Upload
antoniocarpinto9542
View
55
Download
12
Embed Size (px)
Citation preview
Respiratory conditions & Immunological disorders
Wellspring Seminars Module 9Slide # 1 of 292NOTICE The information in this CD is subject to change withoutnotice. This guide is provided without warranty of any kind, and Wellspring Seminars disclaims all warranties,express or implied, including any implied warranty ofmerchantability for fitness for a particular purpose. Wellspring Seminars shall not be liable for technical or editorialomissions made herein; nor for incidental orconsequential damages resulting from the furnishing,performance, or use of this material. This guide is protected by copyright. No part of thisguide may be photocopied or reproduced in any formwithout prior written consent from Wellspring Seminars .
Copyright (c) 2008 Wellspring Seminars , All Rights Reserved. Thisproduct was made in the United States of America. 1Ancestral Energy
Classical Clinical Acupuncture
Respiratory ConditionsInstructor Bonnie L Walker, DC L Ac
Module 10 - Advanced Series
Wellspring Seminars2348 Hwy 105, Suite 9Boone, NC 28607828-265-0001
InstructorBonnie L Walker, DC, Dipl Ac, L Ac Classical Clinical Acupuncture
Module 9Respiratory & Immune ConditionsWellspring Seminars Module 9Slide # 3 of 2923Who Am I ?Why Am I HereBonnie L. Walker, BS, DC, Dipl Ac, L Ac2348 NC Hwy 105, Suite #9Boone, NC 28607email: [email protected] 828-265-0001www.wellspring-healing.comWellspring Seminars Module 9Slide # 4 of 2924No animations neededLicensed to practice acupuncture by the North Carolina Acupuncture Licensing Board: L AcBoard Certified in Acupuncture by the National Commission for the Certification of Acupuncture and Oriental Medicine (NCCAOM): Dipl AcMaster of Acupuncture Diploma, Jung Tao School of Classical Chinese Medicine: M AcLicensed to practice chiropractic by the North Carolina Board of Chiropractic Examiners: DCBoard Certified in Chiropractic by the National Board of Chiropractic Examiners (NBCE)Doctor of Chiropractic (DC), Bachelor of Science (BS) Human Biology, National College of Chiropractic Founder & sole practitioner: Wellspring Chiropractic and Acupuncture Center, PA, Boone, NC. Founding faculty, Clinical Supervisor, Biomedical Dean, Jung Tao School of Classical Chinese Medicine (JTS)JTS Instructor in Point Location, General Anatomy, Clinical Skills, Integrative Medicine, TaijiquanNew River Behavioral Health: Board member Slide # 5 of 292Curriculum Vitae5My education has included 4 years personal apprenticeship with Dr Sean Marshall, personal instruction with Dr Nguyen van Nghi, and 10 years ongoing advanced training with Dr Tran viet Dzung.In addition, I was an anatomy teaching assistant for 4 years at National, and have taught seminars in Nimmo Receptor-Tonus Technique and Clinical Kinesiology.My education has included 4 years personal apprenticeship with Dr Sean Marshall, personal instruction with Dr Nguyen van Nghi, and 10 years ongoing advanced training with Dr Tran viet Dzung.In addition, I was an anatomy teaching assistant for 4 years at National, and have taught seminars in Nimmo Receptor-Tonus Technique and Clinical Kinesiology.In my spare time, I enjoy playing & experiencing music, enjoying nature, my family & good friends. Current ResearchNormal Respiratory PhysiologyNormal Immune PhysiologyReview Of Pertinent EnergeticsBronchitisAsthmaPneumoniaAllergiesURI, Colds, FluImmune DeficiencyAutoimmune ConditionsWellspring Seminars Module 9Slide # 6 of 292Respiratory & Immune Conditions6Current Research The bronchodilating effect of acupuncture in patients with acute asthmaTakishima T, Mue S, Tamura G, Ishihara T, Watanabe K 1982 Annals of Allergy 48:44--49One study showed acupuncture to be beneficial for cancer-induced breathlessness (Filshie et al 1996)Fourteen out of 20 patients reported marked symptomatic benefits and there was statistically significant improvement in breathlessness scores, relaxation, anxiety and respiratory rate. The benefits compared favorably with current treatmentSlide # 7 of 292Wellspring Seminars Module 97Current Research The effect of acupuncture on pulmonary function in bronchial asthma. Virsik K, Kiristutek P, Bangha 0, Urban S 1980. Progress in Respiratory Research 14:271-275.Controle spirometrique clans la maladie asthmatique des effets de la puncture de points douloureux thoraciques. Luu M, Maillard D, Pradalier A, Bourcau F 1985 Respiration 48:340-345Effect of acupuncture on bronchial asthma. Yu D Y C, Lee S P 1976 Clinical Science and Molecular Medicine 51: 503-509.Wellspring Seminars Module 9Slide # 8 of 2928Current Research Controlled trial of acupuncture for disabling breathlessness. Jobst K, Chen J 11, McPherson K et al 1986. Lancet 2:1416-1419.Attenuation of exercise induced asthma by acupuncture. Fung K P, Chow 0 K W, So S Y 1986 Lancet 2: 1419-1422.Acupuncture and bronchial asthma. Christensen P A, Laursen L C, Taudorf E, Sorensen S C, Weeke B 1984 Allergy 39:379-385Wellspring Seminars Module 9Slide # 9 of 2929Current Research Comparison of real and placebo acupuncture in histamine-induced asthma. A double-blind crossover study. Tandon M K, Soh P F T 1989 Chest 96:102-105A Case of Chronic Obstructive Pulmonary Disease (COPD) Successfully Treated by AcupunctureSuzuki M, et al. Department of Oriental Medicine, Gifu University of Medicine.Wellspring Seminars Module 9Slide # 10 of 29210A 66-year-old man visited the hospital with symptoms of breathlessness with exercise. In spite of medication, his general condition worsened. Subsequently, a series of acupuncture treatments was started on October 27, 2001. He had level III breathlessness on JRS classification prior to acupuncture treatment. This research design was used to detect the specific efficacy of acupuncture treatment after ten acupuncture treatments over two months, his walking distance, Borg scale and respiratory function were improved compared with before treatment. These findings suggest that acupuncture treatment may be efficacious for advanced cases of COPD.
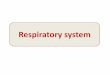
The Gifu University Hospital reported a COPD patient whose respiratory symptoms were improved by acupuncture. Points used:Ki 3 (Fuliu)Lu 9 (Taiyuan)Lu 1 (Zhongfu)CV 12 (Zhongwan)CV 4 (Guanyuan)Bl 13 (Feishu) Bl 23 (Shenshu) Current Research Wellspring Seminars Module 9Slide # 11 of 29211Normal Respiratory PhysiologyRespiratory mechanismLungsDiaphragmIntercostal muscles: internal & externalSlide # 12 of 293Wellspring Seminars Module 912During quiet breathing, the predominant muscle of respiration is the diaphragm. As it contracts, pleural pressure drops, which lowers the alveolar pressure, and draws air in down the pressure gradient from mouth to alveoli. Expiration during quiet breathing is predominantly a passive phenomenon, as the respiratory muscles are relaxed and the elastic lung and chest wall return passively to their resting volume, the functional residual capacity. However, during exercise, many other muscles become important to respiration. During inspiration, the external intercostals raise the lower ribs up and out, increasing the lateral and anteroposterior dimensions of the thorax. The scalene muscles and sternomastoids also become involved, serving to raise and push out the upper ribs and the sternum. During active expiration, the most important muscles are those of the abdominal wall (including the rectus abdominus, internal and external obliques, and transversus abdominus), which drive intra-abdominal pressure up when they contract, and thus push up the diaphragm, raising pleural pressure, which raises alveolar pressure, which in turn drives air out. The internal intercostals assist with active expiration by pulling the ribs down and in, thus decreasing thoracic volume. A pressure gradient is required to generate flow. In spontaneous respiration inspiratory flow is achieved by creating a sub-atmospheric pressure in the alveoli (of the order of -5cmH2O during quiet breathing) by increasing the volume of the thoracic cavity under the action of the inspiratory muscles. During expiration the intra-alveolar pressure becomes slightly higher than atmospheric pressure and gas flow to the mouth results.
Normal Respiratory PhysiologyAccessory myos of respiration ScalenesSCMRectus abdominusInternal & external obliquesTransversus abdominus
Wellspring Seminars Module 9Slide # 13 of 29313During quiet breathing, the predominant muscle of respiration is the diaphragm. As it contracts, pleural pressure drops, which lowers the alveolar pressure, and draws air in down the pressure gradient from mouth to alveoli. Expiration during quiet breathing is predominantly a passive phenomenon, as the respiratory muscles are relaxed and the elastic lung and chest wall return passively to their resting volume, the functional residual capacity. However, during exercise, many other muscles become important to respiration. During inspiration, the external intercostals raise the lower ribs up and out, increasing the lateral and anteroposterior dimensions of the thorax. The scalene muscles and sternomastoids also become involved, serving to raise and push out the upper ribs and the sternum. During active expiration, the most important muscles are those of the abdominal wall (including the rectus abdominus, internal and external obliques, and transversus abdominus), which drive intra-abdominal pressure up when they contract, and thus push up the diaphragm, raising pleural pressure, which raises alveolar pressure, which in turn drives air out. The internal intercostals assist with active expiration by pulling the ribs down and in, thus decreasing thoracic volume. A pressure gradient is required to generate flow. In spontaneous respiration inspiratory flow is achieved by creating a sub-atmospheric pressure in the alveoli (of the order of -5cmH2O during quiet breathing) by increasing the volume of the thoracic cavity under the action of the inspiratory muscles. During expiration the intra-alveolar pressure becomes slightly higher than atmospheric pressure and gas flow to the mouth results.
Neural Control of RespirationArterial pp O2/CO2 is maintained at relatively constant levelsCNS regulates alveolar function on demandRespiratory center feedback regulates alveolar ventilation Wellspring Seminars Module 9Slide # 14 of 29214Motor pathwaysThe diaphragm is the main muscle generating the negative intrathoracic pressure that produces inspiration Innervation is from the phrenic nerves (C3-5) with contraction moving the diaphragm downwards Additional inspiratory efforts are produced by the external intercostal muscles (innervated by their intercostal nerves T1-12) and the accessory muscles of respiration (sternomastoids and scalenes)During quiet breathing expiration is a passive process, relying on the elastic recoil of the lung and chest wall. When ventilation is increased, such as during exercise, expiration becomes active with contraction of the muscles of the abdominal wall and the internal intercostals. Central controlThe mechanism by which respiration is controlled is complex. There is a group of respiratory centres located in the brainstem producing automatic breathing activity. This is then regulated mainly by input from chemoreceptors (see below). This control can be overridden by voluntary control from the cortex. Breath-holding, panting or sighing at will are examples of this voluntary control. The main respiratory centre is in the floor of the 4th ventricle, with inspiratory (dorsal) and expiratory (ventral) neurone groups. The inspiratory neurones fire automatically, but the expiratory ones are used only during forced expiration. The 2 other main centres are the apneustic centre, which enhances inspiration, and the pneumotaxic centre, which terminates inspiration by inhibition of the dorsal neurone group above.The chemoreceptors that regulate respiration are located both centrally and peripherally. Normally control is exercised by the central receptors located in the medulla, which respond to the CSF hydrogen ion concentration, in turn determined by CO2, which diffuses freely across the blood-brain barrier from the arterial blood. The response is both quick and sensitive to small changes in arterial CO2 (PaCO2 ). In addition, there are peripheral chemoreceptors located in the carotid and aortic bodies most of which respond to a fall in O2, but some also to a rise in arterial CO2. The degree of hypoxia required to produce significant activation of the O2 receptors is such that they are not influential under normal circumstances, but will do so if profound hypoxia ( 2 wk because of airway irritation, some patients benefit from a few days of inhaled corticosteroids.
Oral antibiotics are typically not used except in patients with pertussis or in patients with COPD who have at least 2 of the following: Increased coughIncreased dyspneaIncrease in sputum purulenceDrugs include amoxicillin AMOXILTRIMOX500 mg po tid for 7 days, doxycycline PERIOSTATVIBRAMYCIN100 mg po bid for 7 days, azithromycin ZITHROMAX500 mg po once/day for 4 days, or trimethoprim-sulfamethoxazole 160/800 mg po bid for 7 days.Energetic Etiology & Pathogenesis: BronchitisEmptiness of LungsDeficient Lung YinDeficient Lung YangExternal Pathogenic energy can penetrateClinical presentation of an ExcessFalse Excess if due to internal deficiencyWellspring Seminars Module 9Slide # 123 of 292123Viruses live in cold damp areas1st attack sinuses, nasopharynx, upper airways, then descends to bronchii
Penetration of ext PE Wind Cold2 kinds of virus:upper airway; corono virus, adenovirus, rhinoviruslower airway; influenza B & A, parainfluenza 3, respiratory syncytial virusAll thrive in cold damp areas, thus Fall & Winter are flu season.Viral BronchitisDry cough, worse in cold dry airThoracic pain with coughingHoarse voicePharyngitisSore throatChillsFatigueLack of appetiteHeadacheMuscle painWellspring Seminars Module 9Slide # 124 of 292124Bacterial bronchitis is Much more seriousUnderlying condition of chronic bronchitis can worsen any acute bronchitis
Smoke & MucusSmoking, irritants, ozoneCigarette smoke decreases production of healthy mucusIncreases production of poor quality mucusThickened mucus leads to obstruction & COPD
Wellspring Seminars Module 9Slide # 125 of 292125Chemical BronchitisHiatal herniaSubsternal painGERDChemically burn, inflame bronchiiInduce chronic bronchitis
Wellspring Seminars Module 9Slide # 126 of 292126Pathogenic HeatALL of these external irritants are HEATHeat attacks the Blood via 4 Energetic LayersWeiQiYingBloodWellspring Seminars Module 9Slide # 127 of 292127Pathogenic HeatOnce Pathogenic Energy attacks the Blood, it attacks the HeartWhen Heart is attacked, the Mental is disturbedWhen the Mental is disturbed, its ominousWellspring Seminars Module 9Slide # 128 of 293128Energetic Layers and AssociationsSlide # 129 of 292Wellspring Seminars Module 9
129Wei & MucusWei circulates superficial & deepDeep in the mucosaMembranes surrounding each organHeat attacks Wei @ the mucosaMucosa hyper-secretes non functional, poor quality mucusDecreased humidityDecreased defenseCilia become paralyzedMucus stagnates & obstructsCondition becomes chronic
Wellspring Seminars Module 9Slide # 130 of 292130Deficient Lung Yin: Chronic BronchitisClinical presentation:Dry coughBloody, scant expectorationFever, night sweatsRed cheeksHeat in bonesDry mouth & throatVoice hoarsePulse rapidTongue red, thin coatWellspring Seminars Module 9Slide # 131 of 293131Deficient Lung Yin: Chronic BronchitisClinical presentation of evolving pathologyIncreased mucus productionProductive coughObstruction, COPDInsufficient ventilationDeficient gaseous exchangeRespiratory insufficiencyHypoxiaHypercapneaHypoventilation
Wellspring Seminars Module 9Slide # 132 of 292132This is the picture of def Lung Yin if it left untreated or improperly treated; this is what we are working to preventDeficient Lung Yin: Chronic BronchitisDeficient Lung Yin can progress to Deficient Kidney Yin, which can evolve intoEmpty FireKidney Yin deficiency with False Heat signsWellspring Seminars Module 9Slide # 133 of 293133Deficient B lymph, humoral immunity is def Water = def Ki yin, very grave conditionEsp in immunocompromised, congenital IgG def
Stimulation Inhibition CycleWellspring Seminars Module 9Slide # 134 of 293134Deficient Lung Yin: Chronic Bronchitis: TreatmentChronic cough, bronchitisMaximally tonify the LungsBl 13, Lu 1, Lu 9Entry-Exit point of LungsBl 42Tonify Kidney YinCV 4, Bl 23, Ki 3, Ki 7Tonify Kidney YangGV 4, CV 4
Wellspring Seminars Module 9Slide # 135 of 293135Deficient Lung Yang: Acute BronchitisOften due to Deficiency of Spleen Yang causing Deficiency of Lung YangClinical presentationProductive cough (mucusy, damp = Humidity)Dyspnea, short respirationsSweating (spontaneous, daytime)Weakness, fatiguePale complexionWeak, empty pulseTongue paleWhitish coatWellspring Seminars Module 9Slide # 136 of 292136Daytime sweating indicates deficient Lung YangNight sweats indicate deficient Lung Yin
Deficient Lung Yang: Acute Bronchitis: TreatmentShu / Mu / Yuan LungBl 13, Lu 1, Lu 9Treat the MentalEntry Exit PoBl 42Wellspring Seminars Module 9Slide # 137 of 292137Deficient Lung Yang: Acute Bronchitis: TreatmentShu / Mu / Yuan Spleen / StomachBl 20, Li 13, Sp 3Bl 21, CV 12, St 42, St 36Tonify Yang MingCV 12, St 25Treat the MentalEntry exit Yi Bl 49Wellspring Seminars Module 9Slide # 138 of 292138Deficient Lung Yang: Acute Bronchitis: TreatmentMove the ThoughtsSp 1, GB 40, Ki 3Transform PhlegmSt 40, St 37, Sp 3Wei QiCV 22, CV 23, St 5, St 9CV 17Moxa Back Shu points from T1 to T7Treat the KidneysShu / Mu / Yuan Ki Yin & YangCV 4, Bl 23, Ki 3CV 4, GV 4, Bl 64Wellspring Seminars Module 9Slide # 139 of 292139CV 17 stimulates the dorsal respiratory nucleus, Zhong Qi, stim diaphragmatic movement, inspirationzone of transit of wei to chest
Adjunctive Therapies: BronchitisSTOP SMOKING !!!NADABreatheQigongYoga breathingRebirthing, conscious connected breathing, circular breathing, Holotropic breathworkAddress underlying allergies, toxin exposureEmotional counseling, grief supportWellspring Seminars Module 9Slide # 140 of 293140AsthmaWellspring Seminars Module 9Slide # 141 of 293Picture Removed141Clinical Presentation: AsthmaDiffuse airway inflammation triggered by stimuli resulting in bronchoconstriction Contraction of smooth muscles in bronchiolesSymptoms and signsDyspneaChest tightnessCoughWheezing Wellspring Seminars Module 9Slide # 142 of 292142Diffuse airway inflammation caused by triggering stimuli resulting in partially or completely reversible bronchoconstriction. IS LOW ENDOGENOUS CORTISOL A RISK FACTOR FOR ASTHMA? ARTICLE TOP ARTICLE REFERENCES To the Editor: In their paper, Clark and colleagues (1) suggest that low cortisol may relate to pulmonary emphysema. Previous findings in male veterans reported associations of cortisol with low FEV1 or longitudinal change in lung function (2), but were not confirmed by Clark and colleagues. Asthma was an exclusion criteria for both previous reports. The relationships of endogenous cortisol with inflammatory obstructive diseases, such as emphysema or asthma, have not been studied thoroughly until now. We measured serum cortisol in a population of 349policemen 33to 62years of age (3) (meanSD: 13.20.4g/100 ml) at the time of the examination of the subject, i.e., between 8:00 A.M. and 4:30 P.M. The analysis was conducted in 270men, after exclusion of men who were working night shifts, sleeping less than six hours per night or taking sleeping pills. Cortisol was, as expected, related to the hour of blood sampling (p Sp 3, St 37Wellspring Seminars Module 9Slide # 161 of 292161Treatment Strategies: AsthmaDing Chuan EMERGENCY POINTEar Stop AsthmaPurification of Lungs: Thread Lu 9 to Lu 8, 2 c past Lu 8Cranial Thoracic zoneWellspring Seminars Module 9Slide # 162 of 292CURIOUS POINTS FOR ASTHMA162Adjunctive Therapies: AsthmaQi GongRebirthing, conscious connected breathing, yoga breathing, etcStress managementIdentification & avoidance of triggersAnti-inflammatory dietSupplements:Fish oil caps 1000 mg 3-6/day
Wellspring Seminars Module 9Slide # 163 of 292163Pneumonia Wellspring Seminars Module 9Slide # 164 of 293Picture Removed164Clinical Presentation: Pneumonia ProgressiveFeverChillsMalaiseDry coughRhinopharyngeal infectionRalesXR opacity especially at the hilumWellspring Seminars Module 9Slide # 165 of 292165Biomedical Etiology & Pathogenesis : Pneumonia PneumoniaAcute inflammation of the lungs Caused by infection Infections affect alveoli & bronchiolesLobarInterstitialAcute pneumonia is more common in MalesElderlyImmunocompromised patients
Wellspring Seminars Module 9Slide # 166 of 292166Causes, symptoms, treatment, preventive measures, and prognosis differ depending on whether the infection is bacterial, viral, fungal, or parasitic; whether it is acquired in the community, hospital, or nursing home; and whether it develops in a patient who is immunocompetent or immunocompromised.
Biomedical Etiology & Pathogenesis: Pneumonia Causes of PneumoniaViralMost commonVirus thrive in cold environmentsSelf limiting, resolve in 1 weekBacterialMore ominous
Wellspring Seminars Module 9Slide # 167 of 292167Causes, symptoms, treatment, preventive measures, and prognosis differ depending on whether the infection is bacterial, viral, fungal, or parasitic; whether it is acquired in the community, hospital, or nursing home; and whether it develops in a patient who is immunocompetent or immunocompromised.
Virus thrive in cold environments: thus viral pneumonia results from a wind cold invasionFlu, wind cold turn into tai yang syndrome
Biomedical Diagnosis : Pneumonia Initial diagnosis is usually based on chest x-ray.Wellspring Seminars Module 9Slide # 168 of 293168Biomedical Treatment : Pneumonia AntibioticsNSAIDSCortisone Antipyretic RxAntitussive Rx or OTCBed restSupportive care
Wellspring Seminars Module 9Slide # 169 of 292169Energetic Etiology & Pathogenesis : Viral Pneumonia Virus thrive in cold environmentsViral pneumonia results from a Wind Cold invasionFlu, Wind Cold turn into Tai Yang syndromeWellspring Seminars Module 9Slide # 170 of 292170If Tai Yang syndrome is not stopped, external Pathogenic Energy can penetrate into Lungs, causing disturbance of the Lungs themselves. Ling Shu/Shang Han Lung
Treatment Strategies: Viral Pneumonia Distribute the WeiGV 14Stimulate Lung functionBl 13Purification (Cooling) of LungsLI 4, LI 11, GV 14, St 36Tonify the LungsShu/Mu/Yuan LungsBl 13, Lu 1, Lu 9Zhong QiCV 6, CV 17 PoBl 42, Lu 10, Entry-Exit point for PoWellspring Seminars Module 9Slide # 171 of 292171Bacterial PneumoniaPneumococcal pneumoniaInflammation of the alveoli & capillary membraneIncreased permeability of the membranePenetration of liquids & Blood (Heat & Fire)Infection spreads to other alveoli, lobe, lungWellspring Seminars Module 9Slide # 172 of 293172Ominous prognosisBacterial PneumoniaPneumococcal pneumoniaGaseous exchange decreasesDecreased alveolar ventilationHypoxiaHypercapnea% O2 saturation diminishes (down to 78%- 60%)Diminished OxygenationUtilizationRespiration
Wellspring Seminars Module 9Slide # 173 of 292173Ominous prognosisClinical Presentation : Bacterial PneumoniaSudden, Violent onsetChillsHigh feverCoughPurulent sputumThoracic painFever blistersRalesFremitus, resonanceXR opacityIncreased PMNs & WBCsWellspring Seminars Module 9Slide # 174 of 292174Biomedical Treatment: Bacterial PneumoniaCortisoneAntibioticsVaccinesAntitussivesAntipyretics
Wellspring Seminars Module 9Slide # 175 of 292175Energetic Etiology & Pathogenesis: Bacterial PneumoniaEnergy of Ying & Blood diminishesDecreased formation of Organ JingResulting in Poor quality Ying & BloodInsufficient quantity & quality of WeiPoor quality & quantity of Acquired JingPoor maintenance of Innate JingWellspring Seminars Module 9Slide # 176 of 293176Energetic Etiology & Pathogenesis: Bacterial PneumoniaExternal invasion of Pathogenic Wind HeatHeat attacks the BloodPenetrates throughWeiDefense, warms skin, flesh & dermisOpens & closes pores (Lu)QiMixture of Ying & WeiYingNutritive energy, circulates in Principal channelsBloodCirculates deep, near boneWellspring Seminars Module 9Slide # 177 of 292177Energetic Etiology & Pathogenesis: Bacterial PneumoniaWen Rei: Wind Heat (moderate Heat)Penetrates when Lung Jing is deficientAnatomic Jing of the Lungs forms epidermal barrierKeratinocytes, melanocytesWen Rei attacks epidermal layer2 clinical presentations:Attack on pilocutaneous layerDirect attack on LungsWellspring Seminars Module 9Slide # 178 of 292178Heat Attack On Pilocutaneous LayerSigns / SymptomsFeverSlight aversion to coldHeadacheWellspring Seminars Module 9Slide # 179 of 293179Heat Attack On Pilocutaneous Layer: TreatmentTreatmentSudorificationRelease the ExteriorLu 7LI 4Bl 12GB 20Lu 8SJ 1Wellspring Seminars Module 9Slide # 180 of 293180Heat Attack On Pilocutaneous Layer: TreatmentExteriorize the WeiGV 14Tonify Yang MingLu 7, LI 4, St 36, Sp 6Tonify the LungsShu/Mu/Yuan LungsBl 13, Lu 1, Lu 9Zhong QiCV 6, CV 17PoBl 42, Lu 10, Entry-Exit PoTonify Ki Yin & YangBl 23, Bl 52, Ki 3, CV 4, GV 4Wellspring Seminars Module 9Slide # 181 of 292181Lung System: Excess Wind HeatWhen Pathogenic Energy reaches Qi layerAffects all organs & bowels4 clinical presentations:Compression of Heat in ThoraxObstruction of Lung energy by HeatObstruction of Lung Energy by Phlegm FireHeat Attack on the Yang Ming
Wellspring Seminars Module 9Slide # 182 of 292182Pneumonia occurs when Heat attacks the YingLung System: Excess Wind HeatCompression of Heat in thorax Symptoms Continuous fever, thoracic oppression, irritability, anxietyTreat by Purification (Clearing Heat)For high continuous fever LI 4, LI 11, St 36, GV 14 Recheck temp in 10-15 mineffect is immediateRelease the Yang from the Thorax CV 17, XB 6, Sp 1CV 22, Ki 27, Lu 1, St 13Wellspring Seminars Module 9Slide # 183 of 292183Obstruction Of Lung By Excess Wind HeatObstruction of Lung energy by HeatDyspneaContinuous high fever, sweating, thoracic oppression, irritability, anxietyLung Energy cant descend due to Rei Heat destroying and weakening the LungsCausing a disconnection of Root-Summit relationship of Ki-LuTreat Lung and Kidney by Purification for continuous feverLu 7, LI 4, LI 11, GV 14, Lu 8, SJ 1Release the Yang from the Thorax CV 17, XB 6, CV 22, Ki 27, Lu 1, St 13Wellspring Seminars Module 9Slide # 184 of 292184continuous fever, thoracic oppression, irritability, anxiety carry over from compression of Heat in thoraxObstruction Of Lung By Excess Wind HeatTonify the LungsShu/Mu/Yuan LungsBl 13, Lu 1, Lu 9Zhong QiCV 6, CV 17PoBl 42, Lu 10, Entry-Exit PoWellspring Seminars Module 9Slide # 185 of 293185Obstruction Of Lung By Excess Wind HeatMaximally tonify the KidneysShu/Mu/YuanBl 23, CV 4, Ki 3ZhiBl 52, Ki 3, Entry-exit ZhiZhong QiCV 6, CV 4Wellspring Seminars Module 9Slide # 186 of 293186Obstruction Of Lung Energy By Phlegm-fireLung energy cant descend to the Kidneys Goes to Large IntestineSame symptoms as above Fever and dyspneaPlus headache, constipationWellspring Seminars Module 9Slide # 187 of 292187Obstruction Of Lung Energy By Phlegm-FireTreatment strategyReestablish the circulation of Lung energy to Kidney Purification Release Yang from ThoraxLung maxKidney maxMetabolize (transform) the PhlegmSt 40, St 36, Sp 3Treat the constipationShu/Mu/Yuan LI, St,& SISt 39, St 36, St 37, CV 5, SJ 6Wellspring Seminars Module 9Slide # 188 of 292188Heat Attack on the Yang MingWithout Form Attacks LI 20 > St 1> Bl 1Yang Ming fears HeatSymptoms Red faceMalar flushThirstConjunctivitisFever
Wellspring Seminars Module 9Slide # 189 of 292189Thirst because organic liquids are being attackedWithout Form means without distortion in or penetration into structureHeat Attack on the Yang MingWithout Form Treatment strategy Purification (Clear Heat) LI 4, LI 11, St 36, GB 20Activate production of Organic LiquidsShu/Mu/Yuan SpleenKidneySan Jiao CV 9, CV 6Wellspring Seminars Module 9Slide # 190 of 292190Thirst because organic liquids are being attackedHeat Attack on the Yang MingWith form Heat has penetrated the Stomach organAbove symptoms of Red face, thirst, conjunctivitisPlus tidal fever increasing in evening, constipation As it penetrates SpleenHot diarrheaSoft stools with foul odorBurning anusDeliriumMental symptomsWellspring Seminars Module 9Slide # 191 of 292191When the disease progresses to the point it affects the consciousness, its becoming much worseWith Form means it has an impact on structural components, SpleenHeat Attack on the Yang MingTreatment strategyPurgationPurification (Clear Heat)Harmonize Yang Ming, Spleen & Small IntestineBl 25, St 25, LI 4Bl 21, CV12, St 42Bl 20, Li 13, Sp 3Bl 27, CV 4, St 45 or St 44Sp 9, CV 5, SJ 6St 37, St 36, St 39Wellspring Seminars Module 9Slide # 192 of 292192When the disease progresses to the point it affects the consciousness, its becoming much worseHeat Attack on the SpleenIf Heat progresses toward SpleenSymptoms of watery hot diarrhea with nauseating odor, heat in anusTreatment strategy Stop the diarrhea and restore digestive function Shu/Mu/Yuan LI, St, SpTonify St 36, disperse Sp 9Lower He Sea pts St 36, 37, 39 , & Sp 6 Above 4 can stand alone for dysenteryDirect moxa on ginger or onion slice on CV 8Wellspring Seminars Module 9Slide # 193 of 292193Maximum improvement noted in 1 to 3 treatments
External Pathogenic Heat Invasion Of The Ying LevelSymptoms PM tidal feverContinuing mental symptoms with increasing anxiety & agitation to the point of delirium Tip of the tongue redMinor cutaneous eruptionsWellspring Seminars Module 9Slide # 194 of 292194This is pneumoniaExternal Pathogenic Heat Invasion of the Ying LevelTreatment strategyClear Heat LI 4, LI 11, GV 14, SJ 1Circulate the Ying Lu 7, LI 4, LI 11, SI 3, SJ 5, St 36, Bl 60, GB 43Calm the SpiritGV 20, Yin Tang, GB 16, GV 23, CV 17, He 7Access the Zhong QiCV 17, CV 12, CV 4, CV 6Wellspring Seminars Module 9Slide # 195 of 292195This is pneumoniaSyndrome Of Lung HeatDermatological symptoms Psoriasis, eczema, smallpox, chicken pox, fever blisters Eruptive fever, thoracic oppressionDyspneaWellspring Seminars Module 9Slide # 196 of 292196Syndrome of Lung HeatTreatment strategy For the elimination of Heat by the upper wayMaximally tonify the Lungs & KidneyPurification, Clear Heat LI 4, LI 11, GV 14, SJ 1Circulate the Ying Lu 7, LI 4, LI 11, SI 3, SJ 5, St 36, Bl 60, GB 43Access the Zhong QiCV 17, CV 12, CV 4, CV 6Calm the SpiritGV 20, Yin Tang, GB 16, GV 23, CV 17, He 7Protect the BloodSp 10, Bl 17Wellspring Seminars Module 9Slide # 197 of 292197External Pathogenic Heat Penetration to the BloodExtremely ominous, life or death situationNOT a Lung syndromeLast step in penetration of external pathogenic heat via Wei, Qi, Ying, & BloodObstruction & complications in the Xin BaoSymptoms of Anarchic circulation of bloodHemorrhage, epistaxis, hemotaxis, hematemesis, hematuriaHigh feverHallucinations, delirium, comaSpeech distortion, inarticulate soundsWellspring Seminars Module 9Slide # 198 of 292198External Pathogenic Heat Penetration To The BloodTreatment strategyCool the BloodBl 17, Sp 10, Li 3, Bl 15, He 7, Bl 20, Sp 3, Bl 23, Ki 3Circulate the Ying/Zhong QiClear Phlegm Heat St 40, Sp 3, St 37, LI 4, LI 11
Wellspring Seminars Module 9Slide # 199 of 292199External Pathogenic Heat Penetration To The BloodTreatment strategyReanimate the Spirit GV 26Repolarize Yin/Yang All 12 Jing-Well ptsGyn coma Li 1, Ki 1 Gluttony coma St 45, Sp 1Calm the SpiritGV 20Yin TangGB 16, GV 23CV 17, He 7Wellspring Seminars Module 9Slide # 200 of 292200External Pathogenic Heat in Xin Bao with Excess in Small IntestineFeverDeliriumComaUnintelligible speechConstipation, abdominal painMental symptomsIrritationWorryAnxietyDry mouthRed face, palm and soles (heat in the five hearts)Palms hotter than dorsumDiminished hearing or deafnessTremors, contractures, Parkinsons, seizures, tonic - clonic contractionsFaintingWiry liver pulse, kidney pulse emptyRed tongue, yellow coat on tongue
Wellspring Seminars Module 9Slide # 201 of 292201External Pathogenic Heat In Xin Bao With Excess In Small IntestineTreatment strategyClear HeatLI 4, LI 11, GV 14, XB 5Consolidate Kidney YinCV 3, Sp 6Maximally tonify the KidneysTonify the BloodBl 17, Sp 10Treat the Bones and Marrow GB 39, LI 16, GV 15, GV 20, Bl 11, Bl 43Calm the Liver FireGB 34, Li 2>3Reanimate the SpiritGV 26Wellspring Seminars Module 9Slide # 202 of 292202Adjunctive Therapies : Pneumonia Qi GongSpicy foodsStop smokingAddress underlying factorsStressImmunosuppressionSedentary lifestyleExposure to pathogensWellspring Seminars Module 9Slide # 203 of 292203Immunology Wellspring Seminars Module 9Slide # 204 of 293Picture Removed204Immunology Wellspring Seminars Module 9Slide # 205 of 293Physiological functioning of the immune system in health and diseaseMalfunctions of the immune system in immunological disordersAutoimmune diseasesHypersensitivitiesImmune deficiencyAllograft rejection
205 Physical, chemical and physiological characteristics of the components of the immune system in vitro, in situ, and in vivoOur clinical interest is primarily in the causes, treatment, and prevention of these immune challenges
Biomedical ImmunologyLymphocytesProduced in lymphoid organsPrimary lymphoid organs: productionBone marrowThymusSecondary lymphoid organs: circulationLymph nodesSpleen Wellspring Seminars Module 9Slide # 206 of 292206Biomedical ImmunologyFormation of lymphocytesBone marrowB lymphocytes: re humoral immunityUnder influence of thymic hormonesTransform into T lymphocytesT lymphocytes: re cellular immunityNatural killer cellsHelper functionWellspring Seminars Module 9Slide # 207 of 292207LuStSISpKiLIBlGBSourBitterSweetPungentSaltyDa Qi(Air)Ge Qi(Food)YING QINutritive EnergyjinjinjinjinyeyeyeyeyebileurinefecesWEI QIjinLi
O2Wellspring Seminars Module 9Slide # 208 of 293208Energetics of ImmunologyThe Wei will heal us but will also kill usWhen available in sufficient quantity & quality, Wei will protect us from thousands of diseasesWhen Wei is inadequate, pathological or misdirected, it can produce many diseasesWellspring Seminars Module 9Slide # 209 of 293209Energetics of Immune FunctionDefense mechanism begins at Water = KidneyHumoral immunity begins in bone marrow with production of B lymphocytesDeficient Kidney Yin results indeficient humoral immunitydeficient antibodies, lymphocytes= Deficient Wei
Wellspring Seminars Module 9Slide # 210 of 293210Energetics of Immune FunctionExternal Pathogenic EnergyAllergens, microbes, environmental irritants Deficient Innate Procreative Fire of the Jing of Kidney YangAdrenals are expression of Kidney YangSympathetic nervous system disturbance creates deficiency in epinephrine & norepinephrineWellspring Seminars Module 9Slide # 211 of 293211Immune Deficiency Immunodeficiency disorders increase susceptibility to infectionThey may be secondary or primarySecondary is more common
Wellspring Seminars Module 9Slide # 212 of 293212Immune Deficiency Secondary immunodeficienciesNonimmune systemic disordersDiabetes, undernutrition, HIV infectionImmunosuppressive treatmentsChemotherapy, radiation therapyCritically ill, older, or hospitalized patientsWellspring Seminars Module 9Slide # 213 of 293213Clinical Presentation: Immune Deficiency Wellspring Seminars Module 9Slide # 214 of 293Picture Removed214Biomedical Etiology & Pathogenesis: Immune Deficiency Immunodeficiency can result from loss of serum proteins (particularly IgG and albumin) through the kidneys in the nephrotic syndrome, through skin in severe burns or dermatitis, or through the GI tract in enteropathy Enteropathy may also lead to lymphocyte loss, resulting in lymphopenia These disorders can mimic B- and T-cell defects Wellspring Seminars Module 9Slide # 215 of 292215Biomedical Diagnosis: Immune Deficiency Immunodeficiency typically manifests as recurrent infections Immunodeficiency should be suspected when recurrent infections are severe, complicated, resistant to treatment, or caused by unusual organisms Wellspring Seminars Module 9Slide # 216 of 292216Biomedical Diagnosis: Immune Deficiency Infections due to immunodeficiency are typically upper and lower respiratory tract infections Sinusitis, bronchitis, pneumoniaGastroenteritisMay be serious bacterial infections Meningitis, sepsisWellspring Seminars Module 9Slide # 217 of 292217Biomedical Diagnosis: Immune Deficiency Immunodeficiency should also be suspected in infants or young children with chronic diarrhea and failure to thrive, especially when the diarrhea is caused by unusual viruses (e.g., adenovirus) or fungi (e.g., Cryptosporidium sp). Other signs include skin lesions (e.g., eczema, warts, abscesses, pyoderma, alopecia), oral or esophageal thrush, oral ulcers, and periodontitis.Less common manifestations include severe viral infection with herpes simplex or varicella zoster virus and CNS problems (e.g., chronic encephalitis, delayed development, seizure disorder). Wellspring Seminars Module 9Slide # 218 of 292218Frequent use of antibiotics may mask many of the common symptoms and signs.
Biomedical Diagnosis: Immune DeficiencyHistory and physical examination are helpful but must be supplemented by immune function testingHistoryRisk factors for infectionSymptoms and risk factors for secondary immunodeficiency disordersOnset of infections before age 12 mo suggests combined B- and T-cell defects or a B-cell defect, which becomes evident when maternal antibodies are disappearing (at about age 6 mo)In general, the earlier the age at onset in children, the more severe the immunodeficiencyWellspring Seminars Module 9Slide # 219 of 292219Certain other primary immunodeficiencies (eg, common variable immunodeficiency [CVID]) may not manifest until adulthood
Biomedical Treatment: Immune Deficiency Treatment focuses on the underlying disorderDiet high in medium-chain triglycerides may decrease loss of IGs and lymphocytes from the GI tract and be remarkably beneficialWellspring Seminars Module 9Slide # 220 of 293220Wei Qi: Humoral ImmunityMaximal Kidney tonification Ki YinBl 23, Bl 52, CV 4, Ki 7 > Ki 8, Ki 3Ki YangCV 4, GV 4Marrow (bone & brain)LI 16, GB 39GV 15, GV 20BonesBl 11JingBl 43ZhiBl 52Ki 3Entry-exit point ZhiWellspring Seminars Module 9Slide # 221 of 292221Immune function begins in the KidneysMaximal Kidney tonification to stimulate humoral immunity & production of B lymphocytesWei Qi: Cellular ImmunityLower JiaoCV 5, CV 7Stimulate SJ purifications preceding Li>WeiShu/MuSI: Bl 27, CV 4 LI: Bl 25, St 25Ki: Bl 23, CV 4, GV 4Li: Bl 18, Li 14Mobilize & exteriorize WeiSt 9, St 5, CV 22, CV 23St 30, Li 13, Li 14St 30, Bl 57Wellspring Seminars Module 9Slide # 222 of 292222To stimulate T lymphocytesExteriorization of Wei points will direct lymphocytes towards the lymph nodes in their areawei to head pts for any pathology supra umbilicalSt 30, Li 13 & 14 for below umbilicuswei to feet points all lower extremity pathologiesDeep Circulation of WeiDeep circulation of Wei follows the posterior and anterior aspect of the spine over the course of 28 daysPoints to stimulate deep circulation of WeiGV 16GV 14GV 4GV 1CV 22CV 23Sp 4XB 6Wellspring Seminars Module 9Slide # 223 of 292223At the end of the day-night cycle the Wei gathers at GV 16Next day it descends 1 vertebra, arriving at the 21st day at GV 1On the 22nd day it penetrates deep, follows the Fu Chong along the (anterior longitudinal ligament) of the spine upwards to reach CV 22Then to CV 23 and back to GV 16
This 2nd circulation of Wei is used in the treatment of certain cancersWei Qi Production & CirculationProduction of WeiCV 5, CV 7: Lower JiaoShu/Mu/Yuan LiverBl 18, Li 14, Li 3Shu/Mu/Yuan SpleenBl 20, Li 13, Sp 3Shu/Mu/Yuan KidneyBl 23, (GB 25), CV 4, Ki 3Wellspring Seminars Module 9Slide # 224 of 293224Circulation of WeiZones of TransitHead GV 20Thorax CV 17All Back-Shu pts from T1 to T7 Bl 13, Bl 14, Bl 15, Bl 17Abdomen All Back-shu pts from T7-S1 Bl 17, Bl 18, Bl 19, Bl 20, Bl 21, Bl 22, Bl 23, Bl 25, Bl 27, Bl 28Feet Bl 57Wellspring Seminars Module 9Slide # 225 of 293225Circulation of WeiExteriorizationHeadCV 22, CV 23, St 9, St 5AbdomenLi 14, Li 13FeetSt 30, St 36SuperficialGV 14, Jing-Well ptsInteriorizationKi 16, St 25Wellspring Seminars Module 9Slide # 226 of 293226Adjunctive Therapies: Immune Deficiency Qi Gong, Taiji QuanDietary changesProtein, veggiesAntioxidantsEliminate refined CHOsSupplementsAstra Isatis, EnhanceMarrow Plus, Astra EssenceYin Chiao, Gan Mao Ling, Zhong Gan LingUltimate Zinc Wellspring Seminars Module 9Slide # 227 of 293227Allergies Allergic disorders are the most common human disorders
Wellspring Seminars Module 9Slide # 228 of 292
228Allergies Commonly affect nose, eyes, skin, and lungsAtopic dermatitisContact dermatitisUrticariaAngioedemaLatex allergyAllergic lung disordersAsthma, allergic bronchopulmonary aspergillosis, hypersensitivity pneumonitis Allergic reactions to venomous stingsWellspring Seminars Module 9Slide # 229 of 292229Atopy and allergy are often used interchangeably but are different. all atopic disorders are type I hypersensitivity disorders.
All atopic disorders are considered allergic, but many allergic disorders (eg, hypersensitivity pneumonitis) are not atopic. Commonly affect nose, eyes, skin, and lungsAtopic dermatitisContact dermatitisUrticariaAngioedemaLatex allergyAllergic lung disordersAsthma, allergic bronchopulmonary aspergillosis, hypersensitivity pneumonitis Allergic reactions to venomous stings
Allergies Type I hypersensitivity reactions underlie all atopic and many allergic disordersAtopy is an exaggerated IgE-mediated immune responseAllergy is any exaggerated immune response to a foreign antigen regardless of mechanism
Wellspring Seminars Module 9Slide # 230 of 292230Atopy and allergy are often used interchangeably but are different. all atopic disorders are type I hypersensitivity disorders.
All atopic disorders are considered allergic, but many allergic disorders (eg, hypersensitivity pneumonitis) are not atopic. What are the 4 types of allergies?
The four types are: Type 1 involves IgE antibodies, which attach to mucus membranes which release histamine. Allergic reactions usually occur within 1 to 60 minutes. They cause classic symptoms, such as: asthma, rhinitis, (running nose), eczema, hives, red cheeks, etc. It is the most dangerous, and can be life threatening. The best test for this is the modified RAST blood test (IgE). Type 2 involves lectin allergens that bind to ABO markers on cells, which include: red blood cells, mucous membranes, intestinal lining, and most other cells. This attracts IgG antibodies and killer cells, which destroy our red blood cells, and may cause anemia. About 70 known food lectins attach specifically to A, B or O blood types. Most lectins are destroyed by cooking and digestion, and rarely cause serious problems. These allergens have been identified by the scientific literature for each blood type. Type 3 involves food allergens, IgG antibodies, and neutrophils (white blood cells), which clump together to form large immune complexes in the blood. These deposit in the organs and tissues, where they cause inflammation and tissue damage, leading to chronic degenerative symptoms or diseases, such as autoimmune conditions, arthritis or kidney disease. The best tests for this are either a modified RAST or an ELISA blood test (IgG). Type 4 involves T-Cells in the skin and soft tissues. Macrophages (white scavenger cells) engulf food allergens and transfer these to T-Cells. Both cells release interleukins (cell messengers) which stimulate the immune system and cause inflammation and tissue damage, leading to degenerative symptoms. The best test for this is the ELISA/ACT LRA blood test.
Allergies Early childhood exposure to bacterial and viral infections and endotoxins (lipopolysaccharide) normally shifts native TH2-cell responses to helper type 1 T (TH1)-cell responsesSuppress TH2 cells and induce tolerance to foreign antigensMechanism may be mediated by Toll-like receptor-4 and occur through development of a population of regulatory T (CD4+CD25+) cells that suppress TH2-cell responsesWellspring Seminars Module 9Slide # 231 of 292231Normally, early childhood exposure to bacterial and viral infections and endotoxins (eg, lipopolysaccharide) shifts native TH2-cell responses to helper type 1 T (TH1)-cell responses, which suppress TH2 cells and induce tolerance to foreign antigens; the mechanism may be mediated by Toll-like receptor-4 and occur through development of a population of regulatory T (CD4+CD25+) cells that suppress TH2-cell responses. But trends in developed countries toward smaller families with fewer children, cleaner indoor environments, and early use of vaccinations and antibiotics may deprive children of these exposures and inhibit TH2-cell suppression; such behavioral changes may explain the increased prevalence of some allergic disorders. Other factors thought to contribute to allergy development include chronic allergen exposure and sensitization, diet, and physical activity.Site-specific factors include adhesion molecules in bronchial epithelium and in skin and molecules in the GI tract that direct TH2 cells to target tissues.
Allergies Trends in developed countries toward smaller families with fewer children, cleaner indoor environments, and early use of vaccinations and antibiotics may deprive children of these exposures and inhibit TH2-cell suppressionSuch behavioral changes may explain the increased prevalence of some allergic disordersWellspring Seminars Module 9Slide # 232 of 293232Normally, early childhood exposure to bacterial and viral infections and endotoxins (eg, lipopolysaccharide) shifts native TH2-cell responses to helper type 1 T (TH1)-cell responses, which suppress TH2 cells and induce tolerance to foreign antigens; the mechanism may be mediated by Toll-like receptor-4 and occur through development of a population of regulatory T (CD4+CD25+) cells that suppress TH2-cell responses. But trends in developed countries toward smaller families with fewer children, cleaner indoor environments, and early use of vaccinations and antibiotics may deprive children of these exposures and inhibit TH2-cell suppression; such behavioral changes may explain the increased prevalence of some allergic disorders. Other factors thought to contribute to allergy development include chronic allergen exposure and sensitization, diet, and physical activity.Site-specific factors include adhesion molecules in bronchial epithelium and in skin and molecules in the GI tract that direct TH2 cells to target tissues.
Allergies Other factors which contribute to allergy development include Chronic allergen exposure and sensitizationDietPhysical activitySite-specific factors include adhesion molecules in bronchial epithelium and in skin and molecules in the GI tract that direct TH2 cells to target tissues.Wellspring Seminars Module 9Slide # 233 of 292233Normally, early childhood exposure to bacterial and viral infections and endotoxins (eg, lipopolysaccharide) shifts native TH2-cell responses to helper type 1 T (TH1)-cell responses which suppress TH2 cells and induce tolerance to foreign antigens; the mechanism may be mediated by Toll-like receptor-4 and occur through development of a population of regulatory T (CD4+CD25+) cells that suppress TH2-cell responses. But trends in developed countries toward smaller families with fewer children, cleaner indoor environments, and early use of vaccinations and antibiotics may deprive children of these exposures and inhibit TH2-cell suppression; such behavioral changes may explain the increased prevalence of some allergic disorders. Other factors thought to contribute to allergy development include chronic allergen exposure and sensitization, diet, and physical activity.Site-specific factors include adhesion molecules in bronchial epithelium and in skin and molecules in the GI tract that direct TH2 cells to target tissues.
Allergies By definition, an allergen induces IgE-mediated and TH2-cell immune responsesAllergic triggers are almost always low molecular weight proteins, many of which are airborne particlesMost common airborne allergens responsible for acute and chronic allergic reactions includehouse dustmite fecesanimal danderpollens (tree, grass, and weed)moldsWellspring Seminars Module 9Slide # 234 of 292234By definition, an allergen induces IgE-mediated and TH2-cell immune responsesAllergic triggers are almost always low molecular weight proteins, many of which can be constituted as airborne particlesAllergens most commonly responsible for acute and chronic allergic reactions include house dust, mite feces, animal dander, pollens (tree, grass, and weed), and molds
Allergies When allergen binds to IgEhistamine is released from intracellular granules of mast cells, which are widely distributed but most concentrated in skin, lungs, and GI mucosahistamine reinforces immune cell activation and is the primary mediator of clinical atopyPhysical disruption of tissue and various chemicals (e.g., tissue irritants, opioids, surface-active agents) can trigger histamine release directly, independent of IgEWellspring Seminars Module 9Slide # 235 of 292235When allergen binds to IgE, histamine is released from intracellular granules of mast cells, which are widely distributed but most concentrated in skin, lungs, and GI mucosa; histamine reinforces immune cell activation and is the primary mediator of clinical atopy. Physical disruption of tissue and various chemicals (eg, tissue irritants, opioids, surface-active agents) can trigger histamine release directly, independent of IgE.Histamine causes local vasodilation (producing erythema), increased capillary permeability and edema (producing a wheal), surrounding arteriolar vasodilation mediated by neuronal reflex mechanisms (producing flare), and stimulation of sensory nerves (producing itching). Histamine causes smooth muscle contraction in the airways (bronchoconstriction) and in the GI tract (increased GI motility) and increases salivary and bronchial gland secretions. When released systemically, it is a potent arteriolar dilator and can cause extensive peripheral pooling of blood and hypotension; cerebral vasodilation may be a factor in vascular headache. Histamine increases capillary permeability; the resulting loss of plasma and plasma proteins from the vascular space can worsen circulatory shock. It triggers a compensatory catecholamine surge from adrenal chromaffin cells.
Allergies Histamine causesLocal vasodilation ErythemaIncreased capillary permeability and edema WhealSurrounding arteriolar vasodilation mediated by neuronal reflex mechanisms FlareStimulation of sensory nerves Itching Wellspring Seminars Module 9Slide # 236 of 292236When allergen binds to IgE, histamine is released from intracellular granules of mast cells, which are widely distributed but most concentrated in skin, lungs, and GI mucosa; histamine reinforces immune cell activation and is the primary mediator of clinical atopy. Physical disruption of tissue and various chemicals (eg, tissue irritants, opioids, surface-active agents) can trigger histamine release directly, independent of IgE.Histamine causes local vasodilation (producing erythema), increased capillary permeability and edema (producing a wheal), surrounding arteriolar vasodilation mediated by neuronal reflex mechanisms (producing flare), and stimulation of sensory nerves (producing itching). Histamine causes smooth muscle contraction in the airways (bronchoconstriction) and in the GI tract (increased GI motility) and increases salivary and bronchial gland secretions. When released systemically, it is a potent arteriolar dilator and can cause extensive peripheral pooling of blood and hypotension; cerebral vasodilation may be a factor in vascular headache. Histamine increases capillary permeability; the resulting loss of plasma and plasma proteins from the vascular space can worsen circulatory shock. It triggers a compensatory catecholamine surge from adrenal chromaffin cells.
Allergies Histamine causesSmooth muscle contractionAirways (bronchoconstriction)GI tract (increased GI motility)Increases salivary and bronchial gland secretionsWellspring Seminars Module 9Slide # 237 of 293237When allergen binds to IgE, histamine is released from intracellular granules of mast cells, which are widely distributed but most concentrated in skin, lungs, and GI mucosa; histamine reinforces immune cell activation and is the primary mediator of clinical atopy. Physical disruption of tissue and various chemicals (eg, tissue irritants, opioids, surface-active agents) can trigger histamine release directly, independent of IgE.Histamine causes local vasodilation (producing erythema), increased capillary permeability and edema (producing a wheal), surrounding arteriolar vasodilation mediated by neuronal reflex mechanisms (producing flare), and stimulation of sensory nerves (producing itching). Histamine causes smooth muscle contraction in the airways (bronchoconstriction) and in the GI tract (increased GI motility) and increases salivary and bronchial gland secretions. When released systemically, it is a potent arteriolar dilator and can cause extensive peripheral pooling of blood and hypotension; cerebral vasodilation may be a factor in vascular headache. Histamine increases capillary permeability; the resulting loss of plasma and plasma proteins from the vascular space can worsen circulatory shock. It triggers a compensatory catecholamine surge from adrenal chromaffin cells.
Allergies Systemically, histamine is a potent arteriolar dilatorCan cause extensive peripheral pooling of bloodHypotensionCerebral vasodilation may be a factor in vascular headacheWellspring Seminars Module 9Slide # 238 of 292238When allergen binds to IgE, histamine is released from intracellular granules of mast cells, which are widely distributed but most concentrated in skin, lungs, and GI mucosa; histamine reinforces immune cell activation and is the primary mediator of clinical atopy. Physical disruption of tissue and various chemicals (eg, tissue irritants, opioids, surface-active agents) can trigger histamine release directly, independent of IgE.Histamine causes local vasodilation (producing erythema), increased capillary permeability and edema (producing a wheal), surrounding arteriolar vasodilation mediated by neuronal reflex mechanisms (producing flare), and stimulation of sensory nerves (producing itching). Histamine causes smooth muscle contraction in the airways (bronchoconstriction) and in the GI tract (increased GI motility) and increases salivary and bronchial gland secretions. When released systemically, it is a potent arteriolar dilator and can cause extensive peripheral pooling of blood and hypotension; cerebral vasodilation may be a factor in vascular headache. Histamine increases capillary permeability; the resulting loss of plasma and plasma proteins from the vascular space can worsen circulatory shock. It triggers a compensatory catecholamine surge from adrenal chromaffin cells.
Clinical Presentation: Allergies SymptomsRhinorrheaSneezingNasal congestion (upper respiratory tract) Wheezing and dyspnea (lower respiratory tract)Itching (eyes, skin)
Wellspring Seminars Module 9Slide # 239 of 293239Clinical Presentation: Allergies Signs Nasal turbinate edemaSinus pain on palpationWheezingConjunctival hyperemia and edemaSkin lichenificationStridor, wheezing, and hypotension are life-threatening signs of anaphylaxis Wellspring Seminars Module 9Slide # 240 of 292240Clinical Presentation: Allergies Allergic facies are associated with chronic allergy in some childrenNarrow and high-arched palateNarrow chinElongated maxilla with overbiteWellspring Seminars Module 9Slide # 241 of 293241Biomedical Etiology & Pathogenesis: Allergies EtiologyGeneticEnvironmentalSite-specific factors
Wellspring Seminars Module 9Slide # 242 of 293242Biomedical Diagnosis: Allergies Thorough history is generally more reliable than testing or screeningHistoryFrequency and duration of attacksChanges over timeTriggering factorsSeasonal or situational settingsPollen seasonsExposure to animals, hay, or dustExerciseParticular placesFamily history Responses to treatmentsWellspring Seminars Module 9Slide # 243 of 292243DiagnosisA thorough history is generally more reliable than testing or screeningHistory should include questions about:Frequency and duration of attacks and changes over timeTriggering factors if identifiableRelation to seasonal or situational settingsPredictably occurring during pollen seasonsAfter exposure to animals, hay, or dustDuring exerciseIn particular placesFamily history of similar symptoms or of atopic disordersResponses to attempted treatmentsBiomedical Diagnosis: Allergies Age at onset is important in asthmaChildhood asthma is likely to be atopic Asthma beginning after age 30 is notCBC should be ordered to detect eosinophilia in all patients except those taking corticosteroids, which reduce the eosinophil count Total WBC is usually normalConjunctival or nasal secretions or sputum can be examined for leukocytesFinding any eosinophils indicates that TH2-mediated allergic inflammation is likelyWellspring Seminars Module 9Slide # 244 of 292244An eosinophil differential of 5 to 15% of total WBCs suggests atopy but is nonspecific; 16 to 40% may reflect atopy or other conditions (eg, drug hypersensitivity, cancer, autoimmune disorders, parasitic infection); a differential of 50 to 90% almost never occurs in atopic disorders and is more characteristic of hypereosinophilic syndrome or visceral larva migrans.Serum IgE levels are elevated in atopic disorders but are of little help in diagnosis because they are also elevated in parasitic infections, infectious mononucleosis, autoimmune disorders, drug reactions, immunodeficiency disorders and in some forms of multiple myeloma. IgE levels are probably most helpful for following response to therapy in allergic bronchopulmonary aspergillosisBiomedical Diagnosis: Allergies Skin testing uses standardized concentrations of antigen introduced directly into skin Most commonly used antigens are pollens (tree, grass, and weed), molds, house dust mites, animal danders and sera, insect venom, foods, and -lactam antibiotics Wellspring Seminars Module 9Slide # 245 of 293245Skin testing has higher positive predictive values for diagnosing allergic rhinosinusitis and conjunctivitis than for diagnosing allergic asthma or food allergy; negative predictive value for food allergy is high.Skin testing uses standardized concentrations of antigen introduced directly into skin and is indicated when a detailed history and physical examination do not identify the cause and triggers for symptoms. The most commonly used antigens are pollens (tree, grass, and weed), molds, house dust mites, animal danders and sera, insect venom, foods, and -lactam antibiotics. Choice of antigens to include is based on patient history and geographic prevalence. Two techniques can be used, percutaneous (prick) and intradermal. The prick test can detect most allergies. The intradermal test is more sensitive but less specific; it can be used to evaluate sensitivity to allergens with negative or equivocal prick test results.
Biomedical Diagnosis: Allergies Radioallergosorbent testing (RAST) detects the presence of allergen-specific serum IgE
Provocative testing involves direct exposure of the mucosae to allergen Wellspring Seminars Module 9Slide # 246 of 293246Radioallergosorbent testing (RAST) detects the presence of allergen-specific serum IgE and is indicated when skin testing is contraindicated because of generalized dermatitis, dermatographism, history of anaphylaxis to the allergen, or need to continue antihistamines. A known allergen in the form of an insoluble polymer-allergen conjugate is mixed with the serum to be tested and with 125I-labeled anti-IgE antibody. Any allergen-specific IgE in the serum binds the conjugate and can be quantified by measuring the 125I-labeled antibody.
Provocative testing involves direct exposure of the mucosae to allergen and is indicated for patients who must document their reaction (eg, for occupational or disability claims) and sometimes for diagnosis of food allergy.
Ophthalmic testing has no advantage over skin testing and is rarely used. Nasal and bronchial challenge are primarily research tools, but bronchial challenge is sometimes used when the clinical significance of a positive skin test is unclear or when no antigen extracts are available (eg, for occupation-related asthma).
Biomedical Treatment: Allergies Environmental controlRemoval or avoidance of allergic triggers is the primary biomedical treatment of allergyAntihistaminesAntihistamines do not affect histamine production or metabolism but block receptorsImmunotherapyExposure to allergen in gradually increasing doses (hyposensitization or desensitization) via injection or sublingually can induce tolerance Wellspring Seminars Module 9Slide # 247 of 292247TreatmentEnvironmental control: Removal or avoidance of allergic triggers is the primary treatment of allergy. Strategies include use of synthetic fiber pillows and impermeable mattress covers; frequent washing of bed sheets, pillowcases, and blankets in hot water; removal of upholstered furniture, soft toys, carpets, and pets; house cleaning and extermination (to eliminate cockroach exposure); and use of dehumidifiers in basements and other poorly aerated, damp rooms. Other measures may include treating homes with heat-steam, using high-efficiency particulate air (HEPA) vacuums and filters, avoiding food triggers, limiting pets to certain rooms, and frequently cleaning cloth furniture and carpets. Adjunctive nonallergenic triggers (eg, cigarette smoke, strong odors, irritating fumes, air pollution, cold temperatures, high humidity) should also be avoided or controlled when possible.Antihistamines: Antihistamines do not affect histamine production or metabolism but block receptors. H1 blockers are a mainstay of treatment for allergic disorders. H2 blockers are used primarily for gastric acid suppression and have limited usefulness for allergic reactions; they may be indicated for certain atopic disorders, especially chronic urticaria.Oral H1 blockers provide symptomatic relief in various atopic and allergic disorders (eg, seasonal hay fever, allergic rhinitis, conjunctivitis, urticaria, other dermatoses, minor reactions to blood transfusion incompatibilities and to x-ray radiopaque dyes); they are less effective for allergic bronchoconstriction and vasodilation. Onset of action is usually 15 to 30 min, with peak effects in 1 h; duration of action is usually 3 to 6 h.Oral H1 blockers are classified as sedating or nonsedating (better thought of as less sedating). Sedating antihistamines are widely available without prescription. All have significant sedative and anticholinergic properties; they pose particular problems for the elderly and patients with glaucoma, benign prostatic hyperplasia, constipation, and dementia. Nonsedating (non-anticholinergic) antihistamines are preferred except when sedative effects may be therapeutic (eg, for nighttime relief of allergy or short-term treatment of insomnia in adults or nausea in younger patients). Anticholinergic effects may also partially justify use of sedating antihistamines for symptomatic relief of rhinorrhea in URIs.Immunotherapy: Exposure to allergen in gradually increasing doses (hyposensitization or desensitization) via injection or in high doses sublingually can induce tolerance and is indicated when allergen exposure cannot be avoided and drug treatment is inadequate. Mechanism is unknown but may involve induction of IgG antibodies, which compete with IgE for allergen or block IgE from binding with mast cell IgE receptors; induction of interferon , IL-12, and cytokines secreted by TH1 cells; or induction of regulatory T cells.
Allergies: Energetic Etiology & PathogenesisEtiologyFrequently begins in Middle Jiao = St/SpResults in deficient production & circulation of Ying & WeiComplicated by Liver Heat flaring & destroying the WeiWellspring Seminars Module 9Slide # 248 of 293248Energetic Diagnosis: Allergies History & PhysicalChannel trajectoryTissues involved, colorsTiming & seasonCBC with diff, skin testing, RAST or ELISAAK, CKAllergy challenge testPulsesHeat or ColdBounding or thready & submergedLu & Li often deficientSp/St, SJWellspring Seminars Module 9Slide # 249 of 292249Energetic Treatment : Allergies Tonify Sp, Lu, LiShu/Mu/Yuan SpleenBl 20, Li 13, Sp 3Shu/Mu/Yuan LungBl 13, Lu 1, Lu 9Shu/Mu/Yuan LiverBl 18, Li 14, Li 3Zhong QiCV 4, CV 6, CV 12, CV 17Yi & PoBl 47, Sp 1, Entry-exit YiBl 42, Lu 10, Entry-exit PoWellspring Seminars Module 9Slide # 250 of 292250Energetic Treatment : Allergies Production & circulation of YingZhong QiCV 6, CV 12, CV 17Circulate YingLu 7, LI 4, St 36, Sp 6Production & circulation of WeiCV 5, Li 14, Li 13, CV 17CV 22, CV 23, St 9, St 5 GV 20, GV 14Wellspring Seminars Module 9Slide # 251 of 292251Adjunctive Therapies: Allergies Identify allergenAllergy challenge, AK or labsAvoidance or rotation for food allergiesAK, CK, NAETDietary modificationsAnti-inflammatory diet http://www.fatresistancediet.comBlood Type diet http://www.dadamo.comSupplementsDigestive enzymesTAPSAntronexXanthium Relieve SurfaceFish OilQuercetin Wellspring Seminars Module 9Slide # 252 of 292252Digestive enzymes Both with and between meals
URI, Colds, Flu Wellspring Seminars Module 9Slide # 253 of 293Picture Removed253URI, Colds, Flu: Clinical PresentationThe common cold is an acute, usually afebrile, self-limited viral infection involving upper respiratory symptoms, such as rhinorrhea, cough, and sore throat Influenza often mimics a cold, but also may present with fever, myalgia, and malaiseWellspring Seminars Module 9Slide # 254 of 293254Biomed Etiology & Pathogenesis: URI, Colds, Flu About 50% of all colds are caused by one of the > 100 serotypes of rhinoviruses Coronaviruses cause some outbreaks, and infections caused by influenza, parainfluenza, and respiratory syncytial viruses may also manifest as the common cold, particularly in patients who are experiencing reinfectionRhinovirus infections are most common during fall and spring and are less common during winter months Rhinoviruses are most efficiently spread by direct person-to-person contact, although spread may also occur via large-particle aerosolsWellspring Seminars Module 9Slide # 255 of 292255It is the common medical belief that Susceptibility to colds is not affected by exposure to cold temperature, host health and nutrition, or upper respiratory tract abnormalities (eg, enlarged tonsils or adenoids). The most potent deterrent to infection is the presence of specific neutralizing antibodies in the serum and secretions, induced by previous exposure to the same or a closely related virus. URI, Colds, Flu: Biomedical DiagnosisSymptoms & SignsAfter an incubation period of 24 to 72 h, symptoms begin with a scratchy or sore throat, followed by sneezing, rhinorrhea, nasal obstruction, and malaiseTemperature is usually normal, particularly when the pathogen is a rhinovirus or coronavirusNasal secretions are watery and profuse during the first days but then become more mucoid and purulentCough is usually mild but often lasts into the 2nd wkMost symptoms due to uncomplicated colds resolve within 10 daysWellspring Seminars Module 9Slide # 256 of 292256URI, Colds, Flu: Biomedical TreatmentNo specific biomedical treatment existsSymptomatic relief can be afforded by use of antipyretics, analgesics, nasal decongestants & antihistamines There are no globally effective vaccines Hand washing and use of surface disinfectant in a contaminated environment reduce spread of infectionAntibiotics should not be given unless there is evidence of secondary bacterial infection Wellspring Seminars Module 9Slide # 257 of 292257A cold if treated lasts seven days, untreated it lasts a week.Topical nasal decongestants are more effective than oral decongestants, but the use of topical drugs for > 3 to 5 days may result in rebound congestion. Zinc, echinacea, and vitamin C have all been evaluated as common cold therapies but none have been clearly demonstrated to be beneficial.
URI, Colds, Flu: Energetic Etiology & PathogenesisEtiologyDeficient Ying results in deficient WeiVirulent pathogen overwhelms even robust immune defenseThe illness is not the invasion, its a weakness that allows the invasion to occurWellspring Seminars Module 9Slide # 258 of 293258URI, Colds, FluDiagnosisClinical symptoms of sore throat, rhinorrhea, sneezing, itchy watery eyesSigns of Heat or ColdWatery eyes, slow pulse, clear or white tongue coat, clear mucus, lack of sweating, craves Heat = ColdRed sclera, rapid pulse, yellow tongue coat, green/yellow mucus, fever, sweating, myalgia, prefers coolness = HeatWellspring Seminars Module 9Slide # 259 of 292259Remember that extreme Cold converts to Heat, & vice versa. Depends on the stage of the disease progression just what you will find.Energetic Etiology & Pathogenesis: URI, Colds, FluExcess Wind ColdExternal Pathogenic Cold attacks the Energy, penetrating via the Liu QiExternal Pathogenic Energy invasionWei Energy cannot fill the epidermisDeficient Wei due to deficient YingVirulent or extreme external invasionWellspring Seminars Module 9Slide # 260 of 293260 Progression of Wind ColdProgression of invasion of Wind Cold Skin/nasal mucosaPilocutaneous area to capillary channelsTendinomuscular channelsPrincipal channelsWellspring Seminars Module 9Slide # 261 of 293261Progression of invasion of Wind Cold Skin/nasal mucosaPilocutaneous area to capillary channelsTendinomuscular channelsPrincipal channels
Progression of Wind ColdIf Lungs are weak, External Pathogenic Cold tries to attack the LungsIf repelled by Lungs, it next goes to the noseLI 20, producing nasal congestionProgressing upward to the eyes & bridge of noseBl 1 tearing; Bl 2, sneezingThen up Bl channel to forehead & vertexBl 7 frontal HA, to GV 20, vertex HA, Bl 8 heavy head, GB 8 ringing earsTreat Bl 7, GV 20, Bl 8, GB 8Wellspring Seminars Module 9Slide # 262 of 292262For next presentation of this module, create animation from Bl channel trajectoryProgression of Wind ColdIf Ext Pathogenic Cold arrives @ occipital region, Bl 10, occipital HA, stiff neckTreat GV 16, Bl 10, GB 20, SJ 16Ext Pathogenic Cold then progresses along spineBase of neck GV 14, GV 13Following Bl channel along entire spine Bl 11 to Bl 23, back pain, curvature of spine When it arrives at Bl 23, Ext Pathogenic Cold penetrates Kidney & BladderWellspring Seminars Module 9Slide # 263 of 292 IT IS URGENT TO TREAT BEFORE IT REACHES THIS LEVEL !!!263Progression of Wind Cold: TreatmentDilate the pores to release the exterior Sudorification Lu 7, LI 4, Bl 12, GB 20, Lu 8, Lu 10Tonify the Essential Energy Lu 7, LI 4, St 36, Sp 6Maximally tonify LungsShu/Mu/Yuan Bl 13, Lu 1, Lu 9 PoBl 42, Lu 10, entry-exit Po Zhong Qi CV 6 & CV 17Wellspring Seminars Module 9Slide # 264 of 292264Progression of Wind Cold: TreatmentDistribute the Wei Interiorize Ki 16 Exteriorize GV 14Increase Internal Organic Cold to repel External Pathogenic Cold Tonify the KidneysShu/Mu/Yuan KidneyBl 23, CV 4, GV 4, Ki 3Zhong QiCV 6, CV 4ZhiBl 52, Ki 3, entry-exit ZhiWellspring Seminars Module 9Slide # 265 of 292265Adjunctive Therapies: URI, Colds, Flu Yin ChiaoGan Mao LingZhong Gan LingZinc lozengesBed restFluidsWellspring Seminars Module 9Slide # 266 of 293266Research has shown that chicken soup actually does move mucus better than other hot liquidsAutoimmune Conditions Wellspring Seminars Module 9Slide # 267 of 292Picture Removed267Immunologic Features Of ToleranceDifferent from non-specific immunosuppression and immunodeficiencyActive antigen-dependent process in response to the antigenSpecific immunological non-reactivity to an antigen Results from previous exposure to same antigenLike immunological memory, tolerance is specificCan exist in T-cells, B cells or bothTolerance at the T cell level is longer lasting than at the B cell levelWellspring Seminars Module 9Slide # 268 of 292268TOLERANCEIntroduction Tolerance refers to the specific immunological non-reactivity to an antigen resulting from a previous exposure to the same antigen. While the most important form of tolerance is non-reactivity to self antigens, it is possible to induce tolerance to non-self antigens. When an antigen induces tolerance, it is termed tolerogen.Induction of tolerance to non-selfTolerance can be induced to antigenic components on both soluble proteins and cells (tissues) by injecting these materials into animals. Induction of such a tolerance depends on a number of variables.Tolerance to tissues and cellsTolerance to tissue and cell antigens can be induced by injection of hemopoietic (stem) cells in neonatal or severely immunocompromised (by lethal irradiation or drug treatment) animals. Also, grafting of allogeneic bone marrow or thymus in early life results in tolerance to the donor type cells and tissues. Such animals are known as chimeras. These findings are of significant practical application in bone marrow grafting.Tolerance to soluble antigensA state of tolerance to a variety of T-dependent and T-independent antigens has been achieved in various experimental models. Based on these observations it is clear that a number of factors determine whether an antigen will stimulate an immune response or tolerance (Table 1).
Immunologic features of toleranceTolerance is different from non-specific immunosuppression and immunodeficiency. It is an active antigen-dependent process in response to the antigen. Like immune response, tolerance is specific and like immunological memory, it can exist in T-cells, B cells or both and like immunological memory, tolerance at the T cell level is longer lasting than tolerance at the B cell level. Induction of tolerance in T cells is easier and requires relatively smaller amounts of tolerogen than tolerance in B cells. Maintenance of immunological tolerance requires persistence of antigen. Tolerance can be broken naturally (as in autoimmune diseases) or artificially (as shown in experimental animals, by x-irradiation, certain drug treatments and by exposure to cross reactive antigens). Tolerance may be induced to all epitopes or only some epitopes on an antigen and tolerance to a single antigen may exist at the B cell level or T cell level or at both levels.Mechanism of tolerance inductionThe exact mechanism of induction and maintenance of tolerance is not fully understood. Experimental data, however, point to several possibilities.Clonal deletion: Functionally immature cells of a clone encountering antigen undergo a programmed cell death; for example, auto-reactive T-cells are eliminated in the thymus following interaction with self antigen during their differentiation (negative selection). Recent studies have shown that a variety of antigens are expressed in thymic epithelial cells. Likewise, differentiating early B cells become tolerant when they encounter cell-associated or soluble self antigen. B cells expressing only IgM (no IgD) on their surface when exposed to antigen are more prone to tolerance induction than immune response. Clonal deletion has been shown to occur also in the periphery.
Clonal anergy: Auto-reactive T cells, when exposed to antigenic peptides which do not possess co-stimulatory molecules (B7-1 or B7-2), become anergic to the antigen. Also, B cells when exposed to large amounts of soluble antigen down regulate their surface IgM and become anergic. These cells also up-regulate the Fas molecules on their surface. An interaction of these B cells with Fas-ligand-bearing cells results in their death via apoptosis.
Clonal ignorance: T cells reactive to self antigen not represented in the thymus will mature and migrate to the periphery, but they may never encounter the appropriate antigen because it is sequestered in inaccessible tissues. Such cells may die out for lack of stimulus. Auto-reactive B cells that escape deletion may not find the antigen or the specific helper T-cells and hence not be activated and die out.
Receptor editing: B cells which encounter large amounts of soluble antigen, as they do in the body, and bind to this antigen with very low affinity become activated to re-express their RAG1 and RAG2 genes. These genes cause them to undergo DNA recombination and change their specificity.
Anti-idiotype antibody: Anti-idiotype antibodies produced experimentally have been demonstrated to inhibit immune response to specific antigens. Anti-idiotype antibodies are produced during the process of tolerization and such antibodies have been demonstrated in tolerant animals. These antibodies prevent the receptor from combining with antigen.
Suppressor cells: Both low and high doses of antigen may induce suppressor Tcells which can specifically suppress immune responses of both Band Tcells, either directly or by production of cytokines, most importantly, TGF-beta and IL-10.
Termination of toleranceExperimentally induced tolerance can be terminated by prolonged absence of exposure to the tolerogen, by treatments which severely damage the immune system (x-irradiation) or by immunization with cross reactive antigens. These observations are of significance in the conceptualization of autoimmune diseases.
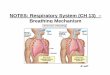
AUTOIMMUNITYDefinitionAutoimmunity can be defined as breakdown of mechanisms responsible for self tolerance and induction of an immune response against components of the self. Such an immune response may not always be harmful (e.g., anti-idiotype antibodies). However, in numerous autoimmune diseases it is well recognized that products of the immune system cause damage to the self.
Effector mechanisms in autoimmune diseasesBoth antibodies and effector T cells can be involved in the damage in autoimmune diseases.General classificationAutoimmune diseases are generally classified on the basis of the organ or tissue involved. These diseases may fall in an organ-specific category in which the immune response is directed against antigen(s) associated with the target organ being damaged or a non-organ-specific category in which the antibody is directed against an antigen not associated with the target organ (Table 2). The antigen involved in most autoimmune diseases is evident from the name of the disease (Table 2).Genetic predisposition for autoimmunityStudies in mice and observations in humans suggest a genetic predisposition for autoimmune diseases. Association between certain HLA types and autoimmune diseases has been noted (HLA: B8, B27, DR2, DR3, DR4, DR5 etc.). Figure 1 Hyperpigmentation of buccal mucosa in Addison's disease Bristol Biomedical Archive. Used with permission
Etiology of autoimmunity diseaseThe exact etiology of autoimmune diseases is not known. However, various theories have been offered. These include sequestered antigen, escape of auto-reactive clones, loss of suppressor cells, cross reactive antigens including exogenous antigens (pathogens) and altered self antigens (chemical and viral infections).Sequestered antigen: Lymphoid cells may not be exposed to some self antigens during their differentiation, because they may be late-developing antigens or may be confined to specialized organs (e.g., testes, brain, eye, etc.). A release of antigens from these organs resulting from accidental traumatic injury or surgery can result in the stimulation of an immune response and initiation of an autoimmune disease.Escape of auto-reactive clones: The negative selection in the thymus may not be fully functional to eliminate self reactive cells. Not all self antigens may be represented in the thymus or certain antigens may not be properly processed and presented. AutoimmunityBreakdown of mechanisms responsible for self tolerance Induction of an immune response against components of the selfWellspring Seminars Module 9Slide # 269 of 292269Clinical Presentation: AutoimmuneTwo general types Those that damage several organs Systemic autoimmune diseases Only a single organ or tissue is directly damaged by the autoimmune process Localized autoimmune diseases Wellspring Seminars Module 9Slide # 270 of 292270However, the distinctions become blurred as the effect of localized autoimmune disorders frequently extends beyond the targeted tissues, indirectly affecting other body organs and systems. Some of the most common types of autoimmune disorders include:
Autoimmune DiseasesWellspring Seminars Module 9Slide # 271 of 293Picture Removed271Biomedical Etiology & Pathogenesis: Autoimmune Immune system produces antibodies to an endogenous antigenAntibody-coated cells, like any similarly coated foreign particle, activate the complement system resulting in tissue injurySometimes the mechanism of injury involves deposition of antibody-antigen complexes (type III hypersensitivity reaction)Wellspring Seminars Module 9Slide # 272 of 292272Autoimmune Disorders In autoimmune disorders, the immune system produces antibodies to an endogenous antigen. Antibody-coated cells, like any similarly coated foreign particle, activate the complement system resulting in tissue injury. Sometimes the mechanism of injury involves deposition of antibody-antigen complexes (type III hypersensitivity reaction).
EtiologySeveral mechanisms may account for the body's attack on itself.Autoantigens may become immunogenic because they are altered chemically, physically, or biologically. Certain chemicals couple with body proteins, making them immunogenic (as in contact dermatitis). Drugs can produce several autoimmune reactions by binding covalently to serum or tissue proteins (see below). Photosensitivity exemplifies physically induced autoallergy: Ultraviolet light alters skin protein, to which the patient becomes allergic. In animal models, persistent infection with an RNA virus that combines with host tissues alters autoantigens biologically, resulting in an autoallergic disorder resembling SLE.Antibodies produced in response to a foreign antigen may cross-react with normal autoantigens (eg, cross-reaction between streptococcal M protein and human heart muscle).Normally, autoimmune reactions are probably restrained by specific regulatory T cells. A regulatory T-cell defect could accompany or result from any of the above mechanisms. Anti-idiotype antibodies (antibodies to the antigen-combining site of other antibodies) may interfere with regulation of antibody activity.Genetic factors play a role. Relatives of patients with autoimmune disorders often have the same type of autoantibodies, and incidence of autoimmune disorders is higher in identical than fraternal twins. Women are affected more often than men. The genetic role appears to be one of predisposition. In predisposed people, environmental factors may provoke disease (eg, certain drugs can trigger hemolytic anemia in patients with G6PD deficiency).Biomedical Etiology & Pathogenesis: Autoimmune Autoantigens may become immunogenic because they are altered chemically, physically, or biologicallyCertain chemicals couple with body proteins, making them immunogenic as in contact dermatitisDrugs can produce several autoimmune reactions by binding covalently to serum or tissue proteinsWellspring Seminars Module 9Slide # 273 of 292273Autoimmune Disorders In autoimmune disorders, the immune system produces antibodies to an endogenous antigen. Antibody-coated cells, like any similarly coated foreign particle, activate the complement system resulting in tissue injury. Sometimes the mechanism of injury involves deposition of antibody-antigen complexes (type III hypersensitivity reaction).
EtiologySeveral mechanisms may account for the body's attack on itself.Autoantigens may become immunogenic because they are altered chemically, physically, or biologically. Certain chemicals couple with body proteins, making them immunogenic (as in contact dermatitis). Drugs can produce several autoimmune reactions by binding covalently to serum or tissue proteins (see below). Photosensitivity exemplifies physically induced autoallergy: Ultraviolet light alters skin protein, to which the patient becomes allergic. In animal models, persistent infection with an RNA virus that combines with host tissues alters autoantigens biologically, resulting in an autoallergic disorder resembling SLE.Antibodies produced in response to a foreign antigen may cross-react with normal autoantigens (eg, cross-reaction between streptococcal M protein and human heart muscle).Normally, autoimmune reactions are probably restrained by specific regulatory T cells. A regulatory T-cell defect could accompany or result from any of the above mechanisms. Anti-idiotype antibodies (antibodies to the antigen-combining site of other antibodies) may interfere with regulation of antibody activity.Genetic factors play a role. Relatives of patients with autoimmune disorders often have the same type of autoantibodies, and incidence of autoimmune disorders is higher in identical than fraternal twins. Women are affected more often than men. The genetic role appears to be one of predisposition. In predisposed people, environmental factors may provoke disease (eg, certain drugs can trigger hemolytic anemia in patients with G6PD deficiency).Biomedical Etiology & Pathogenesis: Autoimmune Photosensitivity exemplifies physically induced autoallergyUltraviolet light alters skin proteinto which the patient becomes allergicPersistent infection with an RNA virus that combines with host tissues biologically alters autoantigensresults in autoallergic disorder resembling SLEAntibodies produced in response to a foreign antigen cross-react with normal autoantigenscross-reaction between streptococcal M protein and human heart muscleWellspring Seminars Module 9Slide # 274 of 292274Autoimmune Disorders In autoimmune disorders, the immune system produces antibodies to an endogenous antigen. Antibody-coated cells, like any similarly coated foreign particle, activate the complement system resulting in tissue injury. Sometimes the mechanism of injury involves deposition of antibody-antigen complexes (type III hypersensitivity reaction).
EtiologySeveral mechanisms may account for the body's attack on itself.Autoantigens may become immunogenic because they are altered chemically, physically, or biologically. Certain chemicals couple with body proteins, making them immunogenic (as in contact dermatitis). Drugs can produce several autoimmune reactions by binding covalently to serum or tissue proteins (see below). Photosensitivity exemplifies physically induced autoallergy: Ultraviolet light alters skin protein, to which the patient becomes allergic. In animal models, persistent infection with an RNA virus that combines with host tissues alters autoantigens biologically, resulting in an autoallergic disorder resembling SLE.Antibodies produced in response to a foreign antigen may cross-react with normal autoantigens (eg, cross-reaction between streptococcal M protein and human heart muscle).Normally, autoimmune reactions are probably restrained by specific regulatory T cells. A regulatory T-cell defect could accompany or result from any of the above mechanisms. Anti-idiotype antibodies (antibodies to the antigen-combining site of other antibodies) may interfere with regulation of antibody activity.Genetic factors play a role. Relatives of patients with autoimmune disorders often have the same type of autoantibodies, and incidence of autoimmune disorders is higher in identical than fraternal twins. Women are affected more often than men. The genetic role appea