Embed Size (px)
Citation preview
Respiratory Failure in less than 30 minutes or your lecture is free*
Matthew Exline, MD MPH
* Just kidding you still have to pay tuition
Learning Objectives
2
Define the mechanisms of hypoxemia. Use A-a gradient to differentiate the cause of
hypoxemia in the clinical setting. Recognize depressed respiratory drive,
inadequate neuromuscular competence and excessive respiratory system load as causes of ventilatory failure.
Describe clinical treatment strategy to improve oxygen delivery based on the oxygen delivery equation.
Describe the use of Positive Pressure Ventilation in the treatment of respiratory failure.
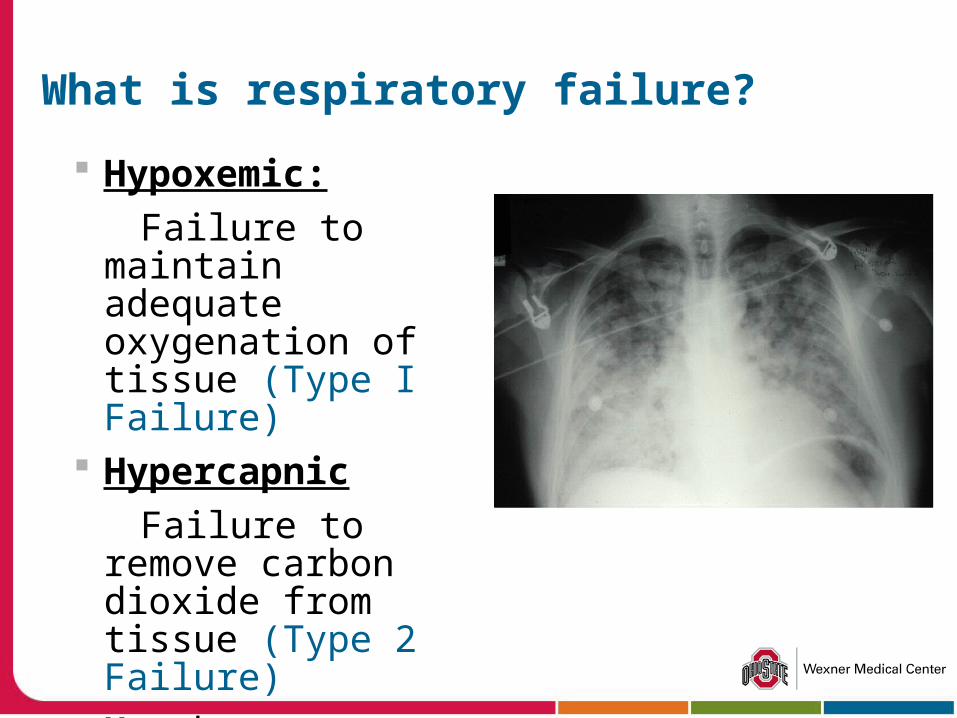
What is respiratory failure?
Hypoxemic:
Failure to maintain adequate oxygenation of tissue (Type I Failure)
Hypercapnic
Failure to remove carbon dioxide from tissue (Type 2 Failure)
May be acute, chronic, or acute on chronic
4
Causes of Hypoxia (NEW!)
Low partial pressure of oxygen Hypoventilation Impaired diffusion Shunt Increased dead space ventilation Abnormal hemoglobin binding Abnormal mitochondrial usage
5
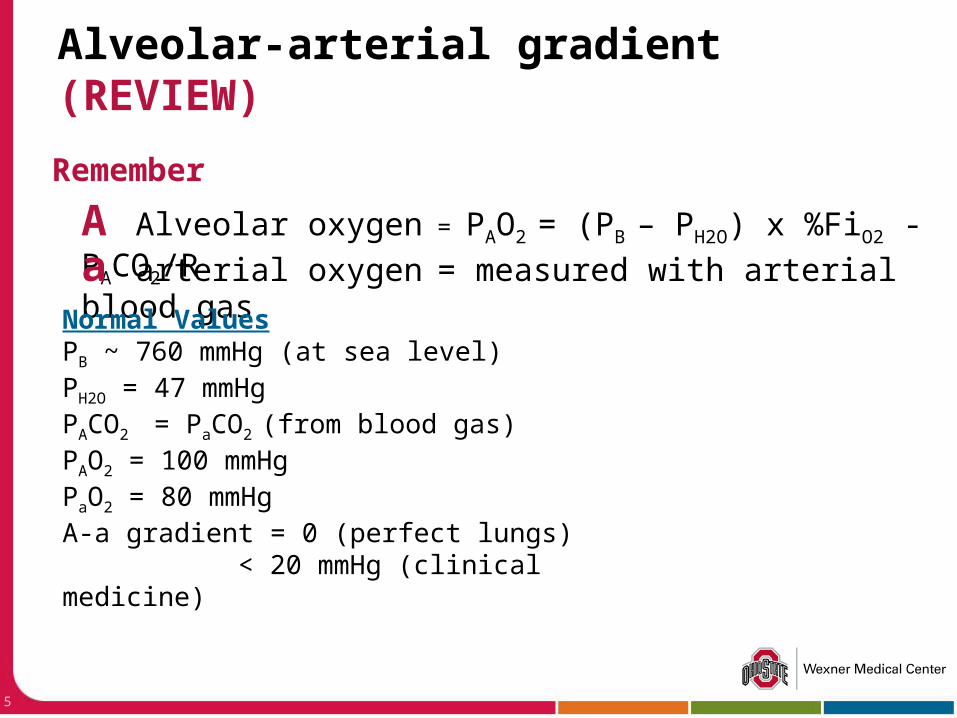
Remember
Alveolar-arterial gradient (REVIEW)
A Alveolar oxygen = PAO2 = (PB – PH2O) x %FiO2 - PACO2/R
a arterial oxygen = measured with arterial blood gas
Normal ValuesPB ~ 760 mmHg (at sea level)PH2O = 47 mmHgPACO2 = PaCO2 (from blood gas)PAO2 = 100 mmHgPaO2 = 80 mmHgA-a gradient = 0 (perfect lungs)
< 20 mmHg (clinical medicine)
Causes of Hypercapnia
Causes of Hypercapnia (simple version)
Inhalation of CO2
Increased production CO2
Fever Increased calories
Pump Failure Competence - not
enough effort Load – too much work
Apollo 13 Carbon Dioxide Scrubbers
“I suggest you gentlemen invent a way to put a square peg in a round hole. Rapidly.”
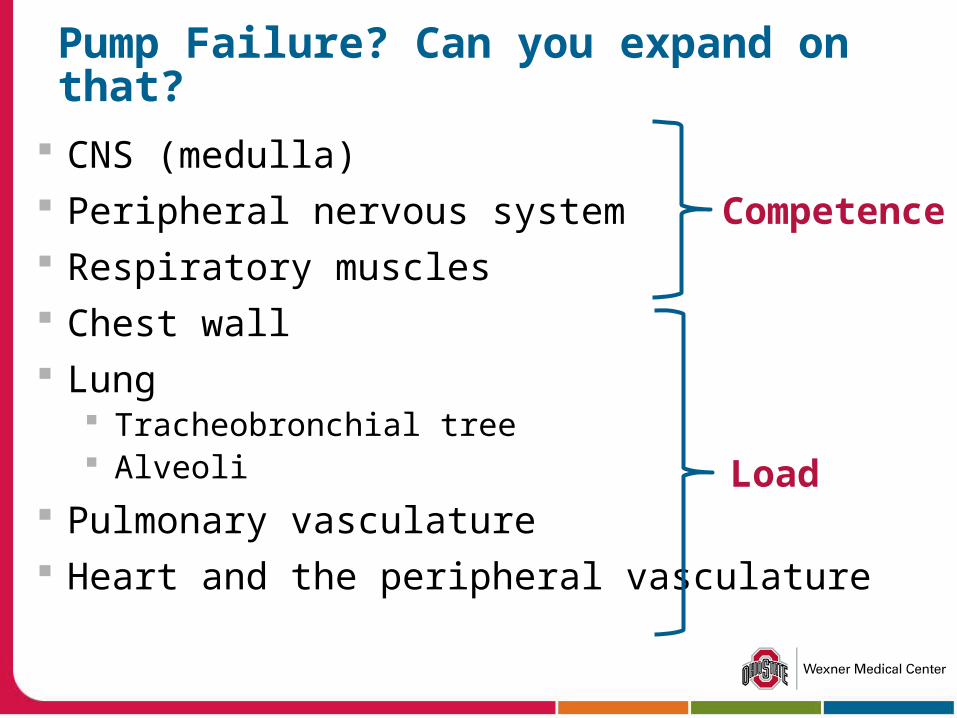
Pump Failure? Can you expand on that?
CNS (medulla) Peripheral nervous system Respiratory muscles Chest wall Lung
Tracheobronchial tree Alveoli
Pulmonary vasculature Heart and the peripheral vasculature
Load
Competence
9
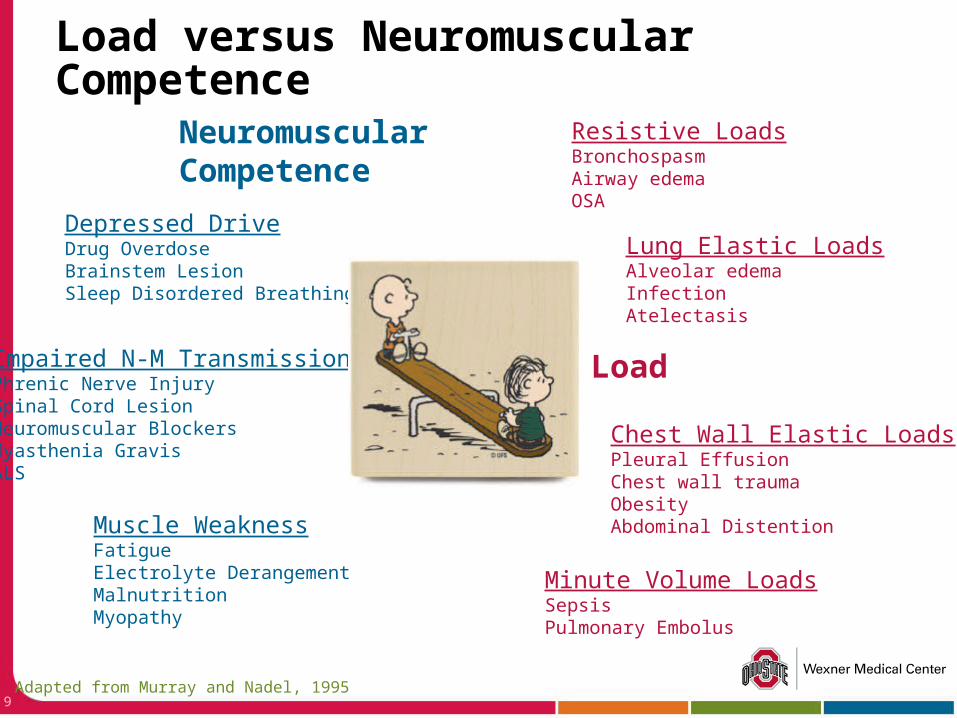
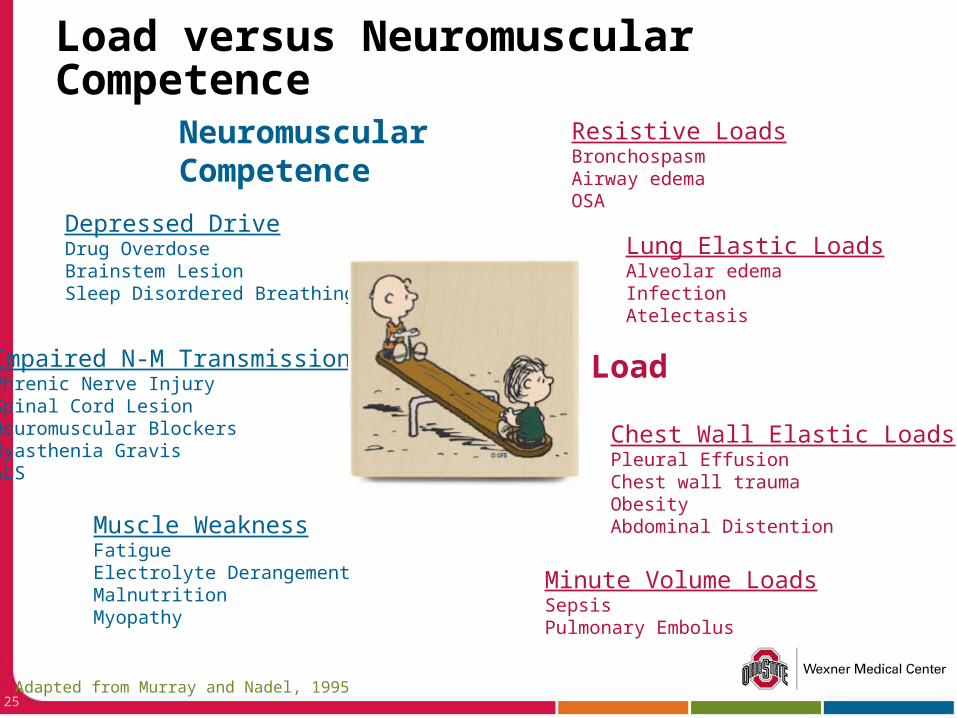
Load versus Neuromuscular Competence
Load
NeuromuscularCompetence
Depressed DriveDrug OverdoseBrainstem LesionSleep Disordered Breathing
Impaired N-M TransmissionPhrenic Nerve InjurySpinal Cord LesionNeuromuscular BlockersMyasthenia GravisALS
Muscle WeaknessFatigueElectrolyte DerangementMalnutritionMyopathy
Resistive LoadsBronchospasmAirway edemaOSA
Lung Elastic LoadsAlveolar edemaInfectionAtelectasis
Chest Wall Elastic LoadsPleural EffusionChest wall traumaObesityAbdominal Distention
Minute Volume LoadsSepsisPulmonary Embolus
Adapted from Murray and Nadel, 1995
Detection of Respiratory Failure
Examine the patient Oximetry Blood Gas
René Laennec
11
“How’s your breathing?” Evaluate mental status Work of breathing
Respiratory rate Accessory Muscle Use
General signs of distress Abnormal heart rate Abnormal blood
pressure
Oxygen Saturation
Patient Exam
CPR Annie
12
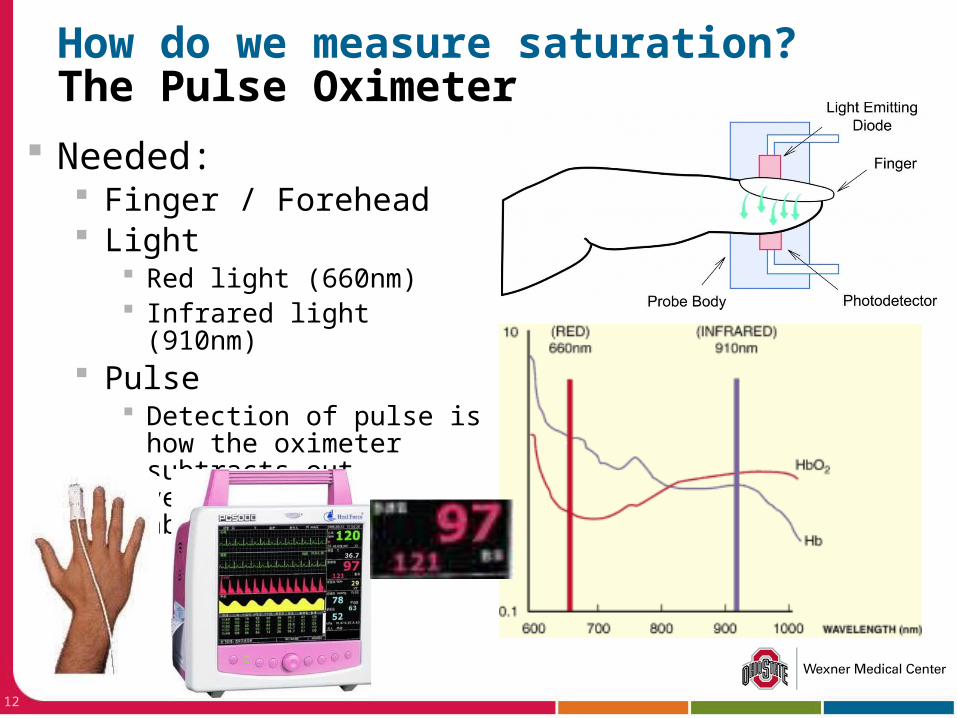
Needed: Finger / Forehead Light
Red light (660nm) Infrared light (910nm)
Pulse Detection of pulse is how
the oximeter subtracts out venous/tissue absorption
How do we measure saturation?The Pulse Oximeter
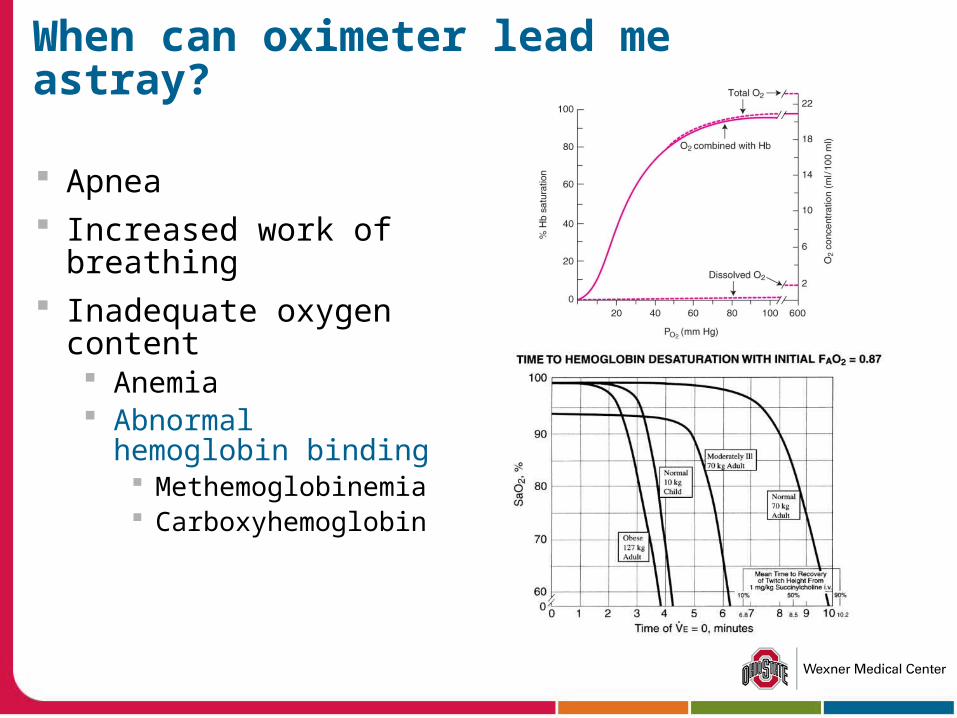
When can oximeter lead me astray?
Apnea Increased work of
breathing Inadequate oxygen
content Anemia Abnormal hemoglobin
binding Methemoglobinemia Carboxyhemoglobin
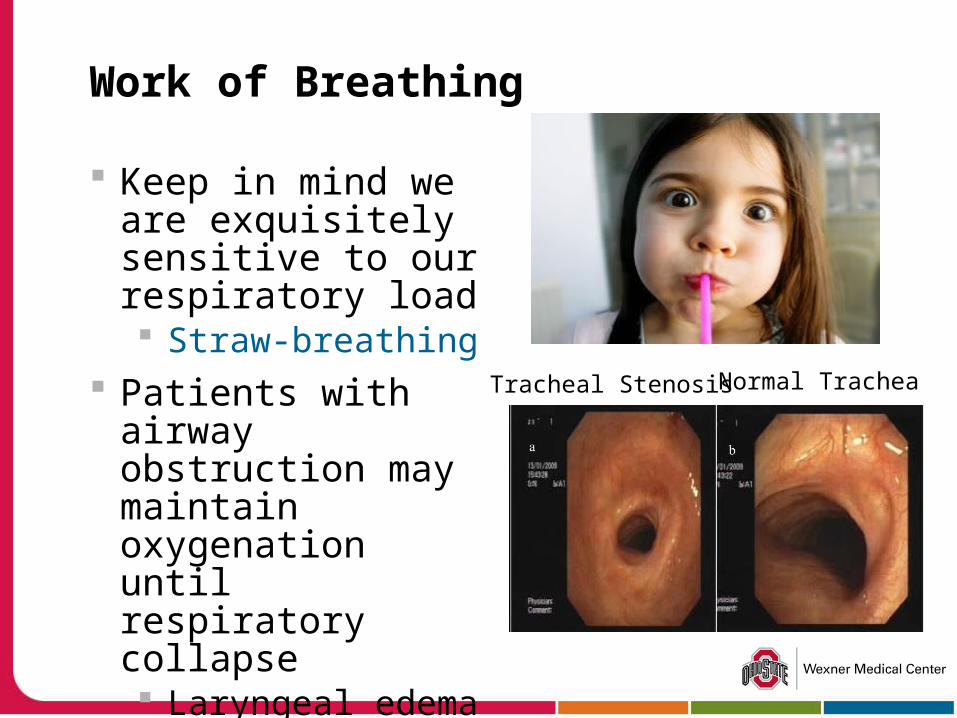
Work of Breathing
Keep in mind we are exquisitely sensitive to our respiratory load Straw-breathing
Patients with airway obstruction may maintain oxygenation until respiratory collapse Laryngeal edema Tracheal stenosis
Tracheal Stenosis Normal Trachea
What to I really care about? (REVIEW)
Remember oxygen content (CaO2) is a more important management measure than PaO2
([Hb] * %Sat * 1.34 ml/g) + (PaO2 * 0.003) Oxygen delivery the key parameter
CaO2 * Cardiac output (CO)
Always correlated your oxygenation status with your clinical picture!
16
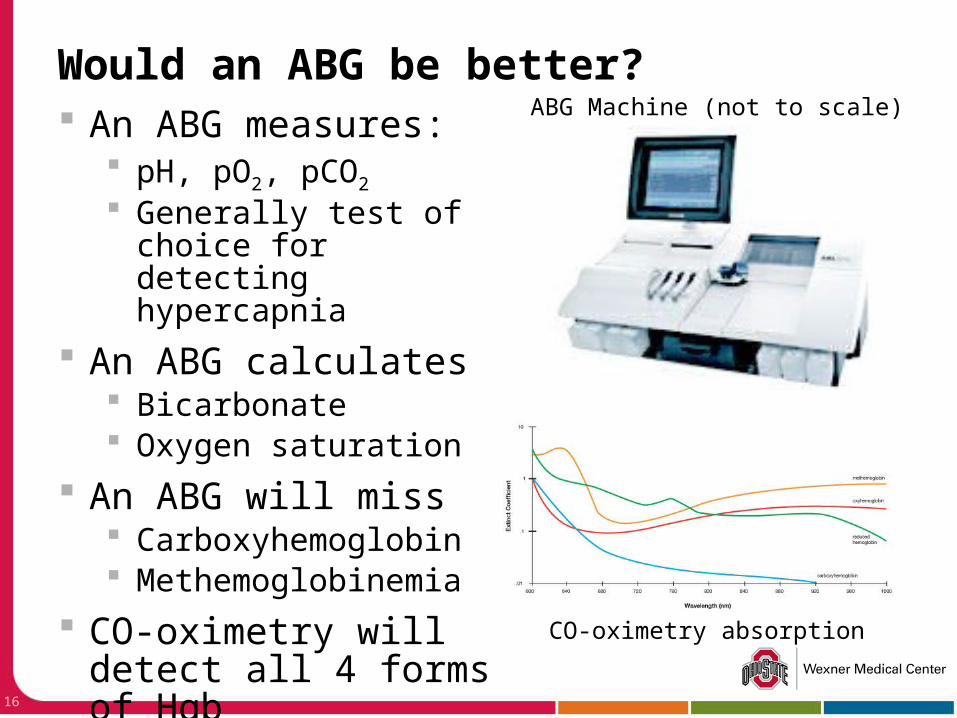
An ABG measures: pH, pO2, pCO2
Generally test of choice for detecting hypercapnia
An ABG calculates Bicarbonate Oxygen saturation
An ABG will miss Carboxyhemoglobin Methemoglobinemia
CO-oximetry will detect all 4 forms of Hgb
Would an ABG be better?ABG Machine (not to scale)
CO-oximetry absorption
17
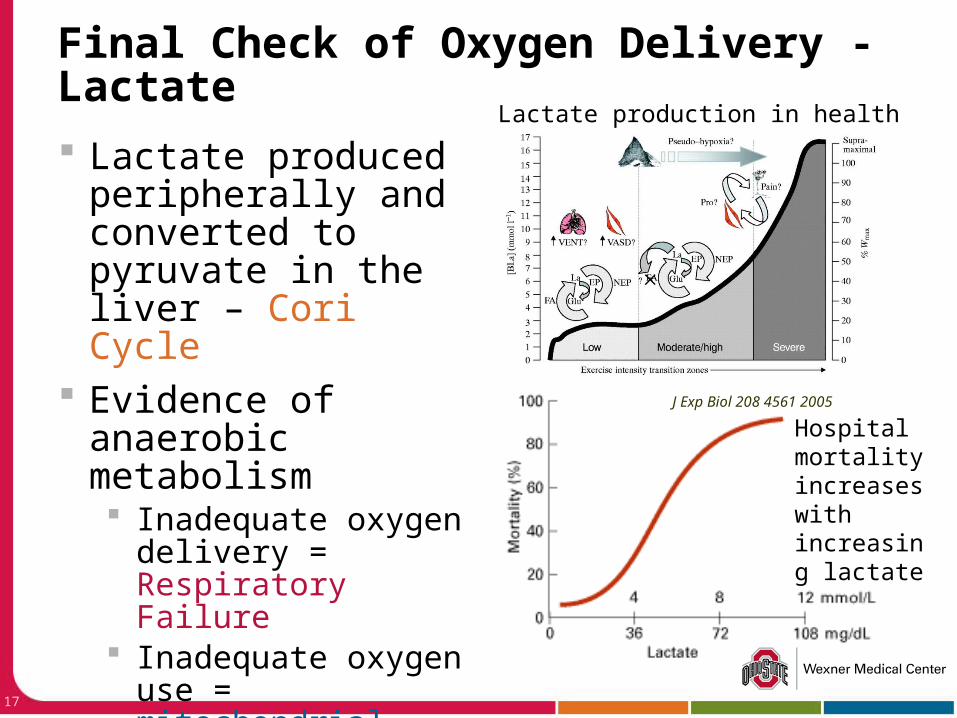
Lactate produced peripherally and converted to pyruvate in the liver – Cori Cycle
Evidence of anaerobic metabolism Inadequate oxygen
delivery = Respiratory Failure
Inadequate oxygen use = mitochondrial dysfunction Will discuss more in
Sepsis lecture
Final Check of Oxygen Delivery - Lactate
J Exp Biol 208 4561 2005
Hospital mortality increases with increasing lactate
Lactate production in health
Treatment of Respiratory Failure
Hypoxemic Supplemental oxygen
Hypercapnic Decrease production CO2 Decrease ventilatory load Improve neuromuscular competence
Hypoxemia / Hypercapnia Positive-pressure ventilation
Supplemental Oxygen: Nasal Cannula
1-6 LPM
*1L=24%
*2L=28%
*3L=32%
*4L=36%
*5L=40%
*6L=44%
**Now “High Flow” Nasal Cannula can deliver up to 15 LPM of oxygen and estimated FIO2 of ~ 80%
20
Advantages and Disadvantages of the Nasal Cannula
Advantages: Comfortable Able to communicate Patient can eat and
take oral medications Easy to use at home
Disadvantages: Nasal obstruction
may impede gas flow.
May cause nasal mucosal drying (can be humidified with sterile water)
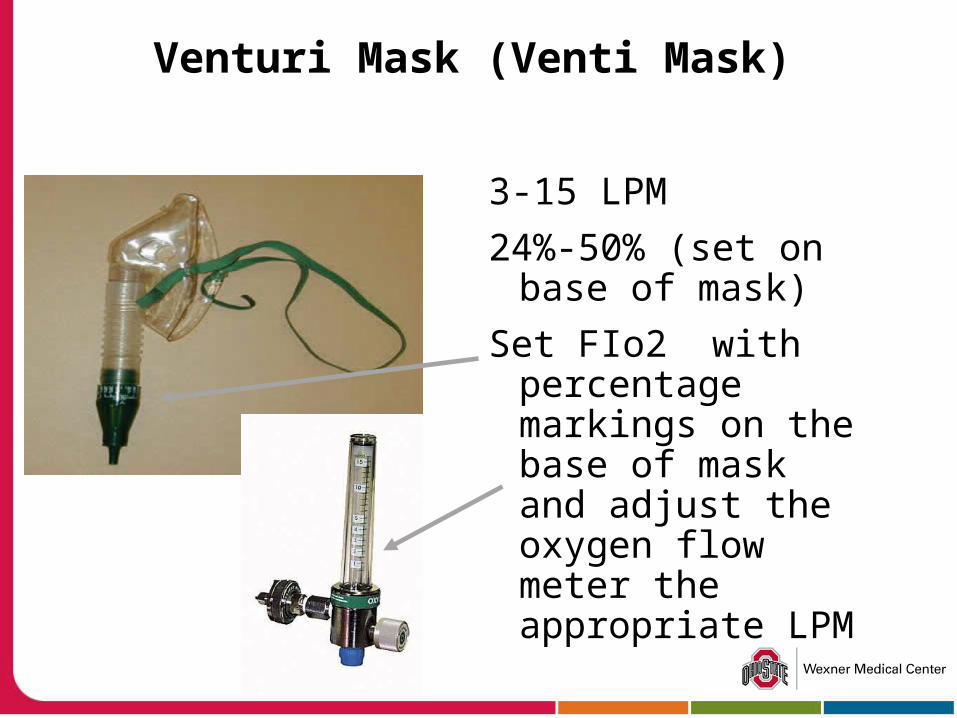
Venturi Mask (Venti Mask)
3-15 LPM
24%-50% (set on base of mask)
Set FIo2 with percentage markings on the base of mask and adjust the oxygen flow meter the appropriate LPM
22
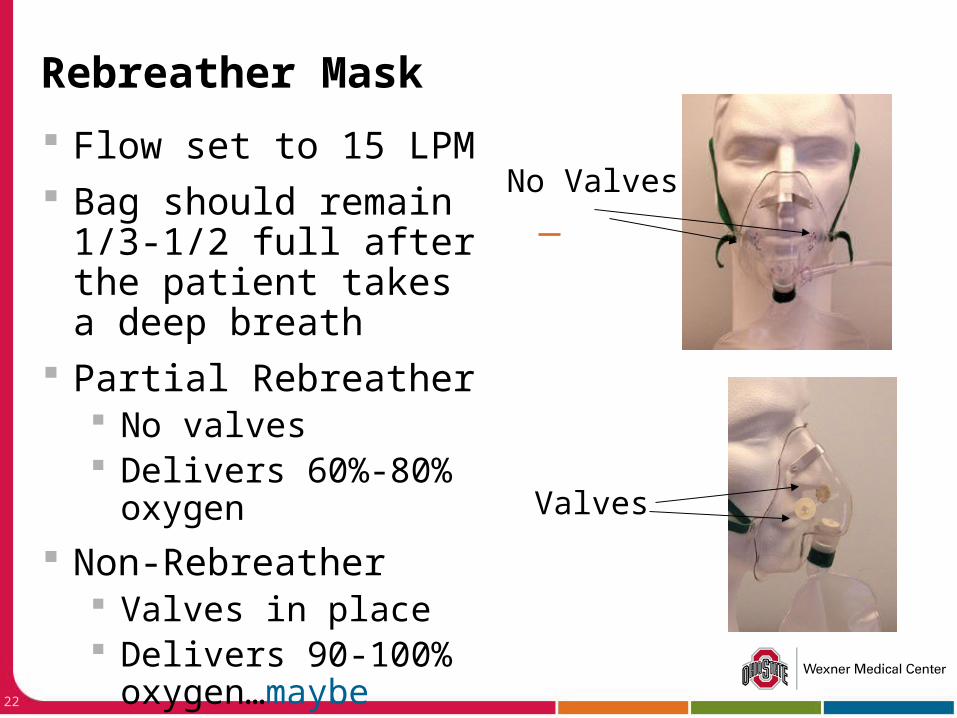
Rebreather Mask
Flow set to 15 LPM Bag should remain 1/3-
1/2 full after the patient takes a deep breath
Partial Rebreather No valves Delivers 60%-80%
oxygen
Non-Rebreather Valves in place Delivers 90-100%
oxygen…maybe
No Valves
Valves
Treatment of Respiratory Failure
Hypoxemic Supplemental oxygen
Hypercapnic Decrease production CO2
Decrease ventilatory load Improve neuromuscular competence
Hypoxemia / Hypercapnia Positive-pressure ventilation
Reduce feverAttention to nutrition
Treatment of Respiratory Failure
Hypoxemic Supplemental oxygen
Hypercapnic Decrease production CO2 Decrease ventilatory load Improve neuromuscular competence
Hypoxemia / Hypercapnia Positive-pressure ventilation
25
Load versus Neuromuscular Competence
Load
NeuromuscularCompetence
Depressed DriveDrug OverdoseBrainstem LesionSleep Disordered Breathing
Impaired N-M TransmissionPhrenic Nerve InjurySpinal Cord LesionNeuromuscular BlockersMyasthenia GravisALS
Muscle WeaknessFatigueElectrolyte DerangementMalnutritionMyopathy
Resistive LoadsBronchospasmAirway edemaOSA
Lung Elastic LoadsAlveolar edemaInfectionAtelectasis
Chest Wall Elastic LoadsPleural EffusionChest wall traumaObesityAbdominal Distention
Minute Volume LoadsSepsisPulmonary Embolus
Adapted from Murray and Nadel, 1995
Treatment of Respiratory Failure
Hypoxemic Supplemental oxygen
Hypercapnic Decrease production CO2 Decrease ventilatory load Improve neuromuscular competence
Hypoxemia / Hypercapnia Positive-pressure ventilation
When should I use Positive Pressure Ventilation?
Respiratory distress with moderate to severe dyspnea use of accessory muscles of respiration, abdominal
paradox Increased respiratory rate (~RR 30) or work of
breathing Acidosis (~pH < 7.2 to 7.3) Inability to oxygenate (SpO2 < 90%) despite
supplemental oxygen Inability to protect airway THIS GUY/GAL IS SICK…
* All values are relative
Positive Pressure Ventilation
Machine CPAP – helps oxygenation BiPAP – helps oxygenation and ventilation “Ventilator” – one stop shop for Respiratory Failure
Home CPAP machine
Hospital BiPAP machine
Hospital Ventilator
Positive Pressure Ventilation
Interface Mask
Awake patient, easily removable Endotracheal Tube
Patient can be sedated Can be difficult to place
Tracheotomy Permanent airway
Face Masks
“Trach” patient
Sedated, mechanically ventilated patient with ET tube
How should I deliver ventilatory support? Non-invasive (CPAP or BiPAP)
Awake, cooperative patient Hemodynamically stable Suspected temporary condition
COPD exacerbation, CHF exacerbation Use mask and either
CPAP is purely oxygenation issue BiPAP if ventilatory support is needed
(hypercapnia)
How should I deliver ventilatory support? Full mechanical support
Patient not protecting airway (coma) Patient delirious, not cooperative Hemodynamically unstable (shock) Expected longer duration of illness > 24 to 48 hours
temporary condition Failure of non-invasive ventilation
Patient will need endotracheal intubation and mechanical ventilation (aka “life support”)
* All values are relative
What should I remember from this?
Causes of hypoxia Causes of hypercapnia Function and utility of pulse oximeter Approximate FiO2 of supplemental oxygen When to use mechanical ventilation
Respiratory Failure Quiz
Questions / Comments / Suggestions
If you look like this at the end of lecture, go back and restart the slides…
Please email me:[email protected]
Survey
We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module.
The survey is both optional and anonymous and should take less than 5 minutes to complete.
Survey