Embed Size (px)
Citation preview

Research ArticleHigh Prevalence of Panton-Valentine Leukocidin (PVL)Genes in Nosocomial-Acquired Staphylococcus aureus Isolatedfrom Tertiary Care Hospitals in Nepal
Bidya Shrestha1 Winny Singh2 V Samuel Raj2
Bharat Mani Pokhrel3 and Tribhuban Mohan Mohapatra4
1 Tri-Chandra Campus Tribhuvan University GPO Box 3285 Kathmandu Nepal2 New Drug Discovery Research Ranbaxy Research Laboratories R amp D III Sector-18 Gurgaon India3 Institute of Medicine Tribhuvan University Kathmandu Nepal4 Institute of Medical Sciences Banaras Hindu University Varanasi India
Correspondence should be addressed to Bidya Shrestha b shrestha 07hotmailcom
Received 7 March 2014 Revised 1 June 2014 Accepted 4 June 2014 Published 18 June 2014
Academic Editor Ana Lucia Nascimento
Copyright copy 2014 Bidya Shrestha et alThis is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Methicillin-resistant Staphylococcus aureus (MRSA) carrying the important virulence determinant Panton-Valentine leukocidin(PVL) is an emerging infectious pathogen associatedwith skin and soft tissue infections as well as life-threatening invasive diseasesIn carrying out the first PVL prevalence study in Nepal we screened 73 nosocomial isolates of S aureus from 2 tertiary care Nepalihospitals and obtained an overall PVL-positivity rate of 356 among the hospital isolates 261 of MRSA and 519 of methicillinsensitive S aureus (MSSA) isolates were found to be positive for the PVL genes PVL prevalence was not associated with a specific(i) infection site (ii) age group or (iii) hospital of origin It was found to be positively associated with heterogeneousMRSA (733)compared to homogeneous MRSA (32) and MSSA (519) negatively associated with multiresistant MRSA (22) compared tononmultiresistant MRSA (60) and MSSA (519) and positively associated with macrolide-streptogramin B resistance (938)compared to macrolide-lincosamide-streptogramin B resistance (0) and no-resistance (458) types Macrolide-streptogramin Bresistance was confirmed by the presence ofmsr(A) gene Restriction pattern analyses provided evidence to support the circulationof a limited number of clones of PVL-positive MRSA arguing for the adaptability of these isolates to a hospital setting
1 Introduction
First reported in 1932 Panton-Valentine leukocidin (PVL)is a potent cytotoxin and an important virulence factor ofStaphylococcus aureus The toxin causes tissue necrosis andselectively disrupts leukocyte membranes thus leading toenhanced virulence Comprising two exoproteins encoded bytwo contiguous cotranscribed phage-encoded genes lukS-PV and lukF-PV [1 2] PVL has been epidemiologicallyassociated with virulent and highly transmissible strains of Saureus PVL-carrying S aureus strains can cause serious skinand soft tissue infections and life-threatening invasive dis-eases like necrotizing fasciitis [3] purpura fulminans [4]and necrotizing hemorrhagic pneumonia [5] PVL-relatedinfections exhibit a preference towards attacking skin and soft
tissues [6] but when the infection spreads to the lungs theresulting necrotizing pneumonia rapidly destroys lung tissueand it has been proven to be lethal in 75 of the cases [7]
PVL-positive S aureus as a rapidly emerging worldwidephenomenon is exerting a powerful presence in the globalpublic health landscape Even though heightened surveil-lance and improved case recognition might have playeda role in increased reporting of such strains the rapidgrowth of PVL-carrying S aureus nonetheless should notbe undermined In 2010 Shallcross and colleagues reporteddata from the United Kingdom where 20 of S aureusisolates obtained from skin and soft tissue infections werecharacterized as PVL positive [8] This is an alarming risefrom the 16 prevalence rate of PVL-positive S aureusreported in the country in 2005 [9] Evenwithin the timespan
Hindawi Publishing CorporationBioMed Research InternationalVolume 2014 Article ID 790350 7 pageshttpdxdoiorg1011552014790350
2 BioMed Research International
Table 1 PVLprevalence grouped according to infection site age groupmethicillin resistance andmacrolide lincosamide and streptograminB resistance types
PVL-negative isolates () PVL-positive isolates ()
Infection site
Body fluid (119899 = 2) 1 (500) 1 (500)SSI (119899 = 54) 35 (648) 19 (353)Lower RTI (119899 = 9) 7 (778) 2 (222)UTI (119899 = 8) 4 (500) 4 (500)
Age group le30 years (119899 = 27) 17 (630) 10 (370)ge31 years (119899 = 46) 30 (652) 16 (348)
Methicillin resistance
MSSA (27) 13 (481) 14 (519)MRSA (46) 34 (739) 12 (261)
(i) Heterogeneous MRSA (119899 = 15) 4 (267) 11 (733)(ii) Homogeneous MRSA (119899 = 31) 30 (968) 1 (32)
(i) nmMRSA (119899 = 5) 2 (400) 3 (600)(ii) mMRSA (119899 = 41) 32 (780) 9 (220)
Macrolide lincosamide andstreptogramin B resistance
No resistance (119899 = 24) 13 (542) 11 (458)MSB (119899 = 16) 1 (62) 15 (938)MLSB (119899 = 32) 32 (1000) 0 (00)
SSI surgical site infection RTI respiratory tract infection UTI urinary tract infection nmMRSA nonmultiresistant MRSA mMRSA multiresistant MRSAMSB macrolide-streptogramin B resistance MLSB macrolide-lincosamide-streptogramin B resistance
of one year between 2005 and 2006 Ellington et al noted a 2-fold increase in PVL-positive S aureus in England andWales[10] Comparatively countries in western and central Africaboast a higher prevalence rate at 57 raising valid concernsfor the spread of virulent PVL-positive MRSA clones [11]Along similar lines data from across the globe paints a variedpicture for the prevalence of PVL-positive S aureus 128 inChina [12] 30 inGermany [13] 18 in Ireland [14] 09 inKorea [15] 116 in Singapore [16] 4 in Turkey [17] and astriking 97 in the United States [18 19]
Albeit being a relatively recent phenomenon S aureusclones that combine PVL production with methicillin resis-tance are rapidly emerging This global emergence andpropagation of clones combining methicillin resistance andPVL toxin production necessitates commensurate counterac-tion with improved vigilance enhanced case ascertainmentand effective management of PVL-related disease Rightfullyregarded as a ldquosuperbugrdquo methicillin-resistant S aureus(MRSA) by itself is a prominent cause of nosocomial infec-tions and has been exacting a substantial toll on healthcareresources worldwide [20 21] Acquisition of the PVL genesby MRSA therefore represents a challenging conundrum indisease management and infection control
To date PVL has emerged as a significant virulencefactor of community-acquired MRSA (CA-MRSA) [22] withrelatively rare incidence of the toxin in hospital-acquiredMRSA (HA-MRSA) infections We conducted this studyto investigate PVL prevalence among hospital isolates ofS aureus in tertiary care facilities of Nepal To the bestof our knowledge this report on PVL carriage and genedetection is the first of its kind in Nepal In this study weexplore the following the presence of PVL genes in both HA-MSSAandHA-MRSA the association betweenPVLgene and
methicillin susceptibility pattern its linkage with macrolidelincosamide and streptogramin resistance pattern and theepidemiologic molecular typing of PVL-positive S aureus byPCR-RFLP
2 Material and Methods
21 Clinical Isolates A total of 404 consecutive nonrepeatnosocomial S aureus isolates were obtained from Lalitpur-Based Hospital (119899 = 100) and Kathmandu-Based Hospital(119899 = 304) from November 2007 to June 2009 A nosocomialinfection was defined as any infection acquired by a patientafter 48 hours of hospital admission Isolate identificationwasbased on observed fermentation in oxidation-fermentationtest and positivity for catalase clumping factor staphylo-coagulase DNase staphytect plus and mannitol fermen-tation The isolates were categorized into four groups onthe basis of infection sites (Table 1) body fluid surgicalsite infection (SSI) lower respiratory tract infection (RTI)and urinary tract infection (UTI) Antibiotic susceptibilityprofiles were developed using penicillin oxacillin cefoxitinerythromycin clindamycin cotrimoxazole chlorampheni-col ciprofloxacin rifampicin gentamicin and tetracycline(Oxoid Japan) as recommended by Clinical and LaboratoryStandards Institute (CLSI) 2007 [23] However for urinaryisolates erythromycin ciprofloxacin and chloramphenicolwere replaced by novobiocin (to allow for the differentiationbetween S aureus and S saprophyticus) norfloxacin andnitrofurantoin (Oxoid Japan)
MSSA and MRSA were identified based on their respec-tive sensitivity or resistance to both oxacillin and cefox-itin Oxacillin disc diffusion test result was confirmed byminimum inhibitory concentration (MIC) using the E test
BioMed Research International 3
(a)
Coefficient000 066 132 198 265
48
62
72
78
117
193
198
154
161
120
3
41
21
29
147
177
(b)
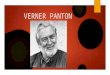
Figure 1 (a) PCR-RFLP of coa and spa amplified products of PVL-positive MRSA (12 isolates 48ndash198) and PVL-negative MRSA (4 isolates3ndash41) digested by HaeII M = 1 kb DNA ladder PVL-negative MRSA isolates cluster under a single restriction pattern while PVL-positiveMRSA isolates demonstrate clustering under two distinct restriction types type I (48ndash120 154ndash161 and 193ndash198) and type II (147 177) Theisolates were obtained from two tertiary care hospitals (b) Corresponding dendogram of the PCR-RFLP of PVL-positive and PVL-negativeMRSA isolates
and microbroth dilution Methicillin resistance was furtherconfirmed by the amplification of mecA gene by polymerasechain reaction and by the MRSA screen test for the detectionof the protein PBP2a responsible for reduced affinity ofMRSA to 120573-lactam antibiotics (Denka Seiken Japan)
Heterogeneous MRSA was identified on the basis of (i)the presence of colonies inside the oxacillin and cefoxitinzones of inhibition in the disc diffusion test and inside theoxacillin strip inhibition zone in the E test and (ii) oxacillinMIC valueslt100 120583gmL in E test andmicrobroth dilution test[24] Also on the basis of resistance to non-120573-lactam antibi-otics MRSA isolates were grouped as multiresistant (resis-tant to ge3) and nonmultiresistant (resistant to le2) MRSAas described by Gosbell and colleagues in 2001 [25]
And finally macrolide-lincosamide-streptogramin B(MLSB) and macrolide-streptogramin B(MSB) resistancetypes were assessed via D test using erythromycin andclindamycin [23] Isolates resistant to erythromycin andsusceptible to clindamycin were identified as MSB resistancetype isolates resistant to both erythromycin and clindamycinas MLSB resistance type and isolates sensitive to bothantibiotics as no-resistance type MLSB and MSB resistancewere confirmed by the amplification of erm(A) erm(B)erm(C) andmsr(A) as described by Lina et al 1999 [6] MSBresistance was supported by the detection ofmsr(A) gene
22 PVL Genes Identification From our pool of clinical iso-lates 46 MRSA and 27 MSSA (total 73 isolates) were geneti-cally analyzed for PVLpositivity by screening for the presenceof the adjacent cotranscribed luk-PV genes namely lukS-PVand lukF-PV which encode the Panton-Valentine leukocidintoxin These 73 isolates were randomly selected to includehomogenous MRSA heterogeneous MRSA and MSSA Saureus ATCC 29213 and S aureus ATCC 49775 were usedas negative and positive controls respectively The primers(Sigma-Aldrich Germany) used for the coamplification of
PVL genes lukS-PV and lukF-PV were lukPV-1 (51015840-ATC ATTAGG TAAAAT GTC TGGACA TGA TCC A) and luk-PV-2(51015840-GCA TCA ACT GTA TTG GAT AGC AAA AGC) [26]Total DNA was isolated from the clinical isolates and usedas template for PVL gene identification The samples weredenatured at 94∘C for 3 minutes followed by 30 cycles of thefollowing steps denaturation at 94∘C for 30 seconds anneal-ing at 55∘C for 30 seconds extension at 72∘C for 1 minuteand final extension at 72∘C for 5 minutes [6] The imageswere visualized and analyzed in Gel Doc (Bio-Rad USA)by using the Quantity One 1-D Analysis Software
23 PCR-RFLP for Coa and Spa From the study samplesize of 73 clinical isolates all the PVL-positive isolates wereselected for PCR-RFLP including 12 MRSA and 14 MSSAisolates (further described in Section 3) The coa and spagenes of these 26 PVL-positive isolates (12 MRSA and 14MSSA) and additional 9 PVL-negative isolates (4 MRSA and5MSSA) were amplified using the primer pairs coa1 (51015840-CGAGAC CAA GAT TCA ACA AG) and coa2 (51015840-AAA GAAAAC CAC TCA CAT CAG T) and spa1 (51015840-ATC TGG TGGCGTAACACCTG) and spa2 (51015840-CGCTGCACCTAACGCTAA TG) (Sigma Aldrich Germany [27])
PCR-RFLP was carried out using HaeII digestion of theamplified products Unique PCR-RFLP patterns obtainedfollowing the electrophoresis of the HaeII digested PCRproducts were each designated as an independent restrictionpattern (Figures 1 and 2)
24 Susceptibility Patterns of the PVL-Positive and PVL-Negative MRSA and MSSA MIC of 12 different antibioticswas determined for 26 PVL-positive (12MRSA and 14MSSA)and 9 PVL-negative isolates (4 MRSA and 5 MSSA) bymicrobroth dilution [23] The antibiotics included fusidicacid tetracycline Augmentin clindamycin levofloxacinerythromycin trimethoprim-sulfamethoxazole gentamicin
4 BioMed Research International
(a)
Coefficient000 059 118 177 237
H30
194
14
31
185
54
16
47
190
32
109
118
46
149
189
(b)
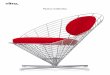
Figure 2 (a) PCR-RFLP of coa and spa amplified products of PVL-positive MSSA (14 isolates 14ndash194) and PVL-negative MSSA (3 isolates79ndash113) digested by HaeIIM = 1 kb DNA ladder PVL-positive MSSA isolates 16 and 47 cluster under one restriction type and isolates 14 31and 185 cluster under another The remaining nine PVL-positive MSSA isolates and all three PVL-negative MSSA isolates exist as singletons(b) Corresponding dendogram of the PCR-RFLP of PVL-positive and PVL-negative MSSA isolates
vancomycin linezolid kanamycin and rifampicin (Sigma-Aldrich Germany) The clinical isolates were suspendedin physiological saline (05 McFarland) using Densimat(Biomerieux Italy) followingwhich 100120583L of each suspendedisolate was dispensed into microtiter wells containing dou-bling dilutions of the 12 antibiotics in cation-adjustedMuellerHinton Broth (Becton Dickinson and Company USA) Themicrotiter plates were incubated at 37∘C for 18 hrs and wereread in reflected light
Data was analyzed using the statistical software SPSS 115
3 Results
The source sample of 404 hospital-acquired isolates consistedof 197 (488) MRSA isolates of which 148 (751) werehomogenous and 49 (249) were heterogeneous [28] Asmentioned earlier from the total sample of 404 clinicalisolates 73 isolates were randomly selected for further anal-ysis owing to resource limitations Of these 73 isolates thatcomprised of 46 MRSA and 27 MSSA isolates PVL genewas detected in 12 MRSA (261) and 14 MSSA (519) for acumulative prevalence rate of 356 As indicated in Table 1the PVL carriage was high in samples from UTI (50 48)SSI (352 1954) and lower RTI (222 29) Howevercross tab calculation between UTI and SSI (1198832 = 0655119875 = 0418) and SSI and lower RTI (1198831198912 = 0583 119875 = 0445)showed that the difference in PVL prevalence in these sitesdid not reach statistical significance
For our analysis the patient population was grouped into2 age groups le30 years (119899 = 27) and ge31 years (119899 = 46) ThePVL-positivity rates were 37 for le30 age group and 348for ge31 age group (Table 1) these values were not found to bestatistically significantly different (1198832 = 0038 119875 = 0846)We also did not find any association between PVL positivityand hospital of origin (Table 2) The PVL prevalence of 321at KBH and of 450 at LBH did not meet the statisticalcriteria for significant difference (1198832 = 1058 119875 = 0304)
Upon conducting a pooled evaluation of isolates fromboth hospitals PVL prevalence rates were found to be 733in heterogeneous MRSA 519 inMSSA and 32 in homo-geneous MRSA (Table 1) PVL occurrence was observed tobe significantly associated with a heterogeneous methicillinresistance pattern compared to homogeneous MRSA andMSSA (1198832 = 2659 119875 lt 0001) However a pooled sample ofboth homogeneous and heterogeneous MRSA failed to showany correlation with PVL carriage when compared to MSSA(1198832 = 4925 119875 = 0026)
As mentioned previously MRSA that was resistant toge3 non-120573-lactam antibiotics was categorized as multire-sistant MRSA (mMRSA) and that resistant to le2 non-120573-lactam antibiotics was identified as nonmultiresistant MRSA(nmMRSA) The distribution of PVL carriage rates was519 amongMSSA 60 among nmMRSA and 22 amongmMRSA (Table 1) Compared to MSSA and nmMRSAmMRSA had lesser prevalence of PVL positivity (1198832 = 7739119875 = 0021)
In assessing the putative relation between PVL prevalenceand macrolide lincosamide and streptogramin resistancetypes we found that none of the isolates withMLSB resistance(119899 = 32) was positive for PVL Among MSB resistancetypes PVL positivity was at 938 and among nonresistantisolates depicting susceptibility to both erythromycin andclindamycin PVL carriage was at 458 (Table 1) We foundthat MSB resistance types were significantly associated withPVL gene carriage when compared toMLSB resistance (119883
2=
4211 119875 lt 0001) and no-resistance types (1198832 = 9689 119875 =0002) Isolates susceptible to erythromycin and clindamycin(no-resistance type) had 177 greater odds of being PVL neg-ative as compared to MSB resistance types (OR = 17727 95CI 20 to 1565)
The MSB resistance type was genotypically confirmed bythe presence ofmsr(A) geneThe isolates harboring this genedepicted a strong associationwithPVLgene possession (1198832 =12049119875 = 0001) Compared to isolates carrying themsr(A)
BioMed Research International 5
Table 2 Hospital-specific PVL prevalence rates and methicillin resistance in S aureus
Strains (119899) Lalitpur Hospital Kathmandu Hospital TotalPVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos
MSSA (27) 4 3 571 10 10 500 519 (1427)Homo-MRSA (31) 0 7 385a 1 23 212b 261 (1246)Hetero-MRSA (15) 5 1 6 3Total (73) 9 11 450 17 36 321 356 (2673)aTotal PVL-positive prevalence rate in Lalitpur HospitalbTotal PVL-positive prevalence rate in Kathmandu HospitalHetero heterogeneous Homo homogeneous Pos positive Neg negative
gene no-resistance type isolates lacking this gene were 455times more likely to be not positive for PVL (OR = 455 95CI 35 to 5947)
The MIC of the 26 PVL-positive and 7 PVL-negativeisolates was determined by microbroth dilution method Nosubstantial difference could be noted in the resistance patternbetween PVL-positive and PVL-negative S aureus strains(both MRSA and MSSA) with the exception of tetracyclineand clindamycin to which PVL-positive and PVL-negativeisolates responded differently It was observed that whilePVL-positive MRSA was sensitive to both clindamycin andtetracycline PVL-negative MRSA was uniformly resistantto these antibiotics Further both PVL-positive and PVL-negativeMSSA isolateswere also sensitive to clindamycin andtetracycline
With regard to restriction types identified by PCR-RFLPPVL-positive MRSA PVL-negative MRSA PVL-positiveMSSA and PVL-negative MSSA isolates depicted two oneeleven and three restriction types respectively (Figures 1 and2) The majority of the PVL-positive MRSA isolates wereclustered under one restriction type (1012 DNA fragmentslength 400 bp and 750 bp) with the remaining two isolatesbeing grouped under the second restriction type (212 DNAfragments length 500 bp and 800 bp) All four isolates of PVL-negative MRSA belonged to a single restriction type ForPVL-positive MSSA two and three isolates were includedunder two distinct restriction types while the remainingnine isolates and all three of the PVL-negative MSSA isolatesexisted as singletons within their unique restriction types(Figure 2)
4 Discussion
In the present day context when microbial antibiotic resis-tance is progressively morphing into an intractable predica-ment acquisition of the potent PVL gene by MRSA whichrepresents a rather difficult challenge in itself would pavethe way to an alarming healthcare paradox In this paper wepresent the findings from the first PVL prevalence study inNepal which includes (i) heretofore unidentified associationsbetween PVL positivity and MSB resistance verified bymsr(A) gene (ii) PVL carriage rates specific to MRSA andMSSA isolates obtained from two premiere tertiary carehospitals (iii) evaluation of putative predilection of PVL-positive S aureus to a select patient profile (iv) compar-ative assessment of PVL prevalence among heterogeneous
MRSA-homogeneous MRSA-MSSA and among mMRSA-nmMRSA-MSSA and (v) restriction pattern characterizationof PVL-positive and PVL-negative hospital isolates
In the current study we report PVL gene carriage rateof 356 among nosocomial S aureus isolates 261 amongMRSA and 519 among MSSA (Table 1) These numberstrack along some of the highest reported PVL-positive Saureus prevalence rates and should rightfully be regarded as amatter of grave concern Further restriction pattern analysesof PVL-positive MRSA and MSSA have revealed that whilePVL-positive MSSA can be grouped into eleven restrictiontypes with a majority of the isolates existing as singletons(Figure 2) PVL-positiveMRSA seamlessly clusters under tworestriction types (Figure 1)This is an anticipated finding sinceMRSA isolates belong to a single clone while MSSA isolatespropagated from multiple clones Such spread of a limitednumber of PVL-carrying MRSA clones suggests that com-pared to their MSSA counterparts these microbes are well-adapted to thrive in the hospital environmentThe restrictiontype limitationwould also follow from the fact that theMRSAisolates are hospital strains that cause infection in any sus-ceptible host with the right combination of risk factors Alsothe restriction pattern clusters included isolates from bothLBH and KBH suggesting an interhospital transmission ofpathogenic strains These findings in conjunction with thehigh PVL-positive S aureus prevalence rates warrant theimmediate institution of effective infection control measures
In addition to clone limitation lack of any trend ofhigher PVL prevalence among a younger age group is anotherfinding explained by the hospital-acquired nature of the PVL-positive S aureus strains in the study At prevalence rates of37 for le30 years age group and 348 for ge31 years agegroup (Table 1) the PVL-positive isolates fail to show any age-related predilection Previous studies have shown a strongpredisposition of PVL-positive S aureus isolates for youngerand previously healthy patients [14 29] In a 2008 Australianstudy by Munckhof et al the authors observed a steadydecline in PVL occurrence with increasing age which theyascribed to age-associated strengthening of immunity and tothe natural penchant of children and young adults to acquirePVL-positive S aureus from skin contamination duringplayful and contact sports [29] This increased likelihood ofPVL-positive S aureus to infect younger age groups as seenin earlier studies may be attributed to the fact that a majorityof PVL-carrying S aureus isolates from these studies werecommunity-acquired In contrast our study exclusively
6 BioMed Research International
investigated nosocomial isolates which regardless of age caninfect any patient presenting with the right risk factors foracquiring an infection originating in the hospital
As with age PVL prevalence also exhibited no associationwith infection site or hospital of origin Although the highestnumbers of PVL-carrying S aureus isolates were recoveredfrom UTI (50) followed by SSI (352) and lower RTI(222) the prevalence rate difference between the sites didnot reach statistical significance (Table 1) Along similar linesthe 45 carriage rate of PVL gene in LBHwas not statisticallysignificantly different from the 321 prevalence rate at KBH(Table 2) On the basis of vastly different occurrence of thePVL-positive organisms in different parts of the world itappears that the PVL carriage depends largely on the geo-graphical location and the organisms that are endemic in aparticular locality
Overall PVL carriage rates were 519 (1427) amongMSSA 733 (1115) among heterogeneous MRSA and 32(131) among homogeneous MRSA (Table 1) Comparedto MSSA and homogeneous MRSA heterogeneous MRSAdepicted a positive association with PVL carriage Howeverwhen heterogeneous and homogeneous MRSA were pooledtogether into a single cohort of MRSA isolates and comparedto MSSA MRSA was found to have a negative associationwith PVL prevalence The negative correlation between PVLand MRSA as a whole can be attributed to the 30 (968)PVL-negative homogeneousMRSA isolates which would off-set the PVL positivity of the 11 (733) heterogeneous MRSAisolates These findings suggest that in the observed hospitalsettings PVL positivity was associated with heterogeneousMRSA but not with homogeneous MRSA Consequentlycrude analyses ofMSSAversus pooledMRSA strains could bepotentially misleading a thorough evaluation of PVL emer-gence should constitute a breakdown of MRSA into homo-geneous and heterogeneous strains
A phenotypic analysis of the clinical isolates based ontheir antibiotic profiles allowed for a grouping of the isolatesinto 3 categories each of which revealed a relatively highPVL prevalence 60 nmMRSA 22 mMRSA and 519MSSA (Table 1) Munckhof and colleagues (2008) [29] reporta similar rate of PVLpositivity among their nmMRSA isolates(55) However their PVL prevalence rates of 2 amongmMRSA and 16 among MSSA are much lower comparedto this study
Classifying the clinical isolates cohort on the basis ofmacrolide lincosamide and streptogramin resistance typesit was found that while PVL positivity was 938 forMSB and458 for no-resistance types none of the isolates withMLSBresistance harbored the PVL gene (Table 1) This finding thatisolates characterized as MSB resistance type are more likelyto depict PVL positivity compared to either MLSB resistanceor no-resistance type was verified by testing for the presenceof msr(A) gene which showed a positive association withPVL
While it would have been ideal to carry out these molec-ular epidemiological analyses on the entire cohort of 404 iso-lates the study needed to limit its sample size to 73 randomlyselected isolates due to resource and monetary restric-tions Todayrsquos context of PVL diagnosis and epidemiology
is constrained by the lack of a reliable phenotypic testfor PVL positivity Studies that focus on developing suchnovelmethodologies for phenotypic characterization of PVL-positive bacterium which would complement the currentlyavailable genetic test will have substantial utility in promot-ing the early detection of these virulent microbes
5 Conclusion
Our study has shown a relatively high prevalence rate of PVLpositivity in HA-S aureus isolates from two tertiary care hos-pitals of Nepal PVL carriage was associated with heteroge-neous MRSA and MSB resistance type (confirmed bymsr(A)gene positivity) Compared toMSSAandnmMRSAmMRSAwas significantly less likely to harbor the PVL genes Noassociationwith age site of infection or hospital of originwasobserved Such an absence of predilection for a younger agegroup and the observed restriction pattern limitation of PVL-positive MRSA are in alignment with the fact that these wereclinical isolates obtained from hospital-acquired infectionsThe relatively high rates of PVL presence among HA-MRSAandHA-MSSA isolates and the interhospital spread of strainssupport the need for system-wide implementation of patientsafety and infection control initiatives
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] J Kaneko and Y Kamio ldquoBacterial two-component and hetero-heptameric pore-forming cytolytic toxins structures pore-formingmechanism and organization of the genesrdquo BioscienceBiotechnology and Biochemistry vol 68 no 5 pp 981ndash10032004
[2] G Prevost B Cribier P Couppie et al ldquoPanton-valentineleucocidin and gamma-hemolysin from Staphylococcus aureusATCC 49775 are encoded by distinct genetic loci and have dif-ferent biological activitiesrdquo Infection and Immunity vol 63 no10 pp 4121ndash4129 1995
[3] L GMiller F Perdreau-Remington G Rieg et al ldquoNecrotizingfasciitis caused by community-associated methicillin-resistantStaphylococcus aureus in Los AngelesrdquoTheNewEngland Journalof Medicine vol 352 no 14 pp 1445ndash1453 2005
[4] G R Kravitz D J Dries M L Peterson and P M SchlievertldquoPurpura fulminans due to Staphylococcus aureusrdquo ClinicalInfectious Diseases vol 40 no 7 pp 941ndash947 2005
[5] B McGrath F Rutledge and E Broadfield ldquoNecrotisingpneumonia Staphylococcus aureus andPanton-Valentine leuko-cidinrdquo The Journal of the Intensive Care Society vol 9 pp 170ndash172 2008
[6] G Lina Y Piemont F Godail-Gamot et al ldquoInvolvement ofPanton-Valentine leukocidin-producing Staphylococcus aureusin primary skin infections and pneumoniardquo Clinical InfectiousDiseases vol 29 no 5 pp 1128ndash1132 1999
[7] Y Gillet B Issartel P Vanhems et al ldquoAssociation betweenStaphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia
BioMed Research International 7
in young immunocompetent patientsrdquoThe Lancet vol 359 no9308 pp 753ndash759 2002
[8] L J Shallcross K Williams S Hopkins R W Aldridge AM Johnson and A C Hayward ldquoPanton-Valentine leukocidinassociated staphylococcal disease a cross-sectional study at aLondon hospital Englandrdquo Clinical Microbiology and Infectionvol 16 no 11 pp 1644ndash1648 2010
[9] A Holmes M Ganner S McGuane T L Pitt B D Cooksonand A M Kearns ldquoStaphylococcus aureus isolates carryingpanton-valentine leucocidin genes in England and Wales fre-quency characterization and association with clinical diseaserdquoJournal of Clinical Microbiology vol 43 no 5 pp 2384ndash23902005
[10] M J EllingtonMGanner IM Smith C Perry B D Cooksonand A M Kearns ldquoPanton-Valentine Leucocidin-related dis-ease in England andWalesrdquo Clinical Microbiology and Infectionvol 16 no 1 pp 86ndash88 2010
[11] S Breurec C Fall R Pouillot et al ldquoEpidemiology of met-hicillin-susceptible Staphylococcus aureus lineages in five majorAfrican towns high prevalence of Panton-Valentine leukocidingenesrdquoClinicalMicrobiology and Infection vol 17 no 4 pp 633ndash639 2011
[12] F Yu Z Chen C Liu et al ldquoPrevalence of Staphylococcus aureuscarrying Panton-Valentine leukocidin genes among isolatesfrom hospitalised patients in Chinardquo Clinical Microbiology andInfection vol 14 no 4 pp 381ndash384 2008
[13] S Monecke P Slickers M J Ellington A M Kearns andR Ehricht ldquoHigh diversity of Panton-Valentine leukocidin-positive methicillin-susceptible isolates of Staphylococcusaureus and implications for the evolution of community-associatedmethicillin-resistant S aureusrdquoClinical Microbiologyand Infection vol 13 no 12 pp 1157ndash1164 2007
[14] A S Rossney A C Shore P M Morgan M M Fitzgibbon BOConnell and D C Coleman ldquoThe emergence and importa-tion of diverse genotypes ofmethicillin-resistant Staphylococcusaureus (MRSA) harboring the panton-valentine leukocidingene (pvl) reveal that pvl is a poor marker for community-acquired MRSA strains in Irelandrdquo Journal of Clinical Microbi-ology vol 45 no 8 pp 2554ndash2563 2007
[15] J S Kim J S ParkW Song et al ldquoPanton-Valentine leukocidinpositive Staphylococcus aureus isolated from blood in KoreardquoThe Korean Journal of Laboratory Medicine vol 27 no 4 pp286ndash291 2007
[16] L-Y Hsu T-H Koh A Kurup J Low M P Chlebicki andB-H Tan ldquoHigh incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospi-tal in Singaporerdquo Clinical Infectious Diseases vol 40 no 3 pp486ndash489 2005
[17] Z C Karahan A Tekeli R Adaleti E Koyuncu I Dolapciand O A Akan ldquoInvestigation of Panton-Valentine leukocidingenes and SCCmec types in clinical Staphylococcus aureus iso-lates from TurkeyrdquoMicrobial Drug Resistance vol 14 no 3 pp203ndash210 2008
[18] D J Skiest K Brown T W Cooper H Hoffman-Roberts HR Mussa and A C Elliott ldquoProspective comparison of met-hicillin-susceptible and methicillin-resistant community-associated Staphylococcus aureus infections in hospitalizedpatientsrdquo Journal of Infection vol 54 no 5 pp 427ndash434 2007
[19] H C Baggatt T W Hennessy K Rudolph et al ldquoCommunity-onset methicillin-resistant Staphylococcus aureus associated
with antibiotic use and the cytotoxin Panton-Valentine leuko-cidin during a furunculosis outbreak in rural Alaskardquo Journalof Infectious Diseases vol 189 no 9 pp 1565ndash1573 2004
[20] J M Boyce B Cookson K Christiansen et al ldquoMeticillin-resistant Staphylococcus aureusrdquo Lancet Infectious Diseases vol5 no 10 pp 653ndash663 2005
[21] H Grundmann M Aires-de-Sousa J Boyce and E Tiem-ersma ldquoEmergence and resurgence of meticillin-resistantStaphylococcus aureus as a public-health threatrdquoTheLancet vol368 no 9538 pp 874ndash885 2006
[22] F Vandenesch T Naimi M C Enright et al ldquoCommunity-acquired methicillin-resistant Staphylococcus aureus carryingpanton-valentine leukocidin genes worldwide emergencerdquoEmerging Infectious Diseases vol 9 no 8 pp 978ndash984 2003
[23] Clinical Laboratory Standards Institute Performance Standardfor Antimicrobial Susceptibility Testing Seventeenth Informa-tional Supplement M100-S17 Clinical Laboratory StandardsInstitute Wayne Pa USA 2007
[24] B Cauwelier B Gordts P Descheemaecker and H van Lan-duyt ldquoEvaluation of a disk diffusion method with cefoxitin(30 120583g) for detection of methicillin-resistant StaphylococcusaureusrdquoEuropean Journal of ClinicalMicrobiology and InfectiousDiseases vol 23 no 5 pp 389ndash392 2004
[25] I BGosbell J LMercer S ANeville et al ldquoNon-multiresistantand multiresistant methicillin-resistant Staphylococcus aureusin community-acquired infectionsrdquo Medical Journal of Aus-tralia vol 174 no 12 pp 627ndash630 2001
[26] K K Bonnstetter D J Wolter F C Tenover L K McDougaland R V Goering ldquoRapid multiplex PCR assay for identifi-cation of USA300 community-associated methicillin-resistantStaphylococcus aureus isolatesrdquo Journal of Clinical Microbiologyvol 45 no 1 pp 141ndash146 2007
[27] T A Wichelhaus K P Hunfeld B Boddinghaus P Kraiczy VSchafer and V Brade ldquoRapid molecular typing of methicillinresistant Staphylococcus aureus by PCR-RFLPrdquo Infection Controland Hospital Epidemiology vol 22 no 5 pp 294ndash298 2001
[28] B Shrestha ldquoComparative prevalence ofMRSA in twoNepalesetertiary care hospitalsrdquoOpen Journal of Clinical Diagnostics vol3 pp 67ndash73 2013
[29] W J Munckhof G R Nimmo J Carney et al ldquoMethicillin-susceptible non-multiresistant methicillin-resistant and mul-tiresistant methicillin-resistant Staphylococcus aureus infec-tions a clinical epidemiological and microbiological compar-ative studyrdquo European Journal of Clinical Microbiology andInfectious Diseases vol 27 no 5 pp 355ndash364 2008
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
Table 1 PVLprevalence grouped according to infection site age groupmethicillin resistance andmacrolide lincosamide and streptograminB resistance types
PVL-negative isolates () PVL-positive isolates ()
Infection site
Body fluid (119899 = 2) 1 (500) 1 (500)SSI (119899 = 54) 35 (648) 19 (353)Lower RTI (119899 = 9) 7 (778) 2 (222)UTI (119899 = 8) 4 (500) 4 (500)
Age group le30 years (119899 = 27) 17 (630) 10 (370)ge31 years (119899 = 46) 30 (652) 16 (348)
Methicillin resistance
MSSA (27) 13 (481) 14 (519)MRSA (46) 34 (739) 12 (261)
(i) Heterogeneous MRSA (119899 = 15) 4 (267) 11 (733)(ii) Homogeneous MRSA (119899 = 31) 30 (968) 1 (32)
(i) nmMRSA (119899 = 5) 2 (400) 3 (600)(ii) mMRSA (119899 = 41) 32 (780) 9 (220)
Macrolide lincosamide andstreptogramin B resistance
No resistance (119899 = 24) 13 (542) 11 (458)MSB (119899 = 16) 1 (62) 15 (938)MLSB (119899 = 32) 32 (1000) 0 (00)
SSI surgical site infection RTI respiratory tract infection UTI urinary tract infection nmMRSA nonmultiresistant MRSA mMRSA multiresistant MRSAMSB macrolide-streptogramin B resistance MLSB macrolide-lincosamide-streptogramin B resistance
of one year between 2005 and 2006 Ellington et al noted a 2-fold increase in PVL-positive S aureus in England andWales[10] Comparatively countries in western and central Africaboast a higher prevalence rate at 57 raising valid concernsfor the spread of virulent PVL-positive MRSA clones [11]Along similar lines data from across the globe paints a variedpicture for the prevalence of PVL-positive S aureus 128 inChina [12] 30 inGermany [13] 18 in Ireland [14] 09 inKorea [15] 116 in Singapore [16] 4 in Turkey [17] and astriking 97 in the United States [18 19]
Albeit being a relatively recent phenomenon S aureusclones that combine PVL production with methicillin resis-tance are rapidly emerging This global emergence andpropagation of clones combining methicillin resistance andPVL toxin production necessitates commensurate counterac-tion with improved vigilance enhanced case ascertainmentand effective management of PVL-related disease Rightfullyregarded as a ldquosuperbugrdquo methicillin-resistant S aureus(MRSA) by itself is a prominent cause of nosocomial infec-tions and has been exacting a substantial toll on healthcareresources worldwide [20 21] Acquisition of the PVL genesby MRSA therefore represents a challenging conundrum indisease management and infection control
To date PVL has emerged as a significant virulencefactor of community-acquired MRSA (CA-MRSA) [22] withrelatively rare incidence of the toxin in hospital-acquiredMRSA (HA-MRSA) infections We conducted this studyto investigate PVL prevalence among hospital isolates ofS aureus in tertiary care facilities of Nepal To the bestof our knowledge this report on PVL carriage and genedetection is the first of its kind in Nepal In this study weexplore the following the presence of PVL genes in both HA-MSSAandHA-MRSA the association betweenPVLgene and
methicillin susceptibility pattern its linkage with macrolidelincosamide and streptogramin resistance pattern and theepidemiologic molecular typing of PVL-positive S aureus byPCR-RFLP
2 Material and Methods
21 Clinical Isolates A total of 404 consecutive nonrepeatnosocomial S aureus isolates were obtained from Lalitpur-Based Hospital (119899 = 100) and Kathmandu-Based Hospital(119899 = 304) from November 2007 to June 2009 A nosocomialinfection was defined as any infection acquired by a patientafter 48 hours of hospital admission Isolate identificationwasbased on observed fermentation in oxidation-fermentationtest and positivity for catalase clumping factor staphylo-coagulase DNase staphytect plus and mannitol fermen-tation The isolates were categorized into four groups onthe basis of infection sites (Table 1) body fluid surgicalsite infection (SSI) lower respiratory tract infection (RTI)and urinary tract infection (UTI) Antibiotic susceptibilityprofiles were developed using penicillin oxacillin cefoxitinerythromycin clindamycin cotrimoxazole chlorampheni-col ciprofloxacin rifampicin gentamicin and tetracycline(Oxoid Japan) as recommended by Clinical and LaboratoryStandards Institute (CLSI) 2007 [23] However for urinaryisolates erythromycin ciprofloxacin and chloramphenicolwere replaced by novobiocin (to allow for the differentiationbetween S aureus and S saprophyticus) norfloxacin andnitrofurantoin (Oxoid Japan)
MSSA and MRSA were identified based on their respec-tive sensitivity or resistance to both oxacillin and cefox-itin Oxacillin disc diffusion test result was confirmed byminimum inhibitory concentration (MIC) using the E test
BioMed Research International 3
(a)
Coefficient000 066 132 198 265
48
62
72
78
117
193
198
154
161
120
3
41
21
29
147
177
(b)
Figure 1 (a) PCR-RFLP of coa and spa amplified products of PVL-positive MRSA (12 isolates 48ndash198) and PVL-negative MRSA (4 isolates3ndash41) digested by HaeII M = 1 kb DNA ladder PVL-negative MRSA isolates cluster under a single restriction pattern while PVL-positiveMRSA isolates demonstrate clustering under two distinct restriction types type I (48ndash120 154ndash161 and 193ndash198) and type II (147 177) Theisolates were obtained from two tertiary care hospitals (b) Corresponding dendogram of the PCR-RFLP of PVL-positive and PVL-negativeMRSA isolates
and microbroth dilution Methicillin resistance was furtherconfirmed by the amplification of mecA gene by polymerasechain reaction and by the MRSA screen test for the detectionof the protein PBP2a responsible for reduced affinity ofMRSA to 120573-lactam antibiotics (Denka Seiken Japan)
Heterogeneous MRSA was identified on the basis of (i)the presence of colonies inside the oxacillin and cefoxitinzones of inhibition in the disc diffusion test and inside theoxacillin strip inhibition zone in the E test and (ii) oxacillinMIC valueslt100 120583gmL in E test andmicrobroth dilution test[24] Also on the basis of resistance to non-120573-lactam antibi-otics MRSA isolates were grouped as multiresistant (resis-tant to ge3) and nonmultiresistant (resistant to le2) MRSAas described by Gosbell and colleagues in 2001 [25]
And finally macrolide-lincosamide-streptogramin B(MLSB) and macrolide-streptogramin B(MSB) resistancetypes were assessed via D test using erythromycin andclindamycin [23] Isolates resistant to erythromycin andsusceptible to clindamycin were identified as MSB resistancetype isolates resistant to both erythromycin and clindamycinas MLSB resistance type and isolates sensitive to bothantibiotics as no-resistance type MLSB and MSB resistancewere confirmed by the amplification of erm(A) erm(B)erm(C) andmsr(A) as described by Lina et al 1999 [6] MSBresistance was supported by the detection ofmsr(A) gene
22 PVL Genes Identification From our pool of clinical iso-lates 46 MRSA and 27 MSSA (total 73 isolates) were geneti-cally analyzed for PVLpositivity by screening for the presenceof the adjacent cotranscribed luk-PV genes namely lukS-PVand lukF-PV which encode the Panton-Valentine leukocidintoxin These 73 isolates were randomly selected to includehomogenous MRSA heterogeneous MRSA and MSSA Saureus ATCC 29213 and S aureus ATCC 49775 were usedas negative and positive controls respectively The primers(Sigma-Aldrich Germany) used for the coamplification of
PVL genes lukS-PV and lukF-PV were lukPV-1 (51015840-ATC ATTAGG TAAAAT GTC TGGACA TGA TCC A) and luk-PV-2(51015840-GCA TCA ACT GTA TTG GAT AGC AAA AGC) [26]Total DNA was isolated from the clinical isolates and usedas template for PVL gene identification The samples weredenatured at 94∘C for 3 minutes followed by 30 cycles of thefollowing steps denaturation at 94∘C for 30 seconds anneal-ing at 55∘C for 30 seconds extension at 72∘C for 1 minuteand final extension at 72∘C for 5 minutes [6] The imageswere visualized and analyzed in Gel Doc (Bio-Rad USA)by using the Quantity One 1-D Analysis Software
23 PCR-RFLP for Coa and Spa From the study samplesize of 73 clinical isolates all the PVL-positive isolates wereselected for PCR-RFLP including 12 MRSA and 14 MSSAisolates (further described in Section 3) The coa and spagenes of these 26 PVL-positive isolates (12 MRSA and 14MSSA) and additional 9 PVL-negative isolates (4 MRSA and5MSSA) were amplified using the primer pairs coa1 (51015840-CGAGAC CAA GAT TCA ACA AG) and coa2 (51015840-AAA GAAAAC CAC TCA CAT CAG T) and spa1 (51015840-ATC TGG TGGCGTAACACCTG) and spa2 (51015840-CGCTGCACCTAACGCTAA TG) (Sigma Aldrich Germany [27])
PCR-RFLP was carried out using HaeII digestion of theamplified products Unique PCR-RFLP patterns obtainedfollowing the electrophoresis of the HaeII digested PCRproducts were each designated as an independent restrictionpattern (Figures 1 and 2)
24 Susceptibility Patterns of the PVL-Positive and PVL-Negative MRSA and MSSA MIC of 12 different antibioticswas determined for 26 PVL-positive (12MRSA and 14MSSA)and 9 PVL-negative isolates (4 MRSA and 5 MSSA) bymicrobroth dilution [23] The antibiotics included fusidicacid tetracycline Augmentin clindamycin levofloxacinerythromycin trimethoprim-sulfamethoxazole gentamicin
4 BioMed Research International
(a)
Coefficient000 059 118 177 237
H30
194
14
31
185
54
16
47
190
32
109
118
46
149
189
(b)
Figure 2 (a) PCR-RFLP of coa and spa amplified products of PVL-positive MSSA (14 isolates 14ndash194) and PVL-negative MSSA (3 isolates79ndash113) digested by HaeIIM = 1 kb DNA ladder PVL-positive MSSA isolates 16 and 47 cluster under one restriction type and isolates 14 31and 185 cluster under another The remaining nine PVL-positive MSSA isolates and all three PVL-negative MSSA isolates exist as singletons(b) Corresponding dendogram of the PCR-RFLP of PVL-positive and PVL-negative MSSA isolates
vancomycin linezolid kanamycin and rifampicin (Sigma-Aldrich Germany) The clinical isolates were suspendedin physiological saline (05 McFarland) using Densimat(Biomerieux Italy) followingwhich 100120583L of each suspendedisolate was dispensed into microtiter wells containing dou-bling dilutions of the 12 antibiotics in cation-adjustedMuellerHinton Broth (Becton Dickinson and Company USA) Themicrotiter plates were incubated at 37∘C for 18 hrs and wereread in reflected light
Data was analyzed using the statistical software SPSS 115
3 Results
The source sample of 404 hospital-acquired isolates consistedof 197 (488) MRSA isolates of which 148 (751) werehomogenous and 49 (249) were heterogeneous [28] Asmentioned earlier from the total sample of 404 clinicalisolates 73 isolates were randomly selected for further anal-ysis owing to resource limitations Of these 73 isolates thatcomprised of 46 MRSA and 27 MSSA isolates PVL genewas detected in 12 MRSA (261) and 14 MSSA (519) for acumulative prevalence rate of 356 As indicated in Table 1the PVL carriage was high in samples from UTI (50 48)SSI (352 1954) and lower RTI (222 29) Howevercross tab calculation between UTI and SSI (1198832 = 0655119875 = 0418) and SSI and lower RTI (1198831198912 = 0583 119875 = 0445)showed that the difference in PVL prevalence in these sitesdid not reach statistical significance
For our analysis the patient population was grouped into2 age groups le30 years (119899 = 27) and ge31 years (119899 = 46) ThePVL-positivity rates were 37 for le30 age group and 348for ge31 age group (Table 1) these values were not found to bestatistically significantly different (1198832 = 0038 119875 = 0846)We also did not find any association between PVL positivityand hospital of origin (Table 2) The PVL prevalence of 321at KBH and of 450 at LBH did not meet the statisticalcriteria for significant difference (1198832 = 1058 119875 = 0304)
Upon conducting a pooled evaluation of isolates fromboth hospitals PVL prevalence rates were found to be 733in heterogeneous MRSA 519 inMSSA and 32 in homo-geneous MRSA (Table 1) PVL occurrence was observed tobe significantly associated with a heterogeneous methicillinresistance pattern compared to homogeneous MRSA andMSSA (1198832 = 2659 119875 lt 0001) However a pooled sample ofboth homogeneous and heterogeneous MRSA failed to showany correlation with PVL carriage when compared to MSSA(1198832 = 4925 119875 = 0026)
As mentioned previously MRSA that was resistant toge3 non-120573-lactam antibiotics was categorized as multire-sistant MRSA (mMRSA) and that resistant to le2 non-120573-lactam antibiotics was identified as nonmultiresistant MRSA(nmMRSA) The distribution of PVL carriage rates was519 amongMSSA 60 among nmMRSA and 22 amongmMRSA (Table 1) Compared to MSSA and nmMRSAmMRSA had lesser prevalence of PVL positivity (1198832 = 7739119875 = 0021)
In assessing the putative relation between PVL prevalenceand macrolide lincosamide and streptogramin resistancetypes we found that none of the isolates withMLSB resistance(119899 = 32) was positive for PVL Among MSB resistancetypes PVL positivity was at 938 and among nonresistantisolates depicting susceptibility to both erythromycin andclindamycin PVL carriage was at 458 (Table 1) We foundthat MSB resistance types were significantly associated withPVL gene carriage when compared toMLSB resistance (119883
2=
4211 119875 lt 0001) and no-resistance types (1198832 = 9689 119875 =0002) Isolates susceptible to erythromycin and clindamycin(no-resistance type) had 177 greater odds of being PVL neg-ative as compared to MSB resistance types (OR = 17727 95CI 20 to 1565)
The MSB resistance type was genotypically confirmed bythe presence ofmsr(A) geneThe isolates harboring this genedepicted a strong associationwithPVLgene possession (1198832 =12049119875 = 0001) Compared to isolates carrying themsr(A)
BioMed Research International 5
Table 2 Hospital-specific PVL prevalence rates and methicillin resistance in S aureus
Strains (119899) Lalitpur Hospital Kathmandu Hospital TotalPVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos
MSSA (27) 4 3 571 10 10 500 519 (1427)Homo-MRSA (31) 0 7 385a 1 23 212b 261 (1246)Hetero-MRSA (15) 5 1 6 3Total (73) 9 11 450 17 36 321 356 (2673)aTotal PVL-positive prevalence rate in Lalitpur HospitalbTotal PVL-positive prevalence rate in Kathmandu HospitalHetero heterogeneous Homo homogeneous Pos positive Neg negative
gene no-resistance type isolates lacking this gene were 455times more likely to be not positive for PVL (OR = 455 95CI 35 to 5947)
The MIC of the 26 PVL-positive and 7 PVL-negativeisolates was determined by microbroth dilution method Nosubstantial difference could be noted in the resistance patternbetween PVL-positive and PVL-negative S aureus strains(both MRSA and MSSA) with the exception of tetracyclineand clindamycin to which PVL-positive and PVL-negativeisolates responded differently It was observed that whilePVL-positive MRSA was sensitive to both clindamycin andtetracycline PVL-negative MRSA was uniformly resistantto these antibiotics Further both PVL-positive and PVL-negativeMSSA isolateswere also sensitive to clindamycin andtetracycline
With regard to restriction types identified by PCR-RFLPPVL-positive MRSA PVL-negative MRSA PVL-positiveMSSA and PVL-negative MSSA isolates depicted two oneeleven and three restriction types respectively (Figures 1 and2) The majority of the PVL-positive MRSA isolates wereclustered under one restriction type (1012 DNA fragmentslength 400 bp and 750 bp) with the remaining two isolatesbeing grouped under the second restriction type (212 DNAfragments length 500 bp and 800 bp) All four isolates of PVL-negative MRSA belonged to a single restriction type ForPVL-positive MSSA two and three isolates were includedunder two distinct restriction types while the remainingnine isolates and all three of the PVL-negative MSSA isolatesexisted as singletons within their unique restriction types(Figure 2)
4 Discussion
In the present day context when microbial antibiotic resis-tance is progressively morphing into an intractable predica-ment acquisition of the potent PVL gene by MRSA whichrepresents a rather difficult challenge in itself would pavethe way to an alarming healthcare paradox In this paper wepresent the findings from the first PVL prevalence study inNepal which includes (i) heretofore unidentified associationsbetween PVL positivity and MSB resistance verified bymsr(A) gene (ii) PVL carriage rates specific to MRSA andMSSA isolates obtained from two premiere tertiary carehospitals (iii) evaluation of putative predilection of PVL-positive S aureus to a select patient profile (iv) compar-ative assessment of PVL prevalence among heterogeneous
MRSA-homogeneous MRSA-MSSA and among mMRSA-nmMRSA-MSSA and (v) restriction pattern characterizationof PVL-positive and PVL-negative hospital isolates
In the current study we report PVL gene carriage rateof 356 among nosocomial S aureus isolates 261 amongMRSA and 519 among MSSA (Table 1) These numberstrack along some of the highest reported PVL-positive Saureus prevalence rates and should rightfully be regarded as amatter of grave concern Further restriction pattern analysesof PVL-positive MRSA and MSSA have revealed that whilePVL-positive MSSA can be grouped into eleven restrictiontypes with a majority of the isolates existing as singletons(Figure 2) PVL-positiveMRSA seamlessly clusters under tworestriction types (Figure 1)This is an anticipated finding sinceMRSA isolates belong to a single clone while MSSA isolatespropagated from multiple clones Such spread of a limitednumber of PVL-carrying MRSA clones suggests that com-pared to their MSSA counterparts these microbes are well-adapted to thrive in the hospital environmentThe restrictiontype limitationwould also follow from the fact that theMRSAisolates are hospital strains that cause infection in any sus-ceptible host with the right combination of risk factors Alsothe restriction pattern clusters included isolates from bothLBH and KBH suggesting an interhospital transmission ofpathogenic strains These findings in conjunction with thehigh PVL-positive S aureus prevalence rates warrant theimmediate institution of effective infection control measures
In addition to clone limitation lack of any trend ofhigher PVL prevalence among a younger age group is anotherfinding explained by the hospital-acquired nature of the PVL-positive S aureus strains in the study At prevalence rates of37 for le30 years age group and 348 for ge31 years agegroup (Table 1) the PVL-positive isolates fail to show any age-related predilection Previous studies have shown a strongpredisposition of PVL-positive S aureus isolates for youngerand previously healthy patients [14 29] In a 2008 Australianstudy by Munckhof et al the authors observed a steadydecline in PVL occurrence with increasing age which theyascribed to age-associated strengthening of immunity and tothe natural penchant of children and young adults to acquirePVL-positive S aureus from skin contamination duringplayful and contact sports [29] This increased likelihood ofPVL-positive S aureus to infect younger age groups as seenin earlier studies may be attributed to the fact that a majorityof PVL-carrying S aureus isolates from these studies werecommunity-acquired In contrast our study exclusively
6 BioMed Research International
investigated nosocomial isolates which regardless of age caninfect any patient presenting with the right risk factors foracquiring an infection originating in the hospital
As with age PVL prevalence also exhibited no associationwith infection site or hospital of origin Although the highestnumbers of PVL-carrying S aureus isolates were recoveredfrom UTI (50) followed by SSI (352) and lower RTI(222) the prevalence rate difference between the sites didnot reach statistical significance (Table 1) Along similar linesthe 45 carriage rate of PVL gene in LBHwas not statisticallysignificantly different from the 321 prevalence rate at KBH(Table 2) On the basis of vastly different occurrence of thePVL-positive organisms in different parts of the world itappears that the PVL carriage depends largely on the geo-graphical location and the organisms that are endemic in aparticular locality
Overall PVL carriage rates were 519 (1427) amongMSSA 733 (1115) among heterogeneous MRSA and 32(131) among homogeneous MRSA (Table 1) Comparedto MSSA and homogeneous MRSA heterogeneous MRSAdepicted a positive association with PVL carriage Howeverwhen heterogeneous and homogeneous MRSA were pooledtogether into a single cohort of MRSA isolates and comparedto MSSA MRSA was found to have a negative associationwith PVL prevalence The negative correlation between PVLand MRSA as a whole can be attributed to the 30 (968)PVL-negative homogeneousMRSA isolates which would off-set the PVL positivity of the 11 (733) heterogeneous MRSAisolates These findings suggest that in the observed hospitalsettings PVL positivity was associated with heterogeneousMRSA but not with homogeneous MRSA Consequentlycrude analyses ofMSSAversus pooledMRSA strains could bepotentially misleading a thorough evaluation of PVL emer-gence should constitute a breakdown of MRSA into homo-geneous and heterogeneous strains
A phenotypic analysis of the clinical isolates based ontheir antibiotic profiles allowed for a grouping of the isolatesinto 3 categories each of which revealed a relatively highPVL prevalence 60 nmMRSA 22 mMRSA and 519MSSA (Table 1) Munckhof and colleagues (2008) [29] reporta similar rate of PVLpositivity among their nmMRSA isolates(55) However their PVL prevalence rates of 2 amongmMRSA and 16 among MSSA are much lower comparedto this study
Classifying the clinical isolates cohort on the basis ofmacrolide lincosamide and streptogramin resistance typesit was found that while PVL positivity was 938 forMSB and458 for no-resistance types none of the isolates withMLSBresistance harbored the PVL gene (Table 1) This finding thatisolates characterized as MSB resistance type are more likelyto depict PVL positivity compared to either MLSB resistanceor no-resistance type was verified by testing for the presenceof msr(A) gene which showed a positive association withPVL
While it would have been ideal to carry out these molec-ular epidemiological analyses on the entire cohort of 404 iso-lates the study needed to limit its sample size to 73 randomlyselected isolates due to resource and monetary restric-tions Todayrsquos context of PVL diagnosis and epidemiology
is constrained by the lack of a reliable phenotypic testfor PVL positivity Studies that focus on developing suchnovelmethodologies for phenotypic characterization of PVL-positive bacterium which would complement the currentlyavailable genetic test will have substantial utility in promot-ing the early detection of these virulent microbes
5 Conclusion
Our study has shown a relatively high prevalence rate of PVLpositivity in HA-S aureus isolates from two tertiary care hos-pitals of Nepal PVL carriage was associated with heteroge-neous MRSA and MSB resistance type (confirmed bymsr(A)gene positivity) Compared toMSSAandnmMRSAmMRSAwas significantly less likely to harbor the PVL genes Noassociationwith age site of infection or hospital of originwasobserved Such an absence of predilection for a younger agegroup and the observed restriction pattern limitation of PVL-positive MRSA are in alignment with the fact that these wereclinical isolates obtained from hospital-acquired infectionsThe relatively high rates of PVL presence among HA-MRSAandHA-MSSA isolates and the interhospital spread of strainssupport the need for system-wide implementation of patientsafety and infection control initiatives
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] J Kaneko and Y Kamio ldquoBacterial two-component and hetero-heptameric pore-forming cytolytic toxins structures pore-formingmechanism and organization of the genesrdquo BioscienceBiotechnology and Biochemistry vol 68 no 5 pp 981ndash10032004
[2] G Prevost B Cribier P Couppie et al ldquoPanton-valentineleucocidin and gamma-hemolysin from Staphylococcus aureusATCC 49775 are encoded by distinct genetic loci and have dif-ferent biological activitiesrdquo Infection and Immunity vol 63 no10 pp 4121ndash4129 1995
[3] L GMiller F Perdreau-Remington G Rieg et al ldquoNecrotizingfasciitis caused by community-associated methicillin-resistantStaphylococcus aureus in Los AngelesrdquoTheNewEngland Journalof Medicine vol 352 no 14 pp 1445ndash1453 2005
[4] G R Kravitz D J Dries M L Peterson and P M SchlievertldquoPurpura fulminans due to Staphylococcus aureusrdquo ClinicalInfectious Diseases vol 40 no 7 pp 941ndash947 2005
[5] B McGrath F Rutledge and E Broadfield ldquoNecrotisingpneumonia Staphylococcus aureus andPanton-Valentine leuko-cidinrdquo The Journal of the Intensive Care Society vol 9 pp 170ndash172 2008
[6] G Lina Y Piemont F Godail-Gamot et al ldquoInvolvement ofPanton-Valentine leukocidin-producing Staphylococcus aureusin primary skin infections and pneumoniardquo Clinical InfectiousDiseases vol 29 no 5 pp 1128ndash1132 1999
[7] Y Gillet B Issartel P Vanhems et al ldquoAssociation betweenStaphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia
BioMed Research International 7
in young immunocompetent patientsrdquoThe Lancet vol 359 no9308 pp 753ndash759 2002
[8] L J Shallcross K Williams S Hopkins R W Aldridge AM Johnson and A C Hayward ldquoPanton-Valentine leukocidinassociated staphylococcal disease a cross-sectional study at aLondon hospital Englandrdquo Clinical Microbiology and Infectionvol 16 no 11 pp 1644ndash1648 2010
[9] A Holmes M Ganner S McGuane T L Pitt B D Cooksonand A M Kearns ldquoStaphylococcus aureus isolates carryingpanton-valentine leucocidin genes in England and Wales fre-quency characterization and association with clinical diseaserdquoJournal of Clinical Microbiology vol 43 no 5 pp 2384ndash23902005
[10] M J EllingtonMGanner IM Smith C Perry B D Cooksonand A M Kearns ldquoPanton-Valentine Leucocidin-related dis-ease in England andWalesrdquo Clinical Microbiology and Infectionvol 16 no 1 pp 86ndash88 2010
[11] S Breurec C Fall R Pouillot et al ldquoEpidemiology of met-hicillin-susceptible Staphylococcus aureus lineages in five majorAfrican towns high prevalence of Panton-Valentine leukocidingenesrdquoClinicalMicrobiology and Infection vol 17 no 4 pp 633ndash639 2011
[12] F Yu Z Chen C Liu et al ldquoPrevalence of Staphylococcus aureuscarrying Panton-Valentine leukocidin genes among isolatesfrom hospitalised patients in Chinardquo Clinical Microbiology andInfection vol 14 no 4 pp 381ndash384 2008
[13] S Monecke P Slickers M J Ellington A M Kearns andR Ehricht ldquoHigh diversity of Panton-Valentine leukocidin-positive methicillin-susceptible isolates of Staphylococcusaureus and implications for the evolution of community-associatedmethicillin-resistant S aureusrdquoClinical Microbiologyand Infection vol 13 no 12 pp 1157ndash1164 2007
[14] A S Rossney A C Shore P M Morgan M M Fitzgibbon BOConnell and D C Coleman ldquoThe emergence and importa-tion of diverse genotypes ofmethicillin-resistant Staphylococcusaureus (MRSA) harboring the panton-valentine leukocidingene (pvl) reveal that pvl is a poor marker for community-acquired MRSA strains in Irelandrdquo Journal of Clinical Microbi-ology vol 45 no 8 pp 2554ndash2563 2007
[15] J S Kim J S ParkW Song et al ldquoPanton-Valentine leukocidinpositive Staphylococcus aureus isolated from blood in KoreardquoThe Korean Journal of Laboratory Medicine vol 27 no 4 pp286ndash291 2007
[16] L-Y Hsu T-H Koh A Kurup J Low M P Chlebicki andB-H Tan ldquoHigh incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospi-tal in Singaporerdquo Clinical Infectious Diseases vol 40 no 3 pp486ndash489 2005
[17] Z C Karahan A Tekeli R Adaleti E Koyuncu I Dolapciand O A Akan ldquoInvestigation of Panton-Valentine leukocidingenes and SCCmec types in clinical Staphylococcus aureus iso-lates from TurkeyrdquoMicrobial Drug Resistance vol 14 no 3 pp203ndash210 2008
[18] D J Skiest K Brown T W Cooper H Hoffman-Roberts HR Mussa and A C Elliott ldquoProspective comparison of met-hicillin-susceptible and methicillin-resistant community-associated Staphylococcus aureus infections in hospitalizedpatientsrdquo Journal of Infection vol 54 no 5 pp 427ndash434 2007
[19] H C Baggatt T W Hennessy K Rudolph et al ldquoCommunity-onset methicillin-resistant Staphylococcus aureus associated
with antibiotic use and the cytotoxin Panton-Valentine leuko-cidin during a furunculosis outbreak in rural Alaskardquo Journalof Infectious Diseases vol 189 no 9 pp 1565ndash1573 2004
[20] J M Boyce B Cookson K Christiansen et al ldquoMeticillin-resistant Staphylococcus aureusrdquo Lancet Infectious Diseases vol5 no 10 pp 653ndash663 2005
[21] H Grundmann M Aires-de-Sousa J Boyce and E Tiem-ersma ldquoEmergence and resurgence of meticillin-resistantStaphylococcus aureus as a public-health threatrdquoTheLancet vol368 no 9538 pp 874ndash885 2006
[22] F Vandenesch T Naimi M C Enright et al ldquoCommunity-acquired methicillin-resistant Staphylococcus aureus carryingpanton-valentine leukocidin genes worldwide emergencerdquoEmerging Infectious Diseases vol 9 no 8 pp 978ndash984 2003
[23] Clinical Laboratory Standards Institute Performance Standardfor Antimicrobial Susceptibility Testing Seventeenth Informa-tional Supplement M100-S17 Clinical Laboratory StandardsInstitute Wayne Pa USA 2007
[24] B Cauwelier B Gordts P Descheemaecker and H van Lan-duyt ldquoEvaluation of a disk diffusion method with cefoxitin(30 120583g) for detection of methicillin-resistant StaphylococcusaureusrdquoEuropean Journal of ClinicalMicrobiology and InfectiousDiseases vol 23 no 5 pp 389ndash392 2004
[25] I BGosbell J LMercer S ANeville et al ldquoNon-multiresistantand multiresistant methicillin-resistant Staphylococcus aureusin community-acquired infectionsrdquo Medical Journal of Aus-tralia vol 174 no 12 pp 627ndash630 2001
[26] K K Bonnstetter D J Wolter F C Tenover L K McDougaland R V Goering ldquoRapid multiplex PCR assay for identifi-cation of USA300 community-associated methicillin-resistantStaphylococcus aureus isolatesrdquo Journal of Clinical Microbiologyvol 45 no 1 pp 141ndash146 2007
[27] T A Wichelhaus K P Hunfeld B Boddinghaus P Kraiczy VSchafer and V Brade ldquoRapid molecular typing of methicillinresistant Staphylococcus aureus by PCR-RFLPrdquo Infection Controland Hospital Epidemiology vol 22 no 5 pp 294ndash298 2001
[28] B Shrestha ldquoComparative prevalence ofMRSA in twoNepalesetertiary care hospitalsrdquoOpen Journal of Clinical Diagnostics vol3 pp 67ndash73 2013
[29] W J Munckhof G R Nimmo J Carney et al ldquoMethicillin-susceptible non-multiresistant methicillin-resistant and mul-tiresistant methicillin-resistant Staphylococcus aureus infec-tions a clinical epidemiological and microbiological compar-ative studyrdquo European Journal of Clinical Microbiology andInfectious Diseases vol 27 no 5 pp 355ndash364 2008
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
(a)
Coefficient000 066 132 198 265
48
62
72
78
117
193
198
154
161
120
3
41
21
29
147
177
(b)
Figure 1 (a) PCR-RFLP of coa and spa amplified products of PVL-positive MRSA (12 isolates 48ndash198) and PVL-negative MRSA (4 isolates3ndash41) digested by HaeII M = 1 kb DNA ladder PVL-negative MRSA isolates cluster under a single restriction pattern while PVL-positiveMRSA isolates demonstrate clustering under two distinct restriction types type I (48ndash120 154ndash161 and 193ndash198) and type II (147 177) Theisolates were obtained from two tertiary care hospitals (b) Corresponding dendogram of the PCR-RFLP of PVL-positive and PVL-negativeMRSA isolates
and microbroth dilution Methicillin resistance was furtherconfirmed by the amplification of mecA gene by polymerasechain reaction and by the MRSA screen test for the detectionof the protein PBP2a responsible for reduced affinity ofMRSA to 120573-lactam antibiotics (Denka Seiken Japan)
Heterogeneous MRSA was identified on the basis of (i)the presence of colonies inside the oxacillin and cefoxitinzones of inhibition in the disc diffusion test and inside theoxacillin strip inhibition zone in the E test and (ii) oxacillinMIC valueslt100 120583gmL in E test andmicrobroth dilution test[24] Also on the basis of resistance to non-120573-lactam antibi-otics MRSA isolates were grouped as multiresistant (resis-tant to ge3) and nonmultiresistant (resistant to le2) MRSAas described by Gosbell and colleagues in 2001 [25]
And finally macrolide-lincosamide-streptogramin B(MLSB) and macrolide-streptogramin B(MSB) resistancetypes were assessed via D test using erythromycin andclindamycin [23] Isolates resistant to erythromycin andsusceptible to clindamycin were identified as MSB resistancetype isolates resistant to both erythromycin and clindamycinas MLSB resistance type and isolates sensitive to bothantibiotics as no-resistance type MLSB and MSB resistancewere confirmed by the amplification of erm(A) erm(B)erm(C) andmsr(A) as described by Lina et al 1999 [6] MSBresistance was supported by the detection ofmsr(A) gene
22 PVL Genes Identification From our pool of clinical iso-lates 46 MRSA and 27 MSSA (total 73 isolates) were geneti-cally analyzed for PVLpositivity by screening for the presenceof the adjacent cotranscribed luk-PV genes namely lukS-PVand lukF-PV which encode the Panton-Valentine leukocidintoxin These 73 isolates were randomly selected to includehomogenous MRSA heterogeneous MRSA and MSSA Saureus ATCC 29213 and S aureus ATCC 49775 were usedas negative and positive controls respectively The primers(Sigma-Aldrich Germany) used for the coamplification of
PVL genes lukS-PV and lukF-PV were lukPV-1 (51015840-ATC ATTAGG TAAAAT GTC TGGACA TGA TCC A) and luk-PV-2(51015840-GCA TCA ACT GTA TTG GAT AGC AAA AGC) [26]Total DNA was isolated from the clinical isolates and usedas template for PVL gene identification The samples weredenatured at 94∘C for 3 minutes followed by 30 cycles of thefollowing steps denaturation at 94∘C for 30 seconds anneal-ing at 55∘C for 30 seconds extension at 72∘C for 1 minuteand final extension at 72∘C for 5 minutes [6] The imageswere visualized and analyzed in Gel Doc (Bio-Rad USA)by using the Quantity One 1-D Analysis Software
23 PCR-RFLP for Coa and Spa From the study samplesize of 73 clinical isolates all the PVL-positive isolates wereselected for PCR-RFLP including 12 MRSA and 14 MSSAisolates (further described in Section 3) The coa and spagenes of these 26 PVL-positive isolates (12 MRSA and 14MSSA) and additional 9 PVL-negative isolates (4 MRSA and5MSSA) were amplified using the primer pairs coa1 (51015840-CGAGAC CAA GAT TCA ACA AG) and coa2 (51015840-AAA GAAAAC CAC TCA CAT CAG T) and spa1 (51015840-ATC TGG TGGCGTAACACCTG) and spa2 (51015840-CGCTGCACCTAACGCTAA TG) (Sigma Aldrich Germany [27])
PCR-RFLP was carried out using HaeII digestion of theamplified products Unique PCR-RFLP patterns obtainedfollowing the electrophoresis of the HaeII digested PCRproducts were each designated as an independent restrictionpattern (Figures 1 and 2)
24 Susceptibility Patterns of the PVL-Positive and PVL-Negative MRSA and MSSA MIC of 12 different antibioticswas determined for 26 PVL-positive (12MRSA and 14MSSA)and 9 PVL-negative isolates (4 MRSA and 5 MSSA) bymicrobroth dilution [23] The antibiotics included fusidicacid tetracycline Augmentin clindamycin levofloxacinerythromycin trimethoprim-sulfamethoxazole gentamicin
4 BioMed Research International
(a)
Coefficient000 059 118 177 237
H30
194
14
31
185
54
16
47
190
32
109
118
46
149
189
(b)
Figure 2 (a) PCR-RFLP of coa and spa amplified products of PVL-positive MSSA (14 isolates 14ndash194) and PVL-negative MSSA (3 isolates79ndash113) digested by HaeIIM = 1 kb DNA ladder PVL-positive MSSA isolates 16 and 47 cluster under one restriction type and isolates 14 31and 185 cluster under another The remaining nine PVL-positive MSSA isolates and all three PVL-negative MSSA isolates exist as singletons(b) Corresponding dendogram of the PCR-RFLP of PVL-positive and PVL-negative MSSA isolates
vancomycin linezolid kanamycin and rifampicin (Sigma-Aldrich Germany) The clinical isolates were suspendedin physiological saline (05 McFarland) using Densimat(Biomerieux Italy) followingwhich 100120583L of each suspendedisolate was dispensed into microtiter wells containing dou-bling dilutions of the 12 antibiotics in cation-adjustedMuellerHinton Broth (Becton Dickinson and Company USA) Themicrotiter plates were incubated at 37∘C for 18 hrs and wereread in reflected light
Data was analyzed using the statistical software SPSS 115
3 Results
The source sample of 404 hospital-acquired isolates consistedof 197 (488) MRSA isolates of which 148 (751) werehomogenous and 49 (249) were heterogeneous [28] Asmentioned earlier from the total sample of 404 clinicalisolates 73 isolates were randomly selected for further anal-ysis owing to resource limitations Of these 73 isolates thatcomprised of 46 MRSA and 27 MSSA isolates PVL genewas detected in 12 MRSA (261) and 14 MSSA (519) for acumulative prevalence rate of 356 As indicated in Table 1the PVL carriage was high in samples from UTI (50 48)SSI (352 1954) and lower RTI (222 29) Howevercross tab calculation between UTI and SSI (1198832 = 0655119875 = 0418) and SSI and lower RTI (1198831198912 = 0583 119875 = 0445)showed that the difference in PVL prevalence in these sitesdid not reach statistical significance
For our analysis the patient population was grouped into2 age groups le30 years (119899 = 27) and ge31 years (119899 = 46) ThePVL-positivity rates were 37 for le30 age group and 348for ge31 age group (Table 1) these values were not found to bestatistically significantly different (1198832 = 0038 119875 = 0846)We also did not find any association between PVL positivityand hospital of origin (Table 2) The PVL prevalence of 321at KBH and of 450 at LBH did not meet the statisticalcriteria for significant difference (1198832 = 1058 119875 = 0304)
Upon conducting a pooled evaluation of isolates fromboth hospitals PVL prevalence rates were found to be 733in heterogeneous MRSA 519 inMSSA and 32 in homo-geneous MRSA (Table 1) PVL occurrence was observed tobe significantly associated with a heterogeneous methicillinresistance pattern compared to homogeneous MRSA andMSSA (1198832 = 2659 119875 lt 0001) However a pooled sample ofboth homogeneous and heterogeneous MRSA failed to showany correlation with PVL carriage when compared to MSSA(1198832 = 4925 119875 = 0026)
As mentioned previously MRSA that was resistant toge3 non-120573-lactam antibiotics was categorized as multire-sistant MRSA (mMRSA) and that resistant to le2 non-120573-lactam antibiotics was identified as nonmultiresistant MRSA(nmMRSA) The distribution of PVL carriage rates was519 amongMSSA 60 among nmMRSA and 22 amongmMRSA (Table 1) Compared to MSSA and nmMRSAmMRSA had lesser prevalence of PVL positivity (1198832 = 7739119875 = 0021)
In assessing the putative relation between PVL prevalenceand macrolide lincosamide and streptogramin resistancetypes we found that none of the isolates withMLSB resistance(119899 = 32) was positive for PVL Among MSB resistancetypes PVL positivity was at 938 and among nonresistantisolates depicting susceptibility to both erythromycin andclindamycin PVL carriage was at 458 (Table 1) We foundthat MSB resistance types were significantly associated withPVL gene carriage when compared toMLSB resistance (119883
2=
4211 119875 lt 0001) and no-resistance types (1198832 = 9689 119875 =0002) Isolates susceptible to erythromycin and clindamycin(no-resistance type) had 177 greater odds of being PVL neg-ative as compared to MSB resistance types (OR = 17727 95CI 20 to 1565)
The MSB resistance type was genotypically confirmed bythe presence ofmsr(A) geneThe isolates harboring this genedepicted a strong associationwithPVLgene possession (1198832 =12049119875 = 0001) Compared to isolates carrying themsr(A)
BioMed Research International 5
Table 2 Hospital-specific PVL prevalence rates and methicillin resistance in S aureus
Strains (119899) Lalitpur Hospital Kathmandu Hospital TotalPVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos
MSSA (27) 4 3 571 10 10 500 519 (1427)Homo-MRSA (31) 0 7 385a 1 23 212b 261 (1246)Hetero-MRSA (15) 5 1 6 3Total (73) 9 11 450 17 36 321 356 (2673)aTotal PVL-positive prevalence rate in Lalitpur HospitalbTotal PVL-positive prevalence rate in Kathmandu HospitalHetero heterogeneous Homo homogeneous Pos positive Neg negative
gene no-resistance type isolates lacking this gene were 455times more likely to be not positive for PVL (OR = 455 95CI 35 to 5947)
The MIC of the 26 PVL-positive and 7 PVL-negativeisolates was determined by microbroth dilution method Nosubstantial difference could be noted in the resistance patternbetween PVL-positive and PVL-negative S aureus strains(both MRSA and MSSA) with the exception of tetracyclineand clindamycin to which PVL-positive and PVL-negativeisolates responded differently It was observed that whilePVL-positive MRSA was sensitive to both clindamycin andtetracycline PVL-negative MRSA was uniformly resistantto these antibiotics Further both PVL-positive and PVL-negativeMSSA isolateswere also sensitive to clindamycin andtetracycline
With regard to restriction types identified by PCR-RFLPPVL-positive MRSA PVL-negative MRSA PVL-positiveMSSA and PVL-negative MSSA isolates depicted two oneeleven and three restriction types respectively (Figures 1 and2) The majority of the PVL-positive MRSA isolates wereclustered under one restriction type (1012 DNA fragmentslength 400 bp and 750 bp) with the remaining two isolatesbeing grouped under the second restriction type (212 DNAfragments length 500 bp and 800 bp) All four isolates of PVL-negative MRSA belonged to a single restriction type ForPVL-positive MSSA two and three isolates were includedunder two distinct restriction types while the remainingnine isolates and all three of the PVL-negative MSSA isolatesexisted as singletons within their unique restriction types(Figure 2)
4 Discussion
In the present day context when microbial antibiotic resis-tance is progressively morphing into an intractable predica-ment acquisition of the potent PVL gene by MRSA whichrepresents a rather difficult challenge in itself would pavethe way to an alarming healthcare paradox In this paper wepresent the findings from the first PVL prevalence study inNepal which includes (i) heretofore unidentified associationsbetween PVL positivity and MSB resistance verified bymsr(A) gene (ii) PVL carriage rates specific to MRSA andMSSA isolates obtained from two premiere tertiary carehospitals (iii) evaluation of putative predilection of PVL-positive S aureus to a select patient profile (iv) compar-ative assessment of PVL prevalence among heterogeneous
MRSA-homogeneous MRSA-MSSA and among mMRSA-nmMRSA-MSSA and (v) restriction pattern characterizationof PVL-positive and PVL-negative hospital isolates
In the current study we report PVL gene carriage rateof 356 among nosocomial S aureus isolates 261 amongMRSA and 519 among MSSA (Table 1) These numberstrack along some of the highest reported PVL-positive Saureus prevalence rates and should rightfully be regarded as amatter of grave concern Further restriction pattern analysesof PVL-positive MRSA and MSSA have revealed that whilePVL-positive MSSA can be grouped into eleven restrictiontypes with a majority of the isolates existing as singletons(Figure 2) PVL-positiveMRSA seamlessly clusters under tworestriction types (Figure 1)This is an anticipated finding sinceMRSA isolates belong to a single clone while MSSA isolatespropagated from multiple clones Such spread of a limitednumber of PVL-carrying MRSA clones suggests that com-pared to their MSSA counterparts these microbes are well-adapted to thrive in the hospital environmentThe restrictiontype limitationwould also follow from the fact that theMRSAisolates are hospital strains that cause infection in any sus-ceptible host with the right combination of risk factors Alsothe restriction pattern clusters included isolates from bothLBH and KBH suggesting an interhospital transmission ofpathogenic strains These findings in conjunction with thehigh PVL-positive S aureus prevalence rates warrant theimmediate institution of effective infection control measures
In addition to clone limitation lack of any trend ofhigher PVL prevalence among a younger age group is anotherfinding explained by the hospital-acquired nature of the PVL-positive S aureus strains in the study At prevalence rates of37 for le30 years age group and 348 for ge31 years agegroup (Table 1) the PVL-positive isolates fail to show any age-related predilection Previous studies have shown a strongpredisposition of PVL-positive S aureus isolates for youngerand previously healthy patients [14 29] In a 2008 Australianstudy by Munckhof et al the authors observed a steadydecline in PVL occurrence with increasing age which theyascribed to age-associated strengthening of immunity and tothe natural penchant of children and young adults to acquirePVL-positive S aureus from skin contamination duringplayful and contact sports [29] This increased likelihood ofPVL-positive S aureus to infect younger age groups as seenin earlier studies may be attributed to the fact that a majorityof PVL-carrying S aureus isolates from these studies werecommunity-acquired In contrast our study exclusively
6 BioMed Research International
investigated nosocomial isolates which regardless of age caninfect any patient presenting with the right risk factors foracquiring an infection originating in the hospital
As with age PVL prevalence also exhibited no associationwith infection site or hospital of origin Although the highestnumbers of PVL-carrying S aureus isolates were recoveredfrom UTI (50) followed by SSI (352) and lower RTI(222) the prevalence rate difference between the sites didnot reach statistical significance (Table 1) Along similar linesthe 45 carriage rate of PVL gene in LBHwas not statisticallysignificantly different from the 321 prevalence rate at KBH(Table 2) On the basis of vastly different occurrence of thePVL-positive organisms in different parts of the world itappears that the PVL carriage depends largely on the geo-graphical location and the organisms that are endemic in aparticular locality
Overall PVL carriage rates were 519 (1427) amongMSSA 733 (1115) among heterogeneous MRSA and 32(131) among homogeneous MRSA (Table 1) Comparedto MSSA and homogeneous MRSA heterogeneous MRSAdepicted a positive association with PVL carriage Howeverwhen heterogeneous and homogeneous MRSA were pooledtogether into a single cohort of MRSA isolates and comparedto MSSA MRSA was found to have a negative associationwith PVL prevalence The negative correlation between PVLand MRSA as a whole can be attributed to the 30 (968)PVL-negative homogeneousMRSA isolates which would off-set the PVL positivity of the 11 (733) heterogeneous MRSAisolates These findings suggest that in the observed hospitalsettings PVL positivity was associated with heterogeneousMRSA but not with homogeneous MRSA Consequentlycrude analyses ofMSSAversus pooledMRSA strains could bepotentially misleading a thorough evaluation of PVL emer-gence should constitute a breakdown of MRSA into homo-geneous and heterogeneous strains
A phenotypic analysis of the clinical isolates based ontheir antibiotic profiles allowed for a grouping of the isolatesinto 3 categories each of which revealed a relatively highPVL prevalence 60 nmMRSA 22 mMRSA and 519MSSA (Table 1) Munckhof and colleagues (2008) [29] reporta similar rate of PVLpositivity among their nmMRSA isolates(55) However their PVL prevalence rates of 2 amongmMRSA and 16 among MSSA are much lower comparedto this study
Classifying the clinical isolates cohort on the basis ofmacrolide lincosamide and streptogramin resistance typesit was found that while PVL positivity was 938 forMSB and458 for no-resistance types none of the isolates withMLSBresistance harbored the PVL gene (Table 1) This finding thatisolates characterized as MSB resistance type are more likelyto depict PVL positivity compared to either MLSB resistanceor no-resistance type was verified by testing for the presenceof msr(A) gene which showed a positive association withPVL
While it would have been ideal to carry out these molec-ular epidemiological analyses on the entire cohort of 404 iso-lates the study needed to limit its sample size to 73 randomlyselected isolates due to resource and monetary restric-tions Todayrsquos context of PVL diagnosis and epidemiology
is constrained by the lack of a reliable phenotypic testfor PVL positivity Studies that focus on developing suchnovelmethodologies for phenotypic characterization of PVL-positive bacterium which would complement the currentlyavailable genetic test will have substantial utility in promot-ing the early detection of these virulent microbes
5 Conclusion
Our study has shown a relatively high prevalence rate of PVLpositivity in HA-S aureus isolates from two tertiary care hos-pitals of Nepal PVL carriage was associated with heteroge-neous MRSA and MSB resistance type (confirmed bymsr(A)gene positivity) Compared toMSSAandnmMRSAmMRSAwas significantly less likely to harbor the PVL genes Noassociationwith age site of infection or hospital of originwasobserved Such an absence of predilection for a younger agegroup and the observed restriction pattern limitation of PVL-positive MRSA are in alignment with the fact that these wereclinical isolates obtained from hospital-acquired infectionsThe relatively high rates of PVL presence among HA-MRSAandHA-MSSA isolates and the interhospital spread of strainssupport the need for system-wide implementation of patientsafety and infection control initiatives
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] J Kaneko and Y Kamio ldquoBacterial two-component and hetero-heptameric pore-forming cytolytic toxins structures pore-formingmechanism and organization of the genesrdquo BioscienceBiotechnology and Biochemistry vol 68 no 5 pp 981ndash10032004
[2] G Prevost B Cribier P Couppie et al ldquoPanton-valentineleucocidin and gamma-hemolysin from Staphylococcus aureusATCC 49775 are encoded by distinct genetic loci and have dif-ferent biological activitiesrdquo Infection and Immunity vol 63 no10 pp 4121ndash4129 1995
[3] L GMiller F Perdreau-Remington G Rieg et al ldquoNecrotizingfasciitis caused by community-associated methicillin-resistantStaphylococcus aureus in Los AngelesrdquoTheNewEngland Journalof Medicine vol 352 no 14 pp 1445ndash1453 2005
[4] G R Kravitz D J Dries M L Peterson and P M SchlievertldquoPurpura fulminans due to Staphylococcus aureusrdquo ClinicalInfectious Diseases vol 40 no 7 pp 941ndash947 2005
[5] B McGrath F Rutledge and E Broadfield ldquoNecrotisingpneumonia Staphylococcus aureus andPanton-Valentine leuko-cidinrdquo The Journal of the Intensive Care Society vol 9 pp 170ndash172 2008
[6] G Lina Y Piemont F Godail-Gamot et al ldquoInvolvement ofPanton-Valentine leukocidin-producing Staphylococcus aureusin primary skin infections and pneumoniardquo Clinical InfectiousDiseases vol 29 no 5 pp 1128ndash1132 1999
[7] Y Gillet B Issartel P Vanhems et al ldquoAssociation betweenStaphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia
BioMed Research International 7
in young immunocompetent patientsrdquoThe Lancet vol 359 no9308 pp 753ndash759 2002
[8] L J Shallcross K Williams S Hopkins R W Aldridge AM Johnson and A C Hayward ldquoPanton-Valentine leukocidinassociated staphylococcal disease a cross-sectional study at aLondon hospital Englandrdquo Clinical Microbiology and Infectionvol 16 no 11 pp 1644ndash1648 2010
[9] A Holmes M Ganner S McGuane T L Pitt B D Cooksonand A M Kearns ldquoStaphylococcus aureus isolates carryingpanton-valentine leucocidin genes in England and Wales fre-quency characterization and association with clinical diseaserdquoJournal of Clinical Microbiology vol 43 no 5 pp 2384ndash23902005
[10] M J EllingtonMGanner IM Smith C Perry B D Cooksonand A M Kearns ldquoPanton-Valentine Leucocidin-related dis-ease in England andWalesrdquo Clinical Microbiology and Infectionvol 16 no 1 pp 86ndash88 2010
[11] S Breurec C Fall R Pouillot et al ldquoEpidemiology of met-hicillin-susceptible Staphylococcus aureus lineages in five majorAfrican towns high prevalence of Panton-Valentine leukocidingenesrdquoClinicalMicrobiology and Infection vol 17 no 4 pp 633ndash639 2011
[12] F Yu Z Chen C Liu et al ldquoPrevalence of Staphylococcus aureuscarrying Panton-Valentine leukocidin genes among isolatesfrom hospitalised patients in Chinardquo Clinical Microbiology andInfection vol 14 no 4 pp 381ndash384 2008
[13] S Monecke P Slickers M J Ellington A M Kearns andR Ehricht ldquoHigh diversity of Panton-Valentine leukocidin-positive methicillin-susceptible isolates of Staphylococcusaureus and implications for the evolution of community-associatedmethicillin-resistant S aureusrdquoClinical Microbiologyand Infection vol 13 no 12 pp 1157ndash1164 2007
[14] A S Rossney A C Shore P M Morgan M M Fitzgibbon BOConnell and D C Coleman ldquoThe emergence and importa-tion of diverse genotypes ofmethicillin-resistant Staphylococcusaureus (MRSA) harboring the panton-valentine leukocidingene (pvl) reveal that pvl is a poor marker for community-acquired MRSA strains in Irelandrdquo Journal of Clinical Microbi-ology vol 45 no 8 pp 2554ndash2563 2007
[15] J S Kim J S ParkW Song et al ldquoPanton-Valentine leukocidinpositive Staphylococcus aureus isolated from blood in KoreardquoThe Korean Journal of Laboratory Medicine vol 27 no 4 pp286ndash291 2007
[16] L-Y Hsu T-H Koh A Kurup J Low M P Chlebicki andB-H Tan ldquoHigh incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospi-tal in Singaporerdquo Clinical Infectious Diseases vol 40 no 3 pp486ndash489 2005
[17] Z C Karahan A Tekeli R Adaleti E Koyuncu I Dolapciand O A Akan ldquoInvestigation of Panton-Valentine leukocidingenes and SCCmec types in clinical Staphylococcus aureus iso-lates from TurkeyrdquoMicrobial Drug Resistance vol 14 no 3 pp203ndash210 2008
[18] D J Skiest K Brown T W Cooper H Hoffman-Roberts HR Mussa and A C Elliott ldquoProspective comparison of met-hicillin-susceptible and methicillin-resistant community-associated Staphylococcus aureus infections in hospitalizedpatientsrdquo Journal of Infection vol 54 no 5 pp 427ndash434 2007
[19] H C Baggatt T W Hennessy K Rudolph et al ldquoCommunity-onset methicillin-resistant Staphylococcus aureus associated
with antibiotic use and the cytotoxin Panton-Valentine leuko-cidin during a furunculosis outbreak in rural Alaskardquo Journalof Infectious Diseases vol 189 no 9 pp 1565ndash1573 2004
[20] J M Boyce B Cookson K Christiansen et al ldquoMeticillin-resistant Staphylococcus aureusrdquo Lancet Infectious Diseases vol5 no 10 pp 653ndash663 2005
[21] H Grundmann M Aires-de-Sousa J Boyce and E Tiem-ersma ldquoEmergence and resurgence of meticillin-resistantStaphylococcus aureus as a public-health threatrdquoTheLancet vol368 no 9538 pp 874ndash885 2006
[22] F Vandenesch T Naimi M C Enright et al ldquoCommunity-acquired methicillin-resistant Staphylococcus aureus carryingpanton-valentine leukocidin genes worldwide emergencerdquoEmerging Infectious Diseases vol 9 no 8 pp 978ndash984 2003
[23] Clinical Laboratory Standards Institute Performance Standardfor Antimicrobial Susceptibility Testing Seventeenth Informa-tional Supplement M100-S17 Clinical Laboratory StandardsInstitute Wayne Pa USA 2007
[24] B Cauwelier B Gordts P Descheemaecker and H van Lan-duyt ldquoEvaluation of a disk diffusion method with cefoxitin(30 120583g) for detection of methicillin-resistant StaphylococcusaureusrdquoEuropean Journal of ClinicalMicrobiology and InfectiousDiseases vol 23 no 5 pp 389ndash392 2004
[25] I BGosbell J LMercer S ANeville et al ldquoNon-multiresistantand multiresistant methicillin-resistant Staphylococcus aureusin community-acquired infectionsrdquo Medical Journal of Aus-tralia vol 174 no 12 pp 627ndash630 2001
[26] K K Bonnstetter D J Wolter F C Tenover L K McDougaland R V Goering ldquoRapid multiplex PCR assay for identifi-cation of USA300 community-associated methicillin-resistantStaphylococcus aureus isolatesrdquo Journal of Clinical Microbiologyvol 45 no 1 pp 141ndash146 2007
[27] T A Wichelhaus K P Hunfeld B Boddinghaus P Kraiczy VSchafer and V Brade ldquoRapid molecular typing of methicillinresistant Staphylococcus aureus by PCR-RFLPrdquo Infection Controland Hospital Epidemiology vol 22 no 5 pp 294ndash298 2001
[28] B Shrestha ldquoComparative prevalence ofMRSA in twoNepalesetertiary care hospitalsrdquoOpen Journal of Clinical Diagnostics vol3 pp 67ndash73 2013
[29] W J Munckhof G R Nimmo J Carney et al ldquoMethicillin-susceptible non-multiresistant methicillin-resistant and mul-tiresistant methicillin-resistant Staphylococcus aureus infec-tions a clinical epidemiological and microbiological compar-ative studyrdquo European Journal of Clinical Microbiology andInfectious Diseases vol 27 no 5 pp 355ndash364 2008
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
(a)
Coefficient000 059 118 177 237
H30
194
14
31
185
54
16
47
190
32
109
118
46
149
189
(b)
Figure 2 (a) PCR-RFLP of coa and spa amplified products of PVL-positive MSSA (14 isolates 14ndash194) and PVL-negative MSSA (3 isolates79ndash113) digested by HaeIIM = 1 kb DNA ladder PVL-positive MSSA isolates 16 and 47 cluster under one restriction type and isolates 14 31and 185 cluster under another The remaining nine PVL-positive MSSA isolates and all three PVL-negative MSSA isolates exist as singletons(b) Corresponding dendogram of the PCR-RFLP of PVL-positive and PVL-negative MSSA isolates
vancomycin linezolid kanamycin and rifampicin (Sigma-Aldrich Germany) The clinical isolates were suspendedin physiological saline (05 McFarland) using Densimat(Biomerieux Italy) followingwhich 100120583L of each suspendedisolate was dispensed into microtiter wells containing dou-bling dilutions of the 12 antibiotics in cation-adjustedMuellerHinton Broth (Becton Dickinson and Company USA) Themicrotiter plates were incubated at 37∘C for 18 hrs and wereread in reflected light
Data was analyzed using the statistical software SPSS 115
3 Results
The source sample of 404 hospital-acquired isolates consistedof 197 (488) MRSA isolates of which 148 (751) werehomogenous and 49 (249) were heterogeneous [28] Asmentioned earlier from the total sample of 404 clinicalisolates 73 isolates were randomly selected for further anal-ysis owing to resource limitations Of these 73 isolates thatcomprised of 46 MRSA and 27 MSSA isolates PVL genewas detected in 12 MRSA (261) and 14 MSSA (519) for acumulative prevalence rate of 356 As indicated in Table 1the PVL carriage was high in samples from UTI (50 48)SSI (352 1954) and lower RTI (222 29) Howevercross tab calculation between UTI and SSI (1198832 = 0655119875 = 0418) and SSI and lower RTI (1198831198912 = 0583 119875 = 0445)showed that the difference in PVL prevalence in these sitesdid not reach statistical significance
For our analysis the patient population was grouped into2 age groups le30 years (119899 = 27) and ge31 years (119899 = 46) ThePVL-positivity rates were 37 for le30 age group and 348for ge31 age group (Table 1) these values were not found to bestatistically significantly different (1198832 = 0038 119875 = 0846)We also did not find any association between PVL positivityand hospital of origin (Table 2) The PVL prevalence of 321at KBH and of 450 at LBH did not meet the statisticalcriteria for significant difference (1198832 = 1058 119875 = 0304)
Upon conducting a pooled evaluation of isolates fromboth hospitals PVL prevalence rates were found to be 733in heterogeneous MRSA 519 inMSSA and 32 in homo-geneous MRSA (Table 1) PVL occurrence was observed tobe significantly associated with a heterogeneous methicillinresistance pattern compared to homogeneous MRSA andMSSA (1198832 = 2659 119875 lt 0001) However a pooled sample ofboth homogeneous and heterogeneous MRSA failed to showany correlation with PVL carriage when compared to MSSA(1198832 = 4925 119875 = 0026)
As mentioned previously MRSA that was resistant toge3 non-120573-lactam antibiotics was categorized as multire-sistant MRSA (mMRSA) and that resistant to le2 non-120573-lactam antibiotics was identified as nonmultiresistant MRSA(nmMRSA) The distribution of PVL carriage rates was519 amongMSSA 60 among nmMRSA and 22 amongmMRSA (Table 1) Compared to MSSA and nmMRSAmMRSA had lesser prevalence of PVL positivity (1198832 = 7739119875 = 0021)
In assessing the putative relation between PVL prevalenceand macrolide lincosamide and streptogramin resistancetypes we found that none of the isolates withMLSB resistance(119899 = 32) was positive for PVL Among MSB resistancetypes PVL positivity was at 938 and among nonresistantisolates depicting susceptibility to both erythromycin andclindamycin PVL carriage was at 458 (Table 1) We foundthat MSB resistance types were significantly associated withPVL gene carriage when compared toMLSB resistance (119883
2=
4211 119875 lt 0001) and no-resistance types (1198832 = 9689 119875 =0002) Isolates susceptible to erythromycin and clindamycin(no-resistance type) had 177 greater odds of being PVL neg-ative as compared to MSB resistance types (OR = 17727 95CI 20 to 1565)
The MSB resistance type was genotypically confirmed bythe presence ofmsr(A) geneThe isolates harboring this genedepicted a strong associationwithPVLgene possession (1198832 =12049119875 = 0001) Compared to isolates carrying themsr(A)
BioMed Research International 5
Table 2 Hospital-specific PVL prevalence rates and methicillin resistance in S aureus
Strains (119899) Lalitpur Hospital Kathmandu Hospital TotalPVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos
MSSA (27) 4 3 571 10 10 500 519 (1427)Homo-MRSA (31) 0 7 385a 1 23 212b 261 (1246)Hetero-MRSA (15) 5 1 6 3Total (73) 9 11 450 17 36 321 356 (2673)aTotal PVL-positive prevalence rate in Lalitpur HospitalbTotal PVL-positive prevalence rate in Kathmandu HospitalHetero heterogeneous Homo homogeneous Pos positive Neg negative
gene no-resistance type isolates lacking this gene were 455times more likely to be not positive for PVL (OR = 455 95CI 35 to 5947)
The MIC of the 26 PVL-positive and 7 PVL-negativeisolates was determined by microbroth dilution method Nosubstantial difference could be noted in the resistance patternbetween PVL-positive and PVL-negative S aureus strains(both MRSA and MSSA) with the exception of tetracyclineand clindamycin to which PVL-positive and PVL-negativeisolates responded differently It was observed that whilePVL-positive MRSA was sensitive to both clindamycin andtetracycline PVL-negative MRSA was uniformly resistantto these antibiotics Further both PVL-positive and PVL-negativeMSSA isolateswere also sensitive to clindamycin andtetracycline
With regard to restriction types identified by PCR-RFLPPVL-positive MRSA PVL-negative MRSA PVL-positiveMSSA and PVL-negative MSSA isolates depicted two oneeleven and three restriction types respectively (Figures 1 and2) The majority of the PVL-positive MRSA isolates wereclustered under one restriction type (1012 DNA fragmentslength 400 bp and 750 bp) with the remaining two isolatesbeing grouped under the second restriction type (212 DNAfragments length 500 bp and 800 bp) All four isolates of PVL-negative MRSA belonged to a single restriction type ForPVL-positive MSSA two and three isolates were includedunder two distinct restriction types while the remainingnine isolates and all three of the PVL-negative MSSA isolatesexisted as singletons within their unique restriction types(Figure 2)
4 Discussion
In the present day context when microbial antibiotic resis-tance is progressively morphing into an intractable predica-ment acquisition of the potent PVL gene by MRSA whichrepresents a rather difficult challenge in itself would pavethe way to an alarming healthcare paradox In this paper wepresent the findings from the first PVL prevalence study inNepal which includes (i) heretofore unidentified associationsbetween PVL positivity and MSB resistance verified bymsr(A) gene (ii) PVL carriage rates specific to MRSA andMSSA isolates obtained from two premiere tertiary carehospitals (iii) evaluation of putative predilection of PVL-positive S aureus to a select patient profile (iv) compar-ative assessment of PVL prevalence among heterogeneous
MRSA-homogeneous MRSA-MSSA and among mMRSA-nmMRSA-MSSA and (v) restriction pattern characterizationof PVL-positive and PVL-negative hospital isolates
In the current study we report PVL gene carriage rateof 356 among nosocomial S aureus isolates 261 amongMRSA and 519 among MSSA (Table 1) These numberstrack along some of the highest reported PVL-positive Saureus prevalence rates and should rightfully be regarded as amatter of grave concern Further restriction pattern analysesof PVL-positive MRSA and MSSA have revealed that whilePVL-positive MSSA can be grouped into eleven restrictiontypes with a majority of the isolates existing as singletons(Figure 2) PVL-positiveMRSA seamlessly clusters under tworestriction types (Figure 1)This is an anticipated finding sinceMRSA isolates belong to a single clone while MSSA isolatespropagated from multiple clones Such spread of a limitednumber of PVL-carrying MRSA clones suggests that com-pared to their MSSA counterparts these microbes are well-adapted to thrive in the hospital environmentThe restrictiontype limitationwould also follow from the fact that theMRSAisolates are hospital strains that cause infection in any sus-ceptible host with the right combination of risk factors Alsothe restriction pattern clusters included isolates from bothLBH and KBH suggesting an interhospital transmission ofpathogenic strains These findings in conjunction with thehigh PVL-positive S aureus prevalence rates warrant theimmediate institution of effective infection control measures
In addition to clone limitation lack of any trend ofhigher PVL prevalence among a younger age group is anotherfinding explained by the hospital-acquired nature of the PVL-positive S aureus strains in the study At prevalence rates of37 for le30 years age group and 348 for ge31 years agegroup (Table 1) the PVL-positive isolates fail to show any age-related predilection Previous studies have shown a strongpredisposition of PVL-positive S aureus isolates for youngerand previously healthy patients [14 29] In a 2008 Australianstudy by Munckhof et al the authors observed a steadydecline in PVL occurrence with increasing age which theyascribed to age-associated strengthening of immunity and tothe natural penchant of children and young adults to acquirePVL-positive S aureus from skin contamination duringplayful and contact sports [29] This increased likelihood ofPVL-positive S aureus to infect younger age groups as seenin earlier studies may be attributed to the fact that a majorityof PVL-carrying S aureus isolates from these studies werecommunity-acquired In contrast our study exclusively
6 BioMed Research International
investigated nosocomial isolates which regardless of age caninfect any patient presenting with the right risk factors foracquiring an infection originating in the hospital
As with age PVL prevalence also exhibited no associationwith infection site or hospital of origin Although the highestnumbers of PVL-carrying S aureus isolates were recoveredfrom UTI (50) followed by SSI (352) and lower RTI(222) the prevalence rate difference between the sites didnot reach statistical significance (Table 1) Along similar linesthe 45 carriage rate of PVL gene in LBHwas not statisticallysignificantly different from the 321 prevalence rate at KBH(Table 2) On the basis of vastly different occurrence of thePVL-positive organisms in different parts of the world itappears that the PVL carriage depends largely on the geo-graphical location and the organisms that are endemic in aparticular locality
Overall PVL carriage rates were 519 (1427) amongMSSA 733 (1115) among heterogeneous MRSA and 32(131) among homogeneous MRSA (Table 1) Comparedto MSSA and homogeneous MRSA heterogeneous MRSAdepicted a positive association with PVL carriage Howeverwhen heterogeneous and homogeneous MRSA were pooledtogether into a single cohort of MRSA isolates and comparedto MSSA MRSA was found to have a negative associationwith PVL prevalence The negative correlation between PVLand MRSA as a whole can be attributed to the 30 (968)PVL-negative homogeneousMRSA isolates which would off-set the PVL positivity of the 11 (733) heterogeneous MRSAisolates These findings suggest that in the observed hospitalsettings PVL positivity was associated with heterogeneousMRSA but not with homogeneous MRSA Consequentlycrude analyses ofMSSAversus pooledMRSA strains could bepotentially misleading a thorough evaluation of PVL emer-gence should constitute a breakdown of MRSA into homo-geneous and heterogeneous strains
A phenotypic analysis of the clinical isolates based ontheir antibiotic profiles allowed for a grouping of the isolatesinto 3 categories each of which revealed a relatively highPVL prevalence 60 nmMRSA 22 mMRSA and 519MSSA (Table 1) Munckhof and colleagues (2008) [29] reporta similar rate of PVLpositivity among their nmMRSA isolates(55) However their PVL prevalence rates of 2 amongmMRSA and 16 among MSSA are much lower comparedto this study
Classifying the clinical isolates cohort on the basis ofmacrolide lincosamide and streptogramin resistance typesit was found that while PVL positivity was 938 forMSB and458 for no-resistance types none of the isolates withMLSBresistance harbored the PVL gene (Table 1) This finding thatisolates characterized as MSB resistance type are more likelyto depict PVL positivity compared to either MLSB resistanceor no-resistance type was verified by testing for the presenceof msr(A) gene which showed a positive association withPVL
While it would have been ideal to carry out these molec-ular epidemiological analyses on the entire cohort of 404 iso-lates the study needed to limit its sample size to 73 randomlyselected isolates due to resource and monetary restric-tions Todayrsquos context of PVL diagnosis and epidemiology
is constrained by the lack of a reliable phenotypic testfor PVL positivity Studies that focus on developing suchnovelmethodologies for phenotypic characterization of PVL-positive bacterium which would complement the currentlyavailable genetic test will have substantial utility in promot-ing the early detection of these virulent microbes
5 Conclusion
Our study has shown a relatively high prevalence rate of PVLpositivity in HA-S aureus isolates from two tertiary care hos-pitals of Nepal PVL carriage was associated with heteroge-neous MRSA and MSB resistance type (confirmed bymsr(A)gene positivity) Compared toMSSAandnmMRSAmMRSAwas significantly less likely to harbor the PVL genes Noassociationwith age site of infection or hospital of originwasobserved Such an absence of predilection for a younger agegroup and the observed restriction pattern limitation of PVL-positive MRSA are in alignment with the fact that these wereclinical isolates obtained from hospital-acquired infectionsThe relatively high rates of PVL presence among HA-MRSAandHA-MSSA isolates and the interhospital spread of strainssupport the need for system-wide implementation of patientsafety and infection control initiatives
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] J Kaneko and Y Kamio ldquoBacterial two-component and hetero-heptameric pore-forming cytolytic toxins structures pore-formingmechanism and organization of the genesrdquo BioscienceBiotechnology and Biochemistry vol 68 no 5 pp 981ndash10032004
[2] G Prevost B Cribier P Couppie et al ldquoPanton-valentineleucocidin and gamma-hemolysin from Staphylococcus aureusATCC 49775 are encoded by distinct genetic loci and have dif-ferent biological activitiesrdquo Infection and Immunity vol 63 no10 pp 4121ndash4129 1995
[3] L GMiller F Perdreau-Remington G Rieg et al ldquoNecrotizingfasciitis caused by community-associated methicillin-resistantStaphylococcus aureus in Los AngelesrdquoTheNewEngland Journalof Medicine vol 352 no 14 pp 1445ndash1453 2005
[4] G R Kravitz D J Dries M L Peterson and P M SchlievertldquoPurpura fulminans due to Staphylococcus aureusrdquo ClinicalInfectious Diseases vol 40 no 7 pp 941ndash947 2005
[5] B McGrath F Rutledge and E Broadfield ldquoNecrotisingpneumonia Staphylococcus aureus andPanton-Valentine leuko-cidinrdquo The Journal of the Intensive Care Society vol 9 pp 170ndash172 2008
[6] G Lina Y Piemont F Godail-Gamot et al ldquoInvolvement ofPanton-Valentine leukocidin-producing Staphylococcus aureusin primary skin infections and pneumoniardquo Clinical InfectiousDiseases vol 29 no 5 pp 1128ndash1132 1999
[7] Y Gillet B Issartel P Vanhems et al ldquoAssociation betweenStaphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia
BioMed Research International 7
in young immunocompetent patientsrdquoThe Lancet vol 359 no9308 pp 753ndash759 2002
[8] L J Shallcross K Williams S Hopkins R W Aldridge AM Johnson and A C Hayward ldquoPanton-Valentine leukocidinassociated staphylococcal disease a cross-sectional study at aLondon hospital Englandrdquo Clinical Microbiology and Infectionvol 16 no 11 pp 1644ndash1648 2010
[9] A Holmes M Ganner S McGuane T L Pitt B D Cooksonand A M Kearns ldquoStaphylococcus aureus isolates carryingpanton-valentine leucocidin genes in England and Wales fre-quency characterization and association with clinical diseaserdquoJournal of Clinical Microbiology vol 43 no 5 pp 2384ndash23902005
[10] M J EllingtonMGanner IM Smith C Perry B D Cooksonand A M Kearns ldquoPanton-Valentine Leucocidin-related dis-ease in England andWalesrdquo Clinical Microbiology and Infectionvol 16 no 1 pp 86ndash88 2010
[11] S Breurec C Fall R Pouillot et al ldquoEpidemiology of met-hicillin-susceptible Staphylococcus aureus lineages in five majorAfrican towns high prevalence of Panton-Valentine leukocidingenesrdquoClinicalMicrobiology and Infection vol 17 no 4 pp 633ndash639 2011
[12] F Yu Z Chen C Liu et al ldquoPrevalence of Staphylococcus aureuscarrying Panton-Valentine leukocidin genes among isolatesfrom hospitalised patients in Chinardquo Clinical Microbiology andInfection vol 14 no 4 pp 381ndash384 2008
[13] S Monecke P Slickers M J Ellington A M Kearns andR Ehricht ldquoHigh diversity of Panton-Valentine leukocidin-positive methicillin-susceptible isolates of Staphylococcusaureus and implications for the evolution of community-associatedmethicillin-resistant S aureusrdquoClinical Microbiologyand Infection vol 13 no 12 pp 1157ndash1164 2007
[14] A S Rossney A C Shore P M Morgan M M Fitzgibbon BOConnell and D C Coleman ldquoThe emergence and importa-tion of diverse genotypes ofmethicillin-resistant Staphylococcusaureus (MRSA) harboring the panton-valentine leukocidingene (pvl) reveal that pvl is a poor marker for community-acquired MRSA strains in Irelandrdquo Journal of Clinical Microbi-ology vol 45 no 8 pp 2554ndash2563 2007
[15] J S Kim J S ParkW Song et al ldquoPanton-Valentine leukocidinpositive Staphylococcus aureus isolated from blood in KoreardquoThe Korean Journal of Laboratory Medicine vol 27 no 4 pp286ndash291 2007
[16] L-Y Hsu T-H Koh A Kurup J Low M P Chlebicki andB-H Tan ldquoHigh incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospi-tal in Singaporerdquo Clinical Infectious Diseases vol 40 no 3 pp486ndash489 2005
[17] Z C Karahan A Tekeli R Adaleti E Koyuncu I Dolapciand O A Akan ldquoInvestigation of Panton-Valentine leukocidingenes and SCCmec types in clinical Staphylococcus aureus iso-lates from TurkeyrdquoMicrobial Drug Resistance vol 14 no 3 pp203ndash210 2008
[18] D J Skiest K Brown T W Cooper H Hoffman-Roberts HR Mussa and A C Elliott ldquoProspective comparison of met-hicillin-susceptible and methicillin-resistant community-associated Staphylococcus aureus infections in hospitalizedpatientsrdquo Journal of Infection vol 54 no 5 pp 427ndash434 2007
[19] H C Baggatt T W Hennessy K Rudolph et al ldquoCommunity-onset methicillin-resistant Staphylococcus aureus associated
with antibiotic use and the cytotoxin Panton-Valentine leuko-cidin during a furunculosis outbreak in rural Alaskardquo Journalof Infectious Diseases vol 189 no 9 pp 1565ndash1573 2004
[20] J M Boyce B Cookson K Christiansen et al ldquoMeticillin-resistant Staphylococcus aureusrdquo Lancet Infectious Diseases vol5 no 10 pp 653ndash663 2005
[21] H Grundmann M Aires-de-Sousa J Boyce and E Tiem-ersma ldquoEmergence and resurgence of meticillin-resistantStaphylococcus aureus as a public-health threatrdquoTheLancet vol368 no 9538 pp 874ndash885 2006
[22] F Vandenesch T Naimi M C Enright et al ldquoCommunity-acquired methicillin-resistant Staphylococcus aureus carryingpanton-valentine leukocidin genes worldwide emergencerdquoEmerging Infectious Diseases vol 9 no 8 pp 978ndash984 2003
[23] Clinical Laboratory Standards Institute Performance Standardfor Antimicrobial Susceptibility Testing Seventeenth Informa-tional Supplement M100-S17 Clinical Laboratory StandardsInstitute Wayne Pa USA 2007
[24] B Cauwelier B Gordts P Descheemaecker and H van Lan-duyt ldquoEvaluation of a disk diffusion method with cefoxitin(30 120583g) for detection of methicillin-resistant StaphylococcusaureusrdquoEuropean Journal of ClinicalMicrobiology and InfectiousDiseases vol 23 no 5 pp 389ndash392 2004
[25] I BGosbell J LMercer S ANeville et al ldquoNon-multiresistantand multiresistant methicillin-resistant Staphylococcus aureusin community-acquired infectionsrdquo Medical Journal of Aus-tralia vol 174 no 12 pp 627ndash630 2001
[26] K K Bonnstetter D J Wolter F C Tenover L K McDougaland R V Goering ldquoRapid multiplex PCR assay for identifi-cation of USA300 community-associated methicillin-resistantStaphylococcus aureus isolatesrdquo Journal of Clinical Microbiologyvol 45 no 1 pp 141ndash146 2007
[27] T A Wichelhaus K P Hunfeld B Boddinghaus P Kraiczy VSchafer and V Brade ldquoRapid molecular typing of methicillinresistant Staphylococcus aureus by PCR-RFLPrdquo Infection Controland Hospital Epidemiology vol 22 no 5 pp 294ndash298 2001
[28] B Shrestha ldquoComparative prevalence ofMRSA in twoNepalesetertiary care hospitalsrdquoOpen Journal of Clinical Diagnostics vol3 pp 67ndash73 2013
[29] W J Munckhof G R Nimmo J Carney et al ldquoMethicillin-susceptible non-multiresistant methicillin-resistant and mul-tiresistant methicillin-resistant Staphylococcus aureus infec-tions a clinical epidemiological and microbiological compar-ative studyrdquo European Journal of Clinical Microbiology andInfectious Diseases vol 27 no 5 pp 355ndash364 2008
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
Table 2 Hospital-specific PVL prevalence rates and methicillin resistance in S aureus
Strains (119899) Lalitpur Hospital Kathmandu Hospital TotalPVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos (119899) PVL Neg (119899) PVL Pos PVL Pos
MSSA (27) 4 3 571 10 10 500 519 (1427)Homo-MRSA (31) 0 7 385a 1 23 212b 261 (1246)Hetero-MRSA (15) 5 1 6 3Total (73) 9 11 450 17 36 321 356 (2673)aTotal PVL-positive prevalence rate in Lalitpur HospitalbTotal PVL-positive prevalence rate in Kathmandu HospitalHetero heterogeneous Homo homogeneous Pos positive Neg negative
gene no-resistance type isolates lacking this gene were 455times more likely to be not positive for PVL (OR = 455 95CI 35 to 5947)
The MIC of the 26 PVL-positive and 7 PVL-negativeisolates was determined by microbroth dilution method Nosubstantial difference could be noted in the resistance patternbetween PVL-positive and PVL-negative S aureus strains(both MRSA and MSSA) with the exception of tetracyclineand clindamycin to which PVL-positive and PVL-negativeisolates responded differently It was observed that whilePVL-positive MRSA was sensitive to both clindamycin andtetracycline PVL-negative MRSA was uniformly resistantto these antibiotics Further both PVL-positive and PVL-negativeMSSA isolateswere also sensitive to clindamycin andtetracycline
With regard to restriction types identified by PCR-RFLPPVL-positive MRSA PVL-negative MRSA PVL-positiveMSSA and PVL-negative MSSA isolates depicted two oneeleven and three restriction types respectively (Figures 1 and2) The majority of the PVL-positive MRSA isolates wereclustered under one restriction type (1012 DNA fragmentslength 400 bp and 750 bp) with the remaining two isolatesbeing grouped under the second restriction type (212 DNAfragments length 500 bp and 800 bp) All four isolates of PVL-negative MRSA belonged to a single restriction type ForPVL-positive MSSA two and three isolates were includedunder two distinct restriction types while the remainingnine isolates and all three of the PVL-negative MSSA isolatesexisted as singletons within their unique restriction types(Figure 2)
4 Discussion
In the present day context when microbial antibiotic resis-tance is progressively morphing into an intractable predica-ment acquisition of the potent PVL gene by MRSA whichrepresents a rather difficult challenge in itself would pavethe way to an alarming healthcare paradox In this paper wepresent the findings from the first PVL prevalence study inNepal which includes (i) heretofore unidentified associationsbetween PVL positivity and MSB resistance verified bymsr(A) gene (ii) PVL carriage rates specific to MRSA andMSSA isolates obtained from two premiere tertiary carehospitals (iii) evaluation of putative predilection of PVL-positive S aureus to a select patient profile (iv) compar-ative assessment of PVL prevalence among heterogeneous
MRSA-homogeneous MRSA-MSSA and among mMRSA-nmMRSA-MSSA and (v) restriction pattern characterizationof PVL-positive and PVL-negative hospital isolates
In the current study we report PVL gene carriage rateof 356 among nosocomial S aureus isolates 261 amongMRSA and 519 among MSSA (Table 1) These numberstrack along some of the highest reported PVL-positive Saureus prevalence rates and should rightfully be regarded as amatter of grave concern Further restriction pattern analysesof PVL-positive MRSA and MSSA have revealed that whilePVL-positive MSSA can be grouped into eleven restrictiontypes with a majority of the isolates existing as singletons(Figure 2) PVL-positiveMRSA seamlessly clusters under tworestriction types (Figure 1)This is an anticipated finding sinceMRSA isolates belong to a single clone while MSSA isolatespropagated from multiple clones Such spread of a limitednumber of PVL-carrying MRSA clones suggests that com-pared to their MSSA counterparts these microbes are well-adapted to thrive in the hospital environmentThe restrictiontype limitationwould also follow from the fact that theMRSAisolates are hospital strains that cause infection in any sus-ceptible host with the right combination of risk factors Alsothe restriction pattern clusters included isolates from bothLBH and KBH suggesting an interhospital transmission ofpathogenic strains These findings in conjunction with thehigh PVL-positive S aureus prevalence rates warrant theimmediate institution of effective infection control measures
In addition to clone limitation lack of any trend ofhigher PVL prevalence among a younger age group is anotherfinding explained by the hospital-acquired nature of the PVL-positive S aureus strains in the study At prevalence rates of37 for le30 years age group and 348 for ge31 years agegroup (Table 1) the PVL-positive isolates fail to show any age-related predilection Previous studies have shown a strongpredisposition of PVL-positive S aureus isolates for youngerand previously healthy patients [14 29] In a 2008 Australianstudy by Munckhof et al the authors observed a steadydecline in PVL occurrence with increasing age which theyascribed to age-associated strengthening of immunity and tothe natural penchant of children and young adults to acquirePVL-positive S aureus from skin contamination duringplayful and contact sports [29] This increased likelihood ofPVL-positive S aureus to infect younger age groups as seenin earlier studies may be attributed to the fact that a majorityof PVL-carrying S aureus isolates from these studies werecommunity-acquired In contrast our study exclusively
6 BioMed Research International
investigated nosocomial isolates which regardless of age caninfect any patient presenting with the right risk factors foracquiring an infection originating in the hospital
As with age PVL prevalence also exhibited no associationwith infection site or hospital of origin Although the highestnumbers of PVL-carrying S aureus isolates were recoveredfrom UTI (50) followed by SSI (352) and lower RTI(222) the prevalence rate difference between the sites didnot reach statistical significance (Table 1) Along similar linesthe 45 carriage rate of PVL gene in LBHwas not statisticallysignificantly different from the 321 prevalence rate at KBH(Table 2) On the basis of vastly different occurrence of thePVL-positive organisms in different parts of the world itappears that the PVL carriage depends largely on the geo-graphical location and the organisms that are endemic in aparticular locality
Overall PVL carriage rates were 519 (1427) amongMSSA 733 (1115) among heterogeneous MRSA and 32(131) among homogeneous MRSA (Table 1) Comparedto MSSA and homogeneous MRSA heterogeneous MRSAdepicted a positive association with PVL carriage Howeverwhen heterogeneous and homogeneous MRSA were pooledtogether into a single cohort of MRSA isolates and comparedto MSSA MRSA was found to have a negative associationwith PVL prevalence The negative correlation between PVLand MRSA as a whole can be attributed to the 30 (968)PVL-negative homogeneousMRSA isolates which would off-set the PVL positivity of the 11 (733) heterogeneous MRSAisolates These findings suggest that in the observed hospitalsettings PVL positivity was associated with heterogeneousMRSA but not with homogeneous MRSA Consequentlycrude analyses ofMSSAversus pooledMRSA strains could bepotentially misleading a thorough evaluation of PVL emer-gence should constitute a breakdown of MRSA into homo-geneous and heterogeneous strains
A phenotypic analysis of the clinical isolates based ontheir antibiotic profiles allowed for a grouping of the isolatesinto 3 categories each of which revealed a relatively highPVL prevalence 60 nmMRSA 22 mMRSA and 519MSSA (Table 1) Munckhof and colleagues (2008) [29] reporta similar rate of PVLpositivity among their nmMRSA isolates(55) However their PVL prevalence rates of 2 amongmMRSA and 16 among MSSA are much lower comparedto this study
Classifying the clinical isolates cohort on the basis ofmacrolide lincosamide and streptogramin resistance typesit was found that while PVL positivity was 938 forMSB and458 for no-resistance types none of the isolates withMLSBresistance harbored the PVL gene (Table 1) This finding thatisolates characterized as MSB resistance type are more likelyto depict PVL positivity compared to either MLSB resistanceor no-resistance type was verified by testing for the presenceof msr(A) gene which showed a positive association withPVL
While it would have been ideal to carry out these molec-ular epidemiological analyses on the entire cohort of 404 iso-lates the study needed to limit its sample size to 73 randomlyselected isolates due to resource and monetary restric-tions Todayrsquos context of PVL diagnosis and epidemiology
is constrained by the lack of a reliable phenotypic testfor PVL positivity Studies that focus on developing suchnovelmethodologies for phenotypic characterization of PVL-positive bacterium which would complement the currentlyavailable genetic test will have substantial utility in promot-ing the early detection of these virulent microbes
5 Conclusion
Our study has shown a relatively high prevalence rate of PVLpositivity in HA-S aureus isolates from two tertiary care hos-pitals of Nepal PVL carriage was associated with heteroge-neous MRSA and MSB resistance type (confirmed bymsr(A)gene positivity) Compared toMSSAandnmMRSAmMRSAwas significantly less likely to harbor the PVL genes Noassociationwith age site of infection or hospital of originwasobserved Such an absence of predilection for a younger agegroup and the observed restriction pattern limitation of PVL-positive MRSA are in alignment with the fact that these wereclinical isolates obtained from hospital-acquired infectionsThe relatively high rates of PVL presence among HA-MRSAandHA-MSSA isolates and the interhospital spread of strainssupport the need for system-wide implementation of patientsafety and infection control initiatives
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] J Kaneko and Y Kamio ldquoBacterial two-component and hetero-heptameric pore-forming cytolytic toxins structures pore-formingmechanism and organization of the genesrdquo BioscienceBiotechnology and Biochemistry vol 68 no 5 pp 981ndash10032004
[2] G Prevost B Cribier P Couppie et al ldquoPanton-valentineleucocidin and gamma-hemolysin from Staphylococcus aureusATCC 49775 are encoded by distinct genetic loci and have dif-ferent biological activitiesrdquo Infection and Immunity vol 63 no10 pp 4121ndash4129 1995
[3] L GMiller F Perdreau-Remington G Rieg et al ldquoNecrotizingfasciitis caused by community-associated methicillin-resistantStaphylococcus aureus in Los AngelesrdquoTheNewEngland Journalof Medicine vol 352 no 14 pp 1445ndash1453 2005
[4] G R Kravitz D J Dries M L Peterson and P M SchlievertldquoPurpura fulminans due to Staphylococcus aureusrdquo ClinicalInfectious Diseases vol 40 no 7 pp 941ndash947 2005
[5] B McGrath F Rutledge and E Broadfield ldquoNecrotisingpneumonia Staphylococcus aureus andPanton-Valentine leuko-cidinrdquo The Journal of the Intensive Care Society vol 9 pp 170ndash172 2008
[6] G Lina Y Piemont F Godail-Gamot et al ldquoInvolvement ofPanton-Valentine leukocidin-producing Staphylococcus aureusin primary skin infections and pneumoniardquo Clinical InfectiousDiseases vol 29 no 5 pp 1128ndash1132 1999
[7] Y Gillet B Issartel P Vanhems et al ldquoAssociation betweenStaphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia
BioMed Research International 7
in young immunocompetent patientsrdquoThe Lancet vol 359 no9308 pp 753ndash759 2002
[8] L J Shallcross K Williams S Hopkins R W Aldridge AM Johnson and A C Hayward ldquoPanton-Valentine leukocidinassociated staphylococcal disease a cross-sectional study at aLondon hospital Englandrdquo Clinical Microbiology and Infectionvol 16 no 11 pp 1644ndash1648 2010
[9] A Holmes M Ganner S McGuane T L Pitt B D Cooksonand A M Kearns ldquoStaphylococcus aureus isolates carryingpanton-valentine leucocidin genes in England and Wales fre-quency characterization and association with clinical diseaserdquoJournal of Clinical Microbiology vol 43 no 5 pp 2384ndash23902005
[10] M J EllingtonMGanner IM Smith C Perry B D Cooksonand A M Kearns ldquoPanton-Valentine Leucocidin-related dis-ease in England andWalesrdquo Clinical Microbiology and Infectionvol 16 no 1 pp 86ndash88 2010
[11] S Breurec C Fall R Pouillot et al ldquoEpidemiology of met-hicillin-susceptible Staphylococcus aureus lineages in five majorAfrican towns high prevalence of Panton-Valentine leukocidingenesrdquoClinicalMicrobiology and Infection vol 17 no 4 pp 633ndash639 2011
[12] F Yu Z Chen C Liu et al ldquoPrevalence of Staphylococcus aureuscarrying Panton-Valentine leukocidin genes among isolatesfrom hospitalised patients in Chinardquo Clinical Microbiology andInfection vol 14 no 4 pp 381ndash384 2008
[13] S Monecke P Slickers M J Ellington A M Kearns andR Ehricht ldquoHigh diversity of Panton-Valentine leukocidin-positive methicillin-susceptible isolates of Staphylococcusaureus and implications for the evolution of community-associatedmethicillin-resistant S aureusrdquoClinical Microbiologyand Infection vol 13 no 12 pp 1157ndash1164 2007
[14] A S Rossney A C Shore P M Morgan M M Fitzgibbon BOConnell and D C Coleman ldquoThe emergence and importa-tion of diverse genotypes ofmethicillin-resistant Staphylococcusaureus (MRSA) harboring the panton-valentine leukocidingene (pvl) reveal that pvl is a poor marker for community-acquired MRSA strains in Irelandrdquo Journal of Clinical Microbi-ology vol 45 no 8 pp 2554ndash2563 2007
[15] J S Kim J S ParkW Song et al ldquoPanton-Valentine leukocidinpositive Staphylococcus aureus isolated from blood in KoreardquoThe Korean Journal of Laboratory Medicine vol 27 no 4 pp286ndash291 2007
[16] L-Y Hsu T-H Koh A Kurup J Low M P Chlebicki andB-H Tan ldquoHigh incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospi-tal in Singaporerdquo Clinical Infectious Diseases vol 40 no 3 pp486ndash489 2005
[17] Z C Karahan A Tekeli R Adaleti E Koyuncu I Dolapciand O A Akan ldquoInvestigation of Panton-Valentine leukocidingenes and SCCmec types in clinical Staphylococcus aureus iso-lates from TurkeyrdquoMicrobial Drug Resistance vol 14 no 3 pp203ndash210 2008
[18] D J Skiest K Brown T W Cooper H Hoffman-Roberts HR Mussa and A C Elliott ldquoProspective comparison of met-hicillin-susceptible and methicillin-resistant community-associated Staphylococcus aureus infections in hospitalizedpatientsrdquo Journal of Infection vol 54 no 5 pp 427ndash434 2007
[19] H C Baggatt T W Hennessy K Rudolph et al ldquoCommunity-onset methicillin-resistant Staphylococcus aureus associated
with antibiotic use and the cytotoxin Panton-Valentine leuko-cidin during a furunculosis outbreak in rural Alaskardquo Journalof Infectious Diseases vol 189 no 9 pp 1565ndash1573 2004
[20] J M Boyce B Cookson K Christiansen et al ldquoMeticillin-resistant Staphylococcus aureusrdquo Lancet Infectious Diseases vol5 no 10 pp 653ndash663 2005
[21] H Grundmann M Aires-de-Sousa J Boyce and E Tiem-ersma ldquoEmergence and resurgence of meticillin-resistantStaphylococcus aureus as a public-health threatrdquoTheLancet vol368 no 9538 pp 874ndash885 2006
[22] F Vandenesch T Naimi M C Enright et al ldquoCommunity-acquired methicillin-resistant Staphylococcus aureus carryingpanton-valentine leukocidin genes worldwide emergencerdquoEmerging Infectious Diseases vol 9 no 8 pp 978ndash984 2003
[23] Clinical Laboratory Standards Institute Performance Standardfor Antimicrobial Susceptibility Testing Seventeenth Informa-tional Supplement M100-S17 Clinical Laboratory StandardsInstitute Wayne Pa USA 2007
[24] B Cauwelier B Gordts P Descheemaecker and H van Lan-duyt ldquoEvaluation of a disk diffusion method with cefoxitin(30 120583g) for detection of methicillin-resistant StaphylococcusaureusrdquoEuropean Journal of ClinicalMicrobiology and InfectiousDiseases vol 23 no 5 pp 389ndash392 2004
[25] I BGosbell J LMercer S ANeville et al ldquoNon-multiresistantand multiresistant methicillin-resistant Staphylococcus aureusin community-acquired infectionsrdquo Medical Journal of Aus-tralia vol 174 no 12 pp 627ndash630 2001
[26] K K Bonnstetter D J Wolter F C Tenover L K McDougaland R V Goering ldquoRapid multiplex PCR assay for identifi-cation of USA300 community-associated methicillin-resistantStaphylococcus aureus isolatesrdquo Journal of Clinical Microbiologyvol 45 no 1 pp 141ndash146 2007
[27] T A Wichelhaus K P Hunfeld B Boddinghaus P Kraiczy VSchafer and V Brade ldquoRapid molecular typing of methicillinresistant Staphylococcus aureus by PCR-RFLPrdquo Infection Controland Hospital Epidemiology vol 22 no 5 pp 294ndash298 2001
[28] B Shrestha ldquoComparative prevalence ofMRSA in twoNepalesetertiary care hospitalsrdquoOpen Journal of Clinical Diagnostics vol3 pp 67ndash73 2013
[29] W J Munckhof G R Nimmo J Carney et al ldquoMethicillin-susceptible non-multiresistant methicillin-resistant and mul-tiresistant methicillin-resistant Staphylococcus aureus infec-tions a clinical epidemiological and microbiological compar-ative studyrdquo European Journal of Clinical Microbiology andInfectious Diseases vol 27 no 5 pp 355ndash364 2008
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
investigated nosocomial isolates which regardless of age caninfect any patient presenting with the right risk factors foracquiring an infection originating in the hospital
As with age PVL prevalence also exhibited no associationwith infection site or hospital of origin Although the highestnumbers of PVL-carrying S aureus isolates were recoveredfrom UTI (50) followed by SSI (352) and lower RTI(222) the prevalence rate difference between the sites didnot reach statistical significance (Table 1) Along similar linesthe 45 carriage rate of PVL gene in LBHwas not statisticallysignificantly different from the 321 prevalence rate at KBH(Table 2) On the basis of vastly different occurrence of thePVL-positive organisms in different parts of the world itappears that the PVL carriage depends largely on the geo-graphical location and the organisms that are endemic in aparticular locality
Overall PVL carriage rates were 519 (1427) amongMSSA 733 (1115) among heterogeneous MRSA and 32(131) among homogeneous MRSA (Table 1) Comparedto MSSA and homogeneous MRSA heterogeneous MRSAdepicted a positive association with PVL carriage Howeverwhen heterogeneous and homogeneous MRSA were pooledtogether into a single cohort of MRSA isolates and comparedto MSSA MRSA was found to have a negative associationwith PVL prevalence The negative correlation between PVLand MRSA as a whole can be attributed to the 30 (968)PVL-negative homogeneousMRSA isolates which would off-set the PVL positivity of the 11 (733) heterogeneous MRSAisolates These findings suggest that in the observed hospitalsettings PVL positivity was associated with heterogeneousMRSA but not with homogeneous MRSA Consequentlycrude analyses ofMSSAversus pooledMRSA strains could bepotentially misleading a thorough evaluation of PVL emer-gence should constitute a breakdown of MRSA into homo-geneous and heterogeneous strains
A phenotypic analysis of the clinical isolates based ontheir antibiotic profiles allowed for a grouping of the isolatesinto 3 categories each of which revealed a relatively highPVL prevalence 60 nmMRSA 22 mMRSA and 519MSSA (Table 1) Munckhof and colleagues (2008) [29] reporta similar rate of PVLpositivity among their nmMRSA isolates(55) However their PVL prevalence rates of 2 amongmMRSA and 16 among MSSA are much lower comparedto this study
Classifying the clinical isolates cohort on the basis ofmacrolide lincosamide and streptogramin resistance typesit was found that while PVL positivity was 938 forMSB and458 for no-resistance types none of the isolates withMLSBresistance harbored the PVL gene (Table 1) This finding thatisolates characterized as MSB resistance type are more likelyto depict PVL positivity compared to either MLSB resistanceor no-resistance type was verified by testing for the presenceof msr(A) gene which showed a positive association withPVL
While it would have been ideal to carry out these molec-ular epidemiological analyses on the entire cohort of 404 iso-lates the study needed to limit its sample size to 73 randomlyselected isolates due to resource and monetary restric-tions Todayrsquos context of PVL diagnosis and epidemiology
is constrained by the lack of a reliable phenotypic testfor PVL positivity Studies that focus on developing suchnovelmethodologies for phenotypic characterization of PVL-positive bacterium which would complement the currentlyavailable genetic test will have substantial utility in promot-ing the early detection of these virulent microbes
5 Conclusion
Our study has shown a relatively high prevalence rate of PVLpositivity in HA-S aureus isolates from two tertiary care hos-pitals of Nepal PVL carriage was associated with heteroge-neous MRSA and MSB resistance type (confirmed bymsr(A)gene positivity) Compared toMSSAandnmMRSAmMRSAwas significantly less likely to harbor the PVL genes Noassociationwith age site of infection or hospital of originwasobserved Such an absence of predilection for a younger agegroup and the observed restriction pattern limitation of PVL-positive MRSA are in alignment with the fact that these wereclinical isolates obtained from hospital-acquired infectionsThe relatively high rates of PVL presence among HA-MRSAandHA-MSSA isolates and the interhospital spread of strainssupport the need for system-wide implementation of patientsafety and infection control initiatives
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] J Kaneko and Y Kamio ldquoBacterial two-component and hetero-heptameric pore-forming cytolytic toxins structures pore-formingmechanism and organization of the genesrdquo BioscienceBiotechnology and Biochemistry vol 68 no 5 pp 981ndash10032004
[2] G Prevost B Cribier P Couppie et al ldquoPanton-valentineleucocidin and gamma-hemolysin from Staphylococcus aureusATCC 49775 are encoded by distinct genetic loci and have dif-ferent biological activitiesrdquo Infection and Immunity vol 63 no10 pp 4121ndash4129 1995
[3] L GMiller F Perdreau-Remington G Rieg et al ldquoNecrotizingfasciitis caused by community-associated methicillin-resistantStaphylococcus aureus in Los AngelesrdquoTheNewEngland Journalof Medicine vol 352 no 14 pp 1445ndash1453 2005
[4] G R Kravitz D J Dries M L Peterson and P M SchlievertldquoPurpura fulminans due to Staphylococcus aureusrdquo ClinicalInfectious Diseases vol 40 no 7 pp 941ndash947 2005
[5] B McGrath F Rutledge and E Broadfield ldquoNecrotisingpneumonia Staphylococcus aureus andPanton-Valentine leuko-cidinrdquo The Journal of the Intensive Care Society vol 9 pp 170ndash172 2008
[6] G Lina Y Piemont F Godail-Gamot et al ldquoInvolvement ofPanton-Valentine leukocidin-producing Staphylococcus aureusin primary skin infections and pneumoniardquo Clinical InfectiousDiseases vol 29 no 5 pp 1128ndash1132 1999
[7] Y Gillet B Issartel P Vanhems et al ldquoAssociation betweenStaphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia
BioMed Research International 7
in young immunocompetent patientsrdquoThe Lancet vol 359 no9308 pp 753ndash759 2002
[8] L J Shallcross K Williams S Hopkins R W Aldridge AM Johnson and A C Hayward ldquoPanton-Valentine leukocidinassociated staphylococcal disease a cross-sectional study at aLondon hospital Englandrdquo Clinical Microbiology and Infectionvol 16 no 11 pp 1644ndash1648 2010
[9] A Holmes M Ganner S McGuane T L Pitt B D Cooksonand A M Kearns ldquoStaphylococcus aureus isolates carryingpanton-valentine leucocidin genes in England and Wales fre-quency characterization and association with clinical diseaserdquoJournal of Clinical Microbiology vol 43 no 5 pp 2384ndash23902005
[10] M J EllingtonMGanner IM Smith C Perry B D Cooksonand A M Kearns ldquoPanton-Valentine Leucocidin-related dis-ease in England andWalesrdquo Clinical Microbiology and Infectionvol 16 no 1 pp 86ndash88 2010
[11] S Breurec C Fall R Pouillot et al ldquoEpidemiology of met-hicillin-susceptible Staphylococcus aureus lineages in five majorAfrican towns high prevalence of Panton-Valentine leukocidingenesrdquoClinicalMicrobiology and Infection vol 17 no 4 pp 633ndash639 2011
[12] F Yu Z Chen C Liu et al ldquoPrevalence of Staphylococcus aureuscarrying Panton-Valentine leukocidin genes among isolatesfrom hospitalised patients in Chinardquo Clinical Microbiology andInfection vol 14 no 4 pp 381ndash384 2008
[13] S Monecke P Slickers M J Ellington A M Kearns andR Ehricht ldquoHigh diversity of Panton-Valentine leukocidin-positive methicillin-susceptible isolates of Staphylococcusaureus and implications for the evolution of community-associatedmethicillin-resistant S aureusrdquoClinical Microbiologyand Infection vol 13 no 12 pp 1157ndash1164 2007
[14] A S Rossney A C Shore P M Morgan M M Fitzgibbon BOConnell and D C Coleman ldquoThe emergence and importa-tion of diverse genotypes ofmethicillin-resistant Staphylococcusaureus (MRSA) harboring the panton-valentine leukocidingene (pvl) reveal that pvl is a poor marker for community-acquired MRSA strains in Irelandrdquo Journal of Clinical Microbi-ology vol 45 no 8 pp 2554ndash2563 2007
[15] J S Kim J S ParkW Song et al ldquoPanton-Valentine leukocidinpositive Staphylococcus aureus isolated from blood in KoreardquoThe Korean Journal of Laboratory Medicine vol 27 no 4 pp286ndash291 2007
[16] L-Y Hsu T-H Koh A Kurup J Low M P Chlebicki andB-H Tan ldquoHigh incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospi-tal in Singaporerdquo Clinical Infectious Diseases vol 40 no 3 pp486ndash489 2005
[17] Z C Karahan A Tekeli R Adaleti E Koyuncu I Dolapciand O A Akan ldquoInvestigation of Panton-Valentine leukocidingenes and SCCmec types in clinical Staphylococcus aureus iso-lates from TurkeyrdquoMicrobial Drug Resistance vol 14 no 3 pp203ndash210 2008
[18] D J Skiest K Brown T W Cooper H Hoffman-Roberts HR Mussa and A C Elliott ldquoProspective comparison of met-hicillin-susceptible and methicillin-resistant community-associated Staphylococcus aureus infections in hospitalizedpatientsrdquo Journal of Infection vol 54 no 5 pp 427ndash434 2007
[19] H C Baggatt T W Hennessy K Rudolph et al ldquoCommunity-onset methicillin-resistant Staphylococcus aureus associated
with antibiotic use and the cytotoxin Panton-Valentine leuko-cidin during a furunculosis outbreak in rural Alaskardquo Journalof Infectious Diseases vol 189 no 9 pp 1565ndash1573 2004
[20] J M Boyce B Cookson K Christiansen et al ldquoMeticillin-resistant Staphylococcus aureusrdquo Lancet Infectious Diseases vol5 no 10 pp 653ndash663 2005
[21] H Grundmann M Aires-de-Sousa J Boyce and E Tiem-ersma ldquoEmergence and resurgence of meticillin-resistantStaphylococcus aureus as a public-health threatrdquoTheLancet vol368 no 9538 pp 874ndash885 2006
[22] F Vandenesch T Naimi M C Enright et al ldquoCommunity-acquired methicillin-resistant Staphylococcus aureus carryingpanton-valentine leukocidin genes worldwide emergencerdquoEmerging Infectious Diseases vol 9 no 8 pp 978ndash984 2003
[23] Clinical Laboratory Standards Institute Performance Standardfor Antimicrobial Susceptibility Testing Seventeenth Informa-tional Supplement M100-S17 Clinical Laboratory StandardsInstitute Wayne Pa USA 2007
[24] B Cauwelier B Gordts P Descheemaecker and H van Lan-duyt ldquoEvaluation of a disk diffusion method with cefoxitin(30 120583g) for detection of methicillin-resistant StaphylococcusaureusrdquoEuropean Journal of ClinicalMicrobiology and InfectiousDiseases vol 23 no 5 pp 389ndash392 2004
[25] I BGosbell J LMercer S ANeville et al ldquoNon-multiresistantand multiresistant methicillin-resistant Staphylococcus aureusin community-acquired infectionsrdquo Medical Journal of Aus-tralia vol 174 no 12 pp 627ndash630 2001
[26] K K Bonnstetter D J Wolter F C Tenover L K McDougaland R V Goering ldquoRapid multiplex PCR assay for identifi-cation of USA300 community-associated methicillin-resistantStaphylococcus aureus isolatesrdquo Journal of Clinical Microbiologyvol 45 no 1 pp 141ndash146 2007
[27] T A Wichelhaus K P Hunfeld B Boddinghaus P Kraiczy VSchafer and V Brade ldquoRapid molecular typing of methicillinresistant Staphylococcus aureus by PCR-RFLPrdquo Infection Controland Hospital Epidemiology vol 22 no 5 pp 294ndash298 2001
[28] B Shrestha ldquoComparative prevalence ofMRSA in twoNepalesetertiary care hospitalsrdquoOpen Journal of Clinical Diagnostics vol3 pp 67ndash73 2013
[29] W J Munckhof G R Nimmo J Carney et al ldquoMethicillin-susceptible non-multiresistant methicillin-resistant and mul-tiresistant methicillin-resistant Staphylococcus aureus infec-tions a clinical epidemiological and microbiological compar-ative studyrdquo European Journal of Clinical Microbiology andInfectious Diseases vol 27 no 5 pp 355ndash364 2008
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
in young immunocompetent patientsrdquoThe Lancet vol 359 no9308 pp 753ndash759 2002
[8] L J Shallcross K Williams S Hopkins R W Aldridge AM Johnson and A C Hayward ldquoPanton-Valentine leukocidinassociated staphylococcal disease a cross-sectional study at aLondon hospital Englandrdquo Clinical Microbiology and Infectionvol 16 no 11 pp 1644ndash1648 2010
[9] A Holmes M Ganner S McGuane T L Pitt B D Cooksonand A M Kearns ldquoStaphylococcus aureus isolates carryingpanton-valentine leucocidin genes in England and Wales fre-quency characterization and association with clinical diseaserdquoJournal of Clinical Microbiology vol 43 no 5 pp 2384ndash23902005
[10] M J EllingtonMGanner IM Smith C Perry B D Cooksonand A M Kearns ldquoPanton-Valentine Leucocidin-related dis-ease in England andWalesrdquo Clinical Microbiology and Infectionvol 16 no 1 pp 86ndash88 2010
[11] S Breurec C Fall R Pouillot et al ldquoEpidemiology of met-hicillin-susceptible Staphylococcus aureus lineages in five majorAfrican towns high prevalence of Panton-Valentine leukocidingenesrdquoClinicalMicrobiology and Infection vol 17 no 4 pp 633ndash639 2011
[12] F Yu Z Chen C Liu et al ldquoPrevalence of Staphylococcus aureuscarrying Panton-Valentine leukocidin genes among isolatesfrom hospitalised patients in Chinardquo Clinical Microbiology andInfection vol 14 no 4 pp 381ndash384 2008
[13] S Monecke P Slickers M J Ellington A M Kearns andR Ehricht ldquoHigh diversity of Panton-Valentine leukocidin-positive methicillin-susceptible isolates of Staphylococcusaureus and implications for the evolution of community-associatedmethicillin-resistant S aureusrdquoClinical Microbiologyand Infection vol 13 no 12 pp 1157ndash1164 2007
[14] A S Rossney A C Shore P M Morgan M M Fitzgibbon BOConnell and D C Coleman ldquoThe emergence and importa-tion of diverse genotypes ofmethicillin-resistant Staphylococcusaureus (MRSA) harboring the panton-valentine leukocidingene (pvl) reveal that pvl is a poor marker for community-acquired MRSA strains in Irelandrdquo Journal of Clinical Microbi-ology vol 45 no 8 pp 2554ndash2563 2007
[15] J S Kim J S ParkW Song et al ldquoPanton-Valentine leukocidinpositive Staphylococcus aureus isolated from blood in KoreardquoThe Korean Journal of Laboratory Medicine vol 27 no 4 pp286ndash291 2007
[16] L-Y Hsu T-H Koh A Kurup J Low M P Chlebicki andB-H Tan ldquoHigh incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospi-tal in Singaporerdquo Clinical Infectious Diseases vol 40 no 3 pp486ndash489 2005
[17] Z C Karahan A Tekeli R Adaleti E Koyuncu I Dolapciand O A Akan ldquoInvestigation of Panton-Valentine leukocidingenes and SCCmec types in clinical Staphylococcus aureus iso-lates from TurkeyrdquoMicrobial Drug Resistance vol 14 no 3 pp203ndash210 2008
[18] D J Skiest K Brown T W Cooper H Hoffman-Roberts HR Mussa and A C Elliott ldquoProspective comparison of met-hicillin-susceptible and methicillin-resistant community-associated Staphylococcus aureus infections in hospitalizedpatientsrdquo Journal of Infection vol 54 no 5 pp 427ndash434 2007
[19] H C Baggatt T W Hennessy K Rudolph et al ldquoCommunity-onset methicillin-resistant Staphylococcus aureus associated
with antibiotic use and the cytotoxin Panton-Valentine leuko-cidin during a furunculosis outbreak in rural Alaskardquo Journalof Infectious Diseases vol 189 no 9 pp 1565ndash1573 2004
[20] J M Boyce B Cookson K Christiansen et al ldquoMeticillin-resistant Staphylococcus aureusrdquo Lancet Infectious Diseases vol5 no 10 pp 653ndash663 2005
[21] H Grundmann M Aires-de-Sousa J Boyce and E Tiem-ersma ldquoEmergence and resurgence of meticillin-resistantStaphylococcus aureus as a public-health threatrdquoTheLancet vol368 no 9538 pp 874ndash885 2006
[22] F Vandenesch T Naimi M C Enright et al ldquoCommunity-acquired methicillin-resistant Staphylococcus aureus carryingpanton-valentine leukocidin genes worldwide emergencerdquoEmerging Infectious Diseases vol 9 no 8 pp 978ndash984 2003
[23] Clinical Laboratory Standards Institute Performance Standardfor Antimicrobial Susceptibility Testing Seventeenth Informa-tional Supplement M100-S17 Clinical Laboratory StandardsInstitute Wayne Pa USA 2007
[24] B Cauwelier B Gordts P Descheemaecker and H van Lan-duyt ldquoEvaluation of a disk diffusion method with cefoxitin(30 120583g) for detection of methicillin-resistant StaphylococcusaureusrdquoEuropean Journal of ClinicalMicrobiology and InfectiousDiseases vol 23 no 5 pp 389ndash392 2004
[25] I BGosbell J LMercer S ANeville et al ldquoNon-multiresistantand multiresistant methicillin-resistant Staphylococcus aureusin community-acquired infectionsrdquo Medical Journal of Aus-tralia vol 174 no 12 pp 627ndash630 2001
[26] K K Bonnstetter D J Wolter F C Tenover L K McDougaland R V Goering ldquoRapid multiplex PCR assay for identifi-cation of USA300 community-associated methicillin-resistantStaphylococcus aureus isolatesrdquo Journal of Clinical Microbiologyvol 45 no 1 pp 141ndash146 2007
[27] T A Wichelhaus K P Hunfeld B Boddinghaus P Kraiczy VSchafer and V Brade ldquoRapid molecular typing of methicillinresistant Staphylococcus aureus by PCR-RFLPrdquo Infection Controland Hospital Epidemiology vol 22 no 5 pp 294ndash298 2001
[28] B Shrestha ldquoComparative prevalence ofMRSA in twoNepalesetertiary care hospitalsrdquoOpen Journal of Clinical Diagnostics vol3 pp 67ndash73 2013
[29] W J Munckhof G R Nimmo J Carney et al ldquoMethicillin-susceptible non-multiresistant methicillin-resistant and mul-tiresistant methicillin-resistant Staphylococcus aureus infec-tions a clinical epidemiological and microbiological compar-ative studyrdquo European Journal of Clinical Microbiology andInfectious Diseases vol 27 no 5 pp 355ndash364 2008
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom