Embed Size (px)
Citation preview

Editors' Corner
Allergy at Seventy-Five
It is now 75 years since Von Pirquet proposed the term allergy to describe the changes that an animal undergoes after contact with a foreign substance (1). Allergic and related disorders constitute one of the most important groups of diseases attributable to abnormal immune responses. Classic allergies include such diverse condi- tions as asthma, allergic rhinitis, atopic dermatitis, urticaria, and the ill-defined group of food allergies. The pathogenesis of these diseases is related to the interaction of antigens (often called allergens) with antibody of the immunoglobulin E (IgE) class and the subsequent release from mast cells and basophils of powerful mediators such as histamine, seroto- nin, and the slow-reactive substance of anaphylaxis. There is a general familial susceptibility to this entire group of diseases referred to as atopy. However, the precise mode of inheri- tance is still unclear.
The recognition that IgE is the principal immunoglobulin involved in allergic disorders has permitted rapid advances in investigations of the basic immunochemistry of allergy. Infor-
mation about the structure of IgE and its complementary receptors on basophils and mast cells has accumu- lated during the past few years, and detailed knowledge of the mecha- nisms by which interaction of allergen with cell-bound IgE leads to release of the mediators is expected. In parallel, the genetic and cellular basis of regu- lation of IgE synthesis is being studied in experimental animals and humans. It is now recognized, for example, that a special population of T lymphocytes governs IgE pro- duction.
Despite the accelerating accumu- lation of information about the im- munology of allergic disorders, their diagnosis and treatment remain diffi- cult problems. For diagnosis, the allergist depends primarily on a de- tailed history, supplemented with selected skin tests with a battery of potential allergens. An important recent advance is the introduction of the radioallergosorbent technique (PAST) to measure antibodies of the IgE class. However, correlation of PAST with clinical hypersensitivity is sometimes difficult. Treatment still consists of non-specific control of symptoms or specific injection
therapy with the responsible aller- gens.
An important first step for further study of allergic diseases is better characterization of the substances responsible for initiating these dis- orders. Attempts to prepare purified allergens for use in both diagnosis and specific treatment depend upon the separation of individual antigens in the allergenic preparations. The eventual goal of standardizing aller- genic extracts is discussed by Dr. Harold Baer in this issue of the Newsletter. He points to the con- siderable progress that has been made during the past decade. It is equally obvious, however, that we have only scratched the skin (pardon the pun) of this difficult problem. The 10-15°70 of our population who suffer from significant allergic disorders are anxiously awaiting futher progress.
N. R. R.
Reference 1. C. V. Pirquet. 1906. Allergy. Munch.
Med. Wochenschr. 30:1457. Reprinted in P. G. H. Gell, and R. R. A. Coombs (eds.), Clinical aspects of immunology, F. A. Davis, Philadelphia, 1963, pp. 805-807.
Results of Questionnaire: Automation in Clinical Immunology
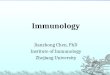
The Newsletter's questionnaire concerning "The Use of Automated Equipment in Clinical Immunology" (Clinical Immunology Newsletter, vol. 2, no. l) yielded only a modest total of 27 responses. Results, how- ever, were most interesting. The majority of respondents (24) use automated or semiautomated equip- ment. The most commonly performed tests are immunoglobulin quantita- tion and measurement of C3 and C4 levels. More than 20 tests were listed as being performed with automated equipment. The most popular piece of equipment is the nephelometer. Spectrophotometers for reading enzyme immunoassays are also used
|
by several laboratories, as is the FIAX apparatus, which permits quantitative fluorometric measure- ment. The rating of the assays in- dicates nephelometry is the method most favored over other assays; the Beckman ICS apparatus is especially popular. Twenty-two out of 24 re- spondents who have used automated equipment indicated that the use of automation is cost-effectivb.
Three individuals who did not employ automated equipment re- sponded to the questionnaire. Two of these respondents indicated that they are familiar with such assays; again nephelometry was most prominently mentioned, and both reported that
they plan to use automation in the future. The third response was from a small community hospital where only a few immunologic tests are per- formed each week.
Although the response was only from a small number of individuals, some general conclusions can be drawn from the comments of the responders. Automated equipment, as currently designed and used, is more appropriate for the medium to large hospital or laboratory in order to be cost-effective. The equip- ment must be versatile and appli- cable to tests for several serum pro- teins. Nephelometry, FIAX and spectrophotometer-based assays for
97
reading enzyme assays all fit these criteria and are generally rated favorably. Automation is well estab-
lished in clinical immunology; refine- ment and improvement of testing with such equipment should expand
the use of automation considerably in the near future.
1. Use of automated equipment: 24 Yes 3 No
2. Tests performed using automation:
22 Immunoglobulin levels (IgG, M, A) 19 Complement components (C3, C4) 12 Haptoglobin 11 X-1 antitrypsin 9 C-reactive protein 8 Antinuclear antibody 8 Transferrin 5 Albumin 5 Rubella 4 Anti-DNA 7 RIA (IgE, DNA, HB~AG) 2 Aminoglycoside levels 1 Ceruloplasmin 1 Carcinoembryonic antigen 1 Lymphocyte blastogenesis,
MLC, CML I Methotrexate
4. Number of immunology technologists/technicians in laboratory: 7 1-2 9 3-4 5 5-6 3 >6
3. Equipment used:
Type Manufacturer 15 Nephelometer Beckman 4 Nephelometer Hyland 5 FIAX International Diagnostic (IDT) 4 EMIT Spectrophotometer Gilford 3 ELISA Spectrophotometer Abbott 2 Liquid Scintillation
counter Beckman 2 Liquid Scintillation
counter Nuclear-Chicago 1 Liquid Scintillation
counter Packard 2 Densitometer Beckman 1 Gamma Counter Tracor 1 Gamma Counter Beckman 2 Automated
Immunoprecipitin (ALP) 1 Sample Harvester M.A. Bioproducts 1 Sample Harvester Otto Heller 1 Titertek Cell Harvester Flow 1 Microprocessor Hewlett-Packard 1 Spectrofluorometer Amicon-Bowman
5. Will you use (increase your use of) technologic equipment in the future?
26 Yes 1 No
7. Equipment known to respondents:
16 Nephelometer (Beckman) 5 Nephelometer (Hyland) 3 Nephelometer (Behring) 7 FlAX (IDT)
15 ELISA/EMIT 6 RIA 3 Automated Microtiter 2 Automated Reagin
testing (ART) (Technicon) 1 AFT-II (Calbiochem) 1 ACA (Dupont) 1 SMA (Technicon) 1 Cytofluorograph
6. Have you found automated equipment to be cost-effective?
22 Yes 2 No 3 Not Applicable
8. Evaluation of equipment used--excellent (1) to poor (5):
1 2 3 4
Nephelometer (Beckman) 8 9 Nephelometer (Hyland) 2 2 Automated microtiter 1 Liquid Scintillation 2 Cell Harvester. 1 RIA 1 FIAX 3 3 1 2 EMIT 2 ELISA 2 Cytofluorograph 1 AIP 1 1 ART 1 Gamma Counting 1
98















![of the innate immune response Clinical Immunology (Orlando ...researchonline.lshtm.ac.uk/1128/1/main.pdf · obtained by parental questionnaire using the ISAAC phase II protocol [8]](https://img.pdfslide.net/doc/110x75/5fe5d3c1cc05a6128714ae8d/of-the-innate-immune-response-clinical-immunology-orlando-obtained-by-parental.jpg)