Embed Size (px)
Citation preview
Renal lesions aggravation are prevented Renal lesions aggravation are prevented
by low doses of sitagliptin in a rat model by low doses of sitagliptin in a rat model
of type 2 diabetes of type 2 diabetes
Renal lesions aggravation are prevented Renal lesions aggravation are prevented
by low doses of sitagliptin in a rat model by low doses of sitagliptin in a rat model
of type 2 diabetes of type 2 diabetes
Cristina Mega, Helena Vala, Jorge Oliveira, Rosa Fernandes, Filipa Mascarenhas-Melo, Belmiro Parada, Rui Pinto, Frederico Teixeira, Flávio Reis, Edite Teixeira de Lemos
Cristina Mega, Helena Vala, Jorge Oliveira, Rosa Fernandes, Filipa Mascarenhas-Melo, Belmiro Parada, Rui Pinto, Frederico Teixeira, Flávio Reis, Edite Teixeira de Lemos
Macrovascular Microvascular
Heine RJ, Spijkerman AM. 2006.
Major complications of Type 2 Diabetes Mellitus (T2DM)
Cardiovascular diseasesCardiovascular diseases
NeuropathyNeuropathy
RetinopathyRetinopathy
NephropathyNephropathy
• Diabetic nephropathy is a major microvascular complication of T2DM
• Incidence of T2DM is rapidly increasing, as well as the prevalence of chronic kidney disease (CKD), resulting from these diabetic complications
• In different regions of the World, it accounts for almost one-third of all cases of end-stage renal disease (ESRD)
• Diabetic nephropathy is a major microvascular complication of T2DM
• Incidence of T2DM is rapidly increasing, as well as the prevalence of chronic kidney disease (CKD), resulting from these diabetic complications
• In different regions of the World, it accounts for almost one-third of all cases of end-stage renal disease (ESRD)
Diabetic Nephropathy – A Major Diabetic Complication
Diabetes remains the single
most important cause of kidney failure
Diabetes remains the single
most important cause of kidney failure
Prevention of Diabetes-Induced dysmetabolism and associated
vascular complications
Blood Glucose levelsBlood Glucose levels Insulin secretion/action
Insulin secretion/action
Therapeutic Goals in Type 2 Diabetes Mellitus (T2DM)

Until now, anti-diabetic drugs were able to
Hyperglycaemia Hyperglycaemia
None were able to preserve β-cells
None were able to preserve β-cells
Therapeutic Goals in Type 2 Diabetes Mellitus (T2DM)
Anti-diabetic drugsAnti-diabetic drugs

incretin defect is a major contributor to β-cell dysfunction
incretins stimulate release of insulin by β-cells incretin inhibits glucagon release by α-cells and that in T2DM the incretin effect is decreased
Sitagliptin
Knowing thatKnowing that
New anti-diabetic drugs, focus on the increase of incretin levels in diabetic patients, like SitagliptinNew anti-diabetic drugs, focus on the increase of incretin levels in diabetic patients, like Sitagliptin
a dipeptidyl peptidase-4 (DPP-4) inhibitor and one of the best known incretin enhancersa dipeptidyl peptidase-4 (DPP-4) inhibitor and one of the best known incretin enhancers

Sitagliptin targets 2 physiologic glucose-lowering actions with a single oral agent
Improves 24 h
glycaemic control
Incretin hormones GLP-1 and GIP are released by the intestine throughout the day
Their levels increase in response to a meal and are found to be reduced in Diabetes
InactiveGIP
DPP-4 enzyme
InactiveGLP-1
Beta cellsBeta cells Insulin(GLP-1 and GIP)
Glucose dependentGlucose dependentGlucose dependentGlucose dependent
Glucagon(GLP-1)Alpha cellsAlpha cellsAlpha cellsAlpha cells
Glucose Glucose uptake byuptake byperipheral peripheral tissuestissues
Glucose Glucose productionproduction
by liver by liver
SITAGLIPTIN allows SITAGLIPTIN allows for a longer for a longer
circulation life for circulation life for incretinsincretins
X
2 - 4 minutes2 - 4 minutes
BBLLOOOODD GGLLUUCCOOSSEE
BBLLOOOODD GGLLUUCCOOSSEE
GIPGLP-1

Preserving pancreatic function
Inhibition of DPP-4 activity, by incretin enhancers, such as Sitagliptin (Known Effects)
but the real impact of low-dose sitagliptin treatment on diabetic nephropathy remains to be elucidated
but the real impact of low-dose sitagliptin treatment on diabetic nephropathy remains to be elucidated
Improve glycaemic control, in diabetic patients
by prolonging the actions of incretin hormones

Prevention of Diabetes-Induced dysmetabolism and microvascular
complications – Diabetic Nephropathy
Assess the effects
SITAGLIPTINAssess the effects
SITAGLIPTIN
????
Evaluate the effects of chronic (6 weeks) inhibition of DPP-4 by low doses of Evaluate the effects of chronic (6 weeks) inhibition of DPP-4 by low doses of
sitagliptin, in the ZDF rat, an animal model of T2DM, on progression ofsitagliptin, in the ZDF rat, an animal model of T2DM, on progression of
renal lesionsrenal lesions
AIM:AIM:

Animals and experimental design:
Divided in 2 subgroups (n = 8 rats)treated with:
- Sitagliptin 10 mg/kg/BW/day oror- Vehicle (orange juice)
SID (6:00 PM), for 6 weeksSID (6:00 PM), for 6 weeks
♂ Zucker Diabetic Fatty (ZDF fa/fa) (n=16)
Age: 20 weeksAge: 20 weeks
Controls: their lean littermates (ZDF +/+) (n=8)
Age: 20 weeksAge: 20 weeks
Sample Collection and Preparation
Blood and tissues - collected at 20 weeks (Ti) and at 26 weeks (Tf) Blood and tissues - collected at 20 weeks (Ti) and at 26 weeks (Tf)
Renal specimens were paraffin-embedded and the 3 µm thick sections
stained for routine histopathological diagnosis with haematoxylin and
eosin (HE) and Periodic Acid of Schiff (PAS)
All samples were examined by light microscopy using a Zeiss Axioplan 2
microscope
Renal specimens were paraffin-embedded and the 3 µm thick sections
stained for routine histopathological diagnosis with haematoxylin and
eosin (HE) and Periodic Acid of Schiff (PAS)
All samples were examined by light microscopy using a Zeiss Axioplan 2
microscope

Arteriolar hyalinosis
Arteriosclerosis.
Arteriolar hyalinosis
Arteriosclerosis.Inflammation
Hyaline cylinders
Tubular basement membrane irregularity
Tubular calcification
Interstitial fibrosis/tubular atrophy (IFTA)
Inflammation
Hyaline cylinders
Tubular basement membrane irregularity
Tubular calcification
Interstitial fibrosis/tubular atrophy (IFTA)
Histomorphological EvaluationHistomorphological Evaluation
Mesangial expansionGBM thickeningCapsule of Bowman thickeningNodular sclerosisGlomerulosclerosisAtrophy Hyalinosis of the vascular pole
Mesangial expansionGBM thickeningCapsule of Bowman thickeningNodular sclerosisGlomerulosclerosisAtrophy Hyalinosis of the vascular pole
R
E
N
A
L
L
E
S
I
O
N
S
R
E
N
A
L
L
E
S
I
O
N
S

0 = absent1 = mild2 = moderate3 = severe
0 = < 25%1 = 25 - 50%2 = 50 - 75%3 = > 75 %
Scored in single blind fashionScored in single blind fashion
Severity Severity
ExtensionExtension
Semi-quantitative scoring of lesions Semi-quantitative scoring of lesions
(Except IFTA)(Except IFTA)
All lesions were evaluated on the total tissue on the slide. All lesions were evaluated on the total tissue on the slide.
++
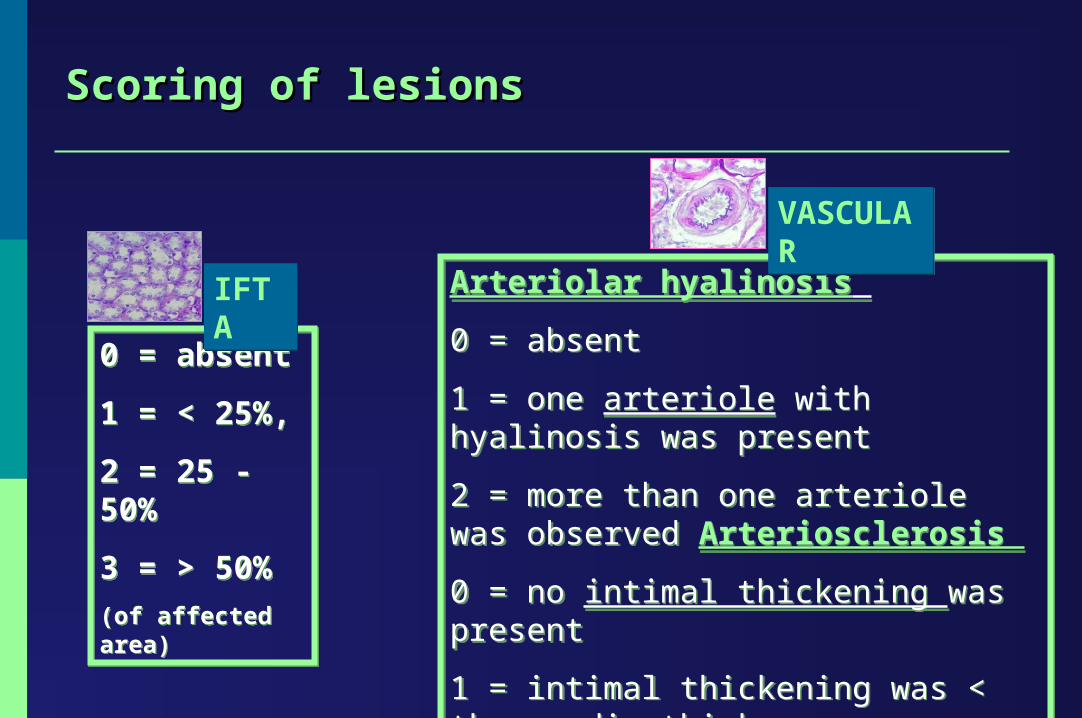
Arteriolar hyalinosis
0 = absent
1 = one arteriole with hyalinosis was present
2 = more than one arteriole was observed Arteriosclerosis
0 = no intimal thickening was present
1 = intimal thickening was < than media thickness
2 = intimal thickening > than media thickness
Arteriolar hyalinosis
0 = absent
1 = one arteriole with hyalinosis was present
2 = more than one arteriole was observed Arteriosclerosis
0 = no intimal thickening was present
1 = intimal thickening was < than media thickness
2 = intimal thickening > than media thickness
0 = absent
1 = < 25%,
2 = 25 - 50%
3 = > 50%
(of affected area)
0 = absent
1 = < 25%,
2 = 25 - 50%
3 = > 50%
(of affected area)
IFTA IFTA
Scoring of lesions Scoring of lesions
VASCULARVASCULAR

RESULTS RESULTS
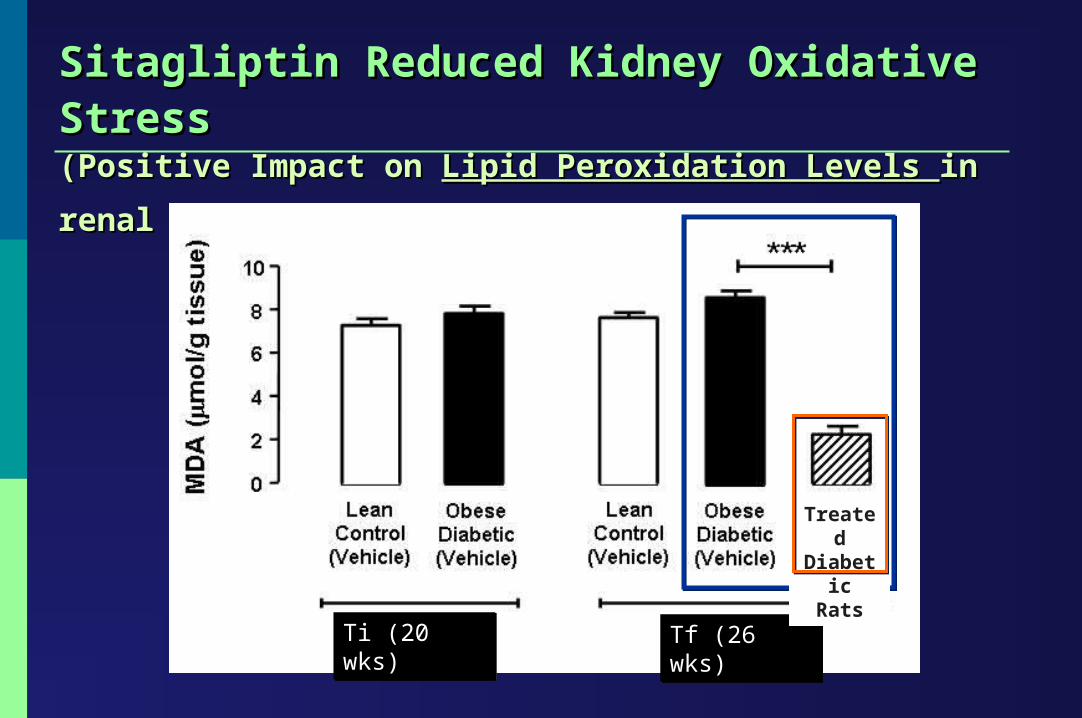
Sitagliptin Reduced Kidney Oxidative Stress Sitagliptin Reduced Kidney Oxidative Stress (Positive Impact on (Positive Impact on Lipid Peroxidation Levels Lipid Peroxidation Levels in renal tissues)in renal tissues)
Tf (26 wks)Tf (26 wks)Ti (20 wks)Ti (20 wks)
Treated Diabetic
Rats
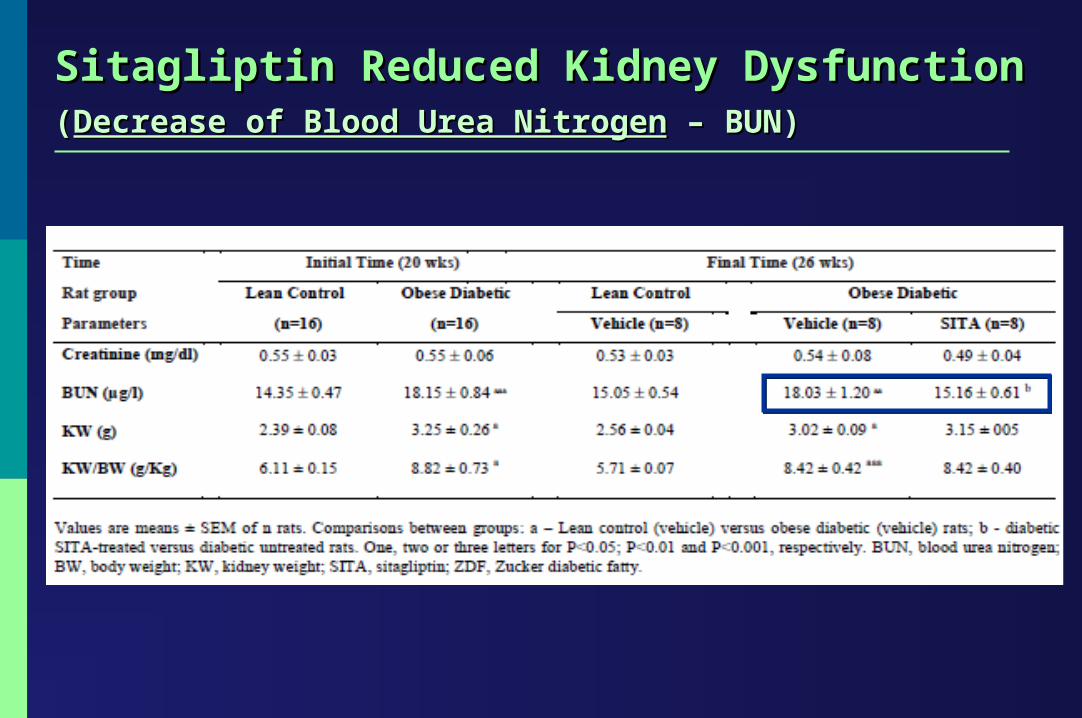
Sitagliptin Reduced Kidney DysfunctionSitagliptin Reduced Kidney Dysfunction((Decrease of Blood Urea NitrogenDecrease of Blood Urea Nitrogen – BUN) – BUN)

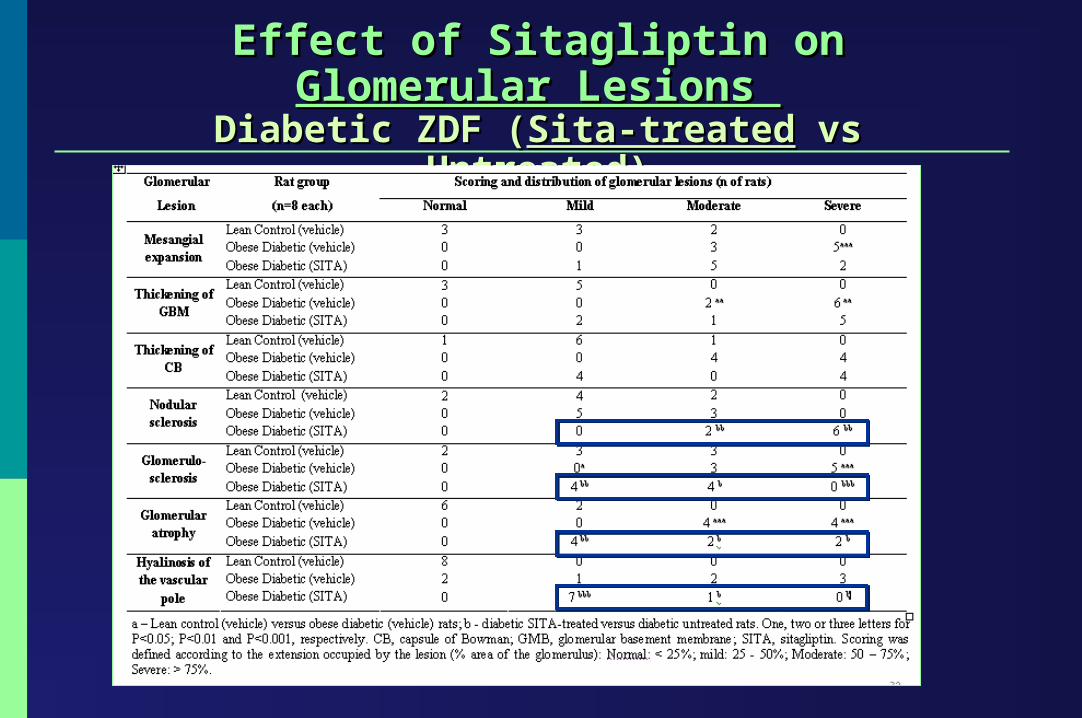
Effect of Sitagliptin on Glomerular Lesions Effect of Sitagliptin on Glomerular Lesions Diabetic ZDF (Diabetic ZDF (Sita-treatedSita-treated vs Untreated) vs Untreated)
UNTREATEDUNTREATED SITA-TREATED RATSSITA-TREATED RATS
50µm50µm
25µm 25µm

Effect of Sitagliptin on Glomerular Lesions Effect of Sitagliptin on Glomerular Lesions Diabetic ZDF (Diabetic ZDF (Sita-treatedSita-treated vs Untreated) vs Untreated)
UNTREATEDUNTREATED SITAGLIPTIN-TREATEDSITAGLIPTIN-TREATED
50µm50µm
25µm 25µm
mnng
Effect of Sitagliptin on Effect of Sitagliptin on Glomerular Lesions Glomerular Lesions Diabetic ZDF (Diabetic ZDF (Sita-treatedSita-treated vs Untreated) vs Untreated)
SITAGLIPTIN-TREATEDSITAGLIPTIN-TREATED
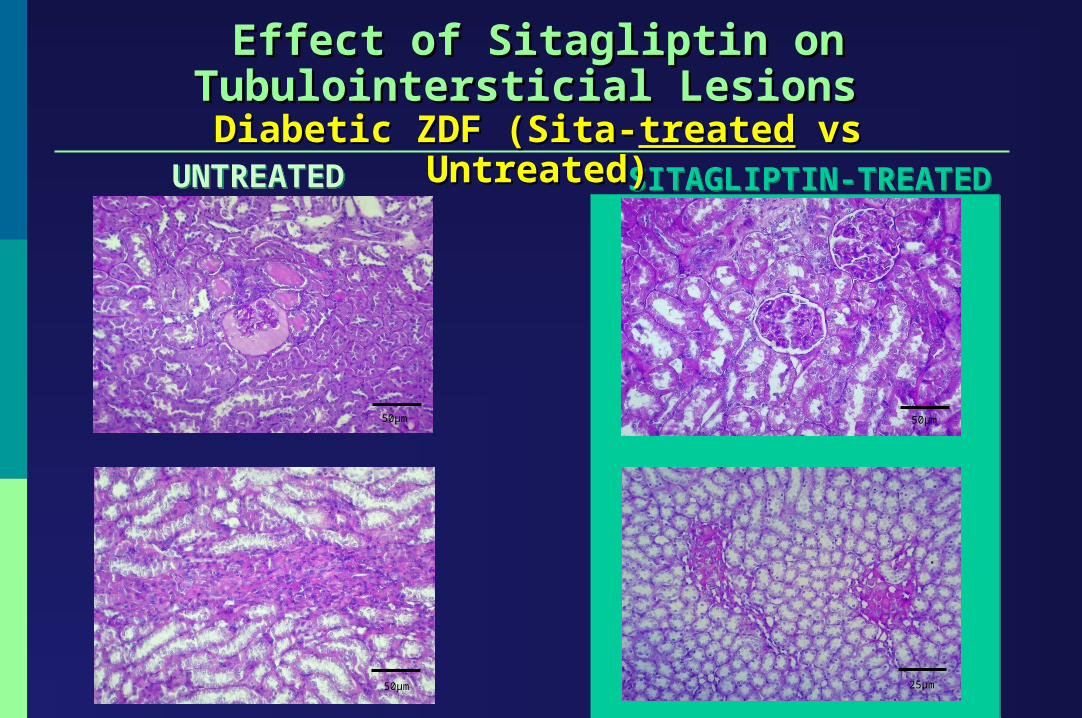
Effect of Sitagliptin on Tubulointersticial Lesions Effect of Sitagliptin on Tubulointersticial Lesions Diabetic ZDF (Sita-Diabetic ZDF (Sita-treatedtreated vs Untreated) vs Untreated)
50µm 50µm
25µm
UNTREATEDUNTREATED
50µm
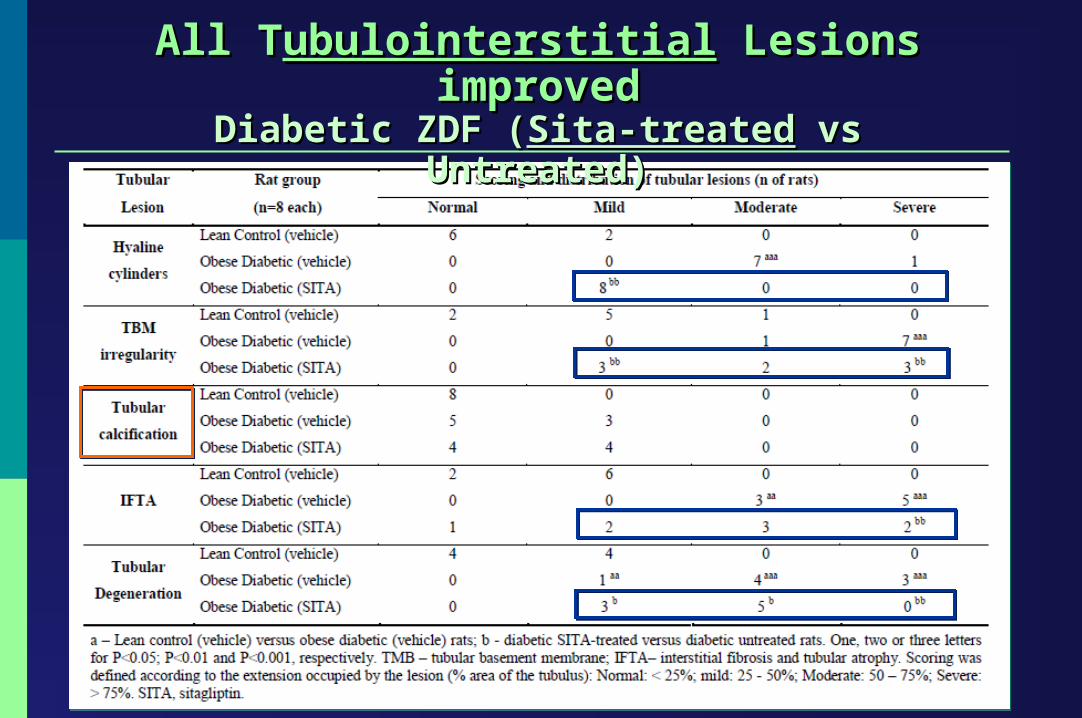
All TAll Tubulointerstitialubulointerstitial Lesions improved Lesions improvedDiabetic ZDF (Diabetic ZDF (Sita-treatedSita-treated vs Untreated) vs Untreated)

25µm
25µm
The Improvement of The Improvement of Glomerular & TubulointerstitialGlomerular & Tubulointerstitial Lesions Lesions Diabetic ZDF (Diabetic ZDF (Sita-treatedSita-treated vs Untreated) vs Untreated)

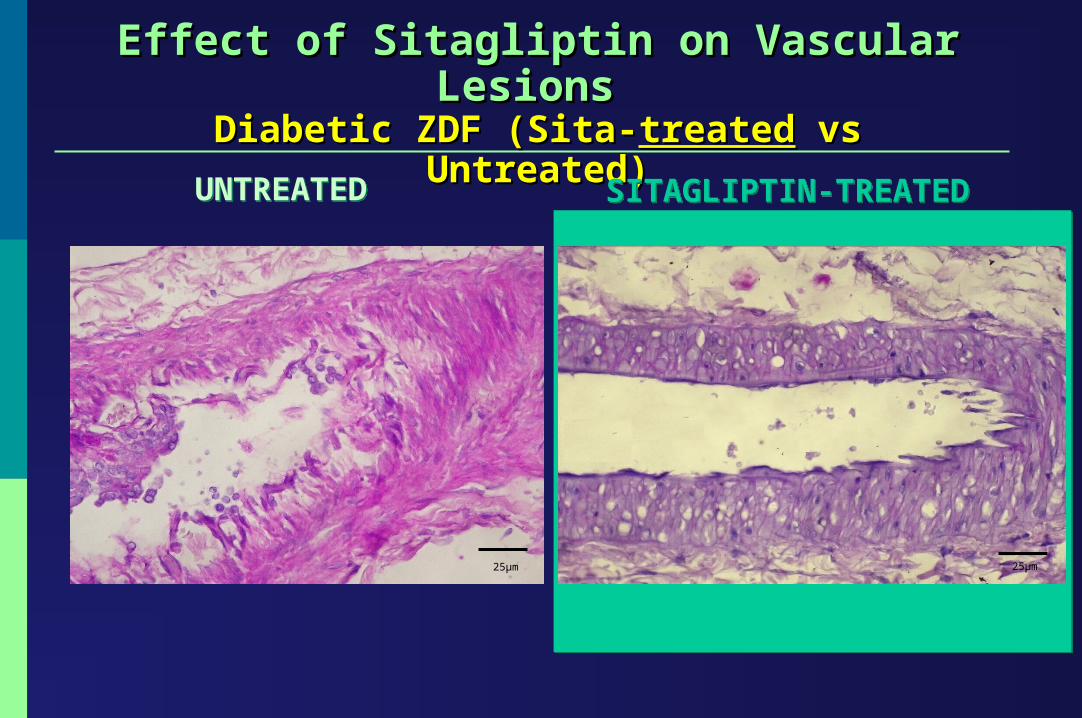
Effect of Sitagliptin on Vascular Lesions Effect of Sitagliptin on Vascular Lesions Diabetic ZDF (Sita-Diabetic ZDF (Sita-treatedtreated vs Untreated) vs Untreated)
UNTREATEDUNTREATED SITA-TREATED ANIMALSSITA-TREATED ANIMALS
25µm25µm

Effect of Sitagliptin on Vascular Lesions Effect of Sitagliptin on Vascular Lesions Diabetic ZDF (Sita-Diabetic ZDF (Sita-treatedtreated vs Untreated) vs Untreated)
UNTREATEDUNTREATED SITAGLIPTIN-TREATEDSITAGLIPTIN-TREATED
25µm25µm
Effect of Sitagliptin on Vascular Lesions Effect of Sitagliptin on Vascular Lesions Diabetic ZDF (Sita-Diabetic ZDF (Sita-treatedtreated vs Untreated) vs Untreated)
UNTREATEDUNTREATED SITAGLIPTIN-TREATEDSITAGLIPTIN-TREATED
25µm25µm

Effect of Sitagliptin on Vascular Lesions Effect of Sitagliptin on Vascular Lesions Diabetic ZDF (Sita-Diabetic ZDF (Sita-treatedtreated vs Untreated) vs Untreated)
UNTREATEDUNTREATED SITAGLIPTIN-TREATEDSITAGLIPTIN-TREATED
25µm 25µm
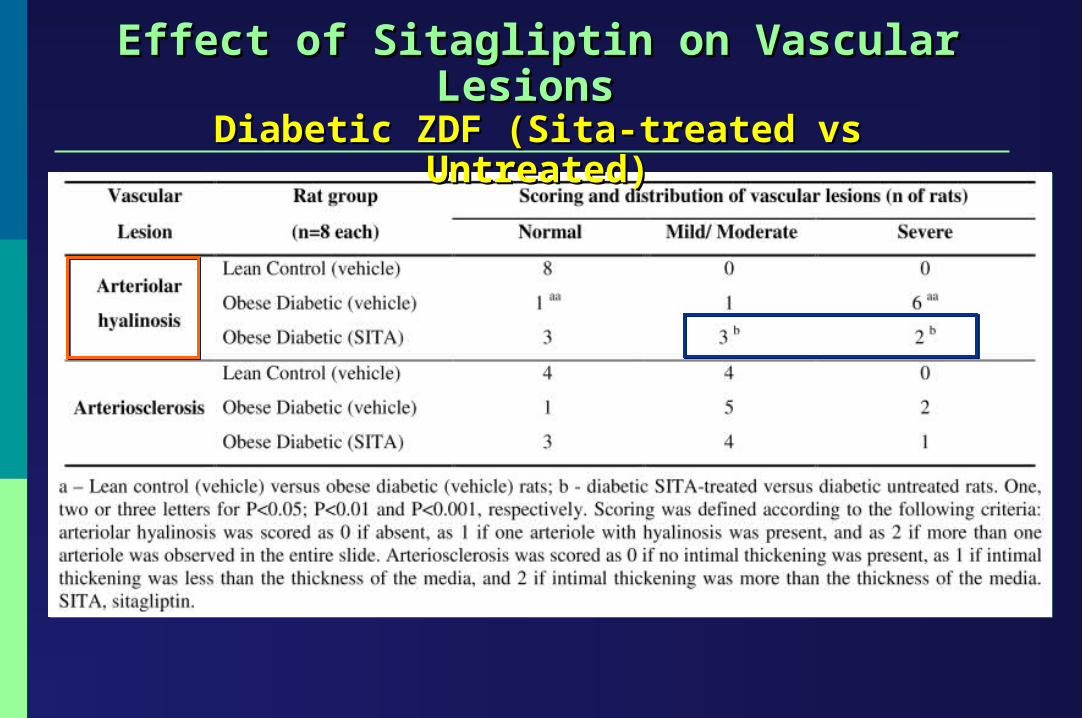
Effect of Sitagliptin on Vascular Lesions Effect of Sitagliptin on Vascular Lesions Diabetic ZDF (Sita-treated vs Untreated)Diabetic ZDF (Sita-treated vs Untreated)

ConclusionsConclusionsIn an animal model of T2DM, a 6 week once daily treatment with a low dose In an animal model of T2DM, a 6 week once daily treatment with a low dose of Sitagliptin promotedof Sitagliptin promoted::In an animal model of T2DM, a 6 week once daily treatment with a low dose In an animal model of T2DM, a 6 week once daily treatment with a low dose of Sitagliptin promotedof Sitagliptin promoted::
- Glomerulosclerosis
- Tubulointerstitial lesions
- Vascular lesions
- Glomerulosclerosis
- Tubulointerstitial lesions
- Vascular lesions
IMPROVEMENT OF
DIABETIC NEPHROPATHY
IMPROVEMENT OF
DIABETIC NEPHROPATHY
REGULATION OF DIABETIC DISMETABOLISM
REGULATION OF DIABETIC DISMETABOLISM
HyperglycaemiaHypertriglyceridaemiaHyperglycaemiaHypertriglyceridaemia
RENAL FUNCTIONRENAL FUNCTION
Oxidative stressBlood Urea NitrogenOxidative stressBlood Urea Nitrogen
Has the effect in
ConclusionsConclusionsSitagliptin was able to delay the development of diabetic Sitagliptin was able to delay the development of diabetic nephropathy in this model of T2DM, viewed by reduction of renal nephropathy in this model of T2DM, viewed by reduction of renal lesionslesions
This effect might be, at least, partially due, to its benefits on This effect might be, at least, partially due, to its benefits on correction of diabetes dysmetabolism (hyperglicaemia, correction of diabetes dysmetabolism (hyperglicaemia, dyslipidaemia and insulin production/sensitivity), as well as due to dyslipidaemia and insulin production/sensitivity), as well as due to a favorable impact on kidney lipid peroxidation a favorable impact on kidney lipid peroxidation
Sitagliptin was able to delay the development of diabetic Sitagliptin was able to delay the development of diabetic nephropathy in this model of T2DM, viewed by reduction of renal nephropathy in this model of T2DM, viewed by reduction of renal lesionslesions
This effect might be, at least, partially due, to its benefits on This effect might be, at least, partially due, to its benefits on correction of diabetes dysmetabolism (hyperglicaemia, correction of diabetes dysmetabolism (hyperglicaemia, dyslipidaemia and insulin production/sensitivity), as well as due to dyslipidaemia and insulin production/sensitivity), as well as due to a favorable impact on kidney lipid peroxidation a favorable impact on kidney lipid peroxidation
TThe he prevention of diabetic nephropathy evolution might prevention of diabetic nephropathy evolution might represent a key step forward in the management of T2DM represent a key step forward in the management of T2DM
and these serious complications and these serious complications
TThe he prevention of diabetic nephropathy evolution might prevention of diabetic nephropathy evolution might represent a key step forward in the management of T2DM represent a key step forward in the management of T2DM
and these serious complications and these serious complications

This presentation was supported by the Polytechnic Institute of Viseu, PortugalThis presentation was supported by the Polytechnic Institute of Viseu, Portugal
Muito obrigada! Muito obrigada!
Cristina Mega, Helena Vala, Jorge Oliveira, Rosa Fernandes, Filipa Mascarenhas-Melo, Belmiro Parada, Rui Pinto, Frederico Teixeira, Flávio Reis, Edite Teixeira de Lemos
Cristina Mega, Helena Vala, Jorge Oliveira, Rosa Fernandes, Filipa Mascarenhas-Melo, Belmiro Parada, Rui Pinto, Frederico Teixeira, Flávio Reis, Edite Teixeira de Lemos
Thank you very much!Thank you very much!
Paljon kiitoksia
Paljon kiitoksia






![Ertugliflozin and Sitagliptin Co-initiation in Patients ...sitagliptin and metformin [18], and in combi-nation with sitagliptin as an add on to met-formin [19, 20] improved glycemic](https://img.pdfslide.net/doc/110x75/5e2a04698dc7ef19de3a2141/ertugliflozin-and-sitagliptin-co-initiation-in-patients-sitagliptin-and-metformin.jpg)