Embed Size (px)
Citation preview

53
RETROPERITONEAL LYMPH
NODE DISSECTION 5TRANSABDOMINAL APPROACH
The transabdominal midline in-cision with complete bowel mobi-lization provides one of the bestsurgical exposures for retroperito-neal lymphadenectomy.
FIG. 5-1. The incision extendsfrom the xiphoid process to 6 cmbelow the umbilicus.
FIGS. 5-2 AND 5-3. For both left- andright-sided tumors, a right-sided,
posterior parietal peritoneal inci-sion extends from the foramen ofWinslow, around the cecum, andup the mesenteric root to the liga-ment of Treitz.
If there is bulky disease, it iscritical to make the incision intothe foramen of Winslow and to di-vide the ligament of Treitz itself.Small vessels within the ligamentneed to be coagulated.1
5-1
5-2
5-3
Umbilicus
Kidney
Duodenum
Inferiormesenteric vein
Incision of parietal peritoneum
Ascendingcolon
Gallbladder
Liver
Colon
Duodenum
Kidney
Hepatoduodenalligament
(portal triad)
Parietal peritonealincision extending
into foramenof Winslow

54 Critical Operative Maneuvers in Urologic Surgery
FIGS. 5-4 AND 5-5. The inferior mes-enteric vein drains part of the lefttransverse colon, the descendingcolon, and the rectum. The infe-rior mesenteric vein can vary in itslocation and may join the splenicvein laterally or medially or eventhe superior mesenteric vein di-rectly. The superior mesentericvein drains the ascending colonand right transverse colon. Whenbulky disease compresses thevena cava, this inferior mesentericvein can become quite large. Thisvessel may be under tension afterthe bowel is mobilized. Depend-ing on the location and size of theinferior mesenteric vein, we gen-erally divide it to gain furtherexposure.
FIG. 5-6. The Kocher maneuverfrees the duodenum, exposing theright kidney and part of the venacava (see pp. 11-12).
The right colon, part of thetransverse colon, and the smallbowel are packed with a laparot-omy pad into a bowel bag andplaced over the chest wall. The lap-arotomy pad prevents the bowelfrom slipping out.
FIG. 5-7. Anterior to the superiormesenteric artery, pancreas, andrenal pedicles, there are bands ofsmall lymphatic tributaries thatmust be divided to gain theproper exposure.
FIG. 5-8. Part of the body of thepancreas is now reflected cepha-lad with the superior mesentericartery and the duodenum. Whenthe Harrington retractor blade isplaced over the region of the re-flected pancreas, the assistantshould be aware that excessivecompression causes pancreaticcontusions.
Duodenum
Ligament of Treitz
Incisedparietal peritoneum
Possible positions ofinferior mesenteric vein
321
5-4
5-5
5-6
Portalvein
Portalvein
Portalvein
Splenicvein
Splenicvein
Splenicvein
Superiormesenteric
vein
Superiormesenteric
vein
Superiormesenteric
vein
Inferiormesenteric
vein
Inferiormesenteric
veinInferior
mesentericvein
Variations in Anatomy of Inferior Mesenteric Vein
A B C
Pancreas
Superiormesenteric
artery
Venacava
Duodenum
Kocher Maneuver

Chapter 5 Retroperitoneal Lymph Node Dissection 55
LYMPHADENECTOMY
FIG. 5-9. We prefer to use the tem-plate method of lymphadenec-tomy for emission preservation2
rather than a specific nerve-spar-ing dissection.3,4 There is 95%chance of preservation of emis-sion by the template method.
The templates shown here forright-sided and left-sided lymphnode dissection represent a com-plete bilateral dissection above thelevel of the inferior mesentericartery and a unilateral dissectionbelow the inferior mesentericartery. On the right side, the dis-section is carried along the rightrenal hilar area to the level of theright ureter and down to wherethe ureter crosses the common il-iac artery. The ipsilateral gonadalvessels are removed to the level ofthe deep inguinal ring and thepreviously ligated stump of thespermatic cord. For left-sided dis-section, the template is similar,with the exception of the right lat-eral margin. Since nodal spreadtends to occur from right to left,dissection is carried only to thelateral margin of the inferior venacava rather than all the way to theright ureter.
5-7
5-8
Vena cava Aorta
Incisedparietalperitoneum
Lymphnode
Rightkidney Ligated and
divided inferiormesenteric vein
Lymphatic channels
Pancreas
Lymphnode
Gonadalvein
Venacava Aorta
Superior mesenteric artery
Renal veinand artery
Inferiormesentericartery
Duodenumreflected
cephalad
Modified template for right-sidedretroperitoneal lymph node dissection
5-9
From Richie JP: Modified retroperitoneallymphadenectomy for patients with clinical stage Itesticular cancer. In Lepor H, Ratliff TL, editors:Urologic oncology, ed 3, Boston, 1989, Kluwer.
Modified template for left-sidedretroperitoneal lymph node dissection
B
A
56 Critical Operative Maneuvers in Urologic Surgery
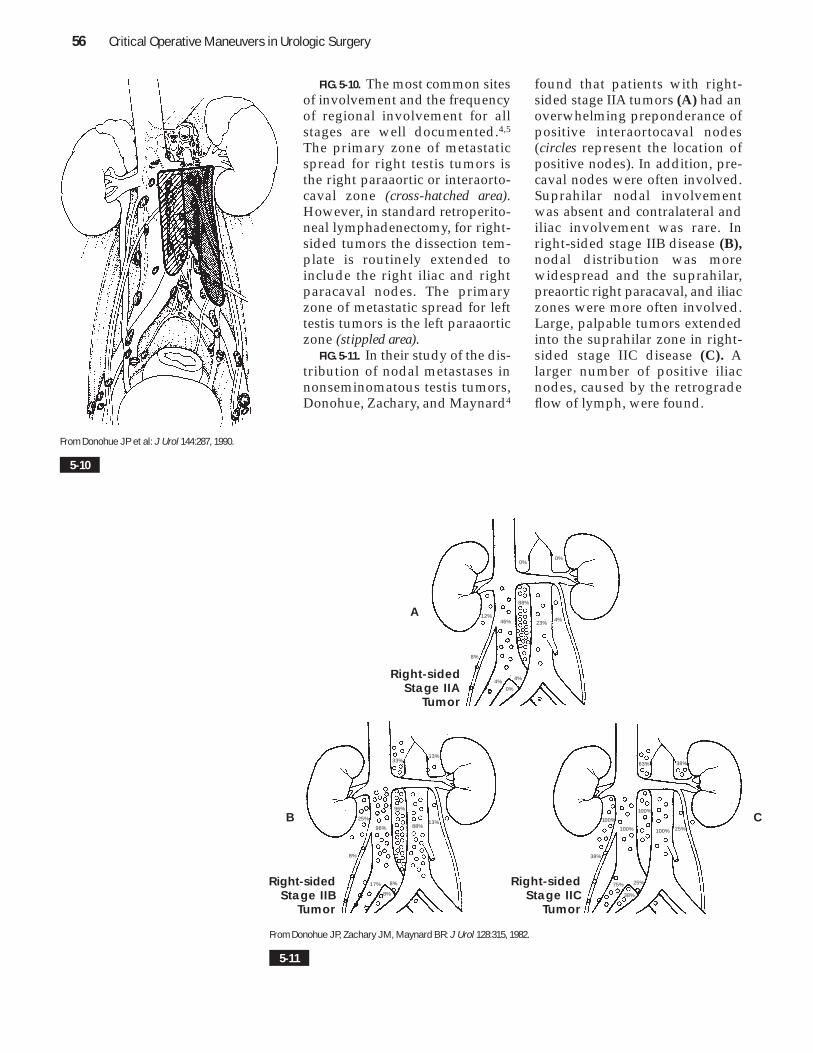
FIG. 5-10. The most common sitesof involvement and the frequencyof regional involvement for allstages are well documented.4,5
The primary zone of metastaticspread for right testis tumors isthe right paraaortic or interaorto-caval zone (cross-hatched area).However, in standard retroperito-neal lymphadenectomy, for right-sided tumors the dissection tem-plate is routinely extended toinclude the right iliac and rightparacaval nodes. The primaryzone of metastatic spread for lefttestis tumors is the left paraaorticzone (stippled area).
FIG. 5-11. In their study of the dis-tribution of nodal metastases innonseminomatous testis tumors,Donohue, Zachary, and Maynard4
found that patients with right-sided stage IIA tumors (A) had anoverwhelming preponderance ofpositive interaortocaval nodes(circles represent the location ofpositive nodes). In addition, pre-caval nodes were often involved.Suprahilar nodal involvementwas absent and contralateral andiliac involvement was rare. Inright-sided stage IIB disease (B),nodal distribution was morewidespread and the suprahilar,preaortic right paracaval, and iliaczones were more often involved.Large, palpable tumors extendedinto the suprahilar zone in right-sided stage IIC disease (C). Alarger number of positive iliacnodes, caused by the retrogradeflow of lymph, were found.
5-10
From Donohue JP et al: J Urol 144:287, 1990.
5-11
From Donohue JP, Zachary JM, Maynard BR: J Urol 128:315, 1982.
Right-sidedStage IIA
Tumor
12%
0%0%
88%
23% 4%
8%
4%0%
4%
46%
Right-sidedStage IIB
Tumor
13%33%
96%
13%88%96%
25%
8%
17% 8%
8%
Right-sidedStage IIC
Tumor
100%100%
100%
63% 38%
25%
75% 25%
38%
38%
100%
A
B C

Chapter 5 Retroperitoneal Lymph Node Dissection 57
FIG. 5-12. In left-sided stage IIAdisease, the left paraaortic zonebelow the renal vein and thepreaortic zone were most com-monly involved (A). Contralateralcaval, paracaval, and iliac in-volvement was absent. In a fewcases, the suprahilar nodes wereinvolved but they were paraaorticand located just above the level ofthe renal arteries. Left-sided stageIIB tumors spread into the in-teraortocaval, precaval, and su-prahilar zones (B), whereas left-sided stage IIC palpable massesinvolved the suprahilar zones bydirect extension of the tumor mass(C). In addition, in stage IIC dis-ease, the iliac zones and precavalzones were often involved due tothe tumor size.
FIG. 5-13. Division of the retro-peritoneum into zones is usefulfor orientation and sequential dis-section. We prefer to send multi-ple specimens placed on a sche-matic diagram (as shown) forpathologic evaluation.
A large marking stitch (0 silk) isplaced above the inferior mesen-teric artery because this site is theinferior midline landmark. Beforeany dissection distorts the anat-omy, marking stitches are placedto define template borders.
5-12
From Donohue JP, Zachary JM, Maynard BR: J Urol 128:315, 1982.
5-13
Left-sidedStage IIA
Tumor
7% 14%
29%
0%
0%
71%79%
14%
14%0%
0%
Left-sidedStage IIB
Tumor
100%
95%
11%
84%
42%16%
5%
47%
32%5%
0%
Left-sidedStage IIC
Tumor
100%
33%
67%
11%11%
56%
0%
89%
67% 100%
100%
4 32
Zones for Template Tissue Parcels
1
56
Lower marginfor nerve-sparingprocedures
Inferiormesentericartery
Kidney
AortaVena cava
A
B C

58 Critical Operative Maneuvers in Urologic Surgery
FIG. 5-14. The split-and-roll ma-neuver first described by Dono-hue5 is the simplest approach fornode dissection. After tissues aresplit anteriorly over the vena cavaand aorta, the surgeon sweeps thegreat vessels away from adjacentfatty tissue and lymph nodes.
This maneuver is easiest if trac-tion is applied with Singley for-ceps to hold the nodes laterallywhile the surgeon uses Kitner dis-sectors (tonsil clamp with ball ofgauze clamped at tip) to push thevessels medially.
FIG. 5-15. With a thin layer of drysponge between the surgeon’s fin-ger and the blood vessel, the sur-geon gently rolls the vessel medi-ally. The lateral lumbar vessels arethus easily exposed at the base.
In general, the three pairs oflumbar vessels below the renalpedicle can be divided withoutcomplication since most of the pa-tients are young, healthy men.The surgeon should avoid ligatingany lumbar arteries at or abovethe level of the renal pedicle toavoid the unusual but real com-plication of damage to the spinalcord.6,7
VENOUS HEMORRHAGE
FIG. 5-16. During the dissection,inadvertent tears of the lumbar
veins are common. Under directvision, the surgeon uses an Allisclamp to grasp the torn lumbarvein before it recedes into the softtissues.8
FIG. 5-17. If a sudden tear of thevena cava occurs when it is nearlyskeletonized, the surgeon can usea three-finger maneuver to arrestthe bleeding. The index and mid-dle fingers lift and compress thevessel while the thumb can moveback and forth in preparation forthe closure with a double-armstitch (4-0 Prolene) for two rows ofstitches.
FIG. 5-18. If there is an early tearof the vena cava before the vesselis skeletonized, the surgeon canuse two sponge sticks to compressthe vena cava above and belowthe injury after the vena cava isfreed from the aorta. Once theblood has been evacuated withlaparotomy pads, the surgeon canrepair the laceration. An Allisclamp is placed at each end of thelaceration and the surgeon uses arunning stitch (4-0 Prolene) toclose the defect.9
The placement of vessel loopsaround the vena cava above andbelow the injury is also helpful. Itshould be remembered that thevena cava has friable walls, whichare easily torn, particularly at thepoints where tributaries enter.
Split-and-Roll Maneuver(Cross-sectional View)
Lymph nodes
Vena cava
Lumbar vein
Venacava Vena
cava
Aorta Aorta
Aorta
Lumbar artery
5-14
5-15
Lumbar vessel
Rolling mainvessel to isolatelumbar vessel

Chapter 5 Retroperitoneal Lymph Node Dissection 59
5-18
From Hinman F Jr: Atlas of urologic surgery, Philadelphia, 1989, WB Saunders.
5-16
5-17
Lumbarvein orartery
Allis clamp
Three-Finger Compressionof Vena Cava

60 Critical Operative Maneuvers in Urologic Surgery
5-19
From Skinner DG: J Urol 117:605, 1977.
Superiormesentericartery
TumorTumor
Inferiormesentericartery
Bowelbag
Tumor
Tumor
Descendingcolon
Left kidney
A B
DC
Chapter 5 Retroperitoneal Lymph Node Dissection 61
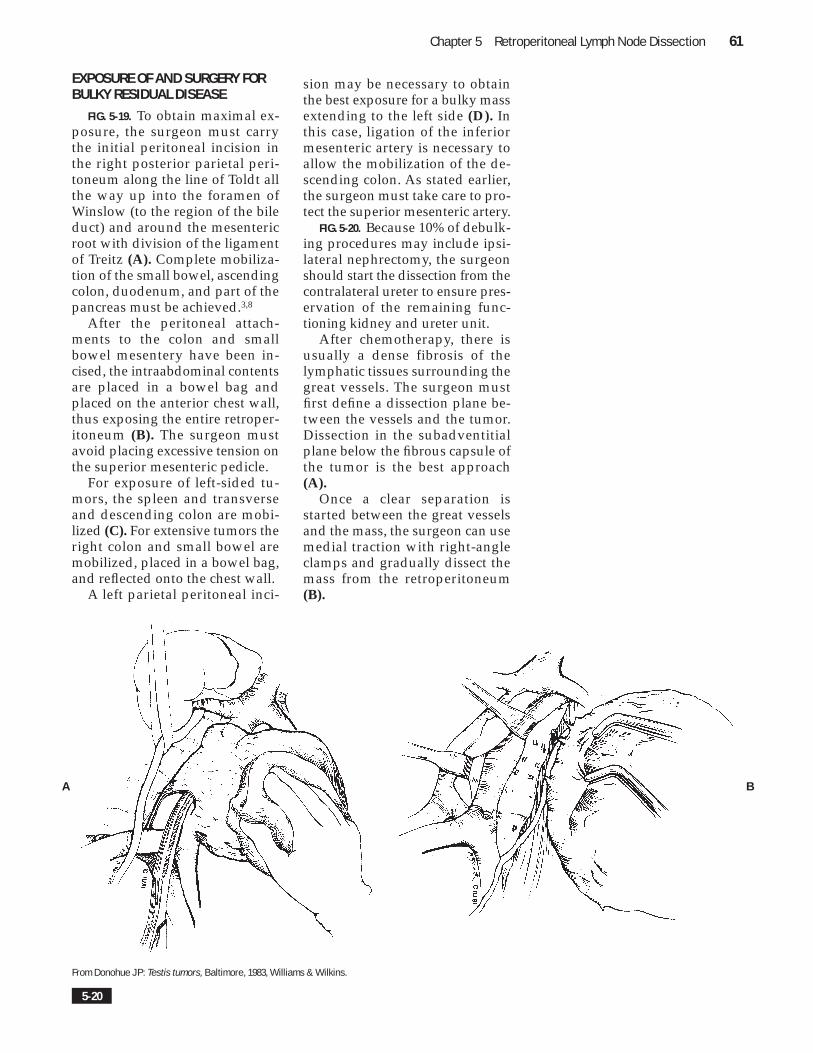
EXPOSURE OF AND SURGERY FORBULKY RESIDUAL DISEASE
FIG. 5-19. To obtain maximal ex-posure, the surgeon must carrythe initial peritoneal incision inthe right posterior parietal peri-toneum along the line of Toldt allthe way up into the foramen ofWinslow (to the region of the bileduct) and around the mesentericroot with division of the ligamentof Treitz (A). Complete mobiliza-tion of the small bowel, ascendingcolon, duodenum, and part of thepancreas must be achieved.3,8
After the peritoneal attach-ments to the colon and smallbowel mesentery have been in-cised, the intraabdominal contentsare placed in a bowel bag andplaced on the anterior chest wall,thus exposing the entire retroper-itoneum (B). The surgeon mustavoid placing excessive tension onthe superior mesenteric pedicle.
For exposure of left-sided tu-mors, the spleen and transverseand descending colon are mobi-lized (C). For extensive tumors theright colon and small bowel aremobilized, placed in a bowel bag,and reflected onto the chest wall.
A left parietal peritoneal inci-
sion may be necessary to obtainthe best exposure for a bulky massextending to the left side (D). Inthis case, ligation of the inferiormesenteric artery is necessary toallow the mobilization of the de-scending colon. As stated earlier,the surgeon must take care to pro-tect the superior mesenteric artery.
FIG. 5-20. Because 10% of debulk-ing procedures may include ipsi-lateral nephrectomy, the surgeonshould start the dissection from thecontralateral ureter to ensure pres-ervation of the remaining func-tioning kidney and ureter unit.
After chemotherapy, there isusually a dense fibrosis of thelymphatic tissues surrounding thegreat vessels. The surgeon mustfirst define a dissection plane be-tween the vessels and the tumor.Dissection in the subadventitialplane below the fibrous capsule ofthe tumor is the best approach(A).
Once a clear separation isstarted between the great vesselsand the mass, the surgeon can usemedial traction with right-angleclamps and gradually dissect themass from the retroperitoneum(B).
5-20
From Donohue JP: Testis tumors, Baltimore, 1983, Williams & Wilkins.
A B

62 Critical Operative Maneuvers in Urologic Surgery
SUPRAHILAR NODAL DISEASE
If suprahilar nodal involve-ment is anticipated from preop-erative radiologic studies, the sur-geon should be prepared to ex-tend the midline incision and cre-ate a thoracoabdominal incision.In addition, the patient should bepositioned at a 45-degree angle atthe chest level as for a thoracoab-dominal radical nephrectomy toobtain the best exposure of thehigh retroperitoneum with mobi-lization of the liver (see pp. 2-3).
FIGS. 5-21 AND 5-22. In general,nodal involvement occurs behind
the crus of the diaphragm andabove. The crura can easily be pal-pated as two leaves on either sideof the aorta and can be divided forimproved exposure.5,10 This ma-neuver is blind, guided by onlythe surgeon’s finger palpation ofthe diaphragmatic crus.
To learn this maneuver, theurologist should assist a thoracicsurgeon with cases involving aor-tic aneurysm repair.
Residual higher masses shouldbe approached directly from abovein the pleural cavity.
Diaphragmaticcrus
Finger placementon either side
before division
Celiac trunk
Superior mesentericartery
Renal artery
Aorta
Diaphragm
Diaphragmaticcrus
Aorta
Celiac trunk
Superior mesentericartery
5-21
5-22

Chapter 5 Retroperitoneal Lymph Node Dissection 63
� An incision is made lateral to theright colon extending from theforamen of Winslow, around thececum, and up the mesentericroot to the ligament of Treitz.
� The inferior mesenteric vein isdivided.
� The bowel is packed into a bowelbag and is reflected cephalad onthe chest.
� With the pancreas reflected ceph-alad, the superior mesentericartery is located by palpationand the Harrington retractor isplaced over the region of the re-flected pancreas.
� For a template nerve-sparingprocedure, a large marking stitchis placed over the inferior mesen-teric artery and other markingstitches are inserted to definetemplate borders.
� The split-and-roll maneuver isperformed.
� A multiple specimen analysis onthe schematic diagram is pre-pared.
� Diaphragmatic crus division isperformed for suprahilar nodedissection.
� Bulky disease dissection is per-formed with preservation of thefunctioning contralateral renalunit.
� Poor exposure: Check the incisionto the foramen of Winslow andaround to the ligament of Treitz→ divide the ligament of Treitz→ divide the inferior mesentericvein
� Vena cava tear: Use a three-fingermaneuver → apply compressionwith sponge sticks above and be-low the tear → control the vesselabove and below the tear withvessel loops → perform double-arm stitch (Prolene 4-0) for clo-sure
� Injury of inferior mesenteric artery:Proceed with surgery
� Injury of lumbar artery above renalpedicle unilaterally: Preserve theother side and all other lumbararteries above the pedicles
� Difficult lymphadenopathy in supra-hilar area: Divide diaphragmaticcrura bilaterally
� Area at inferior margin near inferiormesenteric artery shows positivebiopsy: Perform a full-node dis-section and disregard the nerve-sparing template
P O T E N T I A LP R O B L E M S
K E YP O I N T S

64 Critical Operative Maneuvers in Urologic Surgery
REFERENCES11 Edwards EA et al: The duodenum,
pancreas, and spleen. In EdwardsEA, Malone PD, MacArthur JD, edi-tors: Operative anatomy of the abdomenand pelvis, ed 9, Philadelphia, 1975,Lea & Febiger, pp 37-44.
12 Richie JP: Modified retroperitoneallymphadenectomy for patients withclinical stage I testicular cancer. InLepor H, Ratliff TL, editors: Urologiconcology, ed 3, Boston, 1989, Kluwer,pp 36-53.
13 Donohue JP: Testis tumors. In Lib-ertino JA, editor: International per-spectives in urology, Baltimore, 1983,Williams & Wilkins.
14 Donohue JP, Zachary JM, MaynardBR: Distribution of nodal metastasesin nonseminomatous testis cancer, JUrol 128:315, 1982.
15 Donohue JP: Nerve-sparing tech-niques in urological surgery. Post-graduate course 23, American Uro-logical Association Meeting, 1991.
16 Ferguson LR et al: Spinal ischemiafollowing abdominal aortic surgery,Ann Surg 181:267, 1975.
17 Kaswick JA, Bloomberg SD, SkinnerDG: Radical retroperitoneal nodedissection: how effective is removalof all retroperitoneal nodes? J Urol115:70, 1976.
18 Skinner DG: Considerations formanagement of large retroperitonealtumors: use of the modified thora-coabdominal approach, J Urol 117:605, 1977.
19 Hinman F Jr: Atlas of urologicsurgery, Philadelphia, 1989, WBSaunders.
10 Stoney RJ, Effeney DJ: Thoracoab-dominal aorta and its branches. InStoney RJ, Effeney DJ, editors:Wylie’s atlas of vascular surgery,Philadelphia, 1992, JB Lippincott.
SUGGESTED READINGSDonohue JP et al: Nerve-sparing retro-
peritoneal lymphadenectomy withpreservation of ejaculation, J Urol144:287, 1990.
Jewett MAS et al: Retroperitoneal lym-phadenectomy for testis tumor withnerve-sparing for ejaculation, J Urol139:1220, 1988.
Lange PH et al: Return of fertility aftertreatment for nonseminomatous tes-ticular cancer: changing concepts, JUrol 129:1131, 1983.
Skinner DG: Technique of nephroure-terectomy with regional lymph nodedissection, Urol Clin North Am 5(1):253, 1978.
![Yu Yu Hakusho Yu Hakusho [multi]/Yu-Yu...sua doutrina secreta. Para tanto a mestra criou um torneio de artes marciais para quem quisesse participar. Ao vencedor seria dada a honra](https://img.pdfslide.net/doc/110x75/60c6bec3b5c6ab42591d3057/yu-yu-hakusho-yu-hakusho-multiyu-yu-sua-doutrina-secreta-para-tanto-a-mestra.jpg)