Embed Size (px)
Citation preview

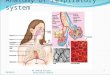
Respiratory module part 2 Lecture number 6
Dr.Ghada Al-jussani MBCHB.,FRCpath (UK)
Fellowship of Royal college of Pathologist (UK)
Iraqi board in Pathology , Jordainan Board in pathology
European Board In Pathology
Assistant Professor Consultant pathologist
Faculty of medicine ,Hashemite university

Objectives
❑ Interstitial Lung disease
❑ Idiopathic pulmonary fibrosis /Usual Interstitialpneumonia
❑ Pneumonia Syndromes
❑ Community Acquired typical pneumonia
❑ Community acquired Atypical pneumonia

Diffuse Interstitial Lung Disease
❑ Diffuse interstitial (in-tur-STISH-ul) lung disease refers to a large group of lung disorders
that affect the interstitium, which is the connective tissue that forms the support structure
of the alveoli (air sacs) of the lungs. Normally when you inhale, the alveoli fill with air and
oxygen passes into the blood stream. When you exhale, carbon dioxide passes from the
blood into the alveoli and is then expelled from the body.
❑ When interstitial disease is present, the lung becomes inflamed and stiff, preventing the
alveoli from fully expanding. This limits both the delivery of oxygen to the blood stream
and the removal of carbon dioxide from the body.
❑ As the disease progresses, the interstitium and the walls of the alveoli thicken, which
further impedes lung function.
❑ Blood tests, pulmonary function tests (spirometry), pulse oximetry, chest x-ray, chest CT,
bronchoscopy with biopsy, or surgical biopsy may be performed to help diagnose your
condition.
❑ Treatment may depend on the underlying cause of the disease and your health status.
Medication, respiratory therapy or surgery may be prescribed to help improve lung
function.

❖ Idiopathic❖ Idiopathic interstitial pneumonia is the term given to ILDs with an unknown cause.
They represent the majority of cases of interstitial lung diseases (up to two-thirds of
cases).They were subclassified by the American Thoracic Society in 2002 into 7
subgroups:
❖ Idiopathic pulmonary fibrosis (IPF): the most common subgroup
❖ Desquamative interstitial pneumonia (DIP)
❖ Acute interstitial pneumonia (AIP): also known as Hamman-Rich syndrome
❖ Nonspecific interstitial pneumonia (NSIP)
❖ Respiratory bronchiolitis-associated interstitial lung disease (RB-ILD)
❖ Cryptogenic organizing pneumonia (COP): also known as Bronchiolitis Obliterans
Organizing Pneumonia (BOOP)❖ Lymphoid interstitial pneumonia (LIP)
❖Secondary❖ Secondary ILDs are those diseases with a known etiology, including:
❖ Connective tissue and Autoimmune diseases

❖ Interstitial lung diseases can be grouped based on cause, association with other diseases, or
pathology.
❑ Interstitial lung disease may be associated with autoimmune or inflammatory diseases such
as:
❖ rheumatoid arthritis
❖ scleroderma (systemic sclerosis)
❖ polymyositis and dermatomyositis (an inflammatory disease that causes muscle weakness)
❖ inflammatory bowel disease
It may also be caused by exposure to drugs, such as:
❖ chemotherapy agents
❖ antiarrythmics (used to treat irregular heart rhythm)
❖ statins (used to lower cholesterol levels)
❖ antibiotics
It may also stem from the inhalation of substances, such as
❖ asbestos
❖ silica
❖ chemicals
❖ animal proteins
❖ mold
❖ smoke

Infection
Corona virus disease 2019
Atypical pneumonia
Pneumocystic pneumonia
Tuberculosis
ChlamydiaTrachomatus
Resoiratory syncytial virus
Malignancy
Lymphangitis carcinomatosis


❑ (Idiopathic pulmonary fibrosis) IPF is defined as a chronic
progressive fibrotic ILD, with unknown aetiology and a pattern of
usual interstitial pneumonia (UIP), which is represented by
heterogeneous lesions at different stages of evolution with foci o
proliferative fibroblasts.
❑ IPF is generally considered to be unresponsive to “standard”
therapies and has a poor prognosis, with most patients dying
within 5 years of diagnosis .
❑ In systemic sclerosis (SSc) patients, the change in the trend of
scleroderma-related deaths over the past 30 years demonstrate
that lung involvement (both pulmonary hypertension and
pulmonary fibrosis) is among the primary causes of mortality .

❑ Histopathologic classification plays a key role in separating multiple forms of
idiopathic interstitial pneumonia into clinically meaningful categories with
important differences in natural history, prognosis, and treatment.
❑ Microscopic criteria in diagnosis of these entities include the pattern and
microanatomic distribution of inflammation, fibroblast proliferation, collagen
deposition, and architectural remodeling.
❑ Usual interstitial pneumonia (UIP) defines idiopathic pulmonary fibrosis
and is the most common of the idiopathic interstitial pneumonias.
❑ UIP has distinctive morphologic features that allow precise diagnosis in
classical cases.
❑ Other forms of idiopathic interstitial pneumonia include desquamative
interstitial pneumonia, respiratory bronchiolitis–associated interstitial lung
disease, acute interstitial pneumonia, and nonspecific interstitial pneumonia.
These latter categories differ from UIP in that the histopathologic findings do
not, by themselves, allow specific diagnosis in most cases and require careful
correlation with clinical and radiologic findings.

❑ The most common symptoms of diffuse interstitial lung disease
are shortness of breath and dry cough. As the disease
progresses, weight loss, muscle and joint pain, and fatigue may
also occur.
❑ At a more advanced stage, individuals may develop an enlarged
heart, enlargement of the fingertips clubbing),
and cyanosis (blue coloration in the lips, skin and fingernails as
a result of reduced oxygen levels in the blood).
❑ Individuals might also experience nonrespiratory symptoms,
such as muscle pain, joint pain, or thickening or tightness of the
skin, particularly in the presence of autoimmune disease.

How are interstitial lungs diseases diagnosed?
Spirometry. A spirometer is a device used to
check lung function. ...
Peak flow monitoring. This device is used to measure how fast
you can blow air out of the lungs. ...
Chest X-rays. ...
Blood tests. ...
CT scan. ...
Bronchoscopy. ...
Bronchoalveolar lavage. ...
Lung biopsy.

❑ Microsopically :❑ Usual interstitial pneumonia (UIP) refers to a morphologic entity defined by a
combination of (1) patchy interstitial fibrosis with alternating areas of normal lung,
(2) temporal heterogeneity of fibrosis characterized by scattered fibroblastic foci
in the background of dense acellular collagen, and (3) architectural alteration due
to chronic scarring or honeycomb change.
❑ The term UIP is often used interchangeably with idiopathic pulmonary fibrosis
(IPF), but other clinical conditions are associated with UIP, although less
commonly, including collagen vascular disease, drug toxicity, chronic
hypersensitivity pneumonitis, asbestosis, familial IPF, and Hermansky-Pudlak
syndrome.
❑ Thus, UIP is not entirely synonymous with IPF, and diagnosis of IPF requires an
exclusion of possible underlying clinical conditions, as mentioned above

▶Pulmonary infections
▶Pneumonia

Pneumonias I
▶ Pulmonary infections in the form of pneumonia is common due to the
following reasons :
▶ 1- The epithelial surfaces of the lung are constantly exposed to many
liters of air containing various microbial contaminants .
▶2- Nasopharyngeal flora are regularly aspirated during sleep , even
by healthy persons .
▶ 3- Other common lung diseases render lung parenchyma vulnerable
to virulent organisms .

▶Pneumonia
▶Definition : Infection of the lung parenchyma.
▶May present as acute fulminant clinical disease or as a
chronic disease with a more protracted course .
▶Acute bacterial pneumonia may present as one of two
anatomic & radiographic patterns :
▶ I- Broncho-pneumonia .
▶ II- Lobar pneumonia

▶Broncho - pneumonia :
▶ Implies a patchy distribution of inflammation that
generally involves one or more than one lobe .
▶This pattern results from infection of the bronchi &
bronchioles , with extension into adjacent alveoli .
▶Lobar pneumonia :▶The contiguous airspaces of part or all of a lobe are
homogenously filled with exudate that can be
visualized by radiograph as lobar or segmental
consolidation .


▶ Pneumonia Syndromes
▶ Pneumonias can be classified into seven distinct settings in which
infections & the implicated pathogens are specific to each category .
Including :
▶ I- Community-acquired typical pneumonia .
▶ II- Community acquired atypical pneumonia .
▶ III- Nosocomial ( hospital acquired pneumonia) .
▶ IV-Aspiration pneumonia .
▶ V- Lung abscess ( Necrotizing pneumonia ) .
▶ VI- Chronic pneumonia .
▶ VII-Pneumonia in the immuno- compromised patients

▶Pneumonia Syndromes :
▶I- Community acquired typical pneumonia :
▶Most community acquired pneumonias are bacterial infections , not uncommon
this infection follows viral upper respiratory tract infection .
▶ The onset is usually abrupt , with high fever, shaking chills , pleuritic
chest pain & a productive muco-purulant cough , occasional patients
may have haemoptysis .
▶ Streptococcus pneumoniae is the most
▶ common cause of community-acquired acute pneumonia , hence called
pneumococcal pneumonia .
▶Other bacteria may be involved like , Morexella catarrhalis, Staphyllococcus
aureus , Hemophilus influenzae , Legionella pneumophila & Klebsiella as well as
Pseudomonas sp.

▶ It occurs with increasing frequency in three groups :
(1) Those with underlying chronic lung▶ diseases such as congestive heart failure(CHF) , chronic obstructive pulmonary
diseases (COPD) , or diabetes .
(2 ) Those with either congenital or acquired
immunoglobulin defects (AIDS ) .
(3) Those with decreased or absent splenic▶ function ( sickle cell disease or after splenectomy ) This occurs because the
spleen contains the largest collection of phagocytes & is therefore the major
organ responsible for removal of pneumococci from the blood .
▶ As well as it is capable of production of antibodies against encapsulated
bacteria .

▶Morphology :
▶ In this type of pneumonia both patterns lobar or bronchopneumonia may occur
▶ Bronchopneumonia being more prevalent with advanced age . Regardless to
the pattern , the lower lobes or the right middle lobe are the most frequently
involved.
▶ Before the introduction of antibiotics , the entire lobe is involved by
pneumococcal pneumoniae and evolved into four stages :
❑ Stage of congestion .
❑ Stage of red hepatization .
❑ Stage of gray hepatization .
❑ Stage of resolution .
▶ Early antibiotic therapy alters this typical progression .

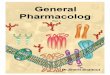
Figure 2 : Chest X-ray of patient with pneumonia. The lower lobe is
consolidated (arrow) showing dense homogenous whitish appearance of
pneumonic inflammation of the right lower lobe .

❑ I- Stage of congestion :
▶ During this stage , the affected lobe or lobes are heavy , red & boggy
▶ Histologically : vascular congestion is seen with proteinaceous fluid,
scattered neutrophils & many bacteria in the alveolar spaces .
❑ II- Stage of red hepatization :
▶Occurs within few days after infection .
▶ The lungs have a red color , liver-like consistency , the alveolar
spaces are packed with bacteria , red blood cells & fibrin with few
neutrophils .

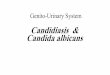
Figure 3 : Microscopic view of the lung in pneumococcal pneumonia ,stage of congestion , showing
congested capillaries in alveolar septa .

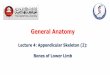
Figure 4 : Gross appearance of the lung in pneumonia stage of red hepatization,
the lung is heavy , dark red liver –like consistency .

Figure 5 : Microscopic view of lung in pneumonia , stage of red hepatization , the alveolar spaces
are filled with RBCs & bacteria , fibrin & few neutrophils .

Figure 6 : High power view of lung tissue in pneumonia ,stage arrows). ) ,RBCs seen with bacteria of
red hepatization

▶III- Stage of gray hepatization :
▶ The lung is dry , gray & firm , with a liver like consistancy because the red cells
are lysed while the fibrino- suppurative exudate persists within the alveoli
.Microscopically: the alveoli are filled with neutrophils & scanty bacteria & RBCs.
▶IV- Stage of resolution :▶ Follows uncomplicated cases as the exudates within alveoli are enzymatically
digested to produce granular semi fluid debris that is resorbed or ingested by
macrophages , coughed out or may be organized by fibroblasts growing into it .
▶ The pleural reaction includes fibrinous or fibrino-purulant pleuritis which may
similarly resolve , or undergo organization , leaving fibrous thickening or
permanent adhesions .

Figure 7 : Gross appearance of lobar pneumonia ,showing homogenous gray
consolidation of the entire lower lobe of the lung (stage of gray hepatization ) .

Figure 8 : Microscopic view (high power) of lung tissue in stage of gray hepatization showing
numerous neutrophils (arrows) & macrophages within alveolar spaces ,congested blood vessels
(arrow head ) seen in alveolar septa ..

Figure 9 : Microscopic view of lung tissue in stage of gray hepatization of pneumococcal
pneumonia,the alveolar spaces contain numerous neutrophils with fibrin. Alveolar septa show

Figure 10 : Microscopic view of lung tissue with features of pneumonia showing organization with
fibrous tissue deposition on fibrin in alveolar spaces , occurring in unresolved pneumonia .

▶ In broncho-pneumonia pattern :
▶ The foci of inflammatory consolidation distributed in patches throughout one or several lobes most frequently bilateral & basal .
▶Well-developed lesions 3 or 4 cm. in diameter are slightly elevated & are gray –red to yellow .
▶ Confluence of these foci may occur in severe cases producing the appearance of
lobar consolidation .
▶The lung substance surrounding the areas of consolidation is usually hyperemic & edematous , but the larger intervening areas are generally normal
▶ Pleural involvement is less common than in lobar pneumonia .
▶Histologically : The reaction consists of focal suppurative exudate that
fills the bronchi , bronchioles and the adjacent alveolar spaces .
▶With appropriate therapy complete restitution of the lung is the rule for both forms of pneumococcal pneumonia .

Figure 11 : Gross appearance of the lung with broncho-pneumonia ,showing patchy
involvement of lung tissue by whitish areas of inflammation surrounded by red congested
lung tissue .

Figure 12 : Microscopic view of lung tissue showing broncho-pneumonia , supurative inflammation
of the bronchiole with extension of the inflammation to the surrounding alveoli, distended alveoli
of the normal lung tissue seen at the margin.

Figure 13 : Microscopic view of lung tissue in broncho-pneumonia. Dense supurative
exudate fill the lumen of inflamed bronchiole ,extending to surrounding lung tissue .

Figure 14 : Microscopic view of lung involved in broncho-
pneumonia .

▶Complications of severe cases may include :
(1) Abscess formation results from tissue destruction and necrosis .
(2)Empyema which results from accumulation of suppurative material
in the pleural cavity .
(3)Organization of intra-alveolar exudate may convert areas of the
lung into solid fibrous tissue
(4)Bacteremic dissemination may lead to meningitis , arthritis or
infective endocarditis .
▶ The complications are much more likely with serotype 3
pneumococci.

▶Diagnosis :
▶First from the symptoms ,Fever ,Rigor ,cough, difficulty in breathing ,sputum with hemoptysis .
▶Chest X-ray
▶Examination of gram-stained sputum is an important step in the diagnosis .
▶During early stages of illness, blood culture may be positive in 20%-30% of cases .
▶Antibiotic sensitivity test must be performed .
▶Commercial pneumococcal vaccines containing capsular
polysaccharides from the common serotypes of bacteria are
available, and there use in those at risk is recommended .

❖Haemophilus influenzae pneumonia :
▶Gram negative micro-organisms ,both encapsulated &
unencapsulated forms are important cause of the
community acquired pneumonia ,the former can cause a
life-threatening form of pneumonia & meningitis in children, often following a viral respiratory tract infections .
▶Adults at risk of infection are those with chronic pulmonary
diseases as chronic bronchitis , cystic fibrosis and
bronchiectasis .
▶ It is the most common cause of bacterial exacerbation in
COPD .

Moraxilla catarrhalis :▶ It is being recognized as a common cause of bacterial
pneumonia in the elderly , and it is the second commonest cause of bacterial exacerbation in COPD in adults .
Staphyllococus aureus :▶ Is an important cause of secondary bacterial pneumonia in
children & healthy adults following viral respiratory diseases as measles in children & influenza both in children & adults .
▶ It is associated with high incidence of complications as lung abscess & empyemia .
▶ Staphylococcal pneumonia occurring in association with rightsided staphylococcal endocarditis is a serious complication ofintravenous drug abuse .

❖Klebsiella Pneumonia :
▶ Is the most frequent cause of gram negative bacterial
pneumonia.
▶ It frequently affect debilitated and mal nourished persons
particularly chronic alcoholics .
▶Thick & gelatinous sputum is characteristic because the
micro organism produces an abundant viscid capsular
polysaccharides, which the individual have a difficulty to
cough out .

❖Pseudomonas aeroginosa :▶ Associated with cystic fibrosis , it is most commonly seen in
nosocomial settings , it is common in people who are neutropenic usually secondary to chemotherapy , in victims of extensive burn & in those requiring mechanical ventilation .
▶ Psudomonas aeroginosa have a tendency to invade blood vessels at
the site of infection with consequent intrapulmonary spread .
▶ Pseudomonas bacteremia is a fulminant disease , death occurs within few days .
▶Histological examination :
▶ Reveals coagulation necrosis of lung parenchyma, with micro organisms invading walls of blood vessels causing pseudomonas vasculitis .

Figure 15 : Microscopic view of lung tissue in pseudomonas pneumonia,showing
involvement of blood vessels by bacteria ,I . e pseudomonas vasculitis & focal
infarction .

❖Legionella pneumophila :
▶ Is the agent of legionnaire disease which is an epidemic & sporadic form of pneumonia .
▶Pontiac fever : Is a self –limited upper respiratory tract infection caused by L. pneumophila without pneumonic symptoms .
▶Legionella pneumophila flourishes in artificial aquatic environment such as water-cooling towers & within the tubing systems of domestic water supplies .
▶The mode of transmission is thought to be either inhalation of aerosolized organisms or aspiration of contaminated drinking water .

▶ It is common in persons with predisposing conditions such
as cardiac, renal or immunologic or hematologic diseases .
▶Organ-transplant recipients are particularly susceptible .
▶This type of pneumonia can be severe necessitating
hospitalization , fatality may reach 30%-50% in immuno-suppressed individuals .
▶Diagnosis is by demonstration of Legionella antigen in the
urine of the patient or by fluorescent antibody test on sputum samples .
▶Sputum culture is the gold standard of diagnosis .