Embed Size (px)
Citation preview

Clinical and Experimental Ophthalmology
2003;
31
: 96–102
Original Article
_____________________________________
Original Article
Retinal detachment in cytomegalovirus retinitis: intravenous versus intravitreal therapy
Stephanie Young
FRANZCO
,
1,2
Peter McCluskey
FRANZCO
,
3,4
Darwin C Minassian
FRCOphth
,
5
Paul Joblin
MB ChB
,
3
Colin Jones
FRCOphth
,
1,2
Minas T Coroneo
FRANZCO
6
and Susan Lightman
FRCOphth
1,2
Departments of
1
Clinical Ophthalmology and
5
Epidemiology and International Eye Health, Institute of Ophthalmology,
2
Department of Ophthalmology, Moorfields Eye Hospital, London, UK,
3
Department of Ophthalmology, Royal Prince Alfred Hospital,
4
Department of Ophthalmology, St Vincent’s Hospital and
6
The Eye Clinic, Prince of Wales Hospital, Sydney, Australia
A
BSTRACT
Purpose:
To compare the rate of retinal detachment in agroup of patients treated with intravitreal ganciclovir to therate of retinal detachment in a group of patients treatedwith systemic ganciclovir.
Methods:
A retrospective non-randomized comparativecase series was conducted. The participants were 186consecutive patients with cytomegalovirus (CMV) retinitistreated at two centres over the period from June 1990 toMay 1997. Of the 186, 133 patients had systemic therapyof whom 113 had intravenous ganciclovir or foscarnet and20 had oral ganciclovir, and 53 patients had intravitrealinduction and maintenance therapy. The main outcomemeasure was the rate of retinal detachment, which wascalculated using person-months-at-risk denominators. Theeffect measure used in the main comparative analysis wasthe hazard ratio obtained from multiple regression usingthe Cox proportional hazards model.
Results:
Retinal detachment occurred in three of 53patients in the intravitreal therapy group, one of 20 patientsreceiving oral maintenance therapy and 21 of 113 patientsreceiving intravenous maintenance therapy. The risk ofretinal detachment with systemic therapy was 14-foldhigher than with intravitreal therapy (
P
< 0.001) and up tofourfold higher with oral maintenance therapy.
Conclusions:
Intravitreal therapy offers a significant advan-tage over systemic therapy in the treatment of CMVretinitis by substantially reducing the risk of CMV-relatedretinal detachment.
Keywords:
cytomegalovirus retinitis, intravitreal ganciclovir,retinal detachment, systemic ganciclovir.
I
NTRODUCTION
Cytomegalovirus (CMV) retinitis is the most frequent visionthreatening complication of AIDS affecting up to 40% ofpatients.
1–6
The management and prevention of complica-tions of active and quiescent CMV retinitis remains animportant goal in patient care. Although CMV retinitis canusually be controlled, retinal detachment affects the courseof 10–29% of patients on maintenance intravenoustherapy
7–9
with a cumulative probability of retinal detach-ment in at least one eye of up to 50% at 1 year.
7
Intravitrealtherapy may offer an advantage in this respect with retinaldetachment reported in 8–14% of patients receiving intra-vitreal ganciclovir injections
10–13
and 11–23% of patientsreceiving ganciclovir implants.
14–17
The advent of highly active antiretroviral therapy(HAART) has increased the survival of patients with AIDSand has greatly reduced the incidence of opportunisticinfections, including CMV retinitis. However, with anexpanding cohort of HIV-positive patients and longerpatient survival times, resistance to HAART may result in ahigher incidence of CMV retinitis than at present. Addition-ally, CMV retinitis remains a significant cause of ocularmorbidity in patients who are immunosuppressed for otherreasons.
18
The present study determined the incidence of retinaldetachment in patients with CMV retinitis receiving sys-temic or intravitreal therapy in order to identify whetherthere was any difference in the rate of retinal detachmentbetween the treatment groups.
M
ETHODS
Patients
A retrospective review was undertaken of the medicalrecords of consecutive patients with AIDS and CMV retinitisattending two centres over the period from June 1990 to
�
Correspondence:
Dr Peter McCluskey, 357 Beamish Street, Campsie, NSW 2194, Australia. Email: [email protected]

CMV-related retinal detachment 97
May 1997. The authors had managed the CMV retinitis ofthe patients attending these centres over this period.Patients had been treated throughout with intravenousganciclovir or foscarnet or oral ganciclovir as maintenancetherapy or with intravitreal injections of ganciclovir and/orfoscarnet.
Cytomegalovirus retinitis was diagnosed clinically byophthalmologists experienced in the diagnosis of CMVretinitis and treated within 2 weeks of diagnosis regardlessof position or extent. Patients treated with intravitrealtherapy were seen at weekly intervals while those managedon systemic treatment were seen 2–4 weekly.
The CMV retinitis was classified according to the loca-tion and size of the retinitis. The location of retinitis wasdivided into three retinal zones using the SOCA classifica-tion.
19
The area of the retina involved was arbitrarily definedas: area 1 < 25% and area 2
≥
25% of retinal involvement byCMV retinitis. Presence of retinal detachment, position andassociated holes or tears was noted. When patients pre-sented with bilateral CMV retinitis the eye with the largerarea of retinitis was followed. In cases where contralateralCMV retinitis occurred after presentation, the first eyediagnosed was followed to assess the risk of retinal detach-ment. Retinal photography was not routinely used in thediagnosis and management of patients.
Relapse of CMV retinitis was diagnosed clinically by thepresence of new lesions of 0.25 disc area or more in size orextension of previously inactive areas by 750
µ
m in thepresence of opaque borders.
Intravenous therapy
Patients treated intravenously received ganciclovir or foscar-net using a biphasic treatment regimen. Initial higher doseinduction dose of ganciclovir 5 mg/kg twice daily for14–21 days, was followed by lifelong maintenance therapyof 5 mg/kg daily ganciclovir for 3–7 days per week. Patientswere given the maximum tolerated intravenous maintenancedoses. Ganciclovir therapy was reduced or interrupted if theneutrophil count fell below 700 cells/mL and granulocytecolony stimulating factor (GCSF) was used as needed tomaintain the neutrophil count. Once available, some patientswere given oral ganciclovir maintenance therapy followinginitial intravenous ganciclovir induction therapy, using adose of 3 g daily in three divided doses instead of intravenoustherapy. Patients were not swapped between intravenousand oral ganciclovir maintenance regimens.
Intravenous foscarnet was given using a similar biphasicinduction therapy of 180 mg/kg per day in 2–3 doses for14–21 days, followed by lifelong maintenance therapy of120 mg/kg per day in two doses 3–7 days weekly withadjustments for impaired renal function. Patients were givenintravenous hydration therapy prior to their foscarnet doses.
Relapse was managed in the first instance by re-inductionof the initial agent when appropriate or substitution with thealternative drug.
Intravitreal therapy
Intravitreal ganciclovir therapy was delivered on an out-patient basis using a standardized technique.
20
The dose ofganciclovir used was 2 mg/0.1 mL and that of foscarnet was2.4 mg/0.05 mL. Induction treatment consisted of twiceweekly injections for 3 weeks followed by weekly mainte-nance injections. Relapse was treated with twice weeklyinjections until resolution (2–3 weeks) and the usual mainte-nance regimen resumed. Once available a small number ofpatients were treated with oral ganciclovir as prophylaxis forsecond eye involvement.
Outcome measure
The primary outcome was occurrence of retinal detachmentand this outcome was measured by the rate of retinaldetachment using person-months-at-risk denominators. Theeffect measure used in the main comparative analysis wasthe hazard ratio (the event being retinal detachment)obtained from multiple regression using the Cox propor-tional hazards model.
The three comparison groups were defined as follows:
●
Treatment group A: Intravitreal therapy (
n
= 53)
●
Treatment group B: Systemic therapy with oral ganci-clovir (
n
= 20)
●
Treatment group C: Systemic therapy with intravenousganciclovir or foscarnet (
n
= 113).The following classifications of prognostic factors were
used in the analysis: age group (20–39 years, 40–59 years);area of retinal involvement (<25%,
≥
25%); zone of retinainvolved (zone 1 only, zone 2 only, zone 3 only, mixedzones); study centre; and bilaterality of the CMV retinitis atbaseline (unilateral, bilateral). Gender and intravenous druguse were also considered as possible prognostic factors.However, there were only three women and only eightintravenous drug users in the study cohort.
Statistical analysis
Cox proportional hazards regressions were used to comparethe retinal detachment rates in the three treatment groups,with adjustment for effects of other prognostic factors. Thiswas performed after a simple comparison of incidence ratesin the three treatment groups using rate ratios and ‘exact’procedures to compute confidence limits and
P
values.Other initial analysis prior to the multiple regressionincluded cross-tabulations to assess the relationshipsbetween the prognostic factors and to identify any extremecorrelation that might cause problems of extreme colinear-ity in the regression models. As there were too few womento allow inclusion of gender in the multiple regressionanalysis, the analysis was performed with and without inclu-sion of the three women. The same approach was adoptedfor the eight intravenous drug users. Analysis was also per-formed with treatment groups B and C combined.

98 Young
et al.
R
ESULTS
The medical records of 189 patients with CMV retinitis andHIV infection were identified. Three patients had presentedwith retinal detachment and were excluded. Therefore, 186patients were included in the study. The baseline character-istics of the three comparison treatment groups are shownin Table 1. The follow up (i.e. months at risk) is shown inTable 2. The median follow-up period for the study cohortwas 5.1 months.
The three main comparison groups comprised 53patients in treatment group A (intravitreal therapy); 20 ingroup B (systemic therapy with oral ganciclovir), and 113 ingroup C (systemic therapy with intravenous ganciclovir orfoscarnet). Initial maintenance treatment was intravenousganciclovir in 85 patients, oral ganciclovir in 20 patients andintravenous foscarnet in 28 patients. Therapy was changedfrom ganciclovir to foscarnet or vice versa in 40 patients.Three patients were given combination therapy with bothagents. Intravitreal induction and maintenance therapy wasused in 53 patients. In this group, eight patients had addi-tional systemic treatment: five had oral ganciclovir asprophylaxis when it became available and three patients hada single course of intravenous ganciclovir induction treat-ment when they developed gastrointestinal CMV disease.The median CD4 count at diagnosis for both groups was0.01
×
10
9
/L. Information regarding HIV viral loads was notavailable.
Detailed information regarding the dose and duration ofantiretroviral therapy was not available. Most patients weretreated with one or two nucleotide analogues. The studylargely predated the availability of highly active antiretro-viral therapy (HAART) and only a small number of patients(<10 patients) took such treatment for short periods of time(<12 weeks) towards the end of the study.
Table 1.
Baseline characteristics of the three comparison treatment groups: group A, intravitreal induction therapy (
n
= 53); group B,systemic therapy with oral ganciclovir (
n
= 20); and group C, systemic therapy with intravenous ganciclovir or foscarnet (
n
= 113)
Characteristic Group ANo. patients (%)
Group BNo. patients (%)
Group CNo. patients (%)
P
value
Study centreCentre 1 10 (18.9) 18 (90.0) 98 (86.7) <0.001Centre 2 43 (81.1) 2 (10.0) 15 (13.3)
Age group*20–39 years 39 (73.6) 10 (50.0) 72 (63.7) 0.1640–59 years 14 (26.4) 10 (50.0) 41 (36.3)
Male sex 52 (98.1) 19 (95.0) 112 (99.1) 0.20Area involved
<25% 37 (69.8) 17 (85.0) 72 (63.7) 0.15
≥
25% 16 (30.2) 3 (15.0) 41 (36.3)Zone involved
Zone 1 only 17 (32.1) 3 (15.0) 12 (10.6) 0.001Zone 2 only 17 (32.1) 5 (25.0) 21 (18.6)Zone 3 only 9 (17.0) 2 (10.0) 29 (25.7)Mixed zones 10 (18.9) 10 (50.0) 51 (45.1)
Bilateral disease 22 (41.5) 5 (25.0) 41 (36.3) 0.50Intravenous drug user 4 (7.6) 1 (5.0) 3 (2.7) 0.20Visual acuity
6/6–6/12 43 (81.1) 19 (95.0) 97 (85.8) 0.806/18–6/30 6 (11.3) 1 (5.0) 10 (8.9)
≥
6/60 4 (7.6) 0 6 (5.3)
*Mean
±
SD ages for the three treatment groups were: group A 35.7
±
7.2 (range 24–54) years; group B 39.9
±
6.9 (range 28–54) years;and group C 37.7
±
7.7 (range 23–59) years.
Table 2.
Follow up (months at risk) for the study cohort
Treatment group
n
Months at risk* Mean (range)
Group A 53 6.9 (1.8–15.7)Group B 20 9.2 (0.9–29.0)Group C 113 6.4 (0.5–28.6)
Group A, intravitreal induction therapy; group B, systemictherapy with oral ganciclovir; group C, systemic therapy withintravenous ganciclovir or foscarnet.
*Months at risk for retinal detachment cases was the months offollow up from the start of study to the time of occurrence of theretinal detachment. For the non-cases, it was the months of follow-up from the start of study to last visit.

CMV-related retinal detachment 99
Retinal detachment
Retinal detachment occurred in 25 patients: three in treat-ment group A, one in treatment group B and 21 in treatmentgroup C.
The incidence rates of retinal detachment for the threetreatment groups are shown in Table 3. The retinal detach-ment incidence rate was significantly higher in group C(systemic therapy with intravenous ganciclovir or foscarnet;29 per 1000 person-months-at-risk), compared to that ingroup A (intravitreal therapy; 8 per 1000 person-months-at-risk). The rate ratio was 3.6 (
P
= 0.023).Two patients from the intravenous treatment group later
developed retinal detachment in the second eye. There wereno bilateral cases in the intravitreal group.
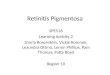
Analysis by multiple regression to adjust for effects ofother prognostic factors confirmed the superiority of intra-vitreal therapy. The adjusted rate ratios (hazard ratios) fromthe Cox proportional hazards regression model are shown inTable 4. In comparison to intravitreal therapy, the hazardratios for the two systemic therapies were substantiallygreater than 1.0 and highly significant for treatment groupC, suggesting that the risk of retinal detachment for thissystemic treatment was about 14-fold higher (hazard ratio13.8,
P
= 0.001), compared to intravitreal therapy. Thedetachment-free survival curves obtained from the Coxmultiple regression model are shown in Fig. 1. Combiningtreatment groups B and C into a single systemic treatmentgroup did not alter the findings (hazard ratio 13.8,
P
= 0.001, for systemic treatment).Other factors associated with higher risk of retinal detach-
ment were the area of retinal involvement (hazard ratio 6.6,
P
< 0.001, for area
≥
25%), and the study centre (hazardratio 4.0,
P
= 0.018, for centre 2). Within each study centre,however, intravitreal treatment was superior (retinal detach-ment rates in centre 1, 0.000 for intravitreal
vs
0.021 forother treatments; and in centre 2, 0.01
vs
0.081) (Table 5).This was manifest in the multiple regression reported inTable 4 where the differences between treatments remainedsignificant after adjustment for the ‘centre effect’. Patientswith involvement of retinal zone 1 seemed to have lower
risk of retinal detachment compared to those with zones2–3 involvement, but the effect was not significant.
Further adjustment for possible effects of bilaterality ofCMV retinitis did not materially alter the findings, nor didthe exclusion of the three women or exclusion of the eightintravenous drug users from the analysis. There was noevidence of significant effect modification (interaction) byage, study centre, area or zone of retinal involvement. Thus,the observed superiority of intravitreal therapy over sys-temic treatment was apparent in both study centres and inall other main subgroups of the study cohort.
Table 3.
Incidence rates of retinal detachment in the three comparison treatment groups, with no adjustment for effects of other prognosticfactors
Treatment group
n
No. retinal detachments Total PMAR* Incidence rate Rate ratio(95% CI)
‘Exact’
P
-value
Group A 53 3 367 0.008 (referent)Group B 20 1 184 0.005 0.66 (0.01–8.28) 0.80Group C 113 21 724 0.029 3.55 (1.06–18.58) 0.02
Group A, intravitreal induction therapy; group B, systemic therapy with oral ganciclovir; group C, systemic therapy with intravenousganciclovir or foscarnet; PMAR, person-months-at-risk.
*Months at risk for retinal detachment cases was the months of follow up from the start of study to the time of occurrence of the retinaldetachment. For the non-cases, it was the months of follow-up from the start of study to last visit.
Comparing group B with group C: Rate ratio (C/B) = 5.34, Exact
P
= 0.0521.
Table 4.
Multiple regression analysis of the effects of treatment
Variable Retinal detachment Hazard ratio
(95% CI)
P
value
Treatment GroupGroup A (referent)Group B 3.9 (0.3–52.0) 0.30Group C 13.8 (2.9–66.5) 0.001
Study centreCentre 1 (referent)Centre 2 4.0 (1.3–12.9) 0.02
Age group*20–39 years (referent)40–59 years 0.8 (0.3–2.2) 0.70
Area of retina involved<25% (referent)
≥
25% 6.6 (2.5–17.1) < 0.001Retinal zone involved
Zone 1 only (referent)Zone 2 only 3.6 (0.4–33.0) 0.26Zone 3 only 3.6 (0.4–30.6) 0.24Mixed zones 2.4 (0.3–19.4) 0.42
Group A, intravitreal induction therapy; group B, systemictherapy with oral ganciclovir; group C, systemic therapy withintravenous ganciclovir or foscarnet.
*Substituting age as a non-categorical (linear) term did not alterthe findings.

100 Young
et al.
Relapse of CMV retinitis occurred in 77 patients. It wassignificantly more common among groups B and C (45%and 57%) compared to the intravitreal group (5.7%,
P
< 0.001). Relapse was also more common in patients whodeveloped retinal detachment compared to those who didnot (68%
vs
37%,
P
= 0.005). The excess risk of retinaldetachment in group C, however, could not be explainedentirely by (was largely independent of) the frequency ofrelapse. Including relapse as a term in the multiple regres-sion model did not materially alter the hazards ratios; thehazard ratio for group C was only slightly reduced from13.8 to 13.3, and remained significant (
P
= 0.003).
D
ISCUSSION
This retrospective non-randomized comparative case seriescompared the rate of retinal detachment in 133 patients whohad systemic therapy with 53 patients who had intravitrealinduction and maintenance therapy. Retinal detachmentoccurred in three eyes in the intravitreal therapy group and22 eyes of patients receiving intravenous or oral mainte-nance therapy. The risk of retinal detachment with systemictherapy was 14-fold higher than intravitreal therapy(
P
< 0.001) and up to fourfold higher with oral maintenancetherapy.
Retinal detachment has been reported to occur in10–29% of patients with CMV retinitis who are treated withsystemic antiviral therapy (ganciclovir or foscarnet).
7–9
Themedian time interval between the diagnosis of CMV retini-tis and retinal detachment in the first eye has been reportedto be 12–83 weeks
7,8,21,22
and the 1 year cumulative proba-bility of detachment has been estimated to be 24–59%.
7–9
Bilateral detachments have been reported in 15–56% ofpatients with bilateral CMV retinitis.
9,23–25
Prevention of retinal detachment in CMV retinitis is animportant goal of management as the visual outcome ofretinal detachment surgery in CMV retinitis patients ispoor. Median survival following surgery has been reportedto be 4–9 months and has increased with HAART.
7,22,26
Untreated, detachments frequently progress to no percep-tion of light
7,26
and treatment with laser demarcation hashad limited and variable success.
21,25–27
Most CMV-relateddetachments require pars plana vitrectomy and injection ofgas or silicone oil to tamponade the retina, offset tractionalforces and protect against detachment from future breaks.
8,28
Anatomical success for such procedures ranges from 70 to100%; however, visual results are disappointing with onlyambulatory vision being achieved in the majority ofpatients.
7,23,25,29
Reduced visual function may result fromdisease progression, optic atrophy, cataract and refractiveproblems associated with silicone oil.
25,30
The risk of retinal detachment in CMV retinitis is relatedto the size and position of the lesion. Jabs
et al.
reportedthe cumulative probability of retinal detachment amongpatients presenting with lesions involving 50% or more ofthe retina to be 50% at 6 months compared with 50% at12 months for patients with lesions less than 50% of theretina in size.
7
An association between retinal detachmentand extension of retinitis to the ora (peripheral retina) wasalso noted in all but one in this series of 38 retinal detach-ments.
7
Similarly Freeman
et al.
reported that an increase inthe surface area of retinitis outside the posterior pole at thelatest clinical examination was a significant risk factor forretinal detachment and suggested that differences in retinalthickness and its relationship with the posterior vitreousmay be responsible.
8
Peripheral involvement of more than25% of retinal surface area increased the risk of retinaldetachment fivefold when compared with eyes that had10% of the retinal area involved.
8
Although relapse was notthought to contribute to the risk of retinal detachment,
Figure 1.
Survival functions (event = retinal detachment) for thethree treatment groups, obtained from the Cox proportionalhazards model shown in Table 4. (…) Group A, intravitreal induc-tion therapy; ( ) group B, systemic therapy with oral ganciclovir;(—) group C, systemic therapy with intravenous ganciclovir orfoscarnet.
Table 5.
Analysis of retinal detachment rate by centre
Centre
n
No. retinal detachments
PMAR Retinal detachment
incidence rate
Centre 1Group A 10 0 62 0.000Group B 18 1 177 0.006Group C 98 17 682 0.002
Centre 2Group A 43 3 305 0.004Group B 2 0 7 0.0Group C 15 4 42 0.02
Group A, intravitreal induction therapy; group B, systemictherapy with oral ganciclovir; group C, systemic therapy withintravenous ganciclovir or foscarnet; PMAR, person-months-at-risk.

CMV-related retinal detachment 101
active retinitis increased the risk of retinal detachmentalmost threefold in this group, although it was not thoughtto be contributory in the patients reported by Jabs
et al.
7
andFreeman
et al
.
8
Kempen et al. studied the incidence of retinal detach-ments in patients treated with ganciclovir implants andthose treated with HAART.31 The rate of retinal detachmentwas the same in patients treated with ganciclovir implantswhen compared to those treated with systemic anti-CMVdrug therapy. This study also showed that increasing lesionsize and peripheral retinal involvement were risk factors fordetachment. HAART had the greatest effect of any variableevaluated in the study and resulted in a 60% reduction in therisk of retinal detachment. This effect was thought to be dueto a combination of improved control of retinitis preventingrelapses and increasing area of retinal involvement, andincreased immune response against CMV resulting instronger adhesion between the neurosensory retina and theunderlying retinal pigment epithelium.
In the present study, the risk of retinal detachment in thesystemically treated patients was substantially higher thanthat in the intravitreal group, and the risk of retinal detach-ment increased sixfold when 25% or more of the retinal areawas involved. The increased risk of detachment withincreased area of CMV retinitis is in agreement with previ-ous findings for patients on intravenous therapy.7,8
Several factors may contribute to the difference in risk ofretinal detachment between patients treated with intra-vitreal and systemic therapy found in the present study.Although not thought to directly contribute to the risk ofretinal detachment,7,8 relapse may significantly increase thesize of retinitis lesions and extend their borders anteriorlytoward the ora serrata and vitreous base. In the presentstudy, a relation was found between relapse and retinaldetachment but there was insufficient detail concerning thenumber and timing of relapses to allow a full analysis.Similarly, there were insufficient data concerning otherfactors (such as zone of retinal involvement and bilateralinvolvement) for a full assessment as possible risk factors forretinal detachment.
Retina infected by CMV becomes necrotic and is largelyreplaced by thin glial scar tissue that is poorly adherent tothe underlying retinal pigment epithelium and choroid.Attached posterior hyaloid may apply traction to such areasresulting in retinal tears and detachment. Martin et al.reported that all retinal detachments that developed in theirstudy of patients with CMV retinitis treated with ganciclo-vir implants, occurred at the time of posterior vitreousdetachment.15 Our study did not specifically evaluatewhether a posterior vitreous detachment was present inpatients with a retinal detachment and it was not possible togo back and obtain these data in sufficient patients to enableuseful analysis to be performed. Despite this, it is likely thatrapid effective control of retinitis followed by posteriorvitreous separation, induced by the intravitreal injections, isthe mechanism that resulted in a lower rate of retinaldetachment in patients in this study.
Although retinal detachment has been reported duringan intravitreal injection for treatment of CMV retinitis10 andpatients are routinely warned of this possibility, we have notexperienced this in over 1500 injections. Other rare compli-cations of intravitreal injection have been reported such asvitreous haemorrhage and intraocular infection.11–13 Thesewere not seen in the present study population.
In our study there was an increased risk of detachment inpatients treated at centre 2. The reason for this is unclear. Itis most likely related to recruitment bias and bias related tomanagement decisions made by the treating clinicians atcentre 2 that were unable to be assessed in this study. Theremay also be other unknown factors that biased the distribu-tion of other prognostic factors not identified in this study,or the result may have occurred by chance. Bias is aninherent weakness of studies such as the present one; how-ever, this must be balanced against the fact that studies ofthis design report the ‘real world’ experience of clinicianswho have managed a group of patients with the disease.
This study predates the use of HAART, so that follow-uptimes are shorter than would now be expected. Long-termintravitreal injections have been largely replaced by the useof sustained release ganciclovir implants, which have asimilar risk of retinal detachment to that of systemic ther-apy.15,31 Based on the results of the present study and morerecent changes in the management of HIV infection, ourapproach to the management of newly diagnosed CMVretinitis is to initially control the infection with intravitrealinduction treatment. Once the retinitis is healed and intra-vitreal injections have induced a partial vitreous detach-ment, a sustained release ganciclovir implant is placed in theinvolved eye(s) as an elective procedure. The patient is alsostarted on HAART and oral ganciclovir to protect the felloweye if necessary. Once immune reconstitution has occurredand the CD4 count has risen sufficiently (more than100–150), the oral ganciclovir can be ceased and the patientfollowed. A single ganciclovir implant provides effectivetherapy for 28–32 weeks and is usually sufficient to allowcontrol of HIV infection and elevation of the CD4 count toa level that restores immune responses against CMV. Thisapproach to treatment of CMV retinitis is now standardpractice at the authors’ treatment centres.
The treatment of CMV retinitis has changed greatly overthe last decade due to the development of specific anti-CMV drugs and the complex effects of HAART on thenatural history of HIV infection and opportunistic infec-tions such as CMV. Effective treatment of CMV retinitisremains an important management goal to protect visionfrom the devastating effects of CMV retinitis and CMV-related retinal detachment.
REFERENCES
1. Detels R, Munoz A, McFarlane G et al. Effectiveness of potentantiretroviral therapy on time to AIDS and death in men withknown HIV infection duration. Multicenter AIDS CohortStudy Investigators. JAMA 1998; 280: 1497–503.

102 Young et al.
2. Chene G, Binquet C, Moreau JF et al. Changes in CD4+ cellcount and the risk of opportunistic infection or death afterhighly active antiretroviral treatment. AIDS 1998; 12: 2313–20.
3. Jacobson MA, French M. Altered natural history of AIDS-related opportunistic infections in the era of potent combinationantiretroviral therapy. AIDS 1998; 12 (Suppl. A): S157–63.
4. Jacobson MA. Cytomegalovirus retinitis: new developments inprophylaxis and therapy. AIDS Clin Rev 1997–98: 249–69.
5. Jabs DA, Enger C, Bartlett JG. Cytomegalovirus retinitis andacquired immunodeficiency syndrome. Arch Ophthalmol 1989;107: 75–80.
6. Peters BS, Beck EJ, Anderson S et al. Cytomegalovirus infectionin AIDS. Patterns of disease, response to therapy and trends insurvival. J Infect 1991; 23: 129–37.
7. Jabs DA, Enger C, Haller J, de Bustros S. Retinal detachmentsin patients with cytomegalovirus retinitis. Arch Ophthalmol1991; 109: 794–9.
8. Freeman WR, Friedberg DN, Berry C et al. Risk factors fordevelopment of rhegmatogenous retinal detachment inpatients with cytomegalovirus retinitis. Am J Ophthalmol 1993;116: 713–20.
9. Studies of Ocular Complications of AIDS Research Group inCollaboration with the AIDS Clinical Trials Group. Rhegma-togenous retinal detachment in patients with cytomegalovirusretinitis: the foscarnet-ganciclovir cytomegalovirus retinitistrial. Am J Ophthalmol 1997; 124: 61–70.
10. Ussary FM, Gibson SR, Conklin RH, Piot DF, Stool EW,Conklin J. Intravitreal ganciclovir in the treatment of AIDS-associated cytomegalovirus retinitis. Ophthalmology 1988; 95:640–64.
11. Heinemann M-H. Long-term intravitreal ganciclovir forcytomegalovirus retinitis. Arch Ophthalmol 1989; 107: 1767–72.
12. Cochereau-Massin I, Lehoang P, Lautier-Frau M et al. Efficacyand tolerance of intravitreal ganciclovir in cytomegalovirusretinitis in acquired immune deficiency syndrome. Ophthalmol-ogy 1991; 98: 1348–55.
13. Young S, Morlet N, Besen G et al. High dose intravitrealganciclovir in the treatment of CMV retinitis. Ophthalmology1998; 105: 1404–10.
14. Anand R, Nightingale SD, Fish RH, Smith TJ, Ashton P.Control of cytomegalovirus retinitis using sustained release ofintraocular ganciclovir. Arch Ophthalmol 1993; 111: 223–7.
15. Martin DF, Parks DJ, Mellow SD et al. Treatment of cyto-megalovirus retinitis with an intraocular sustained-releaseganciclovir implant. A randomized controlled clinical trial.Arch Ophthalmol 1994; 112: 1531–9.
16. Hatton MP, Duker JS, Reichel E, Morley MG, Puliafito CA.Treatment of relapsed cytomegalovirus retinitis with sustained-release ganciclovir implant. Retina 1998; 18: 50–55.
17. Shah R, Versace P, McCluskey PJ. Outcomes of cytomegalo-virus retinitis following use of sustained release ganciclovirimplant. Aust NZ J Ophthalmol 1998; 26: 207–10.
18. Ng P, McCluskey PJ, McCaughan G, MacDonald P,Glanville A, Keogh A. Ocular complications of heart, lung andliver transplantation. Br J Ophthalmol 1998; 82: 423–8.
19. Studies of Ocular Complications of AIDS Research Group inCollaboration with the AIDS Clinical Trials Group. Mortalityof patients with the acquired immunodeficiency syndrometreated with either foscarnet or ganciclovir for cytomegalovi-rus retinitis. New Engl J Med 1992; 326: 213–20.
20. Morlet N, Young SH, Strauhan D, Coroneo MT. Techniqueof intravitreal injection. Aust NZ J Ophthalmol 1993; 21:130–31.
21. Studies of Ocular Complications of AIDS Research Group incollaboration with the AIDS Clinical Trials Group. Foscarnet-ganciclovir cytomegalovirus retinitis trial. 4. Visual outcomes.Ophthalmology 1994; 101: 1250–56.
22. Dowler JGF, Towler HMA, Mitchell SM, Cooling RJ, Light-man SL. Retinal detachment and herpesvirus retinitis inpatients with AIDS. Br J Ophthalmol 1995; 79: 575–80.
23. Kupperman BD, Flores-Aguilar M, Quiceno JI et al. Amasked prospective evaluation of outcome parameters forcytomegalovirus-related retinal detachment surgery in patientswith Acquired Immune Deficiency Syndrome. Ophthalmology1994; 101: 46–55.
24. Chuang EL, Davis JL. Management of retinal detachmentassociated with CMV retinitis in AIDS patients. Eye 1992; 6:28–34.
25. Freeman WR, Quiceno JI, Crapotta JA, Listhaus A,Munguia D, Aguilar MF. Surgical repair of rhegmatogenousretinal detachment in immunosuppressed patients withcytomegalovirus retinitis. Ophthalmology 1992; 99: 466–74.
26. Orellana J, Teich S, Lieberman RM, Restrepo S, Peairs R.Treatment of retinal detachments in patients the AcquiredImmune Deficiency Syndrome. Ophthalmology 1991; 98:939–43.
27. McCluskey P, Grigg J, Playfair TJ. Retinal detachments inpatients with AIDS and CMV retinopathy: a role for laserphotocoagulation. Br J Ophthalmol 1995; 79: 153–6.
28. Freeman WR, Henderly DE, Lee Wan W et al. Prevalence,pathophysiology and treatment of rhegmatogenous retinaldetachment in treated cytomegalovirus retinitis. Am J Ophthal-mol 1987; 103: 527–36.
29. Regillo CD, Vander JF, Duker JS, Fischer DH, Belmont JB,Kleiner R. Repair of retinitis-related retinal detachment withsilicon oil in patients with acquired immunodeficiency syn-drome. Am J Ophthalmol 1992; 113: 21–7.
30. Sandy CJ, Bloom PA, Graham EM. Retinal detachment inAIDS-related cytomegalovirus retinitis. Eye 1995; 9: 277–81.
31. Kempen JH, Jabs DA, Dunn JP, West SK, Tonascia J. Retinaldetachment risk in cytomegalovirus retinitis related to theacquired immunodeficiency syndrome. Arch Ophthalmol 2001;119: 33–40.