Embed Size (px)
Citation preview

Hindawi Publishing CorporationComputational and Mathematical Methods in MedicineVolume 2013, Article ID 659038, 7 pageshttp://dx.doi.org/10.1155/2013/659038
Research ArticleMaximum Equilibrium Prevalence of Mosquito-BorneMicroparasite Infections in Humans
Marcos Amaku,1 Marcelo Nascimento Burattini,2 Francisco Antonio Bezerra Coutinho,2
Luis Fernandez Lopez,2,3 and Eduardo Massad2,4
1 School of Veterinary Medicine, University of Sao Paulo, Avenida Prof. Dr. Orlando Marques de Paiva 87,Cep 05508-270 Sao Paulo, SP, Brazil
2 School of Medicine, University of Sao Paulo and LIM 01-HCFMUSP, Rua Teodoro Sampaio 115, Cep 05405-000 Sao Paulo, SP, Brazil3 CIARA, Florida International University, Miami, FL 33199, USA4London School of Hygiene and Tropical Medicine, London University, London WC1E 7HT, UK
Correspondence should be addressed to Marcos Amaku; [email protected]
Received 4 August 2013; Accepted 23 November 2013
Academic Editor: Chris Bauch
Copyright © 2013 Marcos Amaku et al.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
To determine the maximum equilibrium prevalence of mosquito-borne microparasitic infections, this paper proposes a generalmodel for vector-borne infections which is flexible enough to comprise the dynamics of a great number of the known diseasestransmitted by arthropods. From equilibrium analysis, we determined the number of infected vectors as an explicit function of themodel’s parameters and the prevalence of infection in the hosts. From the analysis, it is also possible to derive the basic reproductionnumber and the equilibrium force of infection as a function of those parameters and variables. From the force of infection, we wereable to conclude that, depending on the disease’s structure and the model’s parameters, there is a maximum value of equilibriumprevalence for each of the mosquito-bornemicroparasitic infections.The analysis is exemplified by the cases of malaria and denguefever. With the values of the parameters chosen to illustrate those calculations, the maximum equilibrium prevalence found was31% and 0.02% for malaria and dengue, respectively. The equilibrium analysis demonstrated that there is a maximum prevalencefor the mosquito-borne microparasitic infections.
1. Introduction
Vector-borne diseases such as malaria, dengue, yellow fever,plague, trypanosomiasis, and leishmaniasis have been majorcauses ofmorbidity andmortality through human history [1].
Currently, half of the world’s population is infected withat least one type of vector-borne pathogens [2, 3]. Only onemosquito-borne infection, dengue fever, affects the lives of 3.6billion people worldwide [4, 5].
In the 17th through early 20th centuries, human morbid-ity and mortality due to vector-borne diseases outstrippedall other causes combined [6]. By the 1960s the majorityof vector-borne infections have been effectively controlledor targeted for intensive programmes. However, such pro-grammes were discontinued in the 1970s because vector-borne infections were no longer considered major public
health problems [7–10]. As a consequence, in the 1980s, theworld observed a resurgence of old vector-borne diseases andthe emergence of new ones [11].
The historical paradigm of mosquito-borne infections,malaria, accounts for the most deaths than any other humanvector-borne diseases, with approximately 300million peopleinfected and up to one million deaths every year [12, 13].Explosive epidemics have also marked the resurgence ofdengue and yellow fever [1], and a great number of themost important vector-borne human diseases have exhibiteddramatic changes in incidence and geographic range in recentdecades [11].
Vectors of human diseases are typically species ofmosquitoes that are able to transmit viruses, bacteria, or par-asites to humans and other warm-blooded hosts [14]. Amongthe mosquito-borne infections, arthropod-borne viruses

2 Computational and Mathematical Methods in Medicine
Table 1: Model variables and their biological meanings.
Variable Biological meaning𝑆𝐻
Susceptible humans density𝐿𝐻
Latent humans density𝐼𝐻
Infectious humans density𝑅𝐻
Recovered humans density𝑆𝑀
Uninfected mosquitoes density𝐿𝑀
Latent mosquitoes density𝐼𝑀
Infectious mosquitoes density𝑆𝐸
Uninfected eggs (imm. stages) density𝐼𝐸
Infected aquatic forms density
(arboviruses) comprise the largest class of vector-bornehuman pathogens with more than 500 arboviruses beingdescribed up to now, 20 percent of which causing humandiseases [6, 15, 16]. Examples of arboviruses include dengueand dengue haemorrhagic fever, yellow fever, Rift Valleyfever, West Nile virus, and Japanese encephalitis among [6,16, 17].
Approximately 80 percent of vector-borne disease trans-mission typically occurs among 20 percent of the hostpopulations [19, 20]. Thus, the overwhelming impact of thedistribution of vector-borne infections is disproportionatelyon tropical and subtropical countries [2]. Unfortunately, thisconsiderable economic, ecological, and public health impactof vector-borne infections is expected to continue, givenlimited capabilities for detecting, identifying, and addressinglikely epidemics [1].
This paper proposes a general model for vector-borneinfections which is flexible enough to comprise the dynamicsof some known diseases transmitted by arthropods. Fromequilibrium analysis, we determined the number of infectedvectors as an explicit function of the model’s parameters andthe prevalence of infection in the hosts. From the analysis, it isalso possible to derive the basic reproduction number and theequilibrium force of infection as a function of those param-eters and variables. From the force of infection, we were ableto conclude that, depending on the disease’s structure and themodel’s parameters, there is a maximum value of equilibriumprevalence for each mosquito-borne microparasitic infec-tions.This is important because of the following: (a) knowingthemaximum prevalence at equilibrium (neglecting seasonalvariations, see below), we can calculate the maximum forceof infection and, therefore, the maximum probability that avisitor gets the disease when visiting an endemic region; (b)the maximum force of infection can be immediately usedto calculate the maximum incidence of the disease (againneglecting seasonal variations) in an affected endemic region;(c) if a vector-borne disease is introduced in an unaffectedarea, we can predict the maximum prevalence at equilibriumfor the demographic and disease-related parameters in thatarea. This gives a very good idea of the amount of resourcesthat will be needed to care for these cases. This allows publichealth authorities to anticipate the (economic and social)importance of a given disease in order to increase publichealth preparedness to deal with such challenges.
The model we present in this paper is a deterministicmodel. However, as we will show, it is possible to introducesome elements of stochasticity.
The whole analysis is exemplified by the cases of malariaand dengue fever.
2. The Model
The model that is used to calculate the efficiency of controlstrategies can be found in [21–23].
The populations involved in the transmission are humanhosts, mosquitoes, and their eggs. For the purposes of thispaper, the term “eggs” also includes the intermediate stages,such as larvae and pupae. Therefore, the population densitiesare divided into the compartments described in Table 1.
We first write down themodel equations and then explainthe meanings of their terms. The model equations are
𝑑𝑆𝐻
𝑑𝑡= −𝑎𝑏𝐼
𝑀
𝑆𝐻
𝑁𝐻
− 𝜇𝐻𝑆𝐻+ 𝑟𝐻𝑁𝐻(1 −
𝑁𝐻
𝜅𝐻
)
+ 𝜎𝐻𝑅𝐻+ 𝜃𝐻𝐼𝐻,
𝑑𝐿𝐻
𝑑𝑡= 𝑎𝑏𝐼𝑀
𝑆𝐻
𝑁𝐻
− (𝜇𝐻+ 𝛿𝐻) 𝐿𝐻,
𝑑𝐼𝐻
𝑑𝑡= 𝛿𝐻𝐿𝐻− (𝜇𝐻+ 𝛼𝐻+ 𝛾𝐻+ 𝜃𝐻) 𝐼𝐻,
𝑑𝑅𝐻
𝑑𝑡= 𝛾𝐻𝐼𝐻− 𝜇𝐻𝑅𝐻− 𝜎𝐻𝑅𝐻,
𝑑𝑆𝑀
𝑑𝑡= 𝑝𝑐𝑆 (𝑡) 𝑆𝐸 − 𝜇𝑀𝑆𝑀 − 𝑎𝑐𝑆𝑀
𝐼𝐻
𝑁𝐻
,
𝑑𝐿𝑀
𝑑𝑡= 𝑎𝑐𝑆
𝑀
𝐼𝐻
𝑁𝐻
− 𝛾𝑀𝐿𝑀− 𝜇𝑀𝐿𝑀,
𝑑𝐼𝑀
𝑑𝑡= 𝛾𝑀𝐿𝑀− 𝜇𝑀𝐼𝑀+ 𝑝𝑐𝑆 (𝑡) 𝐼𝐸,
𝑑𝑆𝐸
𝑑𝑡= [𝑟𝑀𝑆𝑀+ (1 − 𝑔) 𝑟
𝑀(𝐼𝑀+ 𝐿𝑀)]
× (1 −(𝑆𝐸+ 𝐼𝐸)
𝜅𝐸
) − 𝜇𝐸𝑆𝐸− 𝑝𝑐𝑆 (𝑡) 𝑆𝐸,
𝑑𝐼𝐸
𝑑𝑡= [𝑔𝑟𝑀(𝐼𝑀+ 𝐿𝑀)] (1 −
(𝑆𝐸+ 𝐼𝐸)
𝜅𝐸
)
− 𝜇𝐸𝐼𝐸− 𝑝𝑐𝑆 (𝑡) 𝐼𝐸,
where
𝑁𝐻= 𝑆𝐻+ 𝐿𝐻+ 𝐼𝐻+ 𝑅𝐻,
𝑁𝑀= 𝑆𝑀+ 𝐿𝑀+ 𝐼𝑀,
𝑁𝐸= 𝑆𝐸+ 𝐼𝐸
(1)
and 𝑐𝑆(𝑡) = (𝑑
1− 𝑑2sin(2𝜋𝑓𝑡 + 𝜙)) is a factor mimicking
seasonal influences in the mosquito population [5, 24]. Theseasonal influence was considered in another paper [21]. In

Computational and Mathematical Methods in Medicine 3
Table 2: Model’s parameters and their biological significance.
Parameter Biological meaninga Average daily rate of biting (see text)b Fraction of bites actually infective to humans𝜎𝐻
Loss of immunity rate𝛿𝐻
Latency rate in humans𝜃𝐻
Loss of infectiousness in humans𝜇𝐻
Human natural mortality rate𝑟𝐻
Birth rate of humans𝜅𝐻
Carrying capacity of humans𝛼𝐻
Disease mortality in humans𝛾𝐻
Human recovery ratep Hatching rate of susceptible eggs𝛾𝑀
Latency rate in mosquitoes𝜇𝑀
Natural mortality rate of mosquitoes𝑟𝑀
Oviposition rateg Proportion of infected eggs𝜅𝐸
Carrying capacity of eggs𝜇𝐸
Natural mortality rate of eggsc Fraction of bites actually infective to mosquitoes𝑐𝑆
Climatic factor
this paper, however, as a first approximation, which is verygood in some tropical areas, 𝑐
𝑠(𝑡) = 𝑐
𝑠= constant.
Remark 1. As mentioned above, seasonal influence in themosquito population was not considered in this paper. Thereason for this is that including seasonal variation, thatis, considering 𝑐
𝑠(𝑡) = constant, implies additional analytical
difficulties (see, e.g., [25–27]). In most tropical regions, themosquito population varies very little along the year [28],and, therefore, this additional complication is unnecessary.Furthermore, at least for part of the year, the equilibriumis reached even when seasonality is important. Also, in thispaper, we want to make a comparison of the maximumprevalence attained at endemic equilibrium among variousvector-transmitted diseases. As explained in the Introduc-tion, endemic equilibrium is important to help public healthauthorities to plan and control such diseases and to bet-ter understand the enormous differences in prevalence ofdistinct vector-borne diseases like the observed equilibriumprevalence of malaria as compared to dengue.
The model’s parameters are described in Table 2.Let us explain the meaning and limitations of the above
model. First, as mentioned, the variables are densities, that is,number of humans/vectors per unit area.Therefore, to use themodel as it is written above, we should consider an areawherethe populations are approximately homogenously distributedand multiply each variable by this area. One particularimportant point is raised by the term 𝑎𝑏𝐼
𝑀(𝑆𝐻/𝑁𝐻).
Let us explain the meaning of this term. The parameter𝑎 is a composed quantity. Let 𝐴 be the area explored bya mosquito by the joint movement of the humans and themosquitoes. Let 𝜉 be the number of bites a mosquito inflicts
Table 3: Model’s structure as a function of the parameters.
Model’s structure 𝛿𝐻
𝛾𝐻
𝜎𝐻
𝜃𝐻
SI →∞ 0 0 0
SIS →∞ 0 0 =0SIR →∞ =0 0 0
SIRS →∞ =0 =0 0
SEIR =0 =0 0 0
SEIRS =0 =0 =0 0
per unit time and per unit area in the humans. Then, 𝜉𝐴𝐼𝑀is
the number of bites that 𝐴𝐼𝑀
infected mosquitoes inflict on𝑁𝐻𝐴 people. Hence, the fraction of bites given on susceptible
humans is 𝜉𝐴𝐼𝑀(𝑆𝐻𝐴/𝑁𝐻𝐴) = 𝑎𝐼
𝑀(𝑆𝐻/𝑁𝐻), where 𝑎 = 𝜉𝐴.
Therefore, the number of susceptible humans that getthe infection per unit time from infected mosquitoes is𝑎𝑏𝐼𝑀(𝑆𝐻/𝑁𝐻), where 𝑏 is the probability that a bite from an
infected mosquito results in an infected (latent) human.Analogously, the term 𝑎𝑐(𝐼
𝐻/𝑁𝐻)𝑆𝑀represents the den-
sity of new infections per unit time in mosquitoes due tomosquitoes’ bites on infective humans.
The term 𝑟𝐻𝑁𝐻(1−𝑁
𝐻/𝐾𝐻), where 𝑟
𝐻is the Malthusian
parameter and 𝐾𝐻
is the carrying capacity, represents thebirth rate per unit area. We assume that all the individualsare born susceptible.
The terms
[𝑟𝑀𝑆𝑀+ (1 − 𝑔) 𝑟
𝑀(𝐼𝑀+ 𝐿𝑀)] (1 −
(𝑆𝐸+ 𝐼𝐸)
𝜅𝐸
) ,
[𝑔𝑟𝑀(𝐼𝑀+ 𝐿𝑀)] (1 −
(𝑆𝐸+ 𝐼𝐸)
𝜅𝐸
)
(2)
represent the birth rate per unit area of susceptible andinfected eggs, respectively. Note that we assume that eggs canbe born infected, a phenomenon called vertical transmissionin the literature.
The term 𝑝𝑐𝑠(𝑡)𝑆𝐸represents the number of noninfected
eggs per unit time per unit area that reaches the adult stage.The parameter 𝑐
𝑠(𝑡)was introduced tomimic seasonality and,
asmentioned before, in this paper is made constant.The term𝑝𝑐𝑠(𝑡)𝐼𝐸represents the number of infected eggs per unit time
per unit area that reaches the infected adult stage.The other terms are transition terms between the com-
partments as explained, for example, in [22].Model (1) is a very general model for some known vector-
borne infections.Therefore, depending on the values of someparameters, the model can describe any type of dynamics inthe human subpopulation, such as that seen in Table 3.
The model can also include vaccination, for instance,against yellow fever or dengue, but this subject will not betreated in this work.
From system (1), it is possible to determine the equilib-rium densities of the variables of interest. We carried outdetailed equilibrium analysis in a related article [18]. For our

4 Computational and Mathematical Methods in Medicine
purposes, we calculate the equilibrium densities of 𝐼∗𝑀, the
number of infected mosquitoes:
𝐼∗
𝑀= (𝛿𝐻+ 𝜇𝐻) (𝜇𝐻+ 𝛾𝐻+ 𝛼𝐻+ 𝜎𝐻) 𝐼∗
𝐻
× (𝑎𝑏𝛿𝐻
×(1−((𝜇𝐻+𝜎𝐻)(𝜇𝐻+𝛾𝐻+𝛼𝐻+𝛿𝐻+𝜃𝐻)+𝛾𝐻𝛿𝐻
𝛿𝐻(𝜇𝐻+𝜎𝐻)
)
×𝐼∗
𝐻
𝑁∗
𝐻
))
−1
.
(3)
Replacing the values of 𝐼∗𝐻and𝑁∗
𝐻given in (3), it is possible
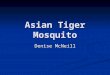
to see that 𝐼∗𝑀
increases with the biting rate 𝑎, as shown inFigure 1.
The expressions for 𝐼∗𝐻and 𝑁
∗
𝐻, in terms of the model’s
parameters, that appear in (3) are
𝐼∗
𝐻
𝑁∗
𝐻
=(𝛾𝑀+ 𝑔𝜇𝑀) 𝑎2𝑏𝑐 (𝑁
∗
𝑀/𝑁∗
𝐻)−𝑄 (𝜇
𝑀+ 𝛾𝑀) 𝜇𝑀(1 − 𝑔)
(𝛾𝑀+ 𝑔𝜇𝑀) 𝑎2𝑏𝑐𝛿
𝐻(𝑁∗
𝑀/𝑁∗
𝐻) 𝑍+𝑎𝑐𝑄 (𝜇
𝑀+𝛾𝑀)
,
(4)
which is the equilibrium prevalence of the infection inhumans and where
𝑄 = ((𝜇𝐻+ 𝜎𝐻) (𝜇𝐻+ 𝛾𝐻+ 𝛼𝐻+ 𝛿𝐻+ 𝜃𝐻) + 𝛾𝐻𝛿𝐻
𝛿𝐻(𝜇𝐻+ 𝜎𝐻)
) ,
𝑍 = [((𝛿𝐻+ 𝜇𝐻) (𝜇𝐻+ 𝛾𝐻+ 𝛼𝐻+ 𝜎𝐻))
𝛿𝐻
] ,
𝑁∗
𝑀=𝑝𝑐𝑆
𝜇𝑀
𝜅𝐸[1 −
(𝜇𝑀) (𝜇𝐸+ 𝑝𝑐𝑆)
𝑟𝑀𝑝𝑐𝑆
] .
(5)
The calculation of the total human population expressionat equilibrium, 𝑁∗
𝐻, is slightly more complicated and results
in
𝑁∗
𝐻=−𝐵 + √𝐵2 − 4𝐴𝐶
2𝐴, (6)
where
𝐴 = 𝑎𝑐𝑟𝐻Ω,
𝐵 = −𝑎𝑐Ω𝜅𝐻(𝑟𝐻− 𝜇𝐻) + Γ𝑍𝑟
𝐻− Ω𝜇𝑀(1 − 𝑔) 𝛼
𝐻𝜅𝐻,
𝐶 = −Γ𝜅𝐻(𝑟𝐻− 𝜇𝐻) 𝑍 + Γ𝛼
𝐻𝜅𝐻,
Ω = 𝑄 (𝛾𝑀+ 𝜇𝑀) ,
Γ = (𝛾𝑀+ 𝑔𝜇𝑀) 𝑎2𝑏𝑐𝛿𝐻𝑁∗
𝑀.
(7)
From (4), it is possible to deduce the expression of thebasic reproduction number of model (1) as [22, 29, 30]
𝑅0= (𝛾𝑀+ 𝑔𝜇𝑀) 𝑎2𝑏𝑐𝑁𝑀 (0)
𝑁𝐻 (0)
× ((𝜇𝐻+ 𝜎𝐻) (𝜇𝐻+ 𝛾𝐻+ 𝛼𝐻+ 𝛿𝐻+ 𝜃𝐻) + 𝛾𝐻𝛿𝐻
𝛿𝐻(𝜇𝐻+ 𝜎𝐻)
× (𝜇𝑀+ 𝛾𝑀) 𝜇𝑀(1 − 𝑔))
−1
,
(8)
where 𝑁𝑀(0) and 𝑁
𝐻(0) are the population of vectors and
hosts calculated in the absence of the infection.Figure 1 is a plot of (3) as a function of the biting rate, 𝑎,
calculated in two ways: in the red dotted line the number ofinfected vectors is calculated with the host prevalence 𝐼∗
𝐻/𝑁∗
𝐻
directly derived from the dynamics of system (1); in the bluedashed line 𝐼∗
𝐻/𝑁∗
𝐻is calculated from (4) and for 𝑎 such that
𝑅0can be less than one and, therefore, 𝐼∗
𝐻/𝑁∗
𝐻< 0.
Note that, as expected, the number of infected vectors isa monotonically increasing function of the biting rate.
The force of infection (the incidence density rate) forhumans at the equilibrium, 𝜆∗
𝐻, is defined as
𝜆∗
𝐻= 𝑎𝑏
𝐼∗
𝑀
𝑁∗
𝐻
, (9)
which can be explicitly written in terms of the equilibriumprevalence of the infection in humans (3) as
𝜆∗
𝐻= (𝛿𝐻+ 𝜇𝐻) (𝜇𝐻+ 𝛾𝐻+ 𝛼𝐻+ 𝜎𝐻)𝐼∗
𝐻
𝑁∗
𝐻
× (𝛿𝐻× (1
−((𝜇𝐻+𝜎𝐻) (𝜇𝐻+𝛾𝐻+𝛼𝐻+𝛿𝐻+𝜃𝐻)+𝛾𝐻𝛿𝐻
𝛿𝐻(𝜇𝐻+ 𝜎𝐻)
)
×𝐼∗
𝐻
𝑁∗
𝐻
))
−1
.
(10)
From (10), it can be seen that the equilibrium prevalence ofinfection among humans, 𝐼∗
𝐻/𝑁∗
𝐻, is less than a certain value:
(𝐼∗
𝐻
𝑁∗
𝐻
)
<𝛿𝐻(𝜇𝐻+𝜎𝐻)
(𝜇𝐻+𝜎𝐻) (𝜇𝐻+ 𝛾𝐻+𝛼𝐻+𝛿𝐻+𝜃𝐻)+𝛾𝐻𝛿𝐻
.
(11)
Hence, depending on the disease, the model’s structurewill determine whether the maximum equilibrium preva-lence
(𝐼∗
𝐻
𝑁∗
𝐻
)
MAX=
𝛿𝐻(𝜇𝐻+𝜎𝐻)
(𝜇𝐻+𝜎𝐻) (𝜇𝐻+𝛾𝐻+𝛼𝐻+𝛿𝐻+𝜃𝐻)+𝛾𝐻𝛿𝐻
(12)

Computational and Mathematical Methods in Medicine 5
300000
200000
100000
0
0.10 0.15 0.20 0.25 0.30 0.35 0.40Biting rate
Equi
libriu
m n
umbe
r of i
nfec
ted
vect
ors
Figure 1: Plot of 𝐼∗𝑀(3) as a function of the biting rate, 𝑎, calculated
in two ways: (a) the red dotted line shows the number of infectedvectors calculated with the host prevalence 𝐼∗
𝐻/𝑁∗
𝐻directly derived
from the numerical solution of the dynamics of system (1); (b) theblue dashed line shows the number of infected vectors calculatedwith the host prevalence 𝐼∗
𝐻/𝑁∗
𝐻derived from (4). For 𝑎 such that
𝑅0is less than one, we have 𝐼∗
𝐻/𝑁∗
𝐻< 0. For 𝑎 such that 𝑅
0is greater
than one, the two curves coincide.
is large or small. For instance, in a SEIRmodel such as dengue,where the recovery rate, 𝛾
𝐻, is large relatively to the human
mortality rate, 𝜇𝐻, the maximum equilibrium prevalence of
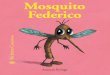
the infection in humans is very low. Figure 2 exemplifiessome theoretical vector-borne infections and theirmaximumequilibrium prevalence in humans as a function of therecovery rate, 𝛾
𝐻, and the rate of loss of immune protection,
𝜎𝐻.Let us illustrate the theory above by comparing two very
distinct vector-borne infections, namely,malaria and dengue.In Table 4 we show the typical values of the key parametersthat determine the maximum equilibrium prevalence forboth malaria and dengue, as in (11).
By applying the parameters’ values above to (12) we endupwithmaximumequilibriumprevalences of 31% formalariaand 0.02% for dengue, which are in accord with typicalprevalences found in endemic places for both diseases. Asummary of the sensitivity analysis of the model is presentedin the Appendix. This sensitivity analysis was carried out onthe parameters that are related to dengue control.
Finally, a comment on an important aspect of (8) forthe basic reproduction number, 𝑅
0. This expression has a
discontinuity when 𝑔 = 1; that is, when 100% of theeggs are laid infected. This is a theoretical possibility andwhen 𝑔 → 1, there is a structural change in our model.The populations of susceptible and infected eggs becomecompletely decoupled. It can be verified that the disease isable to sustain itself even without human hosts. As a matterof fact, as previously demonstrated [31], this is the only waythe infection circulates exclusively among vectors without thehosts.
In addition, when 𝑔 = 1 and the human hosts areintroduced into the system, then since all the eggs of infected
0.2
0.18
0.16
0.14
0.12
0.1
0.08
0.06
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0.02
0.04
00 0.05
0.1
0.1 0.15 0.2
Prevalence upper bound1
Humans recovery rate, 𝛾H (days−1)
Loss
of p
rote
ctio
n ra
te,𝜎
H(d
ays−1)
Figure 2: Some theoretical vector-borne infections and their max-imum equilibrium prevalences in humans as a function of therecovery rate, 𝛾
𝐻, and the rate of loss of immune protection, 𝜎
𝐻.The
values of the other parameters are: 𝜇𝐻= 4.57×10
−5 days−1, 𝛿𝐻= 0.1
days−1, 𝛼𝐻= 0.01 days−1, and 𝜃
𝐻= 0.
mosquitoes are infected, the time evolution leads to a sit-uation where all mosquitoes are infected. Therefore, when𝑔 = 1 and human hosts are introduced, the population ofsusceptible mosquitoes and eggs goes to zero. In any case,there is no known infection that is 100% transmitted tomosquitoes’ eggs.
3. Discussion
Since the seminal work byRonaldRoss,mathematicalmodelshave provided a great deal of theoretical support for under-standing the complex dynamics of vector-borne infections,in addition to the important role those models have played indesigning and assessing control strategies [32]. Key conceptslike the basic reproduction number, vectorial capacity andthe force of infection derived from the theoretical works onvector-borne infections are currently central to the quantifi-cation of transmission, as well as to the proposal of publichealth measures to control them [22].
In this work, we propose a general, although very sketchy,model that considers a great deal of the aspects related tothe dynamics of mosquito-borne microparasites. From theequilibrium analysis, we calculated the prevalence of theinfection in the host populations, from which the numberof infected vectors was deduced. In addition, we deducedan explicit expression for the basic reproduction numberand the equilibrium force of infection. It was possible thento demonstrate that, provided an equilibrium is reached,each mosquito-borne microparasite has a maximum hostprevalence, depending on the disease’s structure and on thevalue of the parameters. This analysis was exemplified bythe calculation of the maximum equilibrium prevalence of

6 Computational and Mathematical Methods in Medicine
Table 4: Parameters’ values that determine the maximum equilib-rium prevalences of Malaria and Dengue.
Parameter Malaria Dengue𝜎𝐻
0.10 days−1 0.00 days−1
𝛿𝐻
0.07 days−1 0.14 days−1
𝜃𝐻
0.00 days−1 0.00 days−1
𝜇𝐻
4.57 × 10−5 days−1 4.57 × 10
−5 days−1
𝛼𝐻
10−3 days−1 10−5 days−1
𝛾𝐻
0.14 days−1 0.20 days−1
malaria and dengue. Once the disease’s structure is deter-mined and the values of the parameters are known, it ispossible to calculate the maximum equilibrium prevalence ofa mosquito-borne microparasitic infection.
It may be argued that malaria is not exactly a good exam-ple of a microparasitic infection. However, although malariacan behave sometimes as a microparasite and sometimes asa macroparasite [33], in the specific context of the proposedmodel, it can be considered as a microparasitic disease.
Another important limitation of our approach is that, inorder to calculate the equilibrium densities of each of themodel’s variables, we have to neglect seasonal fluctuations,which can be very important in the transmission dynamicsof such infections like dengue. However, seasonality in sometropical areas is not too important and the results can beapplied to the average trend in prevalence levels.
At first inspection, (3) may seem odd because the bitingrate appears in the denominator and the number of infectedmosquitoes should be directly proportional to that rate.However, if we write (3) as a function of the parametersonly, that is, by writing the human prevalence term 𝐼
∗
𝐻/𝑁∗
𝐻as
an explicit function of the model’s parameters, it is possibleto see that the number of infected mosquitoes is indeed amonotonically growing function of the biting rate, as shownin Figure 1. We do not show this full equation because it isawkwardly big.
The calculation of a maximum value of equilibriumprevalence for a mosquito-borne microparasitic infectionmay help public health authorities to estimate the resourcesneeded to care for the infected individuals, anticipating theimportance of the disease and increasing the public healthpreparedness to deal with such a challenge.
Appendix
Sensitivity Analysis to Some ParametersRelated to Control
In this appendix, we present a summary of the sensitivityanalysis (explored in detail in [18]) of the equilibrium resultsto some parameters related to control for the case of dengue.The analyzed variables are the basic reproductive number, theforce of infection (incidence density), and prevalence. Theparameters are the biting rate, 𝑎; the immature stages carryingcapacity, 𝜅
𝐸; the mortality rate of the larvae, 𝜇
𝐸; and the
mosquitomortality rate, 𝜇𝑀.These parameters correspond to
Table 5: Results of the sensitivity analysis. The results represent therelative amount of variation (expressed in percentual variation) inthe variable if we vary the parameters by 1% (see [18] for details).
Parameter MeanSensitivity of 𝑅
0to the control parameters
𝑎 1.94𝜅𝐸
0.69𝜇𝐸
(−) 8.28 × 10−4
𝜇𝑀
(−) 2.42Sensitivity of 𝜆 to the control parameters
𝑎 5.02𝜅𝐸
2.32𝜇𝐸
(−) 1.93 × 10−3
𝜇𝑀
(−) 5.40Sensitivity of 𝐼
𝐻/𝑁𝐻to the control parameters
𝑎 2.67𝜅𝐸
1.34𝜇𝐸
(−) 2.31 × 10−2
𝜇𝑀
(−) 3.20
the actual control strategies available. The results are shownin Table 5.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
Acknowledgments
The research from which these results were obtained hasreceived funding from the European Union’s Seventh Frame-work Programme (FP7/2007–2013) under Grant agreementno. 282589, from LIM01 HCFMUSP and CNPq. The fundershad no role in study design, data collection and analysis,decision to publish, or preparation of the paper.
References
[1] S. M. Lemon, P. F. Sparling, and M. A. Hamburg, Vector-BorneDiseases: Understanding the Environmental, Human Health,and Ecological Connections, The National Academies Press,Washington, DC, USA, 2008.
[2] CIESIN (Center for International Earth Science InformationNetwork), “Changes in the incidence of vector-borne diseasesattributable to climate change,” 2012, http://www.ciesin.colum-bia.edu/TG/HH/veclev2.html.
[3] WHO (World Health Organization), “Global strategicframework for integrated vector management,” 2004, http://www.emro.who.int/rbm/PDF/GlobalStratFrameIVM.pdf.
[4] A. Wilder-Smith, K. E. Renhorn, H. Tissera et al., “Dengue-Tools: innovative tools and strategies for the surveillance andcontrol of dengue,”GlobalHealthAction, vol. 5, Article ID 17273,2012.

Computational and Mathematical Methods in Medicine 7
[5] E. Massad, F. A. B. Coutinho, L. F. Lopez, and D. R. DaSilva, “Modeling the impact of global warming on vector-borneinfections,”Physics of Life Reviews, vol. 8, no. 2, pp. 169–199, 2011.
[6] D. J. Gubler, “Resurgent vector-borne diseases as a global healthproblem,” Emerging Infectious Diseases, vol. 4, no. 3, pp. 442–450, 1998.
[7] D. J. Gubler, “Aedes aegyptiand Aedes aegypti-borne diseasecontrol in the 1990s: top down or bottom up. Charles FranklinCraig Lecture,” American Journal of Tropical Medicine andHygiene, vol. 40, no. 6, pp. 571–578, 1989.
[8] D. J. Gubler, “The changing epidemiology of yellow fever anddengue, 1900 to 2003: full circle?” Comparative Immunology,Microbiology and Infectious Diseases, vol. 27, no. 5, pp. 319–330,2004.
[9] D. J. Gubler andM. L.Wilson, “The global resurgence of vector-borne diseases: lessons learned from successful and failedadaptation,” in KIntegration of Public Health with Adaptationto Climate Change: Lessons Learned and New Directions, K. L.Ebi, J. Smith, and I. Burton, Eds., pp. 44–59, Taylor and Francis,London, UK, 2005.
[10] IOM (Institute of Medicine), Emerging Infections: MicrobialThreats to Health in the United States, The National AcademiesPress, Washington, DC, USA, 1992.
[11] D. J. Gubler, “The global emergence/resurgence of arboviral dis-eases as public health problems,” Archives of Medical Research,vol. 33, no. 4, pp. 330–342, 2002.
[12] K. Karunamoorthi, “Global malaria burden: socialomics impli-cations,” Journal of Socialomics, vol. 1, article e108, 2012.
[13] C. J. L. Murray, L. C. Rosenfeld, S. S. Lim et al., “Global malariamortality between 1980 and 2010: a systematic analysis,” TheLancet, vol. 379, no. 9814, pp. 413–431, 2012.
[14] O. P. Forattini, I. Kakitani, E. Massad, and D. Marucci, “Studieson mosquitoes (Diptera: Culicidae) and anthropic environ-ment. 2. Immature stages research at a rice irrigation systemlocation in south-eastern Brazil,” Revista de Saude Publica, vol.27, no. 4, pp. 227–236, 1993.
[15] S. M. Gray and N. Banerjee, “Mechanisms of arthropodtransmission of plant and animal viruses,” Microbiology andMolecular Biology Reviews, vol. 63, no. 1, pp. 128–148, 1999.
[16] WHO (World Health Organization), “Vector-borne viral infec-tions,” in State of the Art Vaccine Research and Develop-ment, 2005, http://www.who.int/vaccine research/documents/Vector Borne Viral Infection.pdf.
[17] CDC (Centers for Diseases Control), “Information of arbovi-ral encephalitis,” 2005, http://www.cdc.gov/ncidod/dvbid/arbor/arbdet.htm.
[18] M. Amaku, F. A. B. Coutinho, S. M. Raimundo, L. F. Lopez,M. N. Burattini, and E. Massad, “A comparative analysis ofthe relative efficacy ofvector-control strategies against denguefever,” http://arxiv.org/abs/1302.1166.
[19] D. L. Smith, J. Dushoff, R. W. Snow, and S. I. Hay, “Theentomological inoculation rate and Plasmodium falciparuminfection in African children,” Nature, vol. 438, no. 7067, pp.492–495, 2005.
[20] M. E. J. Woolhouse, C. Dye, J.-F. Etard et al., “Heterogeneitiesin the transmission of infectious agents: implications forthe design of control programs,” Proceedings of the NationalAcademy of Sciences of the United States of America, vol. 94, no.1, pp. 338–342, 1997.
[21] F. A. B. Coutinho, M. N. Burattini, L. F. Lopez, and E. Massad,“Threshold conditions for a non-autonomous epidemic system
describing the population dynamics of dengue,” Bulletin ofMathematical Biology, vol. 68, pp. 2263–2282, 2006.
[22] L. F. Lopez, F. A. B. Coutinho, M. N. Burattini, and E. Massad,“An approximate threshold condition for non-autonomoussystem: an application to a vector-borne infection,”Mathematicsand Computers in Simulation, vol. 70, no. 3, pp. 149–158, 2005.
[23] F. A. B. Coutinho, M. N. Burattini, L. F. Lopez, and E. Massad,“An approximate threshold condition for non-autonomoussystem: an application to a vector-borne infection,”Mathematicsand Computers in Simulation, vol. 70, no. 3, pp. 149–158, 2005.
[24] M. N. Burattini, M. Chen, A. Chow et al., “Modelling thecontrol strategies against dengue in Singapore,” Epidemiologyand Infection, vol. 136, no. 3, pp. 309–319, 2008.
[25] L. M. Wahl and M. A. Nowak, “Adherence and drug resistance:Predictions for therapy outcome,” Proceedings of the RoyalSociety B: Biological Sciences, vol. 267, no. 1445, pp. 835–843,2000.
[26] N. Bacaer and S. Guernaoui, “The epidemic threshold ofvector-borne diseases with seasonality: the case of cutaneousleishmaniasis in Chichaoua, Morocco,” Journal of MathematicalBiology, vol. 53, no. 3, pp. 421–436, 2006.
[27] W. Wang and X.-Q. Zhao, “Threshold dynamics for compart-mental epidemic models in periodic environments,” Journal ofDynamics and Differential Equations, vol. 20, no. 3, pp. 699–717,2008.
[28] R. A. Erickson, S. M. Presley, L. J. S. Allen, K. R. Long, and S. B.Cox, “A dengue model with a dynamic Aedes albopictus vectorpopulation,” Ecological Modelling, vol. 221, no. 24, pp. 2899–2908, 2010.
[29] G. MacDonald, “The analysis of equilibrium in malaria,” Tropi-cal Diseases Bulletin, vol. 49, no. 9, pp. 813–829, 1952.
[30] E. Massad, F. A. B. Coutinho, H. M. Y. Hyan Mo Yang, H.B. De Carvalho, F. Mesquita, and M. N. Burattini, “The basicreproduction ratio of HIV among intravenous drug users,”Mathematical Biosciences, vol. 123, no. 2, pp. 227–247, 1994.
[31] B. Adams and M. Boots, “How important is vertical transmis-sion in mosquitoes for the persistence of dengue? Insights froma mathematical model,” Epidemics, vol. 2, no. 1, pp. 1–10, 2010.
[32] E. Massad and F. A. B. Coutinho, “Vectorial capacity, basicreproduction number, force of infection and all that: formalnotation to complete and adjust their classical concepts andequations,” Memorias do Instituto Oswaldo Cruz, vol. 107, pp.564–567, 2012.
[33] R. M. Anderson and R. M. May, Infectious Diseases in Humans:Dynamics and Control, Oxford University Press, Oxford, UK,1991.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttp://www.hindawi.com
Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Parkinson’s DiseaseHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com