Embed Size (px)
Citation preview
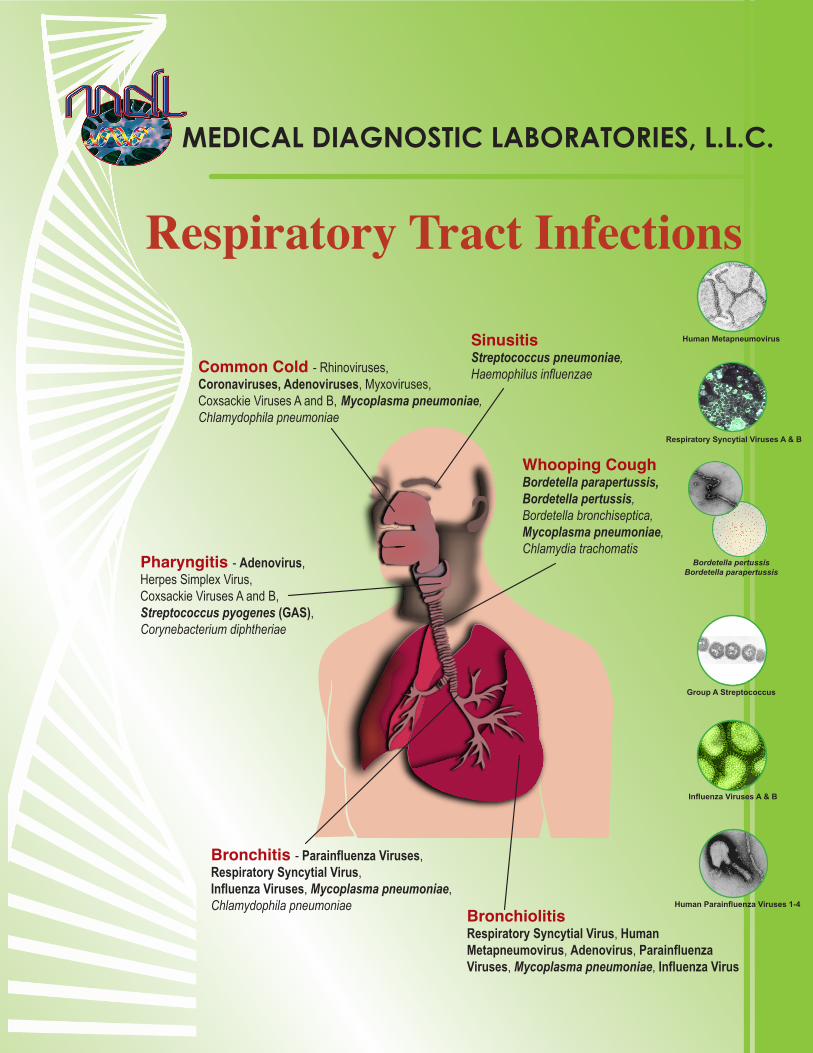
Respiratory Tract Infections
MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
BronchiolitisRespiratory Syncytial Virus, HumanMetapneumovirus, Adenovirus, ParainfluenzaViruses, Mycoplasma pneumoniae, Influenza Virus
Bronchitis - Parainfluenza Viruses,Respiratory Syncytial Virus,Influenza Viruses, Mycoplasma pneumoniae,Chlamydophila pneumoniae
Whooping CoughBordetella parapertussis,Bordetella pertussis,Bordetella bronchiseptica,Mycoplasma pneumoniae,Chlamydia trachomatis
SinusitisStreptococcus pneumoniae,Haemophilus influenzaeCommon Cold - Rhinoviruses,
Coronaviruses, Adenoviruses, Myxoviruses, Coxsackie Viruses A and B, Mycoplasma pneumoniae,Chlamydophila pneumoniae
Pharyngitis - Adenovirus,Herpes Simplex Virus,Coxsackie Viruses A and B, Streptococcus pyogenes (GAS),Corynebacterium diphtheriae
Human Metapneumovirus
Bordetella pertussis Bordetella parapertussis
Group A Streptococcus
Influenza Viruses A & B
Respiratory Syncytial Viruses A & B
Human Parainfluenza Viruses 1-4

Respiratory Tract Infection (RTI)
MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
www.mdlab.com • 877 269 0090
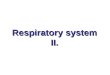
The respiratory tract is susceptible to infection by a host of bacterial and viral pathogens; the fact that they share similar clinical presentations makes differentiation and diagnosis difficult. In response to this, Medical Diagnostic Laboratories, L.L.C. (MDL) has designed a series of tests for the determination of respiratory pathogens utilizing the NasoSwab™ collection and transport device. Expanding upon its OneSwab® and UroSwab® methods of patient sampling, MDL’s NasoSwab™ represents a less invasive method of sample procurement that utilizes Flocked Swab Technology.
Pathogen Lavage (%) NasoSwab™ (%)Human metapneumovirus 13 (13.3) 12 (12.2)
RSV A 15 (15.3) 18 (18.4)RSV B 0 (0.0) 1 (1.0)Influenza A 2 (2.0) 2 (2.0)Influenza B 2 (2.0) 6 (6.0)B. parapertussis 0 (0.0) 0 (0.0)B. pertussis 0 (0.0) 0 (0.0)
Table 1. The NasoSwab™ collection method was directly compared to nasal lavage in a blinded study comprised of 98 pediatric patients. Seven Real-Time PCR assays developed by MDL were used in the comparison.
Determination, when performed, is typically via the somewhat invasive and uncomfortable method of nasal lavage, which typically serves as a deterrent for most patients. The search for a less invasive method of sampling led to the development of several generations of nasal swabs, differing in their choice of fibers (1). The clinical utility of these precursors was not proven, abilities and diagnostic values were consistently out-performed by nasal lavage (1). Some swab variations, particularly calcium alginate, were found to inhibit downstream PCR analyses (2). The flocked nature and conical shape of the MDL NasoSwab™ addresses this issue. A blinded comparison of NasoSwab™ to nasal lavage collection methods revealed substantial agreement between the two methods following Real-time PCR analyses (Table 1).
100. 8
82. 5
45. 4
40. 4
39. 5
6. 1
1. 6
30. 4
14. 3
14. 2
21
17. 7
114. 6
116. 9
0 20 40 60 80 100 120 140
C a n c e r
Dia be te s M e l l i tu s
C HD
A rth ri tis
S tro k e
Hy pe rte n s io n
V ira l R T I
C O P D
C HF
O ste o pe ro s is
A sth m a
M ig ra in e
O titis M e dia
A l le rg ic R h in itis
C o st (B i l l io n s US $)
Figure 1. Economic impact of viral respiratory tract infections in comparison to other common medical disorders. Adapted from (3).
The 2007 National Vital Statistics Report (4) lists chronic lower respiratory diseases and influenza/pneumonia as the fourth and seventh leading causes of death, respectively, when considering all ages. When analyzed by individual age group, chronic lower respiratory diseases are within the ten leading causes of death for ages 19 and under and 45 and up, while influenza/pneumonia remains a risk factor for all age groups (4, 5). Such statistical studies help define the at-risk populations as infants 6 months of age and younger, as well as the elderly and adults already diagnosed with a respiratory tract condition, such as Chronic Obstructive Pulmonary Disease (COPD) or asthma (5, 6). Within these populations, the burden of RTI is greater due to the lack or compromise of a fully developed immune system.
From an economic standpoint, lower respiratory tract infections were the seventh most costly malady in 2003, with 39.5 billion dollars spent on treatment (Figure 1) (3). This figure is further broken down into several factors to show the absolute cost of respiratory illness to an individual family, taking into consideration variables like
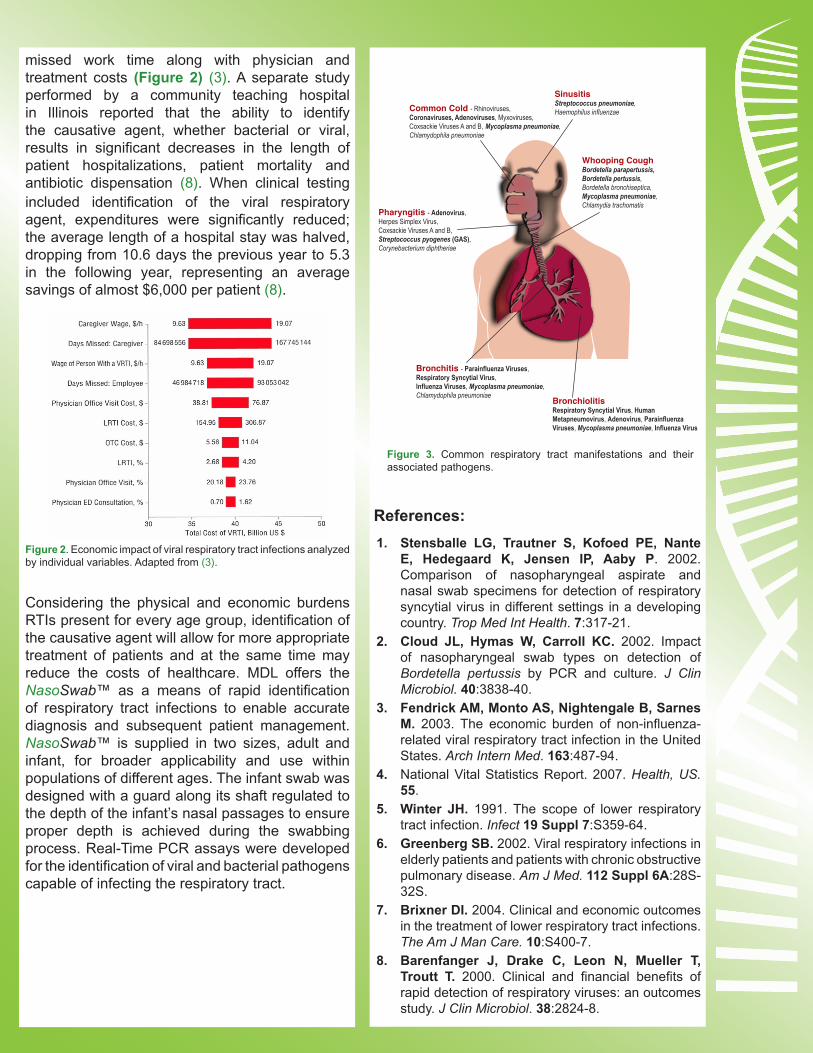
missed work time along with physician and treatment costs (Figure 2) (3). A separate study performed by a community teaching hospital in Illinois reported that the ability to identify the causative agent, whether bacterial or viral, results in significant decreases in the length of patient hospitalizations, patient mortality and antibiotic dispensation (8). When clinical testing included identification of the viral respiratory agent, expenditures were significantly reduced; the average length of a hospital stay was halved, dropping from 10.6 days the previous year to 5.3 in the following year, representing an average savings of almost $6,000 per patient (8).
Figure 2. Economic impact of viral respiratory tract infections analyzed by individual variables. Adapted from (3).
Considering the physical and economic burdens RTIs present for every age group, identification of the causative agent will allow for more appropriate treatment of patients and at the same time may reduce the costs of healthcare. MDL offers the NasoSwab™ as a means of rapid identification of respiratory tract infections to enable accurate diagnosis and subsequent patient management. NasoSwab™ is supplied in two sizes, adult and infant, for broader applicability and use within populations of different ages. The infant swab was designed with a guard along its shaft regulated to the depth of the infant’s nasal passages to ensure proper depth is achieved during the swabbing process. Real-Time PCR assays were developed for the identification of viral and bacterial pathogens capable of infecting the respiratory tract.
1. Stensballe LG, Trautner S, Kofoed PE, Nante E, Hedegaard K, Jensen IP, Aaby P. 2002. Comparison of nasopharyngeal aspirate and nasal swab specimens for detection of respiratory syncytial virus in different settings in a developing country. Trop Med Int Health. 7:317-21.
2. Cloud JL, Hymas W, Carroll KC. 2002. Impact of nasopharyngeal swab types on detection of Bordetella pertussis by PCR and culture. J Clin Microbiol. 40:3838-40.
3. Fendrick AM, Monto AS, Nightengale B, Sarnes M. 2003. The economic burden of non-influenza-related viral respiratory tract infection in the United States. Arch Intern Med. 163:487-94.
4. National Vital Statistics Report. 2007. Health, US. 55.
5. Winter JH. 1991. The scope of lower respiratory tract infection. Infect 19 Suppl 7:S359-64.
6. Greenberg SB. 2002. Viral respiratory infections in elderly patients and patients with chronic obstructive pulmonary disease. Am J Med. 112 Suppl 6A:28S-32S.
7. Brixner DI. 2004. Clinical and economic outcomes in the treatment of lower respiratory tract infections. The Am J Man Care. 10:S400-7.
8. Barenfanger J, Drake C, Leon N, Mueller T, Troutt T. 2000. Clinical and financial benefits of rapid detection of respiratory viruses: an outcomes study. J Clin Microbiol. 38:2824-8.
References:
BronchiolitisRespiratory Syncytial Virus, HumanMetapneumovirus, Adenovirus, ParainfluenzaViruses, Mycoplasma pneumoniae, Influenza Virus
Bronchitis - Parainfluenza Viruses,Respiratory Syncytial Virus,Influenza Viruses, Mycoplasma pneumoniae,Chlamydophila pneumoniae
Whooping CoughBordetella parapertussis,Bordetella pertussis,Bordetella bronchiseptica,Mycoplasma pneumoniae,Chlamydia trachomatis
SinusitisStreptococcus pneumoniae,Haemophilus influenzaeCommon Cold - Rhinoviruses,
Coronaviruses, Adenoviruses, Myxoviruses, Coxsackie Viruses A and B, Mycoplasma pneumoniae,Chlamydophila pneumoniae
Pharyngitis - Adenovirus,Herpes Simplex Virus,Coxsackie Viruses A and B, Streptococcus pyogenes (GAS),Corynebacterium diphtheriae
Figure 3. Common respiratory tract manifestations and their associated pathogens.

MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
www.mdlab.com • 877 269 0090
Bordetella pertussis & Bordetella parapertussis
Pertussis, commonly known as whooping cough, results from an upper respiratory tract infection with Bordetella pertussis or Bordetella parapertussis. A highly contagious and endemic disease, cases induced by infection with Bordetella parapertussis have been found to occur less frequently than those resulting from B. pertussis infection and often result in less severe infections (15). This infection was a significant cause of childhood morbidity and mortality in the early part of the twentieth century and reemerged as a significant health concern in the late 1990’s. The lowest point in the incidence of pertussis infection was attributed to the development and widespread use of pertussis vaccines. In 2002, 8,296 cases of pertussis were reported for an incidence of 3.01 cases per 100,000 people (5). Although a significant decrease from the baseline annual morbidity in 1922 (147,271 cases), the case than that reported in 2002 is a greater than 49% increase in pertussis cases reported in the 1980’s (6, 16). The upward trend in childhood pertussis cases has been primarily attributed to decreased vaccine usage, while the increase in adult pertussis cases is contributed to waning vaccine-induced immunity and the lack of a vaccine approved for use in adults (16). A third possibility, whereby the bacterium has genetically adapted itself to circumvent the vaccine, has also been demonstrated by an almost fifty year retrospective epidemiological study conducted in the Netherlands (15). This study involved the genetic fingerprinting of archived pertussis strains using seven year intervals for the comparative study (Figure 1). An initial decrease in genetic diversity was observed following the institution of widespread vaccination, followed by a period of increased genetic diversity. Genetic sequencing analyses revealed mutations within two key virulent factors, pertussis toxin and pertactin, to be associated with these expanding, diverse strains and the ability to circumvent vaccination strategies (15). Pertussis is the least well controlled of the reportable, vaccine preventable childhood diseases in the United States for which universal vaccination has been recommended (14).
Vaccination Strategies and SchedulesFactors that influence the susceptibility to pertussis infection include age, early administration of antibiotics before the onset of cough and immunity conferred by vaccination (14). A greater importance is given to the role of immunization since younger children are more susceptible to infection due to their lack of mature immune systems and antibiotic intervention following onset of cough has been deemed of limited efficacy. Unfortunately, the protection conferred by childhood pertussis vaccination wanes five to ten years post completion of childhood vaccination schedules, thereby leaving adolescents and adults susceptible (14). In 2005, the United States licensed Tdap, an acellular vaccine that
Figure 1: Increased genetic diversity of Bordetella pertussis following the initiation of widespread vaccination. Adapted from (15).
PathologyB. pertussis is a fastidious gram-negative coccobacillus that enters the respiratory tract through the inhalation of contaminated aerosols. The organism releases toxins that damage the airway epithelium to aid in host entry. While whooping cough can be caused by other Bordetella species, B. parapertussis, B. bronchiseptica and B. holmseii, B. pertussis remains the leading pathogenic cause. Illness caused by these other species is not preventable by vaccination (14). Colonization is achieved by the preferential adherence of B. pertussis to ciliated epithelium in the upper respiratory tract. This interaction is primarily mediated by filamentous hemaglutin (FHA) and Pertussis Toxin (PT) (3, 4, 11, 12, 13). FHA is also involved in the subsequent invasion of respiratory epithelial cells (11, 12). PT disrupts phagocytic functions reducing the body’s ability to clear an infection (1). Reduced mucous movement and coughing results from decreased ciliary beat frequency mediated by the B. pertussis tracheal cytotoxin (7, 9). The typical incubation period ranges from seven to ten days. The catarrhal and early paroxysmal stages of infection, which can last as long as six weeks, are the most infectious time frames and are often indistinguishable from other early stage respiratory infections (14).
SymptomsInfection with B. pertussis is characterized by three phases:the catarrhal, paroxysmal and convalescent phases. The catarrhal phase is generally characterized by fever, coughing, nasal congestion and malaise and lasts approximately ten days. These symptoms are indistinguishable from other upper respiratory infections. The paroxysmal phase is characterized
confers protection against tetanus, diphtheria and pertussis for use in adolescents and adults ages eleven to sixty-four (14). The Advisory Committee on Immunization Practices recommends the following Tdap administration schedule: a single dose to individuals between the ages of nineteen and sixty-four as either a booster or initial vaccination administration, administration as a booster every ten years, administration as a preventive measure for any individuals who are or will be in immediate contact with children under the age of twelve months and all health care workers having direct contact with patients (14).

References:by prolonged coughing followed by a characteristic “whoop” or inhalation as the patient attempts to catch his/her breath. In older children and adults, characteristic phases may not be observed. Instead these individuals typically present with prolonged coughing and headaches. Major complications, including hypoxia, apnea, pneumonia, seizures, and encephalopathy. Malnutrition can also occur, most often in infants or young children. In 2003, thirteen children died from complications of pertussis (5).
TransmissionB. pertussis is typically transmitted through direct contact with respiratory secretions and/or aerosols. It is not uncommon for colonized, older children to inadvertently expose their younger, unvaccinated siblings to B. pertussis. Patients are typically highly contagious during the catarrhal phase of infection, but are also able to transmit bacteria up to three weeks after the onset of coughing. Up to 90% of susceptible household members develop pertussis after exposure to an infected individual (5).
DiagnosisThe World Health Organization (WHO) has defined pertussis as a paroxysmal cough present for greater than 21 days in combination with either culture of B. pertussis or positive serology or contact with a culture-positive individual (17). Culture of B. pertussis can be hampered by the time point during the course of infection at which a sample is taken and by the age of the patient (10). Often B. pertussis cannot be cultured from patients that have entered the paroxysmal phase or from adult patients. Polymerase Chain Reaction (PCR) has also been used to diagnose B. pertussis infections. However, PCR, like culture, is more likely to be positive in the early stages of disease and less sensitive in adults (8). Current serology for B. pertussis infection is largely based upon antibody reactivity to FHA and PT. The presence of IgA is indicative of a natural, recent infection, whereas IgG appears during the paroxysmal phase and remains detectable for more than six months.
MDL utilizes the ViraStripe system for the detection of B. pertussis-specific IgG and IgA antibodies in serum. This Western blot based system detects antibody reactivity to filamentous hemagglutinin (220 kD) and the B subunit of Pertussis toxin (28 kD). The B. pertussis IgG ViraStripe has a sensitivity of 100% and a specificity of 97 to 98%. The B. pertussis IgA ViraStripe has a sensitivity of 100% and a specificity of 96 to 100%.
Pertussis serology may not be of clinical diagnostic value for infants less than three months of age due to the under development of the infants’ IgA response mechanism at this early age or in cases involving IgA-deficient patients of any age. For this reason, as well as for the early detection of respiratory diseases, MDL has expanded its testing to include two Real-Time PCR-based assays to be used in conjunction with their latest method of respiratory sampling, the NasoSwab™, for the detection of both B. pertussis and B. parapertussis. Previous studies have demonstrated the utility of both Dacron and Rayon nasopharyngeal swabs for the detection of pertussis species in PCR-based methodologies and discounted the utility of calcium alginate-based swabs due to their low sensitivity and specificity (2). NasoSwab™, due to its flocked, nylon nature and unique flexible, tapered head represents a marked advancement in respiratory swabbing technology that mirrors both the sensitivity and specificity of nasal lavage sampling methods in an easier, less invasive format.
1. Brown EJ, Newell AM, Gresham HD. 1987. Molecular recognition of phagocytic function. Evidence for involvement of a guanosine triphosphate-binding protein in opsonin-mediated phagocytosis by monocytes. J Immunol. 139:3777-3782.
2. Cloud JL, Hymas W, Carroll KC. 2002. Impact of nasopharyngeal swab types on detection of Bordetella pertussis by PCR and culture. J Clin Micro. 40(10):3838-3840.
3. Carbonetti NH, Artamonova GV, Andreasen C, Dudley E, Mays RM, Worthington ZE. 2004. Suppression of serum antibody responses by pertussis toxin after respiratory tract colonization by Bordetella pertussis and identification of an immunodominant lipoprotein. Infect Immun. 72:3350-3358.
4. Carbonetti NH, Artamonova GV, Mays RM, Worthington ZE. 2003. Pertussis toxin plays an early role in respiratory tract colonization by Bordetella pertussis. Infect Immun. 71:6358-6366.
5. Centers for Disease Control and Prevention. 2003. Pertussis. www.cdc.gov/ncidod/dbmd/diseaseinfo/pertussis_t.htm
6. Centers for Disease Control and Prevention, 1999. Achievements in Public Health, 1900-1999: Impact of Vaccines Universally Recommended for Children – United States, 1990-1998. 48;243-248.
7. Cookson BT, Cho HL, Herwaldt LA, Goldman WE. 1989. Biological activities and chemical composition of purified tracheal cytotoxin of Bordetella pertussis. Infect Immun. 57:2223-2229.
8. Dragsted DM, Dohn B, Madsen J, Jensen JS. 2004. Comparison of culture and PCR for detection of Bordetella pertussis and Bordetella parapertussis under routine laboratory conditions. J Med Microbiol. 53:749-754.
9. Goldman WE, Klapper DG, Baseman JB. 1982. Detection, isolation, and analysis of a released Bordetella pertussis product toxic to cultured tracheal cells. Infect. Immun. 36:782-794.
10. Granstrom, G, Wretlind B, Granstrom M. 1991. Diagnostic value of clinical and bacteriological findings in pertussis. J Infect. 22:17-26.
11. Ishibashi Y, Nishikawa A. 2002. Bordetella pertussis infection of human respiratory epithelial cells up-regulates intercellular adhesion molecule-1 expression: role of filamentous hemagglutinin and pertussis toxin. Microb Pathog. 33:115-125.
12. Ishibashi Y, Relman DA, Nishikawa A. 2001. Invasion of human respiratory epithelial cells by Bordetella pertussis: possible role for a filamentous hemagglutinin Arg-Gly-Asp sequence and α5β1 integrin. Microb Pathog. 30:279-288.
13. Ishibashi Y, Claus S, Relman DA. 1994. Bordetella pertussis filamentous hemagglutinin interacts with a leukocyte signal transduction complex and stimulates bacterial adherence to monocyte CR3 (CD11b/CD18). J Exp Med. 180:1225-1233.
14. Kretsinger K, Broder KR, Cortese MM, Joyce MP, Ortega-Sanchez I, Lee GM, Tiwari T, Cohn AC, Slade BA, Iskander JK, Mijalski CM, Brown KH, Murphy TV. 2006. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine. Centers for Disease Control and Prevention MMWR Recommendations and Reports December 15, 2006/55(RR17);1-33. http://www.cdc. gov/mmwr/preview/mmwrhtml/rr5517a1.htm Accessed May 17, 2007.
15. Mooi FR, van Loo IHM, King AJ. 2001. Adaptation of Bordetella pertussis to vaccination: a cause for its reemergence? Emerg Infect Dis 7(S3):526-528.
16. Tanaka M, Vitek CR, Pascual FP, Bisgard KM, Tate JE, Murphy TV. 2003. Trends in pertussis among infants in the United States, 1980-1999. JAMA. 290:2968-2975.
17. World Health Organization. 1991. WHO meeting on case definitions of pertussis, 10 to 11 January 1991, MIN/EPI/PERT91.1, p.4-5. World Health Organization, Geneva, Switzerland.

MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
www.mdlab.com • 877 269 0090
Group A Streptococcus
Group A Streptococcus (GAS), also referred to as beta hemolytic Streptococcus pyogenes, is a common pathogen of the upper respiratory tract that is commonly associated with acute bacterial pharyngitis (strep throat), as well as the cutaneous infections impetigo and necrotizing fasciitis. Long-term, non-suppurative complications associated with untreated or recurrent infections include rheumatic fever, scarlet fever and acute glomerulonephritis (2, 5). More recently, ever increasing pathogenic strains have been emerging which predominately affect the skin and soft tissue and can lead to potentially life-threatening systemic infections (4).
PathologyMost streptococcal strains have a predilection for the respiratory tract and GAS represents the most common cause of bacterial pharyngitis (5). This genus of bacterium represents a large and diverse group of gram-positive, non-motile cocci that morphologically tend to grow in pairs as short chains within clinical specimens (4, 6). There are more than twenty known streptococcus serotypes, designated alphabetically, of which serotypes A and B are the most clinically relevant (4). Streptococcus pyogenes, also referred to as Group A Streptococcus, is a common human pathogen and is estimated to be present asymptomatically in 5% to 15% of the population (6). Despite this asymptomatic carriage, GAS is considered to be an opportunistic pathogen such that the bacteria can become pathogenic within these carriers when the host’s immune defenses are compromised (6). SymptomologyThe incubation period for strep throat is 2 to 4 days post-exposure. Once infected, individuals can transmit infection for up to three weeks if they remain asymptomatic; however, initiation of an antibiotic regimen usually limits this time to approximately twenty-four hours (2, 5). Despite the quick decline in bacterial transmissibility, it is important that patients complete the full course of antibiotic therapy in order to prevent possible non-suppurative infections, the most notable of which is acute rheumatic fever, from occurring in the subsequent weeks following infection (5).
Transmission occurs via direct contact with contaminated saliva, aerosolized nasal discharge or skin wounds of an infected individual with the mucous membranes or via inhalation by non-infected individuals. Crowded living conditions, such as dormitories and nursing homes, have been shown to increase the rate of transmission. Reports of tainted milk and milk-based products serving as vehicles of transmission have also been reported (2). Transmission from asymptomatic individuals who serve as carriers occurs in very rare instances.
FrequencyGAS infections are endemic worldwide. Within the United States, upper respiratory tract infections (UTI) predominate within northern regions and typically follow a winter/spring seasonal pattern. UTIs rarely affect neonates due to the transplacental exchange of protective antibodies from mother to child but are a common cause of pharyngitis among children older than three years of age (4). The CDC reports that over ten million cases of noninvasive GAS occur annually (1). In contrast, streptococcus-induced skin infections appear to predominate in warmer climates and can occur year round.
ComplicationsPrior to the age of antibiotic therapy, S. pyogenes infections posed a significant public health risk. Both suppurative and non-suppurative complications can occur following GAS infections. Suppurative infections include otitis media and sinusitis within the respiratory tract as well as streptococcal bacteremia, the cutaneous infection, necrotizing fasciitis, and, rarely, meningitis or brain abscess (5). Non-suppurative infections, including rheumatic fever, post-streptococcal glomerulonephritis, Sydenham’s chorea and streptococcal toxic shock syndrome (sTSS), can occur weeks or months following infection. Rheumatic fever, characterized by joint and valvular heart disease, typically occurs within three weeks of infection and was found to be the most frequently occurring complication (1).
VaccineCurrently, there is no vaccine available for GAS but several companies are researching and developing such a product. The impetus behind the development of such a vaccine stems from the non-suppurative infections GAS induces, most notably rheumatic fever.

References:
TreatmentBoth the American Heart Association and the Infectious Disease Society of America have chosen penicillin as the treatment of choice for GAS infections despite studies that have demonstrated higher clinical cure rates to be associated with cephalosporin (5). Treatment typically consists of a ten day course of either penicillin or its derivative, amoxicillin; this single course is quite effective at eradicating the bacterium so long as the patient is fully compliant (5). Although rare, there have been instances where the initial treatment failed and required follow-up administration with a cephalopsporin class drug. The ability to differentiate between true infection and carrier status is critical.
DiagnosisDue to the fact that both pharyngitis and tonsillitis are induced by a number of respiratory pathogens, a confirmatory diagnosis is recommended prior to initiating treatment. Throat culture and point-of-care tests are the most common methods while Polymerase Chain Reaction (PCR)-based amplification methods are on the rise.
Throat Cultures remain the most common confirmatory method of diagnosis. This method requires that a swab of the patient’s throat be streaked across a blood agar plate, which promotes GAS growth, in the presence of a bacitracin-impregnated disc. The use of blood agar is confirmatory only for the presence of GAS in this assay, whereby, the beta hemolytic activity associated with GAS is evaluated based on the cultured bacterium’s ability to lyse red blood cells and their sensitivity to the drug bacitracin (4). Plates are incubated for at least twenty-four hours, at which point they are monitored for growth. Negatively scored plates are traditionally incubated for an additional twenty-four hours for true confirmation. The limitations of this method include the reporting of a significant number of false negatives and the selective evaluation for GAS only. This method has an estimated 10% false negative reporting rate associated with it; the issue of asymptomatic GAS carriers, or false positives, is resolved based on the lack of overt symptoms that would confirm the presence of an active infection (5). Also, the selective nature of the culturing procedure neither allows for the evaluation nor identification of other possible causative bacterium (5).
Point-of-care tests represent a significant increase over traditional, culture-based methods having the capability to identify causative pathogens in as few as twenty minutes in some instances, allowing for confirmatory diagnosis and treatment while the patient waits. These assays are centered around the identification of a bacterial-specific protein based on its ability to bind a DNA probe in either an enzymatic-based or a chemiluminescent–based assay (5). While these tests are typically highly specific, having 95% or greater specificities, they suffer from a lack of sensitivity, which usually necessitates throat culturing as a follow-up, confirmatory test for all negative specimens.
Real-Time PCR reactions, when designed and validated properly, can be a fast and efficient means of diagnosing infections. This method involves the repeated amplification of specific genetic elements. They also have added benefit of being able to speciate among related pathogens.
MDL has developed a new method of respiratory tract sampling, the NasoSwab™, and a series of Real-Time PCR assays to aid physicians in discerning the causative agents responsible for these overlapping symptoms. The novel “flocked-swab” technology employed by the NasoSwab™ represents a less invasive manner of sampling the upper respiratory tract whose particle retention, as measured by both level of specificity and sensitivity by an independent, blinded study, matches or exceeds the levels obtained with nasal washes. The employ of specialized media allows for room temperature storage of specimens which serves to preserve the integrity of the pathogen better than does the immediate freezing of nasal wash specimens.
1. Centers for Disease Control and Prevention: Division of Bacterial and Mycotic Diseases. October 11, 2005, posting date. Group A Streptococcal (GAS) Disease. Accessed October 18, 2007. http://www.cdc.gov/ncidod/dbmd/diseaseinfo/groupastreptococcal_t.htm.
2. National Institute of Allergy and Infectious Diseases. Group A Streptococcal Infections. Accessed October 15, 2007. http://www.niaid.nih.gov/factsheets/strep.htm.
3. Group A Streptococcal vaccine development: current status and issues of relevance to less developed countries. Accessed October 18, 2007. http://www.who.int/child-adolescent-health/publications/CHILD_HEALTH/DP/Topic_2/paper_3.htm.
4. Schleiss MR. Streptococcal Infection, Group A. Accessed October 15, 2007. http://www.emedicine.com/ped/topic2702.htm.
5. Sharma S. Streptococcus Group A Infections. Accessed October 15, 2007. http://www.emedicine.com/med/topic2184.htm.
6. Todar K. Todar’s Online Textbook of Bacteriology. Accessed October 15, 2007. http://www.textbookofbacteriology.net/
7. Ebell MH, Smith MA, Barry HC, Ives K, Carey M. 2000. The rational clinical examination. Does the patient have strep throat? JAMA Dec 13;284(22):2912-8.
Table 1. Probability of various etiological causes of pharyngitis. Adapted from (7).
Viral StreptococcalEpstein-Barr virusChlamydia pneumoniaeMycoplasma pneumoniaeNeisseria gonorrhoeae Haemophilus influenzae type bCandidiasisDiphtheria
50-80 5-36 1-102-52-51-21-2<1<1
Etiology Probability, %

Influenza Virus
MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
www.mdlab.com • 877 269 0090
The Influenza virus is a segmented, negative sense, single-stranded RNA virus. The genome, which is approximately 12 to 14 kb in size, encodes for ten proteins (7). There are three strains of influenza, A, B and C, that vary from one another in their pathogenicity. Influenza A strains induce the most severe infections and are capable of infecting both humans and animals, while B strain infections are more restricted to humans and are not as severe (12, 18). Influenza C strains are associated with very little illness and are not deemed a public health threat (18). The segmented viral genome of influenza allows for its constant alteration, either by point mutation during viral replication (antigenic drift) or the reassortment of individual genomic segments (antigenic shift) (5). The process of antigenic drift has allowed for adamantine-resistant strains of influenza to surface, rendering both amantadine and rimantadine prophylactic strategies useless. Medical Diagnostic Laboratories, L.L.C. offers free reflexive testing for all influenza A specimens for the determination of resistant strains. Providing this information to physicians allows patients to be better informed and to take the precautionary measures to limit its spread.
Figure 1. Summary of influenza typed strains during the 2006-2007 season. WHO/NREVSS collaborative study (6).
PathogenesisThe process of antigenic drift occurs slowly and affects both A and B viral strains. In contrast, antigenic shift occurs more rapidly and only affects influenza A strains. The reassortment of these genomic segments occurs as a result of coinfections within mammals, allowing for the mixing of viral genomes (19). Within the influenza A viruses, individual reassortant strains are subtyped by the genomic segments that are affected, the hemagglutinin (H) and neuraminidase (N) structural proteins. Due to this, influenza A strains are typically referred to by the type of both hemagglutinins, of which there are 16, and neuraminidase, of which there are 9, incorporated using the HxNx designation. Alterations within these genomic segments impact the infectious process
directly because these structural proteins are critical to the virus’ life cycle: hemagglutinin aids the viral entry of host cells and neuraminidase is required for viral budding from infected cells (11). Every season influenza viruses are typed as a method of surveilling for the emergence of new strains and to aid in determining which strains will be included in the vaccine for the following season.
Pandemic Deaths
United States Worldwide
1918-19 675,000+ 50,000,000+
1957-58 70,000+ 1-2,000,000
1968-69 34,000+ 700,000+
Table 1. The death toll following pandemic influenza viral infections.
The emergence of recombinant strains, against which people have little or no immunity, increases the likelihood of another influenza pandemic (18). In 1918, the worst influenza pandemic to strike the world occurred, killing 50 million people (Table 1). While pandemics of the 1918 proportion typically do not occur frequently, occurring approximately every 50 years, the ability of the influenzas to undergo genetic reassortment increases the likelihood of developing another highly lethal strain (18). The last emergence of a novel influenza A strain occurred during the 1968-69 flu season when H3N2 was introduced, inducing a minor pandemic (15). Recently, the emergence of the H5N1 strain in 1997, often referred to as avian flu due to the fact that it emerged from chickens, has the world prepared for the occurrence of a new pandemic (19).
Clinical SignificanceThe peak of influenza season begins in late December and extends through early March (6, 18). Infections are highly contagious and readily transmitted through the aerosolization of or direct contact with respiratory secretions. Upper respiratory tract epithelial cells serve as the initial site of viral infection, resulting in both the desquamation of ciliated epithelia and the loss of protective mucocilia (20). The incubation period for influenza is typically 1 to 4 days and is dependent upon the level of exposure (18). Infected individuals can transmit the virus prior to the onset of symptoms and continue to shed virus in their nasal secretions for approximately five days (18). Patients will present with typical flu-like symptoms, defined by the sudden onset of fever, headache, chills, malaise and myalgia, all of which are the by-products of interferon production and the activation of the body’s natural defense, the antiviral pathway (10, 18). Individuals with underlying medical conditions or compromised immunity, including the elderly, are prone to more severe infection and are at increased risk of developing pneumonia (8).

TreatmentThe adamantine class of drugs, which includes amantadine and ramantadine, are known to be effective at limiting influenza infections to a subclinical infection in 70% to 90% of the cases (4). These drugs are effective against A strains of influenza, targeting the M2 protein that is unique to these strains. Through both selective pressure and the virus’ propensity to mutate, adamantine-resistant viral strains have emerged. Single point mutations of critical residues within the M2 gene are capable of conferring drug resistance (4, 9). The sudden rise in transmission of resistant H3N2 strains observed within the United States has been attributed to the misuse of over-the-counter amantadine in China following the SARS outbreak (9). Within the United States, the rate of resistance rose 12.6% from the 2004 season, a 1.9% incidence rate, to a 14.5% incidence rate for the first six months of the 2005 season (Table 2) (4). Currently, the CDC recommends administration with either zanamivir or oseltamivir within the first two days of symptom onset when dealing with susceptible strains.
Table 2. Incidence of adamantine resistant influenza isolates. Adopted from (9).
VaccineThe number of hospitalizations as a result of influenza infection is approximately 200,000 annually. Hospitalizations are typically higher in years with circulating type A strains (12). Annually, 3,600 deaths occur as a result of infection in the United States. The elderly and children under the age of two constitute an especially susceptible segment of the population (Figure 2) (2, 17, 18). Children under the age of 23 months are at greater risk of hospitalization; determining an exact rate due to influenza infection is difficult due to the substantial overlap with respiratory syncytial virus (RSV) (14, 21). Adequate vaccination coverage can markedly decrease the infective rate (18). There are currently two types of immunizations available: inactivated influenza vaccine and the live, attenuated influenza vaccine (LAIV). Both vaccine strategies contain strains that are antigenically similar to those predicted to circulate that season, typically including one H3N2, one H1N1 and one B virus (18). For children under the age of 9 years, two administrations of vaccine are suggested for proper effectiveness (1, 16). Several studies have demonstrated reductions in both direct and indirect medical costs as a result of more thorough vaccination, particularly in children and adults 65 years and older (3, 13).
1. Allison MA, Daley MF, Crane LA, Barrow J, Beaty BL, Allred N, Berman S, Kempe A. 2006. Influenza vaccine effectiveness in healthy 6 to 21 month old children during the 2003-2004 season. J Pediatr 149:755-762.
2. Bhat N, Wright JG, Broder KR, Murray EL, Greenberg ME, Glover MJ, Likos AM, Posey DL, Klimov A, Lindstrom SE, Balish A, Medina MJ, Wallis TR, Guarner J, Paddock CD, Shieh WJ, Zaki SR, Sejvar JJ, Shay DK, Harper SA, Cox NJ, Fukuda K, Uyeki TM. 2005. Influenza-associated deaths among children in the United States, 2003-2004. N Engl J Med 353:2559-67.
3. Bridges, CB, Thompson WW, Meltzer MI, Reeve GR, Talamonti WJ, Cox NJ, Lilac HA, Hall A, Klimov A, Fukuda K. 2000. Effectiveness and cost-benefit of influenza vaccination of healthy working adults: A randomized controlled trial. JAMA 284:1655-63.
4. Bright, RA, Shay DK, Shu B, Cox NJ, Klimov AI. 2006. Adamantine resistance among influenza A viruses isolated early during the 2005-2006 influenza season in the United States. JAMA 295:891-4.
5. Centers for Disease Control and Prevention. 2006. High levels of adamantine resistance among influenza A (H3N2) viruses and interim guidelines for use of antiviral agents--United States, 2005-06 influenza season. MMWR Morb Mortal Wkly Rep 55:44-6.
6. Centers for Disease Control and Prevention. 2007. Weekly Report: Influenza Summary Update Week ending May19, 2007-Week 20.
7. Cheung, TK, Poon LL. 2007. Biology of influenza A virus. Ann N Y Acad Sci 1102:1-25.
8. Falsey, AR, Walsh EE. 2006. Viral pneumonia in older adults. Clin Infect Dis 42:518-24.
9. Hayden, FG. 2006. Antiviral resistance in influenza viruses--implications for management and pandemic response. N Engl J Med 354:785-8.
10. Horisberger, MA. 1995. Interferons, Mx genes, and resistance to influenza virus. Am J Respir Crit Care Med 152:S67-71.
11. Lanzrein, M, Schlegel A, Kempf C. 1994. Entry and uncoating of enveloped viruses. Biochem J 302 ( Pt 2):313-20.
12. Meissner, H. C. 2005. Reducing the impact of viral respiratory infections in children. Pediatr Clin North Am 52:695-710, v.
13. Nichol, KL, Wuorenma J, von Sternberg T. 1998. Benefits of influenza vaccination for low, intermediate, and high-risk senior citizens. Arch Intern Med 158:1769-76.
14. O’Brien, MA, Uyeki TM, Shay DK, Thompson WW, Kleinman K, McAdam A, Yu XJ, Platt R, Lieu TA. 2004. Incidence of outpatient visits and hospitalizations related to influenza in infants and young children. Pediatr 113:585-93.
15. Reichert, TA. 2005. Preparing for the next influenza pandemic: lessons from multinational data. Pediatr Infect Dis J 24:S228-31.
16. Ritzwoller, DP, Bridges CB, Shetterly S, Yamasaki K, Kolczak M, France EK. 2005. Effectiveness of the 2003-2004 influenza vaccine among children 6 months to 8 years of age, with 1 vs 2 doses. Pediatr 116:153-9.
17. Simonsen, L, Reichert TA, Viboud C, Blackwelder WC, Taylor RJ, Miller MA. 2005. Impact of influenza vaccination on seasonal mortality in the US elderly population. Arch Intern Med 165:265-72.
18. Smith, NM, Bresee JS, Shay DK, Uyeki TM, Cox NJ, Strikas RA. 2006. Prevention and Control of Influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 55:1-42.
19. Sorrell, EM, Ramirez-Nieto GC, Gomez-Osorio IG, Perez DR. 2007. Genesis of pandemic influenza. Cytogenet Genome Res 117:394-402.
20. Thompson, CI, Barclay WS, Zambon MC, Pickles RJ. 2006. Infection of human airway epithelium by human and avian strains of influenza A virus. J Virol 80:8060-8.
21. Thompson, WW, Shay DK, Weintraub E, Brammer L, Bridges CB, Cox NJ, Fukuda K. 2004. Influenza-associated hospitalizations in the United States. JAMA 292:1333-40.
60,000
50,000
40,000
30,000
0
10,000
20,000
1968-69Pandemic
1968-70to
1979-80
1980-81to
1989-90
1990-91to
2000-2001
>85 65-74
75-84 <65
Figure 2. Influenza-related deaths by age group.
References:
Respiratory Syncytial Virus (RSV)
MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
www.mdlab.com • 877 269 0090
Respiratory syncytial virus, (RSV) is a viral pathogen which most severely affects infants and the elderly. Originally isolated from a chimpanzee with an upper respiratory tract infection (URTI), the virus was named Chimpanzee coryza in 1956 and was not named RSV until its isolation from a child suffering from pneumonia (1). The virus is comprised of ten proteins, all of which are encoded for by a non-segmented RNA genome. The name “respiratory syncytial virus” was assigned based on the pathologic observation that infected cells form syncytia in vitro (13). Two viral subtypes are known, A and B, each having multiple genotypes.
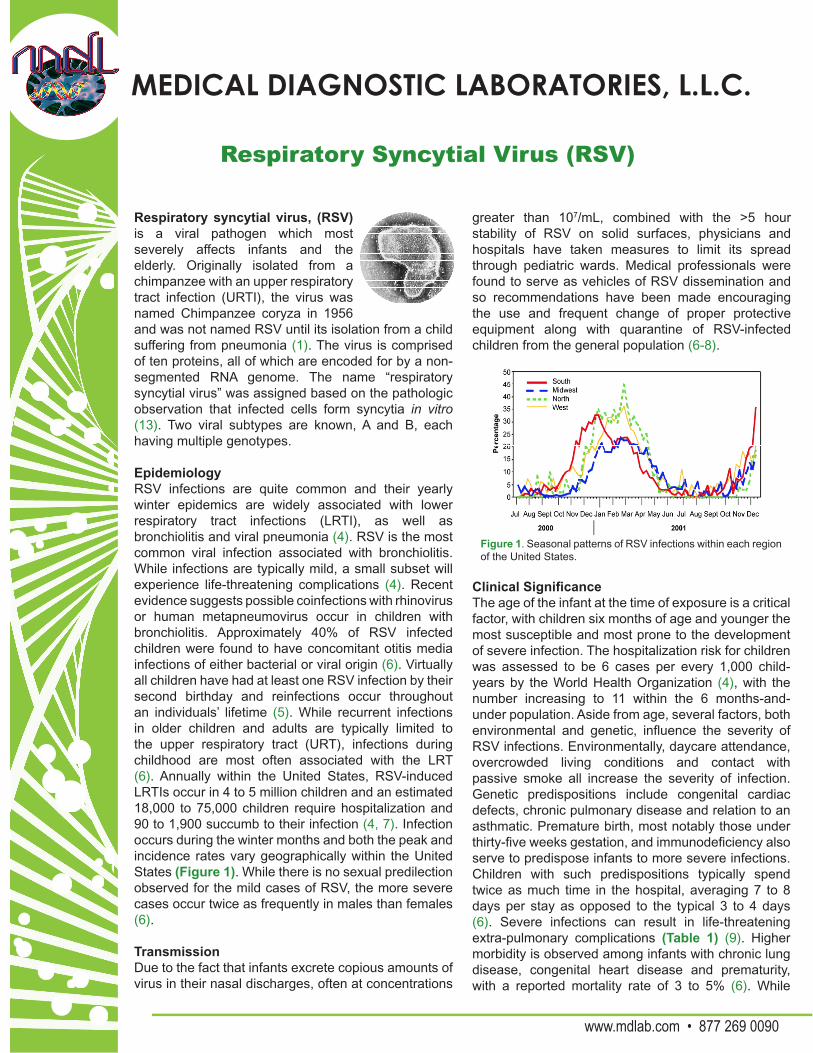
EpidemiologyRSV infections are quite common and their yearly winter epidemics are widely associated with lower respiratory tract infections (LRTI), as well as bronchiolitis and viral pneumonia (4). RSV is the most common viral infection associated with bronchiolitis. While infections are typically mild, a small subset will experience life-threatening complications (4). Recent evidence suggests possible coinfections with rhinovirus or human metapneumovirus occur in children with bronchiolitis. Approximately 40% of RSV infected children were found to have concomitant otitis media infections of either bacterial or viral origin (6). Virtually all children have had at least one RSV infection by their second birthday and reinfections occur throughout an individuals’ lifetime (5). While recurrent infections in older children and adults are typically limited to the upper respiratory tract (URT), infections during childhood are most often associated with the LRT (6). Annually within the United States, RSV-induced LRTIs occur in 4 to 5 million children and an estimated 18,000 to 75,000 children require hospitalization and 90 to 1,900 succumb to their infection (4, 7). Infection occurs during the winter months and both the peak and incidence rates vary geographically within the United States (Figure 1). While there is no sexual predilection observed for the mild cases of RSV, the more severe cases occur twice as frequently in males than females (6).
TransmissionDue to the fact that infants excrete copious amounts of virus in their nasal discharges, often at concentrations
greater than 107/mL, combined with the >5 hour stability of RSV on solid surfaces, physicians and hospitals have taken measures to limit its spread through pediatric wards. Medical professionals were found to serve as vehicles of RSV dissemination and so recommendations have been made encouraging the use and frequent change of proper protective equipment along with quarantine of RSV-infected children from the general population (6-8).
Figure 1. Seasonal patterns of RSV infections within each region of the United States.
Clinical SignificanceThe age of the infant at the time of exposure is a critical factor, with children six months of age and younger the most susceptible and most prone to the development of severe infection. The hospitalization risk for children was assessed to be 6 cases per every 1,000 child-years by the World Health Organization (4), with the number increasing to 11 within the 6 months-and-under population. Aside from age, several factors, both environmental and genetic, influence the severity of RSV infections. Environmentally, daycare attendance, overcrowded living conditions and contact with passive smoke all increase the severity of infection. Genetic predispositions include congenital cardiac defects, chronic pulmonary disease and relation to an asthmatic. Premature birth, most notably those under thirty-five weeks gestation, and immunodeficiency also serve to predispose infants to more severe infections. Children with such predispositions typically spend twice as much time in the hospital, averaging 7 to 8 days per stay as opposed to the typical 3 to 4 days (6). Severe infections can result in life-threatening extra-pulmonary complications (Table 1) (9). Higher morbidity is observed among infants with chronic lung disease, congenital heart disease and prematurity, with a reported mortality rate of 3 to 5% (6). While
Blount RE, Morris JA, Savage RE. 1956. Recovery of cytopathogenic agent from chimpanzees with coryza. Proceedings of the Society for Experimental Biology and Medicine Society for Experimental Biology and Medicine (New York, NY). 92:544-9.
Hall CB, Walsh EE, Schnabel KC, Long CE, McConnochie KM, Hildreth SW, Anderson LJ. 1990. Occurrence of groups A and B of respiratory syncytial virus over 15 years: associated epidemiologic and clinical characteristics in hospitalized and ambulatory children. J Infect Dis 162:1283-90.
Martinello RA, Chen MD, Weibel C, Kahn JS. 2002. Correlation between respiratory syncytial virus genotype and severity of illness. J Infect Dis 186:839-42.
Meissner HC, Long SS. 2003. Revised indications for the use of palivizumab and respiratory syncytial virus immune globulin intravenous for the prevention of respiratory syncytial virus infections. Pediatr 112:1447-52.
Glezen WP, Taber LH, Frank AL, Kasel JA. 1986. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Children (1960) 140:543-6.
Hall CB, Douglas RG, Jr. 1981. Nosocomial respiratory syncytial viral infections. Should gowns and masks be used? Am J Dis Children (1960) 135:512-5.
Murphy D, Todd JK, Chao RK, Orr I, McIntosh K. 1981. The use of gowns and masks to control respiratory illness in pediatric hospital personnel. J Pediatr 99:746-50.
Gala CL, Hall CB, Schnabel KC, Pincus PH, Blossom P, Hildreth SW, Betts RF, Douglas RG Jr. 1986.The use of eye-nose goggles to control nosocomial respiratory syncytial virus infection. JAMA 256:2706-8.
Eisenhut M. 2006. Extrapulmonary manifestations of severe respiratory syncytial virus infection--a systematic review. Crit Care (London, England) 10:R107.
Kho N, Kerrigan JF, Tong T, Browne R, Knilans J. 2004. Respiratory syncytial virus infection and neurologic abnormalities: retrospective cohort study. J Child Neurol 19:859-64.
Sweetman LL, Ng YT, Butler IJ, Bodensteiner JB. 2005. Neurologic complications associated with respiratory syncytial virus. Pediatr Neurol 32:307-10.
Armstrong DS, Menahem S. 1993. Cardiac arrhythmias as a manifestation of acquired heart disease in association with paediatric respiratory syncitial virus infection. J Pediatr Child Health 29:309-11.
Thomas JA, Raroque S, Scott WA, Toro-Figueroa LO, Levin DL. 1997. Successful treatment of severe dysrhythmias in infants with respiratory syncytial virus infections: two cases and a literature review. Crit Care Med 25:880-6.
Hutchison JS, Joubert GI, Whitehouse SR, Kissoon N. 1994. Pericardial effusion and cardiac tamponade after respiratory syncytial viral infection. Pediatr Emerg Care 10:219-21.
Griffin N, Keeling JW, Tomlinson AH. 1979. Reye’s syndrome associated with respiratory syncytial virus infection. Arch Dis Childhood 54:74-6.
MacFarlane P, Denham J, Assous J, Hughes C. 2005. RSV testing in bronchiolitis: which nasal sampling method is best? Arch Dis Childhood 90:634-5.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
References:
Organs Affected Complications References
Brain Apneas; status (10, 11)
epilepticus
HeartVentricular
tachycardia; (12-14)
ventricular fibrilation;
cardiogenic shock;
complete heart blockpericardial tamponade
Brain, liver Reye’s Syndrome (15)
and kidney
Table 1. Life-threatening extrapulmonary complications that can result from severe RSV infection (11).
Saline Nasal Wash NasoSwab™
Positive Negative Total Positive Negative Total
Po
siti
veb
y P
CR Abnormal 9 8 17 15 2 17
Normal 0 11 11 0 12 12
Total 9 19 28 15 14 29
Table 2. Comparison of two collection methods for the detection of RSV in nasal specimens in a blinded study. The standard saline nasal wash was compared to the NasoSwab™ method of collection. The NasoSwab™ collection method proved to be more sensitive, having an 88.2% detection rate as opposed to the 52.9% obtained with the nasal wash method.
most reports concerning RSV are focused on children, RSV has more recently been recognized as a cause of morbidity in elderly populations previously attributed to influenza (4).
DiagnosisProcurement of a respiratory specimen is less painful using a swabbing technique as opposed to a nasal aspirate. A study published in 2005 compared both nasal sampling methods. That study concluded that traditional nasal swabbing techniques were less reliable than nasal aspirates. A similar study undertaken by Medical Diagnostic Laboratories, L.L.C. using flocked swab technology demonstrates the utility of nasal swabbing for the detection of respiratory pathogens in both pediatric and adult populations. The flocked nature of the MDL NasoSwab™ is comprised of Dacron® fibers arranged in a conical shape. The unique shape allows for sampling deeper within the nasal passages unlike traditionally shaped swabs and its flocked nature captures pathogens more completely. The results of this study demonstrate greater accuracy associated with the NasoSwab™, detecting RSV in 15 of 17 samples, while the traditional nasal wash only identified 9 (Table 2). To serve both pediatric and adult populations, NasoSwab™ is packaged with individual swabs for use in either group.
MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
www.mdlab.com • 877 269 0090
Human Parainfluenza Viruses
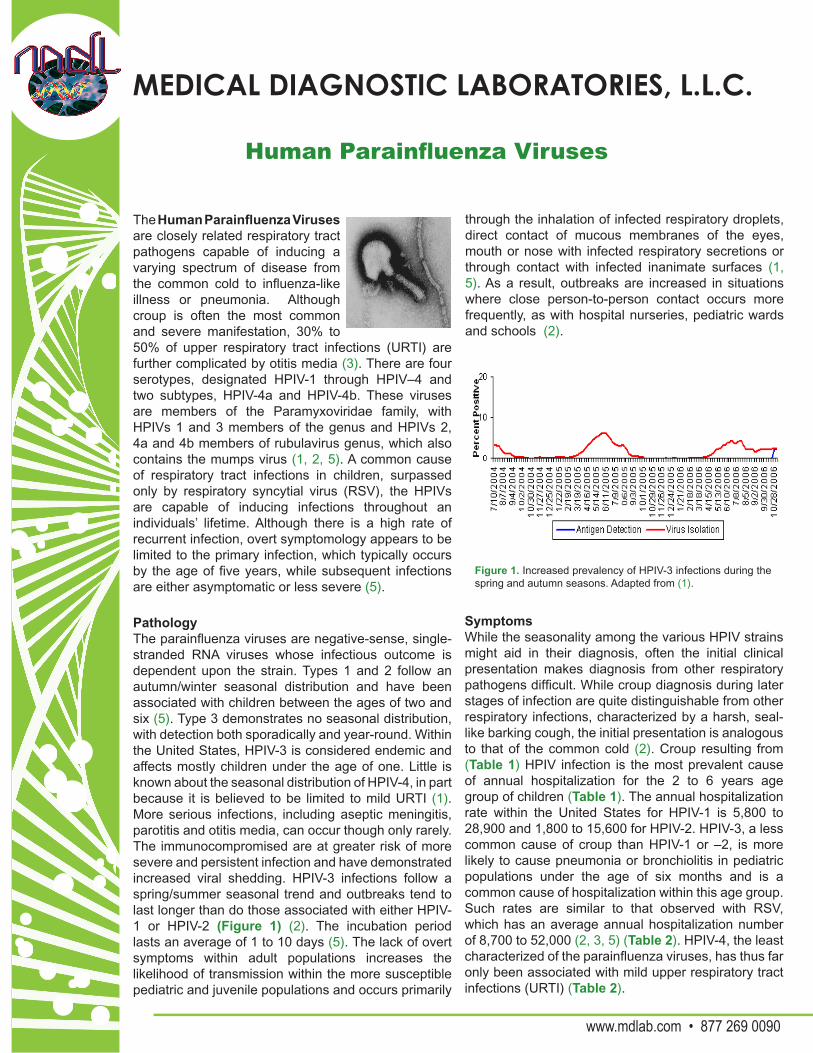
The Human Parainfluenza Viruses are closely related respiratory tract pathogens capable of inducing a varying spectrum of disease from the common cold to influenza-like illness or pneumonia. Although croup is often the most common and severe manifestation, 30% to 50% of upper respiratory tract infections (URTI) are further complicated by otitis media (3). There are four serotypes, designated HPIV-1 through HPIV–4 and two subtypes, HPIV-4a and HPIV-4b. These viruses are members of the Paramyxoviridae family, with HPIVs 1 and 3 members of the genus and HPIVs 2, 4a and 4b members of rubulavirus genus, which also contains the mumps virus (1, 2, 5). A common cause of respiratory tract infections in children, surpassed only by respiratory syncytial virus (RSV), the HPIVs are capable of inducing infections throughout an individuals’ lifetime. Although there is a high rate of recurrent infection, overt symptomology appears to be limited to the primary infection, which typically occurs by the age of five years, while subsequent infections are either asymptomatic or less severe (5).
PathologyThe parainfluenza viruses are negative-sense, single-stranded RNA viruses whose infectious outcome is dependent upon the strain. Types 1 and 2 follow an autumn/winter seasonal distribution and have been associated with children between the ages of two and six (5). Type 3 demonstrates no seasonal distribution, with detection both sporadically and year-round. Within the United States, HPIV-3 is considered endemic and affects mostly children under the age of one. Little is known about the seasonal distribution of HPIV-4, in part because it is believed to be limited to mild URTI (1). More serious infections, including aseptic meningitis, parotitis and otitis media, can occur though only rarely. The immunocompromised are at greater risk of more severe and persistent infection and have demonstrated increased viral shedding. HPIV-3 infections follow a spring/summer seasonal trend and outbreaks tend to last longer than do those associated with either HPIV-1 or HPIV-2 (Figure 1) (2). The incubation period lasts an average of 1 to 10 days (5). The lack of overt symptoms within adult populations increases the likelihood of transmission within the more susceptible pediatric and juvenile populations and occurs primarily
SymptomsWhile the seasonality among the various HPIV strains might aid in their diagnosis, often the initial clinical presentation makes diagnosis from other respiratory pathogens difficult. While croup diagnosis during later stages of infection are quite distinguishable from other respiratory infections, characterized by a harsh, seal-like barking cough, the initial presentation is analogous to that of the common cold (2). Croup resulting from (Table 1) HPIV infection is the most prevalent cause of annual hospitalization for the 2 to 6 years age group of children (Table 1). The annual hospitalization rate within the United States for HPIV-1 is 5,800 to 28,900 and 1,800 to 15,600 for HPIV-2. HPIV-3, a less common cause of croup than HPIV-1 or –2, is more likely to cause pneumonia or bronchiolitis in pediatric populations under the age of six months and is a common cause of hospitalization within this age group. Such rates are similar to that observed with RSV, which has an average annual hospitalization number of 8,700 to 52,000 (2, 3, 5) (Table 2). HPIV-4, the least characterized of the parainfluenza viruses, has thus far only been associated with mild upper respiratory tract infections (URTI) (Table 2).
Figure 1. Increased prevalency of HPIV-3 infections during the spring and autumn seasons. Adapted from (1).
through the inhalation of infected respiratory droplets, direct contact of mucous membranes of the eyes, mouth or nose with infected respiratory secretions or through contact with infected inanimate surfaces (1, 5). As a result, outbreaks are increased in situations where close person-to-person contact occurs more frequently, as with hospital nurseries, pediatric wards and schools (2).

References:
VaccinePresently, there are no vaccines available to confer protection against infection with any of the HPIV strains; children are totally reliant upon the passive immunity transferred to them from their mothers. Presently, there are two HPIV-3 and one HPIV-1 vaccine strategies currently under development. These strategies have thus far been hampered by an inability to balance the viral replication required within the child upon vaccination for the induction of a proper immune response in the presence of maternally conferred antibodies (3).
DiagnosisHPIV infections during childhood are quite common, as revealed by retrospective serological surveys that have shown 90% or greater of children aged five years and under have been exposed to HPIV-3 and approximately 75% of this population has been exposed to HPIV-1 and HPIV-2 based on the presence of strain-specific antibodies (3). The fact that these serotypes display a marked age differential, with respect to infection, makes the ability to differentiate among these species necessary from a diagnostic standpoint. Two methods, direct detection of the virus and indirect methods, are considered acceptable. Direct detection methods encapsulate those methods that directly identify viral elements, whether DNA, RNA or protein, while indirect methods typically infer an infection has occurred based upon the presence of viral-specific antibodies in the patient’s serum.
Indirect Methods:IFA/ ELISABoth the IFA and ELISA methods of indirect detection base the occurrence of infection upon the presence of viral-specific antibodies within patient sera. Such assays can be either for IgM (early stage infection) or IgG (late stage infection) and are subject to the sensitivity and specificity of the antibodies employed; deficiencies in either parameter can increase the likelihood of false positive or false negative determinations. The utilization of such methods, at least with respect to identifying the cause of respiratory infections, is whether or not the patient, particularly pediatric patients, have immune systems capable of producing either antibody class. (Figure 1) demonstrates this point with respect to HPIV-3 detection whereby viral antigens were undetectable within the 1 year and younger age group despite the clear ability to isolate the virus from these individuals (1). Diagnoses of HPIV-4 infections are further complicated due to their antigenic cross-reactivity with the mumps (2).
1. Centers for Disease Control and Prevention: Respiratory and Enteric Virus Branch. Last updated on June 6, 2006. Human Parainfluenza Viruses (Common cold and croup). Accessed October 15, 2007. http://cdc.gov/ncidod/dvrd/revb/respiratory/hpivfeat.htm.
2. Parainfluenza Virus Infections. Accessed October 15, 2007. http://www.merck.com/mmpe/sec14/ch188/ch188e.html
3. The World Health Organization: Initiative for Vaccine Research. Parainfluenza viruses. Accessed October 15, 2007. http://www.who.int/vaccine_research/diseases/ari/en/index2.html.
4. Parainfluenza Viruses. Accessed October 15, 2007. http://virology-online.com/viruses/Parainfluenza.htm.
5. N. Narayan, M. D. Parainfluenza Virus. Accessed October 15, 2007. http://pathmicro.med.sc.edu/virol/para-rsv-aden.htm
6. Drews, A. L., R. L. Atmar, W. P. Glezen, B. D. Baxter, P. A. Piedra, and S. B. Greenberg. 1997. Dual respiratory virus infections. Clin Infect Dis 25:1421-9.
Infectious Outcome Viral TypeMinor URTI 1, 3, 4Bronchitis 1, 3Pneumonia 1, 3Croup 1, 2, 3
Table 1. Infectious outcomes of HPIV subtype infection. Adapted from (4).
Direct Methods:Immunofluorescent StainingRespiratory secretions can be smeared along a glass slide for incubation with viral-specific antibodies and visualized directly through immunofluorescent microscopy. The limitations associated with such assays are the need for specialized, expensive equipment, the unavailability or poor specificity of commercially available antibodies and the high degree of time and skill required to process such samples.
Polymerase Chain Reaction (PCR)PCR reactions, when designed and validated properly, can be a fast and efficient means of diagnosing infections. This method involves the repeated amplification of viral-specific genetic elements that can often serve to speciate among the conserved HPIV viruses.
MDL has developed a new method of respiratory tract sampling, the NasoSwab™, and a series of Real-Time PCR assays to aid physicians in discerning the causative agent responsible for these overlapping symptoms. The novel “flocked-swab” technology employed by the NasoSwab™ represents a less invasive manner of sampling the upper respiratory tract whose particle retention, as measured by both level, of specificity and sensitivity by an independent, blinded study, matches or exceeds the levels obtained with nasal washes. The use of specialized stabilization media allows for room temperature storage of specimen that serves to preserve the integrity of the pathogen better than does the immediate freezing of nasal wash specimen.
Table 2. Incidence of parainfluenza co-infection with other respiratory pathogens. Adapted from (6).
Virus combinations No. of patients (% with DRVI)Influenzavirus A, picornavirus 10 (14.9)Picornavirus, coronavirus 10 (14.9)Adenovirus, picornavirus 7 (10.4)Influenzavirus A, RSV 7 (10.4)RSV, parainfluenzavirus 6 (9.0)RSV, picornavirus 4 (6.0)RSV, coronavirus 4 (6.0)Parainfluenzavirus, coronavirus 4 (6.0)Influenzavirus A, adenovirus 4 (6.0) Influenzavirus A, influenzavirus B 3 (4.5)Influenzavirus A, parainfluenzavirus 2 (3.0)Influenzavirus A, coronavirus 2 (3.0)Influenzavirus B, RSV 2 (3.0Influenzavirus A (H1), influenzavirus A (H3) 1 (1.5)Influenzavirus B, adenovirus 1 (1.5)Influenzavirus B, picornavirus 1 (1.5)Influenzavirus B, coronavirus 1 (1.5)Parainfluenzavirus, adenovirus 1 (1.5)Parainfluenzavirus, picornavirus 1 (1.5)Influenzavirus A, RSV, coronavirus 1 (1.5) Total 67 (100)

MEDICAL DIAGNOSTIC LABORATORIES, L.L.C.
www.mdlab.com • 877 269 0090
Human Metapneumovirus
Human Metapneumovirus (hMPV) is a relatively recently identified cause of respiratory tract infection. Identified in 2001 by a Dutch group performing a retrospective evaluation of nasal secretions collected over a twenty year period, hMPV was found to be present in twenty of the twenty-eight samples that were subjected to random-priming Polymerase Chain Reaction (PCR) amplification (24). Sequence analysis confirmed the isolation of a heretofore unknown respiratory pathogen and also demonstrated it to be most closely related to avian pneumovirus, a member of the genus Metapneumovirus (24). Despite its recent identification, a screen of banked human sera revealed that hMPV did not recently “jump” into human populations but was circulating among them for at least fifty years (24). Sera analyses also revealed that a high rate of infection is associated with hMPV, with nearly all children age five years having had prior exposure to the virus (13) (Table 1).
shown the virus is capable of inducing both chronic and acute inflammatory changes of the airways and organizing lung injuries (2, 23, 25). This common cause of pediatric bronchiolitis is believed to serve as a risk factor for the onset of childhood asthma and has been shown to exacerbate congestive heart disease and chronic obstructive pulmonary disease (COPD) in adult populations (9, 10, 26).
Clinical SignificanceHuman metapneumovirus infections are responsible for a large number of lower respiratory tract infections (LRTI) in pediatric populations, second only to RSV with respect to the number of bronchiolitis cases (3, 4, 17, 18). Various studies report an average incidence rate between 5% and 15%, though higher rates have been documented in individual reports (3, 6, 8, 14, 16). Children age 4 months and younger appear to be the most susceptible population, with relatively high frequencies reported for all children 2 years of age and under (11) (Figure 1). The virus is transmitted via inhalation of infected respiratory droplets or through direct contact with respiratory secretions or contaminated surfaces (15). Symptoms of infection are indistinguishable from those following RSV infection and range from mild upper RTI to more severe LRTI that include bronchiolitis and pneumonia (3). British studies demonstrated that a more severe bronchiolitis was associated with hMPV/RSV co-infections suggesting hMPV may serve as a determinant of RSV disease severity (12, 21). A winter/spring seasonality has been reported within temperate zones, although some summer outbreaks have been reported worldwide (20) (Figure 2).
Table 1. Seroprevalence rates for hMPV and RSV in juvenile populations. Adapted from (7).
PathologyThe genome of hMPV is comprised of negative-sense, single-stranded RNA whose genes are arranged in a manner similar to that of its most closely related human pathogen, respiratory syncytial virus (RSV), another pneumovirus. This relatively high degree of homology between hMPV and RSV, combined with their overlapping epidemiologies and symptomologies and disease courses, complicates diagnoses. However, reverse transcriptase PCR-based (RT-PCR) diagnostic methodologies capable of exploiting the sequence variations between these related viruses do exist and are considered the preferred method of differentiation (5). While the bulk of hMPV pathological information has been obtained from animal studies, two separate reports from analyses of human lung biopsies have
Figure 1. Age distribution of hMPV infections as determined by a Real-Time PCR-based diagnostic method in juvenile populations. Adapted from (11).
hMPV RSV% Positive % Positive
Age (# positive / # tested)
(# positive / # tested)
< 4 months 67 (6/9) 78 (7/9)4 Months to 1 Year 11 (3/27) 48 (13/27)1-2 Years 44 (17/39) 54 (21/39)2-5 Years 76 (19/25) 87 (21/25)

TreatmentAntiviral therapies for viral respiratory infections, with the exception of influenza virus, have not shown much efficacy (13, 17). The ineffectiveness of such therapy is believed to be due to the induction of high levels of inflammation within the airway epithelia following either hMPV or RSV infection. Ribaviran therapy has been employed for severe cases of hMPV and RSV infections with some reported success but remains a controversial form of treatment (1). Presently, the most promising hMPV therapy currently under development is the prophylactic treatment of high-risk children with neutralizing antibodies directed against hMPV’s F protein (22). Presently, there are no available vaccines for the prevention or limitation of hMPV infection.
Figure 2. Seasonal distribution of hMPV infections. Black bars show the number of tested positive specimens while the black line shows the percent positivity for hMPV. Adapted from (19).
1. Committee on Infectious Diseases. 1996. Reassessment of the indications for ribavirin therapy in respiratory syncytial virus infections. American Academy of Pediatrics Committee on Infectious Diseases. Pediatrics 97(1):137-40.
2. Bao, X, Liu T, Spetch L, Kolli D, Garofalo RP, Casola A. 2007. Airway epithelial cell response to human metapneumovirus infection. Virol.(2007). doi:10.1016/j.virol.2007.06.023
3. Boivin G, De Serres G, Cote S, Gilca R, Abed Y, Rochette L, Bergeron MG, Dery P. 2003. Human metapneumovirus infections in hospitalized children. Emerg Infect Dis 9:634-40.
4. Chano F, Rousseau C, Laferriere C, Couillard M, Charest H. 2005. Epidemiological survey of human metapneumovirus infection in a large pediatric tertiary care center. J Clin Microbiol 43:5520-5.
5. Deffrasnes C, Hamelin, Boivin G. 2007. Human metapneumovirus. Semin Respir Crit Care Med 28:213-21.
6. Dollner H, Risnes K, Radtke A, Nordbo SA. 2004. Outbreak of human metapneumovirus infection in norwegian children. Pediatr Infect Dis J 23:436-40.
7. Ebihara T, Endo R, Kikuta H, Ishiguro N, Ishiko H, Kobayashi K. 2004. Comparison of the seroprevalence of human metapneumovirus and human respiratory syncytial virus. J Med Virol 72:304-6.
DiagnosisThe fastidious nature of the virus coupled with the extremely slow nature of direct culturing methods prevents this method to be employed as a diagnostic tool. Currently, RT-PCR methods are considered to be the fastest and most reliable means of clinical evaluation, offering the added benefit of being able to differentiate between a host of respiratory pathogens that present initially with overlapping symptomologies. Serological testing thus far has only proved useful in retrospective studies as the high rate of infections within pediatric populations precludes their use as a diagnostic tool.
8. Esper F, Martinello RA, Boucher D, Weibel C, Ferguson D, Landry ML, Kahn JS. 2004. A 1-year experience with human metapneumovirus in children aged <5 years. J Infect Dis 189:1388-96.
9. Falsey AR, Erdman D, Anderson LJ, Walsh EE. 2003. Human metapneumovirus infections in young and elderly adults. J Infect Dis 187:785-90.
10. Garcia-Garcia ML, Calvo C, Casas I, Bracamonte T, Rellan A, Gozalo F, Tenorio T, Perez-Brena P. 2007. Human metapneumovirus bronchiolitis in infancy is an important risk factor for asthma at age 5. Pediatr Pulmonol 42:458-64.
11. Gray GC, Capuano AW, Setterquist SF, Erdman DD, Nobbs ND, Abed Y, Doern GV, Starks SE, Boivin G. 2006. Multi-year study of human metapneumovirus infection at a large US Midwestern Medical Referral Center. J Clin Virol 37:269-76.
12. Greensill J, McNamara PS, Dove W, Flanagan B, Smyth RL, Hart CA. 2003. Human metapneumovirus in severe respiratory syncytial virus bronchiolitis. Emerg Infect Dis 9:372-5.
13. Kahn JS. 2006. Epidemiology of human metapneumovirus. Clin Microbiol Rev 19:546-57.
14. Maggi F, Pifferi M, Vatteroni M, Fornai C, Tempestini E, Anzilotti S, Lanini L, Andreoli E, Ragazzo V, Pistello M, Specter S, Bendinelli M. 2003. Human metapneumovirus associated with respiratory tract infections in a 3-year study of nasal swabs from infants in Italy. J Clin Microbiol 41:2987-91.
15. Mahalingam S, Schwarze J, Zaid A, Nissen M, Sloots T, Tauro S, Storer J, Alvarez R, Tripp RA. 2006. Perspective on the host response to human metapneumovirus infection: what can we learn from respiratory syncytial virus infections? Microbes Infect 8:285-93.
16. McAdam AJ, Hasenbein ME, Feldman HA, Cole SE, Offermann JT, Riley AM, Lieu TA. 2004. Human metapneumovirus in children tested at a tertiary-care hospital. J Infect Dis 190:20-6.
17. McIntosh K, McAdam AJ. 2004. Human metapneumovirus--an important new respiratory virus. N Engl J Med 350:431-3.
18. Mullins JA, Erdman DD, Weinberg GA, Edwards K, Hall CB, Walker FJ, Iwane M, Anderson LJ. 2004. Human metapneumovirus infection among children hospitalized with acute respiratory illness. Emerg Infect Dis 10:700-5.
19. Pabbaraju K, Wong S, McMillan T, Lee BE, Fox JD. 2007. Diagnosis and epidemiological studies of human metapneumovirus using real-time PCR. J Clin Virol 40(3):186-92.
20. Peiris JS, Tang WH, Chan KH, Khong PL, Guan Y, Lau YL, Chiu SS. 2003. Children with respiratory disease associated with metapneumovirus in Hong Kong. Emerg Infect Dis 9:628-33.
21. Semple MG, Cowell A, Dove W, Greensill J, McNamara PS, Halfhide C, Shears P, Smyth RL, Hart CA. 2005. Dual infection of infants by human metapneumovirus and human respiratory syncytial virus is strongly associated with severe bronchiolitis. J Infect Dis 191:382-6.
22. Skiadopoulos MH, Biacchesi S, Buchholz UJ, Amaro-Carambot E, Surman SR, Collins PL, Murphy BR. 2006. Individual contributions of the human metapneumovirus F, G, and SH surface glycoproteins to the induction of neutralizing antibodies and protective immunity. Virology 345:492-501.
23. Sumino KC, Agapov E, Pierce RA, Trulock EP, Pfeifer JD, Ritter JH, Gaudreault-Keener M, Storch GA, Holtzman NJ. 2005. Detection of severe human metapneumovirus infection by real-time polymerase chain reaction and histopathological assessment. J Infect Dis 192:1052-60.
24. van den Hoogen BG, de Jong JC, Groen J, Kuiken T, de Groot R, Fouchier RA, Osterhaus AD. 2001. A newly discovered human pneumovirus isolated from young children with respiratory tract disease. Nat Med 7:719-24.
25. Vargas SO, Kozakewich HP, Perez-Atayde AR, McAdam AJ. 2004. Pathology of human metapneumovirus infection: insights into the pathogenesis of a newly identified respiratory virus. Pediatr Dev Pathol 7:478-86; discussion 421.
26. Williams JV, Crowe JE, Enriquez R, Minton P, Peebles RS, Hamilton RG, Higgins S, Griffin M, Hartert TV. 2005. Human metapneumovirus infection plays an etiologic role in acute asthma exacerbations requiring hospitalization in adults. J Infect Dis 192:1149-53.
Jan
05
Feb
05
Mar
05
Apr
05
May
05
Jun
05
Jul 0
5
Aug
05
Sep
05
Oct
05
Nov
05
Dec
05
Jan
06
Feb
06
Mar
06
Apr
06
May
06
Jun
06
Jul 0
6
Aug
06
Sep
06
Oct
06
18%
16%
14%
12%10%
8%
6%
4%2%
0%

Medical Diagnostic Laboratories, L.L.C.2439 Kuser Road • Hamilton, NJ 08690-3303
www.mdlab.com • Toll Free 877 269 0090