Embed Size (px)
Citation preview

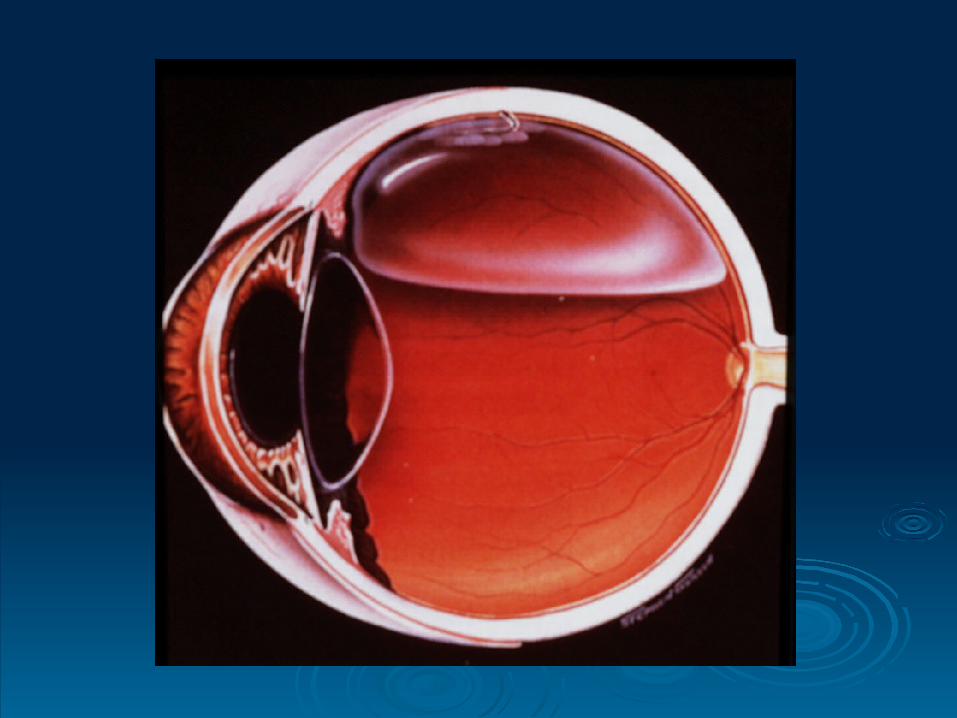
Retinal DetachmentRetinal Detachment
Abdulkrim Alkharashi , MDAbdulkrim Alkharashi , MD
RD History: RD History:
1.1. Theory of distension. Theory of distension.
2.2. Theory of hypotony. Theory of hypotony.
3.3. Theory of exudation. Theory of exudation.
4.4. Theory of retinal breaks. Theory of retinal breaks.
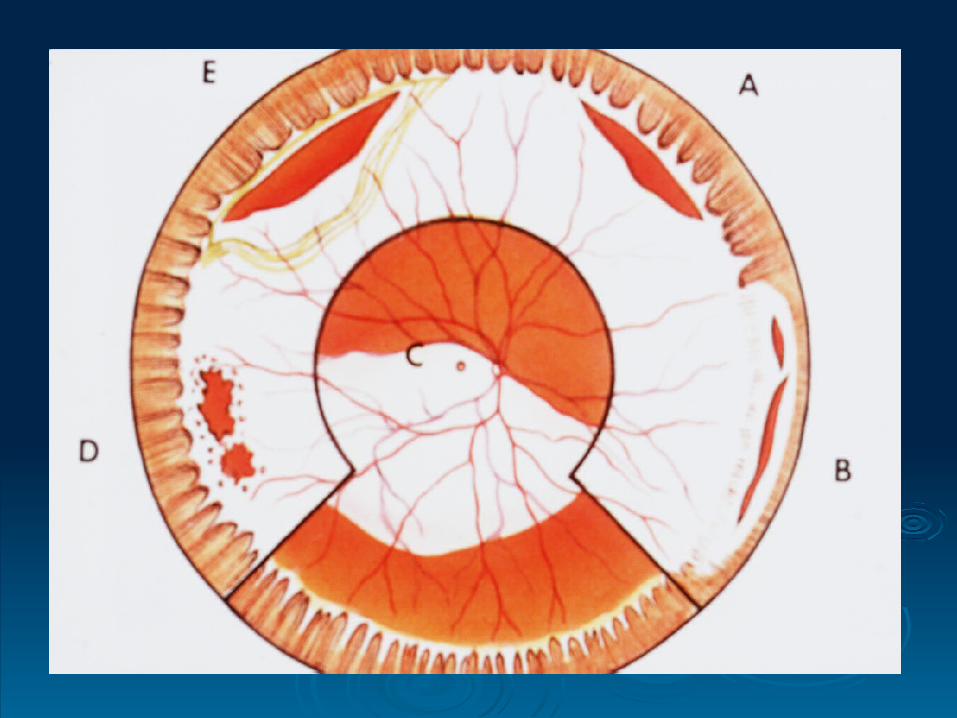
Causes of primary RD:-Causes of primary RD:-
RD History: cont. RD History: cont.
Beer – 1817 first to detect RD clinically. Beer – 1817 first to detect RD clinically. Von Helmholtz – 1851 invented the Von Helmholtz – 1851 invented the
ophthalmoscope. ophthalmoscope. Coccius – 1853 first to find retinal breaks Coccius – 1853 first to find retinal breaks
(r.b.). (r.b.). De Wecker – 1870 first suggested that r.b. De Wecker – 1870 first suggested that r.b.
were the causes of were the causes of RD. RD.
RD History: cont. RD History: cont.
Leber – 1882 found r.b. in 70% of RD, vit. Leber – 1882 found r.b. in 70% of RD, vit. deg. and collapse deg. and collapse traction traction r.b. r.b. RD. RD. Changed to pre-retinal memb. Changed to pre-retinal memb. r.b. (in PVR). r.b. (in PVR).
Jules Gonin – 1919 Father of RD surgery. Jules Gonin – 1919 Father of RD surgery. Performed the first RD operation to close r.b. – Performed the first RD operation to close r.b. – Ignipuncture of Thermocautery. Ignipuncture of Thermocautery.

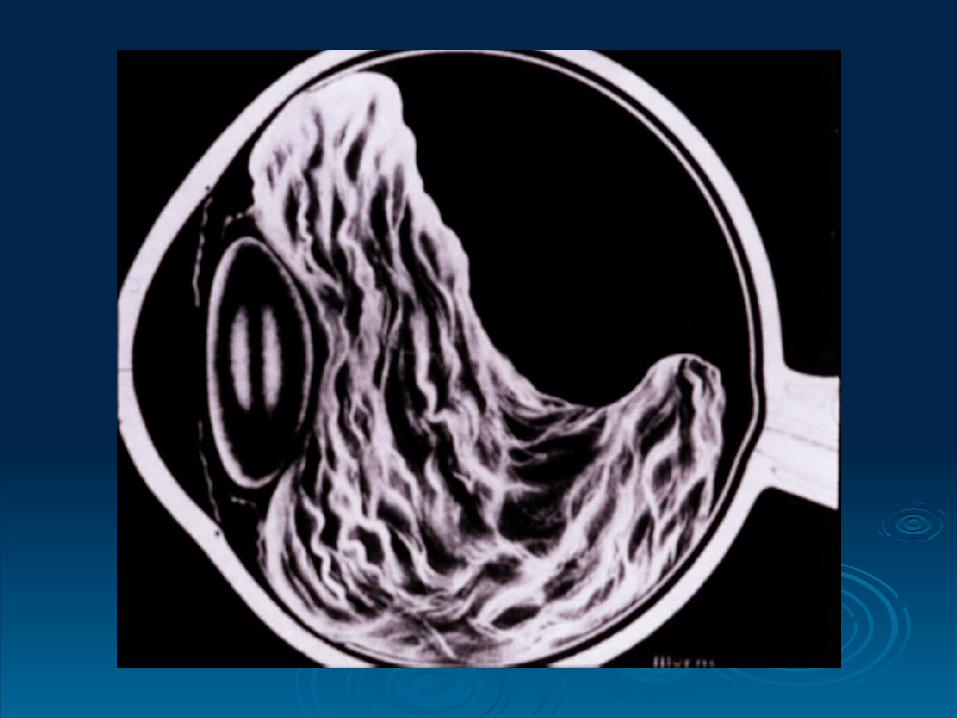
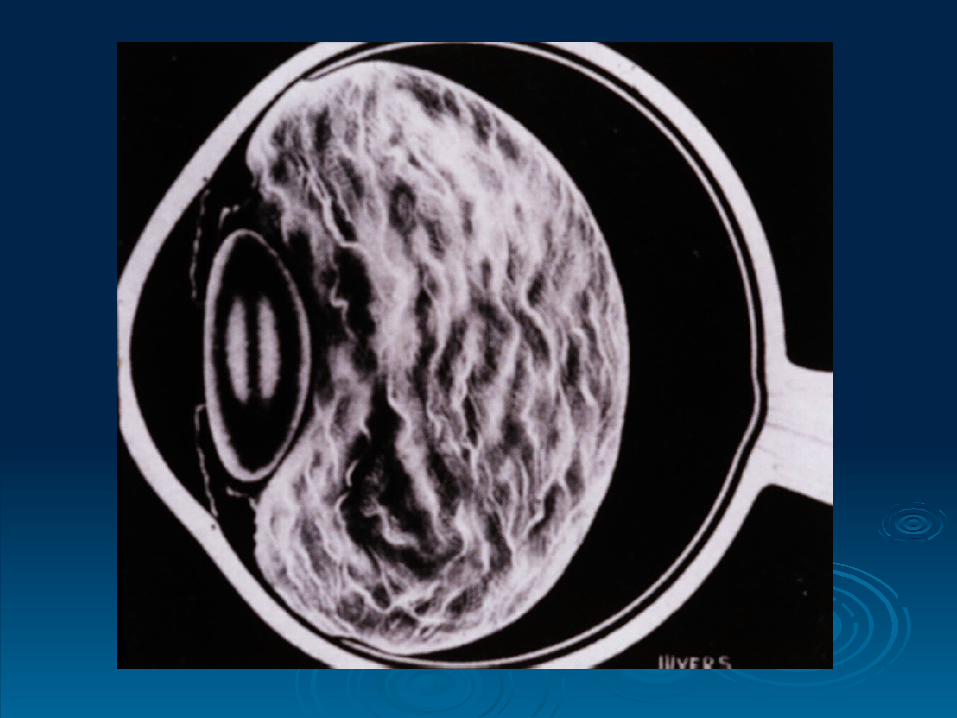
RD:RD:
Rhegmatogenous – Greek thegma = rentRhegmatogenous – Greek thegma = rent
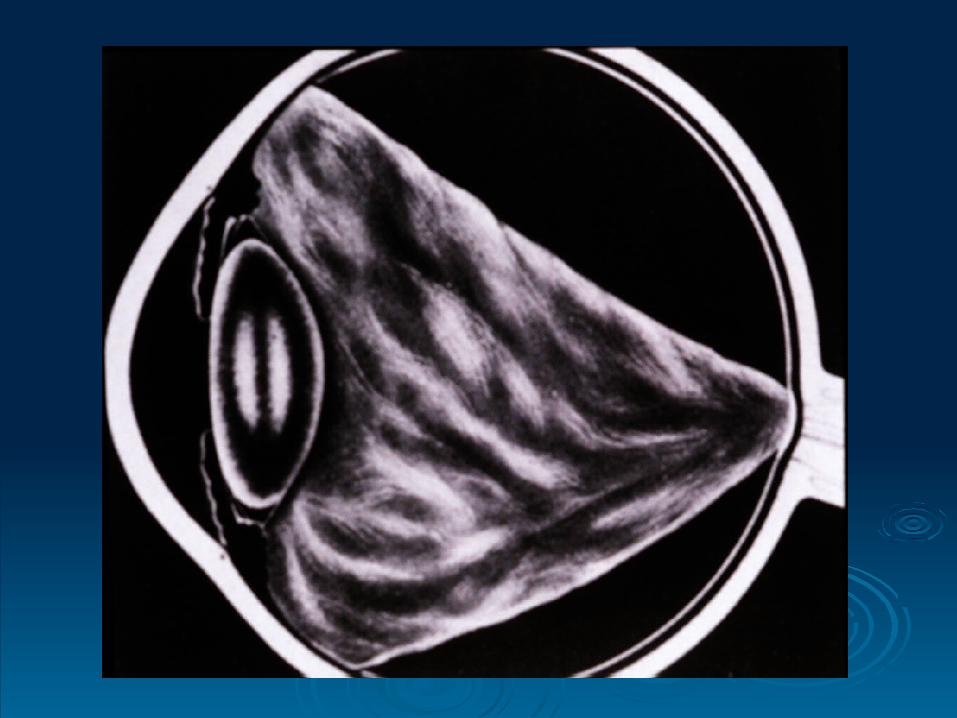
Tractional Tractional
Exudative Exudative
RD Epidemiology: RD Epidemiology:
o Incidence 1: 10,000 / year. Incidence 1: 10,000 / year. o In aphakics: 1– 3%. In aphakics: 1– 3%. o In the second eye (-): 5%. In the second eye (-): 5%. o In the second eye (+): 10%. In the second eye (+): 10%. o 99% of untreated symptomatic RD 99% of untreated symptomatic RD blindness. blindness. o 5 – 15% of population with retinal break(s) 5 – 15% of population with retinal break(s) 7% 7%
of these develop new break(s). of these develop new break(s).
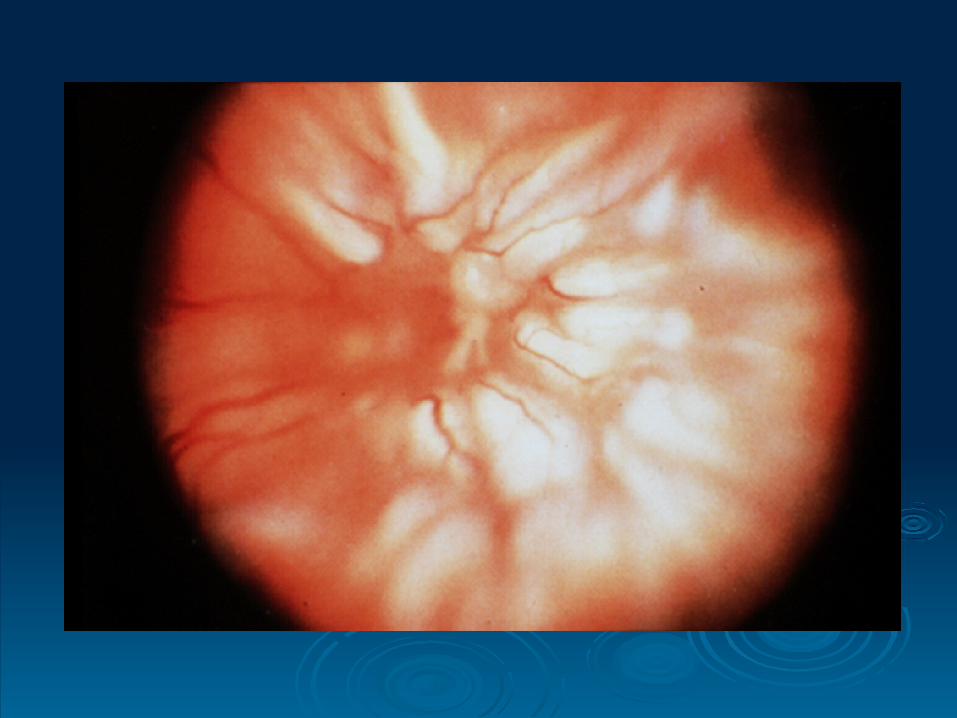
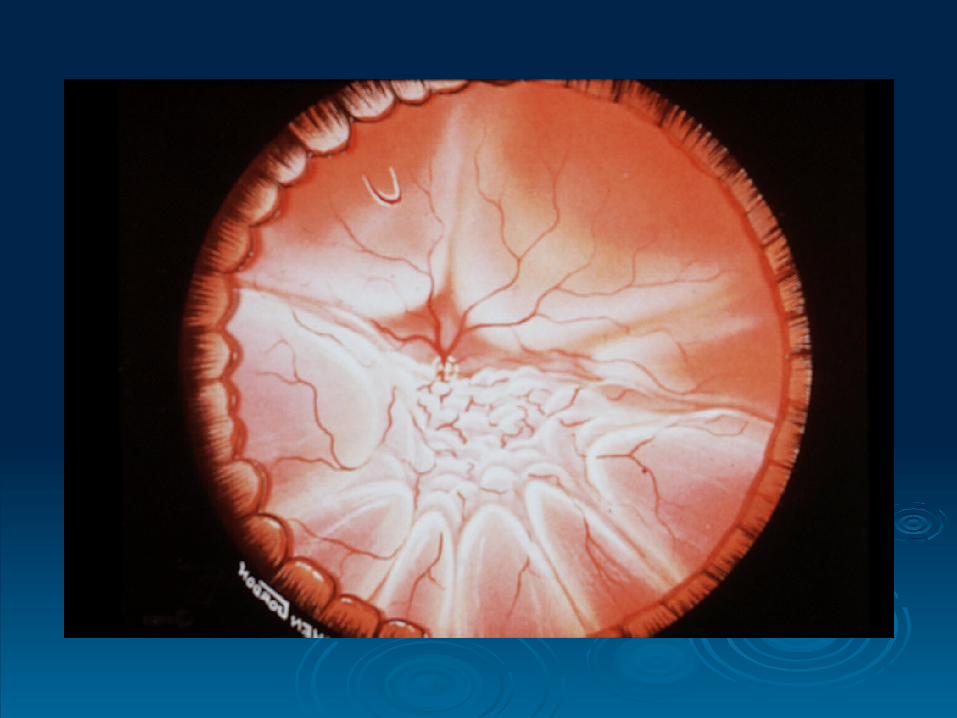
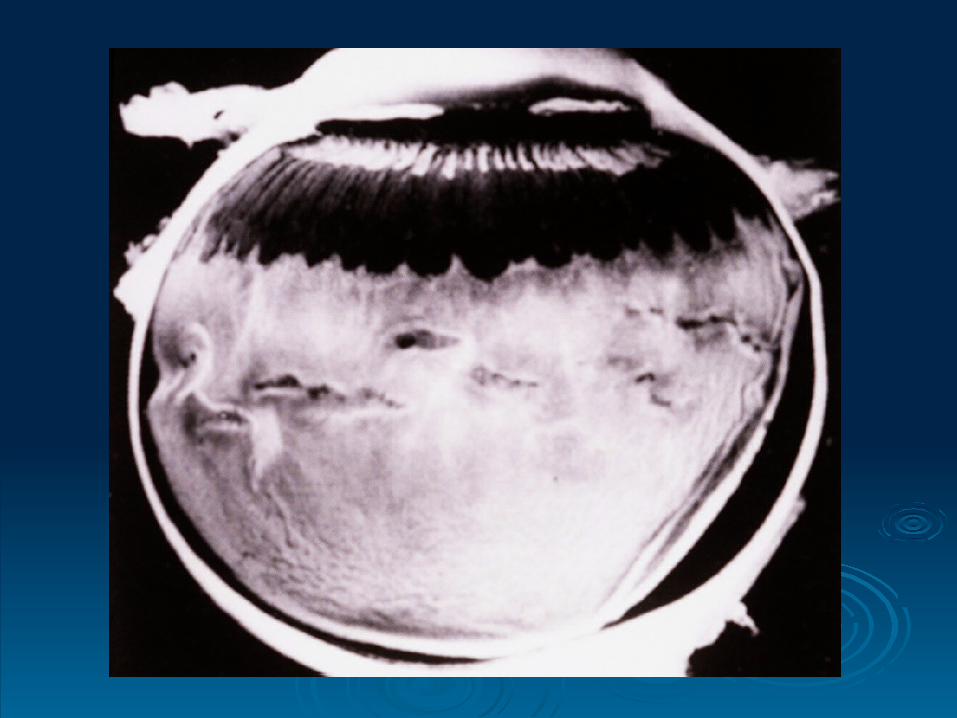
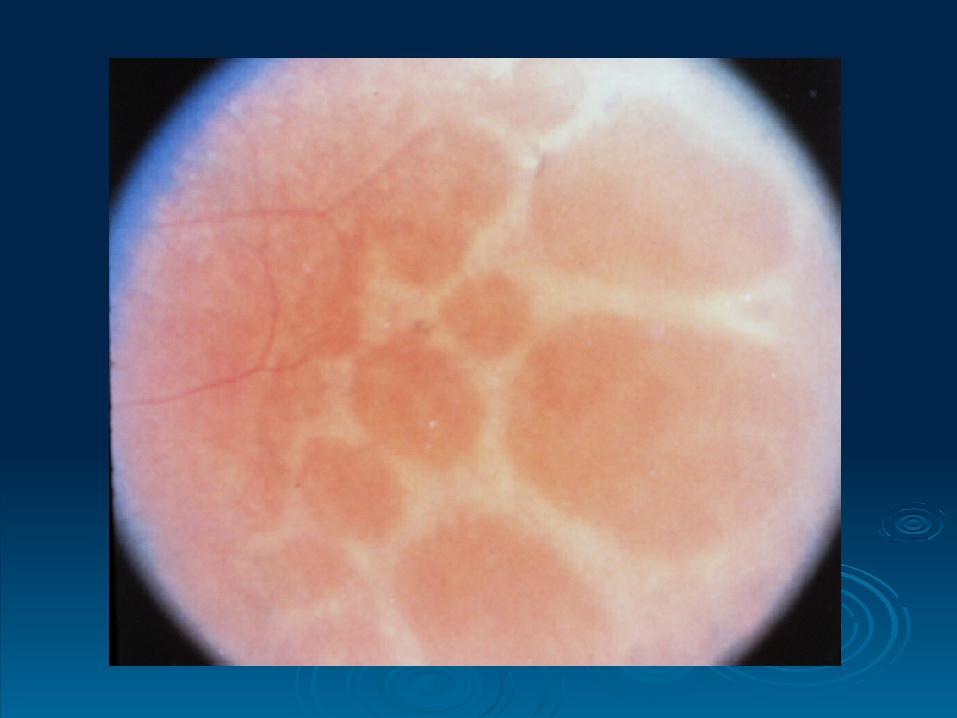
Rhegma. RD: Rhegma. RD:
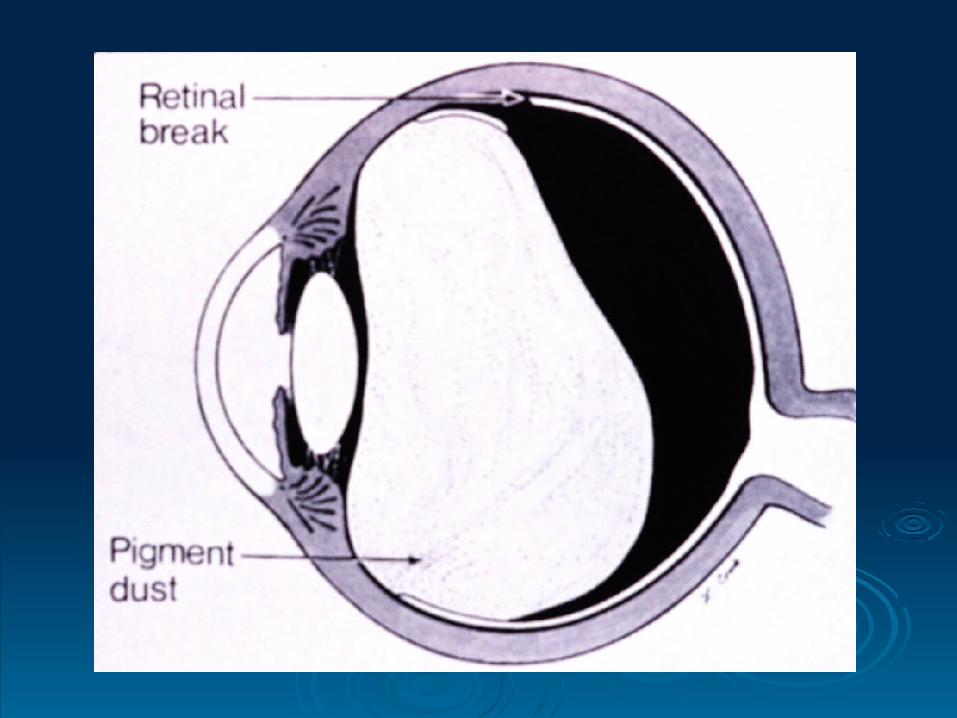
Some degree of vitreous liquifaction. Some degree of vitreous liquifaction. Retinal break: - tear Retinal break: - tear - hole - hole - dialysis - dialysis Eye movements (Edie’s currents) Eye movements (Edie’s currents) PVD, V-R traction PVD, V-R traction
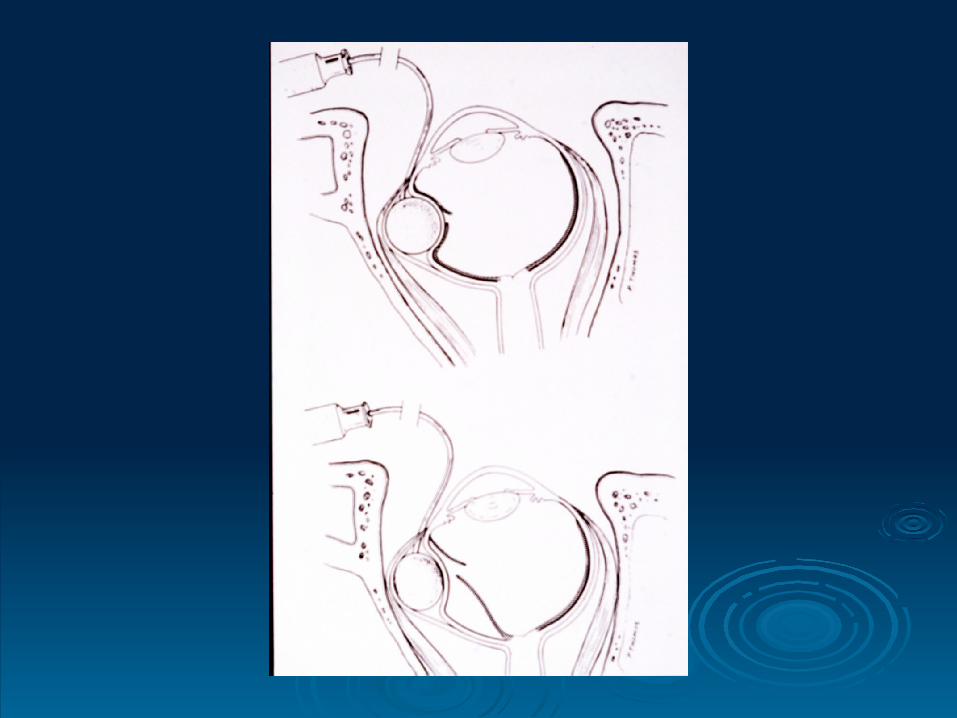
Pre-requisite:-Pre-requisite:-
PVDPVD______________________________________________________________
Due to loss of hyaluronic acid Due to loss of hyaluronic acid collapse of vit. collapse of vit. collagen with liquefaction. collagen with liquefaction.
Rare before 30 yrs. Rare before 30 yrs. Increases with age (63% in > 70 yrs.) Increases with age (63% in > 70 yrs.) Most PVDs are asymptomatic. 2Most PVDs are asymptomatic. 2ndnd eye in 1 yr. eye in 1 yr. 15% of acute PVD have a retinal tear (pathologic).15% of acute PVD have a retinal tear (pathologic). Increases significantly after cataract extraction: Increases significantly after cataract extraction:
pathologic vs. physiologic PVD. pathologic vs. physiologic PVD.
RD RD
13-19% of PVD have vit. Hem. 13-19% of PVD have vit. Hem.
PVD + hem. PVD + hem. 70% with tears. 70% with tears.
PVD + no hem. PVD + no hem. 2-4% with tears. 2-4% with tears.
PVDPVD
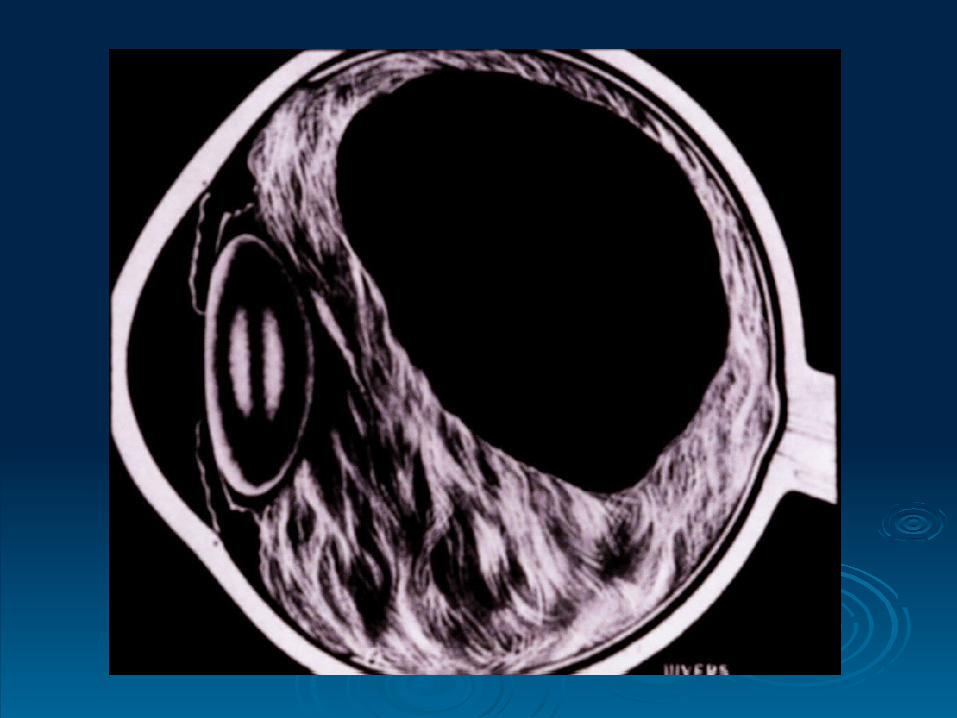
RD F/U: RD F/U:
Examine periphery. Examine periphery.
+ vit. Hem. + vit. Hem.
- rest, patching - rest, patching examine. examine.
U/S. U/S.
Acute PVD:-Acute PVD:-
RD Risk Factors: RD Risk Factors:
Present in 8% of the population. Present in 8% of the population. In SA – 9.1% In SA – 9.1%
As a cause of RD in 20-30%. As a cause of RD in 20-30%. In RDs with L.D.:- In RDs with L.D.:-
30-45% 30-45% Atrophic holes. Atrophic holes.
55-70% 55-70% A tear at edge of L.D. A tear at edge of L.D.
1.1. Lattice and other peripheral deg.:Lattice and other peripheral deg.:
RD Risk Factors: cont.RD Risk Factors: cont.
> 6 D. > 6 D.
60 yr. myope risk of RD is 2.4% whereas 60 yr. myope risk of RD is 2.4% whereas
normal risk 0.06%normal risk 0.06%
2.2. High myopia:High myopia:
RD Risk Factors: cont.RD Risk Factors: cont.
Increases PVD: Does it convert physiological PVD Increases PVD: Does it convert physiological PVD to a pathological one?to a pathological one?
1.3% RD in aphakes. 1.3% RD in aphakes. ICCE > ECCE. ICCE > ECCE. Risk of RD increased with:- Risk of RD increased with:- - P.C. otomy: 1.3%. - P.C. otomy: 1.3%. - Vit. loss. - Vit. loss. 50% of RDs in 150% of RDs in 1stst year. year.
3.3. Cataract surgery:Cataract surgery:
RD Risk Factors: cont.RD Risk Factors: cont.
In general population – 1% COAG. In general population – 1% COAG. In RD patients – 4-7% COAG. In RD patients – 4-7% COAG. > in pigment dispersion synd. > in pigment dispersion synd.
? myopia. ? myopia. Miotics & RD. Miotics & RD.
4.4. Glaucoma:Glaucoma:
RD Risk Factors: cont.RD Risk Factors: cont.
5.5. RD in fellow eye or F/H of RD. RD in fellow eye or F/H of RD.
6.6. Trauma. Trauma.
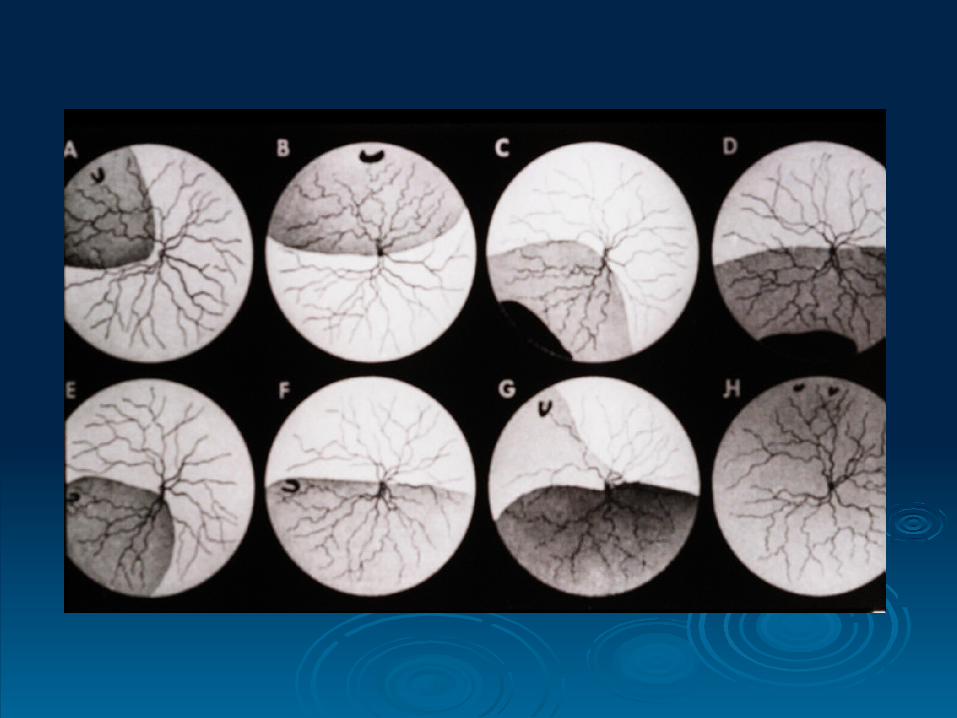
RD Symptoms:RD Symptoms:
PVD – flaches & floaters. PVD – flaches & floaters.
Painless loss of peripheral VF. Painless loss of peripheral VF.
Painless loss of central vision. Painless loss of central vision.
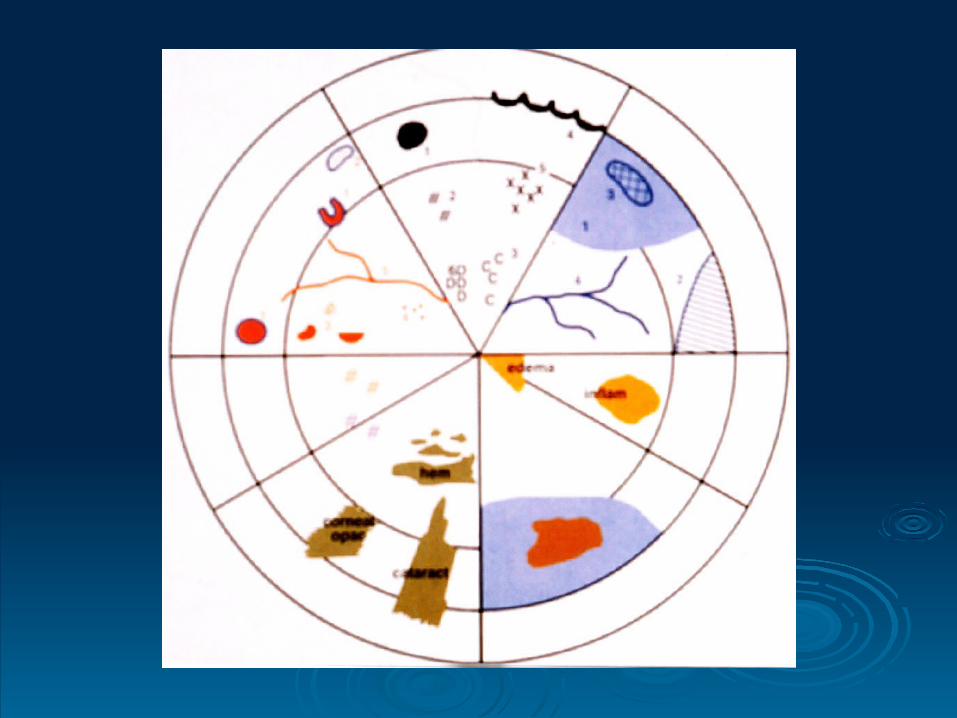
RD Examination:RD Examination:
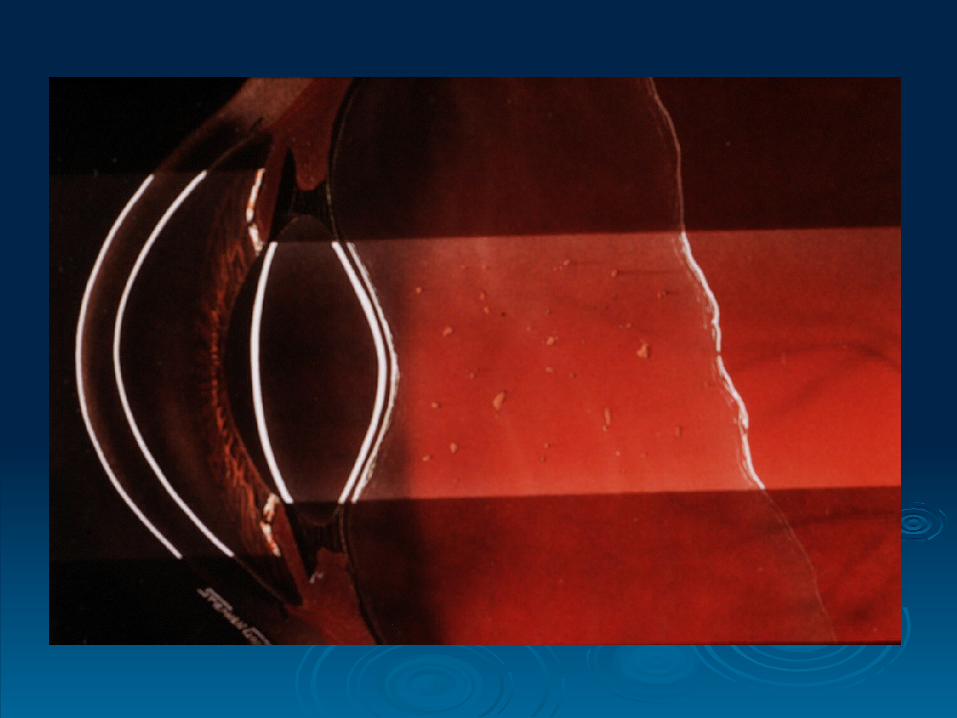
VA. VA. IOP. IOP. SLE – blood, pigment (Shafer’s sign) in the SLE – blood, pigment (Shafer’s sign) in the
vitreous. vitreous. Careful binocular indirect ophthalmoscopy Careful binocular indirect ophthalmoscopy
with scleral indentation. with scleral indentation. C.L. exam. C.L. exam.
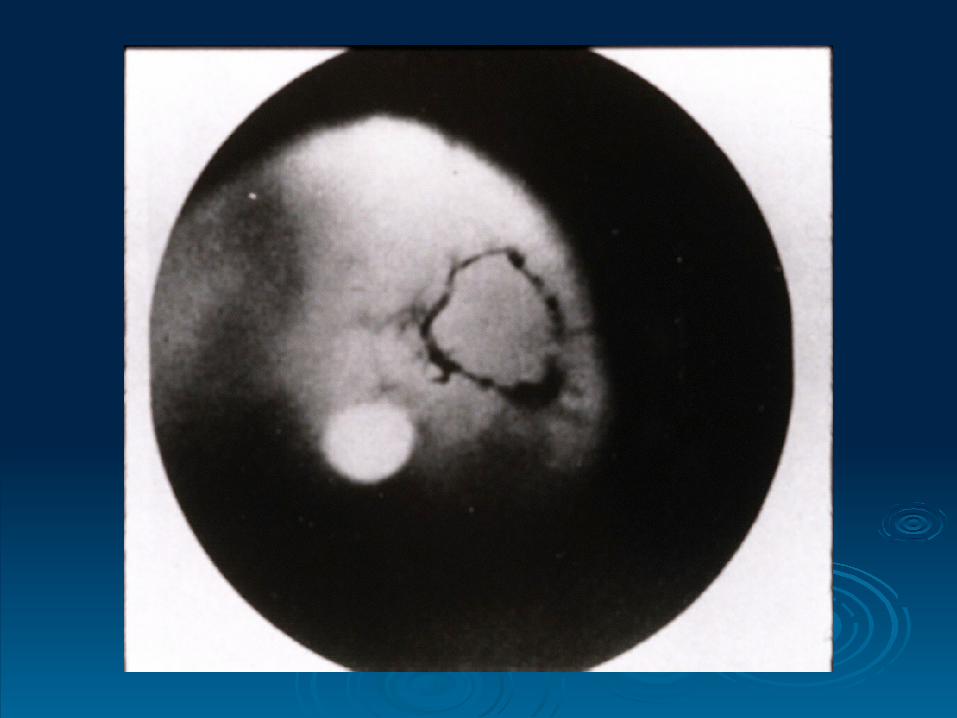
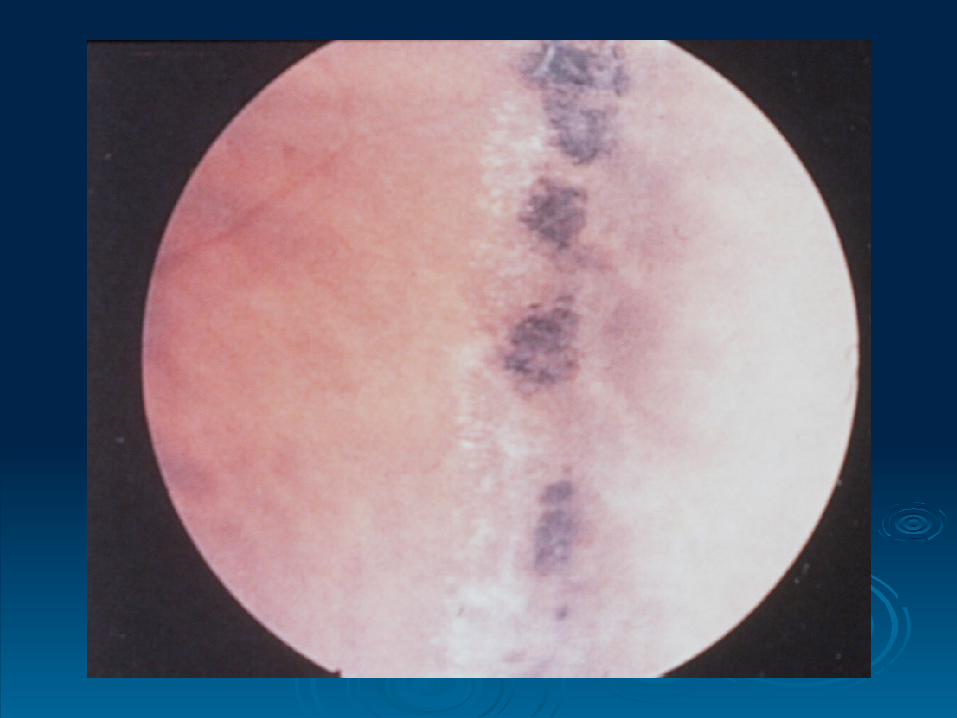
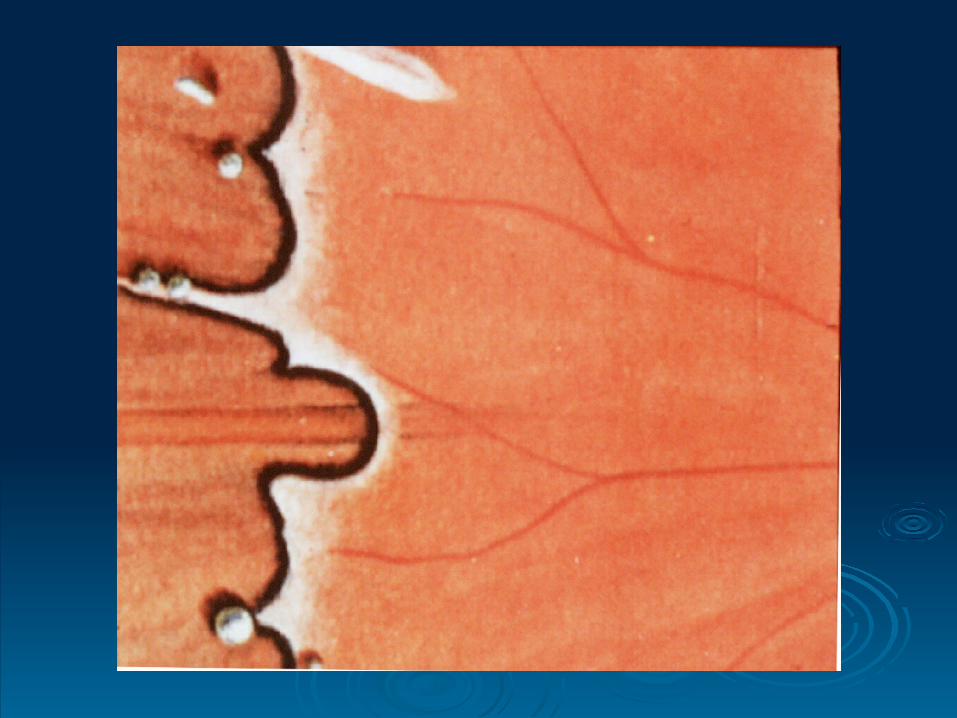
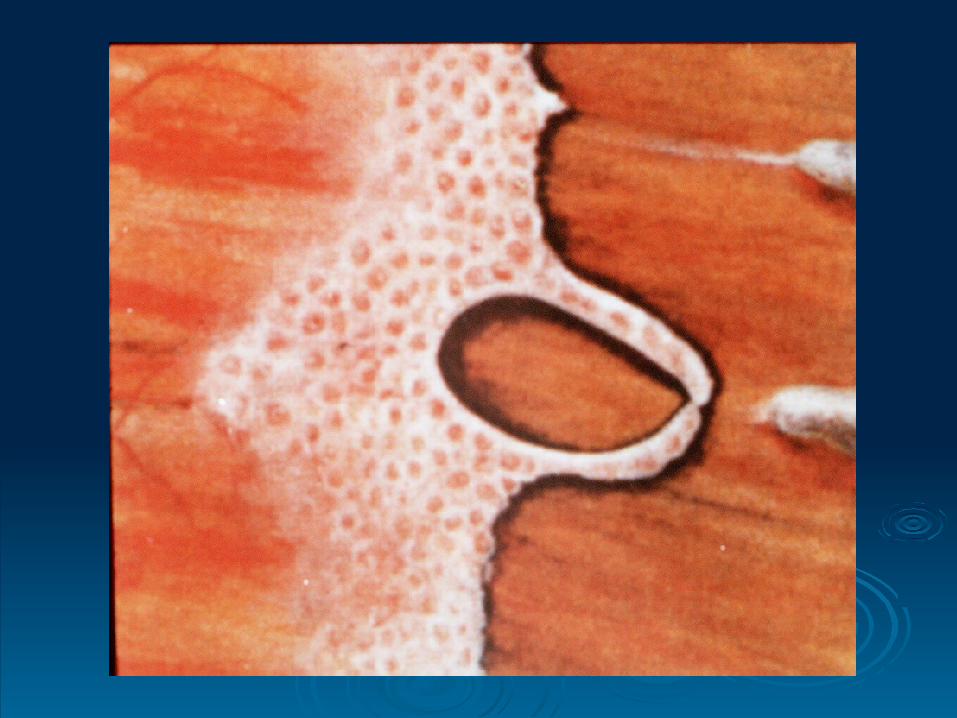
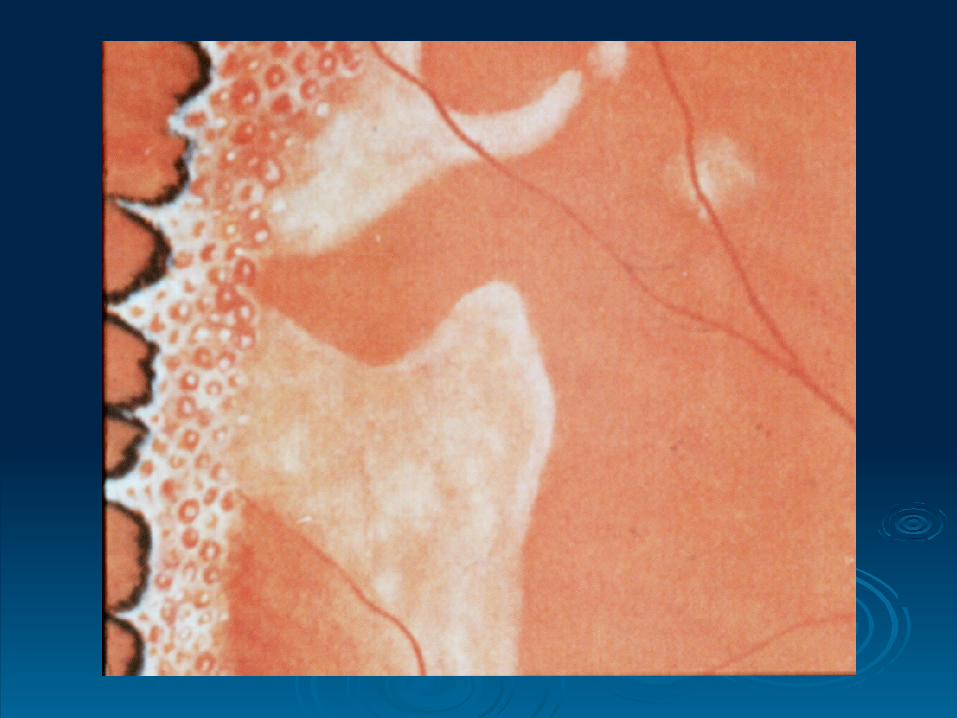
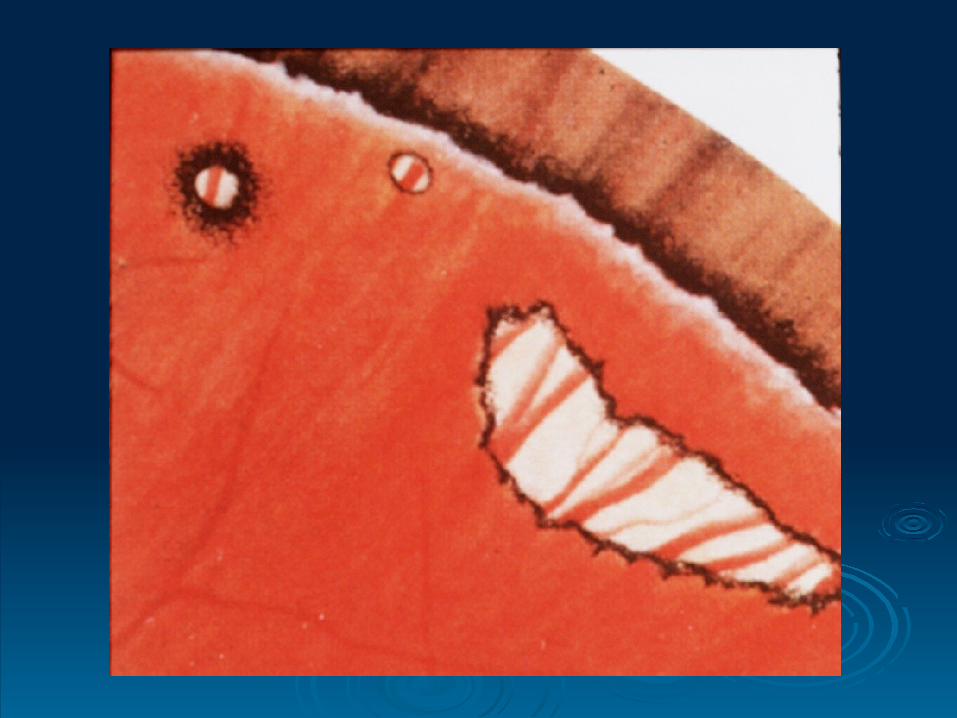
RD Types of Breaks:RD Types of Breaks:
Fresh (acute) tear either:- Fresh (acute) tear either:-
Symptomatic tear. Symptomatic tear.
Tear with retinal hem. at the edge. Tear with retinal hem. at the edge.
A new tear in that location. A new tear in that location. Flap (horseshoe) tear. Flap (horseshoe) tear. An operculated hole. An operculated hole. Atrophic holes. Atrophic holes.

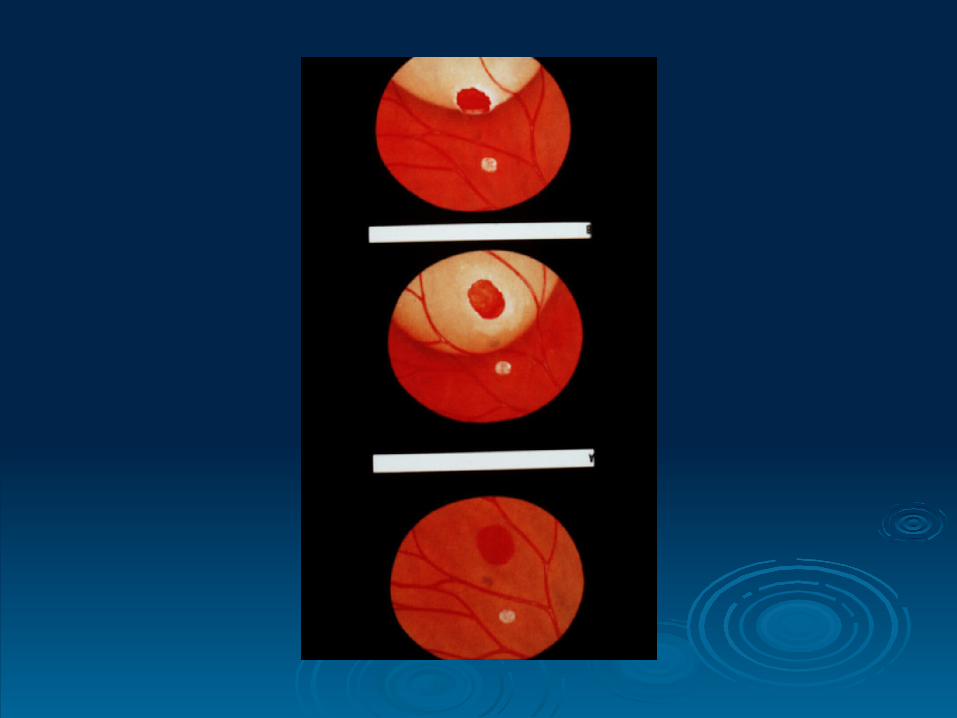
RD DDX: RD DDX:
Neoplasms. Neoplasms. Inflammations – VKH, ICSC, post. Scleritis. Inflammations – VKH, ICSC, post. Scleritis. Cong. Anomalies – optic pit, morning glory, Cong. Anomalies – optic pit, morning glory,
choroidal coloboma, nanophthalmos, uveal choroidal coloboma, nanophthalmos, uveal effusion syndrome effusion syndrome
Exudative RD:-Exudative RD:-
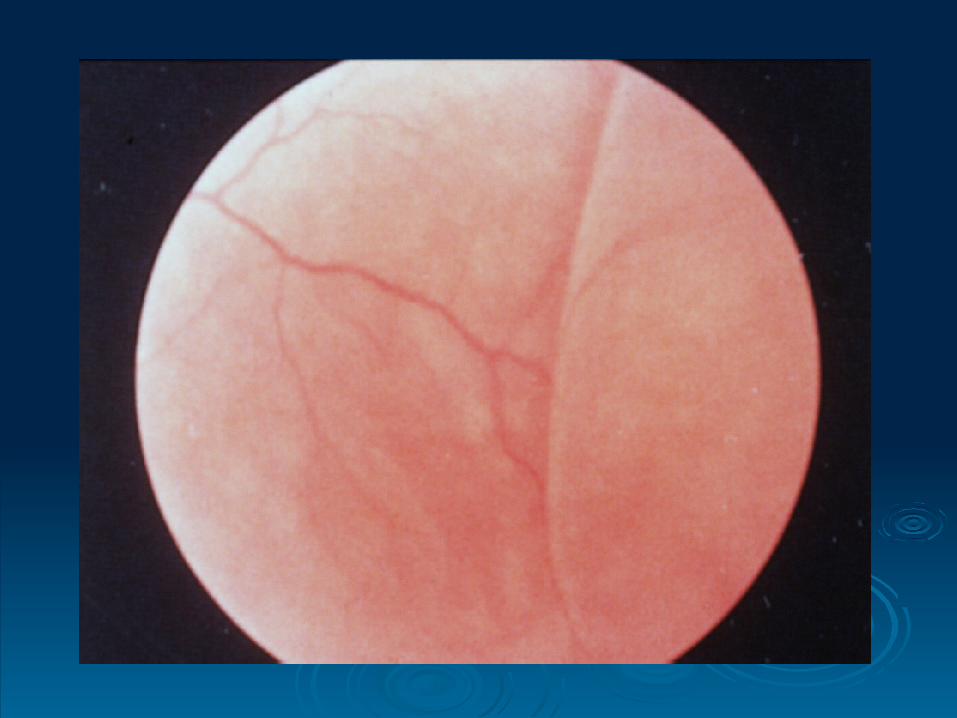
RD DDX: cont.RD DDX: cont.
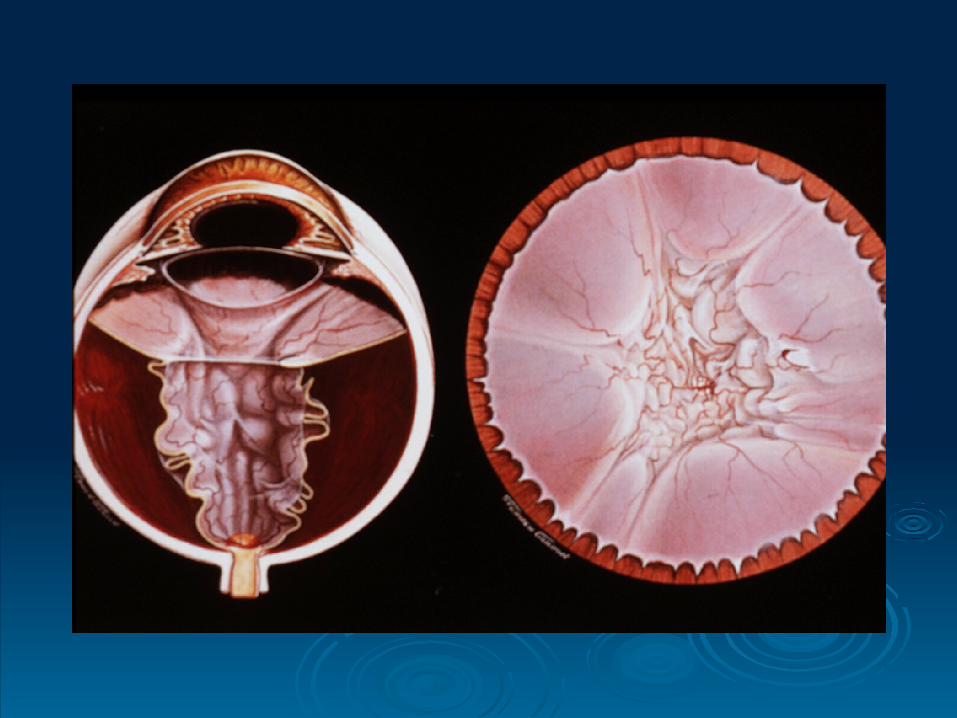
Traction RD. Traction RD.
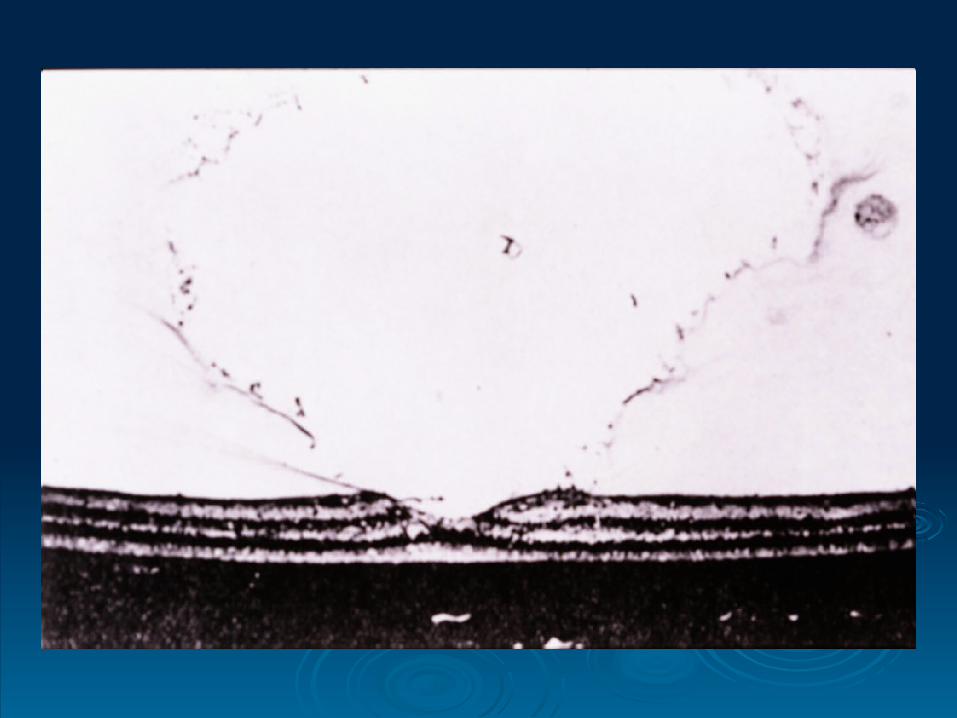
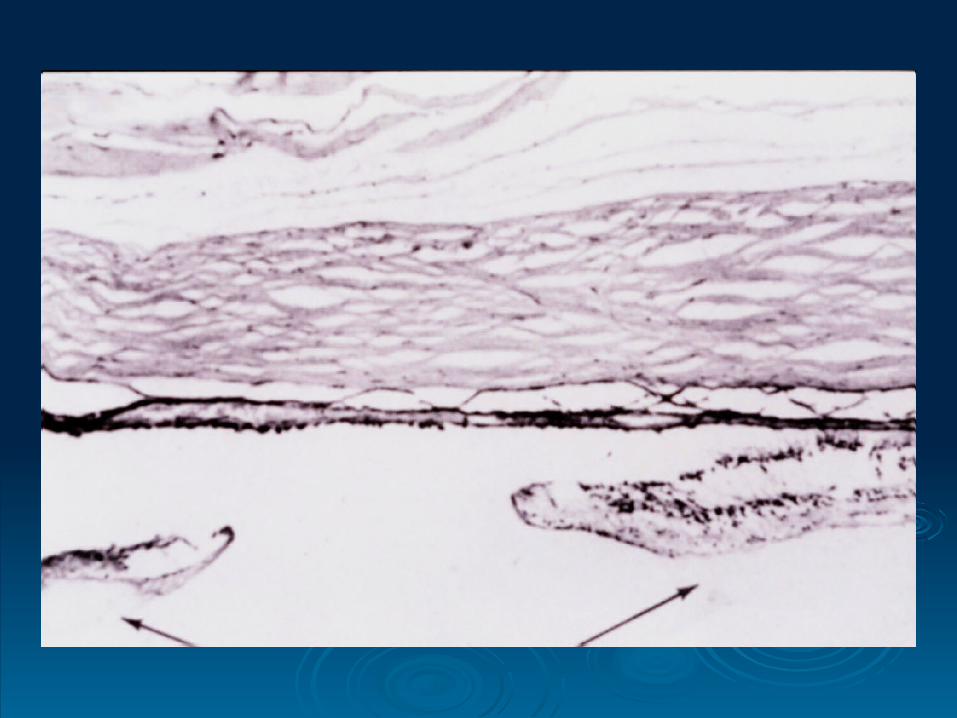
Retinoschisis – senile, juvenile. Retinoschisis – senile, juvenile.
Choroidal detachment. Choroidal detachment.
RD Treatment: RD Treatment:
Olny selected breaks require Rx. Olny selected breaks require Rx.
A symptomatic tear – caused by PVD or vit. A symptomatic tear – caused by PVD or vit.
Traction in the eye of a pt. C/O photopsias Traction in the eye of a pt. C/O photopsias
+/- floaters. +/- floaters.
Prophylactic Rx:-Prophylactic Rx:-
Indications for Prophylactic Treatment Indications for Prophylactic Treatment of Retinal Tears and Holes in of Retinal Tears and Holes in
Symptomatic Patients: Symptomatic Patients:
Flap tears Flap tears Frequently (always) Frequently (always)
Operculated holes Operculated holes Sometimes Sometimes
Atrophic holes Atrophic holes No No
Macular holes Macular holes Rarely Rarely
Lesion Lesion Treatment Treatment __________________________________________________________________________

RD Treatment: RD Treatment:
Cryotherapy. Cryotherapy. Photocoagulation. Photocoagulation. Surround it ant. & post. Surround it ant. & post. Macular pucker. Macular pucker. Tears at margins of Rx scar. Tears at margins of Rx scar.
Prophylactic Rx to breaks:-Prophylactic Rx to breaks:-
RD Treatment: cont.RD Treatment: cont.
Emergency. Emergency. Localization of break(s). Localization of break(s). Creation of C-R adhestion around the Creation of C-R adhestion around the
break(s). break(s). Closure of break(s). Closure of break(s). Relief of V-R traction. Relief of V-R traction.
Principles of Surgery:-Principles of Surgery:-
RD Treatment: cont.RD Treatment: cont.
Scleral buckle. Scleral buckle. Orbital balloon. Orbital balloon. Pneumatic retinopexy. Pneumatic retinopexy. Primary vitrectomy + GFX, Long-term Primary vitrectomy + GFX, Long-term
tamponade. tamponade.
LA/GALA/GA
Surgical techniques:-Surgical techniques:-

RD prognosis & VA: RD prognosis & VA:
90-95% - Anatomic success. 90-95% - Anatomic success.
Overall 40-50% Overall 40-50% 20/50 or > 20/50 or >
25% 25% 20/60 – 20/100 20/60 – 20/100
25% 25% 20/200 or < 20/200 or <
RD prognosis & VA: cont.RD prognosis & VA: cont.
If macula off < 1 wk – 75% If macula off < 1 wk – 75% 20/70 or >. 20/70 or >.
If macula off 1-8 wk – 50% If macula off 1-8 wk – 50% 20/70 pr >. 20/70 pr >.
If macula on 90% If macula on 90% Preop. VA Preop. VA pucker, pucker,
CME, recurrent RD. CME, recurrent RD.
RD Prognosis: RD Prognosis:
Detachments due to dialysis or to small or Detachments due to dialysis or to small or round holes. round holes.
Detachments with demarcation lines. Detachments with demarcation lines. Detachments with minimal subretinal fluid. Detachments with minimal subretinal fluid.
1.1. Excellent prognosis (nearly 100%):Excellent prognosis (nearly 100%):
RD Prognosis: cont.RD Prognosis: cont.
Aphakic detachments. Aphakic detachments. Total detachments. Total detachments. Detachments with associated detachment of Detachments with associated detachment of
the nonpigmented epithelium of the pars the nonpigmented epithelium of the pars plana. plana.
Detachments caused by flap tears. Detachments caused by flap tears.
2.2. Slightly poorer prognosis (95%):Slightly poorer prognosis (95%):
RD Prognosis: cont.RD Prognosis: cont.
Detachments with associated choroidal Detachments with associated choroidal detachment detachment
Detachments with breaks larger than 180Detachments with breaks larger than 180. .
Detachments with PVR. Detachments with PVR. Detachments in patients with stickler’s Detachments in patients with stickler’s
syndrome. syndrome. Detachments caused by acute retinal Detachments caused by acute retinal
necrosis. necrosis.
3.3. Poor prognosis (50 to 70%):Poor prognosis (50 to 70%):