Embed Size (px)
Citation preview

Research in vulnerable groups and target
populations : What works?
Linda-Gail BekkerThe Desmond Tutu HIV Centre
UCT, Cape Town.
2009

AFRICAASIA
E EUROPESOUTHERN AFRICA
IVDU CSW MSM PRISONERS
CONCENTRATED EPIDEMICS
GENERALISED EPIDEMICSHYPERENDEMIC
OTHER
LOW LEVEL EPIDEMICS

Low level scenario
CA
Total population
A: Most at risk –higher rates and risk of HIV
C : People living with HIV diagnosed and undiagnosed
Turkey General risk diffuse and
low level <0.2%Very recent infection.

Concentrated scenarios
C
A
Total population
A: Most at risk –higher rates and risk of HIV
C : People living with HIV diagnosed and undiagnosed
Buenos Aires, ArgentinaMSM : 15%CSW : >5%
Maintained in subpopulationNo spillage to general
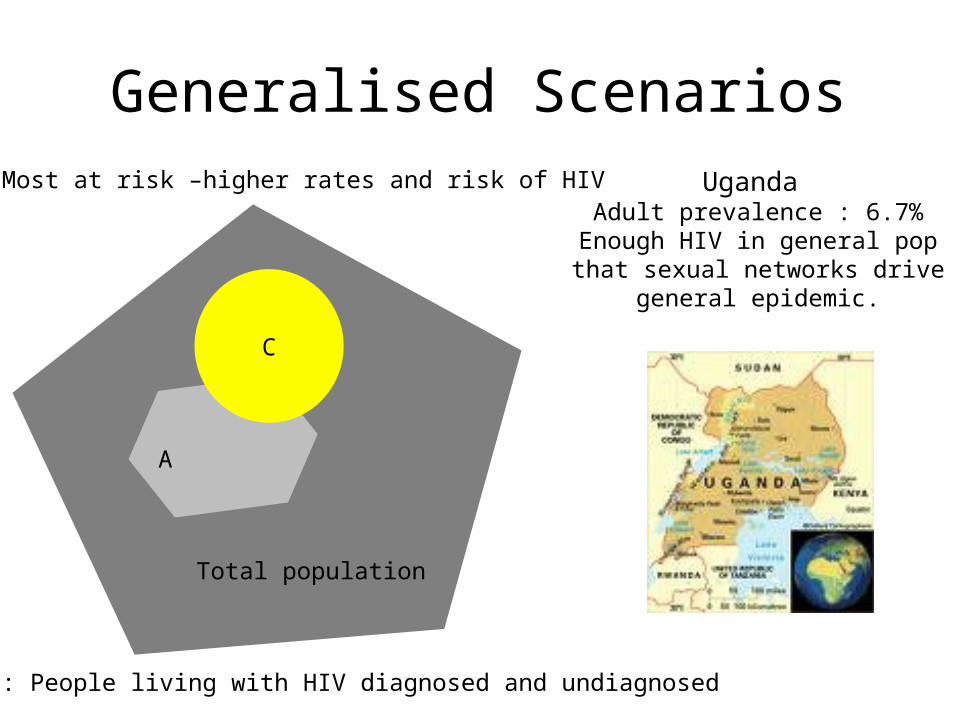
Generalised Scenarios
C
A
Total population
A: Most at risk –higher rates and risk of HIV
C : People living with HIV diagnosed and undiagnosed
Uganda Adult prevalence : 6.7%
Enough HIV in general pop that sexual networks drive general
epidemic.
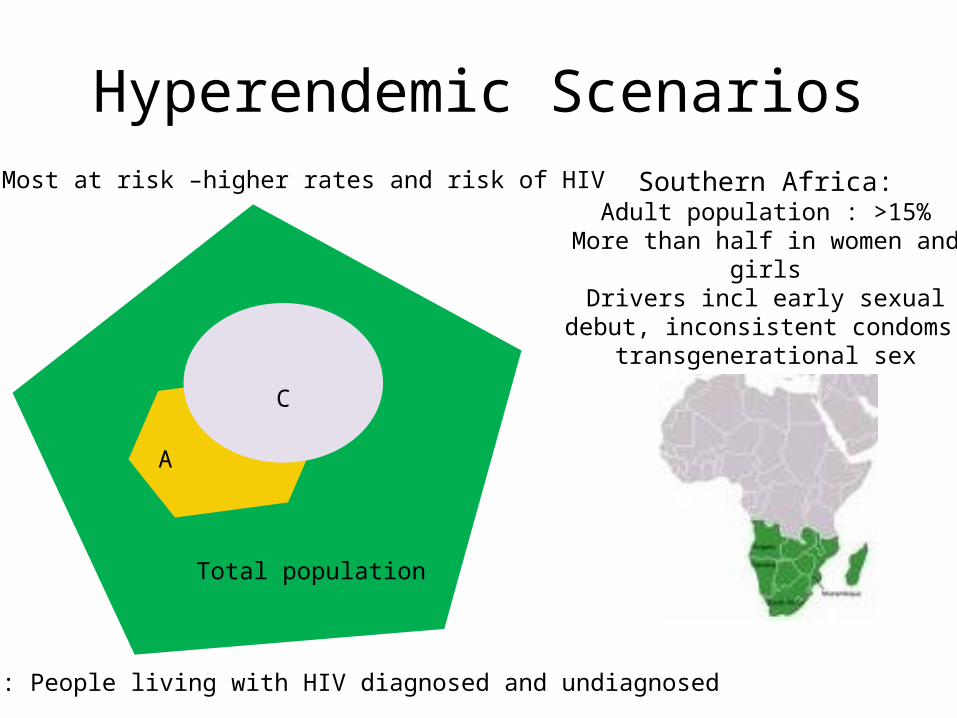
Hyperendemic Scenarios
C
A
Total population
A: Most at risk –higher rates and risk of HIV
C : People living with HIV diagnosed and undiagnosed
Southern Africa:Adult population : >15%
More than half in women and girlsDrivers incl early sexual debut,
inconsistent condoms, transgenerational sex
Concentrated Epidemics
IVDU: Most effective way to transmit HIV

IVDU globally
• 13 M IVDU worldwide
• 80% of all HIV in E Europe and Asia
• 1/3 of all infections outside SSA
• 5% prevention efforts
• New epidemics in SSA…….
(Unaids 2005)
IVDU in Africa
• Assessment of heroin use in Kenya
• Up to 15% substance users had moved from ‘chasing the dragon’ to injecting.
• Needle sharing• 1 needle/syringe
used for 1-3 days(Beckeleg 2004)
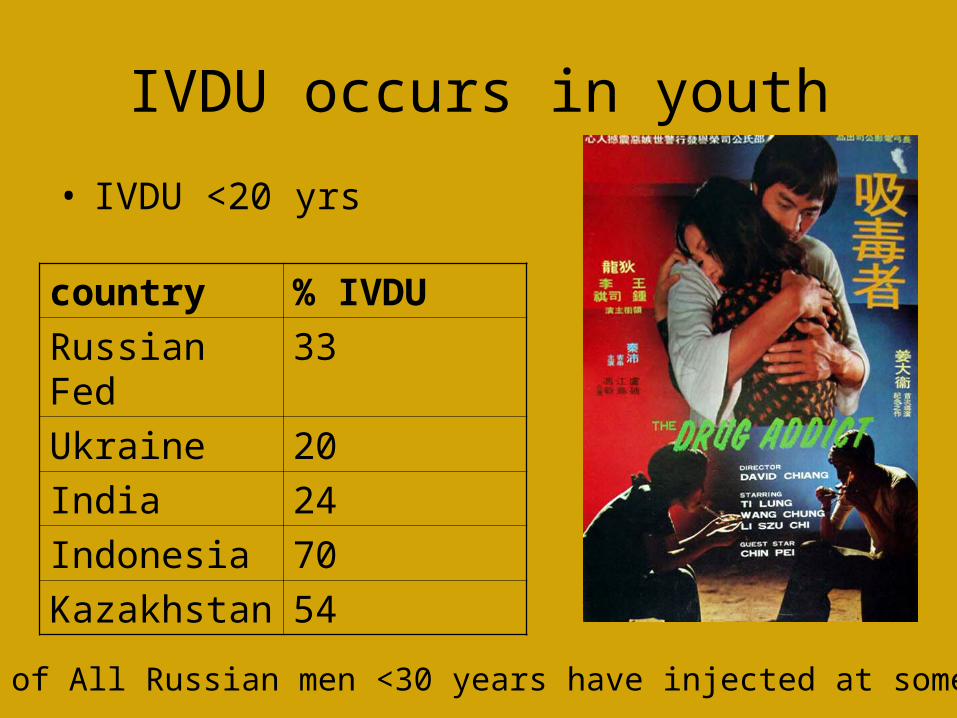
IVDU occurs in youth
• IVDU <20 yrs
country % IVDU
Russian Fed 33
Ukraine 20
India 24
Indonesia 70
Kazakhstan 54
1.5-8% of All Russian men <30 years have injected at some time

IVDU Youth (<24) are HIV infected:
Country% HIV
infected
Russia 55
Brazil 56
Central Asia 48
E Europe 40
Belarus 60
•(WHO 2006)

Young IVDU at risk for HIV:
• Contaminated eqpt accounts for >80% cases in Europe and Asia
• More likely to share needles
• More likely to inject in groups
• More likely to have increased sexual risks.
• Poor HIV Knowledge– Karachi : 1:4 never heard of
AIDS. • (WHO 2006)
• A drug user who shares needles is certain to contract Aids,"
"Its not a question of if, but when.“Director of Asia Harm Reduction, Tom Smits.

Concentrated Epidemics
Commercial sex work:More sex, more partners, more risk

Higher HIV prevalence in CSW
Country CSW General population
Myanmar 27% 1.8%
Ghana 40% 3%
Ecuador 11% 0.3%
73% in Ethiopia, 68% in Zambia, 50% in South Africa
Global prevention efforts: 16% •(WHO 2006)

Majority CSW are <25 years
• Cambodia• China• Lao People Democratic Republic• Myanmar• Russian Federation• Viet Nam
70-80%
In Thailand as many as 35 000 < 18 year old women engaged in sex trade.
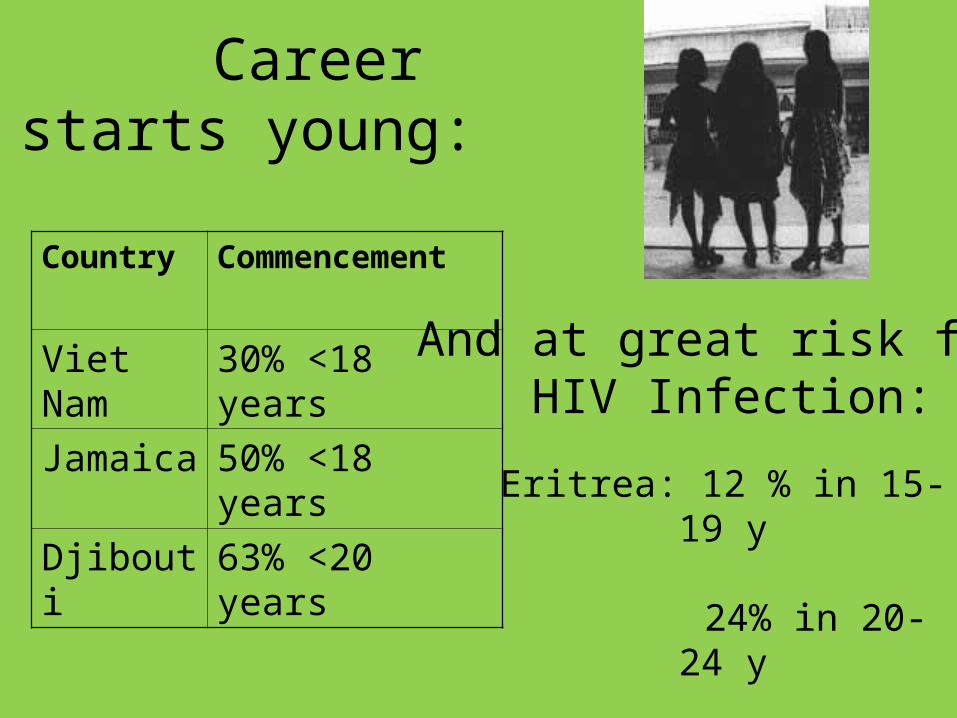
Career starts young:
Country Commencement
Viet Nam 30% <18 years
Jamaica 50% <18 years
Djibouti 63% <20 yearsEritrea: 12 % in 15-19 y
24% in 20-24 y
Myanmar: 41% in 15-19 y
And at great risk for HIV Infection:

Young, ill informedand often criminalized
Ave age CSW : 22.3 yrs
Primary school education level
Only 1:3 interviewed knew they were at HIV risk
None knew where to access HIV/STI services
SSA Truck route study in 2003:
(Omondi.et al 2003)
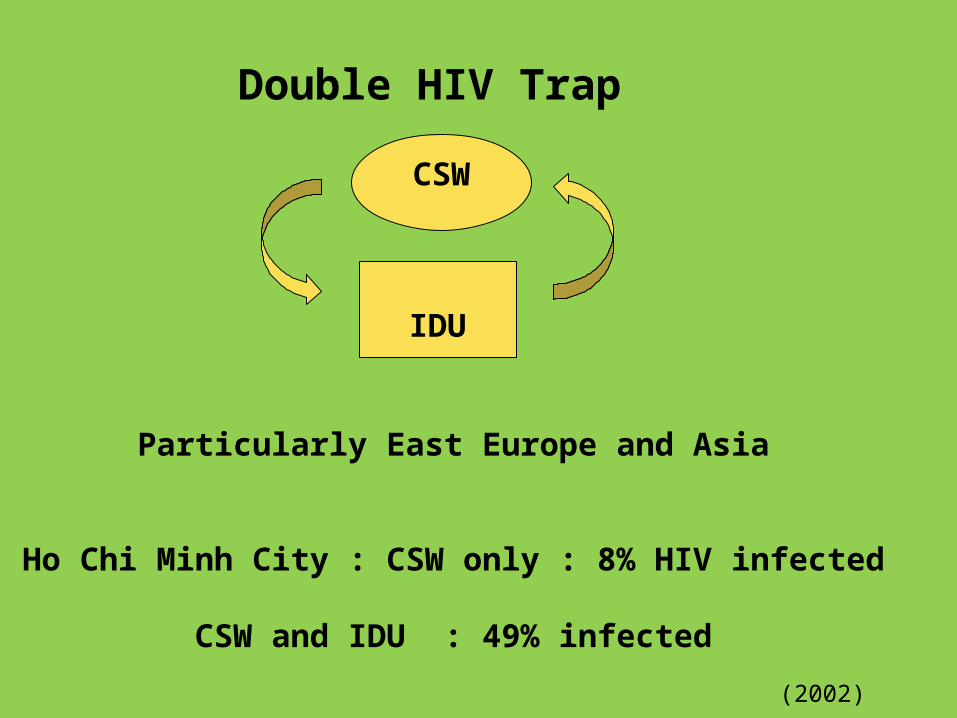
Double HIV Trap
IDU
CSW
Particularly East Europe and Asia
Ho Chi Minh City : CSW only : 8% HIV infected
CSW and IDU : 49% infected
(2002)

Clients of CSW often are youth
• India/Nepal: up to 70% are 20-24 years
• Kosovo : 18% are <20 years 20% are 20-24 years
•(WHO 2006)

Mobile populations
• Voluntary/job related- CSW, Transport industry• Legally required - military• Coerced- refugees, trafficking.• Urbanisation also an important driver• In Thailand 15-19 year olds : most refugees• 5000 youth daily become refugees.
•(WHO 2006)

Concentrated Epidemics
Men who have Sex with Men:
Unprotected anal sex = increased HIV risk
A social and behavioural phenomenon

MSM at higher risk of HIV…
Country MSM prev
Gen pop prev
Argentina 14 % < 1%
El Salvador
18 % < 1%
Global prevention efforts : 11%< 1 : 20 of MSM receive care or prevention
Lack of information and perception of risk…
• Beijing 2004 study: • 482 MSM interviewed, 28% bisexual• Only 15 % perceived any risk• 49% had had unprotected anal sex • <25% had accessed condoms or
lubricants in last 2 years.(Gibson, etal 2004)
MSM, third gendered and
transgendered:• Often invisible in many countries• Poor data due to covert nature• Cape Town: preliminary data in
MCMHP• Studies in Soweto• Studies in Johannesburg and Durban

Criminalization of MSMand homophobia
• MSM relations :• 14 year penal
sentence in Malawi (Goyer 2003)
• Drives MSM underground
• Less able to access information and services
Young men in Ghana are harrassed by the police and often assaulted.
Jailed in Jamaica

MSM are often young….
• Central America: 34% are < 24 yrs• Peru: 50% are < 25 yrs
Young MSM are more at risk….• Central Asia:
• E Europe:
• W Europe : 10 % HIV in 15-24 yr
14-20 % HIV in 15-24 yr
More likely to take risks: ‘bare backing’, crystal meth usage, etcJ. Elford, Current Opinion in Infectious Diseases 2006, 19:26–32
Sexual debut in MSM younger:
• Cambodia 17.7yrs in MSM vs 22yrs
More male CSWs are youth:
• Russia: 40% of male CSW are <19 yrs
Concentrated Epidemics
Prisoners:
The first three groups often supply this groupand the revolving door connects back to society
“The Degree of Civilisation in Society can be judged by entering its prisons.”
(Dostoevsky)

Incubators of contagion
• 9 M in prison at any time• 30M moving back and forth at any time.• HIV, Hep C, TB. (OSI 2004)
• South African prisons estim: 41% HIV prev• Russia Fed: prisoners >4x higher rate in
men and 15X rate in females.• IVDU without needles, MSM without
condoms, Tattooing without sterilty.• Little information and no services.
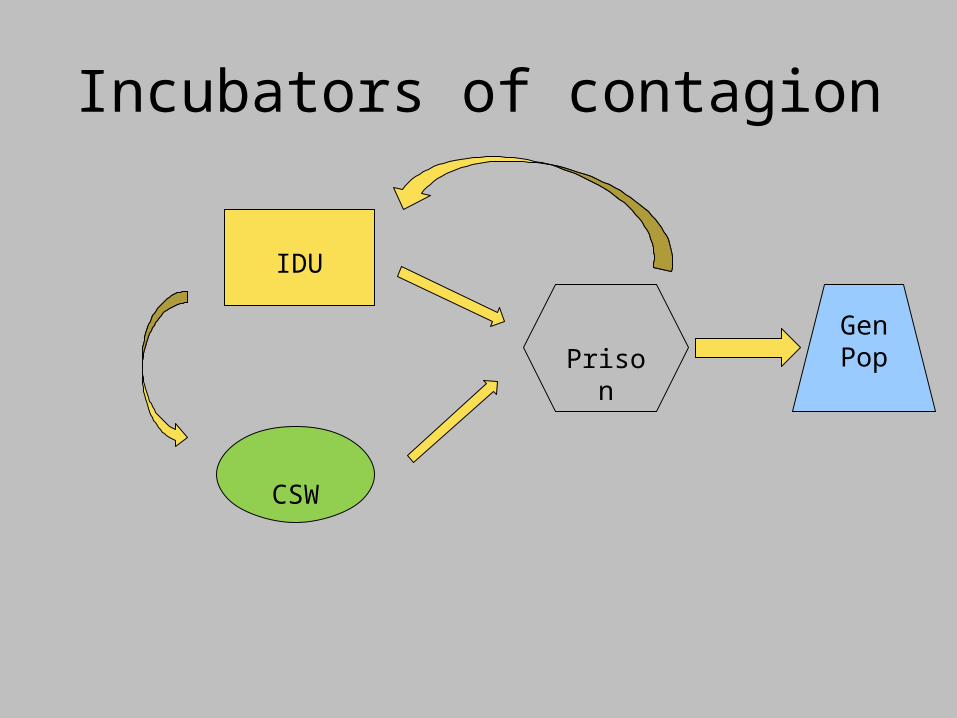
Incubators of contagion
IDU
CSW
PrisonGenPop
Young at risk with no rights
• Russian Fed: CSW in juvenile detention
• 58% had at least 1 bacterial STI• 4% HIV infected. • No access to information• Very little services. (Shakarishvili et al.,2005)
Important other groups
• Disintegration of family units – orphans
• Migratory populations• Victims of conflict and war• Uniformed services• Youth on the street• Pregnant women and girls

Spill over into generalized epidemics
• Young IVDU likely to be sexually active – Less likely to use condoms (Tran, et al 2004)
• Young IVDU likely to engage in CSW and vice versa.– More likely to be HIV infected.(UNAIDS 2006)
• Young MSM likely be having concurrent sexual relations with women.
• Prisoners move back into general population.

“Today’s generation of young people is the largest in human history”
UNFPA, 2005©UNICEF/HQ00-0779/Donna Descare

1,773 billion
people are between the ages of 10 and 24 years
Source: Population Reference Bureau, 2006
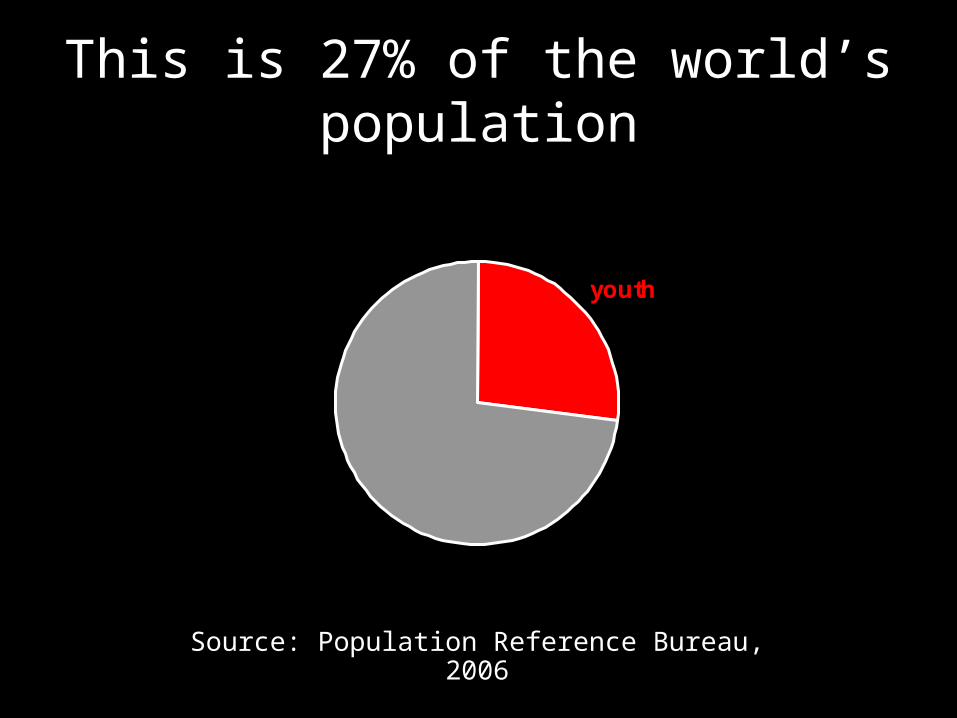
This is 27% of the world’s population
youth
Source: Population Reference Bureau, 2006

11-year-old Thai girl prepares her ARV meds © 2004 Joanne Wong
Half of all new infections occur in youth (age 10 – 24)
Every day, 7000 youth (age 10 – 24) become infected
1 infection every 14 secs
Source: WHO, 2006

10 million youth
living with HIV
Kicosehp NGO (support group for people living with HIV/AIDS). Kenya, Africa. © UNAIDS/G. Pirozzi
SOURCE: UNICEF/UNAIDS, 2004; youth age 15 - 24

Positive Youth63% of HIV positive
youth live in sub-Saharan Africa
sub-SaharanAfrica
S and SE Asia
E Europe andCentral Asia
Latin America
E Asia andPacific
North Africaand MiddleEastCaribbean
Industrializedcountries
SOURCE: UNICEF/UNAIDS, 2004; youth age 15 – 24

Disproportionate impact on young girls
2.4 million young boys living with HIV
SOURCE: UNICEF/UNAIDS, 2004; young boys/ girls age 15 - 24
7.6 million young girls living with HIV


Research in vulnerable populations
• EXPLOITATION vs BENEFIT??
• Often hardest hit• Important to include in research• Often hardest to reach• Need the most human subject
protection• Benefit of being researched?

Challenges:
• Ethico-legal• Representivity• Recruitment• Retention• Data collection

Challenges (and Solutions) in Recruiting MSM

MSM and HIV
• MSM bear major burden of global HIV epidemic– Throughout the Americas– In at least some parts of Asia– Increasingly appreciated in Africa
• MSM populations difficult to reach– Homosexuality is criminalized in 85 countries– Government denial– Religious prejudice
• Real/perceived stigma and discrimination drives HIV epidemic
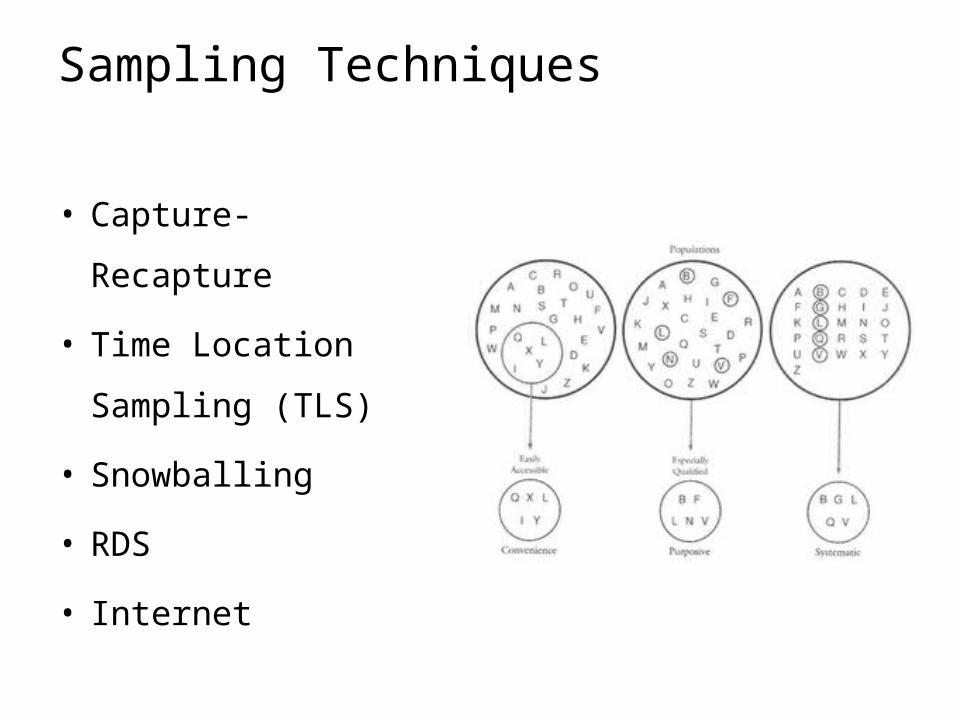
Sampling Techniques
• Capture-
Recapture
• Time Location
Sampling (TLS)
• Snowballing
• RDS
• Internet

Capture-Recapture
• c1 = sample captured at t1
• c2 = sample captured at t2
• c2 recaptures = matches (m)
c1/n = m/c2
• Therefore
n = (c1*c2)/m
• 95% confidence interval estimate for n
95%CI = n ± 1.96*√Var(n)
• Where
Var(n) = [(c1*c2*(c1-m)*(c2-m)]/m3
Kruse N, Sex Transm Dis. 2003; Luan R, Eur J Epidemiol. 2005; Geibel S, AIDS. 2007
Capture-recapture methodology has been employed to estimate the size of hidden or difficult-to-reach human
populations
Capture–Recapture Assumptions
• Closed population• Capture history of each member accurate• Capture sources independent• Equal probability of being captured in both rounds
• “…capture-recapture proved to be low-cost and relatively easy to use techniques for counting a hard-to-reach population.” (Kruse N, Sex Transm Dis. 2003)
• Capture-recapture is cost effective in both time and funds and is highly reproducible (Luan R, Eur J Epidemiol. 2005)
Geibel S, AIDS. 2007
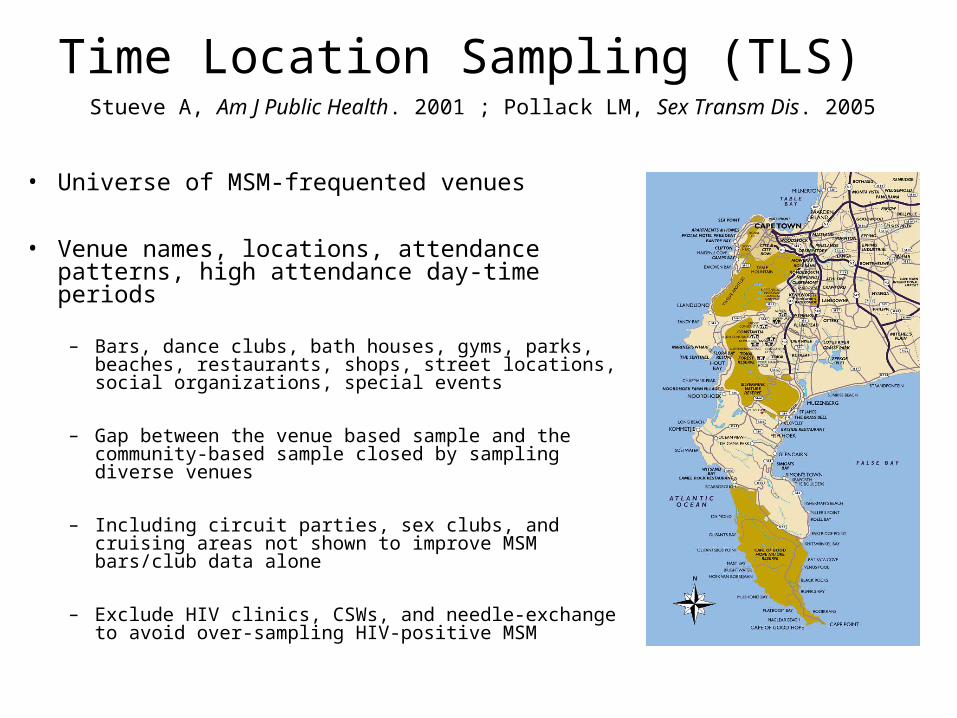
Time Location Sampling (TLS)
• Universe of MSM-frequented venues
• Venue names, locations, attendance patterns, high attendance day-time periods
– Bars, dance clubs, bath houses, gyms, parks, beaches, restaurants, shops, street locations, social organizations, special events
– Gap between the venue based sample and the community-based sample closed by sampling diverse venues
– Including circuit parties, sex clubs, and cruising areas not shown to improve MSM bars/club data alone
– Exclude HIV clinics, CSWs, and needle-exchange to avoid over-sampling HIV-positive MSM
Stueve A, Am J Public Health. 2001 ; Pollack LM, Sex Transm Dis. 2005

• Validation compared to telephonic household probability survey
• Few differences found compared to community-based sample– No significant differences in HIV infection or HIV related risk
behavior– May under-represent
• Older age groups• Closeted men
• Periodic (~5-years) probability-based household surveys
• Technique results in a sample is of venue attendees– Subset of the adult MSM population
Methodology influencing TLSPollack LM, Sex Transm Dis. 2005; Xia Q, Sex Transm Dis. 2006

TLS of MSM in Cape Town
• LGBT venues in city centre– 542 MSM
• 37 days• 16 LGBT venues
• LGBT events in black and coloured township– 200 MSM
• 23 separate events
E Burrell, Abstract LBPE1195 Mexico City IAS. 2008

Snowball Sampling
• Non-probability method• Referrals from “seeds” in
chain pattern• Useful for populations not well
delimited or enumerated• Lower search costs
• Non-random– Several seeds– Varying social groups
• Network size/selection probability correlates
• Seed judgment• Poor reproducibility• Confidentiality
McFarland W, AIDS. 2001; Wade AS, AIDS. 2005; Parry C, Drug Alcohol Depend. 2008
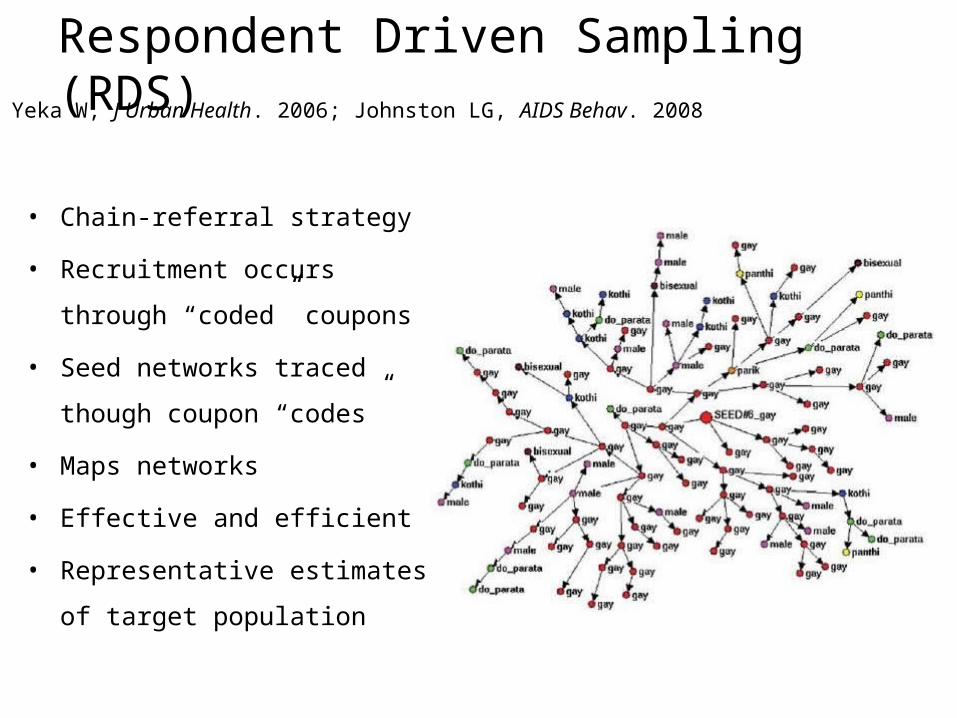
Respondent Driven Sampling (RDS)
• Chain-referral strategy
• Recruitment occurs
through “coded” coupons
• Seed networks traced
though coupon “codes”
• Maps networks
• Effective and efficient
• Representative estimates
of target population
Yeka W, J Urban Health. 2006; Johnston LG, AIDS Behav. 2008

Application of RDS
• Little variation between RDSAT–adjusted versus crude estimate
• Greater penetration and representation compared to hypothetical TLS
• “Overall, the use of RDS among the MSM…had numerous advantages in terms of collecting a required sample size in a short time period, minimizing costs and maximising security for staff and respondents.”
Yeka W, J Urban Health. 2006

Sampling Comparison
• Comparison of snowball, TLS, and RDS surveys of MSM– Socio-economic status (SES)– HIV risk behaviors– AIDS cases
• RDS– Wider inclusion of lower SES – Faster recruitment– Lower cost
Kendall C, AIDS Behav. 2008

• MSM/STI/Internet correlation noticed in 2002– Love– Companionship– Sex– Online behavioral
studies
• Advantages– Rapidity of recruitment– Diverse populations
• Methodologic challenges– Study design– Participant recruitment
and retention– Survey implementation– Interpretation of results– Verifying informed
consent– Surveying minors– Anonymity
InternetAIDS Alert. 2004 Feb;19(2):19-20; Chiasson MA, J Urban Health. 2006

• Smart Sex Quest– Recruitment and
retention– Internet-based RCT
• 3,625 recruited– 563 ineligible– 1,286 left site before
completion– Data for 1,776– Follow-up for 270
(15.2%)
• Severe loss to follow-up
• UAI with partners met– on-line– off-line
• 1,683 recruited– 51% met on-line– 23% UAI
• Equal likelihood of UAI with partners were met on- or off-line
Internet Sampling MethodologyBull SS, AIDS Care. 2004; Chiasson MA, J Acquir Immune Defic Syndr. 2007

Minority Internet User Profile
• Rural MSM– Face-to-face/Snowball– Internet
• Higher risk profile
• Highest risk behaviors– Internet– Sex clubs
• Hispanic MSM– 735 men
• 172 (23%) interviewed– 94.7% AI
• 48.9% inconsistent condom use
– 48.5% club drugs• Associated with UAI
• Internet recruitment– More efficient– Less costly
• Bisexual• HIV+• Lower gay community
attachment
Bowen A, AIDS Behav. 2004 ; Horvath KJ, J Health Psychol. 2006; Fernández MI, AIDS Care. 2004, J Ethn Subst Abuse. 2007

LMIC Internet User Profile
• Internet/Venue-based comparison– Harbin, China
• Internet sample– Younger– More educated– Student– Homosexual
• Community sample– Female partners– 6 or more male
partners
• No difference– UAI– Transactional sex
• Cross-sectional MSM probe– Malawi– Namibia– Botswana
• 537 MSM recruited – 44.7% (238/533) used
Internet
Zhang D, AIDS Care. 2008; Baral S, in publication. 2008

MOTHER CITY MEN’S HEALTH PROJECT
• HIV/AIDS programs in South Africa are heavily heterosexual and female focused
• Collaboration between– Desmond Tutu HIV Foundation– Triangle Project
• New initiatives in male-focused health programs• Include men who have sex with men (MSM) in HIV
prevention and treatment research

Sexual Risk Behavior AndHIV Prevalence Among MSM
• Cross-sectional, anonymous, venue-based HIV risk behaviour and prevalence study– Demographics– Sexual risk behaviour– Self-administered
questionnaire– OraSure® collection device
standard ELISA procedures
• Enrolled 542 self-identified MSM– 37 days– 16 LGBT venues
E Burrell, D Mark, R Grant, R Wood, LG Bekker

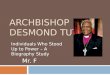
Urban Results
HIV Prevalence
10.7 8.910.7 12.5
1.8 1.8 0 3.63.65.45.47.1
3.65.4
12.57.110.4
0
10
20
30
40
50
60
70
80
90
100
Venue (n)
Sam
ple
(%
)

Descriptive Statistics
9.3
0.2
79.6
5.8
45.8
16.3
72.6
77.2
0
10
20
30
40
50
60
70
80
90
100
Sam
ple
(%)
Urban Results
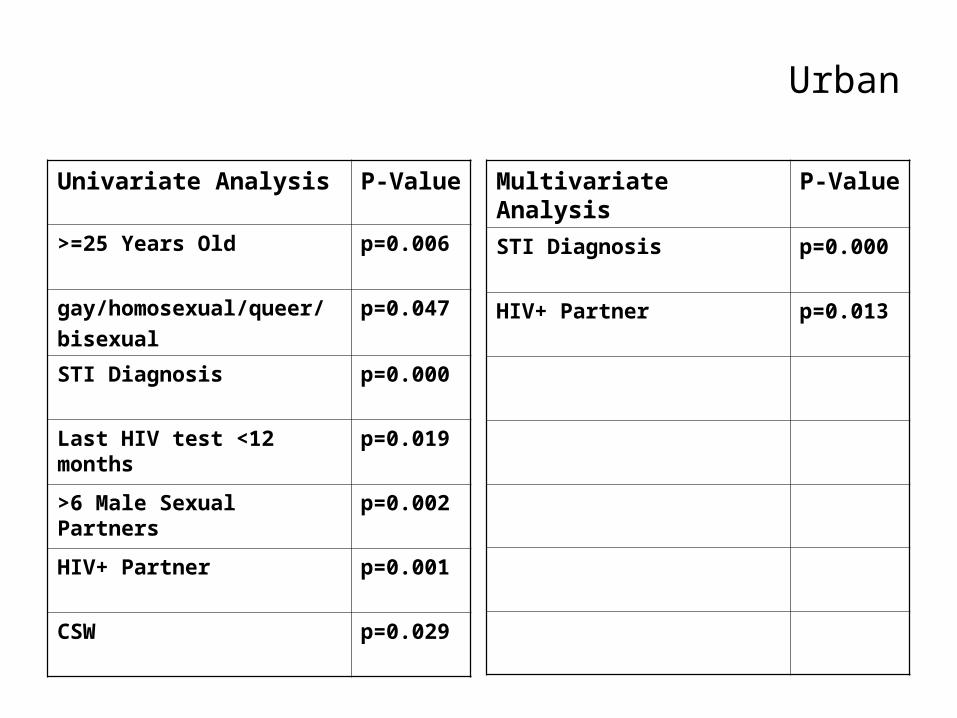
Urban
Univariate Analysis P-Value
>=25 Years Old p=0.006
gay/homosexual/queer/bisexual
p=0.047
STI Diagnosis p=0.000
Last HIV test <12 months
p=0.019
>6 Male Sexual Partners
p=0.002
HIV+ Partner p=0.001
CSW p=0.029
Multivariate Analysis
P-Value
STI Diagnosis p=0.000
HIV+ Partner p=0.013

Rights Violations and HIV PrevalenceAmong MSM in Peri-Urban Cape Town
• Anonymous, venue-based HIV risk behavior and prevalence probe– 200 self-identified MSM– Black and coloured townships– Demographics– Sexual risk behavior– Rights abuse
• Health worker administered questionnaire
• OraQuick® rapid HIV-1/2 antibody test
• Enrolled 200 self-identified MSM
• 20 LGBT venues
E Burrell, S Baral, C Beyrer, R Wood, LG Bekker
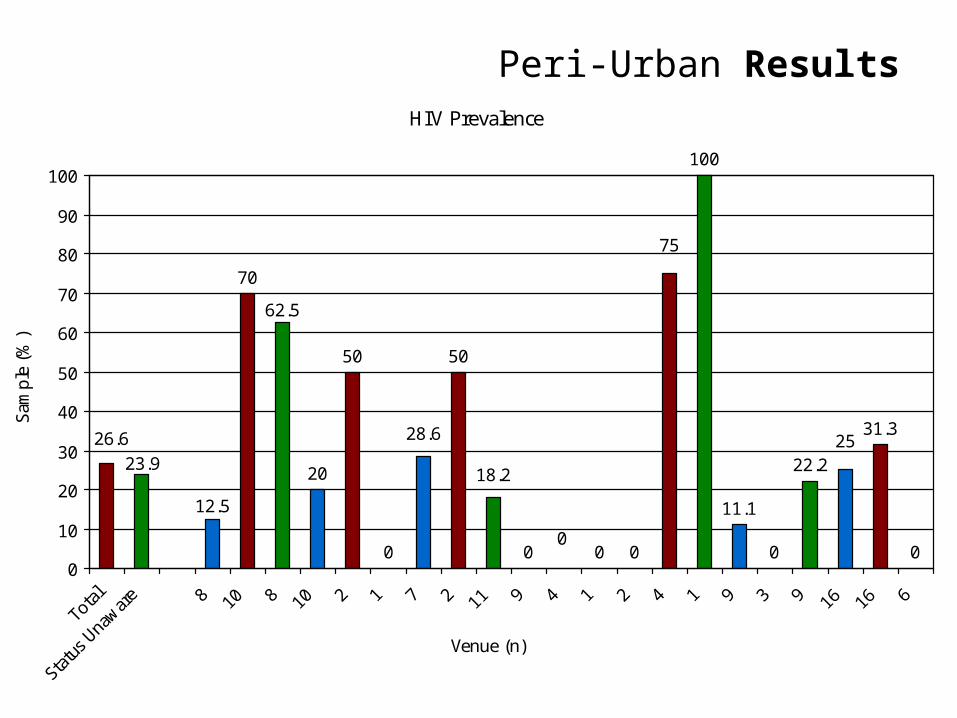
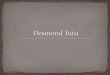
Peri-Urban ResultsHIV Prevalence
70
20
50
0
50
0 0 0
100
11.1
0
22.2
31.3
0
25
75
23.926.6
12.5
62.5
28.6
18.2
0
0
10
20
30
40
50
60
70
80
90
100
Total
Status
Una
ware 8 10 8 10 2 1 7 2 11 9 4 1 2 4 1 9 3 9 16 16 6
Venue (n)
Sam
ple
(%)

Peri-Urban ResultsDescriptive Statistics
14
20.9
2.2
16.6
30.6
77
58.3
88.279
25.9
0
10
20
30
40
50
60
70
80
90
100
Sam
ple
(%)
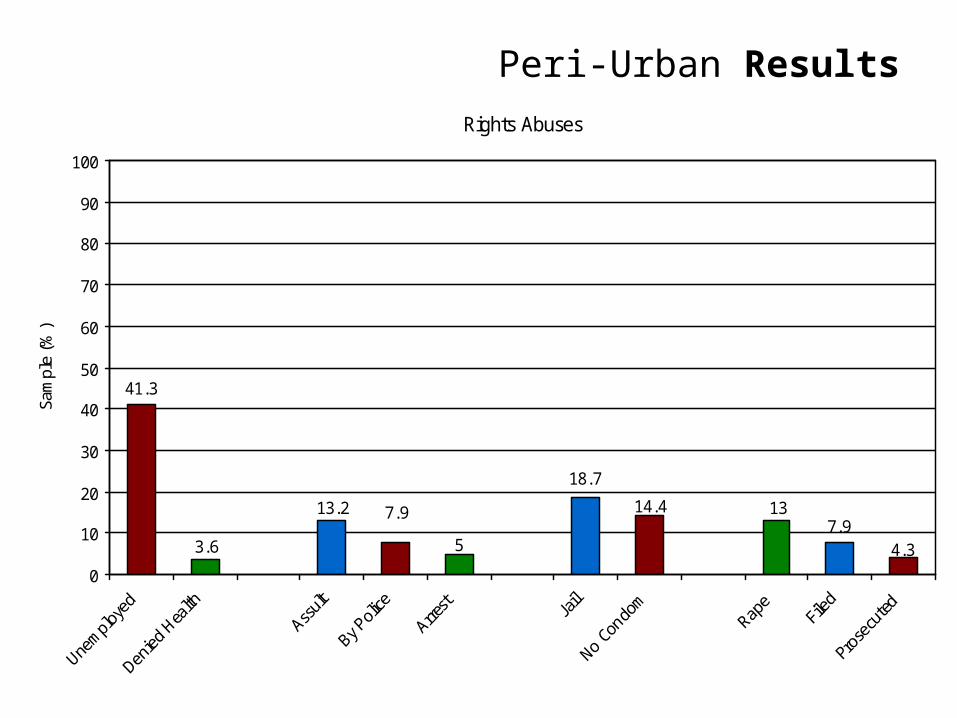
Rights Abuses
7.93.6 5 4.3
14.4 13
41.3
13.2 7.9
18.7
0
10
20
30
40
50
60
70
80
90
100
Sam
ple
(%)
Peri-Urban Results

Peri-Urban Modeling
Univariate Analysis P-Value
Last HIV test >12 months
p=0.001
>5 Male Sexual Partners
p=0.004
Unemployed p=0.043
Receive kind for sex p=0.044
Denied Healthcare p=0.006
Multivariate Analysis
P-Value
Last HIV test >12 months
p=0.001

Conclusions
• Clear correlation between select outcome variables and HIV serostatus– These methods could be used to identify
and track high HIV risk MSM populations
• Targeted risk-reduction and HIV prevention strategies
Conclusions
• Concentrated epidemics may present opportunities for intervention
• We need to know more about networks, risk patterns and drivers.
• Need to overcome ethico-legal barriers.• Will need innovative strategies to reach
hard to reach populations for research• Methodologies need to be validated for
population and particular group