Embed Size (px)
Citation preview
UCL
Gefinancierd door de Programmatorische Federale Overheidsdienst Wetenschapsbeleid Financé par le Service Public fédéral de Programmation Politique Scientifique
ResoPrim Experimental network in primary health care
Primary Healthcare Research Network: the Belgian ResoPrim Recommendations
Etienne DE CLERCQ, Viviane VAN CASTEREN, Pascale JONCKHEER, Peter BURGGRAEVE
MIE2009 congress Sarajevo, 30/08 -02/09/2009
UCL – IRSS, Clos Chapelle aux Champs 30.41, 1200 Brussels | Belgium email: [email protected]
2
Overall aim of the project
Development of a stable experimental network/framework for collection (from the EMR), analysis and dissemination of data from primary health care
To become a reference network/framework, enabling to improve the quality of other health information networks in primary care in Belgium
3
Objectives
To issue recommendations for sustaining development of other networks (early 2009)
On a longer term : to implement (some of) these recommendations to set up a stable EPR-based national research network (2009 - /)
Setting-up the ACHIL research laboratory (Ambulatory Care Health Information Lab)
Part of the Belgian health information strategy
4
ResoPrim
• Financed by Federal Public Planning Service – Science Policy (framework of multi-annual Programme for the Development of the Information Society)
• October 2003 – December 2008 (2 pilot phases)
• 4 partners, 64 GPs, 6 software systems, an international expert committee

5
Specific context
In Belgium: 10,000 GPs; 6,000 GPs using an EPR;
> 18 software systems, … For the ResoPrim project
Volunteer participation of the GPs, No highly specific IT skill required , use of current running systems, No GP patient lists
6
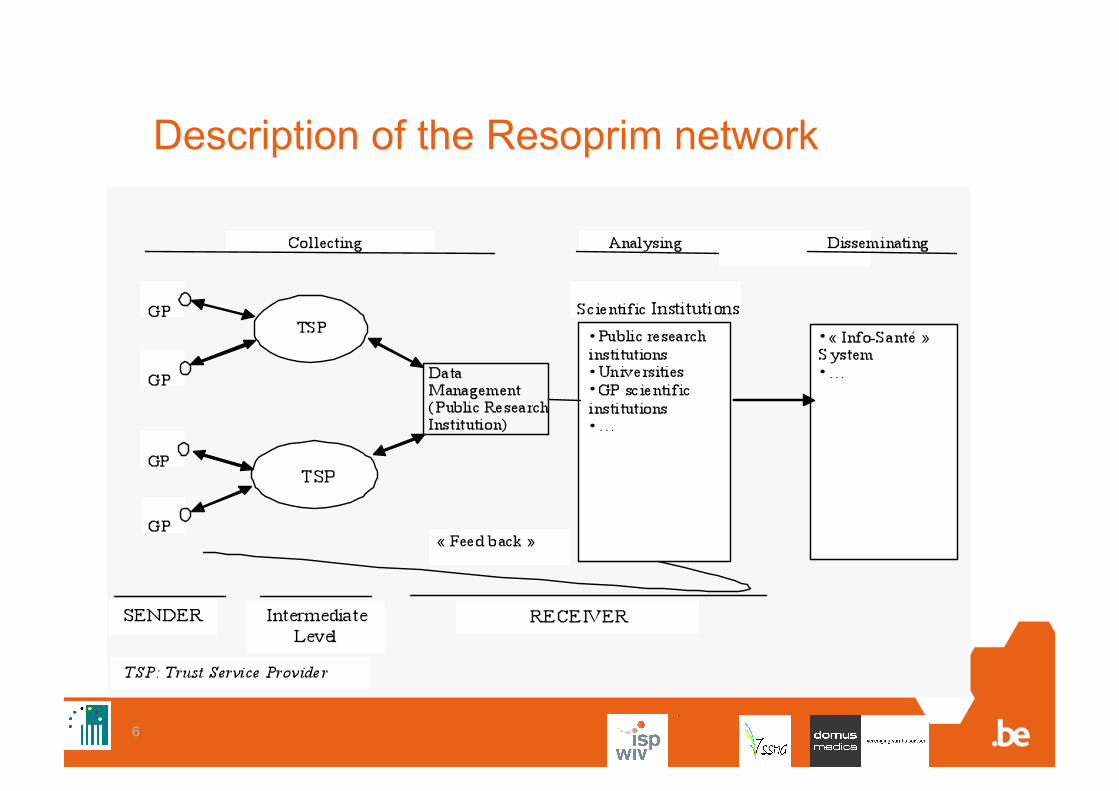
Description of the Resoprim network
7
Objectives (1) Analyse conditions regarding organisation and use of a pilot network • possible routine EPR-based data exploitations in
various domains: epidemiology, quality of care, socio-economy, health research information system
• organisation and management of network • validity of collected data in various domains • benefits/drawbacks for GPs in participating in the
network

8
Methods (1)
• Extended literature review • Definition of research questions • Methods used
Quantitative research Qualitative research Questionnaires to GPs
• Recruitment • Satisfaction survey after data collection • Satisfaction survey after feedback
Analysis of data previously collected
9
Methods (2): Research domains
Epidemiology
Quality of care
HRIS assessment
Denominator and sampling
Socioeconomy
GPs’ education and benefits
10
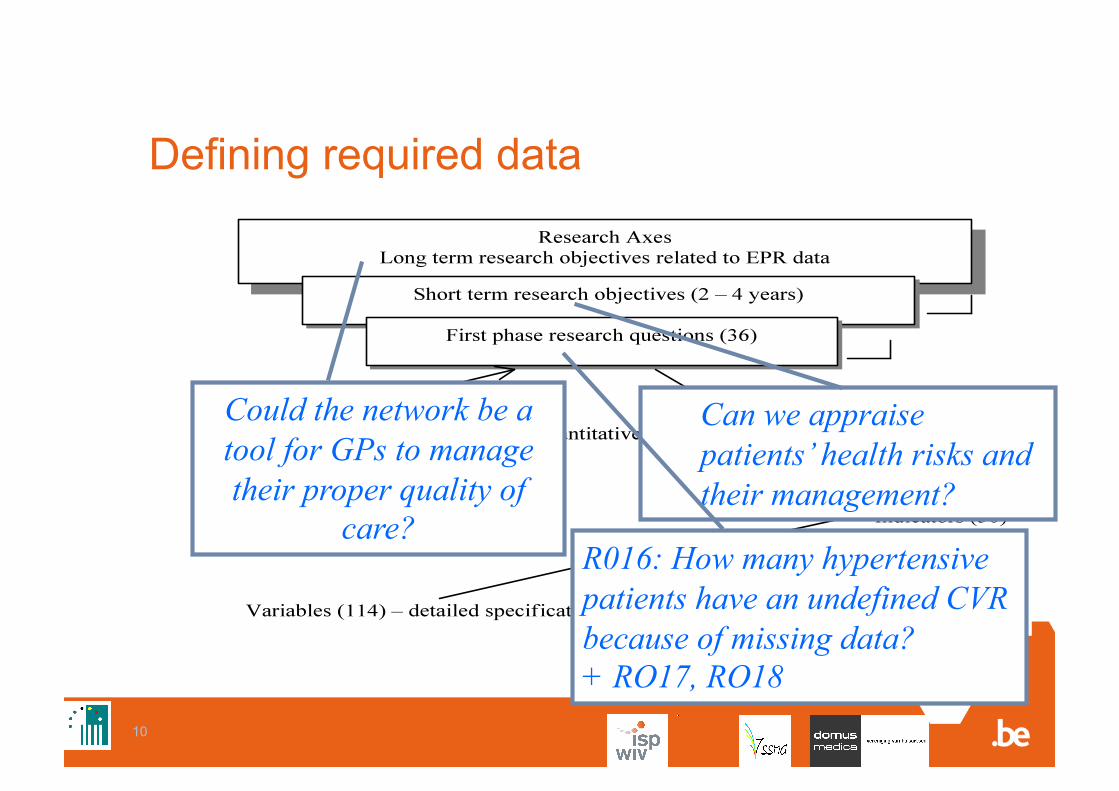
Defining required data
Could the network be a tool for GPs to manage their proper quality of
care?
Can we appraise patients’ health risks and their management?
R016: How many hypertensive patients have an undefined CVR because of missing data? + RO17, RO18
11
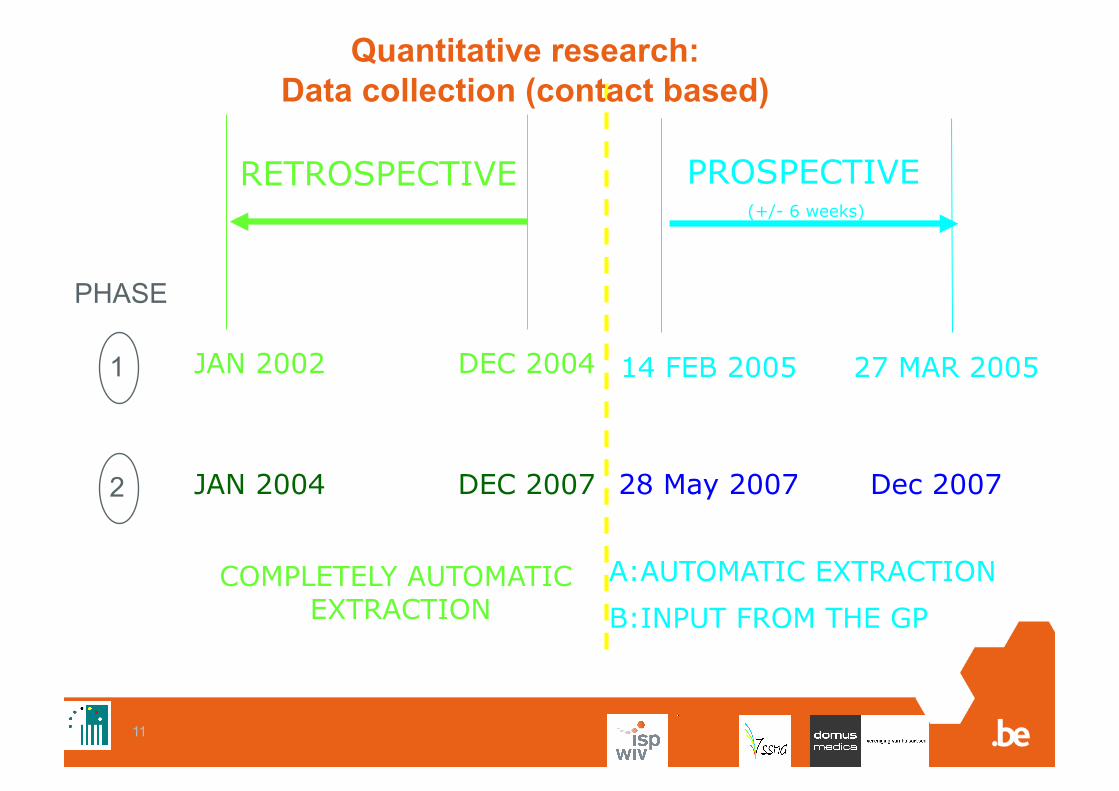
RETROSPECTIVE
JAN 2002 DEC 2004
COMPLETELY AUTOMATIC EXTRACTION
PROSPECTIVE (+/- 6 weeks)
14 FEB 2005 27 MAR 2005
A:AUTOMATIC EXTRACTION
B:INPUT FROM THE GP
Quantitative research: Data collection (contact based)
JAN 2004 DEC 2007 28 May 2007 Dec 2007
PHASE
1
2

12
Quantitative research : Data types
Demographic and contact related data • age, sex, contact date, …)
Clinical data • Diagnoses (ICD10 – ICPC 2) • Some drugs prescribed • The fact that a referral to a specialist has been
made during the contact Some parameters: height, weight, blood pressure,
tobacco use
13
Results
The 18 Recommendations -
Some key features
Much more information on the ResoPrim website: http://www.iph.fgov.be/epidemio/epien/index38.htm
14
Privacy protection
15
Privacy protection
Do we need explicit (written) informed consent from the patients? (i.e.: should the GP actively inform the patient?)
• Not for retrospective data
• Yes for prospective data … …if it does not interfere with the care process
Otherwise …
16
Privacy: Patient’s informed consent
• The patient should at least be informed « passively » by means of a poster and a folder (information that could be taken back home). The GP should also be able to provide additional information.
• At least, the patient’s refusal has to be recorded explicitly. A period to express this refusal has to be foreseen after the consultation/information of the patient (for instance 15 days). GP should also be able to express his/her own refusal.

17
Privacy: Communication to third parties
• The GP should sign a contract in order to restrict the potential usage of the anonymous data (that eventually could be done by third parties).

18
Quality control & assessment

19
A wide & well known underestimation
Sensitivity of automatic extraction from EPR
• Diagnostic (HTA): 54%
• Antihypertensive medication: 60%
• Referral (hypertensive patients): <11%
• Parameter availability (height): 52%

20
Quality control & assessment
HRIS = Tool needs to be calibrated
GP EPR DB
Quality of the DB content
Quality of the extraction modules
(Dummy patient technique)

21
Source validation
GPs’ thoughts
EPR
Research Data Base
Data Base “gold standard”
Source validation

22
Automatic extracted Diagnoses, drugs, referrals Sensitivity and Positive Predictive Value (PPV) of automatic extraction vs questionnaire
Sensitivity (min – max)
PPV (min – max)
Drugs 34.1% - 59.34% 91.5% - 94.1%
Diagnoses 53.6% - 67.1% 42.1% - 94.90%
Referrals < 17% < 37%
% = min. and max. per question

23
HRIS content improvement
We can improve it! How?
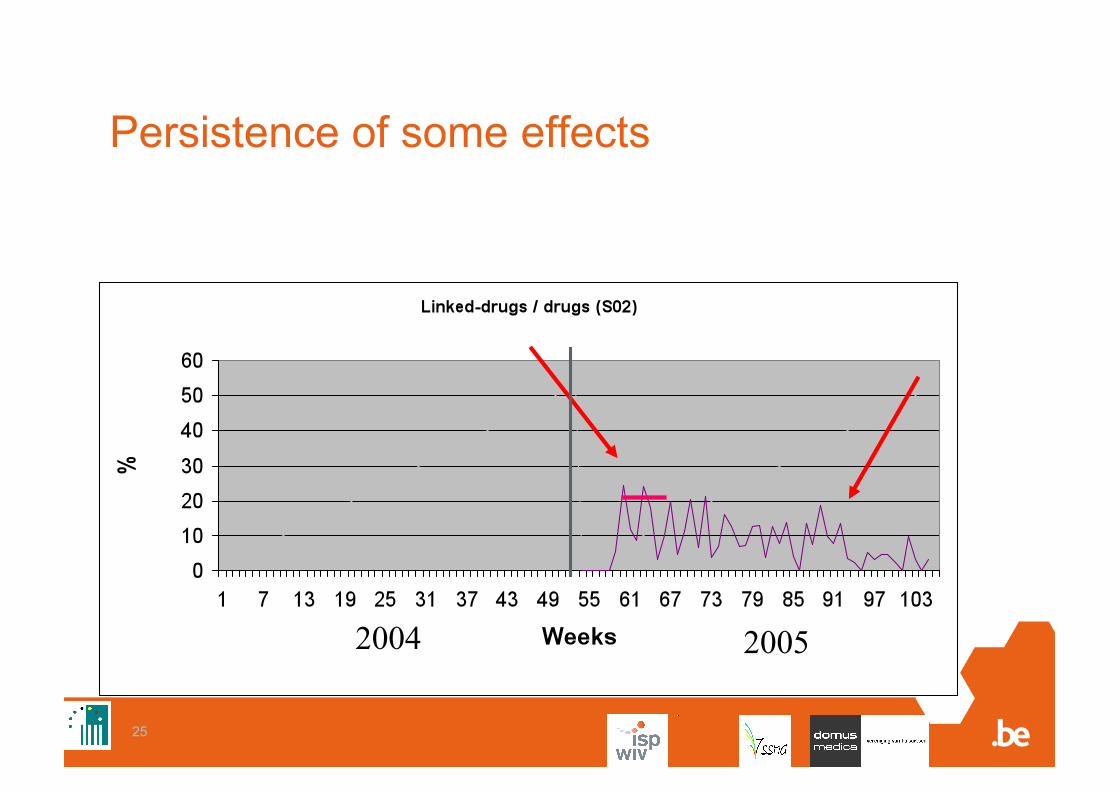
• Participation to (thematic) data collection networks. This effect could last.
• Global measures (e.g.: software homologation)

24
Participation impact ICPC
25
Persistence of some effects
2004 2005
26
Additional strategies
To improve the HRIS content we can also act on • For the drugs sensitivity:
The extraction procedure design The ‘active drugs’ management
• For the diagnosis sensitivity: The education?
• For the Diagnosis PPV The extraction module (family history, derived codes) The questionnaire? (list of questions?)
• For the parameters sensitivity & completeness The software interfaces
27
Can we do something with the data currently available in the EPRs?

28
HRIS and Quality of care
• If no quality control assessment is foreseen, we presently do not recommend to use routine EPR data for identification of a target population.
• It is presently not recommended to compare the quality of care between GPs (too much uncertainty about the “EPR use” of GPs).
• If, however, we assume that incompleteness of data and changes in EHR use are homogeneously spread across various goups or types of patients within any one group of GPs, then it may be possible to compare various subgroups of patients or to monitor some aspects of the quality of care.
29
How to encourage (volunteer) GPs?
30
GPs’ involvement – key factors (1)
• GP invited by a personal contact • Exhaustive information • Trust in the organizers • Use of “anonymous” data • Protection (encryption) of data sent • Scientific objective of the network • Acceptable daily workload • No supplementary request from patient
31
GPs’ involvement – key factors (2)
• An efficient help desk • Learning opportunities or individual feedback
(more controversial) • Financial incentive (also controversial)
…To manage all that at a national level is challenging!
32
Conclusions
A HRIS can be set up with a high acceptable privacy protection.
Such EPR based network can be a useful tool to monitor some aspects of the quality of care
…but … We need a quality control and assessment
procedure to calibrate this tool (and monitor its improvement).
To encourage GPs’ involvement at a broad national level is still challenging.

33

34
Quality of a research DB content
Patient GP EPR DB
Facts Thoughts Registered thoughts
Extracted info
Information System Consultation