Embed Size (px)
Citation preview

Environment International 49 (2012) 100–109
Contents lists available at SciVerse ScienceDirect
Environment International
j ourna l homepage: www.e lsev ie r .com/ locate /env int
Replacing car trips by increasing bike and public transport in the greater Barcelonametropolitan area: A health impact assessment study
D. Rojas-Rueda a,b,c,d,⁎, A. de Nazelle a,b,c,d, O. Teixidó e, M.J. Nieuwenhuijsen a,b,c,d
a Centre for Research in Environmental Epidemiology (CREAL), C. Doctor Aiguader, 88, 08003 Barcelona, Spainb Municipal Institute of Medical Research (IMIM—Hospital del Mar), Barcelona, Spainc CIBER Epidemiología y Salud Pública (CIBERESP), Spaind Universitat Pompeu Fabra (UPF), Barcelona, Spaine Energy and Air Quality Department, Barcelona Regional, C. 60, 25–27, 08040, Barcelona, Spain
Abbreviations: BAU, business as usual; CO2, carbonfunctions; EEA, European Environmental Agency; HEATtool; LUR, land use regression; METs, metabolic equivalefor Economic Co-operation and Development; PA, physmatter less than 10 μm; PM2.5, fine particles (less thTHE PEP, Transportation, Health and Environment Pan-United Nations Economic Commission for Europe; UNEPtal Program; US EPA, United States Environmental ProHealth Organization.⁎ Corresponding author at: CREAL—Centre for Research
Barcelona Biomedical Research Park, Dr. Aiguader, 88; 080932147315; fax: +34 932147301.
E-mail address: [email protected] (D. Rojas-Rueda).
0160-4120/$ – see front matter © 2012 Elsevier Ltd. Allhttp://dx.doi.org/10.1016/j.envint.2012.08.009
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 15 May 2012Accepted 17 August 2012Available online 21 September 20120Keywords:BicyclingPublic transportAir pollutionPhysical activityRoad traffic fatalityHealth impact assessment
Objective: Estimate the health risks and benefits of mode shifts from car to cycling and public transport in themetropolitan area of Barcelona, Spain.Methods: We conducted a health impact assessment (HIA), creating 8 different scenarios on the replacement ofshort and long car trips, by public transport or/and bike. The primary outcome measure was all-cause mortalityand change in life expectancy related to two different assessments: A) the exposure of travellers to physicalactivity, air pollution to particulate matter b2.5 μm (PM2.5), and road traffic fatality; and B) the exposure ofgeneral population to PM2.5, modelling by Barcelona Air-Dispersion Model. The secondary outcome was achange in emissions of carbon dioxide.Results: The annual health impact of a shift of 40% of the car trips, starting and ending in Barcelona City, to cycling(n=141,690) would be for the travellers who shift modes 1.15 additional deaths from air pollution, 0.17 additionaldeaths from road traffic fatality and 67.46 deaths avoided from physical activity resulting in a total of 66.12 deaths
avoided. Fewer deaths would be avoided annually if half of the replaced trips were shifted to public transport(43.76 deaths). The annual health impact in the Barcelona City general population (n=1,630,494) of the 40%reduction in car tripswould be 10.03 deaths avoided due to the reduction of 0.64% in exposure to PM2.5. The deaths(including travellers and general population) avoided in Barcelona City therefore would be 76.15 annually. Furtherhealth benefitswould be obtainedwith a shift of 40% of the car trips from theGreater BarcelonaMetropolitanwhicheither start or end in Barcelona City to public transport (40.15 deaths avoided) or public transport and cycling(98.50 deaths avoided).The carbon dioxide reduction for shifting from car to other modes of transport (bike andpublic transport) in Barcelona metropolitan area was estimated to be 203,251 t/CO2 emissions per year.Conclusions: Interventions to reduce car use and increase cycling and the use of public transport in metropolitanareas, like Barcelona, can produce health benefits for travellers and for the general population of the city. Alsothese interventions help to reduce green house gas emissions.© 2012 Elsevier Ltd. All rights reserved.
dioxide; DRF, dose response, health economic assessmentnt of task; OECD, Organizationical activity; PM10, particulatean 2.5 μm); RR, relative risk;European Programme; UNECE,, United Nations Environmen-tection Agency; WHO, World
in Environmental Epidemiology,03, Barcelona, Spain. Tel.: +34
rights reserved.
1. Introduction
Urban transport faces major challenges due to the continuousgrowth of urban population, private vehicle ownership and congestion.When the urban transport experiencesmajor difficulties, consequencesare felt by households, by businesses, and by the urban community atlarge. Transport may become a binding constraint on economic growth,social development and inclusion, along with increased negativeimpacts on health and on the environment.
The motor vehicles are a major source of environmental and noisepollution in urban areas (Schwela et al., 2008). About 70% of environ-mental pollution and 40% of greenhouse gases in European cities comefrom motorized transport (EEA, 2010). Different programs of govern-mental and international organizations such as the United NationsEnvironmental Programme (UNEP), the European Environmental

101D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
Agency (EEA) and the United States Environmental Protection Agency(US EPA) have suggested changes in public policies to encourage publictransport and non-motorized transport (walking and cycling) in thecities, to combat problems such as climate change, environmental pollu-tion and energy dependency (EEA, 2010; UNEP, 2010; US EPA, 2011).Other programs and tools like the Transport, Health and EnvironmentPan-European Programme (THE PEP) and the health economic assess-ment tools (HEAT) for walking and for cycling from the World HealthOrganization (WHO) and the United Nations Economic Commissionfor Europe (UNECE), and programs from organizations such as theOrganization for Economic Co-operation and Development (OECD) andthe World Bank, are focused not only on the environmental benefits ofreducing the use of motorized transport, but also on its potential healthbenefits (Hunt, 2011; Kahlmeier et al., 2011; The World Bank, 2011;WHO-UNECE, 2010).
The health benefits of replacing the car by the bicycle to travel inurban areas have been quantified in previous studies (de Hartog et al.,2010; Lindsay et al., 2011; Rabl and de Nazelle, 2012; Rojas-Ruedaet al., 2011). These health benefits have been attributed mainly toincreased levels of physical activity (Andersen et al., 2000). Also theeconomic and health benefits of the use of public transport have beenestimated in previous studies, related not only in terms of increasedphysical activity, but also with a reduction of road traffic fatalities andcrime (Edwards, 2008; Litman, 2010). Although these studies onlyincluded in their analysis the replacement of short trips by bicycle,and had not taken into consideration longer trips or other modes oftransport such as public transport.
The city of Barcelona is the second most populated urban area inSpain, composed of 36 municipalities representing 3,231,458 inhabi-tants, of whom 1,630,494 live in the city of Barcelona (DSM, 2011),and a high population density of 15,963 inhabitants/km2 in a spaceof 101 km2. In the Barcelona Metropolitan area 7.7 billion tripswere made in 2010, 17% of which were made by car, 36% by publictransport, 31% by walking, and 1% by cycling. In Barcelona City,walking was also the dominant mode (about 45% of trips), followedby public transport (30%), and while the car accounted for close to10% of all trips and cycling around 2%. Ninety‐nine percent of thepopulation who live in the city of Barcelona has access to public trans-portation and on 28% of roads in the city the bicycles have priority(bike lanes and low speed zones) (DSM, 2011). The conditions forcycling and walking are ideal most of the year (average temp17.3 °C, 74 days of rain), and a topography that is favourable inmost parts of the city with essentially small differences in altitude(16 m over sea) except for hills at the edges of the city.
Table 1Scenarios and results (in travellers) of replacing car trips by bike and/or public transport.
Inside Barcelona scenarios a
Scenario 1 Scenario 2 Scenario
Car trips reduction 20% 40% 20%c
Trips/day replaced by Bike (%) 94,460 (100) 188,920 (100) 47,230 (5Trips/day replaced by Public Transport (%) f 0 0 47,230 (5Health determinants (deaths/year)
Air pollution (PM2.5) 0.57 1.15 0.33Road traffic fatality 0.08 0.17 −0.01Physical activity −33.73 −67.46 −22.2
TotalDeaths/year g −33.06 −66.12 −21.88Months gained h 6.5 6.5 4.7
PM2.5: particulate matterb2.5 μm.a Inside Barcelona Scenarios refers to the trips that start and end in Barcelona City.b Outside Barcelona Scenarios refers to the trips that start or end in Barcelona City and sc Here we assumed that the 50% of the trips were replaced by bike, 22% by bus/tram andd Here we assumed that 26% of the trips are replaced by bus/tram and 74% are by metroe Here we assumed that 20% of the trips are replaced by bike, 21% by bus/tram and 59%f Public transport includes: bus, tram, train and metro.g These results include the sum of deaths from road traffic fatality, physical activity andh Using all-cause hazard rates for males and females in Barcelona region for 2007 (GENC
The aim of our study was to quantify the health impacts of replac-ing the use of car in the metropolitan area of Barcelona by bikes andpublic transport. We have created different scenarios to replace thecar use in the metropolitan area of Barcelona by bus, tram, metro,train and bicycle, and we have quantified the impact on the healthof the travellers who shifted the mode of transport and also the healthimpact on the general population from a reduction of air pollutionresulting from this modal change.
2. Methods
2.1. Scenarios
The scenarios of reduction in car traffic in Barcelona metropolitanarea are presented in Table 1, and were compared to the businessas usual (BAU) scenario represented by the 2009 traffic conditionsreported by the Barcelona City council (DSM, 2010). The eight scenariosdeveloped included various combinations of hypotheses on i) theamount of traffic reductions (20 or 40% reduction), ii) characteristicsof trips reduced (internal to Barcelona City or traffic between theinner-city and the metropolitan region), and iii) mode shifts (from carto bike and/or public transportation). Scenarios 1 to 4 only concernedtrafficwithin BarcelonaCity (with 20% of car trips reduction in scenarios1 and 3, and 40% reduction in scenarios 2 and 4), and are hereafterreferred to as the “inside Barcelona” scenarios, while as in scenarios 5to 8, hereafter referred to as the “outside Barcelona” scenarios,reductions were imposed on traffic that originates in Barcelona Cityand ends in the Barcelona metropolitan area outside the city, or,vice-versa, originates in the Metropolitan area outside the city andends in the Barcelona City itself (with 20% car trips reductions inscenarios 5 and 7, and 40% in scenarios 6 and 8). Lastly, scenarios 1and 2 assumed that all the trips shifted from car to bike; scenarios 3and 4 that 50% of the car trips shifted to bike and the rest to publictransport (Bus, tram, metro and train); scenarios 5 and 6, that all thecar trips shifted to public transport; and scenarios 7 and 8, that 20% ofthe car trips shifted to bike trips, and the rest to public transport.
2.2. Framework
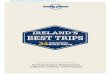
The conceptual framework for assessing impacts in travellers isshown in Fig. 1. We used a health impact assessment framework aspublished by Joffe and Mindell (2002), to estimate the health effects ofmode shifts from car trips to bike or public transport. Exposure–responsefunctions were derived from existing studies and calibrated for current
Outside Barcelona scenarios b
3 Scenario 4 Scenario 5 Scenario 6 Scenario 7 Scenario 8
40%c 20%d 40%d 20%e 40%e
0) 94,460 (50) 0 0 34,065 (20) 68,130 (20)0) 94,460 (50) 170,324 (100) 340,648 (100) 136 259 (80) 272,518 (80)
0.67 0.15 0.3 0.64 1.28−0.02 −0.98 −1.95 −0.71 −1.43−44.4 −19.25 −38.5 −49.17 −98.35
−43.76 −20.07 −40.15 −49.25 −98.54.7 2.8 2.8 4.7 4.7
tart or end in Barcelona metropolitan area.28% are by metro/train.
/train.are by metro/train.
particulate matterb2.5 μm.AT, 2010).

102 D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
exposure and health conditions in Barcelona. We modelled all-causemortality effects due to physical activity behaviour, road traffic fatality,and exposure to air pollution. These three health determinants wereexpected to have the greatest impact and best available data, based ondiscussions held amongst experts during a workshop in Barcelonain 2009 (de Nazelle et al., 2011b). Recent publications of HEAT forwalking and for cycling (Kahlmeier et al., 2011), Woodcock et al.(2009), de Hartog et al. (2010) and Rojas-Rueda et al. (2011) providedfurther guidance for our approach.
First we focused on impacts in Barcelona metropolitan arearesidents who started cycling or who started travelling in publictransport as a result of the mode shift from car (hereafter referredto as “the travellers”). In other words we assessed additional benefitsfrom physical activity and additional risks due to incremental airpollution inhalation and increased exposure to road traffic fatality ofnew public transport passengers and new cyclist, compared toprevious exposures as car users. We focused on the age group 16 to64 because we expected them to conduct the majority of trips(estimated 78%) and travel regularly to work or study.
Secondly, we estimated the potential health impacts of a reduc-tion in air pollution due to the reduction in traffic for the “generalpopulation” using a health impact assessment framework comparingthe concentrations of air pollution between our scenarios and theBAU scenario in all age groups.
2.3. Data modelling
Main input data used in the model are summarized in Table 2.Appendix A provides a detailed description of assumptions and calcu-lation steps used to derive the model inputs from available dataoutlined in this section.
Road TrafficFatality
PhyAct
He
Car Redu
DecisionVariables
HealthDeterminants
OutputVariables
Replaced byPublic Transport
Mortality
Urban TPo
Fig. 1. Conceptual fra
2.3.1. Car, bike and public transport dataTransportation data for car, bike, and public transport were
obtained from a combination of data provided by travel surveysand records conducted by transportation departments of the cityand Metropolitan area (DSM, 2010; RMB, 2006). Based on thesedata sources, we estimated the average length of trips “inside” and“outside” Barcelona (3.1 km and 6.4 km, respectively) and the totalnumber of car trips reduced in each scenario (Table 1). We assumedthat car trips are replaced with either bike or public transportationtrips of the same length. We allocated the public transport tometro or train and bus or tram proportionally to the current publictransport mode share.
2.3.2. Road traffic fatality of travellersWe calculated mortality from road traffic fatalities per billion
kilometres travelled by bicycle, walk, public transport and car fromestimates of the total distance travelled annually by bike, pedestrians,bus, tram, metro, train and car which we linked to traffic mortalitydata by mode reported by the Barcelona Public Health Agency in thelast 9 years (2002–2010) (ASPB, 2011; Santamariña and Perez,2008). We grouped together bus and tram in one group and metroand train in another group. We assumed that every public transporttrip involves 10 min walking. Therefore the risk of suffering a roadtraffic fatality by the pedestrians is integrated in the risk of publictransport. Then we calculated the relative risk (RR) of all-causemortality of road traffic fatality for cyclists, bus/tram passengers andmetro/train passengers compared to car passengers, assuming thesame distance travelled for each mode according to each scenario.
2.3.3. Physical activity of travellersFor physical activity, we followed the approach presented in HEAT
for cycling for bike scenarios and HEAT for walking for public
sicalivity
Air Pollution
alth
Carbon DioxideEmissions
Replaced byBike
Usection
LifeExpectancy
ransportlicy
mework model.

Table 2Barcelona baseline data and key assumptions used in the model.
Inside Barcelonaa Outside Barcelonab
Number of trips per dayc
Car 472,300 851,619Bike 95,193 7,631Public transportd 1,455,703 1,316,996
Trip duration (minutes)e 16.3 33.9Distance travelled per tripf (km) 3.1 6.4
ValueSpeed of each mode (km/h)
Car 23.5 c
Bike 14 f
Bus/tram 11.2 c
Metro/train 25 c
Road traffic fatalities in Barcelona (deaths/billion km travelled)g
Car 3.72Bike 4.54Public transportd 0
Expected mortality per age group (deaths/1000 inhabitants)h
All age groups 9.3616–64 age groups 2.05
Number of trips per person per day f 1.5Time spent walking in a public transport trip (minutes)f 10Total population in Barcelona (inhabitants)c 1.6 millions
a Inside Barcelona refers to the trips that start and ends in Barcelona City.b Outside Barcelona refers to the trips that starts or ends in Barcelona City and start
or ends in Barcelona metropolitan area.c Data from Transport department of Barcelona, (DSM, 2010).d Public transport includes Bus, Tram, Metro and Train.e Data from Daily Mobility Survey of Catalonia (RMB, 2006); f Assumptions, see
Appendix A for description.g Average deaths per billion of km travelled for the period of 2002–10 (ASPB, 2011).h Mortality rate in both sexes in 2007 in Catalan population (GENCAT, 2010).
103D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
transport scenarios (Kahlmeier et al., 2011). HEAT for cycling uses RRof all-cause mortality for commuting in bike compared to non-bikecommuters derived from a study in Copenhagen which is the largesthealth cohort that specifically considered health effects of bicyclecommuting (Andersen et al., 2000). We adjusted the RR function fordaily average distances cycled in Barcelona compared to Copenhagen.HEAT for walking uses RR of all-cause mortality for walking comparedto non-walking derived from a meta-analysis which included ninestudies on mortality among comparable populations identified in asystematic review, adjusted for other types of physical activity. Wealso adjusted the RR function for weekly average walking duration,reported in this meta-analysis. We assumed that for each trip inpublic transport (bus, tram, metro and train) the traveller walkedfor 10 min.
2.3.4. Travellers air pollution exposureThe travellers' air pollution assessment model considered the
exposure to particulate matter less than 2.5 μm (PM2.5), which hasshown strong associations with all-cause mortality (Krewski et al.,2009). We compared exposure concentrations and inhaled dose fortravel by car, bicycle, bus/tram and metro/train. Concentration levelsfor car, bike, walk and bus were obtained from a measurement studyconducted in Barcelona (de Nazelle et al., 2011a). We also assumedthat the relative concentrations between modes collected during thestudy were representative of year-round average concentrations.For levels in the metro and train, we assumed a 3 times greaterconcentration than the background concentrations, similar to datareported by different studies in other cities (Aarnio et al., 2005;Adams et al., 2001; Cheng et al., 2008; Johansson and Johansson,2003; Park and Ha, 2008; Ripanucci et al., 2006). We assigned thesame concentrations to the tram and the bus. We assumed that allpublic transport trips included a 10‐minute walk in the street, for
which we also estimated corresponding exposure concentrations(see Appendix A). We estimated yearly inhaled dose of PM2.5 ac-counting for mode-specific inhalation rates, exposures, and tripduration, as in de Nazelle et al (2009). To simplify, non-travel timeswere assumed to be spent resting and sleeping while exposed toindoor concentration levels of PM2.5. To estimate the RR of mortalityassociated with the increment of pollutant intake for travellers usingthe bike and public transport compared to car users, similar tode Hartog et al. (2010), we applied the ratio between the estimatedinhaled dose for travellers (in bike, bus/tram and metro/train) andfor car users to exposure-response functions reported in the litera-ture. We used the update by Krewski et al. (2009) of the RR functionsin PM2.5 reported by Pope et al. (2002). As a sensitivity analysis, wealso carried out this calculation for mortality risks associated withincrements of black smoke (BS) inhalation.
2.3.5. Air pollution in general populationTo assess the health impacts of the reduction in the concentrations
in PM2.5 in Barcelona City, we employed the Barcelona Air-DispersionModel (Lao and Teixido, 2011). With this dispersion model for PM10,we estimated the concentration of PM2.5, applying the ratio of 0.6(PM2.5/PM10), for the BAU scenario; and then we estimated theconcentration for a reduction of 20% in car trips and for a reduction of40% of car trips. This dispersion model was used only for BarcelonaCity and its population, and did not include the whole metropolitanarea of Barcelona. We estimated the change in concentration in eachdifferent census area in Barcelona (1482 census areas) taking intoaccount the number of inhabitants and age distribution (consider allage groups) for each census area.We estimated the expectedmortality,RR, and attributable fraction among exposed in each census area toobtain the health impacts related with PM2.5 reduction.
2.3.6. Mortality ratesFor the travellers' impact assessment scenarios we used the RR
functions from our three health determinants derived for our studyconditions in Barcelona and we calculated the change in mortality(increment or decrement) associated with travel by bike or publictransport (bus/tram and metro/train). We applied the RR to thenumber of deaths in our population to obtain the population attribut-able number of deaths for each scenario (Perez and Kunzli, 2009;WHO, 2008). We used all-cause mortality rates in the population be-tween 16 and 64 years (with average age 39 years) in the Barcelonaregion (2.05 deaths per 1000 inhabitants per year in 2007, whichrepresents around 2200 deaths per year), as reported by the StatisticalInstitute of Catalonia (GENCAT, 2010).
Since there is no information available on the specific age distribu-tion in each different mode of transport, was conducted a sensitivityanalysis to quantify the effects on mortality related to physicalactivity for each scenario using a younger age distribution (average33 years) based on a report on cycling in Spain (GESOP, 2009) andan older age distribution (average 48 years) (see online Appendix C).
For the general population, we used mortality rates for the entirepopulation (9.36 deaths per 1000 inhabitants per year in 2007), asreported by the Statistical Institute of Catalonia (GENCAT, 2010),adjusting for the age distribution of each census area (see Table 2).
2.3.7. Life expectancyWe present results as a number of attributable deaths that could
be prevented per year in each scenario. Since death cannot beprevented but only postponed, some authors suggest presentingresults in changes in life expectancy rather than in preventabledeaths. We estimated average change in life expectancy in eachscenario (inside and outside Barcelona) for travellers and for thegeneral population, based on all-cause mortality rates for males andfemales in Barcelona region for 2007 (GENCAT, 2010), and applyingstandard life table methods reported by Miller and Hurley (2003).

104 D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
2.3.8. CO2 emissionsCO2 emission savings estimates were calculated following guide-
lines and emission factors provided by the Catalan Office of ClimateChange (OCCC, 2010b) and calibrated to the Barcelona vehicle fleet(number of vehicles using diesel or gasoline and engine efficiency)(DGT, 2008).
2.4. Model
The different model parts of health impact assessment for travel-lers outlined above were linked together in a quantitative modelbuilt in Analytica 4.2 (Lumina Decisions Systems, CA, 2010) MonteCarlo simulation program. The main model employed average valuesfor all inputs described previously.
We carried out a sensitivity analysis testing the impact of usingalternative values for 20 of the input variables in a Monte Carlosimulation. These 20 variables were inputs used either to constructother variables or directly used in the analysis. The sensitivity analysiswas meant to 1) assess the stability of our results when employing arange of possible input values, 2) provide a range of likely outcomesas a simple form of uncertainty and variability analysis, and 3)identify which inputs are most influential in determining theoutcomes. The range of values included for each tested variabledepended on the type of information available on the probabilitydistribution for each variable (a summary of ranges used is shownin Appendix A). When the data was available, the mean and standarddeviation were used to create normal distribution. If data was notavailable or the source of data did not include information fromdistribution parameters, we used triangular distributions. If it waspossible to select a minimum andmaximum from the data or by com-paring the results of different datasets, we chose a triangular distribu-tion with a maximum and minimum based on the data. For inputvariables without any other information than mean, we assumedthe triangular distribution with minimum and maximum values 50%around the mean value. This uncertainty range was chosen to avoidunderestimation of the uncertainty. We identified input variables ofhighest importance by calculating rank-order correlations betweeneach variable and the model outcome.
3. Results
The scenarios presented represent a reduction from 94,460 (scenario1) to 340,648 (scenario 8) daily trips by car in Barcelona (Table 1), thenumber of trips depends on the scenario (e.g. 20% or 40% of car tripsreduction or if it is inside or outside of Barcelona). These car trip reduc-tions represent between 5.9% (scenario 1) and 23% (scenario 8) of allmotorized vehicles trips in Barcelona.
3.1. Trips starting and ending inside Barcelona City
3.1.1. TravellersFor physical activity the relative risk for all-cause mortality related
to travellers who cycled inside Barcelona compared to car passengerswas 0.81, corresponding to an attributable fraction of−0.23. In publictransport users, we estimated the physical activity benefits from the10‐minute walk included in each trip and we found that the RR forall-cause mortality compared to car passengers was 0.93, with anattributable fraction of −0.07. Combining cyclists and public trans-port users, deaths avoided annually due to increments in physicalactivity range from 22.2 (scenario 3) to 67.4 (scenario 2), as shownin Table 1.
The relative risk of all cause mortality related to the incremental in-halation of PM2.5 inside Barcelona for cyclists was 1.004, which repre-sents an attributable fraction of 0.004. The relative risk for all causemortality due to inhalation of PM2.5 inside Barcelona, in travellers ofpublic transport compared to car passengers was for metro/train
1.001, corresponding to an attributable fraction of 0.001 and for bus/tram users the RRwas 1.0003, corresponding to an attributable fractionof 0.0003. All together, incremental annual deaths due to inhalation ofPM2.5 ranged from 0.33 to 1.15 (Table 1).
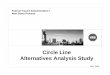
The RR for mortality related with road traffic fatalities insideBarcelona in cyclist compared to car passengers was 1.0006, with anattributable fraction of 0.0006. The RR for mortality related to roadtraffic fatalities inside Barcelona in public transport passengers com-pared to car passengers was both for metro/train and bus/tram 0.99,with an attributable fraction for metro/train of −0.0009 and forbus/tram the attributable fraction was −0.0006. In total, 0.01 and0.02 deaths were avoided from reduction in road traffic fatalities inscenarios 3 and 4 respectively, while scenarios 1 and 2 lead to 0.08and 0.17 additional deaths (Table 1). We illustrated the impact ofuncertainty using a Tornado Plot which shows the effect on the over-all model results of varying each input variable individually (Fig. 2).
3.1.2. General populationOn average across Barcelona City, the 20% car trip reduction inside
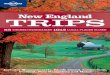
Barcelona (scenarios 1 or 3) would lead to an 0.07 μg/m3 decrease inPM2.5 concentration, and the 40% car trip reduction (scenarios 2 or 4)to an in 0.14 μg/m3 decrease in PM2.5 compared to the BAU scenario.The estimated deaths avoided were 5 for a 20% of reduction in cartrips, and 10.03 for a 40% of reduction in car trips (Table 3 and Fig. 3).
3.1.3. TotalThe number of deaths per year avoided annually adding the impacts
in travellers and in the general population for the “inside Barcelona”scenarios ranged from 26.88 (scenario 3) to 76.15 (scenario 2).
3.2. Trips starting or ending inside Barcelona City within the Metropolitanarea
3.2.1. TravellersThe RR for all-cause mortality related to physical activity in public
transport travellers outside Barcelona compared to car passengerswas 0.93, with an attributable fraction of −0.07. The physical activityrelative risk for all-cause mortality related to travellers who cycledoutside Barcelona compared to car passengers was 0.64, correspond-ing to an attributable fraction of−0.64. Combining cyclists and publictransport users, deaths avoided due to increments in physical activityranged from 19.25 (scenario 5) to 98.35 (scenario 8), as shown inTable 1.
The relative risk for all cause mortality for the inhalation of PM2.5outside Barcelona, in travellers of public transport compared to carpassengers was for metro/train 1.001, corresponding to an attribut-able fraction of 0.001 and the RR for bus/tram related to PM2.5 was0.99, with an attributable fraction of −0.0006. The relative risk ofall cause mortality related to the inhalation of PM2.5 outsideBarcelona for cyclists compared to car passengers was 1.01, whichcorresponded to an attributable fraction of 0.009. All together,incremental annual deaths due to inhalation of PM2.5 ranged from0.15 to 1.28 (Table 1).
The RR for mortality related with road traffic fatalities outsideBarcelona in public transport passengers compared to car passengerswas both for metro/train and bus/tram 0.99, with an attributablefraction of −0.004 and the RR for mortality related with road trafficfatalities outside Barcelona in cyclist compared to car passengerswas 1.001, with an attributable fraction of 0.001. These results in arange of 0.71 to 1.95 deaths avoided due to the reduction in roadtraffic fatalities (Table 1).
3.2.2. General populationOn average across Barcelona City, the 20% car trip reduction from
outside Barcelona (scenarios 5 or 7) would lead to a 0.13 μg/m3
decrease in PM2.5 concentration, and the 40% car trip reduction

Fig. 2. Tornado plot for scenario 4.
105D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
(scenarios 6 or 8) to a 0.26 μg/m3 decrease in PM2.5 compared to theBAU scenario. The estimated deaths avoided would be 9.06 for a 20%of reduction in car trips, and 18.15 for a 40% of reduction in car trips(Table 3 and Fig. 3).
3.2.3. TotalThe number of deaths per year avoided, adding the impacts in
travellers and in the general population for the “outside Barcelona”scenarios, ranged from 29.13 (scenario 5) to 116.65 (scenario 8).
Table 3Air pollution reductions and their impacts in general population.
Percentage ofcar tripsreduction
PM 2.5 a CO2b
Reduction(μg/m3) c
Percentageof reduction(%) d
Deaths(deaths/year)
Days gainedin lifeexpectancy e
Emissionsavoided(ton/year) f
Inside Barcelona g
20% 0.07 0.32 −5 1.14 21,39140% 0.14 0.64 −10.03 2.28 42,783
Outside Barcelona h
20% 0.13 0.58 −9.06 2.05 80,23340% 0.26 1.16 −18.15 4.11 160,467
a PM 2.5=particulate matterb2.5μm.b CO2=carbon dioxide.c Estimated by the Barcelona Air-Dispersion Model for PM 10, applying the ratio of
0.6 (PM2.5/PM10).d Percentage of reduction with respect to the total concentration estimated by the
Barcelona Air-Dispersion Model.e Using all-cause hazard rates for males and females in Barcelona region for 2007
(GENCAT, 2010);f Metric tons.g Inside Barcelona refers to the trips that start and end in Barcelona City.h Outside Barcelona refers to the trips that start or end in Barcelona City and start or
end in Barcelona metropolitan area.
3.3. CO2
The annual reduction in carbon dioxide emissions resulting fromthe reduction in 40% of car trips inside (scenarios 2 or 4) and 40% ofreduction outside (scenarios 6 or 8) Barcelona was estimated to be203,251 t of CO2 (see Table 3).
4. Discussion
Interventions for reducing car use and increasing bicycle andpublic transport use could improve the health of travellers and thegeneral population in Barcelona. The major benefits of the reductionof car trips being replaced by bike or public transport trips comefrom the increase in the levels of physical activity in travellers,followed by the benefits associated with reduction of air pollutionin the general population and to a much lesser extent also from thereduction in the risk of traffic accidents specifically in the case ofpublic transport. Although the reduction in air pollution affects theentire population, we only have been identified few benefits. Thenumber of deaths per year avoided in Barcelona City (including theimpacts in travellers and general population) would be 76.15 with a40% shift from car use to cycling for within-city trips, and fewer(53.79 deaths avoided) if half of them would shift from car to publictransport and the other half to cycling. Further health benefitswould be obtained from a shift of car trips (including the generalpopulation impacts) in the Greater Barcelona Metropolitan Areawhich start or end in Barcelona City to public transport or publictransport and cycling (58.30 and 116.65 deaths avoided respectively,for the 40% car trip reduction scenarios).
As in all risk assessments, our study was limited by the availabilityof data and the necessity to make assumptions to model likelyscenarios. We carried out sensitivity analyses to assess the robustnessof our results and tested effects of deviations from our main assump-tions and data choices. Included in the sensitivity analysis were,for example, relative risk functions from the literature, choice of

* 20% reduction map corresponds to scenarios 1 or 3; 40% reduction map corresponds to scenarios 2 or 4; PM10: Particulate matter less than 10 micrometers; BCN: Barcelona
PM reduction
Fig. 3. Reduction in PM for inside Barcelona scenarios.
106 D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
pollutants, age distribution, and environmental and travel conditionsin Barcelona. Importantly, we found that in all the scenarios we testeda net benefit when replacing car trips by public transport or/andcycling trips.
Our results agree with previous studies suggesting a health benefitby reducing the use of motorized transport and replacing it byother modes of transport. A Dutch study reported the benefits ofbicycling outweighing the risks in terms of months of life gained(2–12 months) compared to travel by car (de Hartog et al., 2010). Astudy in New Zealand found that the health benefits from physicalactivity for shifting 5% of the vehicle kilometres to cycling in allurban areas of the country could lead to 116 deaths avoided annuallyin the cycling population (Lindsay et al., 2011). An international studycompared different future scenarios of increased active transport, andfound health benefits for the general population and a reduction inCO2 emissions (Woodcock et al., 2009). The model used in thisstudy has been previously applied to evaluate specific transportpolicies (the public bicycles system in the city of Barcelona called“Bicing”), but only evaluated the risk and benefits of cycling and notthe health impacts in general population (Rojas-Rueda et al., 2011).It found considerable benefits of cycling. A recent study estimatedthe health impacts of reducing environmental pollution related tothe elimination of short car trips in 11 United States metropolitanareas; the study also quantified the benefit of increasing physicalactivity to replace 50% of these short car trips by bike. The authorsfound that eliminating short car trips decreased PM2.5 levels by0.1 μg/m3 , resulting in a health economic benefit of 3.5 billion dollars
annually and that an extra 3.8 billion dollars could be saved due toincreasing physical activity if 50% of these trips were substituted bybike trips (Grabow et al., 2011). Finally, a recent publication reportedthat, compared to mortality impacts from changes in air pollution,road traffic fatalities, and CO2 emissions, by far the greatest economicbenefits of replacing a regular 5 km commute trip by car with abicycle trip would come from increased physical activity, yieldinga 1310 € / year benefit per subject who shifts mode (Rabl andde Nazelle, 2012).
In contrast to these previous studies we have also included in thescenarios public transport as an alternative mode of transport in addi-tion to the bicycle for replacing the car trips. A further difference withthe previous studies made in this context is that we have included inthe model short (only within Barcelona City) and long trips (from andto Barcelona City) within the same metropolitan area. In addition wecombined in the analysis the health impacts of physical activity,road traffic fatality and air pollution on travellers who make theswitch between modes with the impact of pollution abatement inthe general population.
We found that the health benefits for those who would changetravel modes would be much larger than benefits to the generalpopulation, even though the total number of people affected in thegeneral population would be much larger. This is due to the strongeffects of physical activity and the relatively minor effects of air pollu-tion in the health impact analyses. The estimated health impactsfor physical activity depend though on the shape of the exposureresponse relationship and the initial physical activity levels in the

107D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
population that is shifting modes. Unfortunately we do not haveinformation on the latter, which leaves some uncertainty in theestimates.
To estimate the impact of physical activity we used a linear dose–response function reported by WHO in HEAT for walking and forcycling (Andersen et al., 2000; Kahlmeier et al., 2011). Some authorshave suggested that this dose–response function (DRF) may not belinear, and suggested a curvilinear relationship. We performed a sen-sitivity analysis transforming km cycled or walked into MetabolicEquivalent of Task (METs) to use alternative (curvilinear) dose–response functions from general physical activity and all-cause mortal-ity (Woodcock et al., 2010). Using scenarios 2 and 6 as a references,where 40% of car trips would be replaced, with the 100% of trips madeby one specific mode (bike or public transport), we estimated that67.46 deaths would be avoided by physical activity in scenario 2,using the original analysis (linear DRF) compared to 47.37 deathsavoided using the curvilinear DRF in the same scenario andwe estimat-ed for scenario 6, 38.50 deaths avoided by physical activity in the mainanalysis, compared with 62.76 deaths avoided using a curvilinear rela-tionship (see online Appendix C). Regardless of the DRF that is used,in both cases (linear or curvilinear), the estimated benefits of physicalactivity remain large. The DRF reported by Andersen et al. for physicalactivity, compare the people who cycling to work to those who donot. Some researchers suggest that this DRF also could include some de-gree of exposure to other factors such as air pollution, noise, etc. and thismay imply a double counting in our results, although, as in other publi-cations (de Hartog et al, 2010; Kahlmeier et al., 2011; Rojas-Rueda et al.,2011),we consider theDRF reported byAndersen (2000), as a referenceonly for physical activity.
For the analysis we used data and measurements obtained locally,such as air pollution concentrations, measured previously in differentmicroenvironments (car, walk, bike and bus) in Barcelona (de Nazelleet al., 2011a). To provide the most robust estimates possible, wechose as our main outcome all-cause mortality, for which the stron-gest evidence exists in the epidemiological literature. We performedsensitivity analyses to assess the stability of our results and testedeffects of deviations from our main assumptions and data choices.In the sensitivity analysis we included, for example, relative riskfunctions from the literature, choice of pollutants, age distribution,environmental and travel conditions in Barcelona. Importantly, wefound a net benefit in all the tested scenarios for mode shifts awayfrom the car.
Another important advantage of our study is the considerationof different scenarios for short (within Barcelona City) and long(between Barcelona City and Metropolitan area) trips. We assumedthat short trips could be replaced predominantly by bike trips. Andfor long trips we assumed that the replacement would be predomi-nantly by public transport. This is consistent with the WHO andothers' findings that short trips (less than 5 km) are the most likelyto be modified with policies to promote active transport (Dora andPhillips, 2000). Even with a shift to public transport for the longertrips we estimated considerable health benefits from the increase inphysical activity due to the 10‐minute walk we assumed all publictransport trips included. Further and greater benefits were estimatedfor shifts to cycling but this may also be more difficult to achieve forthese longer journeys.
We only modelled the risk and benefits of travellers aged between16 and 64 since we wanted to focus on commuters (i.e. regulartravellers) which make up the greatest part of the trips (estimates78%). We quantified the impacts from 16 years because the informa-tion derived from surveys of mobility is collected for over 16 yearsold, although the legal age to drive a car in Spain is 18 years. Weconsidered that the 16 to 18 year olds may have been car passengerswho shifted to public transport or cycling. However it is important torealise that the risk of mortality is relatively small between 16 and64 years old and that greater benefits could be expected with older
populations. In contrast the impacts of the reduction of air pollutionin the general population were modelled for all age groups accordingto the age distribution in each census tract in the city since airpollution is expected to affect everyone living in the city.
With respect to the general population air pollution modelling, wequantified the reduction in air pollution levels expected from a 20% or40% reduction in car trips within the city of Barcelona using a disper-sion model. To perform the estimations, the Barcelona dispersionmodel took into account information about different emissionsources, type of motor vehicle, weather and the street canyon effect(a more detailed description of the model is presented in onlineAppendix B). The reduction that we obtained in ambient concentra-tion of PM2.5 was small, but similar to has been reported byGrabow et al. (2011) (0.15 μg/m3 reported by Grabow et al., vs0.14 μg/m3 for 40% of car trips reduction inside Barcelona), but stillhad an impact on health, because it would affect the entire populationof the city (see Table 3). This reduction is relatively minor because a40% reduction in car trips inside Barcelona represents only a 11.8%of reduction of all traffic trips, which would result in a 5% reductionof emissions of PM2.5 and subsequently a 0.64% reduction in PM2.5ambient concentration. We also modelled the possible effects ofshift the outside Barcelona trips (scenarios 5 to 8) and foundthat the reduction of 40% of car trips represent an average annualreduction of 0.26 μg/m3 of PM2.5, avoiding 18.15 deaths annually(see Table 3 and online Appendix B).
Large reductions in PM2.5 are hard to achieve, but as a sensitivityanalysis we modelled also the health impact of a 10% reduction in theconcentration of PM2.5 (1.71 μg/m3) and estimated that in this case113 deaths would be avoided annually, in which case the healthbenefits would be larger than those for travellers. We also conductedsensitivity analyses comparing the health impacts of air pollutionestimations from the dispersion model with the Land use regression(LUR) model of the city of Barcelona, and we also applied an intakefraction approach (Humbert et al., 2011; Marshall et al., 2005) toestimate the change in mortality associated with the reductions ofPM2.5. In all cases we found that estimates from the dispersionmodel, LUR model and intake fraction were similar for all scenarios(see online Appendix C). Finally, for travellers' exposure to air pollu-tion we performed a sensitivity analysis comparing the health im-pacts of black smoke instead of PM2.5 in all scenarios. And wefound that health benefit estimations were keep similar betweenthe two exposures (see online Appendix C).
Some authors have suggested to present the results as a change inlife expectancy rather than in preventable deaths, because deathcannot be prevented but only postponed, for this reason we have alsoestimated impacts of scenarios in terms of a gain in life expectancy. Intravellers who shift the mode, we found a range of 2.8 (scenarios 5and 6) to 6.5 (scenarios 1 and 2) months gained (Table 1) and in thegeneral population we estimated 1.14 to 4.11 days gained due to thereductions in PM2.5 (Table 3).
Our scenarios were based on the new sustainable mobility planpresented by the Basque country (Gobierno Vasco, 2011; DV, 2012),which has as one of its objectives to reduce by 2020 20% of car trips.Also the Catalan Institute of Energy has proposed a 20% reduction incar trips to save the consumption of 452.000 t of oil each year (ICE,2010). We also wanted to present scenarios with a doubling of thereduction, trying to estimate the impacts of larger interventions.Perhaps our scenarios are difficult to achieve with only one specifictransport policy. These scenarios would be considered more realisticif we assumed that transport policies were not implemented alone,but as part of urban mobility plans, as proposed by the Basquecountry, that include an array of policies. However, in a recentgovernmental report of the city of Madrid a reduction of 188,000car trips in one year (2009–2010) was reported (probably due tothe economic crisis), which is a reduction similar to our most ambi-tious scenarios in Barcelona City (scenarios 2 and 4) (CES, 2011).

108 D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
Not only are the direct health benefits important, but so are alsothe potential reductions in greenhouse gas emissions. In our scenarioswe found that the reduction of 40% of car trips (inside and outsideBarcelona) can achieve a reduction of up to 200,000 t of CO2 annually,which represents 1.25% of CO2 emissions from the transport sector inCatalonia ( OCCC, 2010a).
This study shows that interventions to reduce car use in urbanareas can lead to health benefits. Also it shows that urban transportpolicies to encourage active modes of transport such as cycling orpublic transport are a great tool to increase physical activity levelsin the population, providing greater health benefits to the citizens.For this, it is critical that policy makers and stakeholders begin toconsider urban transport policies as tools, not only for improvingurban mobility, but also as tools to improve population health.
5. Conclusion
We conclude that interventions directed to reduce car use andincrease cycling and the use of public transport in metropolitanareas, like Barcelona, can produce important health benefits, relatedmostly with the increase of physical activity in travellers and second-arily the reduction of air pollution impacts in the general populationof the city. Also these interventions can help reduce emissions ofgreenhouse gases to the atmosphere.
Contributors
AdeN and MJN conceived and designed the study. DR-R and AdeNcollected the data. OT did the Barcelona air dispersion study. DR-R,AdeN and MNJ analyzed and interpreted the data and wrote themanuscript. DR-R, AdeN, OT and MNJ edited and approved the finalversion for submission. AdeN and MNJ are guarantors.
Funding
This work is part of the European wide project Transportation Airpollution and Physical ActivitieS: an integrated health risk assessmentprogamme of climate change and urban policies (TAPAS), which haspartners in Barcelona, Basel, Copenhagen, Paris, Prague, and Warsaw.TAPAS is a four year project funded by the Coca-Cola Foundation,AGAUR, and CREAL. http://www.tapas-program.org/.
Competing interests
All authors have completed the ICMJE uniform disclosure form atwww.icmje.org/coi_disclosure.pdf (available on request from thecorresponding author) and declare the following: no support fromany organization for the submitted work; no financial relationshipswith any organizations that might have an interest in the submittedwork in the previous three years; and no other relationships oractivities that could appear to have influenced the submitted work.
Ethical approval
Not required.
Acknowledgements
The dispersion model was built by the Energy and Air QualityDepartment of Barcelona Regional, and we want to thank especiallythe contribution of José Lao, who also helped to develop the emissioninventories and the air quality analysis in this model. The landuse regression models were constructed as part of the ESCAPEproject. Rob Beelen and Gerard Hoek (IRAS, NL) and Kees de Hoogh(Imperial College London, UK) guided the work and we would liketo acknowledge their important contribution. We also would like to
thank Marta Cirach who conducted the scenarios for the concentra-tion reduction using the land use regression models. In previousanalyses furthermore we would like to thank Marko Tainio whohelped to define the sensitivity scenarios in previous analyses.
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.envint.2012.08.009.
References
Aarnio P, Yli-Toumi T, Kousa A, Makela T, Hirsikko A, Hameri K, et al. The concentrationsand composition of and exposure to fine particles (PM2.5) in the Helsinki subwaysystem. Atmos Environ 2005;39:5059–66.
Adams HS, Nieuwenhuijsen MJ, Colvile RN, McMullen MA, Khandelwal P. Fine particle(PM2.5) personal exposure levels in transport microenvironments, London, UK. SciTotal Environ 2001;279:29–44.
Andersen LB, Schnohr P, Schroll M, Hein HO. All-cause mortality associated withphysical activity during leisure time, work, sports, and cycling to work. Arch InternMed 2000;160:1621–8.
ASPB. Reporte de accidentalidad en Barcelona 2002–2010. Barcelona: Agencia de SaludPública de Barcelona; 2011.
CES. Situación Económica y Social de la Comunidad de Madrid 2010. Madrid: ConsejoEconómico y Social de la Comunidad de Madrid; 2011.
Cheng Y-H, Lin Y-L, Liu Ch-Ch. Levels of PM10 and PM2.5 in Taipei rapid transit system.Atmos Environ 2008;42:7242–9.
de Hartog JJ, Boogaard H, Nijland H, Hoek G. Do the health benefits of cycling outweighthe risks? Environ Health Perspect 2010;118:1109–16.
de Nazelle A, Rodriguez DA, Crawford-Brown D. The built environment and health:impacts of pedestrian-friendly designs on air pollution exposure. Sci Total Environ2009;407:2525–35.
de Nazelle A, Fruin S, Westerdahl D, Martinez D, Matamala J, Kubesch N, et al. Trafficexposures and inhalations of Barcelona commuters. Epidemiology 2011a;22:S77–8.
de Nazelle A, Nieuwenhuijsen MJ, Antó JM, Brauer M, Briggs D, Braun-Fahrlander C,et al. Improving health through policies that promote active travel: a review ofevidence to support integrated health impact assessment. Environ Int 2011b;37:766–77.
DGT. Parque Nacional Automóvil, distribuido por provincias, tipos y carburantes.Madrid: Dirección General de Tráfico; 2008.
Dora C, Phillips M. Transport, environment and health. Copenhagen: World HealthOrganization; 2000.
DSM. Dades Bàsiques de Mobilitat 2009. Direcció de Serveis de Mobilitat. Barcelona:Ajuntament de Barcelona; 2010.
DSM. Dades Bàsiques de Mobilitat 2010. Direcció de Serveis de Mobilitat. Barcelona:Ajuntament de Barcelona; 2011.
DV. Cómo hacer desaparecer los coches, Diario Vasco. [16-01] http://www.diariovasco.com 2012Accesed on June 26, 2012 (in Spanish).
Edwards RD. Public transit, obesity, and medical costs: assessing the magnitudes. PrevMed 2008;46:14–21.
EEA. The European environment. State and outlook 2010, urban environment. Copenhagen:European Environment Agency; 2010.
GENCAT. Análisis de la Mortalidad en Cataluña, 2007. Servicio de Informacióny Estudios. Barcelona: Generalitat de Catalunya; 2010.
GESOP. Barómetro anual de la bicicleta. Gabinet d'Estudis Socials i Opinió Pública.Barcelona: Fundación ECA Bureau Veritas; 2009.
Gobierno Vasco. Plan Director de Movilidad Sostenible, Euskadi 2020. Bilbao:Departamento de Vivienda Obras Publicas y Transporte; 2011.
Grabow ML, Spak SN, Holloway T, Stone JB, Mednick AC, Patz JA. Air quality andexercise-related health benefits from reduced car travel in the midwestern UnitedStates. Environ Health Perspect 2011;120:68–76.
Humbert S, Marshall JD, Shaked S, Spadaro JV, Nishioka Y, Preiss P, et al. Intake fractionfor particulate matter: recommendations for life cycle impact assessment. EnvironSci Technol 2011;45:4808–16.
Hunt A. Policy interventions to address health impacts associated with air pollution,unsafe water supply and sanitation, and hazardous chemicals. OECD environmentworking papers; 2011.
ICE. Mobilitat. Instituto Catalan de Energía; 2010 [http://www20.gencat.cat/portal/site/icaen Accesed on June 26, 2012 (in Catalan)].
Joffe M, Mindell J. A framework for the evidence base to support health impact assessment.J Epidemiol Community Health 2002;56:132–8.
Johansson C, Johansson P. Particulate matter in the underground of Stockholm. AtmosEnviron 2003;37:3–9.
Kahlmeier S, Cavill N, Dinsdale H, Rutter H, Gotschi T, Foster C, et al. Health economicassessment tools (HEAT) for walking and for cycling. Copenhague: World HealthOrganization; 2011.
Krewski D, Jerrett M, Burnett RT, Ma R, Hughes E, Shi Y, et al. Extended follow-upand spatial analysis of the American Cancer Society Study linking particulate airpollution and mortality., 140. Boston, USA: HEI (Health Effects Institute); 2009.p. 1-140.[Research Report].
Lao J, Teixido O. Air quality model for Barcelona. 19th International conference onmodelling. Monitoring and Management of Air Pollution; 2011.

109D. Rojas-Rueda et al. / Environment International 49 (2012) 100–109
Lindsay G, Macmillan A, Woodward A. Moving urban trips from cars to bicycles: impacton health and emissions. Aust N Z J Public Health 2011;35:54–60.
Litman T. Evaluating public transportation health benefits. The American PublicTransportation Association. Victoria Transport Policy Institute; 2010.
Marshall JD, Teoh S, Nazaroff W. Intake fraction of nonreactive vehicle emissions in USurban areas. Atmos Environ 2005;39:1363–71.
Miller BG, Hurley JF. Life table methods for quantitative impact assessments in chronicmortality. J Epidemiol Community Health 2003;57:200–6.
OCCC. Cataluña y los objetivos de reducción de emisiones de gases de efecto invernadero.Primer reporte. Barcelona: Oficina Catalana del Cambio Climático; 2010a.
OCCC. Guía Práctica para el cálculo de emisiones de gases de efecto invernadero.Barcelona: Oficina Catalana del Cambio Climático; 2010b.
Park DU, Ha KC. Characteristics of PM10, PM2.5, CO2 and CO monitored in interiors andplatforms of subway train in Seoul, Korea. Environ Int 2008;34:629–34[Jul].
Perez L, Kunzli N. From measures of effects to measures of potential impact. Int J PublicHealth 2009;54:45–8.
Pope III CA, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, et al. Lung cancer, cardio-pulmonary mortality, and long-term exposure to fine particulate air pollution.JAMA 2002;287:1132–41.
Rabl A, de Nazelle A. Benefits of shift from car to active transport. Transp Policy2012;19:121–31.
Ripanucci G, Grana M, Vicentini L, Magrini A, Bergamaschi A. Dust in the undergroundrailway tunnels of an Italian town. J Occup Environ Hyg 2006;3:16–25.
RMB. Encuesta demovilidad Cotidiana 2006. Barcelona: RegiónMetropolitana de Barcelona;2006.
Rojas-Rueda D, de Nazelle A, Tainio M, Nieuwenhuijsen MJ. The health risks and benefitsof cycling in urban environments compared with car use: health impact assessmentstudy. BMJ 2011;343:d4521.
Santamariña E, Perez C. Accidents I Lesionats De Trànsit A Barcelona 2002–2007.Barcelona: Agencia de Salut Publica de Barcelona; 2008.
Schwela D, Zali O, Schwela P. Motor vehicle air pollution public health impact andcontrol measures. Geneva: World Health Organization; 2008.
The World Bank. Urban transport projects: patterns and trends in lending, 1999–2009.Department for international development. Washington: The International Bankfor Reconstruction and Development; 2011.
UNEP. Share the road: investment in walking and cycling road infrastructure. Nairobi:United Nations Environment Programme; 2010.
US EPA. Guide to sustainable transportation performance measures. US, EnvironmentalProtection Agency; 2011.
WHO. Global burden of disease 2004. World Health Organization; 2008.WHO-UNECE. Transport, Health and Environment Pan-European Programme (THE PEP).
World Health Organization — United Nations Economic Commission for Europe;2010.
Woodcock J, Edwards P, Tonne C, Armstrong BG, Ashiru O, Banister D, et al. Publichealth benefits of strategies to reduce greenhouse-gas emissions: urban landtransport. Lancet 2009;374:1930–43.
Woodcock J, Franco OH, Orsini N, Roberts I. Non-vigorous physical activity andall-cause mortality: systematic review and meta-analysis of cohort studies. IntJ Epidemiol 2010;40:121–38.