Embed Size (px)
Citation preview

Ophthalmic Epidemiology 0928-6586/us$3.50
Retinoblastoma referral patterns in Saudi Arabia
Ophthalmic Epidemiology - 1996, Vol. 3, No. I. pp, 35 - 46 Q & o h Press Buren (The Netherlands) 1996
Paul B. Mullaney, FRCSI, FRCOphth’ Zeynet A. Karcioglu, MD’,‘
Saleh Ai-Mesfer, MD’ Mashael Dowaidi, COT’
Accepted 28 September 1995 ’ King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia and ’
Tulane University Medical School, New Orleans, Louisiana
Abstract The purpose of this study was to review the patterns of referral and presentation of patients with retinoblastoma in Saudi Arabia from 1983- 1994. Retinoblastoma represents a particularly high volume at the King Khaled Eye Specialist Hospital and the Hospital’s Retinoblastoma Registry provided relevant data. Records of 257 registered patients were analyzed. Of these, 112 were bilateral whereas 145 were unilateral, resulting in a total of 369 eyes. Referral diagnosis accuracy was high, 75% of referring physicians rank- ing retinoblastoma at the top of their differential diagnosis. Delay in referral was found to average 9.4 weeks. However, 49.4% of eyes were staged at Reese- Ellsworth Stage Vat presentation. Significantly, the number of patients pre- senting with extraocular disease fell from 22.8% (1983-1988) to 12.3% (1989- 1994), highlighting increasing awareness of retinoblastoma and availability of services in Saudi Arabia.
Keywords ferral, incidence
childhood tumors, retinoblastoma, Saudi Arabia, patient re-
Introduction Retinoblastoma has a worldwide incidence of approxi- mately 1/17,000 to 1/34,ooo live births per year.’ In the Kingdom of Saudi Arabia, the overall retinoblastoma incidence has not been established. Reti- noblastoma represents a particularly high volume at King Khaled Eye Spe- cialist Hospital (KKESH) in Riyadh because the majority of retinoblastoma cases in the Kingdom are referred to this center.
Although there are studies regarding retinoblastoma incidence,**’ natural history, and referral patterns: a detailed study regarding referral diagnosis and the source of referral has not been done in the Kingdom of Saudi Arabia. We examined this problem not only because retinoblastoma is a common neoplastic disease of childhood in this country, but also to gather data for the improvement of the referral system. We wanted in particular to study in- formation in relation to reasons for referral, routes of referral, age of referral, and stage of disease at presentation to K K E S H .
Correspondence to: Dr. Paul B. Mullaney cIo Medical Library, King Khaled Eye Specialist Hospital
Riyadh 11462 Kingdom of Saudi Arabia Tel.: +966-1-482-1234 ext. 3775 Fax. +966-1-482-1908
P.O. BOX 7191
Acknowledgements: Because of the cumulative nature of the information, many K K E S H staff have participated in the collection of data and the management of retinoblastoma patients. The authors specifically wish to acknowledge Drs. Susan Senft, Emad Abboud, and Rosalind Stevens, together with Monzer Jabak, R N and Katherine Dabas, R N for their tireless input into the retinoblastoma program at K K E S I ~ which made this study possible.
Retinoblastoma referral in Saudi Arabia 35
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

Materials and methods King Khaled Eye Specialist Hospital is the ter- tiary referral center for ophthalmology in the Kingdom of Saudi Arabia. The population of Saudi Arabia is 15.9 million, including both Saudis and expatri- ates. The current birth rate is 574,000 per year, representing an annual in- crease of 3.6%. A small but constant number of patients are referred from surrounding countries, for example Egypt (population 54.8 x I O ~ ) , Sudan (population 13.3 x 10~1, Syria (population 13.3 x ro6>, eme en (population 10.5 X ro6), and Jordan (population 4.3 x ro6).
The K K E S H Retinoblastoma Registry, which contains 257 patient records, provided pertinent data.The registry commenced in 1983 and is regularly up- dated.This registry is mostly composed of histologically proven retinoblasto- ma patients. A small minority consists of small tumors which receive other forms of treatment. The following parameters were noted route and reason for referral; age, sex, type of symptoms cited; delay between when symptoms were first noted and first presentation at a primary referral source; delay be- tween the primary referral source (Ministry of Health Clinic, General Practi- tioner, etc.) and presentation at the tertiary care unit (KKESH); referral source diagnosis and accuracy; geographic source; and whether self-paying or gov- ernment funded. The efficacy of the K K E s H screening program was ascer- tamed. The laterality of tumors was noted and all were categorized by the Reese-Ellsworth staging schema at time of presentation5 Finally, we noted the number of patients who died or became lost to follow-up since 1984. Com- parison of means between age and time presentations of the different groups was conducted by the use of the two-group t-test. The chi-squared test was used to compare the incidence of extraocular extension between 1983- 1988 and 1989- 1994.
Thirty patients initially presented elsewhere and had their treatment insti- tuted before referral to our hospital for further management.
Results
Age and Sex There are 122 male (47.5%) and 135 female (52.5%) entries in the K K E S H Retinoblastoma Registry. The ages of presentation ranged from under I week to 14.7 years. In general, bilaterally affected patients presented at an earlier age. This is particularly true for males, where 75% of bilateral cases presented prior to 24 months. In females the difference in presentation between bilateral and unilateral patients was not so obvious, being 60% and 50%, respectively, prior to 24 months. Unilateral retinoblastoma was com- mon in both genders over 24 months of age. Of the 257 patients, 112 (43.6%) were bilateral whereas 145 (56.4%) were unilateral. This translates into 369 eyes.
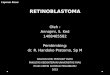
Excluding the 30 patients who presented elsewhere, there are 109 males (48.0%) and 118 females (52.0%) who presented toKKEsH.The ages ofpresen- tation ranged from under I week to 11 years. Unilateral presentation times ranged from 2 to 432 weeks 18 years 3 weeks] (mean= 116.4 weeks) (Figure I). Bilateral presentation times ranged from I to 576 weeks [11 years] (mean 83 weeks) (Figure I). In general, bilaterally affected patients presented at an earlier age. When analyzed with the ?-test the early bilateral presentation was significant (p = 0.0028).
In the comparison between male and female ages of presentation no sta- tistically significant difference was seen. Male presentation times ranged
36 Paul B. Mullaney et al.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

Fig. 1. .4ge at presentation of patients with retinoblastoma at King Khaled Eye Specialist Hospital
%
7-1 1 12-23 24-36 Age (Months)
~ ~~~~~
1 Maleunilateral e Male-bilateral 1 Femaleunilateral a Female-bilateral
from 2 to 384 weeks [7 years 38 weeks] (mean = 103.7 weeks), female presen- tation times ranged from I day to 576 weeks [11 years] (mean = 101.2 weeks).
The presentation times of Saudi (181) and non-Saudi (46) patients were examined and found not to be significantly different. Saudi patients presented at ages from I day to 576 weeks [11 years 7 weeks] (mean= 101.8 weeks). Expatriate patients presented at ages from 8 to 432 weeks [8.3 years] (mean= 104.9). Moreover, Saudi bilateral patients (range I day to 576 weeks Ir1.r years]) (mean = 76.5 weeks) presented significantly earlier than Saudi unilateral patients (range 2 to 432 weeks [8.3 years]) (mean = 118.9 weeks) (p = o.ooog). No statistically significant difference was seen in the presenta- tion times between non-Saudi unilateral and bilateral patients. Expatriate unilateral retinoblastoma presentation times ranged from 8 to 240 weeks [4 years 6 weeks] (mean = 105 weeks) and bilaterals presented at ages from 8 to 432 weeks [8 years 3 weeks] (mean = 104.8 weeks).
Referral Routes The largest group of patients (1201257 or 46.7%) were re- ferred from peripheral hospitals under the auspices of the Ministry of Health. The second largest category were self-referred (52 or 20.3%) and accessed the
Retinobfastoma referrat in Saudi Arabia 37
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

T A B L E I. Referral route of ,I , n '70 retinoblastoma patients to the King __ Khaled Eye Specialist Hospital.
Ophthalmologist (MOH*) I20 (46.7) Royal Order 35 (13.6) Self (KKESH ER**) 30 (11.7) Self ( K K E s H Clinic) 22 ( 8.6)
Family Screening (K K E s H) 8 ( 2.7) Other Hospitals 8 ( 3.2) ARAMCO*** 4 ( 1.9)
Total 257 100%
General practitioner 30 (1 I .7)
* MOH = Ministry of Health; ** ER = Emergency Room; *** A R A M C O = Arabian American Oil Company
Hospital through the Emergency Room or Screening Clinic. General Practi- tioners referred 30 (11.7%). As can be seen in Table I, either the Ministry of Health or the Royal Family paid for the majority of patients. Most patients arrived with a letter of referral from a physician (222 [86.4%]) or carried a Royal Order (29 [11.3%]) requesting treatment. Six patients had no referral document. A single physician was visited by 187 patients (72.8%) prior to pre- sentation. However, 36 patients (14.0%) visited multiple physicians and 34 (13.2%) saw none.
Delay in Referral The delay in presentation to a primary referral source ranged from less than I to greater than 12 weeks, with a mean delay of 6.2 weeks [SD 14.41. In comparison, there was a reduction in the delay of referral from the primary care source to K K E SH (a tertiary care center) of 3.2 weeks [SD 10.51. This second delay ranged from o to 102 weeks. Table 2 elaborates on time delays.
The increase in the number of patients who presented to K K E S H in less than I week (145) after primary referral in comparison to those who presented
T A B L E 2. Delay times from when symptoms were first noticed to presentation at a primary referral
King Khaled Eye Specialist Hospital.
Delay Time (weeks) Primary Care Tertiary Care
source and subsequent presentation at No. (%) No. f %)
o (immediate) 5 ( 2.6) I45 (61) I 76 (38.8) 30 (12.6) 1-4 59 (30.1) 23 ( 9.7) 5-8 26 (13.3) 17 ( 7.1) 9- I 2 9 ( 4.6) 8 ( 3.4) > I2 21 (10.7) 15 ( 6.3)
NA* 61 I9
Total 196 100% 238 100%
* N A =Not Available
38 Paul B. Mullaney et al.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

T A B L E 3. Diagnostic accuracy at the primary referral source and at the
Diagnosis Primary Physician K K E S H ER*
emergency room at the King Khaled W) Eye Specialist Hospital. No. f 3;) No.
Retinoblastoma Investigations Leukocoria Retinal Detachment Cataract Ccilulitis Endophthalrni tis Glaucoma Strabismus Vitreous Hemorrhage Proptosis Other Not Available
169 29
6
4 3 I
I
I
I
I
0
7 34
114 I
11
0
3 I
I
0
0
I
I
7
* A further I 17 (45.5%) patients were seen directly by either a pediatric ophthalmol- ogist or a retinal subspecialist (tertiary care provider).
within I week to the primary care center (5) appears to indicate that once patients were aware of the gravity of the disease they were less likely to delay.
In 61/257 patients no information was available in the Medical Records as to whether a delay occurred between the home and primary care center. A similar recording deficiency was present as to whether there had been a delay for 19 patients between the primary care center and KKESH.
Referral Diagnosis Accuracy Table 3 indicates that 65.7% of referrals from primary sources correctly suspected retinoblastoma as the diagnosis. A further 11.3% were referred for investigations, thus entertaining the possibii- ity of retinobiastoma in the differential diagnosis. Most patients seen by ophthalmologists in the K K E S H Emergency Room were correctly diagnosed. (The Emergency Room ophthalmologists surveyed were not pediatric ophthalmologists or vitreo-retinal subspecialists but were a mixed group of ophthalmologists and ophthalmology residents.)
Ethnic Origin The vast majority of patients referred to K K E S H were Saudi: 202 (78.6%). A wide spread of nationalities from Middle Eastern, Gulf States, and other countries were referred to our tertiary care center. The totals are as follows: Yemeni 13 (5.0%), Egyptian 6 (2.3%), Pakistani 6 (2.3%), Sudanese 5 (1.9%), Syrian 5 (r.g%), Bahraini 4 (1.6%), Jordanian 4 (1.6%), Kuwaiti 3 (1.2%), Filipino 2 (0.8%), Palestinian I (0.4%), others 6 (2.3%), for a total of 257 (100%).
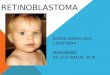
Parental Age Figure 2 graphically depicts the age of the parents. The major- ity of fathers were in their third decade, while the peak age for mothers oc- curred between 26 -30 years of age.
Presenting Complaint The majority of parents (66.6%) noticed leukocoria
Retinobiastoma referral in Saudi Arabia 39
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

Fig. 2. Age groups of the parents.
20 - %
15-
10-
5-
0 ' f
FATHER
MOTHER
20-25 26-30 31-35 3-40 41-45 4550 51-55 58-80 NIA
Age
and sought medical advice for their child. This was followed by strabismus 9'%, panophthalmitis/red eye 2.7%, and proptosis/ buphthalmos 1.4%. Mis- cellaneous complaints comprised 5% and included hyphema, obvious extra- ocular extension, poor vision, photophobia and 'abnormal appearance of eyes.'A number ofpatients (11.4%) were referred from other centers to K K E S H for further care of retinoblastoma and socket-related problems; the K K E S H family screening program detected another eight patients.
Presentation The annual presentation is depicted inTable 4 and varied from 5.4% in 1991 to a high of 11.7% in 1987. The figures for 1983 and 1994 do not accurately reflect annual presentation rates as the Hospital opened in the middle of 1983, and at, the time of statistical compilation 1994 is not yet a complete year.
Stuging ut Time of Presentation All patients were staged according to the Reese-Ellsworth classification! Those patients with bilateral retinoblastoma had both eyes staged independently. Unfortunately, as can be seen inTable 5 , StageV was the presenting category for 49.9% of all eyes. The result showed a statistically significant difference in the stages at time of presentation be- tween u.nilatera1 and bilateral retinoblastoma (X2 = 23.125, p < 0.003 on 5 d.f.). In fact, while only 10.3% of unilateral cases are classified as stages I to 4 compared to 30.3% of bilaterals, stageV was predominant among unilateral retinoblastoma (60.7% vs 41.9%). A higher proportion was also found among unilateral retinoblastoma classified as other stages. Another 27.9% of pa- tients did not correlate to Reese-Ellsworth staging (listed as 'Others' inTable 5) . This group includes patients referred with extraocular extension of retino- blastoma and those enucleated elsewhere for retinoblastoma and who were referred to K K E S H for further management. These had either extraocular dis- ease on presentation or were referred after enucleation for socket-related pro- blems.
40 Paul B. Mullaney et al.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

T A B L E 4. Annual distribution of all retinoblastoma referrals to King
Year Saudi iVon-Saudi ~-
1 I 0
21
15
26 22
I9
I3 14 24
20
I 1
0
6 4 3 4 9 6 9
6 5 5
I
Khaled Eye Specialist Hospital.
Total 202 5.5
During the decade, retinoblastoma referrals were fairly constant, but the incidence of extraocular extension has decreased; i.e., in the first five years,. 29 (22.8%) patients presented with extraocular extension, versus 16 (12.3%) patients seen with extraocular extension during the last five years (Table 6). This reduction achieved significance with p = 0.02 (chi-squared test). The ar- bitrary selection of these time intervals was adopted to show the effect of in- creasing awareness of retinoblastonia in the decade since K K E S H opened.
Screening Program Eight new patients were seen as a result of the screening program established at KKESH in 1983. This program aims to screen all sib- lings of affected children - up to 2 years of age for siblings of unilaterally af-
T A B L E 5. Reese-Ellsworth staging of retinoblastoma referrals at diagnosis5 CIassiFcation Unilateral Bilateral *
-
369 eyes n % n %
Ia 4 2.6 17 1.6 Ib IIa IIb IIIa IIIb IVa IVb Va Vb Others
I
I
I
0
3
5 37 51 42
0
0.7 0.7 0.1 0
2. I
0
3.4 25-5 35.2 29.0
I5 6 9 5
8 6
43 53 60
2
6.7 2.7 4.0
0.9
2.6 18.2 23.7 26.8
2.2
3.6
Total 145eyes 224 eyes
* Both affected eyes were cumulatively staged.
Retinoblastoma referral in Saudi Arabia 41
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

T A B L E 6. Number ofpatients presenting initially at King Khaled Eye
Retinohlastoma Extraocular Years Cases Extension Cases
Specialist Hospital with extraocular - extension.
fected and up to 4 years for those of bilaterally affected children. Six (2.3%) of these were siblings of known unilateral cases and two (0.8%) were siblings of bilateral cases. This figure pertains only to those children who were routinely screened to rule out retinoblastoma. It does not include those who presented opportunistically as a result of a positive family history. Overall, the Retino- blastoma Registry indicates that 22 of the bilateral and 10 of the unilateral patients have a positive family history.
Present Registry Numbers The total number of patients listed in the K K E s H Retinoblastoma Registry is 257; at present, 168 are actively being followed. Currently, 50 patients in the registry are deceased (19.5%) and a further 39 (15.2%) have been lost to follow-up.
Discussion Based on the figures of Sanders et al., approximately 40 new retinoblastoma cases are seen annually by hospitals in England, Scotland and Wales combined? When one considers that on average 21 new cases are seen at K K E S H every year and all these patients are diagnosed, treated, and fol- lowed in this one institution until they die or leave the Kingdom (current hos- pital policy states that retinoblastoma patients are followed at the institution throughout the life of the patient), the numerical significance of the retino- blastoma issue becomes quite clear.
Table I lists the referral routes and shows that the majority of patients are referred to KKESH from peripheral Ministry of Health Hospitals. Many are self-referred while others are sponsored by the King and the Royal Family. Patients in this latter category are usually from outside Saudi Arabia and can- not afford the cost of hospitalization. These patients generally go to a prince’s ofice and petition him to cover the cost of their care. However, Table 2 con- firms that the vast majority of patients come with a doctor’s referral letter. Family screening is a routine requirement and uncovered eight new patients with retinoblastoma. Some patients are referred to K K E S H for further treat- ment having had their treatment initiated elsewhere. This hospital offers the only ocular prosthetics care in the Kingdom, and therefore all patients who had enucleation performed elsewhere must come for socket rehabilitation to K K E SH. This underlies the tertiary care setting in which K K E s H operates. Primary level diagnostic accuracy was high (Table 3) and rose higher when patients were seen in the K K E S H Emergency Room. It is probable that this diagnostic accuracy led to the relatively short mean referral delays.
Retinoblastoma comprises between 3.0% and 7.4% of all childhood t ~ m o r s . ~ ” Almost all statistics from Western countries are based on informa- tion obtained from local Cancer Registries although some patients, particu- larly those who die early with metastases, are not registered and, therefore, not reflected in the statistics. The true incidence rates in Western countries
42 Paul B. Mullaney et al.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

are believed to be approximately ro0/o higher than the reported figures.? In Saudi Arabia, considering the still developing nature of the health care and tumor registry systems, we suspect that the incidence could be increased by as much as 15% to 20% of available figures.
Devesa reported an incidence in the United States of 1/18,ooo live births8 Kaneko estimated the incidence of retinoblastoma in Japan to be 1/14,859 live births.' In South Africa, Freedman and Goldberg estimated the incidence among the Bantu to be I/IO,OOO.'~ Sanders et al.' found an incidence of 1/23,000 live births in England; Tarkkanen and Tuovinen" 1/16,000 in Fin- land; JensenI2 r/I8,ooo in Denmark; Barry and MullaneyI3 1/20,501 in Ire- land; and H ~ r v e n ' ~ 1/12,300 in Norway. We calculate the incidence of reti- noblastoma in Saudi Arabia to be 1/14,525. This translates to an incidence of 1/27,407 for unilaterally affected and 1/30,906 for those with bilateral retino- blastoma. This figure does not include those expatriates with retinoblastoma residing in Saudi Arabia.
Others have described the incidence of retinoblastoma in relation to the total number of ophthalmic patients. For example, Berrisford" described a 1:9,614 ratio at the Royal London Ophthalmic Hospital; McCrae16 found a 1:6,126 ratio in Dublin; and K~dilinye'~ found I retinoblastoma in every 192 ophthalmic patients in Ibadan. In Riyadh, Saudi Arabia, Al-Kaff et al. and Al-Idrissi et al. reported an incidence of I: 11,580 patient^.'^''' However, these two latter reports pertained only to the incidence in Riyadh.
Retinoblastoma is the most common intraocular malignancy in Saudi Arabia, accounting for 41.7%.*' This contrasts with North America where re- tinoblastoma occurs in a much lower proportion of total ocular tumor inci- dence. The proportions reported by the USA.-based National Cancer Institute and the Cancer Registry of the State of New Mexico are 14% and 11.8% of retinoblastoma, respectively.213" However, the markedly lower num- bers of malignant melanoma in Saudi Arabia (according to Huaman and Ca- vender) may make the figures for retinoblastoma look artificially high.*' In our study, more than 50% of the chldren presented under the age of 2
years. This corresponds well with Pendergrass who also found that more than half of the cases presenting in the US. were under 2 years of age.3 Many of our 257 cases presented at a late stage with 49.9% of eyes presenting with tumors of Reese-Ellsworth Stage V. This correlates with what Rubenfeld et al. fo~nd. '~ In their series, whether unilateral or bilateral disease, Group V was the most common presenting intraocular stage. This trend towards late pre- sentation was much more evident in the former years at K K E S H . Series from other developing countries have also highlighted the advanced stages of pre- sentation. The majority of these children presented with extraocular dis-
In comparison, Lennox et al. reported that only five children out of 268 presented with extraocular spread in the United Kingdom during 1962-68.7 This pattern can be seen again in the average age of diagnosis, which in Nigeria in 1984 was 43.4 months for unilateral and bilateral retino- b l a ~ t o m a . ~ ~ This compares with 14.8 months for bilateral, and 23 months for unilaterally affected patients in the United States.30
Over the past ten years, the infrastructure in Saudi Arabia has vastly im- proved. Concurrently, awareness about retinoblastoma among general prac- titioners, pediatricians and the general public has increased, leading to earlier referral. Evidence of this is seen in the reduction in numbers of children pre- senting with advanced extraocular retinoblastoma as shown in Table 6 .
ease.6.10. 17.24-29
Retinoblastoma referral in Saudi Arabia 43
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

Delay in referral is a cause for concern in retinoblastoma cases and many series correlate it with poor p r o g n ~ s i s . ~ ~ ” ~ ’ ~ Table 2 gives the length of time between the onset of symptoms and presentation to a primary referral source. Our results compare well with the figures of Haik et al. in New York State.4 They found a 2-week delay for patients with a positive family history of reti- noblastoma from the onset of symptoms to presentation to the local physi- cian. This was followed by a 5-week delay in referral from physician to ophthalmologist. For their patients with a negative family history of retino- blastoma, these figures were 5 weeks and 4 weeks, respectively. This total aver- age delay of 3.5 and 4.5 weeks compares well to our 6.2 and 3.2 weeks delay. Like Haik et al., we found unacceptably long delays on occa~ion.~ One patient had a 102-week delay between the primary referral center and K K E S H . The fact that 36 (14%) patients had seen multiple doctors prior to coming to K K E S H points to some confusion about the diagnosis.
It is interesting to note that there are 112 bilaterally affected patients in the K K E s H Registry. However, only 22 of these families admit to having a positive family history. This corresponds well to the incidence of positive family his- tory seen in other studies.30 This suggests that most of these bilaterally af- fected patients have new germline mutation^.^^-^^ The number of families with a positive family history of retinoblastoma varies, depending on the re- ported series. Pieroni et al.35 reported a series with a 44% positive family his- tory, as did Carbajal.36 This compares to an absence of positive family histories in Nigeria and among the In both of these African series, patients presented at an advanced stage; 71.4% were extraocular in the Niger- ian series. It is probable that in this situation there would be no survivors to reach reproductive age. This is in contradiction to the United States where Carbajal’s 44% with positive family histories is attributable to greater sur- vival of patients afflicted with retinobla~toma.~~ An increasing incidence of retinoblastoma has been reported from Finland and Holland, among other countries.”*37 This is probably a similar factor in Saudi Arabia, though it is known that increased longevity of patients with retinoblastoma does not adequately explain the increasing incidence of the d i s e a ~ e . ~ ~ . ~ ~ Many of the previous generations afflicted would have died prior to reproductive age. Inaccurate histories and ignorance on the part of the patient as to proper diagnosis would also reduce the numbers of known affected family mem- bers. Families in Saudi Arabia also tend to be large, thus complicating the issue.
Parental age has been implicated in the pathogenesis?’ New mutations are more common with increasing paternal and are thought to arise as a result of errors in meiosis during spermat~genesis.~~-~’ High paternal age is relatively common throughout the Middle East and in Saudi Arabia. This was borne out by Senft et al. who reported that paternal age was elevated in fathers of Saudi Arabian retinoblastoma patients?6 The paternal age was greater than the maternal in our review. The majority of mothers conceived at the usual child-bearing years, between 20 and 35 years of age.The peak age group for fathers was 36 - 40 years of age, and fathers 50 years and over were still prevalent, as depicted in Figure 2.There seems to be a reluctance to coun- tenance the possibility of an hereditary aspect in the etiology of retinoblasto- ma. It is difficult to explain the low discovery rate in family screening. This is possibly attributable to the fact that inheritance is not felt to be a factor. There are also logistical problems associated with screening large families who have
44 Paul B. Mullaney et al.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

to come long distances. Many patients present when parents observe leuko- coria and have had experience of it in a previous family member.
Our Registry indicates that 43.6% of tumors are bilateral. Sanders et al.’ found 34.6% of patients with bilateral tumors in the United Kingdom study while Haik et al.4 found a 50% incidence of bilaterality among those present- ing in New York. However, Pendergrass found only a 20% incidence of bilat- eral disease in the U.S.A.3 We found no significant difference in the male and female incidence of bilateral or unilateral disease. There was a slightly higher incidence of retinoblastoma in females (n = 135) compared with males (n = 122). Almost a quarter (24.5%) of females had bilateral retinoblastoma compared with 19% of males. In bilaterally affected patients, 56% were female and 44% were male. This contrasts with Devesa’s nine female and two male bilateral cases.8 Other series have found the sex incidence to be nearly e q ~ a l . ~ . ~ ’ Mahoney et al.36 in New York State found a slightly higher male in- cidence (g.5/1 million boys versus 8.7/1 million in girls) as did Carbaja148 in his study published 30 years earlier. Herm and Heath found a higher propor- tion of males affected with both unilateral and bilateral re t inobla~torna .~~ They also found an 18.5% incidence of bilaterality in a large un-followed group. However, the bilaterality in a more closely observed group was found to be 25%. This suggests that the reported incidence of bilaterality is partly a function of adequate follow-up.
Unfortunately, 19.5% of our patients are deceased with another 15.2% lost to follow-up; the latter number probably contains more deceased patients. This gives a maximum survival rate of 80.5%. Sanders et a1.’ had an overall survival rate of 87% for 3 years in their U.K. report, and Pendergrass and Davis found a survival rate of 76% in the U.S.A.3 Even if one accepts a survi- val rate much lower than 80.5%~ it is still a remarkable result considering the advanced presenting nature of the disease in Saudi Arabia.
The health care delivery system in the Kingdom of Saudi Arabia is expand- ing rapidly. This, coupled with the improved education of the public and the introduction of new know-how and technology, is leading to more medical conditions being diagnosed and referred to specialists at earlier stages. This phenomenon has been noted with other ophthalmological disease entities5’ This is borne out by the marked reduction in patients presenting with extra- ocular retinoblastoma.
References
I Franqois J, Matton-Van Leuven MT. Recent data on the heredity of retino- blastoma. In: Boniuk M, editor. Ocular and Adnexal Tumors, New and Con- troversial Aspects. St. Louis: Mosby
2 Sanders BM, DraperTJ, Kingston JE. Retinoblastoma in Great Britain 1969- 80: incidence, treatment and survival. Br J Ophthalmol 1988; 72: 576 - 83.
3 Pendergrass TW, Davis S. Incidence of retinoblastoma in the United States.
1964: 123-41.
Arch Ophthalmol 1980; 98: 1204-10. 4 Haik BG, Siedlecki A, Ellsworth RM,
Sturgis-Buckhout L. Documented de- lays in the diagnosis of retinoblastoma. Ann Ophthalmol 1985; 17: 731-2.
on current concepts of retinoblastoma therapy. Ophthalmology 1963; 67: 164- 72.
6 Williams AO. Tumors of childhood in Ibadan, Nigeria. Cancer 1975; 370 - 8.
7 Lennox EL, Draper GJ, Sanders BM. Retinoblastoma: a study of natural history and prognosis of 268 cases.
5 Reese AB, Ellsworth RM. Evaluation
BMJ 1975; 3: 731-4. 8 Devesa SS. The incidence of retino-
blastoma. Am J Ophthalmol 1975; 80: 263 - 5.
9 Kaneko A. The incidence of retino- blastoma in Japan from 1975 to 1979. Atarashii Ganka 1984; I: 724-30.
10 Freedman J, Goidberg L. Incidence of retinoblastoma in the Bantu of South Africa. Br J Ophthalmol 1976; 60: 655- 6.
I I Tarkkanen A, Tuovinen E. Retinoblas- toma in Finland 1912-1964. Acta Oph- thalmol (Kbh) 1971; 49: 293-300.
Retinoblastoma referral in Saudi Arabia 45
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.

I 2
13
14
15
16
I7
18
I9
20
%I
22
23
24
Jensen OA. Retinoblastoma in Den- mark (1943- 1958). Acta Ophthalmol (Kbh) 1965; 43: 821-40. Barry G, Mullaney J. Retinoblastoma in the Republic of Ireland (1955-70). Trans Ophthalmol Soc UK 1971; 91:
Horven I. Retinoblastoma in Norway. Acta Ophthalmol (Kbh) 1974; 52: 107- 9. Berrisford PD. Statistical notes on glioma retinae with a report of 41 cases. Royal London Ophth Hosp Rep 1916; 20: 296. McCrea WBE. Glioma of the retina: a review of 12 cases. Br J Ophthalmol
Kodilinye HC. Retinoblastoma in Nigeria: problems of treatment. Am J Ophthalmol 1967; 63: 469 - 81. Al-Kaff AS, Jaafar M, Senft SH, Ber- quist G. Retinoblastoma in Saudi Ara- bia. Saudi Bull Ophthalmol 1989; 4: 212-6. Al-Idrissi I, Al-Kaff AS, Senft. SH. Cumulative incidence of retinoblastcr. ma in Riyadh, Saudi Arabia. Ophthal- mic Paediatr Genet 1992; 13: 9 - 12. Huaman A, Cavender JC. Tumors of the eye in Saudi Arabia. Ann Saudi Med 1991; 11: 675-80. National Cancer Institute. Malignant cases diagnosed in 1973-77. Monogr Natl Cancer Inst 1981; 57: 60-1. Cancer Registry, State of New Mexico,
Rubenfeld M, Abramson DH, Ells- worth RM, Kitchin FD. Unilateral vs. bilateral retinoblastoma. Correlations between age at diagnosis and stage of ocular disease. Ophthalmology 1986; 93: 1016 - 9. Abiose A, Adido J, Agarwal SC. Child- hood malignancies of the eye and orbit in Northern Nigeria. Cancer 1985; 55:
839 - 55.
1943; 27: 259.
USA 1973 - 87.
2889 - 93. 25 Olurin 0, Williams AO. Orbito-ocular
tumors in Nigeria. Cancer 1972; 30: 580-7.
26
27
28
29
30
31
32
33
34
35
36
37
38
Senft SH, JohnsonTE, Nasr AM. Extraocular retinoblastoma in Saudi Arabia. Orbit 1993; 12: 19-26. Erwenne C, Franco EL. Age and late- ness of referral as determinants of extraocular retinoblastoma. Ophthal- mic Paediatr Genet 1989; 10: 179-84. Sevel D, Sealy R, Lawton E. Retino- blastoma at Groote Schuur Hospital 1952-1972. Trans Ophthalmol SOC UK 1973; 93: 23-32. Sunder-Raj S. Childhood malignancies of the eye and orbit inTanzania with special reference to retinoblastoma. East Afr Med J 1978; 55: 314- 9. Abramson DH, Ellsworth RM, Grum- bach N, Kitchin FD. Retinoblastoma: survival, age at detection and compa- rison 1914-1958,1958-1983. J Pediatr Ophthalmol Strabismus 1985; 22: ,246- 50. Knudson AG. Mutation and cancer: statistical study of retinoblastoma. Proc Natl Acad Sci IJSA 1971; 68: 820- 3. Gallie BL, Dunn JM, Hamel PA, Mun- caster M, et al. How do retinoblastoma tumors form? Eye 199.2; 6: 226-31. Koene Koop RK. Molecular genetics in ophthalmology: the management of retinoblastoma. Ophthalmic Practice
Yandell DW, Campbell TA, Dayton SH, Petersen R, et al. Oncogenic point mutations in the human retinoblasto- ma gene: their application to genetic counselling. New Engl J Mcd 1989; 321(25): 1689-94. Pieroni D, Lashmet MH, Helveston EM. Retinoblastoma. J Pediatr Oph- thalmol Strabismus 1969; 4: 182. Carbajal UM. Observations on retino- blastoma. Am J Ophthalmol 1958; 45:
Schappert-Kimmijser J, Hemmes GD, Nijland R. The heredity of retinoblas- toma. Ophthalmologica 1966; 151: 147- 213. Abramson DM. Retinoblastoma: dia-
1994; 17.: 160-4
391 - 402.
39
40
41
42
43
44
45
46
47
48
49
50
gnosis and management. CA Cancer J Clin 1982; 32: 130-40. Franqois J, Matton MT, De Bei S, et al. Genesis and genetics of retinoblasto- ma. Ophthalmologica 1975; 5: 405-25. Der Kinderen DJ, Koten J W, Tan KEWP, Beemer FA, et al. Parental age in sporadic hereditary retinoblastoma. Am J Ophthalmol 1990; 110: 605-9. Pellii C, Briard ML, Feingold J, Frizal J. Parental age in retinoblastoma. Human Genet 1973; 20(1): 59-62. Matsunaga E. Hereditary retinoblasto- ma: lack of maternal effect. Human Genet 1982; 62(2): 124-8. DryjaTP, Mukai S, Petersen R, Rapa- port JM, et al. Parental origin of muta- tions of the retinoblastoma gene. Nature 1989; 339: 556-8. Zhu X, Dunn JM, Phillips RA, God- dard AD, et al. Preferential germline mutation of the paternal allele in reti- noblastorna. Nature 1989; 340: 312-3. Leach RJ, Magewu AN, Buckley JD, Benedict WF, et al. Preferential reten- tion of paternal alleles in human reti- noblastoma: evidence for genomic im- printing. Cell Growth Differ 1990; I@): 401- 6. Senft SH, Moll AC, Dabas KH, Beze- mer PZ, et al. Influence of paternal age on the incidence of retinoblastoma. Proceedings of the VI International Ketinoblastoma Society, Joint Sympo- sium 1994 June 22 - 25; Niagara-On- The-Lake (ON), Canada. 1994: 16. Bedford MA, Bedotto C, Macfaul PA. Retinoblastoma, a study of 139 cases. Br J Ophthalmol 1971; 55: 19- 27. Mahoney MC, Burnett WS, Majerovics A, Tanenbaum H. The epidemiology of ophthalmic malignancies in New York State. Ophthalmology 1990; 97: 1143-7. Herm RJ, Heath P. A study of retino- blastoma. Am J Ophthalmol 1956; 4: 22-30. Jay JL, Devlin ML. The increasing fre- quency of surgery for cataract. Eye 1990; 4: r27-31.
46 Paul B. Mullaney et al.
Oph
thal
mic
Epi
dem
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B H
eide
lber
g on
11/
14/1
4Fo
r pe
rson
al u
se o
nly.