelets
CFC Dose Cell dose and engraftment after cord blood transplantation
Migliaccio et al. Blood 2000;96
Survival

Page et al., Biology of Blood and Marrow Transplantation, 17:9, 2011.
Postthaw
Postthaw CFU content best correlates with engraftment after Unrelated Umbilical Cord Blood Transplantation
Neutrophils
Platelets
Pre-Cryo

Umbilical Cord BloodMinimally Manipulated, Unrelated
Intermediate Product Requiring cGMP

Page et al., Biology of Blood and Marrow Transplantation, 17:9, 2011.

Aldehyde dehydrogenase (ALDH) is highly expressed in hematopoietic stem and progenitor cellsALDHbr CBU cells coexpress CD34 and CD133 and are highly enriched for CFUs
ALDHbr–based cord blood potency assay

Thawed segments vs fresh or thawed CB Units
ALDHbr–Based Cord Blood Potency Assay
Thawed cord blood segments
ALDHbr Cells & Engraftment
Cord blood segments
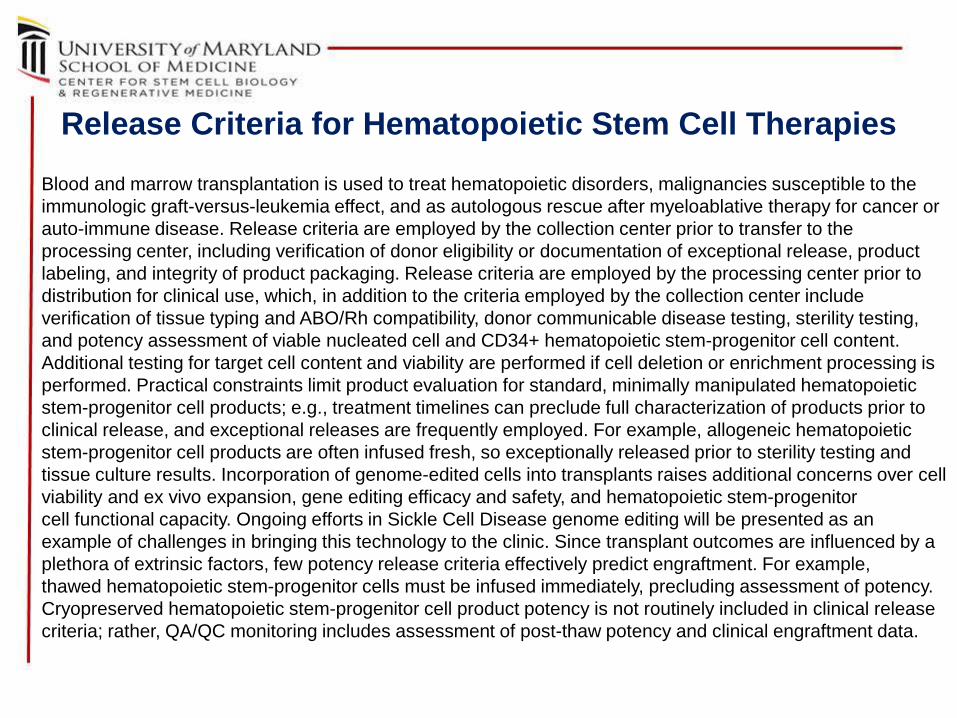
Release Criteria for Hematopoietic Stem Cell TherapiesBlood and marrow transplantation is used to treat hematopoietic disorders, malignancies susceptible to the immunologic graft-versus-leukemia effect, and as autologous rescue after myeloablative therapy for cancer or auto-immune disease. Release criteria are employed by the collection center prior to transfer to the processing center, including verification of donor eligibility or documentation of exceptional release, product labeling, and integrity of product packaging. Release criteria are employed by the processing center prior to distribution for clinical use, which, in addition to the criteria employed by the collection center include verification of tissue typing and ABO/Rh compatibility, donor communicable disease testing, sterility testing, and potency assessment of viable nucleated cell and CD34+ hematopoietic stem-progenitor cell content. Additional testing for target cell content and viability are performed if cell deletion or enrichment processing is performed. Practical constraints limit product evaluation for standard, minimally manipulated hematopoietic stem-progenitor cell products; e.g., treatment timelines can preclude full characterization of products prior to clinical release, and exceptional releases are frequently employed. For example, allogeneic hematopoietic stem-progenitor cell products are often infused fresh, so exceptionally released prior to sterility testing and tissue culture results. Incorporation of genome-edited cells into transplants raises additional concerns over cell viability and ex vivo expansion, gene editing efficacy and safety, and hematopoietic stem-progenitor cell functional capacity. Ongoing efforts in Sickle Cell Disease genome editing will be presented as an example of challenges in bringing this technology to the clinic. Since transplant outcomes are influenced by a plethora of extrinsic factors, few potency release criteria effectively predict engraftment. For example, thawed hematopoietic stem-progenitor cells must be infused immediately, precluding assessment of potency. Cryopreserved hematopoietic stem-progenitor cell product potency is not routinely included in clinical release criteria; rather, QA/QC monitoring includes assessment of post-thaw potency and clinical engraftment data.





![Limited Number of Globin Genes in HumanDNA10-7, or 0.198 ngof globin DNA.FromEq. [1] wecan calculate the %hybridization, P, expected for anynumberof globin gene copiespresent.Forexample,inExp.1,](https://img.pdfslide.net/doc/110x75/60e570f3b76c9678502ef0c0/limited-number-of-globin-genes-in-humandna-10-7-or-0198-ngof-globin-dnafromeq.jpg)