Embed Size (px)
Citation preview
DOI:10.4158/ EP13471.RA © 2014 AACE.
ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset and finalized. This version of the manuscript will be replaced with the final, published version after it has been published in the print edition of the journal. The final, published version may differ from this proof. DOI:10.4158/ EP13471.RA © 2014 AACE.
Review Article EP13471.RA
USE OF INCRETIN-BASED THERAPY IN HOSPITALIZED PATIENTS WITH HYPERGLYCEMIA
Guillermo E. Umpierrez, MD1, and Stanley Schwartz, MD2
Running title: Incretin-based therapy in hospitals
From: 1Professor of Medicine, Emory University School of Medicine, Atlanta, Georgia, USA; 2Affiliate, Main Line Health System, and Clinical Associate Professor of Medicine, Emeritus, University of Pennsylvania, Philadelphia, Pennsylvania, USA
Correspondence Address: Guillermo E. Umpierrez, MD Professor of Medicine, Emory University School of Medicine 49 Jesse Hill Jr. Drive, Atlanta, Georgia 30303 USA E-mail: [email protected]
DOI:10.4158/ EP13471.RA © 2014 AACE.
ABSTRACT
Objective: Hyperglycemia is common in hospitalized patients with and without prior history of
diabetes and is an independent marker of morbidity and mortality in critically and non-critically ill
patients. Tight glycemic control using insulin has been shown to reduce cardiac
morbidity and mortality in hospitalized patients, but also results in hypoglycemic
episodes, which have been linked to poor outcomes. Thus, alternative treatment options
that can normalize blood glucose levels without undue hypoglycemia are being sought.
Incretin-based therapies, such as glucagon-like peptide (GLP)-1 receptor agonists and
dipeptidyl peptidase (DPP)-4 inhibitors, may have this potential.
Methods: A PubMed database was searched to find literature on the use of incretins in hospital
settings. Title searches included the terms diabetes (care, management, treatment), hospital,
inpatient, hypoglycemia, hyperglycemia, glycemic, incretin, dipeptidyl peptidase (DPP)-4
inhibitor, glucagon-like peptide (GLP)-1, and GLP-1 receptor agonist.
Results: The preliminary research experience with native GLP-1 therapy has shown promise,
achieving improved glycemic control with a low risk of hypoglycemia, counteracting the
hyperglycemic effects of stress hormones, and improving cardiac function in patients with heart
failure and acute ischemia. Large, randomized controlled clinical trials are necessary to show
whether these favorable results will extend to the use of GLP-1 receptor agonists and DPP-4
inhibitors.
Conclusions: This review offers hospitalist physicians and healthcare providers involved in
inpatient diabetes care a pathophysiologic-based approach for the use of incretin agents in
patients with hyperglycemia and diabetes, as well as a summary of benefits and concerns of
insulin and incretin-based therapy in the hospital setting.
Key words: incretin; DPP-4; GLP-1; inpatient; hospital; hyperglycemia

DOI:10.4158/ EP13471.RA © 2014 AACE.
INTRODUCTION
Hyperglycemia is a common and serious health care problem in hospitals, reported in
approximately 30% of general medicine and surgery patients with and without a history of prior
diabetes mellitus (1-3). Extensive evidence indicates that hyperglycemia is associated with an
increased risk of complications, a longer hospital or intensive care unit (ICU) stay, and higher
mortality (3,4). The results of observational and randomized controlled trials have also shown
that improvement in glycemic control with insulin therapy in critically ill, general medicine, and
surgery patients reduces hospital complications (4-7). Recent trials and meta-analyses,
however, have shown that intensified insulin therapy increases the risk for severe hypoglycemia
(8-10), which has been associated with increased morbidity and mortality (11). Thus, while an
insulin-based approach is the current standard of care for achieving glycemic control in
hospitalized patients (3,12), the concern about the risk of hypoglycemia as well as potential
cardiovascular risks has led to a search of alternative treatment options, such as incretin-based
therapy (13-15). Incretins are known to stimulate insulin secretion in a glucose-dependent
fashion, thus not causing hypoglycemia when used as monotherapy. In addition, increasing
evidence indicates that incretin therapy results in metabolic and cardiovascular benefits,
including reduced inflammation and oxidative stress (12,14), improved endothelial function, and
improved left ventricular (LV) function, which could benefit critically ill patients (16).
This review offers hospitalist physicians and health care providers involved in inpatient
diabetes care a pathophysiologic-based approach for the use of incretin agents in patients with
hyperglycemia and diabetes, as well as a summary of benefits and concerns of insulin and
incretin-based therapy in the hospital setting.
DOI:10.4158/ EP13471.RA © 2014 AACE.
HYPERGLYCEMIA IN HOSPITALIZED PATIENTS — A MAJOR MEDICAL ISSUE
IRRESPECTIVE OF DIABETES STATUS
Patients with diabetes have a 3-fold greater chance of hospitalization than those without
diabetes (3,17). An estimated 20% of adult patients admitted to the hospital have a diagnosis of
diabetes, with 30% requiring 2 or more hospitalizations in any given year (17). The exact
prevalence of hyperglycemia in hospitalized patients with or without diabetes is unknown, but
has been reported to be 32% to 38% in community hospitals (3,18) and 60% to 80% in critically
ill and cardiac surgery patients (7,19).
There is a strong association between hyperglycemia and complications occurring in
hospitalized patients with or without a history of diabetes (4,20,21). This association is well
documented for the glucose level upon hospital admission and also for the mean glucose level
during the hospital stay (4). Cross-sectional studies have shown that the risk of complications
and mortality relates to the severity of hyperglycemia, with a higher risk observed in patients
without a history of diabetes (new onset and stress-induced hyperglycemia) than in those with a
known diagnosis of diabetes. It is estimated that each 18-mg/dL rise in admission fasting
plasma glucose is associated with a 33% increase in mortality (22). In studies of patients
undergoing cardiac surgeries, it was reported that those with hospital blood glucose values
>200 mg/dL had higher mortality, more wound infections, and longer hospital stays than those
with lower values, irrespective of pre-existing diabetes (23,24). A variety of biochemical
mechanisms are thought to contribute to the detrimental effects of hyperglycemia in the context
of acute illness. The development of hyperglycemia leads to generation of reactive oxygen
species (ROS), lipid peroxidation, and elevated cardiovascular inflammatory markers. It also
increased pro-inflammatory cytokine such as tumor necrosis factor- α (TNFα), interleukin (IL)-6,
and IL-1, which ultimately alter the immune system (25,26). TNFα mediates insulin resistance
DOI:10.4158/ EP13471.RA © 2014 AACE.
by interfering with insulin receptor signaling (27) or synthesis and/or translocation of the glucose
transporter GLUT-4 to the plasma membrane (28). Acute hyperglycemia may also induce
cardiac myocyte death through apoptosis or by exaggerating ischemia-reperfusion cellular injury
(29). In addition, hyperglycemia-induced abnormalities in hemostasis including increased
platelet activation, adhesion, and aggregation (30), reduced plasma fibrinolytic activity, and
increased plasminogen activator inhibitor-1 activity (31). Many of these processes are thought to
contribute to the increase in mortality observed in hospitalized patients experiencing
hyperglycemia (32).
CURRENT STANDARD THERAPY
Insulin, given intravenously or subcutaneously, is the preferred therapeutic agent for blood
glucose control in the hospital setting. Intravenously (IV) administered insulin is most beneficial
to critically ill patients with or without a history of diabetes (12,15). Because of the short half-life
of circulating insulin, IV delivery allows rapid dosing adjustments to address alterations in
patient status. Insulin infusion is ideally administered via validated written or computerized
protocols that allow for predefined adjustments to the insulin infusion rate according to glycemic
fluctuations and insulin dose (12). For most critically ill patients, a starting threshold of no higher
than 180 mg/dL is recommended. Once IV insulin is started, the glucose level should be
maintained between 140 and 180 mg/dL (12). Target levels less than 110 mg/dL are not
recommended due to the risk of hypoglycemia. Clinical guidelines stress that patients should be
monitored closely for hypoglycemia and that insulin protocols should undergo modification, as
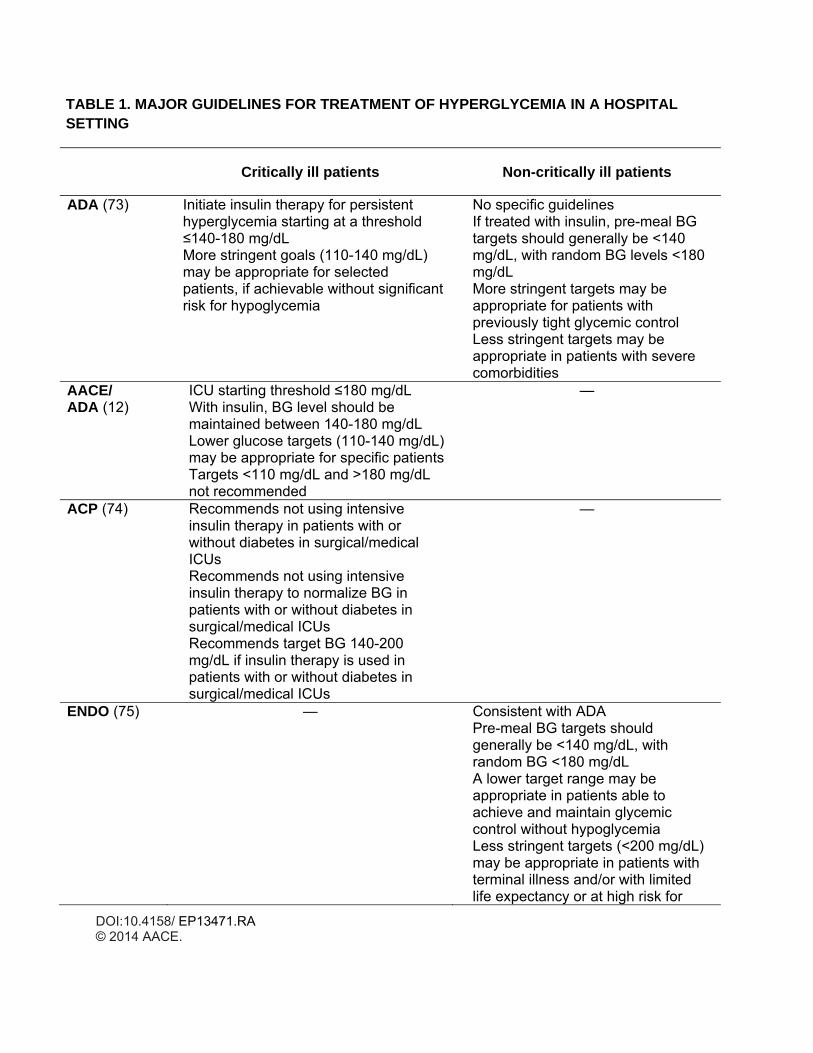
necessary, to prevent hypoglycemia (Table 1).
DOI:10.4158/ EP13471.RA © 2014 AACE.
In non-ICU settings, scheduled subcutaneous insulin therapy with basal analogues (glargine or
detemir) or intermediate acting insulin (NPH) given once or twice a day in combination with
regular or rapid-acting insulin analogues (lispro, aspart or glulisine) administered prior to meals
is preferred as an effective strategy for glucose control in patients with T2DM. The practice of
using sliding scale regular insulin, as a single regimen, to correct hyperglycemia should be
avoided as it results in poor control, increased glycemic variability, and increased risk of hospital
complications. In insulin-naïve patients, a starting insulin dose of 0.3 to 0.5 units per kg/day is
recommended. Elderly patients or those with renal insufficiency (eGFR < 60 ml/min) should be
started on a total daily dose ≤ 0.3 units per kg/day. Patients with adequate oral intake should
receive a basal bolus regimen divided half as basal and half as prandial insulin. Patients with
inadequate oral intake or who will be kept NPO should receive a daily dose of basal insulin
(0.15�0.25 units/kg/day) and rapid-acting insulin analogues as correctional insulin coverage for
glucose >140�180 mg/dl. Clinical guidelines recommend targeting a glucose level <7.8 mmol/L
(140 mg/dl) before meals and a random glucose level <10.0 (180 mg/dl) for the majority of non-
ICU patients (12,15).
Beneficial Mechanistic Effects of Insulin Therapy.
Insulin administration can prevent many of the hormonal and pro-inflammatory aberrations
associated with stress hyperglycemia. Insulin acts to suppress counter-regulatory hormones,
pro-inflammatory transcription factors and may even suppress the formation of reactive
oxidation species (33,34). Several intervention studies and meta-analyses have reported that
intensive insulin therapy improves clinical outcome and mortality in surgical ICU patients (9). A
recent meta-analysis of 7 randomized controlled studies found that intensive insulin therapy
during or after cardiac surgery reduced mortality in the ICU, postsurgical atrial fibrillation, use of
DOI:10.4158/ EP13471.RA © 2014 AACE.
epicardial pacing, duration of mechanical ventilation, and length of ICU stay (35). Insulin has
been shown to have important actions on the cardiovascular system, largely mediated by the
potent vasodilator nitric oxide (33). Recent studies on mediators of inflammation have also
shown that insulin exerts anti-inflammatory, antithrombotic, and anti-atherogenic effects (34).
Insulin counteracts many of the detrimental effects of hyperglycemia, including free radical
formation, oxidative stress, apoptotic cell death, and increased levels of pro-inflammatory
cytokines. Additionally, insulin has been shown to increase cardiac contractility and coronary
vasodilation and preserve endothelial function (36). The antioxidant and anti-inflammatory
effects of insulin are mediated through a number of pathways. Insulin inhibits nuclear factor-κB,
which is at the center of many pro-inflammatory pathways, thereby affecting a range of
downstream events. Inhibition of mitogen-activated protein kinase (MAPK) suppresses IL-6
signaling, while inhibition of c-Jun N-terminal kinase mediates inflammatory processes
downstream of TNFα. TNFα,itself, is suppressed via phosphatidyl-inositol 3-kinase (PI3K)-AKT–
mediated activation of endothelial nitric oxide synthase (34). Taken together, these findings
seem to suggest that there is a cardiac-specific mechanism, which may contribute toward
improved clinical outcomes in this patient group.
LIMITATIONS OF CURRENT PRACTICE
Although intensive insulin therapy in the ICU is the standard of care in hospitals, it also can be
the source of errors and poor outcome. An analysis of medication errors between 2006 and
2008 revealed that insulin was the drug with the greatest number of medication errors in
hospitals (37). Several meta-analyses demonstrated that the risk ratio for occurrence of
hypoglycemic events with intensive insulin therapy versus conventional glycemic control in ICU
was on average 6-fold (9) and 7.7-fold (38) increased, with some studies showing a risk ratio
DOI:10.4158/ EP13471.RA © 2014 AACE.
>10 (ie, NICE-SUGAR [Normoglycaemia in Intensive Care Evaluation and Survival Using
Glucose Algorithm Regulation] study: rate ratio, 13.72) (9). Hypoglycemia has been associated
with adverse cardiovascular outcomes, such as prolonged QT intervals, ischemic
electrocardiogram changes/angina, arrhythmias, sudden death, and increased inflammation
(39).
The evidence regarding a link between hypoglycemia and increased risk of mortality is
varied, with 2 recent studies reporting that hypoglycemia (blood glucose <70 mg/dL) was
independently associated with increased mortality risk in critically ill and ICU patients
independent of their diabetes status (40). In contrast, a recent meta-analysis evaluating clinical
studies in hospitalized patients, including those in ICU, found a small reduction in mortality in
hospitalized patients, whereas no impact on ICU mortality was reported (41).
Insulin-induced hypoglycemia has been associated with increases in C-reactive protein
and proinflammatory cytokines (TNFα, IL-1β, IL-6, and IL-8), markers of lipid peroxidation, ROS,
and leukocytosis (42). In addition, acute hypoglycemia creates a prothrombotic environment,
with increased levels of vasoconstrictors, platelet aggregation, endothelial dysfunction and
vasoconstriction, abnormal cardiac repolarization, as well as catecholamine-induced
cardiovascular changes, such as increase in heart rate, silent myocardial infarction (MI), and
angina and MI, all contributing to increased mortality (42,43).
Because of the limitations of insulin use in hospitalized patients there is a need for other
therapeutic agents that can improve glycemic control while minimizing the risk of hypoglycemia
in critically ill and perioperative settings and reduce the need for insulin administration.

DOI:10.4158/ EP13471.RA © 2014 AACE.
INCRETIN THERAPY IN THE HOSPITAL
Two gut-derived hormones — glucagon-like peptide -1 (GLP-1), released from L cells in the
distal ileum and colon, and glucose-dependent insulinotropic peptide (GIP), released from the
proximal small bowel, both of which stimulate insulin secretion from pancreas in response to
food intake — offer a new way of reducing hyperglycemia by targeting the incretin system.
Several recently published point–counterpoint debates have critically analyzed the benefits and
potential risks of incretin-based therapy in hospitalized patients, with both sides making valid
arguments (13,15,44). While both DPP-4 inhibitors and GLP-1 receptor agonists (RAs) are well
tolerated, the oral administration of DPP-4 inhibitors might be preferred by some patients who
are able to take oral medications. The efficacy and safety of incretin-based therapy for inpatient
use remains to be established and is not currently covered by clinical guidelines, however, the
potential metabolic and cardiovascular benefits make this an attractive possibility.
Beneficial Metabolic Effects of Incretin-based Therapy
Native GLP-1, as well as GLP-1 receptor agonists (RA) such as exenatide and liraglutide, exerts
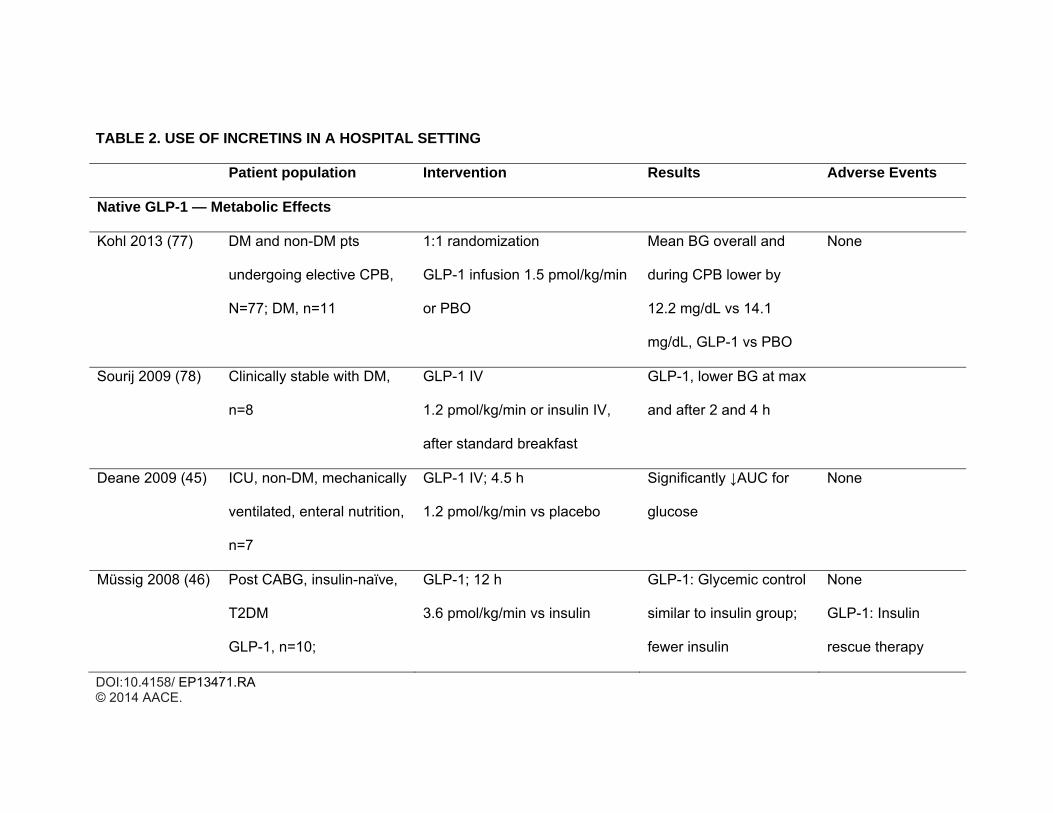
a number of metabolic effects that are advantageous in hospitalized patients. The majority of
small trials have been conducted with native GLP-1, with a few studies using GLP-1 RA (Table
2). In general, native GLP-1 infusion administered to critically ill nondiabetic or diabetic patients
has been shown to normalize the glycemic response after a meal or enteral nutrition similar to
insulin administration, and has been shown to reduce exogenous insulin requirements (45-47)
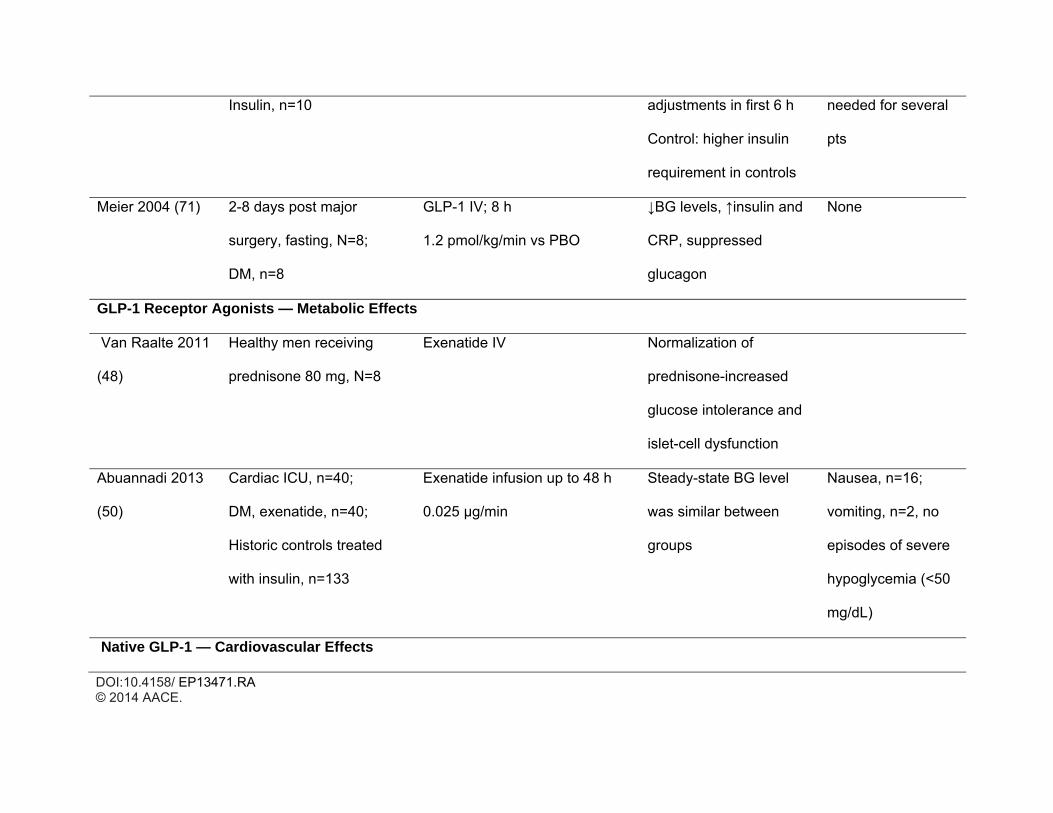
Similarly, the use of exenatide has proven beneficial in settings of corticosteroid-induced or
inpatient hyperglycemia (48). Results from a cross-over study in healthy volunteers showed that
IV exenatide administration prevented glucose intolerance after administration of high-dose
daily prednisolone (48). The hyperglycemic effects of steroids, both endogenous as well as
DOI:10.4158/ EP13471.RA © 2014 AACE.
exogenous, occur, in part, through a mechanism that can be overcome by the GLP-1 pathway in
the beta-cell (48). In a hospital setting, exenatide normalized blood glucose levels in 14 patients,
most of whom were nondiabetic, undergoing various surgeries when exenatide was
administered perioperatively (49) and in 40 diabetic patients in a cardiac ICU when given as an
IV bolus followed by a 48-hour infusion (50).
A recently published open-label, randomized pilot study assessed the safety and efficacy
of the dipeptidyl peptidase-4 (DPP-4) inhibitor sitagliptin for the inpatient management of type 2
diabetes mellitus (T2DM) (14). Patients (n=90) with T2DM treated with diet, oral antidiabetics, or
a low daily insulin dose (≤0.4 units/kg), were randomized to sitagliptin alone or in combination
with low-dose glargine insulin or to a basal bolus insulin regimen plus supplemental doses of
insulin lispro. Similar improvements in glycemic control were observed in all treatment groups.
Patients receiving sitagliptin needed significantly lower total daily insulin doses and fewer insulin
injections than those on the basal bolus regimen. It should be noted that most patients with an
admission blood glucose <180 mg/dL treated with sitagliptin plus correction doses of rapid-
acting insulin responded as well as those on the basal bolus insulin regimen. Patients with an
admission glucose >180 mg/dL treated with sitagliptin alone, however, had higher mean daily
blood glucose compared with patients treated with basal bolus or sitagliptin plus glargine.
Results of this pilot study suggest that treatment with sitagliptin alone or in combination with
basal insulin may represent an effective alternative to the basal bolus regimen in general
medicine and surgery patients with T2DM.
Cardioprotective Effects of Incretin-Based Therapy
Whereas some of the proposed cardioprotective effects of GLP-1 may be exerted indirectly via
normalization of glucose levels, GLP-1 receptors have been found in cardiomyocytes,
DOI:10.4158/ EP13471.RA © 2014 AACE.
endothelial cells, and brain regions involved in autonomic function, suggesting that there may be
a direct effect on the myocardium. Although to date there are no large studies assessing the
cardiovascular effects of incretins, information can be gleaned from inpatient trials with primary
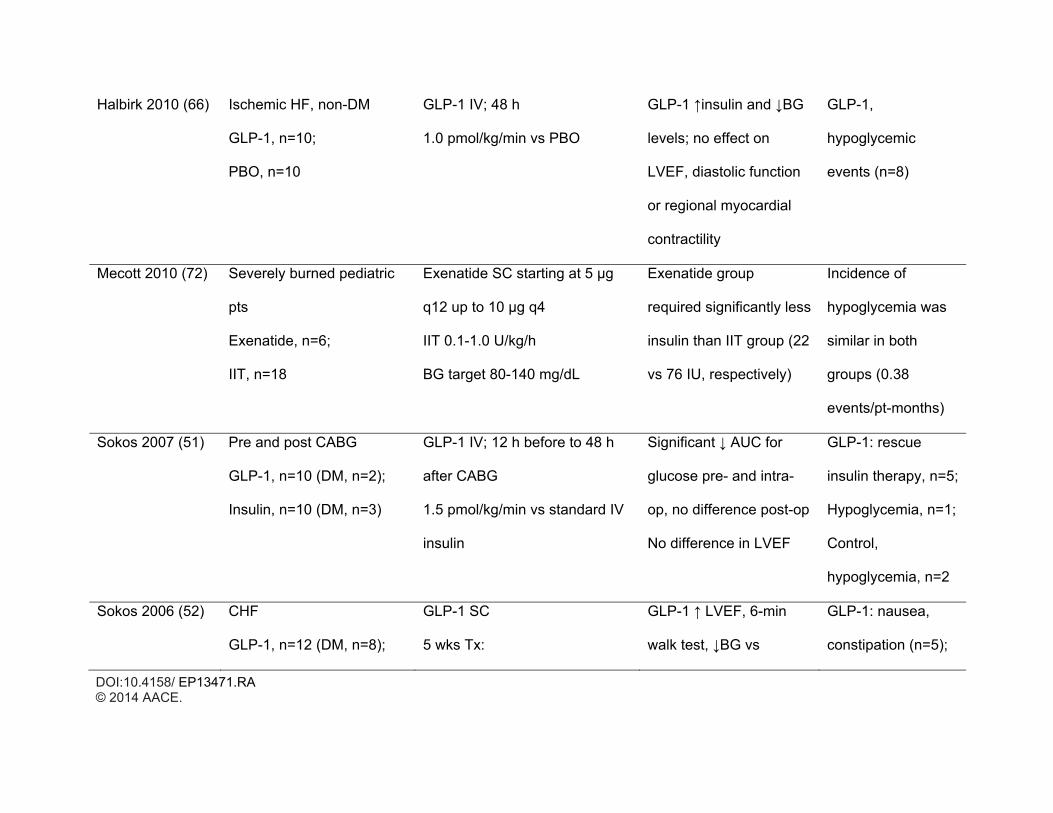
metabolic or cardiac endpoints. For example, perioperative treatment with native GLP-1 in 20
patients undergoing coronary artery bypass graft (CABG) resulted in better glycemic control,
lower post-operative insulin levels, and fewer arrhythmias (51). Similarly, chronic infusion of
GLP-1 significantly improved LV function and functional status in patients with severe heart
failure (52) and regional and global LV function in patients with acute MI and severe systolic
dysfunction after successful angioplasty (53). The observation that these beneficial effects
occurred in patients with or without T2DM, supports a GLP-1 effect on the heart independent of
glycemic control.
Cardioprotective effects with a DPP-4 inhibitor were demonstrated in 14 patients with
coronary artery disease who had improved myocardial response to dobutamine stress and
mitigated myocardial stunning after sitagliptin administration (54). However, cardioprotection
can also occur via GLP-1 independent mechanisms, as demonstrated in the SITAGRAMI trial,
which utilized a combinatiaon of sitagliptin and granulocyte colony-stimulating factor (G-CSF) to
assess cardiac regeneration in 36 patients 6 weeks after acute MI (55). Interim results showed
that the combination of sitagliptin and G-CSF appeared to be safe and a feasible approach to
improve myocardial function after an MI. Past studies using G-CSF for stem cell mobilization as
monotherapy after MI failed to increase global cardiac function, likely because the cardiac
homing process was not optimized (55). Mobilization of stem cells from bone marrow to the
heart occurs mainly by interaction of myocardial stromal cell-derived factor 1 (SDF-1), which is a
substrate for DPP-4, and the cellular homing receptor CXCR-4. Stabilization of SDF-1 levels
DOI:10.4158/ EP13471.RA © 2014 AACE.
using DPP-4 inhibitors, such as sitagliptin, thus has the potential for improving mobilization of
stem cells to the myocardium and thus for improving cardiac function after MI.
While the exact mechanism responsible for the cardioprotective effects of GLP-1�based
therapies is not fully understood, a number of pathways have been implicated in cardiomyocyte
survival, including restoration of regional wall thickening via AKT activation and inhibition of
myocyte apoptosis via the cAMP and PI3-K pathways, as well as reduction of fibrosis, enhanced
LV remodeling, and improved LV function after MI through activation of the antioxidant gene
heme oxygenase-1 (56).
SAFETY AND TOLERABILITY OF INCRETIN-BASED THERAPY IN A HOSPITAL SETTING
The main actions of GLP-1 include enhanced insulin secretion, inhibition of glucagon release,
delayed gastric emptying, and suppressed appetite. However, because GLP-1 receptors are
present in many other tissues, including thyroid, exocrine pancreas, brain, renal tubules, and
bone, there is the potential for unwanted effects. Common side effects reported with GLP-1 and
GLP-1 RA use include nausea and vomiting, which are of particular concern in patients with
altered sensorium, who are maintained in a supine position, or who receive sedating
medications, all of which increase the risk for aspiration pneumonia. However, nausea and
gastrointestinal symptoms and risk diminish over time, and can be minimized by use of
medications (57).
DPP-4 inhibitors, as a group, are generally well-tolerated with adverse effects primarily reported
as increased nasopharyngitis, headache, and upper respiratory infections (58-62).
Renal function in hospitalized patients can fluctuate for various reasons, which may affect
DOI:10.4158/ EP13471.RA © 2014 AACE.
dosage and administration of either GLP-1 RAs or DPP-4 inhibitors. For both exenatide and
liraglutide there are post-marketing reports of renal impairment, sometimes requiring
hemodialysis or kidney transplantation (63,64). Exenatide should not be used in patients with
severe renal impairment or end-stage renal disease; caution should be used in patients with
moderate renal failure (63). Caution is also advised when initiating or escalating doses of
liraglutide in patients with renal impairment (64). All but one DPP-4 inhibitor require a dose
adjustment in patients with renal impairment. Linagliptin, with a primarily hepatobiliary route of
elimination, can be administered at the same dose level approved for patients with normal renal
function, and thus obviate the need to adjust doses as renal function changes during ICU
hospital stays.
Although post-marketing reports are rare, there is concern regarding the development of acute
pancreatitis, including fatal and nonfatal hemorrhagic or necrotizing pancreatitis, with incretin
therapies (58,60,63-65). Therefore, caution should be used in patients with abdominal pain or
postsurgical ileus.
Finally, small increases in heart rate have been observed in hospitalized patients with
cardiovascular disease (52,66). While meta-analyses of clinical trial data have not found any
adverse cardiovascular events with GLP-1 RA (67) or DPP-4 inhibitors (68), longer-term studies
in the critically ill are needed, though two prospective CV outcome trials have recently been
reported for alogliptin and saxagliptin showing no increased risk (69,70).
INCRETIN-BASED APPROACH IN HOSPITALIZED PATIENTS
Current practice guidelines do not support the use of incretins for the management of inpatient
hyperglycemia (Table 1). However, there is increasing evidence on the safety and efficacy of
DOI:10.4158/ EP13471.RA © 2014 AACE.
these agents in the management of hyperglycemia in general medicine and surgical patients
(14) and in critically ill patients in the ICU (50). The use of incretin therapy has been shown to
improve glycemic control and to avoid or reduce the need for insulin administration while
minimizing the risk of hypoglycemia in perioperative settings.
Incretin Therapy in Non-ICU Setting
The results of our recent pilot study indicated that patients with T2DM treated with diet, oral
antidiabetic agents, and low-dose insulin (daily dose ≤0.4 unit/kg) can be safely treated with a
daily dose of DPP-4 inhibitor plus correction (supplemental) doses of rapid-acting insulin before
meals or with the combination of DPP-4 inhibitor plus low-dose basal insulin therapy (14).
Patients on combination therapy of DPP-4 inhibitor plus basal group can be started on a total
daily dose of basal insulin of 0.25 units/kg/day, except in elderly patients (age >70 years) and/or
with a glomerular filtration rate <45 mL/min, in which case a lower starting insulin dose of 0.15
units/kg should be given. No previous randomized studies have investigated the safety and
efficacy of GLP1-RA in the management of non-ICU patients in general wards. Personal
experience of one author (SS) indicates that the subcutaneous administration of liraglutide (0.6
–1.2 mg/day) or exenatide (subcutaneous 5-10 μg twice daily) targeting blood glucose levels of
90-130 mg/dL is effective in improving glycemic control in most of these patients. If necessary,
incretin therapy can be supplemented with correction doses of rapid-acting or basal insulin
formulations, using standard protocols. While not yet supported by evidence from randomized,
controlled clinical studies, or supported by clinical practice guidelines, GLP-1 therapy in a
hospital setting has the potential to improve glycemic control and to reduce the need for insulin
therapy.
DOI:10.4158/ EP13471.RA © 2014 AACE.
Incretin Therapy in Critically Ill and ICU Patients
Increasing evidence indicates that the use of native GLP-1 and GLP-1 RA infusions in the
inpatient setting improve glucose control with low frequency of hypoglycemia and lower need for
insulin administration (46,53). In one study of 20 surgical patients undergoing CABG, glycemic
control and LV function were compared between patients on GLP-1 infusion (1.5 pmol/kg/min)
for 48-h and those receiving standard care (71). In that study, there were no differences in
postoperative blood glucose levels between treatment groups. In addition, there were no
differences in insulin levels, hemodynamic parameters, or the number of hypoglycemic events
during the study period. In a different study, 20 insulin-naïve patients with T2DM were randomly
assigned to 12-h infusions of GLP-1 (3.6 pmol/kg/min) or insulin following elective CABG
procedures (46). The incretin-treated group had similar glycemic control with less insulin and
lower dose adjustments following surgery compared with the insulin-treated group (46). In
cardiac patients, several studies administering native GLP-1 infusions reported improvement in
LV function following acute MI and in patients with congestive heart failure (53).
Two recent small, uncontrolled pilot studies investigated the use of GLP-1 RA for
glycemic management in critically ill patients (50,72). One open-label study compared the
efficacy and safety of subcutaneous administration of exenatide at doses of 5 to 10 mg every 12
h versus standard intensive insulin therapy in severely burned pediatric patients without
diabetes (72). Similar levels of glycemic control were achieved in both dose groups; however,
the dose of administered insulin was significantly lower in the exenatide group. In that study, the
number of blood glucose determinations was identical, as was the incidence of hypoglycemia,
and there were no reported gastrointestinal side effects. In another nonrandomized,
uncontrolled, open-label pilot study evaluating the safety and efficacy of IV exenatide in 40
cardiac ICU patients, 75% of whom had T2DM (50), subjects received an initial 30-min bolus of
DOI:10.4158/ EP13471.RA © 2014 AACE.
0.05 mg/min followed by 0.025 mg/min for 24-48 h. Exenatide infusions resulted in similar mean
steady state glucose and hypoglycemic events when compared with historic control subjects
treated with IV insulin infusions targeting blood glucose 90-119 mg/dL or 100-140 mg/dL.
Hypoglycemia was reported in 10% of patients receiving exenatide compared with 21 and 15%
in those treated with IV insulin. A total of 8 (20%) patients experienced nausea due to exenatide
treatment and 6 (15%) requested early termination because of severe nausea (50).
CLINICAL IMPLICATIONS – How to Minimize Hypoglycemia with Incretins
GLP-1 RA and DPP-4 inhibitors potentiate and augment glucose-dependent insulin secretion;
however, their insulinotropic action is glucose dependent. Thus the risk of hypoglycemia is
minimal if used as monotherapy. In combination with insulin therapy, the reported rate of
hypoglycemia with the use of GLP-1 RAs in the hospital has ranged between 0 and 15% (15).
The use of DPP-4 inhibitors alone should not lead to hypoglycemia as recently shown in the
sitagliptin inpatient trial (14).
CONCLUSION
Hyperglycemia is common in hospitalized patients with and without prior history of diabetes and
is an independent marker of morbidity and mortality in both critically and non-critically ill
patients. Incretin therapy has the potential to achieve improved glycemic control with a low risk
of hypoglycemia (when used without sulfonylureas, glinides, or insulin) and counteract the
hyperglycemic effects of stress hormones. In addition, incretin treatment may have favorable
cardiovascular and metabolic effects (blood pressure, lipid parameters, body weight, ventricular
function) and preventable and controllable minimal gastrointestinal side effects, and may reduce
the need for insulin (Table 3).
DOI:10.4158/ EP13471.RA © 2014 AACE.
The preliminary research experience in native GLP-1 therapy is promising and GLP-1
has the potential to improve cardiac function in patients with heart failure and acute ischemic
cardiovascular events (51,53). It is possible that these favorable results may extend to the use
of GLP-1 RA and DPP-4 inhibitors; however, large, randomized controlled clinical trials are
needed before recommending the widespread use of these agents in the hospital setting.
ACKNOWLEDGMENT
G.E.U. is supported in part by research grants from the American Diabetes Association (7-03-
CR-35) and PHS Grant UL1-RR-025008 from the Clinical and Translational Science Award
program, National Institutes of Health, National Center for Research Resources. He has
received research support (to Emory University) from Sanofi, Merck, Boehringer Ingelheim and
Novo Nordisk, and honoraria for consulting from Sanofi, Novo Nordisk, and Boehringer
Ingelheim
S. S. is on the advisory boards of Novo, Takeda, Merck, and Astra-Zeneca – BMS, and a
member of the speaker's bureaus for Novo, Takeda, Merck, Santarus, BI-Lilly, A-Z- BMS-
Amylin.
The authors were fully responsible for all content and editorial decisions, involved at all stages
of manuscript development, and have approved the final version of the review that reflects the
authors’ interpretation and conclusions. Medical writing assistance, supported financially by
Boehringer Ingelheim, was provided by Linda Merkel, PhD, of Envision Scientific Solutions
during the preparation of this review. Boehringer Ingelheim was given the opportunity to check
the data used in the manuscript for factual accuracy only.
DOI:10.4158/ EP13471.RA © 2014 AACE.
REFERENCES
1. Kosiborod M, Rathore SS, Inzucchi SE, et al. Admission glucose and mortality in
elderly patients hospitalized with acute myocardial infarction: implications for patients
with and without recognized diabetes. Circulation. 2005;111:3078-3086.
2. Swanson CM, Potter DJ, Kongable GL, Cook CB. Update on inpatient glycemic
control in hospitals in the United States. Endocr Pract. 2011;17:853-861.
3. Umpierrez GE, Isaacs SD, Bazargan N, et al. Hyperglycemia: an independent marker
of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab.
2002;87:978-982.
4. Falciglia M, Freyberg RW, Almenoff PL, D'Alessio DA, Render ML. Hyperglycemia-
related mortality in critically ill patients varies with admission diagnosis. Crit Care Med.
2009;37:3001-3009.
5. Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces
mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac
Cardiovasc Surg. 2003;125:1007-1021.
6. Umpierrez GE, Smiley D, Jacobs S, et al. Randomized study of basal-bolus insulin
therapy in the inpatient management of patients with type 2 diabetes undergoing general
surgery (RABBIT 2 surgery). Diabetes Care. 2011;34:256-261.
7. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically
ill patients. N Engl J Med. 2001;345:1359-1367.
8. Finfer S, Chittock DR, Su SY, et al. Intensive versus conventional glucose control in
critically ill patients. N Engl J Med. 2009;360:1283-1297.
DOI:10.4158/ EP13471.RA © 2014 AACE.
9. Griesdale DE, de Souza RJ, van Dam RM, et al. Intensive insulin therapy and mortality
among critically ill patients: a meta-analysis including NICE-SUGAR study data. Cmaj.
2009;180:821-827.
10. Preiser JC, Devos P, Ruiz-Santana S, et al. A prospective randomised multi-centre
controlled trial on tight glucose control by intensive insulin therapy in adult intensive care
units: the Glucontrol study. Intensive Care Med. 2009;35:1738-1748.
11. Finfer S, Liu B, Chittock DR, et al. Hypoglycemia and risk of death in critically ill
patients. N Engl J Med. 2012;367:1108-1118.
12. Moghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical
Endocrinologists and American Diabetes Association consensus statement on inpatient
glycemic control. Diabetes Care. 2009;32:1119-1131.
13. Schwartz S, Defronzo RA. Is incretin-based therapy ready for the care of hospitalized
patients with type 2 diabetes? The time has come for GLP-1 receptor agonists! Diabetes
Care. 2013;36:2107-2111.
14. Umpierrez GE, Gianchandani R, Smiley D, et al. Safety and efficacy of sitagliptin
therapy for the inpatient management of general medicine and surgery pateints with type
2 diabetes. Diabetes Care. 2013 36: [epub] 22 July. doi: 10.2337/dc2313-0277.
15. Umpierrez GE, Korytkowski M. Is Incretin-based therapy ready for the care of
hospitalized patients with type 2 diabetes?: Insulin therapy has proven itself and is
considered the mainstay of treatment. Diabetes Care. 2013;36:2112-2117.
16. Mannucci E, Dicembrini I. Incretin-based therapies and cardiovascular risk. Curr Med
Res Opin. 2012;28:715-721.
17. Jiang HJ, Stryer D, Friedman B, Andrews R. Multiple hospitalizations for patients with
diabetes. Diabetes Care. 2003;26:1421-1426.
DOI:10.4158/ EP13471.RA © 2014 AACE.
18. Cook CB, Kongable GL, Potter DJ, et al. Inpatient glucose control: a glycemic survey
of 126 U.S. hospitals. J Hosp Med. 2009;4:E7-E14.
19. Greci LS, Kailasam M, Malkani S, et al. Utility of HbA(1c) levels for diabetes case
finding in hospitalized patients with hyperglycemia. Diabetes Care. 2003;26:1064-1068.
20. Sinnaeve PR, Steg PG, Fox KA, et al. Association of elevated fasting glucose with
increased short-term and 6-month mortality in ST-segment elevation and non-ST-
segment elevation acute coronary syndromes: the Global Registry of Acute Coronary
Events. Arch Intern Med. 2009;169:402-409.
21. Kosiborod M. Blood glucose and its prognostic implications in patients hospitalised with
acute myocardial infarction Diab Vasc Dis Res. 2008;5:269-275.
22. Baker ST, Chiang CY, Zajac JD, et al. Outcomes for general medical inpatients with
diabetes mellitus and new hyperglycaemia. Med J Aust. 2008;188:340-343.
23. Fraze TK, Jiang HJ, Burgess J. Hospital Stays for Patients with Diabetes, 2008. HCUP
Statistical Brief #93. August 2010. Agency for Healthcare Research and Quality.
Rockville, MD. http://www.hcup-us.arhq.gov/reports/statbriefs/sb93.pdf. 2008;
24. Zerr KJ, Furnary AP, Grunkemeier GL, et al. Glucose control lowers the risk of wound
infection in diabetics after open heart operations. Ann Thorac Surg. 1997;63:356-361.
25. Esposito K, Nappo F, Marfella R, et al. Inflammatory cytokine concentrations are
acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation.
2002;106:2067-2072.
26. Stentz FB, Umpierrez GE, Cuervo R, Kitabchi AE. Proinflammatory cytokines,
markers of cardiovascular risks, oxidative stress, and lipid peroxidation in patients with
hyperglycemic crises. Diabetes. 2004;53:2079-2086.
DOI:10.4158/ EP13471.RA © 2014 AACE.
27. del Aguila LF, Claffey KP, Kirwan JP. TNF-alpha impairs insulin signaling and insulin
stimulation of glucose uptake in C2C12 muscle cells. Am J Physiol. 1999;276:E849-855.
28. Robinson LE, van Soeren MH. Insulin resistance and hyperglycemia in critical illness:
role of insulin in glycemic control. AACN Clin Issues. 2004;15:45-62.
29. Ceriello A, Quagliaro L, D'Amico M, et al. Acute hyperglycemia induces nitrotyrosine
formation and apoptosis in perfused heart from rat. Diabetes. 2002;51:1076-1082.
30. Gresele P, Guglielmini G, De Angelis M, et al. Acute, short-term hyperglycemia
enhances shear stress-induced platelet activation in patients with type II diabetes
mellitus. J Am Coll Cardiol. 2003;41:1013-1020.
31. Pandolfi A, Giaccari A, Cilli C, et al. Acute hyperglycemia and acute hyperinsulinemia
decrease plasma fibrinolytic activity and increase plasminogen activator inhibitor type 1
in the rat. Acta Diabetol. 2001;38:71-76.
32. Dombrowski NC, Karounos DG. Pathophysiology and management strategies for
hyperglycemia for patients with acute illness during and following a hospital stay.
Metabolism. 2013;62:326-336.
33. Chaudhuri A, Dandona P, Fonseca V. Cardiovascular benefits of exogenous insulin. J
Clin Endocrinol Metab. 2012;97:3079-3091.
34. Dandona P, Mohanty P, Chaudhuri A, Garg R, Aljada A. Insulin infusion in acute
illness. J Clin Invest. 2005;115:2069-2072.
35. Haga KK, McClymont KL, Clarke S, et al. The effect of tight glycaemic control, during
and after cardiac surgery, on patient mortality and morbidity: A systematic review and
meta-analysis. J Cardiothorac Surg. 2011;6:3.
DOI:10.4158/ EP13471.RA © 2014 AACE.
36. Ng KW, Allen ML, Desai A, Macrae D, Pathan N. Cardioprotective effects of insulin:
how intensive insulin therapy may benefit cardiac surgery patients. Circulation.
2012;125:721-728.
37. Rashidee A, Hart J, Chen J, Kumar S. High-alert medications: error prevalence and
severity. Available at: http://www.psqh.com/julyaugust-2009/164-data-trends.html
(accessed September 6, 2013).
38. Marik PE, Preiser JC. Toward understanding tight glycemic control in the ICU: a
systematic review and metaanalysis. Chest. 2010;137:544-551.
39. Desouza C, Salazar H, Cheong B, Murgo J, Fonseca V. Association of hypoglycemia
and cardiac ischemia: a study based on continuous monitoring. Diabetes Care.
2003;26:1485-1489.
40. Sechterberger MK, Bosman RJ, Oudemans-van Straaten HM, et al. The effect of
diabetes mellitus on the association between measures of glycaemic control and
intensive care unit mortality: a retrospective cohort study. Crit Care. 2013;17:R52.
41. Jacobi J, Bircher N, Krinsley J, et al. Guidelines for the use of an insulin infusion for
the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40:3251-
3276.
42. Desouza CV, Bolli GB, Fonseca V. Hypoglycemia, diabetes, and cardiovascular
events. Diabetes Care. 2010;33:1389-1394.
43. Rana OA, Byrne CD, Greaves K. Intensive glucose control and hypoglycaemia: a new
cardiovascular risk factor? Heart. 2013 [epub] 22 May. doi: 10.1136/heartjnl-2013-
303871 Web site. http://heart.bmj.com/content/early/2013/05/21/heartjnl-2013-
303871.abstract. Accessed September 6, 2013.
DOI:10.4158/ EP13471.RA © 2014 AACE.
44. Nauck MA. A Critical Analysis of the Clinical Use of Incretin-Based Therapies: The
benefits by far outweigh the potential risks. Diabetes Care. 2013;36:2126-2132.
45. Deane AM, Chapman MJ, Fraser RJ, et al. The effect of exogenous glucagon-like
peptide-1 on the glycaemic response to small intestinal nutrient in the critically ill: a
randomised double-blind placebo-controlled cross over study. Crit Care. 2009;13:R67.
46. Mussig K, Oncu A, Lindauer P, et al. Effects of intravenous glucagon-like peptide-1 on
glucose control and hemodynamics after coronary artery bypass surgery in patients with
type 2 diabetes. Am J Cardiol. 2008;102:646-647.
47. Ritzel RA, Kleine N, Holst JJ, et al. Preserved GLP-1 effects in a diabetic patient with
Cushing's disease. Exp Clin Endocrinol Diabetes. 2007;115:146-150.
48. van Raalte DH, van Genugten RE, Linssen MM, Ouwens DM, Diamant M. Glucagon-
like peptide-1 receptor agonist treatment prevents glucocorticoid-induced glucose
intolerance and islet-cell dysfunction in humans. Diabetes Care. 2011;34:412-417.
49. Kohl BA, Hammond MS, Schwartz S, Ochroch EO. Intravenous exenatide (Byetta) for
the treatment of perioperative hyperglycemia. Paper presented at: Society of Critical
Care Medicine’s 40th Critical Care Congress; January 15-19, 2011; San Diego, CA.
50. Abuannadi M, Kosiborod M, Riggs L, et al. Management of hyperglycemia with the
administration of intravenous exenatide to patients in the cardiac intensive care unit.
Endocr Pract. 2013;19:81-90.
51. Sokos GG, Bolukoglu H, German J, et al. Effect of glucagon-like peptide-1 (GLP-1) on
glycemic control and left ventricular function in patients undergoing coronary artery
bypass grafting. Am J Cardiol. 2007;100:824-829.
DOI:10.4158/ EP13471.RA © 2014 AACE.
52. Sokos GG, Nikolaidis LA, Mankad S, Elahi D, Shannon RP. Glucagon-like peptide-1
infusion improves left ventricular ejection fraction and functional status in patients with
chronic heart failure. J Card Fail. 2006;12:694-699.
53. Nikolaidis LA, Mankad S, Sokos GG, et al. Effects of glucagon-like peptide-1 in
patients with acute myocardial infarction and left ventricular dysfunction after successful
reperfusion. Circulation. 2004;109:962-965.
54. Read PA, Khan FZ, Heck PM, Hoole SP, Dutka DP. DPP-4 inhibition by sitagliptin
improves the myocardial response to dobutamine stress and mitigates stunning in a pilot
study of patients with coronary artery disease. Circ Cardiovasc Imaging. 2010;3:195-
201.
55. Theiss HD, Brenner C, Engelmann MG, et al. Safety and efficacy of SITAgliptin plus
GRanulocyte-colony-stimulating factor in patients suffering from Acute Myocardial
Infarction (SITAGRAMI-Trial)--rationale, design and first interim analysis. Int J Cardiol.
2010;145:282-284.
56. Anagnostis P, Athyros VG, Adamidou F, et al. Glucagon-like peptide-1-based
therapies and cardiovascular disease: looking beyond glycaemic control. Diabetes Obes
Metab. 2011;13:302-312.
57. Ellero C, Han J, Bhavsar S, et al. Prophylactic use of anti-emetic medications reduced
nausea and vomiting associated with exenatide treatment: a retrospective analysis of an
open-label, parallel-group, single-dose study in healthy subjects. Diabet Med.
2010;27:1168-1173.
58. Januvia (sitagliptin) tablets prescribing information. Merck & Co Inc Web site.
http://www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf. Accessed
September 6, 2013.

DOI:10.4158/ EP13471.RA © 2014 AACE.
59. Onglyza (saxagliptin) prescribing information. Briston-Myers Squibb Company Web site.
http://packageinserts.bms.com/pi/pi_onglyza.pdf. Accessed September 6, 2013.
60. GALVUS (vildagliptin). Novartis Pharmaceuticals Australia Pty Ltd Web site.
http://www.novartis.com.au/PI_PDF/gal.pdf. Accessed September 6, 2013.
61. TRADJENTA (linagliptin) Prescribing Information. Boehringer Ingelheim
Pharmaceuticals, Inc. Web site. Accessed Oct 21, 2013.
62. NESINA (alogliptin) Prescribing Information Takeda Pharmaceuticals America, Inc. Web
site. Accessed October 21, 2013.
63. Byetta (exenatide) prescribing information. Amylin Pharmaceuticals Inc Web site.
http://packageinserts.bms.com/pi/pi_byetta.pdf. Accessed September 6, 2013.
64. Victoza (liraglutide) rDNA injection prescribing information Novo Nordisk Inc Web site.
http://www.novo-pi.com/victoza.pdf. Accessed September 6, 2013.
65. Onglyza (saxagliptin) Prescribing Information. Briston-Myers Squibb Company,
Princeton, NJ. Available at: (accessed
66. Halbirk M, Norrelund H, Moller N, et al. Cardiovascular and metabolic effects of 48-h
glucagon-like peptide-1 infusion in compensated chronic patients with heart failure. Am J
Physiol Heart Circ Physiol. 2010;298:H1096-1102.
67. Monami M, Cremasco F, Lamanna C, et al. Glucagon-like peptide-1 receptor agonists
and cardiovascular events: a meta-analysis of randomized clinical trials. Exp Diabetes
Res. 2011;2011:215764.
68. Monami M, Dicembrini I, Martelli D, Mannucci E. Safety of dipeptidyl peptidase-4
inhibitors: a meta-analysis of randomized clinical trials. Curr Med Res Opin. 2011;27
Suppl 3:57-64.
DOI:10.4158/ EP13471.RA © 2014 AACE.
69. Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in
patients with type 2 diabetes mellitus. N Engl J Med. 2013;369:1317-1326.
70. White WB, Pratley R, Fleck P, et al. Cardiovascular safety of the dipetidyl peptidase-4
inhibitor alogliptin in type 2 diabetes mellitus. Diabetes Obes Metab. 2013;
71. Meier JJ, Weyhe D, Michaely M, et al. Intravenous glucagon-like peptide 1 normalizes
blood glucose after major surgery in patients with type 2 diabetes. Crit Care Med.
2004;32:848-851.
72. Mecott GA, Herndon DN, Kulp GA, et al. The use of exenatide in severely burned
pediatric patients. Crit Care. 2010;14:R153.
73. American Diabetes Association. Standards of medical care in diabetes--2013. Diabetes
Care. 2013;36 (suppl 1):S11-66.
74. Qaseem A, Humphrey LL, Chou R, Snow V, Shekelle P. Use of intensive insulin
therapy for the management of glycemic control in hospitalized patients: a clinical
practice guideline from the American College of Physicians. Ann Intern Med.
2011;154:260-267.
75. Umpierrez GE, Hellman R, Korytkowski MT, et al. Management of hyperglycemia in
hospitalized patients in non-critical care setting: an Endocrine Society clinical practice
guideline. J Clin Endocrinol Metab. 2013;97:16-38.
76. Lazar HL, McDonnell M, Chipkin SR, et al. The Society of Thoracic Surgeons practice
guideline series: blood glucose management during adult cardiac surgery. Ann Thorac
Surg. 2009;87:663-669.
77. Kohl BA, Hammond MS, Cucchiara AJ, Ochroch EO. Intravenous GLP-1 (7-36)
amide for prevention of hyperglycemia during cardiac surgery: a randomized, double-
blind, placebo controlled study. J Cardiothorac Vasc Anesth. 2013 [in press]

DOI:10.4158/ EP13471.RA © 2014 AACE.
78. Sourij H, Schmolzer I, Kettler-Schmut E, et al. Efficacy of a continuous GLP-1 infusion
compared with a structured insulin infusion protocol to reach normoglycemia in
nonfasted type 2 diabetic patients: a clinical pilot trial. Diabetes Care. 2009;32:1669-
1671.
79. Lonborg J, Kelbaek H, Vejlstrup N, et al. Exenatide reduces final infarct size in
patients with ST-segment-elevation myocardial infarction and short-duration of ischemia.
Circ Cardiovasc Interv. 2012;5:288-295.
DOI:10.4158/ EP13471.RA © 2014 AACE.
TABLE 1. MAJOR GUIDELINES FOR TREATMENT OF HYPERGLYCEMIA IN A HOSPITAL SETTING
Critically ill patients Non-critically ill patients
ADA (73)
Initiate insulin therapy for persistent hyperglycemia starting at a threshold ≤140-180 mg/dL More stringent goals (110-140 mg/dL) may be appropriate for selected patients, if achievable without significant risk for hypoglycemia
No specific guidelines If treated with insulin, pre-meal BG targets should generally be <140 mg/dL, with random BG levels <180 mg/dL More stringent targets may be appropriate for patients with previously tight glycemic control Less stringent targets may be appropriate in patients with severe comorbidities
AACE/ ADA (12)
ICU starting threshold ≤180 mg/dL With insulin, BG level should be maintained between 140-180 mg/dL Lower glucose targets (110-140 mg/dL) may be appropriate for specific patients Targets <110 mg/dL and >180 mg/dL not recommended
—
ACP (74)
Recommends not using intensive insulin therapy in patients with or without diabetes in surgical/medical ICUs Recommends not using intensive insulin therapy to normalize BG in patients with or without diabetes in surgical/medical ICUs Recommends target BG 140-200 mg/dL if insulin therapy is used in patients with or without diabetes in surgical/medical ICUs
—
ENDO (75)
— Consistent with ADA Pre-meal BG targets should generally be <140 mg/dL, with random BG <180 mg/dL A lower target range may be appropriate in patients able to achieve and maintain glycemic control without hypoglycemia Less stringent targets (<200 mg/dL) may be appropriate in patients with terminal illness and/or with limited life expectancy or at high risk for
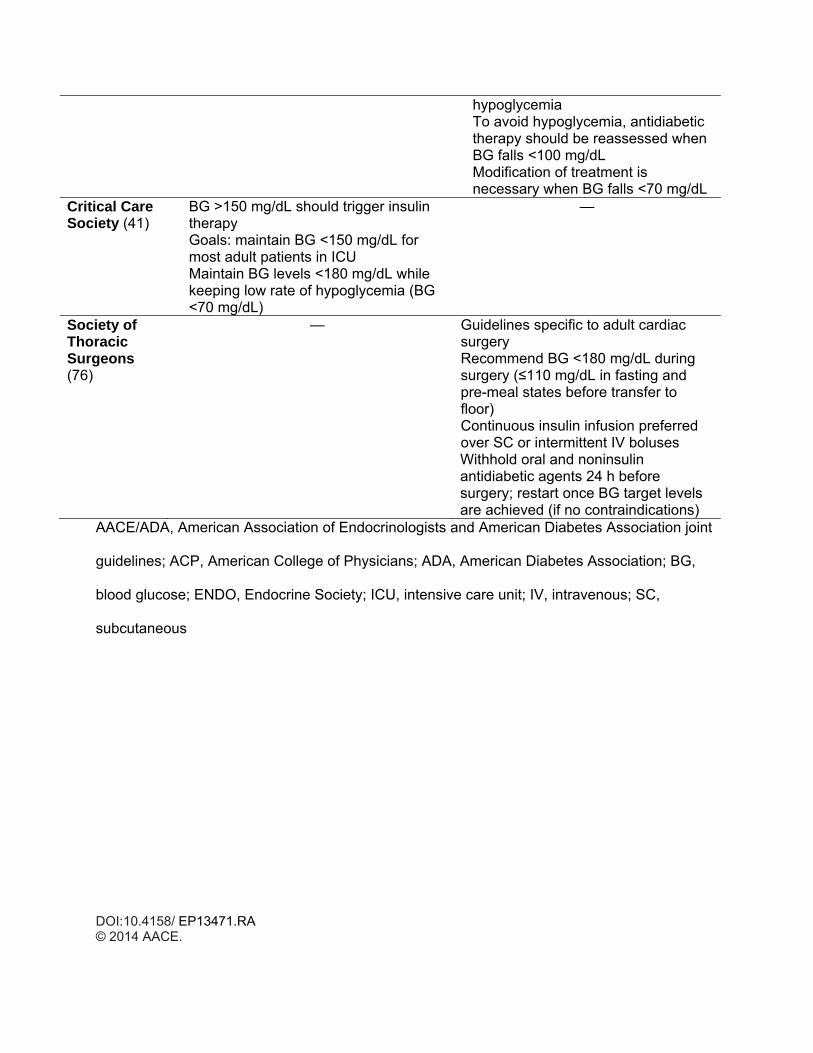
DOI:10.4158/ EP13471.RA © 2014 AACE.
hypoglycemia To avoid hypoglycemia, antidiabetic therapy should be reassessed when BG falls <100 mg/dL Modification of treatment is necessary when BG falls <70 mg/dL
Critical Care Society (41)
BG >150 mg/dL should trigger insulin therapy Goals: maintain BG <150 mg/dL for most adult patients in ICU Maintain BG levels <180 mg/dL while keeping low rate of hypoglycemia (BG <70 mg/dL)
—
Society of Thoracic Surgeons (76)
— Guidelines specific to adult cardiac surgery Recommend BG <180 mg/dL during surgery (≤110 mg/dL in fasting and pre-meal states before transfer to floor) Continuous insulin infusion preferred over SC or intermittent IV boluses Withhold oral and noninsulin antidiabetic agents 24 h before surgery; restart once BG target levels are achieved (if no contraindications)
AACE/ADA, American Association of Endocrinologists and American Diabetes Association joint
guidelines; ACP, American College of Physicians; ADA, American Diabetes Association; BG,
blood glucose; ENDO, Endocrine Society; ICU, intensive care unit; IV, intravenous; SC,
subcutaneous
DOI:10.4158/ EP13471.RA © 2014 AACE.
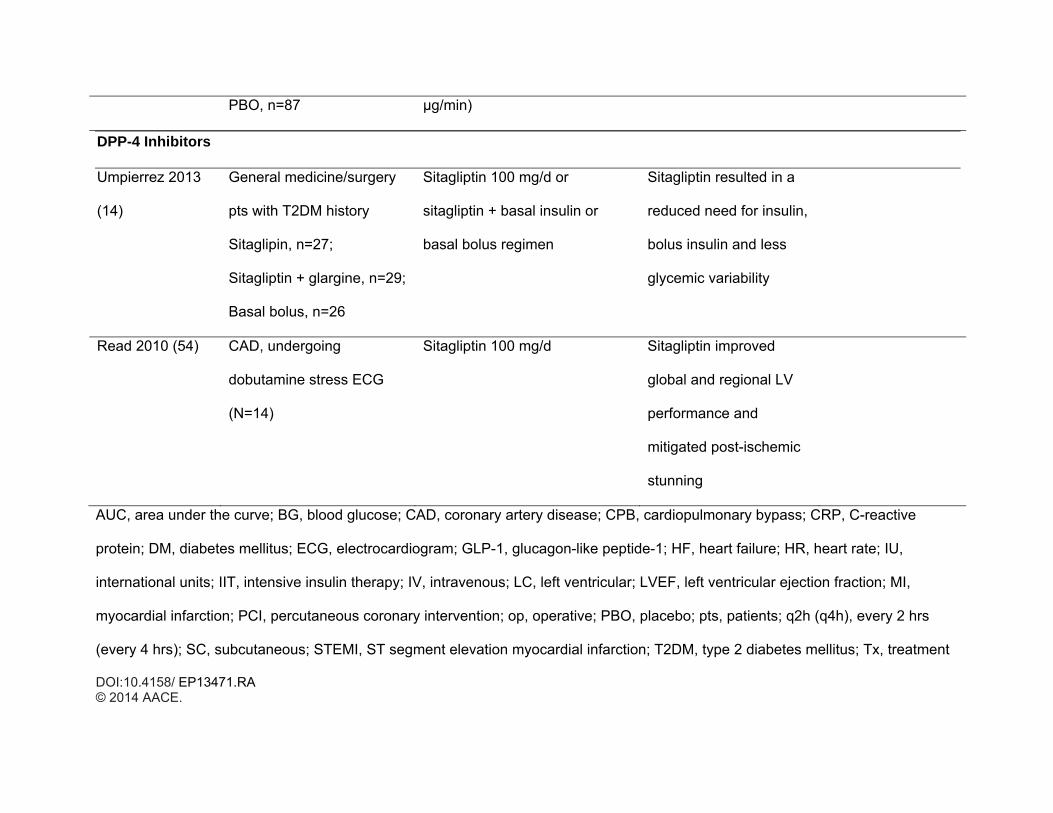
TABLE 2. USE OF INCRETINS IN A HOSPITAL SETTING
Patient population Intervention Results Adverse Events
Native GLP-1 — Metabolic Effects
Kohl 2013 (77) DM and non-DM pts
undergoing elective CPB,
N=77; DM, n=11
1:1 randomization
GLP-1 infusion 1.5 pmol/kg/min
or PBO
Mean BG overall and
during CPB lower by
12.2 mg/dL vs 14.1
mg/dL, GLP-1 vs PBO
None
Sourij 2009 (78) Clinically stable with DM,
n=8
GLP-1 IV
1.2 pmol/kg/min or insulin IV,
after standard breakfast
GLP-1, lower BG at max
and after 2 and 4 h
Deane 2009 (45) ICU, non-DM, mechanically
ventilated, enteral nutrition,
n=7
GLP-1 IV; 4.5 h
1.2 pmol/kg/min vs placebo
Significantly ↓AUC for
glucose
None
Müssig 2008 (46) Post CABG, insulin-naïve,
T2DM
GLP-1, n=10;
GLP-1; 12 h
3.6 pmol/kg/min vs insulin
GLP-1: Glycemic control
similar to insulin group;
fewer insulin
None
GLP-1: Insulin
rescue therapy
DOI:10.4158/ EP13471.RA © 2014 AACE.
Insulin, n=10 adjustments in first 6 h
Control: higher insulin
requirement in controls
needed for several
pts
Meier 2004 (71) 2-8 days post major
surgery, fasting, N=8;
DM, n=8
GLP-1 IV; 8 h
1.2 pmol/kg/min vs PBO
↓BG levels, ↑insulin and
CRP, suppressed
glucagon
None
GLP-1 Receptor Agonists — Metabolic Effects
Van Raalte 2011
(48)
Healthy men receiving
prednisone 80 mg, N=8
Exenatide IV Normalization of
prednisone-increased
glucose intolerance and
islet-cell dysfunction
Abuannadi 2013
(50)
Cardiac ICU, n=40;
DM, exenatide, n=40;
Historic controls treated
with insulin, n=133
Exenatide infusion up to 48 h
0.025 μg/min
Steady-state BG level
was similar between
groups
Nausea, n=16;
vomiting, n=2, no
episodes of severe
hypoglycemia (<50
mg/dL)
Native GLP-1 — Cardiovascular Effects
DOI:10.4158/ EP13471.RA © 2014 AACE.
Halbirk 2010 (66) Ischemic HF, non-DM
GLP-1, n=10;
PBO, n=10
GLP-1 IV; 48 h
1.0 pmol/kg/min vs PBO
GLP-1 ↑insulin and ↓BG
levels; no effect on
LVEF, diastolic function
or regional myocardial
contractility
GLP-1,
hypoglycemic
events (n=8)
Mecott 2010 (72) Severely burned pediatric
pts
Exenatide, n=6;
IIT, n=18
Exenatide SC starting at 5 μg
q12 up to 10 μg q4
IIT 0.1-1.0 U/kg/h
BG target 80-140 mg/dL
Exenatide group
required significantly less
insulin than IIT group (22
vs 76 IU, respectively)
Incidence of
hypoglycemia was
similar in both
groups (0.38
events/pt-months)
Sokos 2007 (51) Pre and post CABG
GLP-1, n=10 (DM, n=2);
Insulin, n=10 (DM, n=3)
GLP-1 IV; 12 h before to 48 h
after CABG
1.5 pmol/kg/min vs standard IV
insulin
Significant ↓ AUC for
glucose pre- and intra-
op, no difference post-op
No difference in LVEF
GLP-1: rescue
insulin therapy, n=5;
Hypoglycemia, n=1;
Control,
hypoglycemia, n=2
Sokos 2006 (52) CHF
GLP-1, n=12 (DM, n=8);
GLP-1 SC
5 wks Tx:
GLP-1 ↑ LVEF, 6-min
walk test, ↓BG vs
GLP-1: nausea,
constipation (n=5);

DOI:10.4158/ EP13471.RA © 2014 AACE.
Control, n=9 (DM, n=5) 1 wk @1.25 pmol/kg/min
4 wks @ 2.5 pmol/kg/min
controls increase in HR;
hypoglycemia, n=4
(9 episodes);
Control:
hypoglycemia, n=2
(4 episodes)
Nikolaidis 2004
(53)
Acute MI, LVEF <40%
GLP-1, n=10 (DM, n=5);
Control, n=11(DM, n=4)
GLP-1 IV; 72 h post
angiography
1.5 pmol/kg/min vs standard
therapy
Glycemic control similar
between groups; GLP-1
significantly ↑LVEF,
global and regional wall
motion indices
GLP-1: nausea
(n=4), vomiting
(n=2), constipation
(n=2), reduced
appetite (n=2),
asymptomatic
hypoglycemia (n=2)
GLP-1 Receptor Agonists — Cardiovascular Effects
Lonborg 2012
(79)
STEMI treated with primary
PCI
Exenatide, n=85;
Exenatide infusion, starting 15
min prior to PCI (0.12 μg/min)
and continuing 6 h (0.043
Myocardial salvage
increased with exenatide
DOI:10.4158/ EP13471.RA © 2014 AACE.
PBO, n=87 μg/min)
DPP-4 Inhibitors
Umpierrez 2013
(14)
General medicine/surgery
pts with T2DM history
Sitaglipin, n=27;
Sitagliptin + glargine, n=29;
Basal bolus, n=26
Sitagliptin 100 mg/d or
sitagliptin + basal insulin or
basal bolus regimen
Sitagliptin resulted in a
reduced need for insulin,
bolus insulin and less
glycemic variability
Read 2010 (54) CAD, undergoing
dobutamine stress ECG
(N=14)
Sitagliptin 100 mg/d Sitagliptin improved
global and regional LV
performance and
mitigated post-ischemic
stunning
AUC, area under the curve; BG, blood glucose; CAD, coronary artery disease; CPB, cardiopulmonary bypass; CRP, C-reactive
protein; DM, diabetes mellitus; ECG, electrocardiogram; GLP-1, glucagon-like peptide-1; HF, heart failure; HR, heart rate; IU,
international units; IIT, intensive insulin therapy; IV, intravenous; LC, left ventricular; LVEF, left ventricular ejection fraction; MI,
myocardial infarction; PCI, percutaneous coronary intervention; op, operative; PBO, placebo; pts, patients; q2h (q4h), every 2 hrs
(every 4 hrs); SC, subcutaneous; STEMI, ST segment elevation myocardial infarction; T2DM, type 2 diabetes mellitus; Tx, treatment
DOI:10.4158/ EP13471.RA © 2014 AACE.
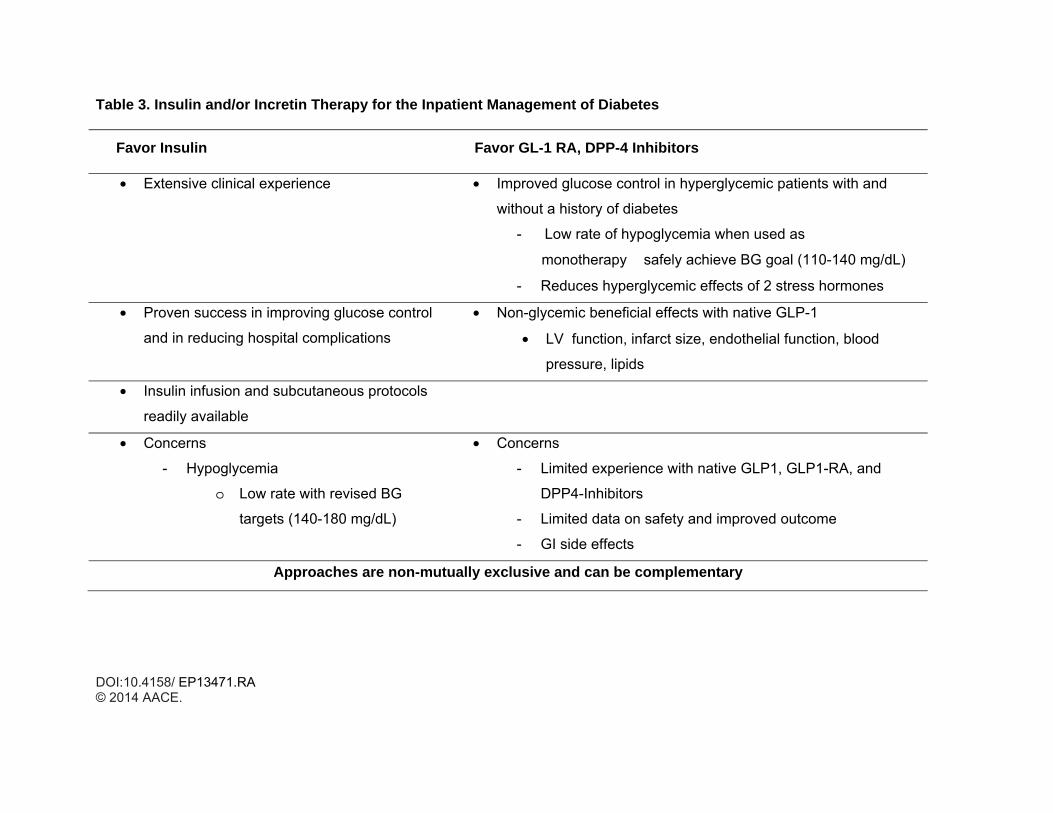
Table 3. Insulin and/or Incretin Therapy for the Inpatient Management of Diabetes
Favor Insulin Favor GL-1 RA, DPP-4 Inhibitors
• Extensive clinical experience • Improved glucose control in hyperglycemic patients with and
without a history of diabetes
- Low rate of hypoglycemia when used as
monotherapy � safely achieve BG goal (110-140 mg/dL)
- Reduces hyperglycemic effects of 2 stress hormones
• Proven success in improving glucose control
and in reducing hospital complications
• Non-glycemic beneficial effects with native GLP-1
• LV function, infarct size, endothelial function, blood
pressure, lipids
• Insulin infusion and subcutaneous protocols
readily available
• Concerns
- Hypoglycemia
o Low rate with revised BG
targets (140-180 mg/dL)
• Concerns
- Limited experience with native GLP1, GLP1-RA, and
DPP4-Inhibitors
- Limited data on safety and improved outcome
- GI side effects
Approaches are non-mutually exclusive and can be complementary
DOI:10.4158/ EP13471.RA © 2014 AACE.





























