Embed Size (px)
Citation preview

Hindawi Publishing CorporationStroke Research and TreatmentVolume 2013, Article ID 263974, 42 pageshttp://dx.doi.org/10.1155/2013/263974
Review ArticleClinical Trials in Cardiac Arrest and Subarachnoid Hemorrhage:Lessons from the Past and Ideas for the Future
Jennifer A. Frontera
Cleveland Clinic Foundation, Neurological Institute, Cerebrovascular Center, Cleveland Clinic, 9500 Euclid Avenue S80, Cleveland,OH 44195, USA
Correspondence should be addressed to Jennifer A. Frontera; [email protected]
Received 17 December 2012; Accepted 29 January 2013
Academic Editor: R. Loch Macdonald
Copyright © 2013 Jennifer A. Frontera.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction. Elevated intracranial pressure that occurs at the time of cerebral aneurysm rupture can lead to inadequate cerebralblood flow, which may mimic the brain injury cascade that occurs after cardiac arrest. Insights from clinical trials in cardiac arrestmay provide direction for future early brain injury research after subarachnoid hemorrhage (SAH).Methods. A search of PubMedfrom 1980 to 2012 and clinicaltrials.gov was conducted to identify published and ongoing randomized clinical trials in aneurysmalSAH and cardiac arrest patients. Only English, adult, human studies with primary or secondarymortality or neurological outcomeswere included. Results. A total of 142 trials (82 SAH, 60 cardiac arrest) met the review criteria (103 published, 39 ongoing). Themajority of both published and ongoing SAH trials focus on delayed secondary insults after SAH (70%), while 100% of cardiac arresttrials tested interventionswithin the first few hours of ictus. No SAH trials addressing treatment of early brain injurywere identified.Twenty-nine percent of SAH and 13% of cardiac arrest trials showed outcome benefit, though there is no overlap mechanistically.Conclusions. Clinical trials in SAH assessing acute brain injury are warranted and successful interventions identified by the cardiacarrest literature may be reasonable targets of the study.
1. Introduction
For decades, research efforts in subarachnoid hemorrhage(SAH) have focused on vasospasm and delayed ischemicneurological deficits. However, brain injury at the time ofaneurysm rupture is a significant predictor of functionaloutcome. Indeed, poor admission neurological status (Hunt-Hess or World Federation of Neurological Surgeons Score),which reflects acute brain injury, is a larger contributor todeath or severe disability than delayed cerebral ischemia[1, 2]. However, the mechanism of early brain injury afteraneurysm rupture remains elusive and no current therapiesare available.
One possible mechanism of acute injury was describedin a small case series of 6 patients with observed recurrentaneurysm rupture either during transcranial Doppler (TCD)or during craniotomy with open skull but intact dura. Theinvestigators report a spike in intracranial pressure (ICP) thatdeveloped over 1 minute and then declined over several min-utes.This abrupt increase in ICP approached levels nearmeanarterial pressure and led to a concomitant drop in cerebral
blood flow resulting in circulatory arrest, as documented byTCD [61]. This study examined aneurysm rebleeding anddoes not provide direct evidence that intracranial circulatoryarrest occurs with de novo aneurysm rupture. However, inad-equate cerebral blood flow is frequently evidenced clinicallyby the transient loss of consciousness that occurs at SAHictus. This mechanism of global transient circulatory arresthas been described in animal models of SAH at the time ofinitial hemorrhage [62, 63] and mimics the anoxic/hypoxicischemic mechanism incurred by cardiac arrest.
In this paper, published and ongoing clinical trials incardiac arrest are compared to those in aneurysmal SAHto identify overlapping or complementary approaches totreatment as well as new avenues for potential research.
2. Methods
A search of PubMed was conducted in 11/2012 to identifyrandomized, controlled trials of aneurysmal SAH and cardiacarrest. Only human studies of adults (≥18 years of age), which

2 Stroke Research and Treatment
Table1:Ra
ndom
ized
controlledtrialsassessingneurologicou
tcom
esaft
eraneursym
alSubarachno
idhemorrhage—
completed
trials.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Calcium
channelblockers—
nimod
ipine
CerebralA
rterialSpasm
—a
controlledTrialof
Nim
odipineinPatie
ntsw
ithSubarachno
idHem
orrhage
Rand
omized,
placebo-controlled,
doub
le-blin
d,multic
enter
prospectives
tudy
ofHun
tHessg
rade
I-IISA
Hpatie
nts
Nim
odipine
0.7m
g/kg
PObo
lus,
then
0.35
mg/kg
q4×
21days.Starting
with
in96
hof
SAH
(𝑁=58)
Placebo
(𝑁=63)
Prim
aryou
tcom
e:neurologicaldeficitfro
marteria
lspasm
andseverity
ofneurologicdeficitat21
days
Nim
odipines
ignificantly
redu
ceddeathor
severe
deficits
from
spasm
at21
days
(2%versus
13%with
placebo,
𝑃=0.03)
Allenetal.,NEJM
1983
[3]
Nim
odipinetreatmentin
poor-grade
aneurysm
patie
nts.Re
sults
ofa
multicenterd
ouble-blind
placebo-controlledtrial
Rand
omized,m
ultic
enter,
doub
le-blin
d,placebo-controlledtrial
Nim
odipine9
0mg
POq4h×21d
(𝑁=91)
Placebo
(𝑁=97)
Prim
aryou
tcom
e:3-mon
thGOS
Second
aryou
tcom
es:
delay
edisc
hemicdeficits,
angiograph
icvasospasm
Bette
r3-m
onth
GOSin
treatmentg
roup
(29%
versus
9%of
treatmentg
roup
,𝑃<0.001).Sign
ificantlyless
delay
edcerebralisc
hemiain
treatmentg
roup
,nodifference
inangiograph
icvasospasm
Petruk
etal.,J
Neurosurg
1988
[4]
Con
trolledstu
dyof
nimod
ipineinaneurysm
patie
ntstreated
early
after
subarachno
idhemorrhage
Rand
omized,dou
ble-blind,
placebo-controlledtrialofall
Hun
t-Hessg
radesw
ithin
96ho
urso
fSAH
Nim
odipine6
0mgq
4hPO×21
days
+Nim
odipine2
00mcg
IVintraoperativ
elyinto
basalcistern
(𝑁=38)
Placebo
(𝑁=37)
Prim
aryou
tcom
e:mortality,cerebralbloo
dflo
wmeasuredby
Xeno
nCT
Second
aryou
tcom
es:
3-mon
thintellectualor
neurologicaldeficit
Mortalitywas
lower
inthe
nimod
ipineg
roup
(4%versus
24%with
placebo,𝑃<0.05).
Nim
odipined
idno
tsig
nificantly
increase
cerebral
bloo
dflo
w
Mee
etal.,
Neurosurgery1988
[5]
Effecto
foraln
imod
ipineo
ncerebralinfarctio
nand
outcom
eafte
rsub
arachn
oid
hemorrhage:British
aneurysm
nimod
ipinetria
l
Rand
omized,dou
ble-blind,
placebo-controlled,
multic
entertria
lwith
in96
hof
SAH
Nim
odipine6
0mgq
4PO×21d(𝑁=276)
Placebo
(𝑁=278)
Prim
aryou
tcom
e:3-mon
thcerebralinfarctio
nSecond
aryou
tcom
e:3-mon
thGOS
Sign
ificantlylesscerebral
infarctio
nin
then
imod
ipine
grou
p(22%
comparedto
33%
inplacebo,𝑃=0.014).Po
orGOSou
tcom
essig
nificantly
redu
cedin
nimod
ipineg
roup
at3-mon
ths
Pickardetal.,BM
J1989
[6]
Early
aneurysm
surgeryand
preventiv
eTherapywith
intravenou
slyadministered
nimod
ipine:Amultic
enter,
doub
le-blin
d,do
se-com
paris
onstu
dy
Rand
omized,dou
ble-blind,
dose-com
paris
on,m
ultic
enter
study
Nim
odipine2
mg/h
IVfor9
–15days
(𝑁=101)
Nim
odipine
3mg/hIV
for
9–15
days
(𝑁=103)
Prim
aryou
tcom
e:delayed
neurologicaldeficits,
adversed
rugreactio
ns
Nodifferenceindelay
edneurologicaldeficits
between
thetwogrou
ps
Gilsbach
etal.,
Neurosurgery1990
[7]

Stroke Research and Treatment 3
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Long
-term
effectsof
nimod
ipineo
ncerebral
infarctsandou
tcom
eafte
raneurysm
alsubarachno
idhemorrhagea
ndsurgery
Rand
omized,dou
ble-blind,
placebo-controlledof
Hun
t-HessI–IIISA
Hpatie
nts
Nim
odipineIV
0.5m
cg/kg/min×
7–10
days
follo
wed
by60
mgq
4hPO×21
days
total
(𝑁=104)
Placebo
(𝑁=109)
Prim
aryou
tcom
e:delayed
ischemicdeterio
ratio
nand
CTinfarcts
Second
aryou
tcom
es:G
OS
at1–3years
Sign
ificantlyfewer
deaths
caused
bydelay
edcerebral
ischemiain
nimod
ipineg
roup
(𝑃=0.01)a
ndfewer
cerebral
infarctson
CT(𝑃=0.05).No
differences
in1–3year
GOSor
CTscan
Ohm
anetal.,J
Neurosurg
1991
[8]
Arand
omized
outcom
estudy
ofenteralversusintraveno
usnimod
ipinein171p
atients
after
acutea
neurysmal
subarachno
idhemorrhage
Rand
omized,single-center
study
Nim
odipine2
mg/h
IV×10
days
then
changedto
PO×6d
(𝑁=87)
Nim
odipine
60mgPO
q4×
16days
(𝑁=84)
Prim
aryou
tcom
e:delayed
ischemicneurological
deficit
Second
aryou
tcom
es:12
mon
thGOS,mRS
,Ka
rnofsky,MRI
infarcts,
HRQ
oL
Nodifferenceindelay
edisc
hemicneurologicaldeficits
(20%
inenteralversus16%
inIV
grou
p,𝑃=0.61),no
differencein12-m
onth
clinical
outcom
es
Sopp
ietal.,World
Neurosurgery2012
[9]
Calcium
channelblockers—
nicardipine
Arand
omized
controlledtrial
ofhigh
-doseintraveno
usnicardipineinaneurysm
alsubarachno
idhemorrhage.A
repo
rtof
thec
ooperativ
eaneurysm
study
Rand
omized,dou
ble-blind,
placebo-controlled,
multic
enterstudy
Nicardipine
IV0.15mg/kg/h
(𝑁=449)
Placebo
(𝑁=457)
Prim
aryou
tcom
e:3-mon
thGOS
Second
aryou
tcom
es:
angiograph
icvasospasm,
TCDvasospasm,m
ortality,
disabilityfro
mvasospasm,
symptom
aticvasospasm,
CTinfarctio
n,NIH
SS
Nodifferencein3-mon
thGOS.Lesssymptom
atic
vasospasm
intre
atmentg
roup
(32%
versus
46%in
placebo
grou
p,P<0.001)andles
sangiograph
icvasospasm
intre
atmentg
roup
(33%
versus
51%of
placebo,P<0.01)a
ndlessTC
Dvasospasm
(23%
versus
49%of
placebo,P<
0.001)
Haley
etal.,J
Neurosurg
1993
[10,11]
Arand
omized
trialoftwo
doseso
fnicardipine
inaneurysm
alsubarachno
idhemorrhage.Arepo
rtof
the
coop
erativea
neurysm
study
Rand
omized,dou
ble-blind,
multic
enterstudy
Nicardipine
IV0.15mg/kg/h×14
days
(N=184)
Nicardipine
IV0.075m
g/kg/h×
14days
(N=181)
Prim
aryou
tcom
e:symptom
aticvasospasm,
adversed
rugevents
Second
aryou
tcom
es:
3-mon
thGOSandNIH
SS,
mortality,disabilitydu
eto
vasospasm,C
Tinfarctio
n
Nodifferenceinsymptom
atic
vasospasm
or3-mon
thou
tcom
e.Morea
dverse
effects
inhigh
-dosen
icardipine
grou
p
Haley
etal.,J
Neurosurg
1994
[12]
Effecto
fnicardipine
prolon
ged-releaseimplantson
cerebralvasospasm
and
clinicaloutcomea
ftersevere
aneurysm
alsubarachno
idhemorrhage.Aprospective,
rand
omized,dou
ble-blind
phaseIIaStud
y
Rand
omized,prospectiv
edo
uble-
blindph
aseIIastu
dyin
clipp
edSA
Hpatie
nts
Nicardipine
prolon
ged-release
implants(10×4m
gprolon
gedreleaser
odshaped
polymers)
placed
inbasal
ciste
rns
(N=16)
Con
trol-b
asal
ciste
rnso
pened
andwashedou
t(N
=16)
Prim
aryou
tcom
e:angiograph
icvasospasm
Second
aryou
tcom
e:delay
edisc
hemiclesio
non
HCT
,1-yearm
RSand
NIH
SS
Ang
iographicv
asospasm
significantly
redu
cedin
treatmentg
roup
(7%versus
73%in
controls,
P<0.05).No
significantd
ifference
inCT
infarct.Decreased
mortalityin
treatmentg
roup
(6%versus
38%in
controlgroup
,P=
0.04
2)andbette
r1-yearm
RSandNIH
SS(P
=0.00
01)
Barthetal.,Stroke
2007
[13]

4 Stroke Research and Treatment
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Antifibrinolytics
Antifibrinolysiswith
tranexam
icacid
inaneurysm
alsubarachno
idhemorrhage:Aconsecutive
controlledclinicaltria
l
Rand
omized,
placebo-controlled,stu
dy
Tranexam
icacid
1gq
4hIV×1w
eekthen
1gq6h
IV×1w
eek
then
1.5gq6h
PO×1
week
(N=30)
Placebo
(N=29)
Prim
aryou
tcom
e:recurrenth
emorrhage
diagno
sedby
LP,H
CT,
echo
enceph
alogram
orautopsy.
Second
aryou
tcom
e:angiograph
icvasospasm,
delay
edcerebralisc
hemia,
death
Tranexam
icacid
protected
againstrebleedingdu
ringthe
first2weeks
oftre
atmentb
utalso
resultedin
cerebral
ischemiccomplications
Fodstadetal.,
Neurosurgery1981
[14]
Com
parativ
eclin
icaltrialof
epsilon
amino-caproica
cid
andtranexam
icacid
inthe
preventio
nof
early
recurrence
ofsubarachno
idhemorrhage
Rand
omized
trial
Epsilon
amino-caproica
cid
6gq6h
IVcontinued
until
surgeryor
discharge
(N=90)
Tranexam
icacid
1gq6h
IVcontinuedun
tilsurgeryor
discharge
(N=61)
Prim
aryou
tcom
e:recurrenth
emorrhage
diagno
sedclinically
byHCT
,LP,or
autopsy
Second
aryou
tcom
e:delay
edisc
hemicdeficit
diagno
sedby
clinical
deterio
ratio
n,angiograph
icvasospasm,and
infarcto
nHCT
Rebleeding
occurred
in8%
ofam
inocaproic-acid-tre
ated
patie
ntsa
nd10%of
tranexam
icacid
treated
patie
nts.Delayed
ischemic
deficits
occurred
in7%
ofam
inocaproicacid
patie
nts
and5%
oftranexam
icacid
patie
nts.Mortalitywas
11%in
each
grou
p.P=NSfora
llou
tcom
es
Chow
dharyand
Sayed,JN
NP1981
[15]
Antifibrinolytictre
atmentin
subarachno
idhemorrhage
Rand
omized,dou
ble-blind,
placebo-controlled,
multic
enterstudy
Tranexam
icacid
1gq
4hIV×1w
eekthen
1gq6h
IV×3weeks
(N=241)
Placebo
(N=238)
Prim
aryou
tcom
e:3-mon
thGOS
Second
aryou
tcom
e:neurologicaldeterio
ratio
n,rebleeding
,infarction,
hydrocephalus,edem
a,epilepsy
Rebleeding
redu
cedfro
m24%
incontrolgroup
to9%
intre
atmentg
roup
(P<0.001),
butw
ithconcurrent
increase
inisc
hemiccomplications
(24%
intre
atmentg
roup
versus
15%in
placebo,P<
0.01).Nodifferencein3
mon
thGOS
Verm
eulenetal.,
NEJM
1984
[16]
Antifibrinolytictre
atmentin
subarachno
idhemorrhage:a
rand
omized
placebo-controlledtrial
(STA
R)
Prospective,do
uble-blin
d,placebo-controlled,
multic
enter,rand
omized
trial
with
in96
hourso
fSAHon
set
inwho
maneurysm
repairwas
delay
edbeyond
48ho
urs
Tranexam
icacid
1gIV
q4h×1w
eekthen
1.5gPO
q6h×2
weeks
(N=229)
Placebo
(N=233)
Prim
aryou
tcom
e:3-mon
thGOS
Second
aryou
tcom
es:
rebleeding
,delayed
cerebral
ischemia,hydroceph
alus,
posto
perativ
eischemia
Nodifferencein3-mon
thGOS.Sign
ificant
decrease
inrebleeding
from
33%in
placebogrou
pto
19%in
treatmentg
roup
.No
differenceindelay
edcerebral
ischemia,hydroceph
alus,or
posto
perativ
eischemia
Roos,N
eurology
2000
[17]
Stroke Research and Treatment 5
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Immediateadministratio
nof
tranexam
icacid
andredu
ced
incidenceo
fearlyrebleeding
after
aneurysm
alsubarachno
idhemorrhage:a
prospectiver
ando
mized
study
Rand
omized,
placebo-controlledtrial
Tranexam
icacid
1gIV
bolus,then
1gIV
q6ho
ursu
ntil
aneurysm
repairor
72ho
ursp
ostictus.
(N=254)
Placebo
(N=251)
Prim
aryou
tcom
e:Re
bleeding
byHCT
Second
aryou
tcom
e:6
-mon
thGOS,clinical
vasospasm/delayed
ischemicneurological
deficit,
TCDspasm
Treatm
entg
roup
hadredu
ced
rebleeding
rateof
2.4%
comparedto
10.8%in
the
placebogrou
p(P<0.01).
Morefavorableou
tcom
einthe
treatmentg
roup
(74.8%
comparedto
70.5%in
the
controlgroup
,P=NS).N
oincreasedris
kof
ischemia
Hillman
etal.,J
Neurosurg
2002
[18]
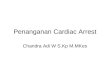
Neuroprotectiv
esdrugs
Ado
uble-blin
dclinical
evaluatio
nof
thee
ffectof
nizofeno
neon
delayed
ischemicneurologicaldeficits
follo
winganeurysm
alrupture
Rand
omized,placebo
controlledtrail
Nizofenon
efor
5–10
days
(N=42)
Placebo
(N=48)
Prim
aryou
tcom
e:delayed
ischemicneurological
deficits
with
angiograph
icallyconfi
rmed
vasospasm.
Second
aryou
tcom
es:
one-mon
thdisabilityindex,
motor,and
speech
functio
n
Nodifferenceindelay
edisc
hemiceventsbetween
treatmentg
roup
s.Amon
gpatie
ntsw
ithvasospasm,tho
sewho
received
nizofeno
nehad
bette
rone-m
onth
functio
nal
outcom
es(P<0.05)
Saito
etal.,Neurol
Res1983[19]
Nizofenon
eadm
inistratio
nin
thea
cutesta
gefollo
wing
subarachno
idhemorrhage.
Results
ofam
ultic
enter
controlleddo
uble-blin
dclinicalstudy
Rand
omized,dou
ble-blind,
placebo-controlled,
multic
enterstudy
ofHun
tHessg
rade
I–IV
Nizofenon
e5mg×2
weeks
(N=102)
Placebo
(N=106)
Prim
aryou
tcom
e:neurologicalexam
at1-m
onth
anddischarge
Sign
ificantlyim
proved
one-mon
thor
discharge
functio
naloutcomein
treatmentg
roup
comparedto
placebo(P<0.05).No
differenceinmortality
Ohtae
tal.,J
Neurosurg
1986
[20]
Effecto
fafre
eradical
scavenger,edaravon
e,in
the
treatmento
fpatientsw
ithaneurysm
alsubarachno
idhemorrhage
Rand
omized,con
trolled,
single-center
study
Edaravon
e30m
gIV
BID×14
days
(N=49)
Con
trol(usual
treatment)
(N=42)
Prim
aryou
tcom
e:delayed
ischemicneurological
deficits
Second
aryou
tcom
es:
cerebralinfarctio
ndu
eto
vasospasm,3-m
onth
GOS
Nodifferenceindelay
edisc
hemicneurologicaldeficits
betweentre
atmentand
controlgroup
s.Lesscerebral
infarctio
nin
treatmentg
roup
(0%versus
66%,P
=0.028).
Poor
outcom
ecausedby
vasospasm
0%in
treatment
grou
pand71%in
control
grou
p(P
=0.04
6)
Mun
akatae
tal.,
Neurosurgery2009
[21]
Eicosapentaeno
icAc
idCerebralV
asospasm
Therapy
Stud
y(EVA
S)
Rand
omized,con
trolled,op
enlabel,multic
enter,effi
cacy
study
ofsurgicallyclipp
edSA
Hpatie
nts
Eicosapentaeno
icacid
(omega3
fatty
acid)
900m
gTID×30
days
(N=81)
Con
trol(usual
treatment)
(N=81)
Prim
aryou
tcom
e:symptom
aticvasospasm
orinfarcto
nHCT
Second
aryou
tcom
e:1-m
onth
GOS
Symptom
aticvasospasm
occurred
significantly
lessin
thetreatmentg
roup
(15%
versus
30%in
controls,
P=
0.022)
asdidinfarctio
nfro
mvasospasm
(7%versus
21%in
controls,
P=0.012)
Yoneda
etal.,
World
Neurosurg
2012
[22]

6 Stroke Research and Treatment
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Safetyandeffi
cacy
ofNA-
1in
patie
ntsw
ithiatro
genics
troke
after
endo
vascular
aneurysm
repair(ENAC
T):a
phase2
,rand
omized,dou
ble-blind,
placebo-controlledtrial
Rand
omized,dou
ble-blind,
placebo-controlledstu
dyof
ruptured
(WFN
S1–3)
and
unruptured
aneurysm
sun
dergoing
endo
vascular
repair
NA-
12.6mg/kg
infusio
nover
10minutes
(N=92)
Placebo
(N=93)
Prim
aryou
tcom
e:safety,
numbera
ndvolumeo
fisc
hemicstrokeso
nMRI
DWIand
FLAIR
12–9
6ho
ursa
fterinfusion
Second
aryou
tcom
e:30-day
mRS
,NIH
SS,
neurocognitiv
eoutcome
NodifferenceinMRI
lesio
nvolume,bu
tfew
erisc
hemic
lesio
nsin
NA-
1group
comparedto
placebo(P
=0.012).IntheS
AHsubgroup
(20%
ofcoho
rt)theirMRI
numbera
ndisc
hemicvolume
was
significantly
lessin
the
treatmentg
roup
.No
differencein30
dayNIH
SSor
mRS
betweengrou
ps
Hill
etal.,Lancet
Neurol2012[23]
Statins
Simvastatin
redu
ces
vasospasm
Afte
raneurysmal
subarachno
idhemorrhage:
results
ofap
ilotrando
mized
clinicaltria
l
Rand
omized,
placebo-controlledpilottria
l
Simvasta
tin80
mgqd
for14days
(N=19)
Placebo
(N=20)
Prim
aryou
tcom
e:delayed
ischemicneurological
deficitconfi
rmed
byTC
Dor
angiograph
y.Second
aryou
tcom
es:liver
transaminases,C
K,von
Willebrand
factor,S100
Vasospasm
occurred
in26%of
treatmentg
roup
comparedto
60%of
placebogrou
p(P<
0.05).Nodifferences
intransaminitiso
rmyositis.
VWFandS100
were
significantly
lower
inthe
treatmentg
roup
(P<0.05)
Lynchetal.,Stroke
2005
[24]
Effectsof
acutetreatmentw
ithpravastatin
oncerebral
vasospasm,autoregulation,
anddelay
edIschem
icdeficits
after
aneurysm
alsubarachno
idhemorrhage.A
phaseIIrando
mized
placebo-controlledtrial
Rand
omized
placebo-controlled,ph
aseII
Trial
Pravastatin
40mgPO
qd×14d
(N=40
)
Placebo
(N=40
)
Prim
aryou
tcom
e:incidence,severity,and
duratio
nof
vasospasm
onTC
D,durationof
impaire
dautoregu
latio
nmeasuredby
transie
nthyperemic
respon
seon
TCD
Second
aryou
tcom
e:vasospasm-rela
teddelay
edisc
hemicdeficits,disa
bility
atdischarge
TCDvasospasm
andsevere
vasospasm
werer
educed
inthetreatmentg
roup
(P=
0.00
6andP=0.04
4,resp.).
Durationof
impaire
dautoregu
latio
nshortenedin
treatmentg
roup
(P<0.01).
Vasospasm-related
delayed
ischemicdeficits
was
redu
ced
(P<0.001)andmortalitywas
redu
ced(P
=0.037)
Tsengetal.,Stroke
2005
[25]
Arand
omized,dou
ble-blind,
placebo-controlledpilotstudy
ofsim
vasta
tinin
aneurysm
alsubarachno
idhemorrhage
Rand
omized,dou
ble-blind,
placebo-controlledpilotstudy
Simvasta
tin80
mgqd
instatin
naıveF
isher
3SA
Hun
tildischarge
or21
days
(N=19)
Placebo
(N=20)
Prim
aryou
tcom
e:death
anddrug
morbidity
(elevatedCK
,transaminases)
Second
aryou
tcom
es:T
CD,
angiograph
icor
clinical
vasospasm,
vasospasm-rela
tedinfarcts,
clinicaloutcomes
atdischarge,cardiac,and
infectious
morbiditie
s
Mortalityin
0%tre
atment
grou
pand15%placebogrou
p.Ang
iographically
confi
rmed
vasospasm
in26%tre
atment
grou
pand25%placebogrou
p.Va
sospasm
infarctsin
11%
treatmentg
roup
and25%
placebogrou
p.Alldifferences
P=NS
Chou
etal.,Stroke
2008
[26]

Stroke Research and Treatment 7
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Biologicaleffectsof
simvastatin
inpatie
ntsw
ithaneurysm
alsubarachno
idhemorrhage:ad
ouble-blind,
placebo-controlled
rand
omized
trial
Dou
ble-blind,
placebo-controlled
rand
omized
trial
Simvasta
tin80
mgPO
×15
days
(N=16)
Placebo
(N=16)
Prim
aryou
tcom
e:effecto
fsim
vasta
tinon
labo
ratory
parameterso
fend
othelial
functio
n,fib
rinolysis,
coagulation,
inflammation
andcholesterol
Second
aryou
tcom
es:T
CDvasospasm,clin
icalsig
nsof
DCI
,3-a
nd6-mon
thGOS
Simvasta
tingrou
phad
significantly
lower
total
cholesteroland
LDL,bu
tno
differences
incoagulation,
fibrin
olysis,
endo
thelium
functio
n,or
inflammation.
No
differences
inTC
Dvasospasm,clin
icalDCI
,or
poor
outcom
e
Vergou
wen
etal.,J
Cereb
Bloo
dFlow
Metab
2009
[27]
Aneurysm
repair
Timingof
operationfor
ruptured
supratentoria
laneurysm
s:ap
rospectiv
erand
omized
study
Rand
omized,prospectiv
estu
dyof
Hun
tHessg
rade
I–III
SAHpatie
nts
Acutes
urgery
(day
0–3aft
erSA
H)
(N=71)
Interm
ediate
surgery(
day4
–7aft
erSA
H)
(N=70)
Latesurgery
(day
8or
later
after
SAH)
(N=70)
Prim
aryou
tcom
e:3-mon
thdead,dependent
orindepend
ent.
Second
aryou
tcom
es:
Neurologicald
eficitfrom
directeffecto
finitia
lbleed,
complicationof
surgery,
confi
rmed
rebleeding
,delay
edisc
hemic
deterio
ratio
n,hydrocephalus,extracranial
complications
Acutes
urgery
patie
ntsw
ere
moreo
ftenindepend
entat
3-mon
ths(92%versus
79%in
interm
ediatetim
ingand80%
inthelatetim
inggrou
p,P<
0.01).Mortalitywas
6%in
the
early
surgerygrou
pversus
13%
inthelates
urgery
grou
p(P
=NS)
Ohm
anand
Heiskanen,J
Neurosurg
1989
[28]
Internationalsub
arachn
oid
aneurysm
trial(ISAT
)of
neurosurgicalclip
ping
versus
endo
vascular
coiling
in2143
patie
ntsw
ithruptured
intracranialaneurysm
s:a
rand
omized
trial
Rand
omized,unb
lindedtrial
ofSA
Hpatie
ntsw
ithan
aneurysm
judged
technically
suitablefor
either
clipp
ingor
coiling
andclinicalequ
ipoise
Surgicalclipp
ing
(N=1070)
Endo
vascular
treatmentb
ydetachable
platinum
coils
(N=1073)
Prim
aryou
tcom
e:1-y
ear
mRS
3–6versus
1-2Second
aryou
tcom
es:
rebleeding
,qualityof
lifea
t1y
ear(euroQol),fre
quency
ofepilepsy,cost
effectiv
eness,
neurop
sychological
outcom
es
Dependent
ordead
at1y
ear:
23.7%endo
vascular
versus
30.6%clipp
ing(P
=0.0019).
Molyn
euxetal.,
ISAT
Collabo
rativ
eGroup
,Lancet
2002
[29]
Internationalsub
arachn
oid
aneurysm
trial(ISAT
)of
neurosurgicalclip
ping
versus
endo
vascular
coiling
in2143
patie
ntsw
ithruptured
intracranialaneurysm
s:a
rand
omized
comparis
onof
effectson
survival,
depend
ency,seizures,
rebleeding
,sub
grou
ps,and
aneurysm
occlu
sion
Rand
omized,unb
lindedtrial
ofSA
Hpatie
ntsw
ithan
aneurysm
judged
technically
suitablefor
either
clipp
ingor
coiling
andclinicalequ
ipoise
Surgicalclipp
ing
(N=1070)
Endo
vascular
treatmentb
ydetachable
platinum
coils
(N=1073)
Prim
aryou
tcom
e:1-y
ear
mRS
3–6versus
1-2Second
aryou
tcom
es:
rebleeding
,qualityof
lifea
t1-y
ear(Eu
roqo
l),fre
quency
ofepilepsy,cost
effectiv
eness,
neurop
sychological
outcom
es
Deador
depend
entat1-year:
23.5%of
endo
vascular
grou
pversus
30.9%of
clipp
ing
grou
p.ARR
7.4%.E
arly
survivaladvantageo
fcoilin
gmaintainedup
to7years(P=
0.03).Lo
wer
riskof
epilepsyin
coiledgrou
pbu
thigherlate
rebleeding
riskin
coiledgrou
p
Molyn
euxetal.,
Lancet2005
[30]
8 Stroke Research and TreatmentTa
ble1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
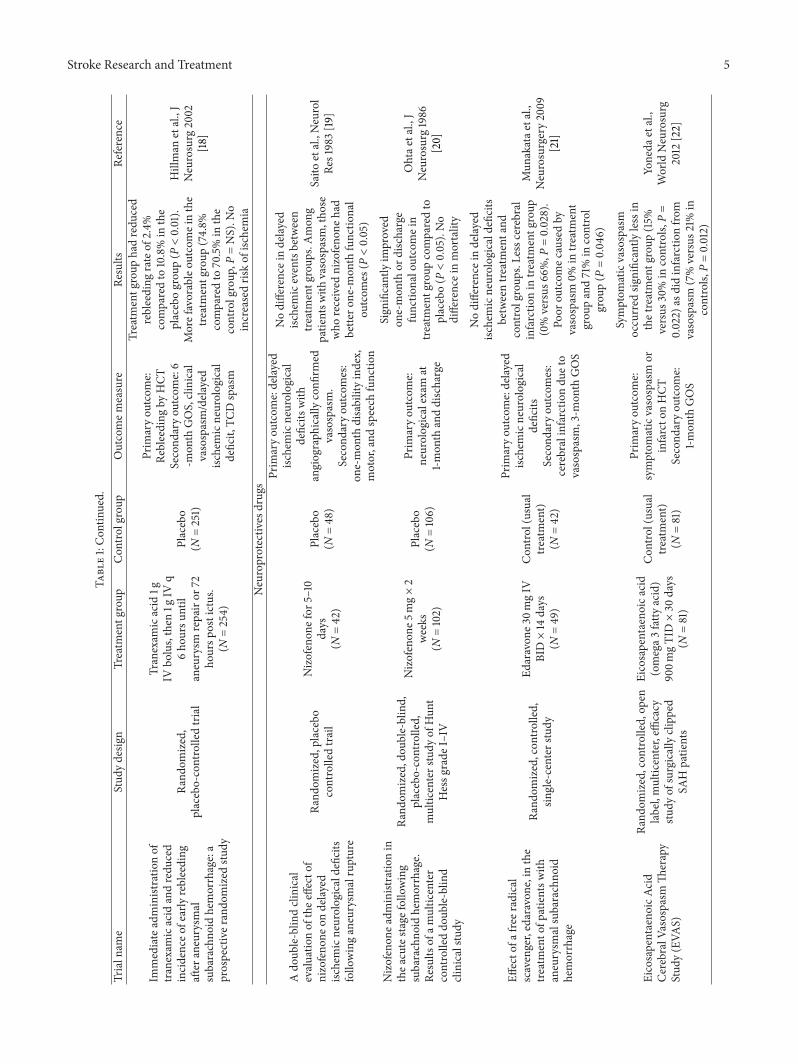
Theb
arrowruptured
aneurysm
trial
Rand
omized,open-label,
prospective,sin
gle-center
study
Surgicalclipp
ing
(N=238)
Endo
vascular
coiling
(N=233)
Prim
aryou
tcom
e:1-y
ear
mRS>2
Poor
outcom
ein33.7%of
clipp
edand23.2%of
coiled
patie
nts(P=0.02)
McD
ougalletal.,J
Neurosurg
2012
[31]
Lipidperoxidatio
ninhibitor
Rand
omized,dou
ble-blind,
vehicle
-con
trolledtrialof
tirilazadmesylateinpatie
nts
with
aneurysm
alsubarachno
idhemorrhage:a
coop
eratives
tudy
inEu
rope,
Austr
alia,and
New
Zealand
Dou
ble-blind,rand
omized,
vehicle
-con
trolledstu
dyin
men
andwom
enwith
aneurysm
alSA
H
Tirilazad
0.6m
g/kg/
(N=257)
Tirilazad
2mg/kg/d
(N=249)
Tirilazad
6mg/kg/d
(N=256)
upto
11days
Placebo
containing
citratev
ehicle
(N=253)
Prim
aryou
tcom
e:Symptom
aticvasospasm
Second
aryou
tcom
e:3-mon
thGOS,NIH
SS,
infarctvolum
eonhead
CT
Thes
ubgrou
p6m
g/kg
treatmentarm
hadredu
ced
mortality(P
=NS)
andbette
r3-mon
thGOS(P
=NS)
comparedto
placebo.Less
symptom
aticvasospasm
in6m
g/kg
grou
p,bu
tnot
significant.Men
show
edmore
benefit
than
wom
en.N
osig
nificantimprovem
entw
ithlower
dosin
ggrou
ps
Kasselletal.,J
Neurosurg
1996
[32]
Arand
omized,dou
ble-blind,
vehicle
-con
trolledtrialof
tirilazadmesylateinpatie
nts
with
aneurysm
alsubarachno
idhemorrhage:a
coop
eratives
tudy
inNorth
America
Dou
ble-blind,rand
omized,
vehicle
-con
trolledstu
dyin
men
andwom
enwith
aneursym
alSA
H
Tirilazad
2mg/kg/d
(N=298)
Tirilazad
6mg/kg/d
(N=299)
upto
11days
Placebo
containing
citratev
ehicle
(N=300)
Prim
aryou
tcom
e:mortalityat76
days
Second
aryou
tcom
e:3-mon
thGOSandNIH
SS,
infarctvolum
eonhead
CTsymptom
aticvasospasm,
incidence,andseverityof
angiograph
icvasospasm
Nodifferenceinmortality,
favorableG
OSou
tcom
e,or
employmentb
etweengrou
ps.
Nodifferences
insymptom
atic
orangiograph
icvasospasm
Haley
etal.,J
Neurosurg
1997
[33]
Dou
ble-blind,rand
omized,
vehicle
-con
trolledstu
dyof
high
-dosetirilazadmesylate
inwom
enwith
aneurysm
alsubarachno
idhemorrhage.
PartIa
coop
eratives
tudy
inEu
rope,A
ustralia,N
ewZe
aland,andSouthAfrica
Dou
ble-blind,rand
omized,
vehicle
-con
trolledstu
dyin
wom
enwith
aneurysm
alSA
H
Tirilazad
mesylate
15mg/kg/d
IVho
urs
for11d
ays
(N=40
5)
Placebo
containing
citratev
ehicle
(N=414)
Prim
aryou
tcom
e:91-day
mortalitySecond
ary
outcom
e:3-mon
thGOS,
clinicalvasospasm
,use
ofhypervolem
ichypertensiv
etherapy,neurological
worsening
from
vasospasm,
cerebralinfarctio
n,useo
fangiop
lasty
,safety
endp
oints
Mortalityratesa
nd3-mon
thGOSno
tdifferentb
etween
grou
ps.L
ower
symptom
atic
vasospasm
intirilazadgrou
p(24.8%
versus
33.7%in
placebogrou
p,P=0.005).
Cerebralinfarction8%
intre
atmentg
roup
versus
13%in
placebogrou
p(P<0.04)
Lanzinoetal.,J
Neurosurg
1999
[34]
Dou
ble-blind,rand
omized,
vehicle
-con
trolledstu
dyof
high
-dosetirilazadmesylate
inwom
enwith
aneursym
alsubarachno
idhemorrhage.
PartIIac
ooperativ
estudy
inNorth
America
Dou
ble-blind,rand
omized,
vehicle
-con
trolledstu
dyin
wom
enwith
aneurysm
alSA
H
Tirilazad
mesylate
15mg/kg/d
IVup
to11
days
(N=410)
Placebo
containing
citratev
ehicle
(N=413)
Prim
aryou
tcom
e:mortalityat91
days
inWFN
SgradeIV-Vpatie
nts
Second
aryou
tcom
es:3
mon
thGOSor
clinical
vasospasm
1–14
days
from
dosin
g,useo
fhypervolem
ichypertensiv
etherapy,neurological
worsening
from
vasospasm,
cerebralinfarctio
n,useo
fangiop
lasty
,safety
endp
oints
Nodifferences
inmortality
whenanalyzingthee
ntire
popu
lation.
Nodifferencein
GOS,symptom
atic
vasospasm,vasospasm
severity.In
WFN
Sgrades
IV-V,low
ermortalityin
treatmentg
roup
(24.6%
versus
43.4%in
placebo,P=0.016).
InWFN
SI–IIIimproved
GOS
inplacebogrou
p(83.3%
versus
76.7%in
treatment
grou
p,P=0.04)
Lanzinoand
Kassell,J
Neurosurg
1999
[35]

Stroke Research and Treatment 9Ta
ble1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Thrombo
lytic
s
Preventio
nof
delayed
ischemicdeficits
after
aneurysm
alsubarachno
idhemorrhageb
yintrathecal
bolusinjectio
nof
tissue
plasminogen
activ
ator
(rTP
A)
Prospective,controlledtrialof
Fisher
IIIclip
pedSA
Hpatie
nts
rTPA
10mgIV
intracisternal
immediately
follo
winganeurysm
clipp
ing±5–10mgIV
TPA
intraventricularlyin
patie
ntsw
ithIV
H(N
=52)
NoTP
Ainstillation
(N=68)
Prim
aryou
tcom
e:clinical
delay
edisc
hemicdeficits
attributed
tovasospasm
Second
aryou
tcom
e:3-mon
thGOS
Sign
ificantlylesstransie
ntand
perm
anentd
elayed
ischemic
deficits
andbette
rGOSin
rTPA
grou
p
Seifertetal.,Ac
taNeurochir1994
[36]
Arand
omized
trialof
intraoperativ
e,intracisternal
tissuep
lasm
inogen
activ
ator
forthe
preventio
nof
vasospasm
Rand
omized,dou
ble-blinded,
placebo-controlled,
multic
enterstudy
rTPA
10mg
intracisternalatthe
timeo
faneurysm
clipp
ing
(N=51)
Placebovehicle
(N=49)
Prim
aryou
tcom
e:angiograph
icvasospasm
Second
aryou
tcom
e:mortality,3-mon
thGOS,
symptom
aticvasospasm,
clotclearance
onCT
,TCD
velocitie
s,useo
fHHHon
angiop
lasty
totre
atvasospasm
Nodifferenceinangiograph
icvasospasm,vasospasm
treatment,TC
Dvelocitie
s,mortality,or
3-mon
thGOS
Find
lay,
Neurosurgery1995
[37]
Efficacy
oflow-dose
tissue-plasminogen
activ
ator
intracisternaladm
inistratio
nforthe
preventio
nof
cerebral
vasospasm
after
subarachno
idhemorrhage
Rand
omized,con
trolledtrial
Interm
ittent
Tisokinase
960,00
0IUvia
ciste
rnaldrain
(N=20)
Con
tinuo
usinfusio
nTisokinase
1920
IU/h
×48
hviac
isternal
drain
(N=20)
Con
trol
(stand
ard
treatment)
(N=20)
Prim
aryou
tcom
e:cle
arance
ofsubarachno
idclo
tsby
HCT
Second
aryou
tcom
e:delay
edcerebralisc
hemia,
3-mon
thmRS
andGOS
Subarachno
idclo
tbyHCT
anddelayedcerebralisc
hemia
weres
ignificantly
lessin
the
treatmentg
roup
scom
paredto
control(P<0.05).Th
einterm
ittently
treated
grou
phadbette
rneurological
outcom
esthan
thec
ontro
lgrou
p(P<0.05)
Yamam
otoetal.,
World
Neurosurgery2010
[38]
Anti-p
latelets
Dipyridam
olea
ndpo
stoperativ
eischemicdeficits
inaneurysm
alsubarachno
idhemorrhage
Rand
omized,
placebo-controlled,
single-blindcontrolledtrial
Dipyridam
ole100
mg
POqd
or10mg/day
IV×3-mon
ths
(N=336)
Placebo
(N=314)
Prim
aryou
tcom
e:3-mon
thGOS
Second
aryou
tcom
e:neurologicaldeterio
ratio
nfollo
winganeurysm
repair
Nodifferences
in3-mon
thGOSor
delayedneurological
deterio
ratio
n
Shaw
etal.,J
Neurosurg
1985
[39]
Rand
omized
controlledtrial
ofacetylsalicylicAc
idin
aneurysm
alsubarachno
idhemorrhage:theM
ASH
study
Rand
omized
controlledpilot
study
;factoria
ldesign
(magnesiu
mversus
placebo
andASA
versus
placebo,
separatedap
riori)
Aspirin100m
gPR
qd×14
days
with
in12
hourso
faneurysm
occlu
sion.
(N=87)
Placebo
(N=74)
Prim
aryou
tcom
e:delayed
ischemicneurological
deficits
with
in3-mon
thso
fSA
Hconsistingof
HCT
infarctsplus
clinicald
eclin
eSecond
aryou
tcom
e:newCT
infarctsof
any
cause,po
stophemorrhage,
mRS≥4,mRS≥1
Nodifferenceindelay
edisc
hemicevents,
CTinfarctio
n,or
3-mon
thou
tcom
es
VandenBe
rgh,
Stroke
2006
[40]

10 Stroke Research and Treatment
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Cilostazolim
proves
outcom
eaft
ersubarachno
idhemorrhage:ap
relim
inary
repo
rt
Rand
omized,single-blind,
prospective,multic
enterstudy
Cilostazol100m
gPO
BID
(N=49)
Con
trol(usual
care)
(N=51)
Prim
aryou
tcom
e:symptom
aticvasospasm
andcerebralinfarctio
n,dischargem
RS
Nodifferenceinsymptom
atic
vasospasm
orcerebral
infarctio
n.mRS
atdischarge
bette
rintre
atmentg
roup
(1.5
versus
2.6in
controls,
P=
0.041)
Suzukietal.,
Cerebrovasc
Dis
2011[41]
Steroids
Effecto
fflud
rocortiso
neacetateinpatie
ntsw
ithsubarachno
idhemorrhage
Rand
omized,placebo
controlled,multic
entertria
l
Flud
rocortiso
ne40
0mcg/day
BID×12
days
POor
IV(N
=46
)
Placebo
(N=45)
Prim
aryou
tcom
e:plasmav
olum
echang
e,flu
idbalance,sodium
balance
Second
aryou
tcom
e:delay
edcerebralisc
hemia
with
in28
days
and28-day
GOS
Treatm
entreduced
negativ
esodium
balance(P=0.014)
butd
idno
taffectplasma
volume.Nosig
nificant
differenceincerebralisc
hemia
(22%
versus
31%in
controls,
P=0.349).Sim
ilaro
utcomein
each
grou
p
Hasan
etal.,Stroke
1989
[42]
Arand
omized
controlledtrial
ofhydrocortison
eagainst
hypo
natre
miain
patie
ntsw
ithaneurysm
alsubarachno
idhemorrhage
Rand
omized,
placebo-controlledstu
dy
Hydrocortiso
ne300m
gq6h×10d
then
tapero
ver4
d(N
=35)
Placebo
(N=36)
Prim
aryou
tcom
e:hypo
natre
mia
<140m
mol/L
Second
aryou
tcom
e:30-day
mRS
,sym
ptom
atic
vasospasm
Lesssodium
excretionand
urinev
olum
eintre
atment
grou
p(P
=0.04).No
significantd
ifferencesin
vasospasm
ormRS
Katayamae
tal.,
Stroke
2007
[43]
Rand
omized,dou
ble-blind,
placebo-controlled,pilottria
lof
high
-dose
methylpredn
isolone
inaneurysm
alsubarachno
idhemorrrhage
Rand
omized,dou
ble-blind,
placebo-controlled,sin
gle
center
study
Methylpredn
isolone
16mg/kg
IVqd×3
days
(N=49)
Placebo
(N=46
)
Prim
aryou
tcom
e:symptom
aticvasospasm
andinfarcto
nHCT
Second
aryOutcomes:1
year
GOS,functio
nal
outcom
escale,
andseverity
ofdelay
edisc
hemicdeficits
Nosig
nificantd
ifference
insymptom
aticvasospasm
orinfarcto
nHCT
.Nodifference
in1-y
earG
OSor
delayed
ischemicdeficits
at3-mon
ths.
Poor
outcom
ebyfunctio
nal
outcom
escalewas
redu
cedin
treatmentg
roup
(P=0.02)
Gom
isetal.,
JNeurosurg
2010
[44]
Transfu
sion/erythrop
oietin/album
in
Acutes
ystemicerythrop
oietin
therapyto
redu
cedelayed
ischemicdeficits
follo
wing
aneurysm
alsubarachno
idhemorrhage:ap
hase
IIrand
omized,dou
ble-blind,
placebo-controlledtrial
PhaseIIrando
mized,
doub
le-blin
d,placebo-controlledtrial
Erythrop
oietin
IV(30,00
0u)
every48
hfora
totalof9
0,00
0U
(N=40
)
Placebo
(N=40
)
Prim
aryou
tcom
e:incidence,du
ratio
nand
severityof
TCDvasospasm;
duratio
nof
impaire
dautoregu
latio
nby
TCD
Second
aryou
tcom
e:incidenceo
fdelayed
ischemicdeficits,m
RS,
GOS,andNIH
SSat
dischargea
nd6-mon
ths
Nodifferences
inincidenceo
fTC
Dvasospasm
oradverse
events.
Treatm
entg
roup
had
lesssevereT
CDvasospasm
(P=−0.037),reduced
delayed
ischemicdeficits/delayed
cerebralinfarcts(P
=0.001),
andshorteneddu
ratio
nof
impaire
dautoregu
latio
n(P<
0.001)andmorefavorable
dischargeo
utcome(P=0.039)
Tsengetal.,
JNeurosurg
2009
[45]

Stroke Research and Treatment 11Ta
ble1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Prospective,rand
omized
trial
ofhigh
ergoalhemoglobin
after
SAH
Prospective,rand
omized
pilot
safety,and
feasibilitystu
dy
Packed
RBC
transfu
sionto
goal
Hgb
11.5g/dL
(N=21)
Packed
RBC
transfu
sionto
goalHgb
10g/dL
(N=23)
Prim
aryou
tcom
es:dayso
fcore
temp>100.4F
,ventilator-fre
edays,
hemoglobinlevel
Second
aryou
tcom
es:
NIH
SS,m
RS,and
MRI
at14
days,m
RSat28
days
and
3-mon
ths
HighertargetH
gbresultedin
moretransfusio
ns.N
odifferenceinsafetyendp
oints.
Num
bero
fMRI
infarcts,
NIH
SS,and
mRS
similar
betweenbo
thgrou
psatall
timepoints
Naidech
etal.,
NeurocritCare
2010
[46]
TheA
lbum
inin
Subarachno
idHem
orrhagem
ulticenterp
ilot
clinicaltria
l:safetyand
neurologicou
tcom
es(A
LISA
H)
Openlabel,do
seescalation
study
Album
inin
3tie
rdo
ses:0.625g/kg/d
(N=20),1.2
5g/kg/d
(N=20),1.8
75g/kg/d
(N=7)×7days
(N=47
total)
NA
Prim
aryou
tcom
es:severe
tolifethreatening
heart
failu
re,anaph
ylaxis
Second
aryou
tcom
es:
functio
naloutcomea
t3-mon
ths
Doses
upto
1.25g/kg/d×7
days
toleratedwith
out
dose-limiting
complications.
Trendtowardbette
routcomes
in1.2
5g/kg/d
dose
compared
to0.625g/kg/d
Suarez
etal.,
Stroke
2012
[47]
Vasodilators—
CRGPandendo
thelin
receptor
antagonist
Effecto
fcalcito
nin-gene-related
peptideinpatie
ntsw
ithdelayedpo
stoperativ
ecerebral
ischemiaaft
eraneurysm
alsubarachno
idhemorrhage
Rand
omized,single-blind,
controlled,multic
enterstudy
Calcito
nin-related
gene
peptide
(0.6mcg/m
in)×
10days
(N=62)
Standard
medicaltherapy
(N=55)
Prim
aryou
tcom
e:3-mon
thGOS
Nodifferencein3-mon
thGOS.Hypotensio
ncommon
intre
atmentg
roup
.
Bell,Eu
ropean
CGRP
insubarachno
idHem
orrhages
tudy
grou
p,Lancet1992
[48]
Clazosentan,
anendo
thelin
receptor
antagonist,
inpatie
ntsw
ithaneurysm
alSA
hun
dergoing
surgicalclipp
ing:
arando
mized,dou
ble-blind,
placebo-controlledph
ase3
trial
(CONSC
IOUS2)
Phase3
rand
omized
placebo-controlled
doub
le-blin
ded
Clazosentan
(5mg/hIV
upto
14days)
(N=748)
Placebo
(N=389)
Prim
aryou
tcom
es:cerebral
vasospasm-rela
ted
morbidity
(DCI
/DIN
D/vasospasm
therapy),all-cause
mortalityat6weeks
Second
aryou
tcom
es:
12-w
eekGOSE
Noeffecto
nprim
aryendp
oint
(21%
incla
zosentan
grou
pand
25%in
placebogrou
pP=NS).
Poor
outcom
e(GOSE
)in29%
clazosentan
and25%placebo
grou
p
MacDon
aldetal.,
LancetNeuol2011
[49]
Rand
omized
trialof
clazosentan
inpatie
ntsw
ithaneurysm
alsubarachno
idhemorrhageu
ndergoing
endo
vascular
coiling
(CONSC
IOUS3)
Phase3
rand
omized
placebo-controlled
doub
le-blin
ded;
term
inated
early
forfutility
(plann
edN=1500)
Clazosentan
(5or
15mg/hIV
upto
14days)
(N=194)
Placebo
(N=189)
Prim
aryou
tcom
es:cerebral
vasospasm
related
morbidity
(DCI
/DIN
D/vasospasm
therapy),all-cause
mortalityat6weeks
Second
aryou
tcom
es:
12-w
eekGOSE
Clazosentan15mg/h
significantly
redu
ced
vasospasm-rela
ted
morbidity/all-causem
ortality
at6weeks
butd
idno
timprove
long
-term
outcom
ePrim
aryou
tcom
e:24%in
clazosentan
5mg/hand27%
inplacebogrou
pP=NSand
15%in
clazosentan
15mg/hP
=0.007
Poor
outcom
ein25%of
clazosentan
5mg/h,28%
clazosentan
15mg/h,and24%
ofplacebogrou
pP=NS.
MacDon
aldetal.,
Stroke
2012
[50]

12 Stroke Research and Treatment
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Hypertensive,hypervolem
ictherapy(proph
ylactic
)
Effecto
fhypervolemictherapy
oncerebralbloo
dflo
waft
ersubarachno
idhemorrhage:A
rand
omized
controlledtrial
Rand
omized,con
trolled,
single-center
study
High-volume
managem
ent(with
collo
idand
crystallo
id)totarget
PADP≥14mmHgor
CVP≥8m
mHg
(N=41)
Normalvolume
managem
ent
(with
collo
idandcrystallo
id)
totargetPA
DP
≥7m
mHgor
CVP≥5m
mHg
(N=41)
Prim
aryou
tcom
e:CB
Fby
Xeno
nCT
andbloo
dvolumeb
ytagged
RBC
Second
aryou
tcom
es:
symptom
aticvasospasm,
medicalcomplications,
GOSand3,6,and12
mon
ths
High-volumem
anagem
ent
patie
ntsreceivedsig
nificantly
morefl
uidbu
tthere
was
noeffecto
nnetfl
uidbalanceo
rbloo
dvolume.Nodifference
inCB
For
vasospasm
Lenn
ihan
etal.,
Stroke
2000
[51]
Prop
hylactichyperdyn
amic
posto
perativ
efluidtherapy
after
aneurysm
alsubarachno
idhemorrhage:a
clinical,prospective,
rand
omized,con
trolledtrial
Rand
omized,con
trolled
Prospective,trialofH
untH
ess
I–IIIp
atients
Hypertensive(MAP
20mmHggreater
than
pre-op
),hypervolem
ic(C
VP
8–12mmHg)
and
hemod
ilutio
nal(Hct
30–35%
)therapy
(N=16)
Normovolem
iccrystallo
idflu
idtherapyun
tilday12
(N=16)
Prim
aryou
tcom
e:TC
Dvasospasm,C
BFby
SPEC
Ton
day12
Second
aryou
tcom
es:1
year
GOS,neurop
sych
outcom
es,and
SPEC
T
Nodifferences
inTC
Dvasospasm
orSP
ECTCB
F.No
differencein1-y
earG
OS,
SPEC
T,or
neurop
sych
outcom
es
Egge
etal.,
Neurosurgery2001
[52]
Magnesiu
m
Intravenou
smagnesiu
msulfatefora
neurysmal
subarachno
idhemorrhage
(IMASH
):ar
ando
mized
doub
le-blin
ded,
placebo-controlled,
multic
enterp
hase
IIItria
l
Rand
omized
doub
le-blin
ded,
placebo-controlled,
multic
enterp
hase
IIItria
l.
MgSO
4IV
infusio
nto
2xbaselin
evalue
(20m
molover
30minutes
then
continuo
usinfusio
nof
80mmol/d×14
days;m
axim
umallowed
serumMgof
2.5m
mol/L
(N=169)
Equivalent
volumeo
fno
rmalsalin
einfusio
n.Occasional
changesin
infusio
nratesto
maintain
blinding
.(N
=158)
Prim
aryou
tcom
e:6-mon
thGOSE
5–8
Second
aryou
tcom
e:clinicalvasospasm
durin
ginitial2weeks,6-m
onth
mRS
,BarthelIndex,and
ShortF
orm
36
Favorable6
-mon
thGOSE
(5–8)6
4%ofMggrou
pand
63%placebo(P
=NS)
NodifferenceinmRS
,Barthel,
ShortF
orm
36,orc
linical
vasospasm.N
osubgroup
differences
Won
getal.,
Stroke
2010
[53]
Magnesiu
mfora
neurysmal
subarachno
idhemorrhage
(MASH
-2):ar
ando
mized
placebo-controlledtrial
Rand
omized,dou
ble-blind,
placebocontrolled,
multic
enter,ph
aseIIItrial
MgSO
4IV
64mmol/day
(N=60
6)
Placebo
(N=507)
Prim
aryou
tcom
e:3-mon
thmRS
4–6
Nodifferenceinpo
orou
tcom
eintheM
gSO
4grou
p(26.2%
versus
25.3%in
placebogrou
p)
Meese
tal.,
Lancet2012
[54]

Stroke Research and Treatment 13
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Adrenergicblockade
Beneficialeffectso
fadrenergic
blockade
inpatie
ntsw
ithsubarachno
idhemorrhage
Rand
omized
controlledtrial
Phentolamine2
0mg
q3h
+prop
rano
lol
80mgq8×3weeks
(N=68)
Placebo
(N=66)
Prim
aryou
tcom
e:neurologicaldeficitat28
days
Trendtowardlessneurological
deficitin
thetreated
grou
p(P
=0.053)
Waltere
tal.,
BMJ1982[55]
Endo
vascular
therapy
Effecto
fproph
ylactic
translu
minalballo
onangiop
lasty
oncerebral
vasospasm
andou
tcom
ein
patie
ntsw
ithFisher
gradeIII
subarachno
idhemorrhage:
results
ofap
hase
IImultic
enter,rand
omized
clinicaltria
l
Unb
linded,rand
omized
phase
IItrialofF
isher
IIIand
Fisher
III+
IVSA
Hpatie
ntsa
fter
clipp
ingor
coiling
with
in96
hof
rupture
Ballo
onangiop
lasty
ofbilateralA1,M1,P1,
basilar,intradu
ral
vertebralartery,and
supraclin
oidICA.
Protocollaterrevise
dto
exclu
deA1and
P1(N
=85)
Noprop
hylactic
ballo
onangiop
lasty
(N=85)
Prim
aryou
tcom
e:3-mon
thGOS
Second
aryou
tcom
e:delay
edisc
hemic
neurologicaldeficit,
TCD
vasospasm,ICU
,and
hospita
llengthof
stay
Non
significantd
ifference
indelay
edisc
hemicneurological
deficits
butlesstherapeutic
angiop
lastyrequ
iredin
treatmentg
roup
(P=0.03).
Nosig
nificantd
ifference
inGOSou
tcom
es.LOSsim
ilar.
Four
patie
ntsh
adprocedure
related
vesselperfo
ratio
n,threeo
fwho
mdied
Zwienenb
erg-Lee
etal.,Stroke
2008
[56]
Rhokinase
inhibitor—
fasudil
Effecto
fAT8
77on
cerebral
vasospasm
after
aneurysm
alsubarachno
idhemorrhage.
Results
ofap
rospectiv
eplacebo-controlled
doub
le-blin
dtrial
Rand
omized,placebo
controlled,do
uble-blin
d,multic
enterstudy
inHun
tHessI–IVclipp
edSA
Hpatie
nts
Fasudil(AT
877)
30mgIV
over
30minutes,T
ID×14
days
(N=131)
Placebo
(N=136)
Prim
aryou
tcom
e:redu
ctionof
incidenceo
rseverityof
angiograph
icvasospasm,reductio
nof
incidencea
ndsiz
eof
low-densityCT
lesio
nsdu
eto
vasospasm,reductio
nof
incidenceo
fsym
ptom
atic
vasospasm,poo
routcome
(1-mon
thGOS)
dueto
vasospasm
Fasudilsignificantly
redu
ced
angiograph
icvasospasm
(38%
intre
atmentg
roup
versus
61%
inplacebogrou
p,P=0.0023),
infarctsredu
ced(16%
intre
atmentversus3
8%in
placebogrou
p,P=0.0013)
andsymptom
aticvasospasm
redu
ced(35%
intre
atment
versus
50%in
placebo,P=
0.0247).Po
orou
tcom
e(GOS
1–4)
attributableto
vasospasm
occurred
in12%of
treatment
grou
pand26%of
placebo
grou
p(P
=0.0152).Noserio
usadversee
ventsinfasudil
grou
p
Shibuyae
tal.,
JNeurosurg
1992
[57]
Efficacy
andsafetyof
fasudil
inpatie
ntsw
ithsubarachno
idhemorrhage:fin
alresults
ofa
rand
omized
trialoffasud
ilversus
nimod
ipine
Rand
omized,openlabel,
multic
enterstudy
ofSA
HHun
t-Hessg
rade
I–IV
clipp
edpatie
nts
Fasudil30m
gIV
TID
×14
days
(N=63)
Nim
odipine
1-2mg/h×14
days
(N=66)
Prim
aryou
tcom
e:symptom
aticvasospasm
orinfarcto
nHCT
Second
aryou
tcom
e:1-m
onth
GOS
Nodifferenceinsymptom
atic
vasospasm
orHCT
infarcts.
Improved
GOSou
tcom
esin
fasudilgroup
(goo
dou
tcom
ein
74.5%versus
61.7%in
nimod
ipineg
roup
,P=0.04
0)
Zhao
etal.,
NeurolM
edCh
ir(Tokyo)2
011[58]

14 Stroke Research and Treatment
Table1:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Intensiveinsulin
therapy
Thee
ffectof
intensiveinsulin
therapyon
infectionrate,
vasospasm,n
eurologic
outcom
eand
mortalityin
neurointensiv
ecareu
nitafte
rintracranialaneurysm
clipp
ingin
patie
ntsw
ithacute
subarachno
idhemorrhage:a
rand
omized
prospectiveP
ilot
trial
Rand
omized,con
trolledstu
dy
IntensiveInsulin
Infusio
n(80–
120m
g/dL
)×14d
(N=40
)
Con
ventional
insulin
infusio
n(glucose
80–220
mg/dL
)×14d
(𝑁=38)
Prim
aryou
tcom
e:infection
Second
aryou
tcom
es:
vasospasm,6-m
onth
mortality,andmRS
Higherinfectio
nratein
the
conventio
nalgroup
(42%
versus
27%in
intensiveg
roup
,𝑃<0.001).Similar
vasospasm,m
ortality,and
mRS
at6mon
ths
Bilotta
etal.,
JNeurosurg
Anesthesio
l2007
[59]
Hypotherm
ia
Mild
intraoperativ
ehypo
thermiadu
ringsurgery
forintracranialaneurysm
(IHAST
)
Rand
omized,prospectiv
e,partially
blinded,controlled,
multic
entertria
lofW
FNS
gradeI–IIISA
Hpatie
nts
Intraoperativ
ehypo
thermia(ta
rget
33∘
Cwith
surfa
cecooling)
(N=499)
Intraoperativ
eno
rmotherm
ia(ta
rget36.5∘
C)(N
=501)
Prim
aryou
tcom
e:GOSat
90days
Second
aryou
tcom
es:
90-day
mRS
,BarthelIndex,
NIH
SS,n
europsychtesting,
adversee
vents
Nodifferencein90
dayGOS.
Goo
dGOSin
66%of
hypo
thermiaversus
63%of
controlp
atients(P=NS).N
odifferences
indeath,leng
thof
stay,ord
ischarged
isposition
.Po
stoperativ
ebacteremia
morec
ommon
inthe
hypo
thermiagrou
p(5%
versus
3%,P
=0.05)
Todd
etal.,
NEJM
2005
[60]

Stroke Research and Treatment 15
Table2:Ra
ndom
ized
controlledtrialsassessingneurologicou
tcom
esaft
ercardiaca
rrest—
completed
trials.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Calcium
channelblockers
Effectsof
nimod
ipineo
ncerebralbloo
dflo
wand
cerebrospinalfl
uidpressure
after
cardiaca
rrest:correlation
with
neurologicou
tcom
e
Rand
omized,
doub
le-blin
dstu
dy
Nim
odipineIV
0.25
mcg/kg/min
(N=25)
Placebo
(N=26)
Prim
aryou
tcom
e:CB
Fmeasuredby
Xeno
nCT
Second
aryou
tcom
es:ICP
,neurologicaldisability
HigherC
BFin
nimod
ipine
grou
pin
first4ho
ursa
fter
arrest(P<0.05)b
utno
differencea
t24ho
urs.No
differenceinneurological
outcom
es
Forsman
etal.,
AnesthAnalg1989
[64]
Neuropsycho
logicalsequelae
ofcardiaca
rrest
Rand
omized,
doub
le-blin
d,placebo-controlled,
study
ofou
t-of-h
ospital
ventric
ular
fibrillatio
n
Nim
odipine10m
cg/kg
IVthen
0.5m
cg/kg/min
×24
hours
(N=35)
Placebo
(N=33)
Prim
aryou
tcom
e:3-
and
12-m
onth
neurop
sychologicaland
cogn
itive
batte
ries
Nodifferencein
neurop
sychologicalor
cogn
itive
outcom
ebetween
grou
ps
Roinee
tal.,
JAMA1992
[65]
Arand
omized
clinicalstudy
ofac
alcium
-entry
blocker
(lido
flazine)inthetreatment
ofcomatoses
urvivorsof
cardiaca
rrest
Rand
omized,
doub
le-blin
d,placebo-controlled,
multic
enterstudy
Lido
flazine
1mg/kg
loadingdo
sethen
0.25
mg/kg
at8and16
hoursa
fterresuscitatio
n(N
=259)
Placebo
(N=257)
Prim
aryou
tcom
e:Pittsbu
rghCerebral
Perfo
rmance
Scalea
t6mon
ths
Second
aryou
tcom
es:
mortality,complications
Nodifferencein6-mon
thneurologicalou
tcom
eor
mortalitybetweengrou
ps
BrainRe
suscitatio
nClinicalTrialIIS
tudy
Group
,NEJM
1991
[66]
Nim
odipinea
fterresuscitatio
nfro
mou
t-of-h
ospital
ventric
ular
fibrillatio
n:a
placebo-controlled,
doub
le-blin
d,rand
omized
trial
Rand
omized,
doub
le-blin
d,placebo-controlled,
study
ofou
t-of-h
ospital
ventric
ular
fibrillatio
n
Nim
odipine10m
cg/kg
IVthen
0.5m
cg/kg/min
×24
hours
(N=75)
Placebo
(N=80)
Prim
aryou
tcom
e:survival,
1-yearG
OS
Second
aryou
tcom
es:death
relatedto
anoxic
enceph
alop
athy,G
CSat24
hoursa
nd1w
eek,3-
and
12-m
onth
mini-m
ental
statee
xam,activities
ofdaily
living,Ba
rthelind
ex,
neurologicalexam
,seizure,
SPEC
T,myocardial
infarctio
n,arrhythm
ias
Nodifferenceinthe
survivalrate,G
OSat3or
12mon
ths.Nodifferencein
minim
entalstateexam
,activ
ities
ofdaily
living,or
seizures
Roinee
tal.,
JAMA1990
[67]
Neuroprotectiv
e
Coenzym
eQ10
combined
with
mild
hypo
thermiaaft
ercardiaca
rrest:ap
relim
inary
study
Rand
omized,
placebo-controlled,
doub
le-blin
d,sin
gle-center
study
ofou
t-of-h
ospitalcardiac
arrest
Hypotherm
ia35-36∘C×
24ho
urs+
Coenzym
eQ10
250m
gPO×1then
150m
gPO
TID
(N=25)
Hypotherm
ia35-36∘C×24
hours+
Placebo
(N=24)
Prim
aryou
tcom
e:survival
toICUdischarge
Second
aryou
tcom
es:
3-mon
thsurvival,3-m
onth
GOS,S100
levels
3-mon
thsurvivalwas
68%
inthetreatmentg
roup
and
29%in
thec
ontro
lgroup
(P=0.0413).Th
erew
asno
significantd
ifference
insurvivalun
tildischargeo
rGOSou
tcom
e
Dam
ianetal.,
Circulation2004
[68]

16 Stroke Research and Treatment
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Thrombo
lytic
s
Apilotrando
mized
trialof
thrombo
lysis
incardiaca
rrest
(theT
ICAtrial)
Rand
omized,
doub
le-blin
d,placebo
controlled,sin
gle-center,
feasibilitytrialfor
out-o
f-hospitalcardiac
arrest
Tenecteplase
50mgIV×
1(N
=19)
Placebo
(N=16)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
survivalto
ED,ICU
and
hospita
ldisc
harge
ROSC
in42%of
tenecteplase
and6%
ofplacebogrou
p.No
differenceinsurvivalto
hospita
ldisc
harge
Fatovich
etal.,
Resuscitatio
n2004
[69]
Thrombo
lysis
durin
gresuscitatio
nfor
out-o
f-hospitalcardiac
arrest
Rand
omized,
doub
le-blin
d,controlled,
multic
enterstudy
ofou
t-of-h
ospitalcardiac
arrest
Tenecteplase
0.5m
g/kg
IV(N
=525)
Placebo
(N=525)
Prim
aryou
tcom
e:survival
at30
days
Second
aryou
tcom
es:
survivalto
admiss
ion,
ROSC
,24-ho
ursurvival,
survivalto
discharge,
cerebralperfo
rmance
score
atdischarge
Nodifferencein30-day
survival,hospital
admission,
ROSC
,24-ho
ursurvival,disc
harge,or
neurologicou
tcom
e.More
intracranialhemorrhages
intre
atmentg
roup
Bottigere
tal.,NEJM
2008
[70]
Steroids
andpressors
Vasopressin
,epineph
rine,and
corticosteroidsfor
In-hospital
cardiaca
rrest
Rand
omized,
doub
le-blin
d,placebo-controlled,
single-center
study
Vasopressin
20IU
IV+
epinephrine1
mgIV
+methylpredn
isolone
40mgIV
follo
wed
byhydrocortison
e(N
=48)
Epinephrine+
placebo
(N=52)
Prim
aryou
tcom
e:RO
SC,
survivalto
discharge
Second
aryou
tcom
es:blood
pressure
after
CPR,
organ
failu
re-fr
eedays,disc
harge
Glasgow
-Pittsburgcerebral
perfo
rmance
scale
MoreR
OSC
intre
atment
grou
p(81%
versus
52%,P
=0.003)
andmores
urvivalto
discharge(19%versus
4%,P
=0.02)
Mentzelop
oulose
tal.,
ArchIntern
Med
2009
[71]
Pressors
Acomparis
onof
standard-dosea
ndhigh
-dose
epinephrineincardiaca
rrest
outside
theh
ospital
Rand
omized,
doub
le-blin
d,prospective,
multi-center
study
Epinephrine0
.2mg/kg
IV(N
=64
8)
Epinephrine
0.02
mg/kg
IV(N
=632)
Prim
aryou
tcom
e:return
ofspon
taneou
scirc
ulation
(ROSC
),admissionto
the
hospita
lSecond
aryou
tcom
e:cerebralperfo
rmance
scale
atadmission,
anddischarge
NodifferenceinRO
SCrates,admiss
ion,
survival,
ordischargen
eurological
status
Brow
netal.,NEJM
1992
[72]
Standard
dosesv
ersus
repeated
high
doseso
fepinephrineincardiaca
rrest
outside
theh
ospital
Rand
omized,
doub
le-blin
d,prospective,
single-center
study
Repeated
epinephrine
5mgIV
(N=271)
Repeated
epinephrine
1mgIV
(N=265)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
admissionto
theh
ospital,
discharge,cerebral
perfo
rmance
category
atdischargea
nd6mon
ths
NodifferenceinRO
SC,
admission,
discharge,or
6-mon
thneurological
outcom
es
Chou
xetal.,
Resuscitatio
n1995
[73]

Stroke Research and Treatment 17
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Arand
omized,dou
ble-blind
comparis
onof
metho
xamine
andepinephrineinhu
man
cardiopu
lmon
aryarrest
Rand
omized,
doub
le-blin
d,sin
gle-center
study
Metho
xamine4
0mg
bolusIVthen
40mg4
minutes
later
(N=77)
Epinephrine
2mgbo
lusthen
2mgIV
q4m
in(N
=68)
Prim
aryou
tcom
e:Mortalityand
Glasgow
-Pittsburgh
coma
score
Second
aryou
tcom
es:
ROSC
,successful
resuscitatio
n
NodifferenceinRO
SCor
neurologicou
tcom
e,initial
resuscitatio
n,or
survivalto
discharge
Patricketal.,
Am
JRespirC
ritCa
reMed
1995
[74]
Rand
omise
dcomparis
onof
epinephrinea
ndvasopressin
inpatie
ntsw
ithou
t-of-h
ospitalventricular
fibrillatio
n
Rand
omized,
doub
le-blin
d,sin
gle-center,con
trolled
study
ofou
t-of-h
ospital
ventric
ular
fibrillatio
npatie
ntsw
hofailed
defib
rillation
Vasopressin
40IU
IV(N
=20)
Epinephrine
1mgIV
(N=20)
Prim
aryou
tcom
e:survival
toadmission
Second
aryou
tcom
e:24-hou
rsurvival,survival
todischarge,GCS
atdischarge
Nosig
nificantd
ifference
insurvivalto
admiss
ionbu
tmorev
asop
ressin
patients
survived
24ho
urs(60%
versus
20%,P
=0.02).No
differenceinsurvivalto
dischargeo
rGCS
atdischarge
Lind
nere
tal.,
Lancet1997
[75]
High-do
seversus
standard-dosee
pineph
rine
treatmento
fcardiac
arrest
after
failu
reof
stand
ard
therapy
Rand
omized,con
trolled,
single-blind,multic
enter
study
ofpatientsw
hohadfailedon
stand
ard
dose
ofepinephrine
0.5–1.0
mgIV
Epinephrine0
.1mg/kg
IVup
to4do
ses
(N=78)
Epinephrine
0.01mg/kg
IVup
to4do
ses
(N=62)
Prim
aryou
tcom
e:im
provem
entincardiac
rhythm
orRO
SCSecond
aryou
tcom
es:G
CSat6,24,and
72ho
urs
Nodifferences
inRO
SC,
survival,orn
eurologic
functio
nbetweengrou
ps
Sherman
etal.,
Pharmacotherarpy1997
[76]
Acomparis
onof
repeated
high
dosesa
ndrepeated
standard
doseso
fepineph
rine
forc
ardiac
arrestou
tside
the
hospita
l
Rand
omized,con
trolled,
prospectivem
ultic
enter
study
Epinephrine5
mgIV
upto
15do
sesa
t3-m
inute
intervals
(N=1677)
Epinephrine
1mgIV
upto
15do
sesa
t3-minute
intervals
(𝑀=1650)
Prim
aryou
tcom
e:RO
SC,
admissionto
theh
ospital,
numbero
fadm
issions
after
asingled
oseo
fepinephrine,ho
spita
ldischarge
Second
aryou
tcom
es:
survival,neurological
outcom
ebyGCS
and
cerebralperfo
rmance
scale
Sign
ificantlymoreR
OSC
inhigh
dose
grou
p(40%
versus
36%of
control
grou
p,P=0.02)a
ndmore
survivalto
admiss
ion
(26.5%
versus
23.6%of
controls,
P=0.05).No
differenceinsurvivalto
dischargeo
rneurological
status
Gueug
niaudetal.,
NEJM
1998
[77]
Vasopressin
versus
epinephrinefor
inho
spita
lcardiaca
rrest:ar
ando
mized
controlledtrial
Rand
omized,con
trolled,
triple-blin
d,multic
enter
study
ofin-hospital
cardiaca
rrestfor
asystole,
PEA,or
refractory
ventric
ular
fibrillatio
n
Vasopressin
40IU
IV(firstp
ressor)
(N=104)
Epinephrine
1mgIV
(first
pressor)
(N=96)
Prim
aryou
tcom
e:survival
for1
hour
Second
aryou
tcom
es:
survivalto
hospita
ldischarge,mod
ified
mini-m
entalstateexam
atdischarge,cerebral
perfo
rmance
scorea
tdischarge,RO
SC,adverse
events
Nodifferenceinsurvivalat
1hou
rorsurvivalto
hospita
ldisc
harge.No
differenceinmini-m
ental
statee
xam
scores
orcerebralperfo
rmance
scores
Stielletal.,
Lancet2001
[78]

18 Stroke Research and Treatment
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Acomparis
onof
vasopressin
andepinephrinefor
out-o
f-hospital
cardiopu
lmon
ary
resuscitatio
n
Rand
omized,con
trolled,
multic
enterstudy
ofou
t-of-h
ospitalcardiac
arrestwith
ventric
ular
fibrillatio
nfailing
defib
rillation,
PEA,or
asystole
Vasopressin
40IU
IV×2
dosesm
axim
um(N
=589)
Epinephrine
1mgIV×2
dosesm
axim
um(N
=597)
Prim
aryou
tcom
e:survival
toho
spita
ladm
ission
Second
aryou
tcom
es:
survivalto
hospita
ldischarge,cerebral
perfo
rmance
scorein
survivors
Nodifferenceinsurvivalto
admiss
ionam
ongpatie
nts
with
ventric
ular
fibrillatio
nor
PEA.H
igherrates
ofho
spita
ladm
issionfor
asystolein
vasopressin
grou
p(29%
versus
20%,P
=0.02)and
hospita
ldisc
harge
(4.7%versus
1.5%with
epinephrine,P=0.04).
Patie
ntsw
horeceived
rescue
epinephrinea
fter
vasopressin
hadbette
rsurvivalto
admissionand
dischargethanthe
epinephrinea
lone
grou
p.Nodifferenceincerebral
perfo
rmance
Wenzeletal.,
NEJM
2004
[79]
Vasopressin
andepinephrine
versus
epinephrinea
lone
incardiopu
lmon
ary
resuscitatio
n
Rand
omized,con
trolled,
multic
entertria
l
Epinephrine1
mgIV
+Va
sopressin
40IU
IV(N
=1442)
Epinephrine
1mgIV
+Placebo
(N=1452)
Prim
aryou
tcom
e:Survival
toho
spita
ladm
ission
Second
aryou
tcom
es:
ROSC
,survivaltoho
spita
ldischarge,good
neurologicalrecovery
bycerebralperfo
rmance
scale,
andGCS
,1-yearsurvival
Nodifferences
insurvival
toadmiss
ion,
ROSC
,survivalto
discharge,1-y
ear
survival,org
ood
neurologicrecovery
Gueug
niaudetal.,
NEJM
2008
[80]
Magnesiu
m
Rand
omise
dtrialof
magnesiu
min
in-hospital
cardiaca
rrest(MAG
ICtrial)
Rand
omized,
placebo-controlled,
single-center
study
ofcardiaca
rrestintheICU
orgeneralw
ard
Magnesiu
m2g
IVbo
lus
then
8gover
24ho
urs
(N=76)
Placebo
(N=80)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
24-hou
rsurvival,survival
toho
spita
ldisc
harge,GCS
,anddischargeK
arno
fsky
NodifferenceinRO
SC,
24-hou
rsurvival,survival
todischarge,or
GCS
Theletal.,
Lancet1997
[81]

Stroke Research and Treatment 19
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Magnesiu
min
cardiaca
rrest
(theM
AGIC
trial)
Rand
omized,
doub
le-blin
d,placebo-controlled,
single-center
study
ofou
t-of-h
ospitalcardiac
arrest
MgSO
45g
IV×1
(N=31)
Placebo
(N=36)
Prim
aryou
tcom
e:EC
Grhythm
2minutes
after
drug
,ROSC
Second
aryou
tcom
es:
survivalto
ED,ICU
,and
hospita
ldisc
harge
Nodifferences
inRO
SCor
survival
Fatovich
etal.,
Resuscitatio
n1997
[82]
Magnesiu
msulfatein
the
treatmento
frefractory
ventric
ular
fibrillatio
nin
the
prehospitalsettin
g
Rand
omized,
doub
le-blin
d,placebo-controlled,
multic
enterstudy
ofprehospitalventricular
fibrillatio
nrefractory
to3shocks
MgSO
42g
IV×1
(N=58)
Placebo
(N=58)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
admiss
ionto
hospita
l,ho
spita
ldisc
harge
NodifferenceinRO
SC,
survivalto
admiss
ionor
discharge
Allegrae
tal.,
Resuscitatio
n2001
[83]
Arand
omized
trialto
investigatethe
efficacy
ofmagnesiu
msulphatefor
refractory
ventric
ular
fibrillatio
n
Rand
omized,
doub
le-blin
d,placebo-controlledtrial
ofventric
ular
fibrillatio
nrefractory
to3shocks
MgSO
42–4g
IV×1
(N=52)
Placebo
(N=53)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
e:ho
spita
ldisc
harge
Nodifferences
inRO
SCor
survivalto
discharge
Hassanetal.,
EmergMed
J2002[84]
Rand
omized
clinicaltria
lof
magnesiu
m,diazepam,or
both
after
out-o
f-hospital
cardiaca
rrest
Rand
omized,
doub
le-blin
d,placebo-controlled
factoriald
esignstu
dy
Tier
1:magnesiu
m2g
IV+placebo
(N=75)
Tier
2:diazepam
10mg
IV+placebo
(N=75)
Tier
3:magnesiu
m2g
IV+Diazepam
10gIV
(N=75)
Placeboon
ly(N
=75)
Prim
aryou
tcom
e:aw
akeningat3mon
ths
(com
prehensib
lespeech
andcommandfollo
wing)
Second
aryo
utcome:days
toaw
akening,days
todeath,
independ
entat3
mon
ths
Nodifferencein
neurologicalou
tcom
ebetweenthe3
grou
ps
Long
strethetal.,
Neurology
2002
[85]
Insulin
Intravenou
sglucose
after
out-o
f-hospital
cardiopu
lmon
aryarrest:
acommun
ity-based
rand
omized
trial
Rand
omized,
single-center
controlled
study
5%dextrose
(D5W
)infusio
n(N
=374)
0.45
salin
einfusio
n(N
=374)
Prim
aryou
tcom
e:commandfollo
wingor
comprehensib
lespeech
Second
aryou
tcom
es:
survivalto
hospita
ladmissionanddischarge
Nodifferencein
neurologicalou
tcom
es,or
survivalto
admiss
ionor
discharge
Long
strethetal.,
Neurology
1993
[86]

20 Stroke Research and Treatment
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Stric
tversusm
oderateg
lucose
controlafte
rresuscitatio
nfro
mventric
ular
fibrillatio
n
Rand
omized,con
trolled,
multic
enterstudy
ofou
t-of-h
ospital
ventric
ular
fibrillatio
ncardiaca
rrest
Stric
tglucose
control
(4–6
mmol/L)w
ithinsulin
infusio
n×48
hours
(N=39)
Mod
erate
glucosec
ontro
l(6–8
mmol/L)
with
insulin
infusio
n×48
hours
(N=51)
Prim
aryou
tcom
e:30-day
all-c
ause
mortalityaft
erRO
SCSecond
aryou
tcom
es:
neuron
-specific
enolase
levelsat24
and48
hours
Nodifferencein30-day
mortality
Oksanen
etal.,Intensive
Care
Med
2007
[87]
Hypotherm
ia
Treatm
ento
fcom
atose
survivorso
fout-of-h
ospital
cardiaca
rrestw
ithindu
ced
hypo
thermia
Rand
omized,con
trolled,
single-blind,prospective
study
Hypotherm
ia33∘
C×12h
(N=43)
Normotherm
ia37∘
C(N
=34)
Prim
aryou
tcom
e:discharged
isposition
Second
aryou
tcom
es:
adversee
vents,
hemod
ynam
icparameters
Goo
ddischarged
isposition
in49%of
treatmentg
roup
comparedto
26%of
norm
otherm
iagrou
p(P
=0.04
6).N
odifferencein
adversee
vents
Bernardetal.,NEJM
2002
[88]
Mild
therapeutic
hypo
thermia
toim
provethe
neurologic
outcom
eafterc
ardiac
arrest
Rand
omized,con
trolled,
single-blind,multic
enter,
prospectives
tudy
Hypotherm
ia32–34∘C×
24h
(N=137)
Normotherm
ia37∘
C(N
=138)
Prim
aryou
tcom
e:6mon
thneurologicou
tcom
eusin
gPittsbu
rghcerebral
perfo
rmance
scale
Second
aryou
tcom
e:6-mon
thmortality,
complications
at7days
Hypotherm
iagrou
phad
morefavorable
neurologicalou
tcom
eat6
mon
ths(55%versus
39%of
norm
otherm
iagrou
p,P=
0.00
9).L
essd
eath
inhypo
thermiagrou
p(41%
versus
55%in
norm
otherm
iagrou
p,P=
0.02).Nodifferencein
complicationrates
Theh
ypotherm
iaaft
ercardiaca
rreststudy
grou
p,NEJM
2002
[89]
Pilotrando
mized
clinicaltria
lof
prehospitalind
uctio
nof
mild
hypo
thermiain
out-o
f-hospitalcardiac
arrest
patie
ntsw
ithar
apid
infusio
nof
4degreesC
norm
alsalin
e
Rand
omized,con
trolled,
safetyandfeasibility
study
ofou
t-of-h
ospital
cardiaca
rrest
2L4∘Cno
rmalsalin
einfusio
n(N
=63)
Standard
care
(N=62)
Prim
aryou
tcom
e:esop
hagealtemperature,
adversee
vents
Second
aryou
tcom
es:
awakening,ho
spita
ldischarge
Sign
ificant
differences
intemperature
between
grou
ps(P<0.001).N
odifferenceinaw
akeningor
hospita
ldisc
harge
Kim
etal.,
Circulation2007
[90]
Prehospitaltherapeutic
hypo
thermiaforc
omatose
survivorso
fcardiac
arrest:
arand
omized
controlledtrial
Rand
omized
controlled
trailofo
ut-of-h
ospital
cardiaca
rrest
4∘CRingerssolution
30mL/kg
totarget
temperature
33∘
C(N
=19)
Con
ventional
fluid
therapy
(N=18)
Prim
aryou
tcom
e:nasoph
aryn
geal
temperature
Second
aryou
tcom
es:
hospita
lmortalityand
cerebralperfo
rmance
scale
Lower
core
temperature
inthetreatmentg
roup
(P<
0.001).N
odifferencein
safety,m
ortality,or
neurologicou
tcom
e
KAmArA
inen
etal.,
ActaAnaesthesiolScand
2009
[91]

Stroke Research and Treatment 21
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Intra-arresttransnasal
evaporativec
oolin
g:a
rand
omized,preho
spita
l,multic
enterstudy
(PRINCE
:pre-rosc
intranasalcooling
effectiv
eness)
Rand
omized,con
trolled,
prospective,
single-blind,multic
enter
study
foro
ut-of-h
ospital
arrest
Intra-arrestintranasal
coolingwith
RhinoC
hill
device
+coolingat
hospita
larrivalto
34∘
C(N
=93)
Standard
care
with
coolingat
hospita
larrival
to34∘
C(N
=101)
Prim
aryOutcome:adverse
events,
leng
thof
stay,
mechanicalventilation
days,R
OSC
,survivalto
discharge,discharge
Pittsbu
rghcerebral
perfo
rmance
scale.
Timetotargettemperature
was
shorterinthe
intranasalcoolinggrou
p(P
=0.03).Nodifferencein
ROSC
,survivalofadm
itted
patie
nts,or
neurologic
outcom
eatd
ischarge
Castren
etal.,
Circulation2010
[92]
Chestcom
pressio
nsAcomparis
onof
activ
ecompressio
n-decompressio
ncardiopu
lmon
ary
resuscitatio
nwith
stand
ard
cardiopu
lmon
ary
resuscitatio
nforc
ardiac
arrests
occurringin
the
hospita
l
Rand
omized,con
trolled,
singlec
enterstudy
CPRusingsuction
device
(Ambu
CardioPu
mp)
(N=29)
Standard
CPR
(N=33)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
24-hou
rsurvival,ho
spita
ldischarge,GCS
at24
hours
ROSC
occurred
in62%of
treatmentg
roup
versus
30%of
controlgroup
(P<
0.03)a
nd45%of
treatment
grou
psurvived
24ho
urs
comparedto
9%of
control
grou
p(P<0.00
4).G
CSat
24ho
ursw
asbette
rinthe
treatmentg
roup
(P<0.02)
Coh
enetal.,
NEJM
1993
[93]
TheO
ntario
TrialofA
ctive
Com
pressio
n-Decom
pressio
nCa
rdiopu
lmon
ary
Resuscitatio
nforIn-Hospital
and
PrehospitalC
ardiac
Arrest
Rand
omized,
single-blind,multic
enter
controlledtrialof
prehospitaland
in-hospitalcardiac
arrest
Activ
ecom
pressio
n-decompressio
nCP
Rusingas
uctio
ndevice
(N=906)
Standard
CPR
(N=878)
Prim
aryou
tcom
e:survival
for1
hour
Second
aryou
tcom
e:survivalto
hospita
ldischarge,mod
ified
mini-m
entalstateexam
,cerebralperfo
rmance
scale
Nodifferences
insurvival
at1h
our,survivalun
tilho
spita
ldisc
hargeo
rmini-m
entalstateexam
for
either
prehospitalor
in-hospitalarrest
Stielletal.,
JAMA1996
[94]
Cardiopu
lmon
ary
resuscitatio
nby
chest
compressio
nalon
eorw
ithmou
th-to
-mou
thventilatio
n
Rand
omized
controlled
study
ofou
t-of-h
ospital
cardiaca
rrest
Bysta
nder
chest
compressio
nplus
mou
thto
mou
thresuscitatio
n(N
=279)
Bysta
nder
chest
compressio
nsalon
e(N
=241)
Prim
aryou
tcom
e:survival
toho
spita
ldisc
harge
Second
aryou
tcom
es:
admissionto
theh
ospital,
neurologicalstatus
Similaro
utcomew
ithbystanderc
hest
compressio
nsalon
eversus
chestcom
pressio
nswith
mou
thto
mou
th
Hallstrom
etal.,
NEJM
2000
[95]
Con
stant
flowinsufflations
ofoxygen
asthes
olem
odeo
fventilatio
ndu
ring
out-o
f-hospitalcardiac
arrest
Rand
omized,con
trolled
study
ofou
t-of-h
ospital
cardiaca
rrest
Con
stant
flow
insufflations
ofoxygen
(N=487)
Standard
endo
tracheal
intubatio
nand
mechanical
ventilatio
n(N
=457)
Prim
aryou
tcom
e:survival
toICUdischarge
Second
aryou
tcom
es:
ROSC
,survivaltoho
spita
ladmission,
spO
2>70%
NodifferenceinRO
SC,
hospita
ladm
issionor
ICU
discharge.HigherO
2satsin
continuo
usflo
winsufflationgrou
p
Bertrand
etal.,Intensive
Care
Med
2006
[96]
Com
pressio
n-on
lyCP
Ror
stand
ardCP
Rin
out-o
f-hospitalcardiac
arrest
Rand
omized,con
trolled,
multic
enterstudy
ofou
t-of-h
ospitalcardiac
arrest
Com
pressio
non
lyCP
R(N
=620)
Standard
CPR
(N=656)
Prim
aryou
tcom
e:30
day
survival
Second
aryou
tcom
es:1
day
survival,R
OSC
,survivalto
hospita
ldisc
harge
Similar3
0-daysurvival,
1-day
survivalandsurvival
toho
spita
ldisc
harge
Svensson
etal.,
NEJM
2010
[97]

22 Stroke Research and Treatment
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
CPRwith
chestcom
pressio
nalon
eorw
ithrescue
breathing
Rand
omized,con
trolled,
multic
enterstudy
ofou
t-of-h
ospitalcardiac
arrest
Chestcom
pressio
nsalon
e(N
=981)
Chest
Com
pressio
ns+
Rescue
breathing(2
breathsto15
chest
compressio
ns)
(N=960)
Prim
aryou
tcom
e:survival
toho
spita
ldisc
harge
Second
aryou
tcom
es:
dischargec
erebral
perfo
rmance
Score,
ROSC
Nodifferenceinsurvivalto
hospita
ldisc
hargeo
rin
neurologicou
tcom
e.Trend
towardim
proved
survival
atdischargeinthosew
ithcardiacc
ause
ofarrestand
shockabler
hythm
(P=
0.09)
Reae
tal.,
NEJM
2010
[98]
Atrialofanim
pedance
thresholddevice
inou
t-of-h
ospitalcardiac
arrest
Rand
omized,con
trolled,
doub
le-blin
ded,
multic
enterstudy
ofou
t-of-h
ospitalcardiac
arrest
Impedancethresho
lddevice
(ITD
)which
increasin
gnegativ
eintratho
racicp
ressure
andim
proves
cardiac
output
(N=4373)
Sham
ITD
(N=4345)
Prim
aryou
tcom
e:survival
toho
spita
ldisc
hargew
ithmRS
0–3
Second
aryou
tcom
es:
survivalto
EDadmiss
ion,
hospita
ladm
issionand
hospita
ldisc
harge,adverse
events
Nodifferenceinsurvival
with
good
mRS
Aufderheidee
tal.,
NEJM
2011[99]
Adenosinea
ntagon
ist
Aminop
hylline
inbradyasysto
liccardiaca
rrest:a
rand
omized
placebo-controlledtrial
Rand
omized,
placebo-controlled,
doub
le-blin
d,multic
enterstudy
ofasystoleandPE
Aarrest
unrespon
siveto
epinephrinea
ndatropine
Aminop
hylline
250m
g(N
=486)
Placebo
(N=485)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
duratio
nof
ROSC
,survival
toadmiss
ion,
survivalto
discharge,len
gthof
stay,
24-hou
rtachyarrhythm
ias,
24-hou
rseizures,1-y
ear
neurologicou
tcom
eby
GCS
,Glasgow
-Pittsburgh
cerebralandoverall
perfo
rmance
scales,
mod
ified
mini-m
entalstate
exam
,fun
ctionalstatus
questio
nnaire
NodifferenceinRO
SC.
Moretachyarrhythm
iasin
thetreatmentg
roup
.Survivalto
hospita
ladmissionandsurvivalto
dischargew
eren
otdifferent
Abu-Labanetal.,Lancet
2006
[100]
Fluidmanagem
ent
Capillary
leakagein
postc
ardiac
arrestsurvivors
durin
gtherapeutic
hypo
thermia:a
prospective,
rand
omized
study
Rand
omized,con
trolled
study
7.2%hyperton
icsalin
ewith
6%po
lysta
rch
solutio
n×24
hours
(N=10)
Standard
Fluid
(Ringer’s
acetate)×24
hours
(N=9)
Prim
aryou
tcom
e:am
ount
offlu
idadministered
in24
hours
Second
aryou
tcom
e:MRI
vasogenice
dema
Thetreatmentg
roup
requ
iredsig
nificantly
less
fluid
than
thec
ontro
lgrou
p.Th
erew
asno
differenceinMRI
brain
edem
a
Heradstv
eitetal.,Scand
JTraum
aResuscE
merg
Med
2010
[101]

Stroke Research and Treatment 23
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Barbitu
rate
Rand
omized
clinicalstudy
ofthiopentalloadingin
comatoses
urvivorsof
cardiac
arrest
Rand
omized,con
trolled,
multic
enterstudy
Thiopental30
mg/kg
IVload
(N=131)
Standard
therapy(N
=131)
Prim
aryou
tcom
e:Pittsbu
rghcerebral
Perfo
rmance
scalea
t6and
12mon
ths
Second
aryou
tcom
es:best
neurologicalperfo
rmance
ever
obtained
durin
gfollo
wup
,tim
etorecovery
Nodifferencein
neurologicalou
tcom
eor
mortalitybetweengrou
ps
BrainRe
suscitatio
nClinicalTrialI
Stud
yGroup
.NEJM
1986
[102]
Calcium
Calcium
chlorid
e:reassessmento
fuse
inasystole
Rand
omized,
doub
le-blin
d,placebo-controlledstu
dyin
prehospitalasysto
liccardiaca
rrestrefractory
toepinephrine,
bicarbon
ate,and
atropine
Calcium
chlorid
e(N
=18)
Placebo
(N=14)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
e:ho
spita
ldisc
harge
NodifferenceinRO
SCStuevenetal.,
Ann
EmergMed
1984
[103]
Thee
ffectivenesso
fcalcium
chlorid
einrefractory
electromechanical
dissociatio
n
Rand
omized,blin
ded,
placebo-controlledstu
dyof
prehospitalP
EAarrest
refractory
toepinephrinea
ndbicarbon
ate
Calcium
chlorid
e(N
=48)
Placebo
(N=42)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
survivalto
hospita
ldischarge
NodifferenceinRO
SCbu
tsubgroup
ofpatie
ntsw
ithwidened
QRS
didhave
moreR
OSC
incalcium
grou
p(P
=0.028)
Stuevenetal.,
Ann
EmergMed
1985
[104]
Lack
ofeffectiv
enesso
fcalcium
chlorid
einrefractory
asystole
Rand
omized,blin
ded,
placebocontrolled
study
ofprehospital
asystolic
cardiaca
rrest
refractory
toepinephrine,
bicarbon
ate,and
atropine
Calcium
chlorid
e(N
=39)
Placebo
(N=34)
Prim
aryou
tcom
e:RO
SCSecond
aryou
tcom
es:
survivalto
hospita
ldischarge
NodifferenceinRO
SCor
hospita
ldisc
harge
Stuevenetal.,
Ann
EmergMed
1985
[105]
Sodium
bicarbon
ate
Buffertherapy
durin
gou
t-of-h
ospital
cardiopu
lmon
ary
resuscitatio
n
Rand
omized,
doub
le-blin
d,placebo-controlledstu
dyof
out-o
f-hospital
asystoleor
ventric
ular
fibrillatio
nrefractory
tofirstdefib
rillation
attempt
Sodium
bicarbon
ate
250m
LIV×1
(N=245)
Placebo
(N=257)
Prim
aryou
tcom
e:survival
toICUadmiss
ion,
survival
toho
spita
ldisc
harge
Nodifferenceinsurvivalto
ICUadmissionor
hospita
ldischarge
Dybviketal.,
Resuscitatio
n1995
[106]

24 Stroke Research and Treatment
Table2:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Outcomem
easure
Results
Reference
Sodium
bicarbon
ateimproves
outcom
einprolon
ged
prehospitalcardiac
arrest
Rand
omized,
doub
le-blin
d,placebo-controlledtrial
ofprehospitalcardiac
arrest
Sodium
bicarbon
ate
(1meq/kg)
IV×1
(N=175)
Placebo
(N=155)
Prim
aryou
tcom
e:survival
toED
Second
aryou
tcom
es:
ROSC
Nodifferenceinsurvivalto
EDadmiss
ionor
ROSC
.Be
ttersurvivalw
ithbicarbon
ateinthe
prolon
ged(>15
minute)
arrestgrou
p(P
=0.007)
Vukm
irandKa
tz,A
mJ
EmergMed
2006
[107]
Hem
ofiltration
High-volumeh
emofi
ltration
after
out-o
f-hospitalcardiac
arrest:
arando
mized
study
Rand
omized,con
trolled
trialofo
ut-of-h
ospital
ventric
ular
fibrillatio
nor
asystolecardiaca
rrest
Tier
1:hemofi
ltration
(200
mL/kg/h)o
ver8
hours
(N=20)
Tier
2:hemofi
ltration
plus
hypo
thermiato
32∘
C×24
hours
(N=22)
Standard
care
(N=19)
Prim
aryou
tcom
e:survival
at6mon
ths
Second
aryou
tcom
e:intractables
hock,
Pittsbu
rghcerebral
perfo
rmance
scale
Sign
ificantlybette
rsurvival
comparedto
controlin
hemofi
ltrationgrou
p(P
=0.026)
andhemofi
ltration
plus
hypo
thermiagrou
p(P
=0.018).N
odifferencein
6-mon
thneurologic
outcom
e
Laurentetal.,
JAm
CollC
ardiol2005
[108]
Rhythm
analysis
Early
versus
laterrhythm
analysisin
patie
ntsw
ithou
t-of-h
ospitalcardiac
arrest
Clusterrando
mized,
controlled,multic
enter
study
ofou
t-of-h
ospital
cardiaca
rrest
Early
rhythm
analysis:
30–6
0second
sofE
MS
CPRfollo
wed
byEC
Ganalysis
(N=5290)
Laterrhythm
analysis:
180
second
sofE
MS
CPRfollo
wed
byEC
Ganalysis
(N=46
43)
Prim
aryou
tcom
e:survival
toho
spita
ldisc
hargew
ithmRS
0–3
Second
aryou
tcom
es:
survivalto
discharge,
survivalto
hospita
ladmiss
ion,
ROSC
Nodifferenceinou
tcom
ebetweenab
riefand
longer
perio
dof
CPRbefore
ECG
analysisof
rhythm
Stielletal.,
NEJM
2011[109]

Stroke Research and Treatment 25
tested an intervention published in English between 1980and 2012, were included. Only trials examining mortality orneurologic outcome as a primary or secondary endpoint werereviewed. Only trials specific to SAH (not trials that includedother neurocritical diagnoses or brain injury diagnoses) wereincluded. Cardiac arrest trials included both out-of-hospitaland in-hospital arrest and all arrest rhythms were included.Post hoc analyses of preexisting trials were not reviewed. Ifphase III results of a trial were available, earlier phases of thesame trial were not included in analysis unless the patientpopulation or methodology differed substantially.
A PubMed search of the term “subarachnoid hemor-rhage” and “neurologic outcome” with the limits of human,age > 18, English and randomized, controlled trial yielded23 results. A PubMed search of the term “subarachnoidhemorrhage” and “mortality” with the limits of human,age > 18, English and randomized, controlled trial yielded78 results. An additional review of articles identified by abroader search of “subarachnoid hemorrhage” with the limitsof human, age > 18, English and randomized, controlledtrial yielded 244 results. Review of these studies yielded 57aneurysmal SAH trials that met inclusion criteria and wereanalyzed. A pubmed search of the terms “cardiac arrest” and“neurologic outcome” with the limits of human, English, age> 18 and randomized, controlled trial yielded 21 results. APubMed search of the terms “cardiac arrest” and “mortality”with the limits of human, English, age > 18 and randomized,controlled trial yielded 197 results. Review of these studiesyielded 46 cardiac arrest trials that met inclusion criteria andwere analyzed.
Clinicaltrials.govwas searched for ongoing interventionaltrials in cardiac arrest and aneurysmal subarachnoid hemor-rhage. Only ongoing studies that were open and recruitingor preparing to recruit were included. Terminated studieswere excluded from review. A search of ongoing studies onclinicaltrials.gov for the term “subarachnoid hemorrhage”,limited to interventional studies of adults ≥18 years old,produced 86 results and a search for the term “cardiac arrest”limited to interventional studies of adults with neurologicoutcomes produced 46 results. Of these, 25 ongoing SAHtrials and 14 cardiac arrest trials met the criteria for review.
3. Results
3.1. Trials Analyzed. A total of 142 trials (82 SAH, 60 cardiacarrest) met review criteria. Of these, 103 were publishedin peer-reviewed journals and 39 were ongoing studies.Fifty-seven published randomized, controlled studies wereidentified in the SAH population and 46 in the cardiac arrestpopulation. These studies are reviewed in detail in Tables 1and 2. Additionally, 25 ongoing SAH trials and 14 ongoingcardiac trials were reviewed (Tables 3 and 4).
3.2. Interventions Studied. The main hypothetical mecha-nisms of intervention tested in published SAH trials wererelated to treating or preventing delayed cerebral ischemia(𝑁 = 40, 70%), preventing aneurysm rebleeding (𝑁 = 5,9%), improving aneurysm repair technique (𝑁 = 5, 9%),
improving fluid balance (𝑁 = 2, 4%), and others (𝑁 = 3, 5%).Among ongoing SAH trials, mechanisms of study includetreating or preventing delayed cerebral ischemia (𝑁 = 19,76%), limiting rebleeding (𝑁 = 1, 4%), improving aneurysmrepair (𝑁 = 1, 4%), seizure control (𝑁 = 2, 8%), and other(𝑁 = 2, 8%).There are no published or ongoing SAH clinicaltrials that focus on treating acute brain injury after aneurysmrupture.
Conversely, themainmechanisms of intervention studiedin published cardiac arrest trials focused on acute interven-tion to treat and limit early brain injury. All 46 (100%)published cardiac arrest trials focused on the acute timeframe (first few hours) after cardiac arrest. Interventionsstudied included decreasing cerebral metabolic demand withhypothermia or barbiturate (𝑁 = 6, 13%), high-quality chestcompressions or pressor use to return cerebral blood flow(𝑁 = 16, 35%), electrolyte/metabolic optimization withcalcium, magnesium, sodium bicarbonate or insulin admin-istration (𝑁 = 12, 26%), neuroprotective drugs includingcalcium channel blockers (𝑁 = 5, 11%), thrombolysis totreat the underlying cause of cardiac arrest (𝑁 = 2, 4%) andother (𝑁 = 5, 11%). Among ongoing cardiac arrest trials,mechanisms of study include decreasing cerebral metabolicdemand with hypothermia (𝑁 = 9, 64%), high-qualitychest compressions to return cerebral blood flow (𝑁 =2, 14%) electrolyte/metabolic optimization with magnesium(𝑁 = 1, 7%), neuroprotective drugs (𝑁 = 1, 7%), andmonitoring cerebral oxygenation (𝑁 = 1, 7%). A detailed listof interventions from published and ongoing studies in boththe SAH and cardiac arrest population are listed in Table 5.
3.3. Outcome Measures. The most common neurologicaloutcomes assessed in the SAH trials were delayed cerebralischemia (𝑁 = 24, 42%), functional outcome (Glasgowoutcome scale, modified Rankin scale or functional outcomescale, 𝑁 = 24, 42%), angiographic or transcranial Dopplervasospasm (𝑁 = 6, 11%), and death (𝑁 = 4, 7%). Amongcardiac arrest trials, the most often assessed neurologicaloutcomes were the Pittsburgh cerebral performance score(𝑁 = 18, 40%), Glasgow outcome score or modified RankinScore (𝑁 = 4, 9%), Glasgow coma score (𝑁 = 4, 9%),awakening and command following (𝑁 = 3, 7%), cognitive orneuropsychological testing (𝑁 = 1, 2%), “disability” (𝑁 = 1,2%), death (𝑁 = 13, 30%), discharge disposition (𝑁 = 1, 2%)and others (𝑁 = 1, 2%).
3.4. Trial Results. Of the clinical trials reviewed for SAH,30% (17/57) showed that the intervention tested had astatistically significant impact on neurological outcome ormortality. These include studies of nimodipine [4–6, 8, 110],phase II data for nicardipine implants during aneurysmclipping [13], the neuroprotectants edavarone [21] andnizofenone [20], pravastatin [25], early aneurysm surgery[28], endovascular coiling [29–31], cilostazol [41], methyl-prednisolone [44], erythropoietin [45], and fasudil [57, 58].Similarly, 30% (17/57) of studies showed a positive impact ondelayed cerebral ischemia, infarction, angiographic or TCDvasospasm, though there was incomplete overlap with the

26 Stroke Research and Treatment
Table3:Ra
ndom
ized
controlledtrialsassessingneurologicou
tcom
esaft
eraneurysm
alSubarachno
idhemorrhage—
ongoingtrials.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Statins
Statinsa
ndcerebralbloo
dflo
win
SAH
Rand
omized,
doub
le-blin
deffi
cacy
study
Simvasta
tin80
mg/d
for2
1days
Placebo
60
Prim
aryou
tcom
e:resting
CBFandautoregu
lation
7–10
days
after
SAH
Second
aryou
tcom
es:O
EFandCM
RO27–10
days
after
SAH
MichaelDiringer,
NCT
00795288
UsesP
ETto
understand
the
mechanism
ofsta
tinuseinvasospasm
Ther
oleo
fstatin
sin
preventin
gcerebral
vasospasm
second
aryto
subarachno
idhemorrhage
Rand
omized,
doub
le-blin
d,parallel
assig
nment
Simvasta
tin80
mgPO
qd×21
days
Placebo
80Prim
aryou
tcom
e:6-mon
thclinicaloutcome
EbervalF
igueire
do,
NCT
01346748
—
Use
ofsim
vastatin
forthe
preventio
nof
vasospasm
inaneurysm
alsubarachno
idhemorrhage
Rand
omized,
doub
le-blin
d,parallel
assig
nmentefficacy
trial
Tier
1:Simvasta
tin40
mg×21dor
Tier
2:Simvasta
tin80
mg×
21d
Placebo
150
Prim
aryou
tcom
e:21-day
GOS,mRS
,and
BarthelInd
exSecond
aryou
tcom
e:clinicalvasospasm
BenRo
itberg,
NCT
00487461
—
High-do
sesim
vastatin
for
aneurysm
alsubarachno
idhemorrhage(HDS-SA
H)
Rand
omized,parallel
assig
nment,
doub
le-blin
deffi
cacy
study
Simvasta
tin80
mgPO
×21
days
Simvasta
tin40
mgPO×21
days
240
Prim
aryou
tcom
e:delay
edisc
hemic
neurologicaldeficit
Second
aryOutcomes:
LFTs,rhabd
omyolysis
,3-mon
thmRS
,cost
effectiv
eness
GeorgeW
ong,
NCT
01077206
Therem
aybe
abiochemicaland
neurop
rotective
dose-related
relatio
nshipbetween
simvasta
tinand
delay
edisc
hemic
neurologicaldeficits.
Simvastatin
inaneurysm
alsubarachno
idhemorrhage
(STA
SH):
amultic
entre
rand
omise
dcontrolledclinicaltria
l
Rand
omized,
placebo-controlled,
doub
le-blin
dph
aseIII
trial
Simvasta
tin40
mgPO
qd×21
days
Placebo
1600
Prim
aryou
tcom
e:6-mon
thmRS
Second
aryou
tcom
e:need
andintensity
ofdelay
edisc
hemicdeficitrescue
therapy,incidencea
nddu
ratio
nof
delayed
ischemicdeficits,incidence
andseverityof
sepsis,
lengthof
stay,disc
harge
disposition
PeterK
irkpatrick,
NCT
00731627
Simvasta
tinmay
improveC
BFand
inflammation
follo
wingSA
H

Stroke Research and Treatment 27Ta
ble3:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Aneurysm
repair
Internationalsub
arachn
oid
aneurysm
trialII
comparin
gclinical
outcom
esof
Surgical
clipp
ingandendo
vascular
coiling
forrup
tured
intracranialaneurysm
snot
inclu
dedin
theo
riginal
ISAT
study
(ISA
TII)
Rand
omized,openlabel,
safety/efficacy
study
ofWFN
SI–IV
SurgicalClipping
Endo
vascular
Coilin
g1724
Prim
aryou
tcom
e:12-m
onth
mRS>2
Second
aryou
tcom
es:ICH
follo
wingtre
atment,failu
reof
aneurysm
occlu
sion,
all
causem
orbidityand
mortality,aneurysm
recurrence,hospitalization
>20
days
ordischarge
otherthanho
me,aneurysm
rebleed
Tim
Darsaut,M
axFind
lay,and
Jean
Raym
ond,
NCT
0166
8563
ISAT
inclu
ded
prim
arily
small
anterio
rcirc
ulation
aneurysm
s.Th
eop
timaltre
atmento
fotherlocations
and
sizes
ofaneurysm
sremains
uncle
arand
coiling
may
notb
eas
durablea
sclip
ping
Lipidperoxidatio
ninhibitor
Acetam
inop
henin
aSAHto
inhibitlipid
peroxidatio
nandcerebralvasospasm
Rand
omized,
doub
le-blin
d,placebo-controlled,
safety/efficacy
trial
Group
1:Ac
etam
inop
hen1g
q6
Group
2:NAC
IV0.5g
/hGroup
3:Ac
etam
inop
hen1g
q6+NAC
0.5g
/hGroup
4:Ac
etam
inop
hen1.5
gq6+NAC
0.5g
/h
Placebo
120
Prim
aryou
tcom
e:F2-IsoP
biom
arkersforlipid
peroxidatio
n.Second
aryou
tcom
e:vasospasm
andbrain
ischemiaas
assessed
byCT
A/CTP
orMRI
DWI
John
Oates,
NCT
00585559
Hem
oglobinreleased
from
lysedRB
Csoxidizes
and
generatesp
rotein
radicalsthatindu
celip
idperoxidatio
n.Metaboliteso
fperoxidatio
ns(F2-iso
prostanes)are
potent
vasoconstrictors.
Acetam
inop
hencan
inhibitthese
metabolitesa
ndNAC
caninhibitlipid
peroxidatio
nNeuroprotectiv
edrugs
Effectsof
tiopron
inon
3-am
inop
ropanalleveland
neurologicou
tcom
eafte
raneurysm
alSA
H
Rand
omized,
doub
le-blin
d,ph
ase2
bioavailability
Tiop
ronin
Placebo
60
Prim
aryou
tcom
e:serum
andCS
F3A
Plevels
Second
aryou
tcom
es:
12mon
thmRS
,Barthel,
Lawton,
NIH
SS,T
ICS
adversee
vents
ESand
erCon
nolly,
NCT
01095731
3APistoxic
metabolite
prod
uced
durin
gcerebral
ischemia.Itis
neutralized
bytio
pron
in
Lycopene
following
aneurysm
alsubarachno
idhaem
orrhage(LA
SH)
Rand
omized,
doub
le-blin
d,placebo-controlled,
efficacy
study
Lycopene
30mgPO
qd×21
days
Placebo
124
Prim
aryou
tcom
e:TC
Dvasospasm,durationof
impaire
dautoregu
latio
nmeasuredby
TCD
Second
aryOutcomes:LDL,
oxy-LD
L,CR
P,circulating
endo
thelialcells,
endo
thelialprogenitorc
ells
KarolB
udoh
oski,
NCT
00905931
Lycopene
isan
atural
antio
xidant
thatmay
redu
cevascular
injury
andinflammation
andlim
itvasospasm

28 Stroke Research and TreatmentTa
ble3:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Thrombo
lytic
s
Intraventricular
tPAin
the
managem
ento
faneurysmal
subarachno
idhemorrhage
Rand
omized,
placebo-controlled,
doub
le-blin
dsafetytrail
tPAintraventricular
q12h×5do
ses
Placebo
administered
q12h×5do
ses
12
Prim
aryou
tcom
e:HCT
rateandvaria
nceo
fventric
ular
andciste
rnal
clotclearance
Second
aryou
tcom
e:hemorrhagic
complications,
ventric
ulostomy-related
infections,T
CDvasospasm,
CTangiovasospasm,
symptom
aticvasospasm,
CSFcytokinesa
ndcoagulationmeasurements,
ICP,feverb
urden,
volume
ofCS
Fdrainage,6-m
onth
GOSE
andEu
roQOL
And
reas
Kram
er,
NCT
01098890
Intraventricular
TPA
may
accelerate
clearance
ofIV
Ham
eliorating
vasospasm,
hydrocephalus,and
ICP
Transfu
sion
Effecto
fred
bloo
dcell
transfu
sionon
brain
metabolism
inpatie
ntsw
ithSA
H
Openlabel
safety/efficacy
study
inSA
Hpatie
ntsw
ithHgb<
12.5g/dL
andDCI
,high
riskforv
asospasm
orangiograph
icvasospasm
Transfu
sionof
1unit
ofpacked
RBCover
1ho
urNA
48
Prim
aryou
tcom
e:percent
ofbrainregion
swith
low
oxygen
deliverybefore
and
1hou
rafte
rtransfusio
nSecond
aryou
tcom
es:
relatio
nshipof
oxygen
deliveryandangiograph
icvasospasm
MichaelDiringer,
NCT
00968227
UsesP
ETto
assessthe
relatio
nshipbetween
Hctandoxygen
deliveryin
SAH
patie
nts
Vasodilators
Sildenafilfor
preventio
nof
cerebralvasospasm
(SIPCE
VA)
Rand
omized,
doub
le-blin
d,placebo-controlled,
safetyandeffi
cacy
study
Tier
1:sildenafil
25mg
POTIDday3–14
after
SAH
Tier
2:sildenafil
50mgPO
TIDday3–14
after
SAH
Placebo
18
Prim
aryou
tcom
e:New
neurologicaldeficitdu
eto
vasospasm
upto
14days
after
SAH
Second
aryou
tcom
es:T
CDspasm,m
ortality,adverse
drug
effects,
leng
thof
stay,
dischargem
RS
And
reCerutti
Franciscatto,
NCT
01091870
—
Safetystu
dyof
dantrolene
inSA
H
Rand
omized,
doub
le-blin
dsafety
study
Dantro
lene
Placebo
30
Prim
aryou
tcom
e:tolerability,hypo
natre
mia
Second
aryou
tcom
es:liver
toxicity,hem
odyn
amics,
ICP,TC
D,ang
iographic
vasospasm
treatments,
90-day
GOS,mRS
,and
Barthel
Susann
eMuehlschlegel,
NCT
01024972
Dantro
lene
isa
muscle
relaxant
that
may
ameliorate
vascular
muscle
tone
andlim
itvasospasm

Stroke Research and Treatment 29Ta
ble3:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Safetyandph
armacokinetic
evaluatio
nof
nitrite
for
preventio
nof
cerebral
vasospasm
Rand
omized,
single-blind,parallel
assig
nmentsafetystu
dy
Tier
1:sodium
nitrite
32nm
ol/kg/min
Tier
2:sodium
nitrite
48nm
ol/kg/min
Tier
3:sodium
nitrite
64nm
ol/kg/min
Placebovehicle
18
Prim
aryou
tcom
e:ph
armacokineticso
f14-day
sodium
nitrite
infusio
nSecond
aryou
tcom
es:safety
andeffi
cacy
EdwardOldfield,
NCT
00873015
—
Effectsof
prostacyclin
infusio
non
cerebralvessels
andmetabolism
inpatie
nts
with
subarachno
idhemorrhage
Rand
omized,placebo
controlled,do
uble-blin
d,parallelassignm
ent,
pharmacod
ynam
ics
study
Tier
1:prostacyclin
1ng/kg/m
inday5–10
after
SAH
Tier
2:prostacyclin
2ng/kg/m
inday5–10
after
SAH
Placebo,IV
infusio
nday
5–10
after
SAH
90
Prim
aryou
tcom
e:vasospasm
measuredby
CTperfusion
Second
aryou
tcom
es:
cerebralmetabolism
measuredby
microdialysis,
3-mon
thGOS,clinical
vasospasm,brain
tissue
oxygen,C
Tangio
vasospasm,M
AP,serum
S100b
Rune
Rasm
ussen,
NCT
0144
7095
Prostacyclinmay
causev
asod
ilatio
nandam
eliorate
vasospasm
Hypertensive,hypervolem
ictherapy
Indu
cedhypertensio
nfor
treatmento
fdelayed
cerebralisc
hemiaaft
eraneurysm
alSA
HHIM
ALA
IA
Rand
omized,Single
blindsafety/efficacy
study
ofpatie
ntsw
ithSA
HandDCI
(clin
ically
defin
ed)
Indu
cedhypertensio
nwith
vasopressorsand
fluidsfor
48ho
urs
Noindu
ced
hypertensio
n240
Prim
aryou
tcom
e:mRS
at3
mon
ths
Second
aryou
tcom
es:
prop
ortio
nof
treated
patie
ntsw
hodidno
thave
clinicalimprovem
ento
fDCI
symptom
swith
in24
hours,30-day
mortality,
3-mon
thBa
rthel,SSQoL
,ho
spita
lanx
ietyand
depressio
nscale,cogn
itive
failu
resq
uestionn
aire,
hospita
lcom
plications,
CTPresults,m
edicalcosts
Arje
nSloo
tera
ndWalterv
andenBe
rgh,
NCT
01613235
CBFmeasuredin
all
patie
ntsu
singCT
Pat
enrollm
entand
24–36
hours
Intensivem
anagem
ento
fpressure
andvolume
expansionin
patie
ntsw
ithsubarachno
idhemorrhage
(IMPR
OVES
)
Rand
omized,
single-blind,factorial
assig
nment
Tier
1:hypervolem
ia+conventio
nalblood
pressure
Tier
2:no
rmovolem
ia+hypertensio
nTier
3:hypervolem
ia+
hypertensio
n
Normalvolume,
norm
albloo
dpressure
20
Prim
aryou
tcom
e:achievem
ento
fhemod
ynam
icgoalsineach
grou
p
Miriam
Treggiari,
NCT
01414894
Thou
ghtripleHisa
common
therapy,its
safetyandeffi
cacy
have
notb
eenwell
quantifi
ed

30 Stroke Research and Treatment
Table3:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
CSFdiversion
EARL
YDRA
IN:outcome
after
early
lumbarC
SF:
drainage
inaneurysm
alsubarachno
idhemorrhage
Rand
omized,2-arm
controlledtrial
Con
tinuo
uslumbar
CSFdrainage
of120m
gqd×7d
Standard
NICU
care
300
Prim
aryou
tcom
e:6-mon
thmRS
Second
aryou
tcom
es:
6-mon
thmortality,
angiograph
icvasospasm,
TCDvasospasm,shu
ntinsertionrateat6mon
ths
BardutzkyJ,
NCT
01258257
Lumbard
rainageto
removeb
lood
from
theb
asalciste
rnsm
aylim
itdelay
edcerebral
ischemia
Cerebrospinalflu
id(C
SF)
drainage
study
Rand
omized,openlabel,
parallelassignm
ent
study
ofSA
Hpatie
nts
requ
iring
external
ventric
ular
drainage
(EVD)
HighvolumeC
SFdiversion(EVDat
5mmHg)×10
days
Con
ventional
CSFdiversion
(EVDat
15mmHg),
weanedat
physician
discretio
n
20
Prim
aryou
tcom
e:90-day
mRS
Second
aryOutcome:
radiologicinfarctio
n,TC
Dor
angiograph
icvasospasm,
shun
tplacement,
ventric
ulitis,discharge
mRS
,90daymini-m
ental
status
exam
,lengthof
stay
Giusepp
eLanzino
,NCT
01420978
Morea
ggressiveC
SFdrainage
may
improveb
rain
microcirculationand
perfusionandlead
tobette
rneurological
outcom
es
Antiepileptics
Com
paris
onof
short
duratio
nlevetiracetam
toextend
edcourse
forseizure
prop
hylaxisa
fter
subarachno
idhemorrhage
Rand
omized,
prospective,op
enlabel,
parallelassignm
ent,
phaseIII,safety/effi
cacy
study
Levetiracetam
1000
mgBID×3days
Levetiracetam
1000
mgBID×
hospita
lstay
460
Prim
aryou
tcom
e:In
hospita
lseizures
Second
aryou
tcom
e:Incidenceo
fseizure
after
hospita
ldisc
harge,adverse
drug
reactio
ns,lengthof
stay,cognitiv
eand
functio
naloutcomes
RajatD
har,
NCT
01137110
Antiepilepticsc
anhave
long
-term
cogn
itive
sidee
ffects.
Ashortcou
rsem
aybe
justas
efficaciou
sas
prolon
geduse
Antiepilepticdrugsa
ndvascular
riskmarkers
Rand
omized,openlabel,
parallelassignm
ent
study
Tier
1:ph
enytoin
5mg/kg/d
dividedin
2do
ses
Tier
2:valproate
15mg/kg/d
dividedin
3do
ses
Tier
3:levetiracetam
1000-1500m
g/d
dividedin
2do
ses
Nodrug
interventio
n200
Prim
aryou
tcom
e:serum
cholesterol,no
n-HDL
cholesterol,HDL,
lipop
rotein
a,CR
PSecond
aryou
tcom
e:acute
seizures,lates
eizures,mRS
at8and16
weeks
Prem
aKish
naand
ScottM
intzer,
NCT
00774306
Certain
seizure
medications
may
raise
cholesterollevels
and
increase
ther
iskof
heartatta
ckand
stroke

Stroke Research and Treatment 31
Table3:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
entg
roup
Con
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Sedatio
n
Effectsof
dexm
edetom
idineo
ninflammatorycytokinesin
patie
ntsw
ithaneurysm
alsubarachno
idhemorrhage
Rand
omized,openlabel,
parallelassignm
ent
efficacy
study
Dexmedetom
idine
0.2–1.5
mcg/kg/h
Prop
ofol5–
80mcg/kg/min
10
Prim
aryou
tcom
e:serum
andCS
Fcytokineso
ver4
8ho
urs
Second
aryou
tcom
es:
sedativ
eand
analgesic
requ
irements,
RASS
and
CAM-ICU
scores,lengthof
stay,delayedcerebral
ischemia,G
OSE
atdischarge
ShaunKe
egan
and
BrittanyWoo
lf,NCT
01565590
Dexmedetom
idine
may
causeless
inflammationover
timethanprop
ofol
Rehabilitation
Rehabilitationof
patie
nts
after
subarachno
idhemorrhage
Non
rand
omized,open
label,parallelassignm
ent
Early
multid
isciplin
ary
rehaband
mob
ilizatio
n
Nointerventio
n160
Prim
aryou
tcom
e:10-w
eek
GOS
Second
aryou
tcom
e:3–6
mon
thand12-m
onth
GOSE
,fun
ctional
independ
ence
measure,
comar
ecoveryscale,
disabilityratin
gscale,
High-levelM
obility
Assessm
enttoo
l,pain
score
TanjaK
aricand
Ang
elika
Sorteberg,
NCT
01656317
Early
rehabmay
redu
cecomplications
andim
provep
hysic
alandcogn
itive
functio
naft
erSA
H
Bloo
dpressure
control
SafetyandEffi
cacy
Stud
yof
ClevidipinetoCon
trol
Hypertensionin
Patie
nts
Admitted
with
Aneurysmal
Subarachno
idHem
orrhage
(CLA
SH)
Openlabel,safety,
efficacy
study,single
grou
passig
nment(Ph
ase
2)
ClevidipineIV
2–32
mg/hfor2
4–48
hours
NA
20Prim
ary:Bloo
dpressure
with
intargetrange
PanayiotisVa
relas,
NCT
00978822
Toassessho
wrapidly
andsafelyClevidipine
canbe
used
tocontrol
bloo
dpressure
inSA
Hpatie
nts.
Other
Cervicalspinalcord
stim
ulationforthe
preventio
nof
cerebral
vasospasm
Non
rand
omized,open
label
Spinalcord
stim
ulationusing
MTS
TrialSystem
3510
NA
12
Prim
aryou
tcom
e:cerebral
vasospasm
Second
aryou
tcom
e:adversee
vents
Konstantin
Slavin,
NCT
00766844
—

32 Stroke Research and Treatment
Table4:Ra
ndom
ized
controlledtrialsassessingneurologicou
tcom
esaft
ercardiaca
rrest—
ongoingtrials.
Trialn
ame
Stud
ydesig
nTreatm
ent
grou
pCon
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Neuroprotectiv
edrugs
Selenium
toIm
prove
NeurologicalO
utcome
after
CardiacA
rrest
(SCP
R)
Rand
omized,
doub
le-blin
d,placebo-controlled,
single-center,phase
2aeffi
cacy
study
Sodium
-sele
nite
infusio
n×7days
Placebo
52
Prim
aryou
tcom
e:neuron
-specific
enolase
Second
aryou
tcom
es:
inflammationand
oxidatives
tressmarkers,
NIH
SSandGlasgow
Pittsbu
rghperfo
rmance
scorea
t6mon
ths,
selenium
bloo
dlevels,
glutathion
eperoxidase
plasmalevels
VanessaS
tadlbauera
ndKa
rlheinz
Smolle,
NCT
01390506
Selenium
canredu
ceoxidatives
tressaft
ercardiaca
rrestand
redu
ceinflammation
Magnesiu
m
ClinicalStud
yof
theL
RSTh
ermoSuitSystem
inPo
stArrestP
atientsw
ithIntravenou
sInfusionof
Magnesiu
mSulfate
Rand
omized,
doub
le-blin
d,parallel
assig
nment,
safety/efficacy
study
ofanyrhythm
Thermosuittotarget
34∘
Cplus
magnesiu
msulfateIV
(30m
g/kg
over
15minutes)
ThermoSuitto
target34∘
Cplus
placebo(normal
salin
e)
14
Prim
aryou
tcom
e:coolingrate
Second
aryou
tcom
es:
timetotarget
temperature,percentage
oftim
eintarget
temperature
range,
shivering,leng
thof
stay,
neurologicstatus
atdischargea
nd6mon
ths,
adversee
vents,survival
at24
hours,discharge
and30
days
MichaelHolzera
ndAnd
reas
Janata,
NCT
00593164
Tests
newdevice
toachievetherapeutic
hypo
thermiaandthe
impactof
magnesiu
mon
coolingperfo
rmance
andhemod
ynam
ics
Hypotherm
ia
TargetTemperature
Managem
entafte
rCa
rdiacA
rrest(TT
M)
Rand
omized,
doub
le-blin
d,parallel
assig
nment,multicenter,
safety/efficacy
trialfor
out-o
f-hospitalcardiac
arrest
Targettemperature
36∘
C×24
h
Target
temperature
33∘
C×24
h850
Prim
aryou
tcom
e:All
causem
ortality
Second
aryou
tcom
es:
6-mon
thcompo
sitea
llcausem
ortalityandpo
orneurologicalou
tcom
eby
cerebralperfo
rmance
scale,bleeding
,6-m
onth
neurologicalstatus
and
quality
oflife,mRS
,Cerebralp
erform
ance
scale,mini-m
entaltest,
IQCO
DE,
SF-36,adverse
events
NiklasN
ielse
nandHans,
FribergNCT
01020916
Attemptstoidentify
optim
alhypo
thermia
targettemperature

Stroke Research and Treatment 33
Table4:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
ent
grou
pCon
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Hypotherm
iaAfte
rin-H
ospitalC
ardiac
Arrest
(HAC
Ainho
spita
l)
Rand
omized,
single-blind,parallel
assig
nment,
single-center,
safety/efficacy
study
for
in-hospitalarrestsof
any
rhythm
Mild
therapeutic
hypo
thermia32–34∘C
×24
hours.
Standard
care,
nohypo
thermia
440
Prim
aryou
tcom
e:all
causem
ortalityat6
mon
ths
Second
aryou
tcom
es:6
mon
thGlasgow
-Pittsburgh
cerebralperfo
rmance
scale,in-hospital
all-c
ause
mortality
SebastianWolfrum
and
Volkhard
Kurowski,
NCT
00457431
Tests
whether
hypo
thermiatre
atment
will
improveo
utcome
after
in-hospitalarresto
fanyrhythm
Intra-arrestTh
erapeutic
Hypotherm
iain
PrehospitalC
ardiac
Arrest
(HITUPP
AC-BIO
)
Rand
omized,openlabel,
parallelassignm
ent,
efficacy
trial
Hypotherm
iaindu
ctionprehospital
Hypotherm
iaindu
ctionat
hospita
larrival
250
Prim
aryou
tcom
es:brain
injury
biom
arkersat72
hSecond
aryou
tcom
es:
ROSC
,survival72h
,GCS
at48
hours,
cerebralperfo
rmance
scalea
t28days
Guillaum
eDebatyJean
FrancoisTimsit,
NCT
00886184
Assessu
tility
ofearly
hypo
thermiaprehospital
Indu
ctionof
Mild
Hypotherm
iaFo
llowing
Out-of-h
ospitalC
ardiac
Arrest
Rand
omized,openlabel,
singleg
roup
assig
nment,
efficacy
study
ofany
rhythm
outo
fhospital
arrest
Rapidinfusio
nof
2Lof
4∘Cno
rmalsalin
epriortoED
arriv
al
Standard
therapy
1364
Prim
aryou
tcom
e:aw
ake
andcommandfollowing
atho
spita
ldisc
harge
Second
aryou
tcom
es:
days
toaw
akening,days
todeath,3mon
thneurologicalou
tcom
e
FrancisK
im,
NCT
00391469
Tests
whether
rapid
indu
ctionof
hypo
thermiawith
cold
salin
einfusionis
efficaciou
s
Com
parin
gTh
erapeutic
Hypotherm
iaUsin
gEx
ternalandInternal
Coo
lingforP
ost-C
ardiac
ArrestP
atients
Rand
omized,openlabel,
parallelassignm
ent,
efficacy
trial
Externaldevice
(Arctic
Sun)
indu
ced
hypo
thermia
Internaldevice
(Alsius)ind
uced
hypo
thermia
51
Prim
aryou
tcom
e:Survivalto
hospita
ldischarge
Second
aryou
tcom
e:1
year
neurologicalstatus
MarcusO
ng,
NCT
00827957
Identifying
them
ost
efficientm
etho
dof
coolingmay
improve
outcom
eafterc
ardiac
arrest
Hypotherm
ia+EC
MO
Refractory
Out-of-H
ospitalC
ardiac
ArrestT
reated
with
MechanicalC
PR,
Hypotherm
ia,E
CMO
andEa
rlyRe
perfusion
(CHEE
R)
Non
rand
omized,single
grou
p,op
enlabel,
safety/efficacy
trailfor
patie
ntsw
hofail
stand
ardresuscitatio
n
Automated
CPR,
ECMO,coron
ary
angiograph
y,therapeutic
hypo
thermia
NA
24
Prim
aryou
tcom
e:survivalto
hospita
ldischarge
Second
aryou
tcom
es:
cerebralperfo
rmance
Scale,tim
etoEC
MO
insertion,
neurologic
biom
arkers,cardiac
recovery
StephenBe
rnardand
DionStub
,NCT
01186614
Aggressiver
esuscitatio
nmay
improveo
utcomein
patie
ntsw
hofail
stand
ardresuscitatio
n

34 Stroke Research and Treatment
Table4:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
ent
grou
pCon
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
Hyperinvasiv
eapp
roach
toou
t-of-h
ospital
cardiaca
rrestu
sing
mechanicalchest
compressio
ndevice,
prehospitalintraarrest
cooling,extracorpo
real
Lifesupp
ortand
early
Invasiv
eassessm
ent
comparedto
stand
ardof
care:P
ragu
eOHCA
Stud
y
Rand
omized,open-label,
parallelgroup
,safety/efficacy
study
Prehospital
mechanical
compressio
ndevice,
intraarrestcoo
ling
andin
hospita
lECL
S(com
pressio
ndevice,
Rhinochill,PL
SEC
MO)
Standard
care
170
Prim
aryou
tcom
e:compo
sitee
ndpo
into
fsurvivalwith
good
neurologicalou
tcom
e(cerebralp
erform
ance
scale)
Second
aryou
tcom
e:30
daycerebral
perfo
rmance
scale,30
daycardiacr
ecovery
JanBe
lohlavek
and
Ond
rejSmid,
NCT
01511666
Aggressive,early
interventio
nmay
improvec
erebral
outcom
es
EmergencyPreservatio
nandRe
suscitatio
n(EPR
)forC
ardiac
Arrestfrom
Trauma(
EPR-CA
T)
Non
rand
omized,open
label,parallel
assig
nment,
safety/efficacy
study
Profou
ndhypo
thermia<10∘
Cwith
cold
salin
einfusio
ninto
aorta
follo
wed
byresuscita
-tio
n/rewarmingwith
cardiopu
lmon
ary
bypass
Standard
treatment
20
Prim
aryou
tcom
e:survivalto
hospita
ldischargew
ithou
tmajor
disabilityby
GOSE
Second
aryou
tcom
es:
achievingtarget
temperature
in1h
our,28
daysurvival,6
mon
thneurologicalfunctio
n,multip
leorgansyste
mdysfu
nctio
n
SamuelT
isherman,
NCT
0104
2015
Resuscitatio
ntechniqu
efortraum
apatientsthat
have
arreste
dfro
mexsang
uinatio
n
HypotherM
ia+xeno
n
Effecto
fxenon
and
therapeutic
hypo
them
iaon
brainandon
neuroloigcalou
tcom
efollo
wingbrainisc
hemia
incardiaca
rrestp
atients
(Xe-hypo
theca)
Rand
omzied,openlabel,
parallelassignm
ent,
phase2
safety/efficacy
trialfor
ventric
ular
fibrillatio
nand
nonp
erfusin
gventric
ular
tachycardia
Hypotherm
ia33∘
C×
24handXe
non
inhalation×24
hours
targetendtid
al40
%
Hypotherm
ia33∘
C×24
h110
Prim
aryou
tcom
e:PE
TandMRI
ischemiaat24
hoursa
nd10
days
Second
aryou
tcom
es:
neurologicalou
tcom
eat
6mon
ths,TT
E
TimoLaitio,
NCT
00879892
Xeno
nmay
besynergistically
neurop
rotectivein
combinatio
nwith
hypo
thermiapo
starrest
bylim
iting
cerebral
hypo
xia,neuron
alloss,
andmito
chon
drial
dysfu
nctio
nCh
estcom
presions
Con
tinuo
uschest
compressio
ns
Rand
omized,openlabel,
multicenter,crossover
assig
nmentstudy
ofou
t-of-h
ospitalcardiac
arrestof
anyrhythm
Con
tinuo
uschest
compressio
ns
Interrup
ted
chest
compressio
nswith
ventilatio
n30
:2
2360
0
Prim
aryou
tcom
e:survivalto
hospita
ldischarge
Second
aryou
tcom
es:
mRS
atdischarge,
adversee
vents
Myron
Weisfe
ldt,
NCT
01372748
Con
tinuo
usCP
Rwith
outinterruptionfor
ventilatio
nmay
besuperio
rtointerrup
ted
compressio
nwith
ventilatio
nratio
of30
:2

Stroke Research and Treatment 35
Table4:Con
tinued.
Trialn
ame
Stud
ydesig
nTreatm
ent
grou
pCon
trolgroup
Target
enrollm
ent
Outcomem
easure
PICom
ments
LUCA
Schest
compressorv
ersus
manualchest
compressio
nin
out-o
f-hospitalsud
den
cardiaca
rrest:LU
CAT
trial
Rand
omized,openlabel,
parallelassignm
ent,
efficacy
study
Mechanical
continuo
uschest
compressio
nsperfo
rmed
byLU
CAS
device
Manualchest
compressio
ns40
0
Prim
aryou
tcom
e:survivalto
hospita
ladmiss
ion,
survivalto
dischargew
ithgood
neurologicalstateb
ycerebralperfo
rmance
Scale
Second
aryou
tcom
es:
ROSC
,end
tidalCO
2,SO
FAscale,leng
thof
stay,m
etabolicand
inflammatorymarkers,
LVfunctio
n
Francesc
Carmon
aJim
enez,R
osa-Maria
Lido
n,NCT
01521208
Mechanicalchest
compressio
nmay
besuperio
rtomanualchest
compressio
n
Cerebraloxygenatio
n
CerebralO
xygenatio
nin
CardiacA
rrestand
Hypotherm
ia
Openlabel,safetyand
efficacy
study
Near-infrared
mon
itorin
g
Standard
therapy,no
mon
itorin
g70
Prim
aryou
tcom
e:survivalto
discharge
Second
aryou
tcom
es:
cerebralperfo
rmance
scalea
tdisc
hargea
nd12
mon
ths
Chris
tianStorm,
NCT
01531426
Near-infrared
spectro
scop
y(N
IRS)
couldbe
anew-non
invasiv
emarker
foro
utcomea
fterc
ardiac
arrest.
LowNIRSmay
correlatew
ithpo
orou
tcom
e

36 Stroke Research and Treatment
Table 5: Number of randomized, controlled trials published and ongoing for aneurysmal subarachnoid hemorrhage and cardiac arrest.
Intervention SAH Cardiac arrestPublished𝑁 (%)
Ongoing𝑁 (%)
Published𝑁 (%)
Ongoing𝑁 (%)
Calcium channel blockers 10 (18) 0 4 (9) 0Antifibrinolytics 5 (9) 0 0 0Neuroprotective drugs 5 (9) 2 (8) 1 (2) 1 (7)Statins 4 (7) 5 (20) 0 0Aneurysm clip or coil 4 (7) 1 (4) NA NALipid peroxidation inhibitor 4 (7) 1 (4) 0 0Thrombolytics 3 (5) 1 (4) 2 (4) 0Antiplatelets 3 (5) 0 0 0Steroids 3 (5) 0 1 (2) 0Transfusion/blood products/erythropoietin 3 (5) 1 (4) 0 0Vasodilators 3 (5) 4 (16) 0 0Pressors or HHH 2 (4) 2 (8) 9 (19.5) 0Magnesium 2 (4) 0 5 (11) 1 (7)Rho-kinase inhibitor (fasudil) 2 (4) 0 0 0Adrenergic blockade 1 (2) 0 0 0Endovascular therapy 1 (2) 0 NA NAInsulin/glucose control 1 (2) 0 2 (4) 0Hypothermia 1 (2) 0 5 (11) 9 (64)CSF diversion 0 2 (8) 0 0Antiepileptics 0 2 (8) 0 0Sedation 0 1 (4) 0 0Rehabilitation 0 1 (4) 0 0Blood pressure 0 1 (4) 0 0Other 0 1 (4) 0 0Chest compressions NA NA 7 (15) 2 (14)Adenosine antagonist 0 0 1 (2) 0Fluid management 0 0 1 (2) 0Barbiturate 0 0 1 (2) 0Cerebral oxygenation 0 0 0 1 (7)Calcium chloride 0 0 3 (7) 0Sodium bicarbonate 0 0 2 (4) 0Hemofiltration 0 0 1 (2) 0Rhythm analysis 0 0 1 (2) 0Total 57 25 46 14
above studies that showed outcome benefit. Eight studiesfound both a significant improvement in delayed cerebralischemia/vasospasm/infarction and outcome including stud-ies of nimodipine [4, 6, 8], nicardipine implants in the basalcistern [13], edavarone [21], pravastatin [25], fasudil [57],and erythropoietin [45]. Nine studies found a benefit fordecreasing delayed cerebral ischemia/vasospasm/infarctionbut no neurologic outcome benefit including studies of IVnicardipine [10, 11], eicosapentaenoic acid (omega-3 fattyacid) [22], the neuroprotectant NA-1 [23], simvastatin [24],tirilazad [34], intracisternal rTPA [36, 38], and clazosentan
[49, 50]. Three studies found improved neurologic out-come despite an insignificant effect on delayed cerebralischemia/vasospasm/infarction including studies of cilosta-zol [41], methylprednisolone [44], and fasudil [58].
Among the cardiac arrest trials, 13% (6/46) demon-strated neurologic or mortality benefit. Improved mortalityrates were demonstrated with mild therapeutic hypothermia[89], coenzyme Q10 [68], vasopressin plus epinephrine plusmethylprednisolone [71], active compression-decompressionCPR [93], and hemofiltration [108]. Improved neurologicaloutcome was demonstrated with early mild therapeutic

Stroke Research and Treatment 37
hypothermia for ventricular fibrillation and pulseless ven-tricular tachycardia arrests [88, 89], and one study of activecompression-decompression CPR [93], though a larger studyof active compression-decompression was negative [94].
3.5. Trial Overlap. Though nimodipine has demonstratedmortality and functional outcome benefit in SAH [4–6, 8,110], it has shown no benefit in cardiac arrest trials [64,65, 67]. Similarly, intracisternal thrombolysis showed somebenefit in reducing delayed cerebral ischemia and infarctionafter SAH [36, 38], but intravenous tenecteplase showedno long-term benefit and, in fact, increased intracranialhemorrhage after cardiac arrest [69, 70]. Neither magnesium[53, 54, 81–85] nor intensive insulin [59, 87] has provenbeneficial after SAH or cardiac arrest. Though hypothermia[88, 89] has been the single most effective treatment forcardiac arrest (the number needed to treat to prevent onedeath is 7 and the number needed to treat to producefavorable neurological outcome is 6), it has not proven usefulin the context of aneurysm surgery after SAH [60]. There islittle mechanistic overlap in ongoing randomized, controlledtrials of SAH and cardiac arrest patients.
4. Discussion
In this paper, a direct comparison is made between ran-domized, controlled clinical trials that evaluate mortality orneurologic outcome after SAH and cardiac arrest. Though28%of SAH studies showed someneurologic outcome benefitin the intervention group, only nimodipine [4–6, 8, 110],fasudil [57, 58], and endovascular coiling [29–31] have beenfound to consistently improve outcome in multiple, multi-center randomized controlled trials. Smaller studies [8, 41,58], single center [21, 44], or phase II safety and feasibilitystudies [13, 25, 45] have shown outcome benefit, but stillrequire larger efficacy trials before integration into standardpractice. Among cardiac arrest trials, only mild therapeutichypothermia has been shown to improve both mortality andneurologic outcome [88, 89]. Little overlap in trial results ormechanisms of study was identified in these different patientpopulations.
Methodological differences in the timing, duration, neu-rological severity, and outcomes studied may explain someof the differences in trial results between SAH and cardiacarrest populations. First, the timing of intervention for SAHand cardiac arrest trials is quite different. With the exceptionof aneurysm repair and aneurysm rebleeding trials (someof which were carried out in the era of delayed surgicaltreatment), the vast majority of SAH trials focus on thedelayed cerebral ischemia period. Conversely, all cardiacarrest trials are directed at intervening against early braininjury. The difference in time frames studied may explain, inpart, the variable results for mild therapeutic hypothermiain each population. Unlike the cardiac arrest trials, whichapplied hypothermia either prior to ED arrival [88] or withina median of 105 minutes from return of spontaneous circula-tion (ROSC) [89] for a duration of 12–24 hours, hypothermiawas applied in the IHAST trial at a median of two days from
SAH onset and only for a brief time (median 5-6 hours) [60].Second, patient selection may result in variable trial resultsfor hypothermia. For example, hypothermia for cardiac arrestwas used for comatose survivors, while relatively neuro-logically intact patients (WFNS I–III) were studied in theIHAST trial. Finally, outcome measures differ in the cardiacarrest and SAH literature. Many cardiac trials measure 30-day or dischargemortality or neurologic outcome, while SAHtrials measure outcomes from 3 months to 1 year. Thoughthe majority of cardiac arrest trials measure neurologic out-come using the Pittsburgh cerebral performance scale, whileSAH trials utilize the Glasgow outcome scale or modifiedRankin scale, all of these scales are very similar and providegross estimates of disability. Despite the aforementionedmethodological differences, certain interventions, such asmagnesium and intensive insulin, have not proven effectivein either population.
Another reason for variable outcome in clinical trialsmaybe due to pathophysiological differences in SAH and cardiacarrest.Though early brain injury in SAHmaymechanisticallymirror the cascade of injury occurring after cardiac arrest,SAH differs from cardiac arrest in that it is not a monophasicdisease. Break down of blood products initiates a distinctiveseries of delayed clinical events that characteristically canlead to ischemia or infarction between SAH days 3–14.The fact that nimodipine has been so successful in SAHtrials, but shown no effect at similar doses in cardiac arresttrials suggests it is acting on a distinct pathway. Indeed,the absolute risk reduction for poor outcome after SAHin a meta-analysis of 16 trials of nimodipine is 5.3% witha number needed to treat for benefit of 19 [111]. No suchsignal for benefit was seen in cardiac arrest trials [64, 65,67]. The mechanism of beneficial effect of nimodipine inSAH has been widely debated and may be related to itseffect on fibrinolysis [112], spreading cortical depression [113],or excitotoxicity. Though nimodipine improves ischemicneurological deficits by clinical criteria and CT-documentedinfarction (with a pooled relative risks of 0.66 (95% CI 0.59–0.75) and 0.78 (95% CI 0.70–0.87), resp.) [111], it has littleeffect on angiographic vasospasm or cerebral blood flow[4, 5]. The corollary to this observation is that interventionsthat improve angiographic vasospasm, such as clazosentan,do not necessarily improve cerebral infarction or outcome.[49, 50, 114, 115]. While angiographic vasospasm seems tobe related to infarction [116], other mechanisms may play arole in neurological deficits, cerebral infarction, and outcome.Such pathophysiological differences may make extrapolationof results from cardiac arrest trials to an SAH populationproblematic. Indeed, delayed cerebral ischemia (DCI) mayblunt the positive effect of hypothermia on early brain injury.Further animal research may better identify mechanisticdifferences of early brain injury in cardiac arrest and SAH.
Despite a second wave of neurological injury in SAH,poor-grade (Hunt Hess 4-5) SAH patients, who are at higherrisk for secondary neurological injury, still have comparable,if not better, outcomes compared to cardiac arrest patientswho are not cooled. Among Hunt-Hess grade 4-5 patients,the 12-monthmortality rate with aggressive treatment is 43%,while 40% had no or slight-moderate disability (mRS 0–3)

38 Stroke Research and Treatment
[117]. By comparison, the 6-month death rate in the control(nonhypothermia) group of the HACA trial was 55%, whilegood neurologic outcome (defined as Pittsburgh cerebralperformance scale 1-2; good outcome or moderate disability)occurred in 26–39% [88, 89]. We have additionally shownthatDCI does not predictmortality after SAHwith aggressivevasospasm treatment, while early brain injury (measured byHunt-Hess grade) does [1]. Thus, despite secondary neuro-logic insults and delayed cerebral ischemia risk, poor-gradeSAH patients do at least as well as normothermic cardiacarrest patients, who may face risks to survival and functionaloutcome related to the underlying cause of the cardiac arrest.Also, the median age of cardiac arrest patients tends to beolder than SAH patients, which may also explain why eventhe sickest SAH patients have relatively good outcomes bycomparison. If nihilism can be overcome in the managementof poor-grade SAH patients, the early application of mildtherapeutic hypothermia may improve outcomes further.
There are some limitations to this review that should bementioned. Amedical librarian was not used and onlyMED-LINE/PubMed and clinicaltrials.gov were used to identifyliterature for review. An Embase search was not performed.Additionally, an exhaustive search for all neurologic outcomebased RCTs was not performed, rather only English studiesin humans were included.
In conclusion, while themechanisms of early brain injuryafter SAH and cardiac arrest may be similar, the prepon-derance of SAH clinical trials do not focus on interventionsaddressing early brain injury. Clinical trials in SAH assessinginterventions that have proven successful in the cardiac arrestliterature, such as early mild therapeutic hypothermia, arewarranted.
References
[1] J. A. Frontera, A. Fernandez, J. M. Schmidt et al., “Definingvasospasm after subarachnoid hemorrhage: what is the mostclinically relevant definition?” Stroke, vol. 40, no. 6, pp. 1963–1968, 2009.
[2] K. E. Wartenberg, J. M. Schmidt, J. Claassen et al., “Impact ofmedical complications on outcome after subarachnoid hemor-rhage,” Critical Care Medicine, vol. 34, no. 3, pp. 617–623, 2006.
[3] G. S. Allen, H. S. Ahn, T. J. Preziosi et al. et al., “Cerebralarterial spasm–a controlled trial of nimodipine in patientswith subarachnoid hemorrhage,” The New England Journal ofMedicine, vol. 308, no. 11, pp. 619–624, 1983.
[4] K. C. Petruk,M.West, G.Mohr et al., “Nimodipine treatment inpoor-grade aneurysm patients. Results of a multicenter double-blind placebo-controlled trial,” Journal of Neurosurgery, vol. 68,no. 4, pp. 505–517, 1988.
[5] E. Mee, D. Dorrance, D. Lowe, and G. Neil-Dwyer, “Controlledstudy of nimodipine in aneurysm patients treated early aftersubarachnoid hemorrhage,” Neurosurgery, vol. 22, no. 3, pp.484–491, 1988.
[6] J. D. Pickard, G. D. Murray, R. Illingworth et al., “Effect of oralnimodipine on cerebral infarction and outcome after subarach-noid haemorrhage: British aneurysm nimodipine trial,” BritishMedical Journal, vol. 298, no. 6674, pp. 636–642, 1989.
[7] J. M. Gilsbach, H. J. Reulen, B. Ljunggren et al., “Earlyaneurysm surgery and preventive therapy with intravenously
administered nimodipine: a multicenter, double-blind, dose-comparison study,” Neurosurgery, vol. 26, no. 3, pp. 458–464,1990.
[8] J. Ohman, A. Servo, and O. Heiskanen, “Long-term effects ofnimodipine on cerebral infarcts and outcome after aneurysmalsubarachnoid hemorrhage and surgery,” Journal of Neuro-surgery, vol. 74, no. 1, pp. 8–13, 1991.
[9] V. Soppi, P. N. Karamanakos, T. Koivisto et al., “A randomizedoutcome study of enteral versus intravenous nimodipine in171 patients after acute aneurysmal subarachnoid hemorrhage,”World Neurosurgery, vol. 78, no. 1-2, pp. 101–109, 2012.
[10] E. C. Haley Jr., N. F. Kassell, and J. C. Torner, “A randomizedtrial of nicardipine in subarachnoid hemorrhage: angiographicand transcranial Doppler ultrasound results. A report of thecooperative aneurysm study,” Journal of Neurosurgery, vol. 78,no. 4, pp. 548–553, 1993.
[11] E. C. Haley Jr., N. F. Kassell, and J. C. Torner, “A random-ized controlled trial of high-dose intravenous nicardipine inaneurysmal subarachnoid hemorrhage. A report of the coop-erative aneurysm study,” Journal of Neurosurgery, vol. 78, no. 4,pp. 537–547, 1993.
[12] E. C. Haley Jr., N. F. Kassell, J. C. Torner, L. L. Truskowski,and T. P. Germanson, “A randomized trial of two doses ofnicardipine in aneurysmal subarachnoid hemorrhage: a reportof the cooperative aneurysm study,” Journal of Neurosurgery,vol. 80, no. 5, pp. 788–796, 1994.
[13] M. Barth,H.H.Capelle, S.Weidauer et al., “Effect of nicardipineprolonged-release implants on cerebral vasospasm and clinicaloutcome after severe aneurysmal subarachnoid hemorrhage: aprospective, randomized, double-blind phase IIa study,” Stroke,vol. 38, no. 2, pp. 330–336, 2007.
[14] H. Fodstad, A. Forssell, B. Liliequist, and M. Schannong,“Antifibrinolysis with tranexamic acid in aneurysmal sub-arachnoid hemorrhage: a consecutive controlled clinical trial,”Neurosurgery, vol. 8, no. 2, pp. 158–165, 1981.
[15] U. M. Chowdhary and K. Sayed, “Comparative clinical trialof epsilon amino-caproic acid and tranexamic acid in theprevention of early recurrence of subarachnoid haemorrhage,”Journal of Neurology, Neurosurgery and Psychiatry, vol. 44, no.9, pp. 810–813, 1981.
[16] M. Vermeulen, K. W. Lindsay, G. D. Murray et al. et al.,“Antifibrinolytic treatment in subarachnoid hemorrhage,” TheNew England Journal of Medicine, vol. 311, no. 7, pp. 432–437,1984.
[17] Y. Roos, “Antifibrinolytic treatment in subarachnoid hem-orrhage: a randomized placebo-controlled trial. STAR StudyGroup,” Neurology, vol. 54, no. 1, pp. 77–82, 2000.
[18] J. Hillman, S. Fridriksson, O. Nilsson, Z. Yu, H. Saveland, andK. E. Jakobsson, “Immediate administration of tranexamic acidand reduced incidence of early rebleeding after aneurysmalsubarachnoid hemorrhage: a prospective randomized study,”Journal of Neurosurgery, vol. 97, no. 4, pp. 771–778, 2002.
[19] I. Saito, T. Asano, and C. Ochiai, “A double-blind clinicalevaluation of the effect of nizofenone (Y-9179) on delayedischemic neurological deficits following aneurysmal rupture,”Neurological Research, vol. 5, no. 4, pp. 29–47, 1983.
[20] T.Ohta,H.Kikuchi, K.Hashi, andY.Kudo, “Nizofenone admin-istration in the acute stage following subarachnoid hemorrhage.Results of amulti-center controlled double-blind clinical study,”Journal of Neurosurgery, vol. 64, no. 3, pp. 420–426, 1986.
[21] A.Munakata, H.Ohkuma, T.Nakano,N. Shimamura, K. Asano,and M. Naraoka, “Effect of a free radical scavenger, edaravone,

Stroke Research and Treatment 39
in the treatment of patients with aneurysmal subarachnoidhemorrhage,” Neurosurgery, vol. 64, no. 3, pp. 423–428, 2009.
[22] H. Yoneda, S. Shirao, J. Nakagawara, K. Ogasawara, T. Tomi-naga, and M. Suzuki, “A prospective, multicenter, randomizedstudy of the efficacy of eicosapentaenoic acid for cerebralvasospasm: the EVAS study,”World Neurosurgery, 2012.
[23] M. D. Hill, R. H. Martin, D. Mikulis et al. et al., “Safety and effi-cacy of NA-1 in patients with iatrogenic stroke after endovascu-lar aneurysm repair (ENACT): a phase 2, randomised, double-blind, placebo-controlled trial,” The Lancet Neurology, vol. 11,no. 11, pp. 942–950, 2012.
[24] J. R. Lynch, H. Wang, M. J. McGirt et al., “Simvastatin reducesvasospasm after aneurysmal subarachnoid hemorrhage: resultsof a pilot randomized clinical trial,” Stroke, vol. 36, no. 9, pp.2024–2026, 2005.
[25] M. Y. Tseng, M. Czosnyka, H. Richards, J. D. Pickard, andP. J. Kirkpatrick, “Effects of acute treatment with pravastatinon cerebral vasospasm, autoregulation, and delayed ischemicdeficits after aneurysmal subarachnoid hemorrhage: a phase IIrandomized placebo-controlled trial,” Stroke, vol. 36, no. 8, pp.1627–1632, 2005.
[26] S. H. Y. Chou, E. E. Smith, N. Badjatia et al., “A randomized,double-blind, placebo-controlled pilot study of simvastatin inaneurysmal subarachnoid hemorrhage,” Stroke, vol. 39, no. 10,pp. 2891–2893, 2008.
[27] M. D. Vergouwen, J. C. Meijers, R. B. Geskus et al., “Biologiceffects of simvastatin in patients with aneurysmal subarachnoidhemorrhage: a double-blind, placebo-controlled randomizedtrial,” Journal of Cerebral Blood Flow and Metabolism, vol. 29,no. 8, pp. 1444–1453, 2009.
[28] J. Ohman and O. Heiskanen, “Timing of operation for rupturedsupratentorial aneurysms: a prospective randomized study,”Journal of Neurosurgery, vol. 70, no. 1, pp. 55–60, 1989.
[29] A. Molyneux, R. Kerr, I. Stratton et al., “International subarach-noid aneurysm trial (ISAT) of neurosurgical clipping versusendovascular coiling in 2143 patients with ruptured intracranialaneurysms: a randomised trial,” The Lancet, vol. 360, no. 9342,pp. 1267–1274, 2002.
[30] A. J. Molyneux, R. S. Kerr, L. M. Yu et al., “InternationalSubarachnoid Aneurysm Trial (ISAT) of neurosurgical clippingversus endovascular coiling in 2143 patients with rupturedintracranial aneurysms: a randomised comparison of effectson survival, dependency, seizures, rebleeding, subgroups, andaneurysm occlusion,” The Lancet, vol. 366, no. 9488, pp. 809–817, 2005.
[31] C. G. McDougall, R. F. Spetzler, J. M. Zabramski et al., “Thebarrow ruptured aneurysm trial,” Journal of Neurosurgery, vol.116, no. 1, pp. 135–144, 2012.
[32] N. F. Kassell, E. C. Haley Jr., C. Apperson-Hansen, and W. M.Alves, “Randomized, double-blind, vehicle-controlled trial oftirilazad mesylate in patients with aneurysmal subarachnoidhemorrhage: a cooperative study in Europe, Australia, and NewZealand,” Journal of Neurosurgery, vol. 84, no. 2, pp. 221–228,1996.
[33] E. C. Haley Jr., N. F. Kassell, C. Apperson-Hansen, M. H.Maile, and W. M. Alves, “A randomized, double-blind, vehicle-controlled trial of tirilazadmesylate in patientswith aneurysmalsubarachnoid hemorrhage: a cooperative study in North Amer-ica,” Journal of Neurosurgery, vol. 86, no. 3, pp. 467–474, 1997.
[34] G. Lanzino, N. F. Kassell, N. W. C. Dorsch et al., “Double-blind, randomized, vehicle-controlled study of high-dose tir-ilazad mesylate in women with aneurysmal subarachnoid
hemorrhage—part I: a cooperative study in Europe, Australia,New Zealand, and South Africa,” Journal of Neurosurgery, vol.90, no. 6, pp. 1011–1017, 1999.
[35] G. Lanzino and N. F. Kassell, “Double-blind, randomized,vehicle-controlled study of high-dose tirilazad mesylate inwomen with aneurysmal subarachnoid hemorrhage—part II: acooperative study in North America,” Journal of Neurosurgery,vol. 90, no. 6, pp. 1018–1024, 1999.
[36] V. Seifert, D. Stolke, M. Zimmermann, and A. Feldges, “Pre-vention of delayed ischaemic deficits after aneurysmal sub-arachnoid haemorrhage by intrathecal bolus injection of tissueplasminogen activator (rTPA). A prospective study,” Acta Neu-rochirurgica, vol. 128, no. 1–4, pp. 137–143, 1994.
[37] J. M. Findlay, “A randomized trial of intraoperative, intracis-ternal tissue plasminogen activator for the prevention ofvasospasm,” Neurosurgery, vol. 37, no. 5, pp. 1026–1027, 1995.
[38] T. Yamamoto, T. Esaki, Y. Nakao, and K. Mori, “Efficacy of low-dose tissue-plasminogen activator intracisternal administrationfor the prevention of cerebral vasospasm after subarachnoidhemorrhage,” World Neurosurgery, vol. 73, no. 6, pp. 675–682,2010.
[39] M. D. Shaw, P. M. Foy, M. Conway et al., “Dipyridamole andpostoperative ischemic deficits in aneurysmal subarachnoidhemorrhage,” Journal of Neurosurgery, vol. 63, no. 5, pp. 699–703, 1985.
[40] W. M. van den Bergh, A. Algra, S. M. D. Mees, F. van Kooten,C. M. Dirven, J. van Gijn et al., “Randomized controlled trialof acetylsalicylic acid in aneurysmal subarachnoid hemorrhage:the MASH study,” Stroke, vol. 37, no. 9, pp. 2326–2330, 2006.
[41] S. Suzuki, T. Sayama, T. Nakamura et al., “Cilostazol improvesoutcome after subarachnoid hemorrhage: a preliminary report,”Cerebrovascular Diseases, vol. 32, no. 1, pp. 89–93, 2011.
[42] D. Hasan, K. W. Lindsay, E. F. M. Wijdicks et al., “Effect offludrocortisone acetate in patients with subarachnoid hemor-rhage,” Stroke, vol. 20, no. 9, pp. 1156–1161, 1989.
[43] Y. Katayama, J. Haraoka, H. Hirabayashi et al., “A randomizedcontrolled trial of hydrocortisone against hyponatremia inpatients with aneurysmal subarachnoid hemorrhage,” Stroke,vol. 38, no. 8, pp. 2373–2375, 2007.
[44] P. Gomis, J. P. Graftieaux, R. Sercombe, D. Hettler, B.Scherpereel, and P. Rousseaux, “Randomized, double-blind,placebo-controlled, pilot trial of high-dose methylprednisolonein aneurysmal subarachnoid hemorrhage,” Journal of Neuro-surgery, vol. 112, no. 3, pp. 681–688, 2010.
[45] M. Y. Tseng, P. J. Hutchinson, H. K. Richards et al., “Acutesystemic erythropoietin therapy to reduce delayed ischemicdeficits following aneurysmal subarachnoid hemorrhage: aphase II randomized, double-blind, placebo-controlled trial:clinical article,” Journal of Neurosurgery, vol. 111, no. 1, pp. 171–180, 2009.
[46] A. M. Naidech, A. Shaibani, R. K. Garg et al., “Prospective,randomized trial of higher goal hemoglobin after subarachnoidhemorrhage,”Neurocritical Care, vol. 13, no. 3, pp. 313–320, 2010.
[47] J. I. Suarez, R. H.Martin, E. Calvillo et al. et al., “The albumin insubarachnoid hemorrhage (ALISAH) multicenter pilot clinicaltrial: safety and neurologic outcomes,” Stroke, vol. 43, no. 3, pp.683–690, 2012.
[48] B. A. Bell, “Effect of calcitonin-gene-related peptide in patientswith delayed postoperative cerebral ischaemia after aneurysmalsubarachnoid haemorrhage,” The Lancet, vol. 339, no. 8797, pp.831–834, 1992.

40 Stroke Research and Treatment
[49] R. L. Macdonald, R. T. Higashida, E. Keller et al., “Clazosentan,an endothelin receptor antagonist, in patients with aneurysmalsubarachnoid haemorrhage undergoing surgical clipping: arandomised, double-blind, placebo-controlled phase 3 trial(CONSCIOUS-2),”The Lancet Neurology, vol. 10, no. 7, pp. 618–625, 2011.
[50] R. L. Macdonald, R. T. Higashida, E. Keller et al. et al.,“Randomized trial of clazosentan in patients with aneurysmalsubarachnoid hemorrhage undergoing endovascular coiling,”Stroke, vol. 43, no. 6, pp. 1463–1469, 2012.
[51] L. Lennihan, S. A. Mayer, M. E. Fink et al., “Effect of hyper-volemic therapy on cerebral blood flow after subarachnoidhemorrhage: a randomized controlled trial,” Stroke, vol. 31, no.2, pp. 383–391, 2000.
[52] A. Egge, K. Waterloo, H. Sjøholm, T. Solberg, T. Ingebrigtsen,and B. Romner, “Prophylactic hyperdynamic postoperativefluid therapy after aneurysmal subarachnoid hemorrhage: aclinical, prospective, randomized, controlled study,” Neuro-surgery, vol. 49, no. 3, pp. 593–606, 2001.
[53] G. K. C. Wong, W. S. Poon, M. T. V. Chan et al., “Intravenousmagnesium sulphate for aneurysmal subarachnoid hemorrhage(IMASH): a randomized, double-blinded, placebo-controlled,multicenter phase III trial,” Stroke, vol. 41, no. 5, pp. 921–926,2010.
[54] S. M. D. Mees, A. Algra, W. P. Vandertop et al. et al., “Magne-sium for aneurysmal subarachnoid haemorrhage (MASH-2): arandomised placebo-controlled trial,” The Lancet, vol. 380, no.9836, pp. 44–49, 2012.
[55] P. Walter, G. Neil-Dwyer, and J. M. Cruickshank, “Beneficialeffects of adrenergic blockade in patients with subarachnoidhaemorrhage,” The British Medical Journal, vol. 284, no. 6330,pp. 1661–1664, 1982.
[56] M. Zwienenberg-Lee, J. Hartman, N. Rudisill et al., “Effectof prophylactic transluminal balloon angioplasty on cerebralvasospasm and outcome in patients with fisher grade IIisubarachnoid hemorrhage: results of a phase II multicenter,randomized, clinical trial,” Stroke, vol. 39, no. 6, pp. 1759–1765,2008.
[57] M. Shibuya, Y. Suzuki, K. Sugita et al., “Effect of AT877 on cere-bral vasospasm after aneurysmal subarachnoid hemorrhage:results of a prospective placebo-controlled double-blind trial,”Journal of Neurosurgery, vol. 76, no. 4, pp. 571–577, 1992.
[58] J. Zhao, D. Zhou, J. Guo et al. et al., “Efficacy and safety offasudil in patients with subarachnoid hemorrhage: final resultsof a randomized trial of fasudil versus nimodipine,” NeurologiaMedico-Chirurgica, vol. 51, no. 10, pp. 679–683, 2011.
[59] F. Bilotta, A. Spinelli, F. Giovannini, A. Doronzio, R. Delfini,and G. Rosa, “The effect of intensive insulin therapy oninfection rate, vasospasm, neurologic outcome, and mortalityin neurointensive care unit after intracranial aneurysm clippingin patients with acute subarachnoid hemorrhage: a randomizedprospective pilot trial,” Journal of Neurosurgical Anesthesiology,vol. 19, no. 3, pp. 156–160, 2007.
[60] M.M. Todd, B. J. Hindman,W. R. Clarke, and J. C. Torner, “Mildintraoperative hypothermia during surgery for intracranialaneurysm,” The New England Journal of Medicine, vol. 352, no.2, pp. 135–145, 2005.
[61] E. Grote and W. Hassler, “The critical first minutes aftersubarachnoid hemorrhage,” Neurosurgery, vol. 22, no. 4, pp.654–661, 1988.
[62] F. A. Sehba, G. Mostafa, V. Friedrich Jr., and J. B. Bederson,“Acute microvascular platelet aggregation after subarachnoid
hemorrhage,” Journal of Neurosurgery, vol. 102, no. 6, pp. 1094–1100, 2005.
[63] F. A. Sehba and J. B. Bederson, “Mechanisms of acute braininjury after subarachnoid hemorrhage,” Neurological Research,vol. 28, no. 4, pp. 381–398, 2006.
[64] M. Forsman, H. P. Aarseth, H. K. Nordby, A. Skulberg, and P.A. Steen, “Effects of nimodipine on cerebral blood flow andcerebrospinal fluid pressure after cardiac arrest: correlationwithneurologic outcome,” Anesthesia and Analgesia, vol. 68, no. 4,pp. 436–443, 1989.
[65] R. O. Roine, S. Kajaste, and M. Kaste, “Neuropsychologicalsequelae of cardiac arrest,”The Journal of the American MedicalAssociation, vol. 269, no. 2, pp. 237–242, 1992.
[66] Brain Resuscitation Clinical Trial II Study Group, “A random-ized clinical study of a calcium-entry blocker (lidoflazine) inthe treatment of comatose survivors of cardiac arrest,”The NewEngland Journal of Medicine, vol. 324, no. 18, pp. 1225–1231, 1991.
[67] R. O. Roine, M. Kaste, A. Kinnunen, P. Nikki, S. Sarna,and S. Kajaste, “Nimodipine after resuscitation from out-of-hospital ventricular fibrillation. A placebo-controlled, double-blind, randomized trial,” The Journal of the American MedicalAssociation, vol. 264, no. 24, pp. 3171–3177, 1990.
[68] M. S. Damian, D. Ellenberg, R. Gildemeister et al., “CoenzymeQ10 combined with mild hypothermia after cardiac arrest: apreliminary study,” Circulation, vol. 110, no. 19, pp. 3011–3016,2004.
[69] D. M. Fatovich, G. J. Dobb, and R. A. Clugston, “A pilotrandomised trial of thrombolysis in cardiac arrest (the TICAtrial),” Resuscitation, vol. 61, no. 3, pp. 309–313, 2004.
[70] B. W. Bottiger, H. R. Arntz, D. A. Chamberlain et al., “Throm-bolysis during resuscitation for out-of-hospital cardiac arrest,”TheNew England Journal of Medicine, vol. 359, no. 25, pp. 2651–2662, 2008.
[71] S. D. Mentzelopoulos, S. G. Zakynthinos, M. Tzoufi et al.,“Vasopressin, epinephrine, and corticosteroids for in-hospitalcardiac arrest,” Archives of Internal Medicine, vol. 169, no. 1, pp.15–24, 2009.
[72] C. G. Brown, D. R. Martin, P. E. Pepe et al. et al., “A comparisonof standard-dose and high-dose epinephrine in cardiac arrestoutside the hospital. The multicenter high-dose epinephrinestudy group,”TheNew England Journal of Medicine, vol. 327, no.15, pp. 1051–1055, 1992.
[73] C. Choux, P. Y. Gueugniaud, A. Barbieux et al., “Standard dosesversus repeated high doses of epinephrine in cardiac arrestoutside the hospital,” Resuscitation, vol. 29, no. 1, pp. 3–9, 1995.
[74] W. D. Patrick, J. Freedman, T. McEwen, R. B. Light, L. Ludwig,and D. Roberts, “A randomized, double-blind comparison ofmethoxamine and epinephrine in human cardiopulmonaryarrest,” The American Journal of Respiratory and Critical CareMedicine, vol. 152, no. 2, pp. 519–523, 1995.
[75] K. H. Lindner, B. Dirks, H. U. Strohmenger, A. W. Prengel,I. M. Lindner, and K. G. Lurie, “Randomised comparison ofepinephrine and vasopressin in patients with out-of-hospitalventricular fibrillation,”The Lancet, vol. 349, no. 9051, pp. 535–537, 1997.
[76] B. W. Sherman, M. A. Munger, G. E. Foulke, W. F. Ruther-ford, and E. A. Panacek, “High-dose versus standard-doseepinephrine treatment of cardiac arrest after failure of standardtherapy,” Pharmacotherapy, vol. 17, no. 2, pp. 242–247, 1997.
[77] P. Y. Gueugniaud, P. Mols, P. Goldstein et al., “A comparison ofrepeated high doses and repeated standard doses of epinephrine

Stroke Research and Treatment 41
for cardiac arrest outside the hospital,”TheNewEngland Journalof Medicine, vol. 339, no. 22, pp. 1595–1601, 1998.
[78] I. G. Stiell, P. C. Hebert, G. A. Wells et al., “Vasopressinversus epinephrine for inhospital cardiac arrest: a randomisedcontrolled trial,”TheLancet, vol. 358, no. 9276, pp. 105–109, 2001.
[79] V. Wenzel, A. C. Krismer, H. R. Arntz, H. Sitter, K. H.Stadlbauer, and K. H. Lindner, “A comparison of vasopressinand epinephrine for out-of-hospital cardiopulmonary resusci-tation,” The New England Journal of Medicine, vol. 350, no. 2,pp. 105–113, 2004.
[80] P. Y. Gueugniaud, J. S. David, E. Chanzy et al. et al., “Vasopressinand epinephrine vs. epinephrine alone in cardiopulmonaryresuscitation,” The New England Journal of Medicine, vol. 359,no. 1, pp. 21–30, 2008.
[81] M. C.Thel, A. L. Armstrong, S. E. McNulty, R. M. Califf, and C.M. O’Connor, “Randomised trial of magnesium in in-hospitalcardiac arrest,” The Lancet, vol. 350, no. 9087, pp. 1272–1276,1997.
[82] D. M. Fatovich, D. A. Prentice, and G. J. Dobb, “Magnesium incardiac arrest (the magic trial),” Resuscitation, vol. 35, no. 3, pp.237–241, 1997.
[83] J. Allegra, R. Lavery, R. Cody et al., “Magnesium sulfate in thetreatment of refractory ventricular fibrillation in the prehospitalsetting,” Resuscitation, vol. 49, no. 3, pp. 245–249, 2001.
[84] T. B. Hassan, C. Jagger, and D. B. Barnett, “A randomised trialto investigate the efficacy of magnesium sulphate for refractoryventricular fibrillation,” EmergencyMedicine Journal, vol. 19, no.1, pp. 57–62, 2002.
[85] W. T. Longstreth Jr., C. E. Fahrenbruch,M. Olsufka, T. R.Walsh,M. K. Copass, and L. A. Cobb, “Randomized clinical trial ofmagnesium, diazepam, or both after out-of-hospital cardiacarrest,” Neurology, vol. 59, no. 4, pp. 506–514, 2002.
[86] W. T. Longstreth Jr., M. K. Copass, L. K. Dennis, M. E. Rauch-Matthews, M. S. Stark, and L. A. Cobb, “Intravenous glucoseafter out-of-hospital cardiopulmonary arrest: a community-based randomized trial,” Neurology, vol. 43, no. 12 I, pp. 2534–2541, 1993.
[87] T. Oksanen, M. B. Skrifvars, T. Varpula et al., “Strict versusmoderate glucose control after resuscitation from ventricularfibrillation,” Intensive Care Medicine, vol. 33, no. 12, pp. 2093–2100, 2007.
[88] S. A. Bernard, T. W. Gray, M. D. Buist et al., “Treatmentof comatose survivors of out-of-hospital cardiac arrest withinduced hypothermia,” The New England Journal of Medicine,vol. 346, no. 8, pp. 557–563, 2002.
[89] The Hypothermia after Cardiac Arrest Study Group, “Mildtherapeutic hypothermia to improvethe neurologic outcomeafter cardiac arrest,” The New England Journal of Medicine, vol.346, no. 8, pp. 549–556, 2002.
[90] F. Kim,M.Olsufka,W. T. Longstreth Jr. et al., “Pilot randomizedclinical trial of prehospital induction of mild hypothermia inout-of-hospital cardiac arrest patients with a rapid infusion of4 ∘C normal saline,” Circulation, vol. 115, no. 24, pp. 3064–3070,2007.
[91] A. Kamarainen, I. Virkkunen, J. Tenhunen, A. Yli-Hankala, andT. Silfvast, “Prehospital therapeutic hypothermia for comatosesurvivors of cardiac arrest: a randomized controlled trial,” ActaAnaesthesiologica Scandinavica, vol. 53, no. 7, pp. 900–907, 2009.
[92] M. Castren, P. Nordberg, L. Svensson et al., “Intra-arresttransnasal evaporative cooling: a randomized, prehospital, mul-ticenter study (PRINCE: pre-ROSCintraNasal cooling effective-ness),” Circulation, vol. 122, no. 7, pp. 729–736, 2010.
[93] T. J. Cohen, B. G. Goldner, P. C.Maccaro et al., “A comparison ofactive compression-decompression cardiopulmonary resuscita-tion with standard cardiopulmonary resuscitation for cardiacarrests occurring in the hospital,” The New England Journal ofMedicine, vol. 329, no. 26, pp. 1918–1921, 1993.
[94] I. G. Stiell, P. C. Hebert, G. A. Wells et al., “The Ontariotrial of active compression-decompression cardiopulmonaryresuscitation for in-hospital and prehospital cardiac arrest,”TheJournal of the AmericanMedical Association, vol. 275, no. 18, pp.1417–1423, 1996.
[95] A. Hallstrom, L. Cobb, E. Johnson, and M. Copass, “Car-diopulmonary resuscitation by chest compression alone orwith mouth-to-mouth ventilation,”The New England Journal ofMedicine, vol. 342, no. 21, pp. 1546–1553, 2000.
[96] C. Bertrand, F. Hemery, P. Carli et al., “Constant flow insuffla-tion of oxygen as the sole mode of ventilation during out-of-hospital cardiac arrest,” Intensive Care Medicine, vol. 32, no. 6,pp. 843–851, 2006.
[97] L. Svensson, K. Bohm, M. Castren et al., “Compression-onlyCPR or standard CPR in out-of-hospital cardiac arrest,” TheNew England Journal of Medicine, vol. 363, no. 5, pp. 434–442,2010.
[98] T. D. Rea, C. Fahrenbruch, L. Culley et al., “CPR with chestcompression alone or with rescue breathing,”The New EnglandJournal of Medicine, vol. 363, no. 5, pp. 423–433, 2010.
[99] T. P. Aufderheide, G. Nichol, T. D. Rea et al. et al., “A trial of animpedance threshold device in out-of-hospital cardiac arrest,”The New England Journal of Medicine, vol. 365, no. 9, pp. 798–806, 2011.
[100] R. B. Abu-Laban, C. M. McIntyre, J. M. Christenson et al.,“Aminophylline in bradyasystolic cardiac arrest: a randomisedplacebo-controlled trial,” The Lancet, vol. 367, no. 9522, pp.1577–1584, 2006.
[101] B. E. Heradstveit, A. B. Guttormsen, J. Langorgen et al. etal., “Capillary leakage in post-cardiac arrest survivors duringtherapeutic hypothermia—a prospective, randomised study,”Scandinavian Journal of Trauma, Resuscitation and EmergencyMedicine, vol. 18, article 29, 2010.
[102] Brain Resuscitation Clinical Trial I Study Group, “Randomizedclinical study of thiopental loading in comatose survivors ofcardiac arrest,” The New England Journal of Medicine, vol. 314,no. 7, pp. 397–403, 1986.
[103] H. A. Stueven, B. M. Thompson, C. Aprahamian, and D. J.Tonsfeldt, “Calcium chloride: reassessment of use in asystole,”Annals of Emergency Medicine, vol. 13, no. 9, pp. 820–822, 1984.
[104] H. A. Stueven, B. Thompson, C. Aprahamian, D. J. Tonsfeldt,and E. H. Kastenson, “The effectiveness of calcium chloridein refractory electromechanical dissociation,” Annals of Emer-gency Medicine, vol. 14, no. 7, pp. 626–629, 1985.
[105] H. A. Stueven, B. Thompson, C. Aprahamian, D. J. Tonsfeldt,and E. H. Kastenson, “Lack of effectiveness of calcium chloridein refractory asystole,” Annals of Emergency Medicine, vol. 14,no. 7, pp. 630–632, 1985.
[106] T.Dybvik, T. Strand, andP.A. Steen, “Buffer therapy during out-of-hospital cardiopulmonary resuscitation,” Resuscitation, vol.29, no. 2, pp. 89–95, 1995.
[107] R. B. Vukmir and L. Katz, “Sodium bicarbonate improvesoutcome in prolonged prehospital cardiac arrest,” AmericanJournal of Emergency Medicine, vol. 24, no. 2, pp. 156–161, 2006.

42 Stroke Research and Treatment
[108] I. Laurent, C. Adrie, C. Vinsonneau et al., “High-volumehemofiltration after out-of-hospital cardiac arrest: a random-ized study,” Journal of the American College of Cardiology, vol.46, no. 3, pp. 432–437, 2005.
[109] I. G. Stiell, G. Nichol, B. G. Leroux et al. et al., “Early versus laterrhythm analysis in patients with out-of-hospital cardiac arrest,”The New England Journal of Medicine, vol. 365, no. 9, pp. 787–797, 2011.
[110] G. S. Allen, H. S. Ahn, T. J. Preziosi et al. et al., “Cerebralarterial spasm: a controlled trial of nimodipine in patientswith subarachnoid hemorrhage,” The New England Journal ofMedicine, vol. 308, no. 11, pp. 619–624, 1983.
[111] S. M. D. Mees, G. J. E. Rinkel, V. L. Feigin et al., “Calciumantagonists for aneurysmal subarachnoid hemorrhage,” Stroke,vol. 39, no. 2, pp. 514–515, 2008.
[112] Y. B. W. E. M. Roos, M. Levi, T. A. Carroll, L. F. M. Beenen,and M. Vermeulen, “Nimodipine increases fibrinolytic activityin patients with aneurysmal subarachnoid hemorrhage,” Stroke,vol. 32, no. 8, pp. 1860–1862, 2001.
[113] J. P. Dreier, K. Korner, N. Ebert et al., “Nitric oxide scavengingby hemoglobin or nitric oxide synthase inhibition by N-nitro-L-arginine induces cortical spreading ischemia when K+ isincreased in the subarachnoid space,” Journal of Cerebral BloodFlow and Metabolism, vol. 18, no. 9, pp. 978–990, 1998.
[114] M. D. Vergouwen, A. Algra, and G. J. Rinkel, “Endothelinreceptor antagonists for aneurysmal subarachnoid hemorrhage:a systematic review and meta-analysis update,” Stroke, vol. 43,no. 10, pp. 2671–2676, 2012.
[115] X.Wang, Y.M. Li,W. Q. Li, C. G. Huang, Y. C. Lu, and L. J. Hou,“Effect of clazosentan in patients with aneurysmal subarach-noid hemorrhage: a meta-analysis of randomized controlledtrials,” PloS ONE, vol. 7, no. 10, Article ID e47778, 2012.
[116] R. W. Crowley, R. Medel, A. S. Dumont et al. et al., “Angio-graphic vasospasm is strongly correlated with cerebral infarc-tion after subarachnoid hemorrhage,” Stroke, vol. 42, no. 4, pp.919–923, 2011.
[117] J. Mocco, E. R. Ransom, R. J. Komotar et al., “Preoperativeprediction of long-term outcome in poor-grade aneurysmalsubarachnoid hemorrhage,” Neurosurgery, vol. 59, no. 3, pp.529–538, 2006.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com