Embed Size (px)
Citation preview
378 AUSTRALIAN AND NEW ZEALAND JOURNAL OF PUBLIC HEALTH 2008 vol. 32 no. 4© 2008 The Authors. Journal Compilation © 2008 Public Health Association of Australia
Cancer Article
Reliability of collecting colorectal cancer stage
information from pathology reports and
general practitioners in Queensland
Interpretation of differences in cancer
survival between population subgroups
o r over t ime requi res accura te
information on cancer stage.1-3 However,
clinical stage is not routinely collected
by population-based cancer registries in
Australia or overseas. Some population-
based registries, such as the SEER program,4
EUROCARE5 and the New South Wales
cancer registry in Australia,6 report a
summary measure of stage that is based
on information from pathology reports or
medical records, however error rates between
12 and 35% for prostate, lung and breast
cancers have been reported.7-10
Collecting information on cancer stage using
resource-intensive methods such as reviews of
medical charts is not practical for large-scale
studies or population-based registries. GPs,
as the gatekeepers to more specialised cancer
services, are a potential source of information
about cancer stage, as are pathology reports.
A Western Australian study suggested that
colorectal cancer is probably the cancer most
Abstract
Objective: To investigate the reliability of
collecting colorectal stage information from
pathology reports and general practitioners
in Queensland, Australia.
Methods: A longitudinal study of colorectal
cancer survivors conducted in 2003 and
2004 (n=1966, response rate=57%)
obtained stage information from clinical
specialists (n=1334), general practitioners
(GP) (n=1417) and by extracting stage
from pathology reports (n=1484). Reliability
of stage information was determined by
comparing stage from GPs and pathology
reports with that reported by the clinical
specialists, using a weighted kappa.
Results: GPs and pathology reports each
had a similar level of agreement with
clinical specialists, with kappa scores of
0.77 (0.75-0.80) (n=1042) and 0.78 (0.75-
0.81) (n=1152), respectively. Results were
similar when restricting to records staged
by all three methods (n=847). GPs had
similar levels of agreement with clinical
specialists within each stage, although
pathology reports tended to under-stage
patients in Stage D (0.37). Collapsing
stage into two categories (A or B, C or D)
increased the reliability estimates from the
pathology reports to 0.91 (0.88-0.93), but
there was little change in GP estimates
0.79 (0.75-0.83).
Conclusions: Extractions from pathology
reports are a valid source of broad stage
information for colorectal cancer.
Implications: In the absence of clinical
stage data, access to pathology records by
population-based cancer registries enables
a more accurate assessment of survival
inequalities in colorectal cancer survival.
Aust N Z Public Health. 2008; 32:378-82
doi: 10.1111/j.1753-6405.2008.00259.x
Submitted: February 2008 Revision Requested: April 2008 Accepted: June 2008Correspondence to: Dr Peter Baade, Epidemiology Unit – Viertel Centre for Research in Cancer Control, The Cancer Council Queensland, PO Box 201, Spring Hill, Queensland 4004. Fax: 07 3258 2310; e-mail: [email protected]
Lauren J. KrnjackiEpidemiology Unit, Viertel Centre for Research in Cancer Control, The Cancer Council Queensland
Peter D. BaadeEpidemiology Unit, Viertel Centre for Research in Cancer Control, The Cancer Council Queensland and School of Public Health, Queensland University of Technology
Brigid M. LynchEpidemiology Unit, Viertel Centre for Research in Cancer Control, The Cancer Council Queensland
Joanne F. AitkenEpidemiology Unit, Viertel Centre for Research in Cancer Control, The Cancer Council Queensland and School of Population Health, Queensland University
amenable to obtaining stage from pathology
reports, with the limitation that information
on metastasis is often lacking.11
A longitudinal study of colorectal cancer
survivors12 collected stage information from
pathology reports, general practitioners
and clinical specialists in Queensland.
This paper reports on the reliability of this
stage information by comparing stage from
pathology reports and general practitioners
with that of clinical specialists.
MethodData were collected as part of the
Colorectal Cancer and Quality of Life
Study, a population-based, longitudinal
study of the predictors of quality of life up
to five years after diagnosis. Full details are
described elsewhere.12 Briefly, all eligible
cases of colorectal cancer were identified
through the Queensland Cancer Registry.
Study participants had a first, histologically
confirmed, primary diagnosis of colorectal

2008 vol. 32 no. 4 AUSTRALIAN AND NEW ZEALAND JOURNAL OF PUBLIC HEALTH 379© 2008 The Authors. Journal Compilation © 2008 Public Health Association of Australia
cancer between 1 January 2003 and 31 December 2004, and were
aged between 20 and 80 years at diagnosis. Of 3,426 eligible
participants, 1,966 (57.4%) completed a baseline telephone
interview. The University of Queensland’s Behavioural and
Social Science Ethical Review Committee approved the study’s
procedures.
Stage information from doctorsDuring the telephone interview, participants were asked to name
their treating doctor(s), including their GP, surgeon and medical
oncologist where applicable. Questionnaires were mailed to these
doctors approximately 12 months after the participant’s diagnosis,
requesting a range of clinical information including the stage at
diagnosis (based on the Australian Clinico-Pathological Staging
(ACPS) system). The ACPS system is essentially an extension
of the traditional Dukes staging method, and is based on a small
number of key variables: direct spread, lymph node metastases,
and known residual tumour.13 Reminder letters were sent at six
and 12 weeks. If the surgeon or medical oncologist preferred,
study personnel extracted the required information from medical
records, including letters of correspondence, outpatient notes,
operative reports, chemotherapy and radiation therapy charts, at the
treating hospital or the clinician’s rooms. In these record reviews,
stage was recorded only if it was stated explicitly in the record. No
effort was made to interpret stage from the clinical information
provided. When stage information differed between surgeons and
medical oncologists, the data from surgeons was used.
Stage information from pathology reportsA research officer trained in the interpretation of colorectal
cancer pathology reports extracted stage information from
pathology reports held by the Queensland Cancer Registry.
Documentation pertaining to the time up to two months post
diagnosis was reviewed. Tumour information was extracted from
the pathology report, using the ‘Tumour, Nodes, Metastasis’
(TNM) staging system.14 In the absence of information on
metastases (MX), it was assumed that there were no metastases
(MO). This method has been used previously in the extraction
of stage from pathology reports.11 The TNM was then classified
according to Australian Clinico-Pathological Staging. The
research officer did not attempt to stage if there was any ambiguity
regarding the level of invasion of the tumour from the information
on the pathology report. The records for 50 participants were
subsequently staged by a second reviewer to assess inter-rater
reliability.
Statistical AnalysesOther studies have suggested that stage data from clinical
records are generally considered to be the best available.10,15
These analyses focused on the reliability of stage information
obtained from pathology reports and GPs compared to clinical
specialists.
Reliability was determined by comparing reported stage
from each source to that reported by the clinical specialist,
using a weighted Kappa. The weighted Kappa calculates
the chance corrected agreement between reporters, and takes
into account the magnitude of the differences in agreement.
It has been suggested that Kappa estimates between 0.4-0.6
represent ‘moderate agreement’, 0.61-0.8 ‘substantial agreement’
and 0.81-1.00 ‘almost perfect agreement’.16 Confidence intervals
for the Kappa estimates were calculated using the bootstrap
method (1000 repetitions). Kappa estimates were also stratified
by (clinical specialist-defined) stage to determine the consistency
of agreement. Per cent agreement was calculated to assist
interpretation.
Pairwise comparisons with the stage reported by clinical
specialists were carried out separately for stage reported by
GPs and stage extracted from the pathology reports. In these
comparisons, records with missing stage information were deleted.
Since these two comparisons were then based on different (albeit
overlapping) samples, we also conducted pairwise comparisons
on those records that had non-missing stage information from all
three collection methods.
We assessed the impact that collapsing stage into broader
categories had on the measured levels of reliability. Five year
survival for Stage A is approximately 88%; 70% for Stage B;
43% for Stage C; 7% for Stage D.17 This supported the collapsing
of stage into ‘Local/Locally advanced’ (Stage A and B) versus
‘Regional/Distant’ (Stage C and D).
The current Australian treatment guidelines for colorectal
cancer recommend different treatment based on the stage of the
tumour.18 Those with Stage A are typically treated with surgery
alone. Patients with Stage C and D are recommended to have
chemotherapy. There is some ambiguity regarding treatment
for patients with Stage B depending on the prognosis and site
of the tumour. This supports the grouping of stage into likely
treatment groups of ‘surgery only’ (Localised – Stage A),
‘possible chemotherapy’ (Non-localised – Stage B) and ‘at least
chemotherapy’ (Regional and Distant – Stages C and D).
ResultsReporting of stage
Approximately 94% of participants had a report of stage
available from at least one of the three data sources. There were
1,950 participants (99.2%) who reported having been treated by
a clinical specialist, and of these, stage information was obtained
for 1,417 (72.6%). This combined clinical stage information was
based on surgical stage for 95.5% of patients, and was obtained
from medical oncologists for the remaining 4.5%. When stage
information was obtained from both surgeons and medical
oncologists (n=427), agreement was very high (92% concordance).
Nearly all (97.7%) participants reported having a regular GP,
and for 1,332 (69%) of these participants we obtained stage
information from the GP.
Since an eligibility requirement for this study was to have
histologically confirmed colorectal cancer, all respondents had
a pathology report available in the Queensland Cancer Registry.
Cancer Colorectal cancer stage information
380 AUSTRALIAN AND NEW ZEALAND JOURNAL OF PUBLIC HEALTH 2008 vol. 32 no. 4© 2008 The Authors. Journal Compilation © 2008 Public Health Association of Australia
Table 1: Comparisons between stage as provided by general practitioners and extracted from pathology reports, using the stage from clinical specialists as the comparison group.
Type of comparison Statistic Stage groups A, B, C, D A, B, C/D A/B, C/DPathology reportsAll comparisons (N=1,152)
W Kappa 0.78 (0.75-0.81) 0.83 (0.80-0.86) 0.90 (0.88-0.93)
% Agr 81.8 86.7 95.2
All three groups (n=847)
Kappa 0.79 (0.76-0.82) 0.84 (0.81-0.87) 0.91 (0.88-0.94)
% Agr 82.2 87.3 95.5
General practitionersAll comparisons (N=1,042)
Kappa 0.77 (0.75-0.80) 0.78 (0.75-0.81) 0.79 (0.75-0.83)
% Agr 79.3 84.1 89.5
All three groups (n=847)
Kappa 0.77 (0.74-0.80) 0.78 (0.74-0.81) 0.78 (0.73-0.82)
% Agr 80.4 83.7 89.1Notes:(a) Weighted Kappa – chance corrected agreement between reporters, taking into account the magnitude of the differences in agreement (include 95% confidence
interval)(b) % Agreement – proportion of exact stage agreement (c) All comparisons – when stage information available for both groups involved in the comparisons (eg. pathology extraction and clinical specialist).(d) All three groups – when stage information available for all three groups of pathology extraction, GP and clinical specialist.
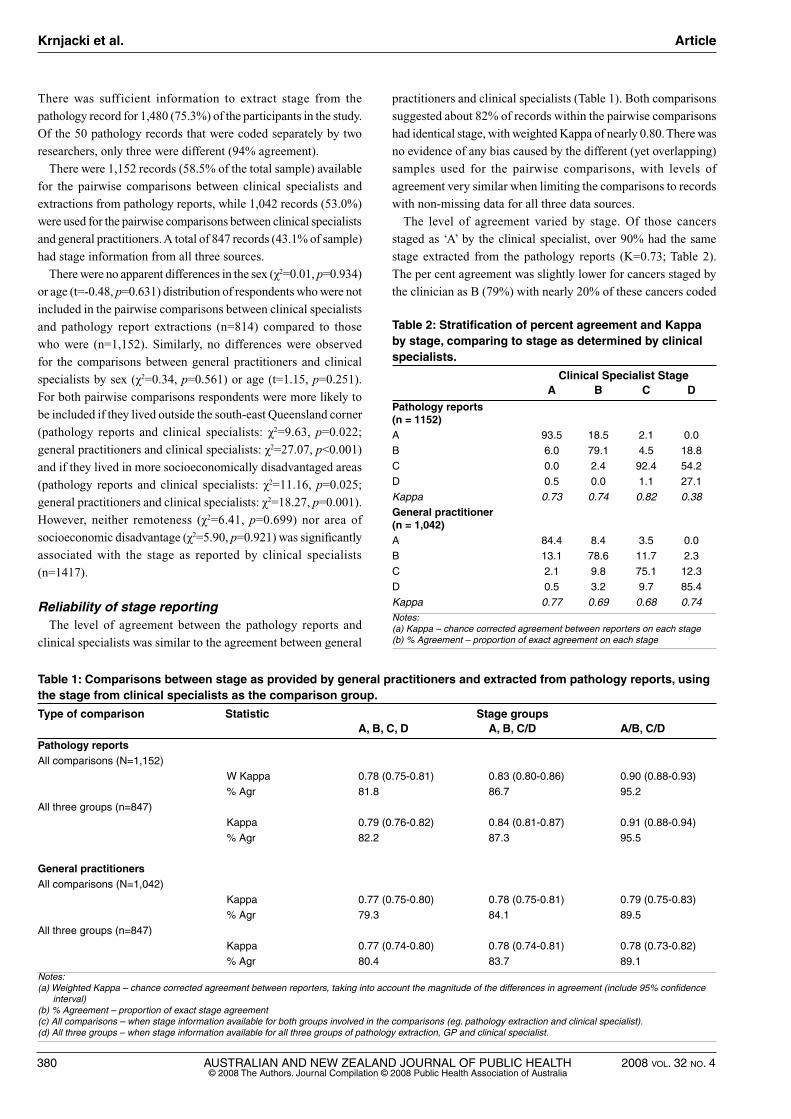
Table 2: Stratification of percent agreement and Kappa by stage, comparing to stage as determined by clinical specialists.
Clinical Specialist Stage A B C DPathology reports (n = 1152)A 93.5 18.5 2.1 0.0
B 6.0 79.1 4.5 18.8
C 0.0 2.4 92.4 54.2
D 0.5 0.0 1.1 27.1
Kappa 0.73 0.74 0.82 0.38
General practitioner (n = 1,042)A 84.4 8.4 3.5 0.0
B 13.1 78.6 11.7 2.3
C 2.1 9.8 75.1 12.3
D 0.5 3.2 9.7 85.4
Kappa 0.77 0.69 0.68 0.74Notes:(a) Kappa – chance corrected agreement between reporters on each stage(b) % Agreement – proportion of exact agreement on each stage
There was sufficient information to extract stage from the
pathology record for 1,480 (75.3%) of the participants in the study.
Of the 50 pathology records that were coded separately by two
researchers, only three were different (94% agreement).
There were 1,152 records (58.5% of the total sample) available
for the pairwise comparisons between clinical specialists and
extractions from pathology reports, while 1,042 records (53.0%)
were used for the pairwise comparisons between clinical specialists
and general practitioners. A total of 847 records (43.1% of sample)
had stage information from all three sources.
There were no apparent differences in the sex (χ2=0.01, p=0.934)
or age (t=-0.48, p=0.631) distribution of respondents who were not
included in the pairwise comparisons between clinical specialists
and pathology report extractions (n=814) compared to those
who were (n=1,152). Similarly, no differences were observed
for the comparisons between general practitioners and clinical
specialists by sex (χ2=0.34, p=0.561) or age (t=1.15, p=0.251).
For both pairwise comparisons respondents were more likely to
be included if they lived outside the south-east Queensland corner
(pathology reports and clinical specialists: χ2=9.63, p=0.022;
general practitioners and clinical specialists: χ2=27.07, p<0.001)
and if they lived in more socioeconomically disadvantaged areas
(pathology reports and clinical specialists: χ2=11.16, p=0.025;
general practitioners and clinical specialists: χ2=18.27, p=0.001).
However, neither remoteness (χ2=6.41, p=0.699) nor area of
socioeconomic disadvantage (χ2=5.90, p=0.921) was significantly
associated with the stage as reported by clinical specialists
(n=1417).
Reliability of stage reporting The level of agreement between the pathology reports and
clinical specialists was similar to the agreement between general
practitioners and clinical specialists (Table 1). Both comparisons
suggested about 82% of records within the pairwise comparisons
had identical stage, with weighted Kappa of nearly 0.80. There was
no evidence of any bias caused by the different (yet overlapping)
samples used for the pairwise comparisons, with levels of
agreement very similar when limiting the comparisons to records
with non-missing data for all three data sources.
The level of agreement varied by stage. Of those cancers
staged as ‘A’ by the clinical specialist, over 90% had the same
stage extracted from the pathology reports (K=0.73; Table 2).
The per cent agreement was slightly lower for cancers staged by
the clinician as B (79%) with nearly 20% of these cancers coded
Krnjacki et al. Article

2008 vol. 32 no. 4 AUSTRALIAN AND NEW ZEALAND JOURNAL OF PUBLIC HEALTH 381© 2008 The Authors. Journal Compilation © 2008 Public Health Association of Australia
instead as Stage A from the pathology reports. However, the kappa
estimate was similar (K=0.74) to that for Stage A. Agreement
with Stage C cancers was the highest of all stages (92%, K=0.82).
Agreement with Stage D cancers was lowest (27%; K=0.38), with
the majority (54%) of clinical Stage D cancers being coded instead
as Stage C from the pathology reports (Table 2).
In contrast, the level of agreement between clinician and GPs
was generally consistent across all stages (Table 2), with agreement
ranging from 75% to 85% (K= 0.68-0.77) for the four stages.
The level of agreement between GPs and clinical specialists
changed only slightly regardless of how the stage categories
were collapsed (Table 1). In contrast, the increased agreement
between pathology-reported stage and clinician stage for “A, B,
C/D” reflects the large proportion of clinician Stage D that were
coded as Stage C from pathology reports (Table 2). The even
higher agreement for “A/B, C/D” (Table 1) reflects the smaller
proportion of clinician Stage B that was coded as Stage A from
the pathology forms. The sensitivity and specificity estimates
(with specialist stage as the “true stage”) for this dichotomised
stage were 91.0% and 98.2% for pathology stage, and 88.3% and
90.5% for general practitioner stage.
Discussion This study found that the stage information extracted from
pathology reports had about 80% agreement with the stage
obtained from clinical specialists, and that this agreement
increased to 95% when collapsing stage to A/B and C/D. A
similar level of agreement between GPs and clinical specialists
was observed, however collapsing stage had little impact on the
levels of agreement.
When comparing the pathology-based stage with that of clinical
specialists, the most obvious difference was the under-reporting
of Stage D tumours when relying on pathology reports. This has
also been found for colorectal cancer stage in other Australian
states (New South Wales6 and Western Australia19). The lower
accuracy for more advanced cancers is due in large part to the
lack of information about metastases provided on the pathology
report.11 Only 14% of histology reports on colorectal cancer
tumours in the Western Australian Cancer Registry contained all
of the necessary information to be fully staged.19 Similarly, a study
conducted in New Zealand found that less than 4% of pathology
reports unequivocally reported the presence of metastasis.20
In contrast to the under-reporting advanced cancers of
pathology-based stage, the accuracy of GPs compared to clinical
stage were consistent across all four categories. Any disagreement
between GPs and specialist clinicians could reflect GPs having
access to less detailed clinical information and increased likelihood
of losing contact with the patient during the 12 months after
diagnosis.
Our study suggests that if four-level stage is required for research
purposes, then there would be a misclassification of stage of at least
20% using pathology records or GPs. The results for pathology
extractions are similar to those reported elsewhere for colorectal
cancer6 and other cancers.7-9,21 Using simulation analyses, Yu and
colleagues6 suggested that this imprecision could make previously
significant area-specific variation non-significant.
However, it is possible that a broader measure of stage could be
useful when used to adjust for disease spread in population-based
studies. The very high agreement between pathology extractions
and clinical specialists when the stage categories are collapsed
suggests a high degree of accuracy when using the collapsed
categories of ‘localised’, ‘locally advanced’ and ‘regional/distant’
and further into ‘localised/locally advanced’ and ‘regional/distant’.
This increase in agreement for the collapsed categories is not
simply due to fewer categories; the same process for GPs resulted
in very little change in the agreement.
Missing dataThere was insufficient information to extract stage from
approximately one-quarter (24.7%) of the pathology reports. This
proportion of missing data is considerably higher than the 14%
reported from the SEER registries22 and 18% in New South Wales.6
In this study, the pathology extracts were obtained by the research
officer as soon as possible after diagnosis, to facilitate prompt
recruitment for the main study. If additional relevant information
arrived in the cancer registry following recruitment of a patient,
then this subsequent information was not used in this study. A
subsequent review of 50 randomly selected cases that had missing
data in the main study noted that 18 (36%) of these were now able
to be staged. Assuming this proportion held across the remaining
missing records, it could reduce the per cent of missing pathology
stage to about 15%, within the range of other similar studies.
We did not include missing data in the reliability calculations.
This has particular relevance when stage information was available
from clinical specialists, but missing for the pathology reports
or general practitioners. Excluding these records may have over-
estimated the reliability estimates.
Limitations Estimates of agreement with clinical specialists for GPs and
pathology reports were based on pairwise comparisons using
different yet overlapping samples. Although this could potentially
bias the comparisons between the groups, when we repeated the
analysis using only those records with non-missing data from all
three sources very similar results were observed.
Only those people who agreed to take part in the initial study were
eligible to be staged. The relatively low response rate (57%), and
the under-representation of older (70 to 80 years) colorectal cancer
survivors, those with rectal cancer and those with more advanced
disease from the initial study12 may have implications for the
generalisability of these results. In particular the lower proportion
of patients with less advanced disease may have spuriously inflated
our reliability estimates. However, our findings were consistent with
those previously reported,11 in that stage information sourced from
pathology reports has least reliability when metastasis is involved,
and this limitation needs to be considered when sourcing stage
information from pathology reports.
Cancer Colorectal cancer stage information

382 AUSTRALIAN AND NEW ZEALAND JOURNAL OF PUBLIC HEALTH 2008 vol. 32 no. 4© 2008 The Authors. Journal Compilation © 2008 Public Health Association of Australia
ConclusionsThe ability to accurately interpret inequalities in cancer survival
between population subgroups or changes over time requires
accurate information on cancer stage.1-3 Since clinical stage
information is not being collected in Australian population-based
cancer registries, the uncertainty of whether observed inequalities
in colorectal cancer survival23-25 are due to differentials in diagnosis
patterns, treatment practices, or a combination of both, limits our
capacity to intervene to reduce these inequalities for colorectal
cancer patients in this country.
This study, the first of its type in Queensland has demonstrated
that it is possible, and feasible, to reliably collect a broad measure
of disease spread for colorectal cancer patients from pathology
reports routinely submitted to the state cancer registry, and that
pathology reports are a better alternative than sourcing stage
information from the primary gatekeepers of medical care, general
practitioners.
Although this method of assessing disease spread cannot take
the place of clinical stage information, the limited progress
in developing population-based clinical cancer registries in
Australia means that, at least for the immediate future, sourcing
stage information for colorectal cancer patients from pathology
reports may be the best alternative. The results from this study
demonstrate that pathology-sourced stage is a valid measure of
disease spread when compared against stage information obtained
from clinical specialists.
ImplicationsThis method of collecting stage requires a lower level of
resources than other potential methods of collecting cancer
stage such as chart reviews, making it feasible to gather this
information for large-scale population-based studies on colorectal
cancer, and increase our ability to correctly interpret reasons for
observed inequalities in colorectal cancer survival. However,
that there are still differences between pathology stage and
clinical stage, particularly when metastasis is involved, highlights
the importance of integrating clinical stage information into
Australia’s population-based cancer registries to improve cancer
control in this country.
AcknowledgementsFunding for this study was provided by The Cancer Council
Queensland. The authors acknowledge Mrs Lyn McPherson and
Mrs Heather Day for their contribution to the data collection.
References1. Ciccolallo L, Capocaccia R, Coleman MP, Berrino F, Coebergh JW,
Damhuis RA, et al. Survival differences between European and US patients with colorectal cancer: role of stage at diagnosis and surgery. Gut. 2005;54(2):268-73.
2. Gatta G, Capocaccia R, Sant M, Bell CM, Coebergh JW, Damhuis RA, et al. Understanding variations in survival for colorectal cancer in Europe: a EUROCARE high resolution study. Gut. 2000;47(4):533-8.
3. Walker J, Quirke P. Prognosis and response to therapy in colorectal cancer. Eur J Cancer. 2002;38(7):880-6.
4. Young JL Jr, Roffers SD, Reis LAG, Fritz AG, Hurlbut AA, editors. SEER Summary Staging Manual – 2000. Bethesda (MD): National Cancer Institute; 2001.
5. EUROCARE. Protocol for Europe-wide Cancer Survival Study. Milan (ITA): Istituto Nazionale per lo Studio e la Cura dei Tumori; 2004.
6. Yu XQ, O’Connell DL, Gibberd RW, Abrahamowicz M, Armstrong BK. Misclassification of colorectal cancer stage and area variation in survival. Int J Cancer. 2007;122(2):398-402.
7. Liu WL, Kasl S, Flannery JT, Lindo A, Dubrow R. The accuracy of prostate cancer staging in a population-based tumor registry and its impact on the black-white stage difference (Connecticut, United States). Cancer Causes Control. 1995;6(5):425-30.
8. Schouten LJ, Langendijk JA, Jager JJ, van den Brandt PA. Validity of the stage of lung cancer in records of the Maastricht cancer registry, The Netherlands. Lung Cancer. 1997;17(1):115-22.
9. Jensen AR, Overgaard J, Storm HH. Validity of breast cancer in the Danish Cancer Registry. A study based on clinical records from one county in Denmark. Eur J Cancer Prev. 2002;11(4):359-64.
10. Malin JL, Kahn KL, Adams J, Kwan L, Laouri M, Ganz PA. Validity of cancer registry data for measuring the quality of breast cancer care. J Natl Cancer Inst. 2002;94(11):835-44.
11. Threlfall T, Wittorff J, Boutdara P, Heyworth J, Katris P, Sheiner H, et al. Collection of population-based cancer staging information in Western Australia – a feasibility study. Population Health Metrics. 2005;3:9.
12. Lynch BM, Baade P, Fritschi L, Leggett B, Owen N, Pakenham K, et al. Modes of presentation and pathways to diagnosis of colorectal cancer in Queensland. Med J Aust. 2007;186(6):288-91.
13. Australian Cancer Network Colorectal Cancer Guidelines Revision Committee. Guidelines for the Prevention, Early Detection and Management of Colorectal Cancer. Sydeny (AUST): The Cancer Council Australia; 2005.
14. American Joint Committee on Cancer. Cancer Staging Manual. 6th ed. New York (NY): Springer-Verlag; 2002.
15. Phillips KA, Milne RL, Buys S, Friedlander ML, Ward JH, McCredie MR, et al. Agreement between self-reported breast cancer treatment and medical records in a population-based Breast Cancer Family Registry. J Clin Oncol. 2005;23(21):4679-86.
16. Lewis RJ. Reliability and Validity: Meaning and Measurement. Proceedings of the Annual Meeting of the Society for Academic Emergency Medicine (SAEM); 1999 May; Boston, Massachusetts. 1999.
17. South Australian Cancer Registry. Incidence and Mortality, 1996. Epidemiology of Cancer in South Australia Incidence, Mortality and Survival 1977 to 1996. Adelaide (AUST): Open Book Publishers; 1997.
18. Australian Cancer Network Colorectal Cancer Guidelines Revision Committee. Guidelines for the Prevention, Early Detection and Management of Colorectal Cancer: Sydney (AUST): The Cancer Council Australia; 2005.
19. Boutard P, Platell C, Threlfall T. Model for collecting colorectal cancer staging information in Western Australia. ANZ J Surg. 2004;74(10):895-9.
20. Keating J, Pater P, Lolohea S, Wickremesekera K. The epidemiology of colorectal cancer: what can we learn from the New Zealand Cancer Registry? N Z Med J. 2003;116(1174):U437.
21. Gulliford MC, Bell J, Bourne HM, Petruckevitch A. The reliability of Cancer Registry records. Br J Cancer. 1993;67(4):819-21.
22. Cooper GS, Yuan Z, Stange KC, Amini SB, Dennis LK, Rimm AA. The utility of Medicare claims data for measuring cancer stage. Med Care. 1999;37(7): 706-11.
23. Baade P, Fritschi L, Aitken J. 2005. Geographical Differences in Cancer Incidence and Survival in Queensland, 1996 to 2002 [www.cancerqld.org.au]. Brisbane (AUST): Viertel Centre for Research in Cancer Control, Queensland Cancer Fund; 2005 [cited July 3 2008]. Available from: http://www.qldcancer.com.au/vcrcc/PDF/GeographicalIncidenceReport.pdf
24. Jong KE, Smith DP, Yu XQ, O’Connell DL, Goldstein D, Armstrong BK. Remoteness of residence and survival from cancer in New South Wales. Med J Aust. 2004;180:618-22.
25. Wilkinson D, Cameron K. Cancer and cancer risk in South Australia: What evidence for a rural-urban health differential. Aust J Rural Health. 2004;12:61-6.
Krnjacki et al. Article