-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
1/24
REMODELING OF FEMORAL STEM
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
2/24
BACKGROUND
FEMUR
The femur is the longest and strongest bone in the skeleton, is
almost perfectly cylindrical in the greater
part of its extent. In the erect posture it is not vertical,
being separated above from its fellow by aconsiderable interval,
which corresponds to the breadth of the pelvis, but inclining
gradually downward
and medialward, so as to approach its fellow toward its lower
part, for the purpose of bringing the knee-
joint near the line of gravity of the body. The degree of this
inclination varies in different persons, and is
greater in the female than in the male, on account of the
greater breadth of the pelvis.
Fractures
A femoral fracture that involves the femoral head, femoral
neckor the shaft of the femur immediately
below the lesser trochanter may be classified as a hip fracture,
especially when associated with
osteoporosis.
FEMORAL STEM
The femoral stem component replaces a large portion of bone in
the femur, and this is therefore the load-
bearing part of the implant. To bear this load, it must have a
Youngs Modulus comparable to that of
cortical bone. If the implant is not as stiff as bone, then the
remaining bone surrounding the implant will
be put under increased stress. If it is stiffer than bone, then
a phenomenon known as stress shielding will
occur.
DESIGN OF FEMORAL STEM
Design of the femoral stem is an important issue in the field of
total hip arthroplasty, but designis just one component in the
success or failure of the operation. Other components are
surgical
technique, cement technique or press-fit technique, bone
quality, as well as patient related
factors.
The quality of design may not also be matched with quality of
manufacturing and machining of
the stem. The ultimate outcome of the arthroplasty obviously
depends also on a matchingacetabular component.
Currently the femoral stem revision rate at 10-15 years is
reported to be between 0% and 4.8%
and does not correlate well with the radiographic stem
loosening.
Femoral stem design options are related to whether the stem is
curved or straight, the presence orabsence of collar support on the
calcar, the stem cross section, the stem offset, the surface
finish,
as well as the value of stem modularity and some metallurgical
issues.
Stem Offset?
http://en.wikipedia.org/wiki/Femoral_fracturehttp://en.wikipedia.org/wiki/Femoral_headhttp://en.wikipedia.org/wiki/Femoral_neckhttp://en.wikipedia.org/wiki/Shaft_of_the_femurhttp://en.wikipedia.org/wiki/Hip_fracturehttp://en.wikipedia.org/wiki/Osteoporosishttp://en.wikipedia.org/wiki/Osteoporosishttp://en.wikipedia.org/wiki/Hip_fracturehttp://en.wikipedia.org/wiki/Shaft_of_the_femurhttp://en.wikipedia.org/wiki/Femoral_neckhttp://en.wikipedia.org/wiki/Femoral_headhttp://en.wikipedia.org/wiki/Femoral_fracture
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
3/24
The offset is the transverse distance between the centre of the
head and the vertical linerepresenting mid-stem or mid-femur
(fig.9). Variability of offset helps to replicate the anatomy
by insuring proper soft tissue tension (fig.10) which balances
the hip bearings. Although a high
offset stem relatively increases its bending moment (fig.11),
various reports show that a highoffset does not increase cement
strain on medial cement mantle.
(fig.9)
Stem offset is the distance between the head centre and vertical
linerepresenting the mid-stem.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
4/24
(fig.10)
The offset of the stem helps to replicate normal soft tissue
tension.
(fig.11)
High offset stem resulted in lateralising the femur by 4.69 mm,
8 years follow
up x-ray.
A preoperative plan using a template (fig.12) of different
offset stems help the surgeon to see
which offset is likely to replicate the soft tissue anatomy.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
5/24
(fig.12)X-ray template help in measuring the right offset for
each patient.
Surface Finish?
How smooth should be the surface of the stem! Is a feature of
great variation as it comes in five
different ranges? Any surface will show peaks and valleys when
examined by scanning electron
microscopy (fig.13), the average between Peak and Valley is
known as the Roughness Average(Ra); according to Ra the surface
finish (fig.14) of femoral stems may be classified as:
1. Highly polished2. Satin3. Matt
4. Rough5. Textured
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
6/24
(fig.13)
Metal surface, as seen by SEM, showing peaks and valleys.
(fig.14)
Different stem finishing levels, polished (a), satin (b), Matt
(c), rough (d), and
textured (e) and (f).
A polished surface will show less fixation strength to cement,
to the contrary of rougher surfaces
which show greater fixation strength to cement.
Debonding is the loss of fixation between metal and cement. When
debonding happens roughsurfaces behave badly, as it will abrade the
adjacent cement and will cause microfractures in
cement mantle, ultimately leading to loss of fixation. This may
lead also to the release into the
effective joint space of abrasive wear debris from cement and
metal, which when ground insidethe bearings will act by 3
rdbody wear mechanism to release submicron poly wear
particles
initiating the process of osteolysis.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
7/24
Surface Features?
These are any irregularities present on the stem surface apart
from its finish discussed above, like
flanges, serrations, centralizers, pre-coated beads and
knobsetc..
The only surface features that may be beneficial are flanges and
centralizers.
Flanges are a part of the stem popularized in later Charnley
design stems (fig.15) to help
pressurize the cement as the proximal stem part is pushed into
the femur.
(fig.15)
The flanged design followed the roundback design in the Charnley
stem series.
The stem centralizer (fig.16) is also beneficial as it prevents
the stem from deviating in the canal,
insuring even cement mantle and perhaps preventing an unwanted
varus position of the stem.
Non end-bearing centralizers may prevent cement fracture below
the stem when subsidenceoccurs.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
8/24
(fig.16)
Stem centraliser insures a regular cement mantle and a centrally
located stem.
Pre-coating with PMMA was a good idea assuming better cement
bonding to the PMMA pre-
coat as compared to metal. This did not seem to work, as there
were reports by Mohler, 1995 of
early femoral loosening in 2-10 years, other reported 15% stem
failure rate over 6 years due topoor cement mantle and
centralization.
Modularity?
Modularity helps intra-operative adjustment of components, most
designs allow neck length
(fig.17) and head size modularity, and a select few allow
modularity in anteversion and CCD
angle.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
9/24
(fig.17)
Modular neck length, the short, standard and long heads can vary
the necklength, allowing adjustments during surgery.
The questions of increased wear and corrosion due to micromotion
between the different piecesof the modular stem remain to be proven
to assume a clinical disadvantage to these designs,
however; the clinical problems of impingement / dislocation
(e.g. by using a skirted extra-long
head, or a very short head on a broad conical neck, fig.18) and
of undue lengthening (fig.19) fall
under the technical control of the surgeon, who must be aware of
design and limitations of thestem he is implanting.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
10/24
(fig.18)
Using a short head, with a combination of conical neck and an
antiluxation
acetabular rim resulted in impingement during external rotation
with slightabduction.
(fig.19)
Leg lengthening due to the use of extra-long head
The modular stem costs more than the monoblock sibling, and adds
to the logistics of the
hospital creating more stock control overload on the
administrator.
CHECK FROM DESIGN CRETERIA
Metallurgical Issues
The current concept in hip arthroplasty prefers Cobalt-Chrome or
Stainless steel for thecemented stems and Titanium for the
cementless. Other ideas are also available; but the majority
of surgeons world wide support this current concept.
The Scope of Stem Design
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
11/24
This presentation stressed mainly on the standard cemented stem,
but the scope of stem design is
much larger, the cementelss stem may share many of the above
points of discussion apart from
those related to cement mantle and bonding. The surface of the
cementless stem and its coatingmay warrant a separate article.
The recent evolution of special stems used in femoral
reconstruction and revisions is also notcovered in this article,
the author believe that these are better understood when discussed
among
topics related to complex femoral reconstruction and revision
arthroplasty
PURPOSE OF FEMORAL STEM REMODELING
A hip replacement with a femoral stem produces an effect on the
bone called adaptive remodeling,
attributable to mechanical and biological factors. All of the
prostheses designs try to achieve an optimal
load transfer in order to avoid stress-shielding, which produces
an osteopenia.
INTRODUCTION
The implantation of a cemented or cementless femoral stem
implies an important change in thephysiological load distribution.
The bone reacts to the new situation, in accordance with Wolff 's
law,
undergoing a process of adaptive remodelling [1], related to
both mechanical and biological factors, being
the most important the initial bone mass [2].
Achieving good primary fixation is of crucial importance in
cementless hip arthroplasty to ensure good
short-term and long-term results. Lack of primary stability
leads to thigh pain and eventual loosening of
the prosthesis because of a continuous disruption of the bone
formation process around the implant (Kim
et al., 2003; Knight et al., 1998;Mont and Hungerford, 1997;
Petersilge et al., 1997). The stability, or the
lack of it, is commonly measured as the amount of relative
motion at the interface between the bone and
the stem under physiological load. Large interfacial relative
movements reduce the chance of
osseointegration, and cause the formation of a fibrous tissue
layer at the boneimplant interface (Pilliar et
al.,1986), which may eventually lead to loosening and failure of
the arthroplasty.
The threshold value of micromotion, above which a fibrous tissue
layer forms, has been studied in both
animals and humans. In a review of dental implants in animals, a
threshold micromotion value between
50 and 150 mm was found (Szmukler-Moncler et al., 1998). A
similar range of values was reported for
orthopaedic implants in humans. In a retrieval study of
cementless femoral components, Engh et al.
(1992) found indications that micromotions less than 40 mm had
resulted in osseointegration while
micro-motions of 150 mm had caused the interposition of a
fibrous tissue layer at the stembone
interface. It can be concluded from these reports that the value
of micromotion, above which
osseointegration is disrupted, ranges from 50 to 150 mm,
possibly skewed towards the lower end of this
range.
While many believe a sufficiently high interference fit is
essential to achieve good primary stability, it is
also clear that introducing a interference fit has caused a
clinically significant increase in intra-operative
femoral canal fractures (Cameron, 2004; Meek et al., 2004), an
effect which has also been demonstrated
during in vitro testing (Jastiet al., 1993; Monti et al., 2001).
The appropriate range of interference fit that
ensures primary stability without risking femoral fracture is
not well understood.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
12/24
There are in principle two parts to this study. In order to get
a rough idea of the interference fit introduced
using current surgical practise, in the first part of this
study, finite element predictions were correlated
with in vitro micromotion measurements. The aim of this was to
enable back calculation of the real
interference fit introduced by the surgeon during the in vitro
experiment. In the second part
of the study, the effect of a range of interference fits on
micromotion predictio ns was investigated using
finite element models of a more physiologically realistic
loading scenario than was possible during thefirst part of the
study.
METHODOLOGY
In the first part of the study, the finite element models were
based on CT scans from the specific bones
used in the experiment. In the second part of the study, the CT
scans from the visible human dataset were
used. Also in the first part of the study, the purpose was
simply to compare finite element predictions and
experiments and to simplify the experiments, a simple load
configuration was chosen. In the second part
of the study, physiological loads including muscle loads were
used.
In vitro experimental set-up
The experiment was designed for direct comparison of micromotion
values between experiment and FE
analyses. Four cadaver femurs and Alloclassic (Zimmer GmbH,
Winterthur, Switzerland) hip stems were
used, and two points, one in the proximal part and another in
the distal part of the stem (Fig. 1), were
chosen for micromotion measurement. In order to avoid damaging
the stembone interface during drilling
action, the two points on the implant were drilled before
implantation. A guide jig ensured that the bone,
subsequent to stem insertion, was drilled in the position
matching these same two points on the stem.
Finally, steel pegs were glued into the holes in the stem and
protruding through the bone (Fig. 1, right). A
linear variable differential transducer (LVDT Model DFg5, DC
Miniature series, Solartron Metrology,
UK), was rigidly fixed to the outside of the femur (Fig. 1,
right). The connecting rod of the LVDT core
rested on the free-end of the steel peg. When the implant was
loaded, the implant and hence the pegmoved relative to the bone and
the LVDT measured the axial movement of the peg relative to the
transducer, thus providing an estimate of the relative axial
movement between bone and stem.
Implantation was carried out by an experienced orthopaedic
surgeon (D.L.). The neck of the femur was
first resected, and the femur was then reamed with firm
impaction using a series of reamers to open the
canal. A femoral stem was then implanted in the femur.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
13/24
Fig. 1. The jig used to position the holes in the bone and the
pegs in the
implant, respectively (left). The implantbone specimen with
LVDT
attached to the femur loaded in compression in the mechanical
testing
machine (right).
The femur was sectioned 250mm distal to the lesser trochanter
and its distal end fixed inside a cylindrical
metal container using polymethyl- methacrylate (PMMA). These
were then placed onto the table bed of a
universal materials testing machine (Instron 5565, Instron
Corp., Canton, MA). The specimen was
adjusted so that the long axis of the stem was coaxial to the
direction of loading. A cyclical axialcompression load of 02 kN and
triangular waveform was applied to the shoulder of the stem for
50
cycles at a rate of 1 kN/min using a 5 kN load cell. Micromotion
readings via the LVDT were taken
manually at maximum load of 2 kN and when fully unloaded at each
cycle.
Finite element methodology for correlation study
A 3D model of a hip stem (Alloclassic, Zimmer GmbH) was
constructed from CAD files received from
the manufacturer (Fig. 2).
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
14/24
Fig. 2. The hip stem used in the study indicating the FE mesh
used (left)
and the implant inserted in the femur (right).
In the correlation part of the study, the finite element model
needs to be as accurate a representation of theexperimental set-up
as possible. Hence, the FE simulations of this part of the study
were based on CT
scans of the specific bones used in the experiments. There were
two sets of scans: one scan prior to
inserting the implant in the femur and a subsequent scan after
implantation. The first set of scans was used
to derive bone geometry and material properties from the
Houndsfield units of the scan, while the second
set of scans was used to ensure that the implant position and
orientation in the FE model precisely
matched the implant position within the femur in the experiment.
The reason for this two-step procedure
is that it would be inappropriate to use the CT datasets from
the implanted femur for bone property
assignment due to artefacts in these datasets caused by the
metal stem.
The construction of 3D models of the hip was done using AMIRA
software (Mercury Computer Systems,
Inc., San Diego, CA). Segmentation was compiled automatically
using the softwares marching cubes
algorithm which generates a 3D triangular surface mesh. The
completed model was then converted to
solid linear tetrahedral elements using Marc.Mentat
(MSC.Software, Santa Ana, CA) software. The mesh
was inspected to ensure it was reasonably shaped throughout. The
Marc finite element software package
was used in this study.
Material properties for the bone were assigned based on the
grey-scale value of the CT images on an
element-by-element basis. The grey-level of the CT images was
related to the apparent density using a
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
15/24
linear correlation (Cann and Genant, 1980; McBroom et al.,
1985). This allowed for the transformation of
the spatial radiological description into the description of
bone density. The modulus of elasticity of
individual elements was then calculated from the assigned
apparent densities using the cubic relationship
proposed by Carter and Hayes (1977). The material properties
were assumed to be linear elastic and
isotropic with Poissons ratio set to 0.35. The FE model was
loaded at the centre of the shoulder of the
stem with 2 kN, the stem being coaxial to the direction of
loading, hence, matching the loadingconfiguration in the
experiment.
Mesh convergence is a standard issue in any finite element
analysis and in a contact analysis, there are
many other numerical parameters that affect the predicted
micromotions. The default contact strategy in
Marc is a direct constraint algorithm (MSC.Marc-Manual, 2004)
which most importantly requires the
input of a contact zone size (CZS). Furthermore, Bernakiewicz
and Viceconti (2002) described the
importance of the convergence tolerance (CTol) in non-linear
analyses. They also suggested that the
appropriate parameter settings should be such that the resultant
change in predicted micromotion between
models with different parameter settings should be small
relative to 150 mm. A sequential sensitivity
analysis involving mesh density, CZS and CTol was carried out
and a model with 12,078 nodes, CZS
0.025mm and CTol 1% was found to be sufficient for an accurate
solution.
We also chose a Coulomb friction model which in Marc requires
theinput of the friction coefficient (m) as
well as a parameter (SL). The Marc software has introduced the
parameter SL, which describes a
smoothing of the step-function of the Coulomb model, only in
order to deal with an otherwise
numerically difficult to handle discontinuity. However, not only
does this parameter dramatically affect
the predicted micromotion (Fig. 3) it also has an important
physical interpretation. Shirazi-Adl et al.
(1993) showed that the boneimplant interface friction curve is
highly non-linear, exhibiting micromotion
on the order of 150 mm (that is in the order of the critical
level for osseointegration) before the slip load
predicted by the Coulomb model is reached. The implication of
Shirazi-Adl et al.s work is that adopting
the ideal Coulomb model is inadequate. However, the SL parameter
can be interpreted and used to
represent this non-linear behaviour.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
16/24
Fig. 3. Contour plots of micromotion over the surface of the
Alloclassic
stem under stairclimbing loads and for different values of the
SL
parameter (SL describes the non-linear friction characteristics
of the
interface).
To establish the appropriate setting of the SL parameter, we
simulated Shirazi-Adl et al.s relatively
simple experiment consisting of a bone cube exposed to normal
and tangential loads moving on a metal
plate. In Fig. 4 is shown Shirazi-Adls experimental curve of
tangential load versus tangential
displacement. The tangential load that would initiate slip
according to the Coulomb model is 30.6. The
finite element predicted curves for various settings of SL is
also shown and a setting of SL 0.1 predicts
the experimental curve well. Hence, in the rest of this study,
this setting was used.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
17/24
Fig. 4. Tangential load versus tangential displacement of bone
cube
sliding on metal plate. The finite element predicted non-linear
friction
behaviour for different levels of the parameter SL is shown as
well as the
experimental curve reported by Shirazi-Adl et al. (1993). The
critical value
at which sliding would initiate according to an ideal Coulomb
friction
model is also indicated.
The effect of friction coefficient on micromotion is relatively
minor for friction coefficients higher than
0.15 (Kuiper and Huiskes, 1996). Viceconti et al. (2000) found
that a friction coefficient between 0.2 and
0.5 led to the best correlation with experiments. Rancourt et
al. (1990) measured friction coefficients
experimentally and found a coefficient of0.4. Based on these
previous studies, a friction coefficient of 0.4
was used in this study.
The objective of this study was to estimate the effective
interference fit. Hence, we varied the interference
fit in the finite element models. The predictions were then
compared to the experimentally measured
values to estimate which level of interference best matched the
experiment.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
18/24
Finite element methodology for parametric study on the effect of
interference fit
In this part of the study, geometry and material
characterisation was based on the CT scans available from
the visible human project (VHP) dataset. The hip stem model was
aligned inside the femur according to
the recommendations of the manufacturer (Alloclassic surgical
technique, Zimmer Ltd., Warsaw, IN) and
an experienced surgeon (D.L.) inspected the resulting
configurations and considered them appropriate.
The models were restrained distally and loaded with
physiological stair-climbing loads including all
relevant muscle forces. Stair-climbing loads were applied as
this loading scenario has been shown to be
more critical than other activities (Kassi et al., 2005).
Similarly, Kassi et al. (2005) showed that it is
essential to include muscle loads although this issue has been
debated (Cristofolini and Viceconti, 2006).
This load configuration was based on the extensive work by
Bergmann (2001) and Heller et al. (2005) in
which load directions and muscle attachments are described. The
magnitudes of the loads in percentage
body weight are shown in Table 1 and a body weight of 82 kg was
used. All other aspects of the modelwere as described in Section
2.2.
RESULTS
In vitro micromotion measurements and correlation with model
predictions
During the experiments, the stem initially subsided into the
bone but after a sufficient number of cycles
the stem settled. Even in this relatively stable state, there
continued to be low levels of reversible motion
at the stembone interface as a result of the continued
loadunload cycle. It is high levels of this
continued disruption of the interface that is thought to prevent
osteogenic cells from bonding to the
surface of the stem (Pilliar et al., 1986). Hence, in terms of
evaluating the ingrowth potential of an
arthroplasty, it is the reversible micromotion rather than
subsidence which is the relevant constituent of
the overall relative motion between bone and implant. The
reversible micromotion during a load cycle
was estimated as the difference between the total micromotion
measured at maximum load and the total
micromotion when the specimen was unloaded. For the remainder of
this study, we will refer to this
quantity as reversible micromotion or just micromotion.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
19/24
In Fig. 5 is shown the experimentally determined reversible
micromotion for each of the four specimens
plotted against load cycles for the distal and proximal parts,
top and bottom, respectively. During the
initial cycles, this micromotion was high but then stabilised at
a lower value. Relatively high levels of
micromotion during the first few times a patient exposes a joint
to loading, are probably not critical. It is
the long term or stabilised value of reversible micromotion that
will continue to disrupt the implantbone
interface and prevent osseointegration. Hence, it is the
converged values of Fig. 5 which are relevant.Based on the data of
Fig. 5, the converged average value in the distal and proximal
regions were 1872 and
1975 mm, respectively.
Fig. 5. Distal micromotion (top) and proximal micromotion
(bottom)
results from the experiment.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
20/24
The results of the FE analyses using different levels of
interference fit and simulating the experiment are
shown in Fig. 6. The figure shows that with just 1 mm of
interference, the level of micromotion is
predicted to be in the range of 2030 mm. With 2 mm of
interference, this drops to 1020 mm.
Comparing this to the experimental values of 18 and 19 mm also
shown in the figure, this implies that the
interference fit introduced by the surgeon is only 1 or 2
mm.
Fig. 6. Contour plots of micromotion over the surface of the
stem under
an axial load of 2 kN, using interference fits of (from left to
right) 0, 1, 2
and 5 mm, respectively. The experimentally determined proximal
and distal
micromotion is also indicated.
This seems perhaps unrealistically low. Shultz et al. (2006)
considered an interference fit of 100 mm to
cause bone interface damage and reported this level of
interference as a threshold value. Therefore, we
included an interference fit of 100 mm in one of the finite
element models and inspected the resulting
tensile hoop stresses (Fig. 7). This model was not exposed to
any other loads. As can be seen from the
figure, interference induced hoop stresses are on the order of
50MPa on the surface of the bone (internally
the stresses are somewhat higher).Comparing this stress level
with the transverse tensile strength of
cortical bone of approximately 50MPa (Reilly and Burstein,
1975), it would seem that 100 mm represents
the critical level of effective interference fit above which the
femoral canal will fracture. The location ofhigh hoop stresses
towards the distal end of the implant seen in Fig. 7 also matches
the location of 77% of
intra-operative fractures (Meek et al., 2004).
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
21/24
Fig. 7. Hoop stresses in femoral bone caused by an interference
fit of
100 mm. No external loads are applied in this model.
Considering that femoral canal fractures are not infrequently
occurring intra-operatively (Cameron, 2004;
Meek et al., 2004), it would seem that surgeons are introducing
close to the critical level of interference fit
of 100 mm.
Assuming that surgeons are able to control the insertion process
within a factor of 2, perhaps a realisticrange of interference fit
can be argued to be in the range of 50100 mm. In summary, this
first part of the
study indicates that the range of realistic interference fits
may be within a range of very low levels (just a
few microns) and up to 100 mm.
The effect of interference fit on micromotion
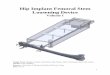
Fig. 8 shows contour plots of predicted micromotion over the
stem surface under stairclimbing loads and
for four different levels of interference fit. Fig. 9 shows the
change in micromotion with levels of
interference fit for the two points labelled P (proximal) and D
(distal) shown on the left model of Fig. 8.
Also in Fig. 9 is indicated, by the grey-coloured region, the
threshold range of micromotion above which
soft tissue formation will be predicted and below which
osseointegration would be expected. From thesetwo figures, it is
clear that the interference fit had a very large effect on
micromotion predictions. In the
case of no interference fit, the entire surface area of the
implant was in or above the grey area indicating
that theprimary stability of the implant is at risk. In
contrast, with 50 mm of interference, all but the mostproximal part
of the implant was predicted to osseointegrate. Interestingly,
increasing the level of
interference beyond 50 mm had negligible effect. Also, it is
clear that the effect of the interference fit was
most dramatic at low levels of interference. Including just 5 mm
of interference causes almost a 50%
reduction in micromotion and including more interference only
has a relatively small effect.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
22/24
Fig. 8. Contour plots of micromotion over the surface of the
stem under
stairclimbing loads and with interference fits of (from left to
right) 0, 5, 25
and 50 mm, respectively.
Fig. 9. Micromotion at points P (proximal) and D (distal) as a
function of
the level of interference fit. Locations of point P and D are
shown in Fig. 8
(left). The grey area indicates the range of the critical
micromotion
threshold. Above this level, fibrous tissue formation would be
expected;
below, osseointegration is anticipated.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
23/24
CONCLUSION
This study has shown that modeling the interference fit
characteristic of hip stems is crucial forquantitative predictions
of micro-motion. Ignoring the interference fit will probably lead
to an under
estimation of the stability of the stem. In contrast, ignoring
the non-linear friction behavior reported byShirazi-Adl et al.
(1993) and reproduced in Fig. 4, will probably to lead to too
optimistic predictions ofstem stability. The magnitude of
interference fit is fundamentally unknown and may be the reason
mostprevious works have omitted this parameter from their finite
element analyses. Indeed, during this study itbecame clear just how
difficult it is to estimate this parameter. Nevertheless, this
study demonstrates theimportance of the interference fit as
including only a small level of interference changed the evaluation
ofthe investigated stem from that of an unstable stem to that of a
stable stem.
Our predictions showed high levels of micro-motion distally and
proximally while micro-motion at the stemmidsection was lower (Fig.
8, left). This is qualitatively consistent with the finite element
predictions byKeaveny and Bartel (1993). Keaveny and Bartel did not
include an interference fit and predicted very highabsolute values
of micromotion (0550 mm). Keaveny and Bartel simulated a
cylindrical stem which islikely to be less resistant to torsional
loads and that may explain the higher levels ofmicromotion as
compared to our results. Viceconti et al. (2000) did simulate a
press-fit although it is notpossible to quantify this press-fit in
a manner that allows a direct correlation with our results.
Vicecontietal. predicted micromotions ranging from 17 to 49 mm
across the surface of the implant which isreasonably consistent
with our results simulating an interference fit of 25 mm (Fig.
8).
The results ofFig. 6 indicate that surgeons introduce very low
interference fits, on the order of 12 mm.Apart from any aspects of
the model that may cause inaccurate predictions, it is of course
also possiblethat the experimental results are inaccurate. Notably,
our experiment, like the vast majority of otherexperimental
micromotion studies, does not measure the actual interface
micromotion but insteadmeasures the motion between the LVDT
fixation point on the bone and the point of the peg insertion onthe
implant. The motion measured, therefore, includes other
flexibilities such as bone deformation and willtend to overestimate
micromotion (Bu hler et al., 1997). If these flexibilities are
substantial compared tothe true interface micromotion, it would
cause our methodology to predict very small levels of
interferencewhich is of course what seems to be the case.
In connection with Fig. 7, we proposed that surgeons are in fact
more likely to introduce interference fitsof 50100 mm. Shultz et
al. (2006) predicted that with an interference fit of 100 mm, the
hoop stresses inthe bone would visco-elastically relax by
approximately 50%. In other words, if a surgeon introduces
aninterference fit of 100 mm, this would relax and represent an
effective interference of 50 mm. Shultzreported that interference
fits lower than 100 mm would relax less than 50%. Therefore, even
if a surgeononly achieves the lower range of the50100 mm
interference, we have estimated, there should be at least25 mm of
effective interference left after relaxation, well above the 12 mm
estimated from theexperiment. We have no evidence to explain the
small levels of interference fit predicted from theexperiments but
we are inclined to believe that the experiment overestimated the
micromotion, for thereasons noted above.
We have assumed a uniform interference fit over the entire
surface of the implant. Accordingly, the press-
fit (pressure) varied considerably from the proximal cancellous
femur to the cortical distal femur asmodelled through the variation
in the local Youngs modulus of the bone adjacent to the implant.
Thisvariation in press-fit between the proximal and distal region
is undoubtedly qualitatively correct. However,our study was not set
up to investigate variation in interference fit. This was not
included due to thepractical difficulty in quantifying the
variation and generalising such variation that is likely to vary
betweenimplants. It is also probable, given the very small
interferences calculated, that surgeons cannot createimplant
cavities with uniform interference across the interface area, so
that clinical cases would includevariations from the micromotions
predicted. The effects of a more realistic scenario are not yet
known.
-
7/30/2019 REMODELING OF FEMORAL STEM(2).docx
24/24
The results of this study support the suggestion made earlier (
Shirazi-Adl et al., 1994) that the cavity thatis created in the
femur is larger than is indicated by the nominal interference of
0.30.5mm (Otani et al.,1995;Ramamurti et al., 1997); such a large
interference would cause the femur to fracture, according toour
results.
Perhaps the most important result of the study and the result
with direct clinical relevance relates to Figs.7 and 9. Fig. 7
predicts that surgery is safe against femoral canal fracture at
interference fits lower than100 mm. Fig. 9 predicts that the stem
would osseointegrate at interference levels of 50 mm. Therefore,the
recommendation is for the surgeon to err on the side of a low
interference fit during surgery as only 50mm is enough to achieve
stability and provides a safety factor of 2 against femoral canal
fracture. Ifconsidering a stem likely to be successful as long as
just the distal part of the stem (embedded in thestrong cortical
bone) osseointegrates, Fig. 9 indicates that just 10 mm of
interference fit is necessary forstability and provides a safety
factor of 10 against femoral canal fracture.
Of course, our computational predictions should be further
investigated before being applied in clinicalpractise. It is
likely, that stems with different geometry or material will behave
differently. The Alloclassicstem in this study, for example, has a
rectangular cross-section, which might be advantageous inresisting
torsional loading during the stairclimbing simulated. Nevertheless,
the predictions clearly indicatea recommendation to modify surgical
practise thereby reducing or even eliminating the 7%
intra-operativefemoral canal fractures during primary hip surgery
reported by Cameron, (2004) and the 650% fracture
rates reported by Meek et al. (2004) in connection with revision
hip surgery.