Embed Size (px)
Citation preview
1 of 73
Number: 0270
Policy
*Please see amendment for Pennsylvania Medicaid at the
end of this CPB.
I. Aetna considers proton beam radiotherapy (PBRT) medically
necessary in any of the following radiosensitive tumors:
A. Chordomas or chondrosarcomas arising at the base of the
skull or cervical spine without distant metastases; or
B. Malignancies in children (21 years of age and younger); or
C. Uveal melanomas confined to the globe (i.e., not distant
metastases) (the uvea is comprised of the iris, ciliary body,
and choroid [the vascular middle coat of the eye]).
Last Review 03/09/2017
Effective: 07/16/1998
Next Review: 03/08/2018
Review History
Definitions
II. Aetna considers proton beam radiotherapy for treatment of
prostate cancer not medically necessary for individuals with
localized prostate cancer because it has not been proven to be
more effective than other radiotherapy modalities for this
indication. Proton beam therapy for metastatic prostate
cancer is considered experimental and investigational.
Clinical Policy Bulletin Notes
3 of 73 5/9/17, 11:20 AM
III. Aetna considers proton beam radiotherapy experimental and
investigational for all other indications, including the following
indications in adults (over age 21) (not an all‐inclusive list)
because its effectiveness for these indications has not been
established:
Adenoid cystic carcinoma Age‐
related macular degeneration
Angiosarcoma
Bladder cancer
Brain tumors
Breast cancer
Cardiac intimal sarcoma
Carotid body tumor
Cavernous hemangioma
Cervical cancer
Cholangiocarcinoma
Choroidal hemangioma
Dermatofibrosarcoma protuberans
Desmoid fibromatosis
Desmoid fibrosarcoma
Desmoid tumor (aggressive fibromatosis)
Ependymoma
Esophageal cancer
Ewing's sarcoma
Fibrosarcoma of the extremities
Gangliomas
Glioma
Head and neck cancer (including nasopharyngeal
carcinoma)
Hemangioendothelioma
Hepatocellular carcinoma
Hodgkin's lymphoma
Intracranial arterio‐venous malformations
Large cell lymphoma
Leiomyosarcoma of the extremities
Liver metastases
Lung cancer (including non‐small‐cell lung carcinoma)
Maxillary sinus tumor
Mesothelioma
Multiple myeloma
Nasopharyngeal tumor
Non‐Hodgkin lymphoma
4 of 73 5/9/17, 11:20 AM
Non‐uveal melanoma
Oligodendroglioma Optic
nerve schwannoma
Optic nerve sheath meningioma
Pancreatic cancer
Parotid gland tumor
Pineal tumor
Pituitary neoplasms
Rectal cancer
Retroperitoneal/pelvic sarcoma
Rhabdomyoma
Salivary gland tumors (e.g., sublingual gland tumor,
submandibular gland tumor)
Seminoma Sino‐nasal
carcinoma
Small bowel adenocarcinoma
Soft tissue sarcoma
Squamous cell carcinoma of the eyelid, tongue/glottis
Thymic tumor
Thymoma
Tonsillar cancer
Uterine cancer
Vestibular schwannoma
Yo lk cell tumor
IV. Aetna considers neutron beam therapy medically necessary
for the treatment of any of the following salivary gland
tumors:
Inoperable tumor; or
Locally advanced tumor especially in persons with gross
residual disease; or
Unresectable tumor.
V. Aetna considers neutron beam therapy experimental and
investigational for all other indications including malignancies
listed below (not an all inclusive list) because its effectiveness
for these indications has not been established:
Colon cancer
Dermatofibrosarcoma protuberans

5 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Ghost cell odontogenic carcinoma
Glioma
Kidney cancer
Laryngeal cancer
Lung cancer
Pancreatic cancer
Prostate cancer
Rectal cancer
Soft tissue sarcoma.
Background
Proton Beam Therapy
Proton beam radiation therapy (PBRT) is a type of external beam
radiation therapy (EBRT) that utilizes protons (positively charged
subatomic particles) that are precisely targeted to a specific tissue
mass. Proton beams have the ability to penetrate deep into
tissues to reach tumors, while delivering less radiation to
superficial tissues such as the skin. This may make PBRT more
effective for inoperable tumors or for those individuals in which
damage to healthy tissue would pose an unacceptable risk.
Proton beams have less scatter than other sources of energy such
as gamma rays, x‐rays, or electrons. Because of this feature,
proton beam radiotherapy (PBRT) has been used to escalate
radiation dose to diseased tissues while minimizing damage to
adjacent normal tissues. Proton beams have been used in
stereotactic radiosurgery of intracranial lesions; the gamma knife
and linear accelerator have also been used in stereotactic
radiosurgery. Proton beam radiotherapy has been shown to be
particularly useful in treating radiosensitive tumors that are
located next to vital structures, where complete surgical excision
or administration of adequate doses of conventional radiation is
difficult or impossible. Examples include uveal melanomas,
chordomas and chondrosarcomas at the base of the skull, and
inoperable arterio‐venous malformations. There is inadequate
data on the application of PBRT for the treatment of non‐uveal
melanoma.
The American Society of Radiation Oncology (ASTRO, 2013) has
6 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
stated: "At the present time, ASTRO believes the comparative
efficacy evidence of proton beam therapy with other prostate
cancer treatments is still being developed, and thus the role of
proton beam therapy for localized prostate cancer within the
current availability of treatment options remains unclear."
The emerging technology committee of the American Society of
Radiation Oncology (ASTRO) concluded that current evidence
provides a limited indication for proton beam therapy (Allen, et
al., 2012). The ASTRO report concluded that current data do not
provide sufficient evidence to recommend proton beam therapy
in lung cancer, head and neck cancer, gastrointestinal
malignancies, and pediatric non‐CNS malignancies. The ASTRO
report stated that, in hepatocellular carcinoma and prostate
cancer, there is evidence for the efficacy of proton beam
therapy but no suggestion that it is superior to photon based
approaches. In pediatric central nervous system (CNS)
malignancies, proton beam therapy appears superior to photon
approaches but more data is needed. The report found that, in
large ocular melanomas and chordomas, there is evidence for a
benefit of proton beam therapy over photon approaches. The
ASTRO report stated that more robust prospective clinical trials
are needed to determine the appropriate clinical setting for
proton beam therapy.
A systematic evidence review (Lodge et al, 2007) compared the
efficacy and cost‐effectiveness of PBRT and other types of hadron
therapy (neutron and heavy and light ion therapy) with photon
therapy. The authors concluded that, overall, the introduction or
extension of PBRT and other types of hadron therapy as a major
treatment modality into standard clinical care is not supported by
the current evidence base. The authors stated, however, that the
efficacy of PBRT appears superior to that of photon therapy for
some ocular and skull base tumours. The authors found that, for
prostate cancer, the efficacy of PBRT seems comparable to
photon therapy. The authors stated that no definitive conclusions
can be drawn for the other cancer types. The authors also noted
that they found little evidence on the relative cost‐effectiveness
of PBRT and other types of hadron therapy compared to photon
therapy or with other cancer treatments. Other systematic

7 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
evidence reviews of PBRT have reached similar conclusions
(Lance, 2010; Brada et al, 2009; Efstathiou et al, 2009; ICER, 2008;
Wilt et al, 2008; Brada et al, 2007; Olsen et al, 2007).
The only randomized controlled clinical trial comparing PBRT to
conventional radiotherapy published to date found no advantage
of PBRT in overall survival (OS), disease‐specific survival, or total
recurrence‐free survival (Shipley, 1995). A total of 202 patients
with stage T3‐T4 prostate cancer were randomly assigned to a
standard dose of conventional radiotherapy plus a 25.2 Gy
equivalent PBRT boost or to a standard dose of conventional
radiotherapy with a 16.8 Gy boost of conventional radiotherapy.
After a median follow‐up of 61 months, there were no significant
differences between the 2 groups in OS, disease‐specific survival,
total recurrence‐free survival, or local control. Local control was
better with the proton beam boost only among the subgroup of
patients with poorly differentiated carcinoma. Patients receiving
the proton beam boost had increased rates of late radiation
sequelae.
Loma Linda University’s experience with PBRT of prostate cancer
was reported in an article published in 1999 by Rossi et al. These
investigators reported the results of an uncontrolled study of
PBRT treatment of 319 patients with biopsy‐proven early‐stage
prostate cancer, with no patient having an initial PSA of greater
than 15. Because the study was uncontrolled, one is unable to
determine whether the results of PBRT are superior to
conventional forms of radiation therapy. In addition, the
definitions of success and failure used in this study are not
comparable to those used in other recent studies of prostate
cancer treatments. In the study by Rossi et al, patients were
considered to have an adequate response if their PSA level fell
below 1.0; most other recent studies define an adequate
response as PSA level below 0.5. In the study by Rossi et al,
patients were considered treatment failures if they had 3
consecutive rises of PSA of 10 % or more, measured at 6‐month
intervals. In other words, for a patient to be considered a
treatment failure, it would take at least 18 months, and patients
would have to have 3 consecutive rises in PSA, each greater than
10 %. By contrast, other reported studies of prostate cancer
8 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
radiotherapy have defined failure as any PSA elevation over a
target PSA nadir. Finally, Rossi et al defined clinical disease free
survival as having "no symptoms and no evidence of disease upon
physical examination or radionuclide scans". These are very gross
tests to determine success, and one would expect these tests to
be negative in a high number of patients who harbored occult
disease.
Of the 319 patients included in the study by Rossi et al, only 288
patients (91 %) who had achieved a nadir (any nadir) or who had
been followed for at least 24 months were included in the
analysis. This would indicate that 31 (9 %) of the patients
originally included in the study either had persistently rising PSA
levels without a nadir despite treatment, had dropped out of the
study, or had not been followed for a sufficient length of time for
some unspecified reason. Only 187 patients (59 % of the original
319 patients) achieved a PSA nadir of 0.5 or less, 66 (21 %)
achieved a PSA nadir of 0.51 to 1.0, and 35 (11 %) achieved a PSA
nadir of 1.0 and above. Thus, only 59 % of patients would be
considered to have had an adequate response by the measure
most commonly used in other recent prostate cancer treatment
studies. In addition, because of the peculiar way the results are
reported, there is no way of knowing how many patients' PSA
nadirs were maintained.
In a randomized, prospective, sham‐controlled, double‐masked
study (n = 37), Ciulla et al (2002) examined the effect of PBRT on
subfoveal choroidal neovascular membranes associated with age‐
related macular degeneration. These investigators concluded
that with the acceptance of photodynamic therapy, future studies
will require more complex design and larger sample size to
determine whether radiation can play either a primary or
adjunctive role in treating these lesions.
In a phase II clinical study (n = 30), Kawashima and colleagues
(2005) assessed the safety and effectiveness PBRT for patients
with hepatocellular carcinoma (HCC). Eligibility criteria for this
study were: solitary HCC; no indication for surgery or local
ablation therapy; no ascites; age of 20 years or older; Zubrod
performance status of 0 to 2; no serious co‐morbidities other

9 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
than liver cirrhosis; written informed consent. Proton beam
radiotherapy was administered in doses of 76 cobalt gray
equivalent in 20 fractions for 5 weeks. No patients received
transarterial chemoembolization or local ablation in combination
with PBRT. All patients had liver cirrhosis, the degree of which
was Child‐Pugh class A in 20, and class B in 10 patients. Acute
reactions of PBRT were well‐tolerated, and PBRT was completed
as planned in all patients. Four patients died of hepatic
insufficiency without tumor recurrence at 6 to 9 months; 3 of
these 4 patients had pre‐treatment indocyanine green retention
rate at 15 minutes of more than 50 %. After a median follow‐up
period of 31 months (range of 16 to 54 months), only 1 patient
experienced recurrence of the primary tumor, and 2‐year
actuarial local progression‐free rate was 96 %. Actuarial overall
survival rate at 2 years was 66 %. These investigators concluded
that PBRT showed excellent control of the primary tumor, with
minimal acute toxicity. They stated that further study is
warranted to scrutinize adequate patient selection in order to
maximize survival benefit of this promising modality.
In a phase II prospective trial, Bush et al (2011) evaluated the
safety and effectiveness of PBRT for HCC. Patients with cirrhosis
who had radiological features or biopsy‐proven HCC were
included in the study. Patients without cirrhosis and patients
with extra‐hepatic metastasis were excluded. The mean age was
62.7 years. The mean tumor size was 5.5 cm. Eleven patients
had multiple tumors, and 46 % were within the Milan criteria.
Patients received 63 Gy delivered over a 3‐week period with
PBRT. A total of 76 patients were treated and followed
prospectively. Acute toxicity was minimal; all patients completed
the full course of treatment. Radiation‐induced liver disease was
evaluated using liver enzyme, bilirubin, and albumin levels; no
significant change supervened 6 months post‐treatment. Median
progression‐free survival for the entire group was 36 months,
with a 60 % 3‐year progression‐free survival rate for patients
within the Milan criteria. Eighteen patients subsequently
underwent liver transplantation; 6 (33 %) explants showed
pathological complete response and 7 (39 %) showed only
microscopic residual. The authors concluded that PBRT was
found to be a safe and effective local‐regional therapy for
10 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
inoperable HCC. They noted that a randomized controlled trial to
compare its efficacy to a standard therapy has been initiated.
Olfactory neuroblastoma (ONB) is a rare disease, and a standard
treatment strategy has not been established. Radiation therapy
for ONB is challenging because of the proximity of ONB to critical
organs. Nishimura et al (2007) analyzed the feasibility and
effectiveness of PBRT for ONB. A retrospective review was
performed on 14 patients who underwent PBRT for ONB as
definitive treatment. The total dose of PBRT was 65 cobalt Gray
equivalents (Gy(E)), with 2.5‐Gy(E) once‐daily fractionations. The
median follow‐up period for surviving patients was 40 months.
One patient died from disseminated disease. There were 2
persistent diseases, 1 of which was successfully salvaged with
surgery. The 5‐year overall survival rate was 93 %, the 5‐year local
progression‐free survival rate was 84 %, and the 5‐year relapse‐
free survival rate was 71 %. Liquorrhea was observed in 1 patient
with Kadish's stage C disease (widely destroying the skull base).
Most patients experienced grade 1 to 2 dermatitis in the acute
phase. No other adverse events of grade 3 or greater were
observed according to the RTOG/EORTC acute and late morbidity
scoring system. The authors concluded that these preliminary
findings of PBRT for ONB achieved excellent local control and
survival outcomes without serious adverse effects. They stated
that PBRT is considered a safe and effective modality that
warrants further study.
Proton beam radiotherapy represents a special case for children
for several reasons (Wilson et al, 2005; Hall, 2006;
Merchant, 2009). It has been shown in dosimetric planning
studies to have a potential advantage over conventional photon
therapy because of the ability to confine the high‐dose treatment
area to the tumor volume and minimize the radiation dose to the
surrounding tissue. This especially important in children, as
children are more sensitive to radiation‐induced cancer than
adults. An increased risk of second cancers in long‐term survivors
is more important in children than older adults. In addition to
second malignant neoplasms, late effects of radiation to normal
tissue can include developmental delay. Also, radiation scattered
from the treatment volume is more important in the small body

11 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
of the child. Finally, the question of genetic susceptibility arises
because many childhood cancers involve a germline mutation.
An assessment of proton beam radiotherapy by the Veterans
Health Administration Technology Assessment Program (VATAP)
(Flynn, 2010) found that available English‐language reviews for
proton therapy generally concur on the state of the literature as
consisting primarily of observational studies from which
conclusions about the relative effectiveness of proton therapy
versus alternatives cannot validly be made. The assessment
reported that available reviews reflect the state of the literature
in that they attempt to cover so much territory (multiple poor‐
prognosis inoperable tumors in both children and adults) that
the reviews themselves are cumbersome to read, not well
organized, and provide only diffuse or equivocal conclusions by
individual diagnoses. "In other words, the literature reflects the
early clinical investigation status of proton therapy, where
observational studies are framed in terms of potential benefits,
reasoning from pathophysiology, dose‐finding, refinement of
treatment protocols, and baseline safety of the entire approach"
(Flynn, 2010). The assessment noted that only prostate cancer is
represented by randomized controlled clinical trials, and in that
case two small ones primarily concerned with refinement of
protocol/dose escalation.
Regarding cost‐effectiveness analyses of PBRT, the VATAP
assessment found that the availability of studies titled by their
authors as “economic evaluations” is misleading (Flynn, 2010).
The assessment stated that such studies require cost and efficacy
data about both the intervention and its alternatives (costs and
consequences of alternative interventions), hence should be
conducted only after efficacy data from randomized controlled
trials are available. The assessment noted that, in the case of
proton therapy, the economic studies are premature, really
should be labeled simple cost rather than cost‐effectiveness
analyses, and their conclusions based on unwarranted efficacy
assumptions. Cost data have been carefully collected and
reported, but these are only one element of decision making
about investment in proton therapy. The VATAP assessment
concluded that there are no indications for which proton therapy

12 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
has been shown unequivocally to be effective, or more effective
than its alternatives. The VATAP assessment also concluded that
no research published subsequent to the searches conducted for
available systematic reviews has changed the conclusions of
those reviews.
Regarding research implications, the VATAP assessment
concluded that, in order to obtain the next generation of data,
explicit decisions need to be made about which malignancies are
amenable to/should require randomized trials (e.g., prostate
cancer is sufficiently common) and which malignancies are
sufficiently rare or difficult to treat with surgery or conventional
radiotherapy (e.g., ocular tumors, tumors of the optical nerve,
spinal cord, or central nervous system) that observational studies
with larger cohorts than studies to date are the best approach
(Flynn, 2010). The VATAP assessment also concluded that future
studies should strongly consider valid and reliable embedded
collection of cost data in order to inform better quality economic
evaluation than currently available.
An assessment prepared for the Agency for Healthcare Research
and Quality (Trikalinos, et al., 2009) found that a large number of
scientific papers on charged particle radiotherapy for the
treatment of cancer currently exist. However, these studies do
not document the circumstances in contemporary treatment
strategies in which radiotherapy with charged particles is superior
to other modalities. Comparative studies in general, and
randomized trials in particular (when feasible), are needed to
document the theoretical advantages of charged particle
radiotherapy to specific clinical situations. The assessment noted
that most eligible studies were noncomparative in nature and had
small sample sizes. The report stated that it is likely that focused
systematic reviews will not be able to provide a definitive answer
on the effectiveness and safety of charged particle beam
radiotherapies compared with alternative interventions. This is
simply because of the relative lack of comparative studies in
general, and randomized trials in particular. The report stated that
comparative studies (preferably randomized) are likely necessary
to provide meaningful answers on the relative safety and
effectiveness of particle beam therapy versus other treatment

13 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
options in the context of current clinical practice. This is especially
true for the treatment of common cancers. The report stated that,
especially for many common cancers, such as breast,
prostate, lung, and pancreatic cancers, it is essential that the
theorized advantages of particle beam therapy versus
contemporary alternative interventions are proven in controlled
clinical trials, along with concomitant economic evaluations.
An assessment of the comparative effectiveness and value of
management options in low‐risk prostate cancer by the Institute
for Clinical and Economic Review (ICER) (Ollendorf et al, 2008)
found that the evidence on the comparative effectiveness and
harms of proton beam therapy is limited to relatively small, highly
selective case series of short duration, making any judgments
about its relative benefit or inferiority to other
options premature. The uncertainty regarding PBRT is
accentuated because this technology involves delivery of a novel
form of radiation, and there remain important questions about
the full spectrum of possible effects. ICER rated PBRT's
comparative clinical effectiveness as "insufficient", indicating that
there is not enough evidence to allow a reasonable judgment of
the likely balance of harms and benefits of PBRT in comparison
to radical prostatectomy or other management options. ICER
judged the comparative value of PBRT to be low compared to
other options. The ICER reported explained, that, while ICER does
not always provide a comparative value rating for
technologies with insufficient evidence on comparative clinical
effectiveness, the decision was made to rate the comparative
value of PBRT as “low” relative to radical prostatectomy, based on
current levels of reimbursement that are more than 3‐fold higher
for PBRT.
The Blue Cross and Blue Shield Association Medical Advisory
Panel (BCBSA, 2010) concluded that proton beam radiation
therapy for treatment of non‐small‐cell lung cancer at any stage
or for recurrent non‐small‐cell lung cancer does not meet the
Technology Evaluation Center criteria. The TEC assessment stated
that, overall, evidence is insufficient to permit conclusions about
the results of proton beam therapy for any stage of non‐small‐cell
lung cancer. The report found that all proton beam
14 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
therapy studies are case series; there are no studies directly
comparing proton beam therapy and stereotactic body
radiotherapy. Among study quality concerns, no study mentioned
using an independent assessor of patient reported adverse
events, adverse events were generally poorly reported, and
details were lacking on several aspects of proton beam
therapy treatment regimens. The proton beam therapy studies
had similar patient ages, but there was great variability in percent
within stage Ia, sex ratio, and percent medically inoperable. There
is a high degree of treatment heterogeneity among the proton
beam therapy studies, particularly with respect to planning
volume, total dose, number of fractions, and number of beams.
Survival results are highly variable. It is unclear if the
heterogeneity of results can be explained by differences in
patient and treatment characteristics. Indirect comparisons
between proton beam therapy and stereotactic body
radiotherapy, comparing separate sets of single‐arm studies
on proton beam therapy and stereotactic body radiotherapy, may
be distorted by confounding. In the absence of randomized,
controlled trials, the comparative effectiveness of proton beam
therapy and stereotactic body radiotherapy is uncertain.
Mizumoto et al (2010) evaluated the efficacy and safety of PBRT
for locoregionally advanced esophageal cancer. The subjects
were 51 patients with esophageal cancer who were treated
between 1985 and 2005 using proton beams with or without X‐
rays. All but 1 had squamous cell carcinoma. Of the 51 patients,
33 received combinations of X‐rays (median of 46 Gy) and protons
(median of 36 GyE) as a boost. The median total dose of
combined X‐rays and proton radiation for these 33 patients was
80 GyE (range of 70 to 90 GyE). The other 18 patients received
PBRT alone (median of 79 GyE, range of 62 to 98 GyE). Treatment
interruption due to radiation‐induced esophagitis or hematologic
toxicity was not required for any patient. The overall 5‐year
actuarial survival rate for the 51 patients was 21.1 % and the
median survival time was 20.5 months (95 % confidence interval
[CI]: 10.9 to 30.2). Of the 51 patients, 40 (78 %) showed a
complete response within 4 months after completing treatment
and 7 (14 %) showed a partial response, giving a response rate of
92 % (47/51). The 5‐year local
15 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
control rate for all 51 patients was 38.0 % and the median local
control time was 25.5 months (95 % CI: 14.6 to 36.3). The
authors concluded that these findings suggested that PBRT is an
effective treatment for patients with locally advanced esophageal
cancer. Moreover, they stated that further studies are needed to
determine the optimal total dose, fractionation schedules, and
best combination of PBRT with chemotherapy. Furthermore,
the National Comprehensive Cancer Network (NCCN) guideline
on esophageal cancer (2011) does not mention the use of PBRT
as a therapeutic option for this condition.
Bassim et al (2010) reviewed the literature on radiation therapy
for the treatment of vestibular schwannoma (VS). PubMed
searches for English language articles on radiation treatment of
VS published from January 2002 to July 2007 were conducted.
Studies presenting outcomes were selected, yielding 56 articles
(58 studies) in journals of neurosurgery (30), oncology (18),
otolaryngology (6), and other (2). Data included type of study,
number of subjects, demographics, follow‐up times, type of
radiation, tumor size, tumor control definition, control rates,
facial nerve function measure and outcome, type of hearing and
vestibular testing and outcomes, and complications. Descriptive
statistics were performed. Studies (72.9 %) were retrospective
reviews with stated sample sizes ranging from 5 to 829.
Gamma‐knife (49.2 %), linear accelerator (35.6 %), and proton
beam (6.8 %) were used with various doses. Average follow‐up
was less than 5 years in 79.6 % of studies, and 67.4 % included
patients at less than or equal to 1 year. Tumor size was reported
as diameter (23.7 %), volume (49.2 %), both (11.9 %), other (3.4
%), or not reported (11.9 %). Definition of tumor control varied:
less than or equal to 2 mm growth (22.0 %), no
visible/measurable change (16.9 %), required surgery (10.2 %),
other (17.0 %), and not clearly specified (33.9 %). Facial nerve
outcome was reported as House‐Brackmann (64.4 %),
normal/abnormal (11.9 %), other (1.7 %), or was not reported (22
%). The authors concluded that the lack of uniform reporting
criteria for tumor control, facial function and hearing
preservation, and variability in follow‐up times make it difficult to
compare studies of radiation treatment for VS. They
recommended consideration of reporting guidelines such as
16 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
those used in otology for reporting VS resection results.
Mizumoto et al (2011) evaluated the safety and effectiveness of
hyper‐fractionated concomitant boost proton beam therapy (PBT)
for patients with esophageal cancer. The study participants were
19 patients with esophageal cancer who were treated with
hyperfractionated photon therapy and PBT between 1990 and
2007. The median total dose was 78 GyE (range of 70 to 83 GyE)
over a median treatment period of 48 days (range of 38 to 53
days). Ten of the 19 patients were at clinical T Stage 3 or 4. There
were no cases in which treatment interruption was required
because of radiation‐induced esophagitis or hematologic toxicity.
The overall 1‐ and 5‐year actuarial survival rates for all 19 patients
were 79.0 % and 42.8 %, respectively, and the median survival
time was 31.5 months (95 % limits: 16.7 to 46.3 months). Of the
19 patients, 17 (89 %) showed a complete response within 4
months after completing treatment and 2 (11 %) showed a partial
response, giving a response rate of 100 % (19/19). The 1‐ and 5‐
year local control rates for all 19 patients were 93.8 % and 84.4
%, respectively. Only 1 patient had late esophageal toxicity of
Grade 3 at 6 months after hyperfractionated PBT. There were no
other non‐hematologic toxicities, including no cases of radiation
pneumonia or cardiac failure of Grade 3 or higher. The authors
concluded that these findings suggested that hyperfractionated
PBT is safe and effective for patients with esophageal cancer.
They stated that further studies are needed to establish the
appropriate role and treatment schedule for use of PBT for
esophageal cancer.
In a phase I clinical study, Hong et al (2011) evaluated the safety
of 1 week of chemo‐radiation with proton beam therapy and
capecitabine followed by early surgery on 15 patients with
localized resectable, pancreatic ductal adenocarcinoma of the
head. Patients received radiation with proton beam. In dose
level 1, patients received 3 GyE × 10 (week 1, Monday to Friday;
week 2, Monday to Friday). Patients in dose levels 2 to 4 received
5 GyE × 5 in progressively shortened schedules: level 2 (week 1,
Monday, Wednesday, and Friday; week 2, Tuesday and Thursday),
level 3 (week 1, Monday, Tuesday, Thursday, and Friday; week 2,
Monday), level 4 (week 1, Monday through Friday). Capecitabine
17 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
was given as 825 mg/m(2) b.i.d. Weeks 1 and 2 Monday through
Friday for a total of 10 days in all dose levels. Surgery was
performed 4 to 6 weeks after completion of chemotherapy for
dose levels 1 to 3 and then after 1 to 3 weeks for dose Level 4.
Three patients were treated at dose levels 1 to 3 and 6 patients at
dose level 4, which was selected as the MTD. No dose limiting
toxicities were observed. Grade 3 toxicity was noted in 4 patients
(pain in 1; stent obstruction or infection in 3). Eleven patients
underwent resection. Reasons for no resection were metastatic
disease (3 patients) and unresectable tumor (1 patient). Mean
post‐surgical length of stay was 6 days (range of 5 to 10 days). No
unexpected 30‐day post‐operative complications, including leak
or obstruction, were found. The authors concluded that pre‐
operative chemo‐radiation with 1 week of PBRT and capecitabine
followed by early surgery is feasible. A phase II study is
underway.
UpToDate reviews on "Management of locally advanced and
borderline resectable exocrine pancreatic cancer" (Ryan and
Mamon, 2012) and "Surgery in the treatment of exocrine
pancreatic cancer and prognosis" (Fernandez‐del Castillo et al,
2012) do not mention the use of proton beam therapy.
Furthermore, the NCCN's clinical practice guideline on "Pancreatic
adenocarcinoma" (2011) does not mention the use of proton
beam.
Available peer‐reviewed published evidence does not support the
use of PBRT for squamous cell carcinomas of the head and neck.
There is a lack of clinical outcome studies comparing PBRT to
stereotactic radiosurgery or other photon‐based methods. What
few comparative studies exist are limited to dosimetric planning
studies and not studies of clinical outcomes. Current guidelines
from the NCCN and the National Cancer Institute (PDQ) include
no recommendation for use of PBRT for squamous cell carcinoma
of the head and neck. A report from the American Society for
Therapeutic and Radiation Oncology (ASTRO) (2012) concludes
that there is insufficient evidence to support the use of proton
beam therapy for head and neck cancers, and conclude that
“current data do not provide sufficient evidence to recommend
PBT in ... head and neck cancer… “. An AHRQ comparative
18 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
effectiveness review (2010) on radiotherapy for head and neck
cancer reached the following conclusions regarding proton beam
therapy versus other radiotherapy treatments for head and neck
cancer: “The strength of evidence is insufficient as there were no
studies comparing proton beam therapy to any other
radiotherapy modality. Therefore, no conclusions can be reached
regarding the comparative effectiveness of proton beam therapy
for any of the four key questions.”
An UpToDate review on "Clinical presentation and management
of thymoma and thymic carcinoma" (Salgia, 2012) does not
mention the use of proton beam therapy. Also, the NCCN's
clinical practice guideline on "Thymoma and thymic carcinomas"
(2011) does not mention the use of proton beam therapy.
Guidelines on soft tissue sarcoma from the National
Comprehensive Cancer Network (2012) indicate a potential role
for proton therapy in retroperitoneal soft tissue sarcomas in
persons who did not receive preoperative radiotherapy. The
guidelines state: "Postoperative RT using newer techniques such
as intensity‐modulated radiation therapy (IMRT), 3D conformal
proton therapy, and intensity modulated proton therapy (IMPT)
may allow tumor target coverage and acceptable clinical
outcomes within normal tissue dose constraints to adjacent
organs at risk in some patients with retroperitoneal STS who did
not receive pre‐operative radiotherapy. Multicenter randomized
controlled trials are needed to address the toxicities and
therapeutic benefits of adjuvant RT techniques in patients with
retroperitoneal STS."
A BCBS TEC assessment found insufficient evidence for PBRT in
the treatment of non‐small‐cell lung cancer. In addition, the
American Society for Radiation Oncology (ASTRO) guidelines
(Allen et al, 2012) found insufficient evidence for PBRT in lung
cancer.
An UpToDate review on "Malignant salivary gland tumors:
Treatment of recurrent and metastatic disease" (Laurie, 2012)
stated that "The most common malignant salivary gland tumors
include mucoepidermoid carcinoma, adenoid cystic carcinoma,
19 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
polymorphous low grade adenocarcinoma, carcinoma ex
pleomorphic adenoma, acinic cell carcinoma, and
adenocarcinoma not otherwise specified". However, it does not
mention the use of PBRT as a therapeutic option.
UpToDate reviews on “Treatment of early (stage I and II) head and
neck cancer: The larynx” (Koch and Machtay, 2012) and
“Treatment of locoregionally advanced (stage III and IV) head and
neck cancer: The larynx and hypopharynx” (Brockstein et al,
2012) do not mention the use of NBT.
Given concerns of excess malignancies following adjuvant
radiation for seminoma, Efstathiou et al (2012) evaluated photon
beam therapy and PBRT treatment plans to assess dose
distributions to organs at risk and model rates of second cancers.
A total of 10 stage I seminoma patients who were treated with
conventional para‐aortic AP‐PA photon radiation to 25.5 Gy at
Massachusetts General Hospital had PBRT plans generated (AP‐
PA, PA alone). Dose differences to critical organs were
examined. Risks of second primary malignancies were
calculated. Proton beam radiotherapy plans were superior to
photons in limiting dose to organs at risk; PBRT decreased dose
by 46 % (8.2 Gy) and 64 % (10.2 Gy) to the stomach and large
bowel, respectively (p < 0.01). Notably, PBRT was found to avert
300 excess second cancers among 10,000 men treated at a
median age of 39 and surviving to 75 (p < 0.01). The authors
concluded that in this study, the use of protons provided a
favorable dose distribution with an ability to limit unnecessary
exposure to critical normal structures in the treatment of early‐
stage seminoma. It is expected that this will translate into
decreased acute toxicity and reduced risk of second cancers, for
which prospective studies are warranted. Furthermore,
UpToDate reviews on “Treatment of stage I seminoma” (Beard,
2012) and “Treatment of stage II seminoma” (Beard and Oh,
2012) do not mention the use of PBRT.
Proton beam radiotherapy has been used as therapeutic option
for choroidal hemangiomas. However, available evidence on its
effectiveness for this indication is mainly in the form of
retrospective reviews with small sample size and a lack of

20 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
comparison to standard therapies. Furthermore, a review on
“Choroidal hemangioma” (Finger, 2013) from the Eye Cancer
Network’s website does not mention PBRT as a therapeutic
option. Thus, PBRT is not an established treatment for patients
with choroidal hemangiomas.
In a retrospective study, Hocht et al (2006) compared the results
of therapy in patients with uveal hemangioma treated with
photon or proton irradiation at a single center. From 1993 to
2002, a total of 44 patients were treated. Until 1998 radiotherapy
was given with 6 MV photons in standard fractionation of 2.0 Gy
5 times per week. In 1998 PBRT became available and was used
since then. A dose of 20 to 22.5 Cobalt Gray Equivalent (CGE; CGE
= proton Gy x relative biological effectiveness 1.1) 68 MeV
protons was given on 4 consecutive days. Progressive symptoms
or deterioration of vision were the indications for therapy. Of the
44 patients treated, 36 had circumscribed choroidal
hemangiomas (CCH) and 8 had diffuse choroidal hemangiomas
(DCH) and Sturge‐Weber syndrome. Of the patients, 19 were
treated with photons with a total dose in the range of 16 to 30
Gy. A total of 25 patients were treated with PBRT. All patients
with DCH but 1 were treated with photons. Stabilization of visual
acuity was achieved in 93.2 % of all patients. Tumor thickness
decreased in 95.4 % and retinal detachment resolved in 92.9 %.
Late effects, although generally mild or moderate, were
frequently detected. In all, 40.9 % showed radiation‐induced
optic neuropathy, maximum Grade I. Retinopathy was found in
29.5 % of cases, but only 1 patient experienced more than Grade
II severity. Retinopathy and radiation‐induced optic neuropathy
were reversible in some of the patients and in some resolved
completely. No differences could be detected between patients
with CCH treated with protons and photons; treatment was less
effective in DCH patients (75 %). The authors concluded that
radiotherapy is effective in treating choroidal hemangiomas with
respect to visual acuity and tumor thickness; but a benefit of
PBRT could not be detected.
In a retrospective review, Levy‐Gabriel et al (2009) evaluated the
long‐term effectiveness and outcome of low‐dose PBRT in the
treatment of symptomatic CCH. A total of 71 patients with
21 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
symptomatic CCH were treated by PBRT between September
1994 and October 2002 using a total dose of 20 CGE. The median
follow‐up was 52 months (range of 8 to 133 months). Retinal re‐
attachment was obtained in all cases. Tumor thickness
decreased in all cases and a completely flat scar was obtained in
65 patients (91.5 %). Visual acuity was improved by 2 lines or
more in 37 of the 71 patients (52 %), and in 30 of the 40 patients
(75 %) treated within 6 months after onset of the first symptoms.
The main radiation complications detected during follow‐up were
cataract (28 %) and radiation‐induced maculopathy (8 %). None
of the 71 patients developed eyelid sequelae or neovascular
glaucoma. The authors concluded that PBRT with a total dose of
20 CGE appeared to be a valid treatment for CCH, inducing
definitive retinal re‐attachment and decreasing tumor thickness.
However, delayed radiation‐induced maculopathy may occur. A
successful functional outcome is dependent on a short interval
between onset of the first symptoms and initiation of therapy.
In a retrospective chart review, Chan et al (2010) described the
clinical outcomes of patients (n = 19) with CCH and DCH treated
by PBRT using a non‐surgical light‐field technique. Choroidal
hemangiomas were treated with PBRT using a light‐field
technique and doses ranging from 15 to 30 CGE in 4 fractions.
Patients with at least 6 months' follow‐up were included in the
study. Tumor regression, visual acuity, absorption of sub‐retinal
fluid, and treatment‐associated complications were evaluated by
clinical examination and ultrasonography. Visual acuity improved
or remained stable in 14 of 18 eyes (78 %). Sub‐retinal fluid was
initially present in 16 of 19 eyes (84 %), and completely resolved
in all 16 eyes. Tumor height, as measured by B‐scan
ultrasonography, decreased in 18 of 19 eyes and remained stable
in 1 of 19, as of the last examination. Complications of radiation
developed in 9 of 19 eyes (47 %) with the total applied dose
ranging from 15 to 30 CGE for these 9 eyes. The authors
concluded that PBRT using a light‐field technique without surgical
tumor localization is an effective treatment option in managing
both CCH and DCH associated with Sturge‐Weber syndrome. A
total proton dose as low as 15 CGE applied in 4 fractions
appeared to be sufficient to reduce tumor size, promote
absorption of sub‐retinal fluid, and improve or stabilize vision in
22 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
most patients.
Published studies of proton beam therapy for Hodgkin lymphoma
are limited to dosimetric planning studies; there is a lack of
published clinical outcome studies of proton beam therapy
demonstrating improvements over photon therapy modalities.
Guidelines on Hodgkin Lymphoma from the National
Comprehensive Cancer Network state, in under the section
Principles of Radiation Therapy, “RT can be delivered with
photons or protons. Preliminary results from single‐institution
studies have shown that significant dose reduction to organs at
risk (OAR; e.g., lung, heart, breasts) can be achieved with proton
beam RT, which can reduce the risk of late effects. Long‐term
follow‐up is needed to confirm the efficacy of proton beam RT.”
Guidelines on radiation therapy for Hodgkin lymphoma from the
International Lymphoma Radiation Oncology Group (2014) state:
“The role of proton therapy has not yet been defined, and it is
not widely available.” National Cancer Institute Guidelines (2014)
and American College of Radiology Appropriateness Criteria
(2010) for adult Hodgkin lymphoma have no recommendation for
proton beam therapy in Hodgkin lymphoma. European Society for
Medical Oncology guidelines on Hodgkin disease (Eichenauer, et
al., 2014) have no recommendation for proton beam therapy.
Other international Hodgkin disease guidelines (British
Committee for Standards in Haematology, 2014; BC Cancer
Agency, 2013; Alberta Health Services, 2013) have no
recommendation for proton beam radiation therapy. Guidelines
on proton beam therapy from Alberta Health Services (2013) do
not recommend proton beam therapy for lymphomas in adults
“due to an insufficient evidence base.”
A technology assessment of proton beam therapy for the
Washington State Health Care Authority (2014) found no
comparative studies of proton beam therapy for lymphomas that
met inclusion criteria for the systematic evidence review. The
assessment concluded that the evidence for proton beam therapy
for lymphomas was “insufficient” based on no evidence, and
reported that their review of guidelines and coverage policies on
proton beam found lymphoma was not recommended or not
covered.
23 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Meyer et al (2012) noted that chemotherapy plus radiation
treatment is effective in controlling stage IA or IIA non‐bulky
Hodgkin's lymphoma in 90 % of patients but is associated with
late treatment‐related deaths. Chemotherapy alone may improve
survival because it is associated with fewer late deaths. These
researchers randomly assigned 405 patients with previously
untreated stage IA or IIA non‐bulky Hodgkin's lymphoma to
treatment with doxorubicin, bleomycin, vinblastine, and
dacarbazine (ABVD) alone or to treatment with subtotal nodal
radiation therapy, with or without ABVD therapy. Patients in the
ABVD‐only group, those with a favorable risk profile as well as
those with an unfavorable risk‐profile, received 4 to 6 cycles of
ABVD. Among patients assigned to subtotal nodal radiation
therapy, those who had a favorable risk‐profile received subtotal
nodal radiation therapy alone and those with an unfavorable risk‐
profile received 2 cycles of ABVD plus subtotal nodal radiation
therapy. The primary end‐point was 12‐year OS. The median
length of follow‐up was 11.3 years. At 12 years, the rate of OS
was 94 % among those receiving ABVD alone, as compared with
87 % among those receiving subtotal nodal radiation therapy
(hazard ratio [HR] for death with ABVD alone, 0.50; 95 % CI: 0.25
to 0.99; p = 0.04); the rates of freedom from disease progression
were 87 % and 92 % in the 2 groups, respectively (HR for disease
progression, 1.91; 95 % CI: 0.99 to 3.69; p = 0.05); and the rates of
event‐free survival were 85 % and 80 %, respectively (HR for
event, 0.88; 95 % CI: 0.54 to 1.43; p = 0.60). Among the patients
randomly assigned to ABVD alone, 6 patients died from Hodgkin's
lymphoma or an early treatment complication and 6 died from
another cause; among those receiving radiation therapy, 4 deaths
were related to Hodgkin's lymphoma or early toxic effects from
the treatment and 20 were related to another cause. The authors
concluded that among patients with Hodgkin's lymphoma, ABVD
therapy alone, as compared with treatment that included subtotal
nodal radiation therapy, was associated with a higher
rate of OS owing to a lower rate of death from other causes. This
study did not address the use of PBT for the treatment of Hodgkin
lymphoma; in fact it argued against the combination use of
chemo‐ and radiation‐therapy.
National Comprehensive Cancer Network’s clinical practice

24 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
guideline on “Head and neck cancers” (Version 2.2013) stated
that “the role of proton therapy is being investigated”.
The Alberta Health Services, Cancer Care’s clinical practice
guideline on “Proton beam radiation therapy” (2013) noted that
“Members of the working group do not currently recommend
that patients with prostate cancer, non‐small cell lung cancer, or
most lymphomas be referred for proton beam radiotherapy, due
to an insufficient evidence base”.
The European Society for Medical Oncology’s guidelines on biliary
cancers (Eckel et al, 2011) made no recommendation regarding
the use of PBT in the treatment of cholangiocarcinoma.
Furthermore, NCCN guidelines on “Hepatobiliary cancers”
(Version 2.2013) made no recommendation for use PBT in
cholangiocarcinoma.
A systematic evidence review of proton beam therapy prepared
for the Washington State Healthcare Authority (2014) reviewed
studies comparing proton beam therapy to photon therapies. The
investigators identified two poor‐quality retrospective
comparative cohort studies of primary PBT for brain, spinal, and
paraspinal tumors. One was an evaluation of proton beam
therapy versus photon therapy in 40 adults who received surgical
and radiation treatment of medulloblastoma at MD Anderson
Cancer Center (citing Brown, et al., 2013). No statistical
differences between radiation modalities were seen in Kaplan‐
Meier assessment of either overall or progression‐free survival at
two years. A numeric difference was seen in the rate of local or
regional failure (5% for PBT vs. 14% for photon), but this was not
assessed statistically. The second study involved 32 patients
treated for intramedullary gliomas at Massachusetts General
Hospital (citing Kahn, et al., 2011) with either proton beam
therapy (n=10) or IMRT (n=22). While explicit comparisons were
made between groups, the proton beam therapy population was
primarily pediatric (mean age 14 years), while the IMRT
population was adult (mean age 44 years). Patients in both
groups were followed for a median of 24 months. While the crude
mortality rate was lower in the proton beam therapy group
(20% vs. 32% for IMRT), in multivariate analyses controlling for
25 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
age, tumor pathology, and treatment modality, proton beam
therapy was associated with significantly increased mortality risk
(Hazard Ratio 40.0, p = 0.02). The rate of brain metastasis was
numerically higher in the proton beam therapy group (10% vs. 5%
for IMRT), but this was not statistically tested. Rates of local or
regional recurrence did not differ between groups.
NCCN guidelines on central nervous system cancers (2014) have
no recommendation for proton beam therapy. International
guidelines on CNS malignancies (ESMO, 2010; Alberta Cancer
Care, 2012; Cancer Council Australia, 2009) have no
recommendation for proton beam therapy. An ASTRO Technology
Review of proton beam therapy (2012) stated that, for CNS
malignancies other than skull base and cervical spine chordomas
and chondrosarcomas, “the potential benefit of proton beam
therapy remains theoretical and deserving of further study.”
Dermatofibrosarcoma protuberans is an uncommon tumor that
arises in the skin. The tumor is firm and often flesh‐colored
although it can be reddish, bluish, or purplish. The tumor is often
found on the chest or shoulders, but it can be found on other
parts of the body. Dermatofibrosarcoma protuberans may cause
no symptoms, and the initial size of the tumor tends to be around
1 to 5 centimeters. This tumor has a low potential to spread to
other tissues (metastasize). Treatment often involves surgery to
remove the tumor, such as by Mohs’ micrographic surgery.
https://rarediseases.info.nih.gov/GARD/Condition
/9569/Dermatofibrosarcoma_protuberans.aspx
(https://rarediseases.info.nih.gov/GARD/Condition
/9569/Dermatofibrosarcoma_protuberans.aspx). Moreover,
NCCN’s clinical practice guideline on “Dermatofibrosarcoma
protuberans” (Version 1.2014) does not mention proton or
neutron beam therapy as a therapeutic option.
Plastaras et al (2014) stated that the dose distributions that can
be achieved with protons are usually superior to those of
conventional photon external‐beam radiation. There are special
cases where proton therapy may offer a substantial potential
benefit compared to photon treatments where toxicity concerns
dominate. Re‐irradiation may theoretically be made safer with
26 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
proton therapy due to lower cumulative lifetime doses to
sensitive tissues, such as the spinal cord. Proton therapy has
been used in a limited number of patients with rectal, pancreatic,
esophageal, and lung cancers. Chordomas and soft tissue
sarcomas require particularly high radiation doses, posing
additional challenges for re‐irradiation. Lymphoma is another
special case where proton therapy may be advantageous. Late
toxicities from even relatively low radiation doses, including
cardiac complications and second cancers, are of concern in
lymphoma patients with high cure rates and long life
expectancies. Proton therapy has begun to be used for
consolidation after chemotherapy in patients with Hodgkin and
non‐Hodgkin lymphoma. Breast cancer is another emerging area
of proton therapy development and use. Proton therapy may
offer advantages compared to other techniques in the setting of
breast boosts, accelerated partial breast irradiation, and post‐
mastectomy radiotherapy. In these settings, proton therapy may
decrease toxicity associated with breast radiotherapy. The
authors concluded that as techniques are refined in proton
therapy, one may be able to improve the therapeutic ratio by
maintaining the benefits of radiotherapy while better minimizing
the risks.
Mendenhall et al (2014) reported 5‐year clinical outcomes of 3
prospective trials of image‐guided proton therapy for prostate
cancer. A total of 211 prostate cancer patients (89 low‐risk, 82
intermediate‐risk, and 40 high‐risk) were treated in institutional
review board‐approved trials of 78 cobalt gray equivalent (CGE) in
39 fractions for low‐risk disease, 78 to 82 CGE for intermediate‐
risk disease, and 78 CGE with concomitant docetaxel therapy
followed by androgen deprivation therapy for high‐risk disease.
Toxicities were graded according to Common Terminology Criteria
for Adverse Events (CTCAE), version 3.0.
Median follow‐up was 5.2 years. Five‐year rates of biochemical
and clinical freedom from disease progression were 99 %, 99 %,
and 76 % in low‐, intermediate‐, and high‐risk patients,
respectively. Actuarial 5‐year rates of late CTCAE, version 3.0 (or
version 4.0) grade 3 gastrointestinal and urologic toxicity were 1.0
% (0.5 %) and 5.4 % (1.0 %), respectively. Median pre‐treatment
scores and International Prostate Symptom Scores at greater than
27 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
4 years post‐treatment were 8 and 7, 6 and 6, and 9 and 8,
respectively, among the low‐, intermediate‐, and high‐risk
patients. There were no significant changes between median
pre‐treatment summary scores and Expanded Prostate Cancer
Index Composite scores at greater than 4 years for bowel, urinary
irritation and/or obstructive, and urinary continence. The
authors concluded that 5‐year clinical outcomes with image‐
guided proton therapy included extremely high efficacy, minimal
physician‐assessed toxicity, and excellent patient‐reported
outcomes. Moreover, they stated that further follow‐up and a
larger patient experience are needed to confirm these favorable
outcomes.
Furthermore, NCCN’s clinical practice guideline on “Prostate
cancer” (Version 1.2015) states that “An ongoing prospective
randomized trial is accruing patients and comparing prostate
proton therapy to prostate IMRT. The NCCN panel believes that
there is no clear evidence supporting a benefit or decrement to
proton therapy over IMRT for either treatment efficacy or long‐
term toxicity”.
Amsbaugh (2012) reported acute toxicities and preliminary
outcomes for pediatric patients with ependymomas of the spine
treated with proton beam therapy at the MD Anderson Cancer
Center. A total of 8 pediatric patients received proton beam
irradiation between October 2006 and September 2010 for spinal
ependymomas. Toxicity data were collected weekly during
radiation therapy and all follow‐up visits. Toxicities were graded
according to the Common Terminology Criteria for Adverse Events
version 3.0. All patients had surgical resection of the tumor
before irradiation (7 subtotal resection and 1 gross total
resection). Six patients had World Health Organization Grade I
ependymomas, and 2 had World Health Organization Grade II
ependymomas. Patients had up to 3 surgical interventions before
radiation therapy (range of 1 to 3; median, 1). Three patients
received proton therapy after recurrence and 5 as part of their
primary management. The entire vertebral body was treated in
all but 2 patients. The mean radiation dose was 51.1 cobalt gray
equivalents (range of 45 to 54 cobalt gray equivalents). With a
mean follow‐up of 26 months from the radiation therapy start
28 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
date (range of 7 to 51 months), local control, event‐free survival,
and overall survival rates were all 100 %. The most common
toxicities during treatment were Grade 1 or 2 erythema (75 %)
and Grade 1 fatigue (38 %). No patients had a Grade 3 or higher
adverse event. Proton therapy dramatically reduced dose to all
normal tissues anterior to the vertebral bodies in comparison to
photon therapy. The authors concluded that preliminary
outcomes showed the expected control rates with favorable
acute toxicity profiles. They noted that proton beam therapy
offers a powerful treatment option in the pediatric population,
where adverse events related to radiation exposure are of
concern. Moreover, they stated that extended follow‐up will be
required to assess for late recurrences and long‐term adverse
effects.
The American College of Radiology’s “Appropriateness Criteria®
retreatment of recurrent head and neck cancer after prior
definitive radiation” (McDonald et al, 2014) stated that “Newer
conformal radiation modalities, including stereotactic body
radiation therapy and proton therapy, may be appropriate in
select cases. Additional data are needed to determine which
patient subsets will most likely benefit from these modalities”.
In a review on “Promise and pitfalls of heavy‐particle therapy”,
Mitin and Zietman (2014) stated that “Particle therapy [including
proton beam], on a relatively thin evidence base, has established
itself as the standard of care for these rare malignancies
[chordoma and chondrosarcoma]”.
An UpToDate review on “Ependymoma” (Kieran, 2014) does not
mention proton beam as a therapeutic option.
Greenberger et al (2014) reported their experience with pediatric
patients treated with PBT. A total of 32 pediatric patients with
low‐grade gliomas of the brain or spinal cord were treated with
PBT from 1995 to 2007; 16 patients received at least 1 regimen of
chemotherapy before definitive radiotherapy (RT). The median
radiation dose was 52.2 GyRBE (48.6 to 54 GyRBE). The median
age at treatment was 11.0 years (range of 2.7 to 21.5 years), with
a median follow‐up time of 7.6 years (range of 3.2 to 18.2 years).
29 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
The 6‐year and 8‐year rates of progression‐free survival were 89.7
% and 82.8 %, respectively, with an 8‐year overall survival of 100
%. For the subset of patients who received serial neurocognitive
testing, there were no significant declines in Full‐Scale Intelligence
Quotient (p = 0.80), with a median neurocognitive
testing interval of 4.5 years (range of 1.2 to 8.1 years) from
baseline to follow‐up, but subgroup analysis indicated some
significant decline in neurocognitive outcomes for young children
(less than 7 years) and those with significant dose to the left
temporal lobe/hippocampus. The incidence of endocrinopathy
correlated with a mean dose of greater than or equal to 40 GyRBE
to the hypothalamus, pituitary, or optic chiasm. Stabilization or
improvement of visual acuity was achieved in 83.3 % of patients
at risk for radiation‐induced injury to the optic pathways. The
authors concluded that this report of late effects in children with
low‐grade gliomas after PBT is encouraging. Proton beam therapy
appears to be associated with good clinical outcome, especially
when the tumor location allows for increased sparing of the left
temporal lobe, hippocampus, and hypothalamic‐pituitary axis.
The authors also stated that larger cohorts are likely needed to
enable accurate assessment of the incidence of moyamoya
disease after PBT.
In a review on “Promise and pitfalls of heavy‐particle therapy”,
Mitin and Zietman (2014) stated that “In others, the benefits are
likely to be small or non‐existent such as with skin cancer; and
proton beam therapy should not be considered”.
Li et al (2011) stated that the papillary tumor of the pineal region
(PTPR) is a distinct entity that is particularly rare in the pediatric
population. The authors documented the youngest reported
patient with this clinicopathological entity to date. These
researchers described the case of PTPR in a 15‐month old boy.
Initially thought to be a tectal glioma, the tumor was later
identified as a pineal region tumor after demonstrating growth on
routine imaging. Diagnosis of PTPR was established by
histopathological evaluation of biopsy samples, which revealed
papillary, cystic, and solid tumor components. The patient's post‐
operative course was complicated by tumor growth despite
several debulking procedures and chemotherapy, as well as
30 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
persistent hydrocephalus requiring 2 endoscopic third
ventriculostomies and eventual ventriculo‐peritoneal shunt
placement. After a 15‐month follow‐up period, the patient has
received proton‐beam therapy (PBT) and has a stable tumor size.
The PTPR is a recently described tumor of the CNS that must be
included in the differential diagnosis of pineal region masses. The
biological behavior, prognosis, and appropriate treatment of PTPR
have yet to be fully defined.
An UpToDate review on “Pineal gland masses” (Moschovi and
Chrousos, 2014) does not mention PBT as a therapeutic option.
Clivio et al (2013) evaluated intensity modulated proton therapy
(IMPT) in patients with cervical cancer in terms of coverage,
conformity, and DVH parameters correlated with
recommendations from magnetic resonance imaging (MRI)‐
guided brachytherapy. A total of 11 patients with histologically
proven cervical cancer underwent primary chemo‐radiation for
the pelvic lymph nodes, the uterus, the cervix, and the
parametric region, with a symmetric margin of 1 cm. The
prescription was for 50.4 Gy, with 1.8 Gy per fraction. The
prescribed dose to the parametria was 2.12 Gy up to 59.36 Gy in
28 fractions as a simultaneous boost. For several reasons, the
patients were unable to undergo brachytherapy. As an
alternative, IMPT was planned with 5 fractions of 6 Gy to the
cervix, including the macroscopic tumor with an MRI‐guided
target definition, with an isotropic margin of 5 mm for PTV
definition. Groupe‐Europeen de Curietherapie and European
society for Radiotherapy and Oncology (GEC‐ESTRO) criteria were
used for DVH evaluation. Reference comparison plans were
optimized for volumetric modulated rapid arc (VMAT) therapy
with the RapidArc (RA). The dose to the high‐risk volume was
calculated with α/β = 10 with 89.6 Gy. For IMPT, the clinical
target volume showed a mean dose of 38.2 ± 5.0 Gy (35.0 ± 1.8
Gy for RA). The D98% was 31.9 ± 2.6 Gy (RA: 30.8 ± 1.0 Gy). With
regard to the organs at risk, the 2Gy Equivalent Dose (EQD2) (α/β
= 3) to 2 cm(3) of the rectal wall, sigmoid wall, and bladder wall
was 62.2 ± 6.4 Gy, 57.8 ± 6.1 Gy, and 80.6 ± 8.7 Gy (for RA: 75.3 ±
6.1 Gy, 66.9 ± 6.9 Gy, and 89.0 ± 7.2 Gy, respectively). For the
IMPT boost plans in combination with external beam radiation
31 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
therapy, all DVH parameters correlated with less than 5 % risk for
grades 2 to 4 late gastro‐intestinal and genitourinary toxicity. The
authors concluded that in patients who are not eligible for
brachytherapy, IMPT as a boost technique additionally to external
beam radiation therapy provides good target coverage and
conformity and superior DVH parameters, compared with
recommendations to MRI‐guided brachytherapy. They stated that
for selected patients, IMPT might be a valid alternative to
brachytherapy and also superior to reference VMAT plans. (These
preliminary findings from a small study [n = 11] need to be
validated by well‐designed studies).
UpToDate reviews on “Approach to adjuvant treatment of
endometrial cancer” (Plaxe and Mundt, 2014) and “Treatment of
recurrent or metastatic endometrial cancer” (Campos and Cohn,
2014) do not mention proton beam therapy as a therapeutic
option.
Moreover, the National Comprehensive Cancer Network’s clinical
practice guideline on “Uterine cancer” (Version 1.2015) does not
list proton beam therapy as a therapeutic option.
An UpToDate review on “Management of anaplastic
oligodendroglial tumors” (van den Bent, 2014) does not mention
proton beam therapy as a therapeutic option.
Romesser et al (2016) stated that re‐irradiation therapy (re‐RT) is
the only potentially curative treatment option for patients with
locally recurrent head and neck cancer (HNC). Given the
significant morbidity with head and neck re‐RT, interest in proton
beam radiation therapy (PBRT) has increased. These investigators
reported the first multi‐institutional clinical experience using
curative‐intent PBRT for re‐RT in recurrent HNC. A retrospective
analysis of ongoing prospective data registries from 2 hybrid
community practice and academic proton centers was
conducted. Patients with recurrent HNC who underwent at least
1 prior course of definitive‐intent external beam radiation therapy
(RT) were included. Acute and late toxicities were assessed with
the National Cancer Institute Common Te rminology Criteria for
Adverse Events version 4.0 and the Radiation Therapy Oncology
32 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Group late radiation morbidity scoring system, respectively. The
cumulative incidence of loco‐regional failure was calculated with
death as a competing risk. The actuarial 12‐month freedom‐
from‐distant metastasis and overall survival (OS) rates were
calculated with the Kaplan‐Meier method. A total of 92
consecutive patients were treated with curative‐intent re‐RT with
PBRT between 2011 and 2014. Median follow‐up among
surviving patients was 13.3 months and among all patients was
10.4 months. The median time between last RT and PBRT was
34.4 months. There were 76 patients with 1 prior RT course and
16 with 2 or more courses. The median PBRT dose was 60.6 Gy
(relative biological effectiveness, [RBE]); 85 % of patients
underwent prior HNC RT for an oropharynx primary, and 39 %
underwent salvage surgery before re‐RT. The cumulative
incidence of loco‐regional failure at 12 months, with death as a
competing risk, was 25.1 %. The actuarial 12‐month freedom‐
from‐distant metastasis and OS rates were 84.0 % and 65.2 %,
respectively. Acute toxicities of grade 3 or greater included
mucositis (9.9 %), dysphagia (9.1 %), esophagitis (9.1 %), and
dermatitis (3.3 %). There was 1 death during PBRT due to disease
progression. Grade 3 or greater late skin and dysphagia toxicities
were noted in 6 patients (8.7 %) and 4 patients (7.1 %),
respectively; 2 patients had grade 5 toxicity due to treatment‐
related bleeding. The authors concluded that proton beam re‐RT
of the head and neck can provide effective tumor control with
acceptable acute and late toxicity profiles likely because of the
decreased dose to the surrounding normal, albeit previously
irradiated, tissue, although longer follow‐up is needed to confirm
these findings.
McDonald et al (2016) reported the clinical outcomes of head and
neck re‐RT with proton therapy. From 2004 to 2014, a total of 61
patients received curative‐intent proton re‐irradiation, primarily
for disease involving skull base structures, at a median of 23
months from the most recent previous course of radiation. Most
had squamous cell (52.5 %) or adenoid cystic (16.4 %) carcinoma.
Salvage surgery before re‐irradiation was undertaken in 47.5 %.
Gross residual disease was present in 70.5 %. For patients with
microscopic residual disease, the median dose of re‐irradiation
was 66 Gy (relative biological effectiveness), and for gross disease
33 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
was 70.2 Gy (relative biological effectiveness). Concurrent
chemotherapy was given in 27.9 %. The median follow‐up time
was 15.2 months and was 28.7 months for patients remaining
alive. The 2‐year OS estimate was 32.7 %, and the median OS
was 16.5 months. The 2‐year cumulative incidence of local failure
with death as a competing risk was 19.7 %; regional nodal failure,
3.3 %; and distant metastases, 38.3 %. On multi‐variable analysis,
Karnofsky performance status less than or equal to 70 %, the
presence of a gastrostomy tube before re‐irradiation, and an
increasing number of previous courses of radiation therapy were
associated with a greater hazard ratio for death. A cutaneous
primary tumor, gross residual disease, increasing gross tumor
volume, and a lower radiation dose were associated with a
greater hazard ratio for local failure. Grade greater than or equal
to 3 toxicities were seen in 14.7 % acutely and 24.6 % in the late
setting, including 3 treatment‐related deaths. The authors
concluded that re‐irradiation with proton therapy, with or
without chemotherapy, provided reasonable loco‐regional
disease control, toxicity profiles, and survival outcomes for an
advanced‐stage and heavily pre‐treated population. Moreover,
they stated that additional data are needed to identify which
patients are most likely to benefit from aggressive efforts to
achieve local disease control and to evaluate the potential benefit
of proton therapy relative to other modalities of re‐irradiation.
Desmoid Fibromatosis:
UpToDate reviews on “Desmoid tumors: Epidemiology, risk
factors, molecular pathogenesis, clinical presentation, diagnosis,
and local therapy” (Ravi et al, 2016) and “Desmoid tumors:
Systemic therapy” (Ravi and Patel, 2016) do not mention PBT as a
therapeutic option.
Hemangioendothelioma:
Hemangioendothelioma refers to a group of vascular neoplasms
that may be considered benign as well as malignant, depending
on the specific group member's activity. The primary treatment
of intra‐cranial hemangioendothelioma is surgical excision.
Although some have advocated adjuvant radiotherapy or

34 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
chemotherapy, there is insufficient evidence on the use of PBT for
hemangioendotheliomas. The “Consensus‐derived practice
standards plan for complicated Kaposiform
hemangioendothelioma” (Drolet et al, 2013) had no
recommendation for PBT.
An UpToDate review on “Tufted angioma, kaposiform
hemangioendothelioma, and the Kasabach‐Merritt phenomenon”
(Adams and Frieden, 2016) does not mention PBT as a therapeutic
option.
Mesothelioma:
Cao and colleagues (2014) noted that IMPT is commonly
delivered via the spot‐scanning technique. To “scan” the target
volume, the proton beam is controlled by varying its energy to
penetrate the patient's body at different depths. Although
scanning the proton beamlets or spots with the same energy can
be as fast as 10 to 20 m s(‐1), changing from one proton energy to
another requires approximately 2 additional seconds. The total
IMPT delivery time thus depends mainly on the number of proton
energies used in a treatment. Current treatment planning
systems typically use all proton energies that are required for the
proton beam to penetrate in a range from the distal edge to the
proximal edge of the target. The optimal selection of proton
energies has not been well‐studied. In this study, these
researchers sought to determine the feasibility of optimizing and
reducing the number of proton energies in IMPT planning. They
proposed an iterative mixed‐integer programming optimization
method to select a subset of all available proton energies while
satisfying dosimetric criteria. They applied their proposed
method to 6 patient datasets: 4 cases of prostate cancer, 1 case of
lung cancer, and 1 case of mesothelioma. The numbers of
energies were reduced by 14.3 % to 18.9% for the prostate cancer
cases, 11.0 % for the lung cancer cases and 26.5 % for the
mesothelioma case. The results indicated that the number of
proton energies used in conventionally designed IMPT plans can
be reduced without degrading dosimetric performance. The
IMPT delivery efficiency could be improved by energy layer
optimization leading to increased throughput for a busy proton
35 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
center in which a delivery system with slow energy switch is
employed. This was a small (n = 6; 1 case of mesothelioma)
feasibility study; it did not provide any data regarding the
effectiveness of PBRT for the treatment of mesothelioma.
In a case‐series study, Pan et al (2015) described their experience
implementing IMPT for lung‐intact malignant pleural
mesothelioma (MPM), including patient selection, treatment
planning, dose verification, and process optimization. A total of 7
patients with epithelioid MPM were reviewed; 6 underwent
pleurectomy, whereas 1 had biopsy alone. Four patients received
IMPT and 3 received intensity modulated radiation therapy.
Treatment plans for the other modality were created for
dosimetric comparisons. Quality assurance processes included
dose verification and robustness analysis. Image‐guided set‐up
was performed with the first isocenter, and couch shifts were
applied to reposition to the second isocenter. Treatment with
IMPT was well‐tolerated and completed without breaks. IMPT
plans were designed with 2 isocenters, 4 beams, and ≤64 energy
layers per beam. Dose verification processes were completed in 3
hours. Total daily treatment time was approximately 45 minutes
(20 minutes for set‐up and 25 minutes for delivery). IMPT
produced lower mean doses to the contralateral lung, heart,
esophagus, liver, and ipsilateral kidney, with increased
contralateral lung sparing when mediastinal boost was required
for nodal disease. The authors concluded that their initial
experience showed that IMPT was feasible for routine care of
patients with lung‐intact MPM. This was a small (n = 4) feasibility
study; it did not provide any data regarding the effectiveness of
PBRT for the treatment of mesothelioma.
Retroperitoneal/Pelvic Sarcoma:
Kelly et al (2015) compared outcomes of patients with
retroperitoneal or pelvic sarcoma treated with peri‐operative (RT
versus those treated without peri‐operative RT. Prospectively
maintained databases were reviewed to retrospectively compare
patients with primary retroperitoneal or pelvic sarcoma treated
during 2003 to 2011. Multivariate Cox regression models were
used to assess associations with the primary end‐points: local
36 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
recurrence‐free survival (LRFS) and disease‐specific survival. At 1
institution, 172 patients were treated with surgery alone,
whereas at another institution 32 patients were treated with
surgery and peri‐operative PBRT or IMRT with or without intra‐
operative RT. The groups were similar in age, tumor size, grade,
and margin status (all p > 0.08). The RT group had a higher
percentage of pelvic tumors (p = 0.03) and a different distribution
of histologies (p = 0.04). Peri‐operative morbidity was higher in
the RT group (44 % versus 16 % of patients; p = 0.004). After a
median follow‐up of 39 months, 5‐year LRFS was 91 % (95 % CI:
79 % to 100 %) in the RT group and 65 % (57 % to 74 %) in the
surgery‐only group (p = 0.02). On multivariate analysis, RT was
associated with better LRFS (HR, 0.26; p = 0.03); 5‐year disease‐
specific survival was 93 % (95 % CI: 82 % to 100 %) in the RT
group and 85 % (78 % to 92 %) in the surgery‐only group (p = 0.3).
The authors concluded that the addition of advanced‐
modality RT to surgery for primary retroperitoneal or pelvic
sarcoma was associated with improved LRFS, although this did
not translate into significantly better disease‐specific survival.
They stated that this treatment strategy warrants further
investigation in a randomized trial.
Salivary Gland Tumors:
An UpToDate review on “Salivary gland tumors: Treatment of
locoregional disease” (Lydiatt and Quivey, 2016) mentions
neutrons and carbon ions, but not protons, for the treatment of
salivary gland tumors.
Choroidal Melanoma:
In a retrospective review, Patel and colleagues (2016) reported
visual outcomes in patients undergoing PBRT of tumors located
within 1 disc diameter of the fovea. Patients with choroidal
melanoma involving the fovea treated with proton beam therapy
between 1975 and 2009 were included in this analysis. A total of
351 patients with choroidal melanomas located 1 disc diameter
(DD) or less from the fovea and more than 1 DD away from the
optic nerve were included in this study. In a subgroup of 203 of
the patients with small and medium choroidal melanomas, the

37 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
effect of a reduced dose of radiation, 50 Gy (relative biological
effectiveness [RBE]) versus 70 Gy (RBE), on visual outcomes was
analyzed. The Kaplan‐Meier method and Cox regression analysis
were performed to calculate cumulative rates of vision loss and to
assess risk factors for vision loss, respectively. Visual acuity (VA)
and radiation complications, which included radiation
maculopathy, papillopathy, retinal detachment, and rubeosis,
were assessed. This study had a mean follow‐up time of 68.7
months. More than 1/3 of patients (35.5 %) retained 20/200 or
better vision 5 years after PBRT. For those patients with a
baseline VA of 20/40 or better, 16.2 % of patients retained this
level of vision 5 years after PBRT. Tu mor height less than 5 mm
and baseline VA 20/40 or better were associated significantly with
a better visual outcome (p < 0.001). More than 2/3 (70.4 %) of
patients receiving 50 Gy (RBE) and nearly half (45.1 %) of patients
receiving 70 Gy (RBE) retained 20/200 or better vision 5 years
after treatment, but this difference was not significant.
Approximately 20 % of patients with these smaller macular
tumors retained 20/40 vision or better 5 years after irradiation.
The authors concluded that the results of this retrospective
analysis demonstrated that despite receiving a full dose of
radiation to the fovea, many patients with choroidal melanoma
with foveal involvement maintain useful vision. A radiation dose
reduction from 70 to 50 Gy (RBE) did not appear to increase the
proportion of patients who retain usable vision. The major
drawbacks of this study were: (i) its retrospective design, and (ii)
despite decreasing the risk of coincidental maculopathy and
papillopathy by choosing tumors more than 1 DD away from the
optic nerve, there is still a definite overlap in the incidence of
maculopathy and papillopathy occurring in these patients. These
researchers were unable to distinguish whether the cause of
vision loss in individual patient was the result of radiation effects
on the macula or the optic nerve. The authors stated that further
elucidation of factors that distinguish the small minority of
patients able to retain excellent vision is needed for future
improvement of visual outcomes.
Desmoid Tu mor (Aggressive Fibromatosis):
UpToDate reviews on “Desmoid tumors: Epidemiology, risk
38 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
factors, molecular pathogenesis, clinical presentation, diagnosis,
and local therapy” (Ravi et al, 2016) and “Desmoid tumors:
Systemic therapy” (Ravi and Patel, 2016) do not mention PBT as a
therapeutic option.
Multiple Myeloma:
UpToDate reviews on “Overview of the management of multiple
myeloma” (Rajkumar, 2016a) and “Treatment of relapsed or
refractory multiple myeloma” (Rajkumar, 2016b) do not mention
proton beam therapy as a therapeutic option.
Furthermore, National Comprehensive Cancer Network’s clinical
practice guideline on “Multiple myeloma” (Version 3.2017) does
not mention proton beam therapy as a therapeutic option.
Thymic Tu mor:
Vogel et al (2016) stated that radiation is an important modality
in treatment of thymic tumors. However, toxicity may reduce its
overall benefit. These researchers hypothesized that double‐
scattering proton beam therapy (DS‐PT) can achieve excellent
local control with limited toxicity in patients with thymic
malignancies. Patients with thymoma or thymic carcinoma
treated with DS‐PT between 2011 and 2015 were prospectively
analyzed for toxicity and patterns of failure on an IRB‐approved
study. A total of 27 consecutive patients were evaluated.
Patients were a median of 56 years and had thymoma (85 %).
They were treated with definitive (22 %), salvage (15 %) or
adjuvant (63 %) DS‐PT to a median of 61.2/1.8 Gy [CGE]. No
patient experienced grade greater than or equal to 3 toxicity.
Acute grade 2 toxicities included dermatitis (37 %), fatigue (11 %),
esophagitis (7 %), and pneumonitis (4 %). Late grade 2 toxicity
was limited to 1 patient with chronic dyspnea. At a median
follow‐up of 2 years, 100 % local control was achieved; 3‐year
regional control, distant control, and overall survival (OS) rates
were 96 % (95 % confidence interval [CI]: 76 to 99 %), 74 % (95 %
CI: 41 to 90 %), and 94 % (95 % CI: 63 to 99 %), respectively. The
authors concluded that this was the first cohort and prospective
series of proton therapy to treat thymic tumors, demonstrating

39 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
low rates of early toxicity and excellent initial outcomes.
Parikh et al (2016) evaluated the dosimetric differences between
proton beam therapy (PBT) and intensity modulated radiation
therapy (IMRT) for resected thymoma. These investigators
simultaneously reported their early clinical experience with PBT
in this cohort. These researchers identified 4 patients with
thymoma or thymic carcinoma treated at their center from 2012
to 2014 who completed adjuvant PBT to a median dose of 57.0
cobalt Gy equivalents (CGE; range of 50.4 to 66.6 CGE) after
definitive resection. Adjuvant radiation was indicated for positive
(n = 3) or close margin (n = 1). Median age was 45 (range of 32 to
70) years. Stages included II (n = 2), III (n = 1), and IVA (n = 1).
Analogous IMRT plans were generated for each patient for
comparison, and pre‐set dosimetric end‐points were evaluated.
Early toxicities were assessed according to retrospective chart
review. Compared with IMRT, PBT was associated with lower
mean doses to the lung (4.6 versus 8.1 Gy; p = 0.02), esophagus
(5.4 versus 20.6 Gy; p = 0.003), and heart (6.0 versus 10.4 Gy; p =
0.007). Percentages of lung, esophagus, and heart receiving
radiation were consistently lower in the PBT plans over a wide
range of radiation doses. There was no difference in mean breast
dose (2.68 versus 3.01 Gy; p = 0.37). Of the 4 patients treated
with PBT, 3 patients experienced grade 1 radiation dermatitis, and
1 patient experienced grade 2 dermatitis, which resolved after
treatment. With a median follow‐up of 5.5 months, there were
no additional grade greater than or equal to 2 acute or sub‐acute
toxicities, including radiation pneumonitis. The authors
concluded that PBT is clinically well‐tolerated after surgical
resection of thymoma, and was associated with a significant
reduction in dose to critical structures without compromising
coverage of the target volume. Moreover, they stated that
prospective evaluation and longer follow‐up is needed to assess
clinical outcomes and late toxicities.
Furthermore, National Comprehensive Cancer Network’s clinical
practice guideline on “Thymomas and thymic carcinomas”
(Version 3.2016) does not mention proton beam radiotherapy as
a therapeutic option.

40 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Yo lk Cell Tu mor:
Park et al (2015) performed dosimetric comparisons between
proton beam therapy and intensity modulated radiotherapy
(IMRT) of intra‐cranial germ cell tumors (ICGCTs) arising in various
locations of the brain. IMRT, passively scattered proton therapy
(PSPT), and spot scanning proton therapy (SSPT) plans were
performed for 4 different target volumes: (i) the whole ventricle
(WV), (ii) pineal gland (PG), (iii) supra‐sellar (SS), and (iv) basal
ganglia (BG); 5 consecutive clinical cases were selected from the
patients treated between 2011 and 2014 for each target volume.
A total 20 cases from the 17 patients were included in the
analyses with 3 overlap cases which were used in plan
comparison both for the whole ventricle and boost targets. The
conformity index, homogeneity index, gradient index, plan quality
index (PQI), and doses applied to the normal substructures of the
brain were calculated for each treatment plan. The PQI was
significantly superior for PSPT and SSPT than IMRT for ICGCTs in
all locations (median; WV: 2.89 and 2.37 versus 4.06, PG: 3.38
and 2.70 versus 4.39, SS: 3.92 and 2.49 versus 4.46, BG: 3.01 and
2.49 versus 4.45). PSPT and SSPT significantly reduced the mean
dose, and the 10 and 15 Gy dose volumes applied to the normal
brain compared with IMRT (p ≤ 0.05). PSPT and SSPT saved
significantly greater volumes of the temporal lobes and
hippocampi (p < 0.05) in the SS and PG targets than IMRT. For
tumors arising in the BG, PSPT and SSPT also saved greater
volumes of the contralateral temporal lobes. The authors
concluded that PSPT and SSPT provided superior target volume
coverage and saved more normal tissue compared with IMRT for
ICGCTs in various locations. Moreover, they stated that future
studies should examine if the extent of normal tissue saved has
clinical benefits in children with ICGCTs.
Furthermore, an UpToDate review on “Diagnosis and treatment
of relapsed and refractory testicular germ cell tumors” (Gilligan
and Kantoff, 2016) does not mention proton beam radiotherapy
as a therapeutic option.
Neutron Beam Therapy:
41 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Most radiation therapies utilize photons ‐‐ lightweight particles
that damage cancerous cells. Neutron beam therapy (NBT) uses
neutrons, which are much heavier than photons and appear to be
more effective in destroying very dense tumors. Compared to
roentgen ray (X‐ray), neutrons are characterized by several
properties: (i) reduced oxygen enhancement factor, (ii) less or no
repair of sub‐lethal or potentially lethal cell damage, and (iii) less
variation of sensitivity through cell cycle.
Neutron beam radiation therapy (NBRT) is a specialized type of
EBRT that uses high energy neutrons (neutral charged subatomic
particles). The neutrons are targeted toward tissue masses that
are characterized by lower tumor oxygen levels and a slower cell
cycle, since neutrons require less oxygen and are less dependent
on the cell’s position in the cell division cycle. Neutrons impact
with approximately 20 to 100 times more energy than
conventional photon radiation and may be more damaging to
surrounding tissues. For that reason, the radiation is delivered
utilizing a sophisticated planning and delivery system.
Neutron beam therapy entails the use of a particle accelerator;
protons from the accelerator are deflected by a magnet to a
target which creates the neutron beam. Neutron bean therapy
has been employed mainly for the treatment of the salivary gland
cancers. It has also been used to treat other malignancies such as
soft tissue sarcoma (STS) as well as lung, pancreatic, colon, kidney
and prostate cancers. Nevertheless, NBT has not gained wide
acceptance because of the clinical difficulty in generating neutron
particles. It should be noted that NBT is different from boron
neutron capture therapy (BNCT), which is a radiotherapy based
on the preferential targeting of tumor cells with non‐radioactive
isotope (10)B and subsequent activation with thermal neutrons
to produce a highly localized radiation, and is often used to treat
brain tumors. In BNCT, the patient is given a drink containing
boron, which is taken up by tumor cells. The tumor is then
irradiated with a neutron beam, causing the boron to split into
two highly energetic particles (helium and lithium) that destroy
the cancerous cells while largely sparing adjacent healthy cells.
Salivary Gland Cancer:

42 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
In the treatment of patients with salivary gland cancer, primary
radiation including NBT may play a role in certain histological
types or non‐operative patients (Day, 2004). Neutron beam
therapy has been most extensively used either for an
incompletely excised primary tumor or for recurrent disease.
In a randomized clinical study, Laramore and associates (1993)
compared the effectiveness of fast neutron radiotherapy versus
conventional photon and/or electron radiotherapy for
unresectable, malignant salivary gland tumors. Eligibility criteria
included either inoperable primary or recurrent major or minor
salivary gland tumors. Patients were stratified by surgical status
(primary versus recurrent), tumor size (less than or greater than 5
cm), and histology (squamous or malignant mixed versus other).
After a total of 32 patients were entered into this study, it
appeared that the group receiving fast neutron radiotherapy had
a significantly improved local/regional control rate and also a
borderline improvement in survival and the study was stopped
earlier than planned for ethical reasons. Twenty‐five patients
were study‐eligible and analyzable. Ten‐year follow‐up data for
this study was presented. On an actuarial basis, there was a
statistically‐significant improvement in local/regional control for
the neutron radiotherapy group (56 % versus 25 %, p = 0.009),
but there was no statistically significant improvement in OS (15 %
versus 25 %). Patterns of failure were analyzed and it was
demonstrated that distant metastases account for the majority of
failures on the neutron radiotherapy arm and local/regional
failures account for the majority of failures on the
photon/electron radiotherapy arm. Long‐term, treatment‐related
morbidity was analyzed and while the incidence of morbidity
graded "severe" was greater on the neutron arm, there was no
significant difference in "life‐threatening" complications. These
investigators concluded that fast neutron radiotherapy appeared
to be the treatment‐of‐choice for patients with inoperable
primary or recurrent malignant salivary gland tumors.
Prott et al (2000) reported their findings of fast neutron therapy
in 72 patients with adenoid cystic carcinoma (ACC) of the salivary
glands. The median age was 54 years; and the median follow‐up
was 50 months. This study showed that 39.1 % of the patients

43 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
achieved a complete remission and 48.6 % achieved partial
remission. The survival probability was 86 % after 1 year, 73 %
after 2 years and 53 % after 5 years. The recurrence‐free survival
was 83 % after 1 year, 71 % after 2 years and 45 % after 5 years.
These investigators concluded that NBT appeared to have been
an effective treatment in these selected patients.
Huber and colleagues (2001) compared retrospectively
radiotherapy with neutrons, photons, and a photon/neutron
mixed beam in patients (n = 75) with advanced ACC of the head
and neck. Local control, survival, distant failure, and
complications were analyzed. Follow‐up ranged from 1 to 160
months (median 51 months), and the surviving patients had a
minimum follow‐up of 3 years at the time of analysis. The
actuarial 5‐year local control was 75 % for neutrons, and 32 % for
both mixed beam and photons (p = 0.015, log‐rank). This
advantage for neutrons in local control was not transferred to
significant differences in survival (p > 0.1). In multi‐variate
analysis post‐operative radiotherapy (p = 0.003) and small tumor
size (p = 0.01) were associated with high local control, while
primary therapy (p = 0.006) and negative lymph nodes (p = 0.01)
were associated with longer survival. While acute toxicity was
similar in all 3 radiotherapy groups, severe late grade 3 and 4
toxicity tended to be more prevalent (p > 0.1) with neutrons (19
%) than with mixed beam (10 %) and photons (4 %). These
researchers concluded that fast neutron radiotherapy provides
higher local control rates than a mixed beam and photons in
advanced, recurrent or not completely resected ACC of the major
and minor salivary glands. Neutron radiotherapy can be
recommended in patients with bad prognosis with
gross/macroscopic residual disease (R2 resection), with
unresectable tumors, or inoperable tumors.
Douglas et al (2003) evaluated the effectiveness of fast neutron
radiotherapy for the treatment of salivary gland neoplasms. Of
the 279 patients, 263 had evidence of gross residual disease at
the time of treatment, while16 had no evidence of gross residual
disease; 141 had tumors of a major salivary gland, and 138 had
tumors of minor salivary glands. The median follow‐up period
was 36 months (range of 1 to 142 months). The main outcome
44 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
measures were local‐regional control, cause‐specific survival, and
freedom from metastasis. The 6‐year actuarial cause‐specific
survival rate was 67 %. Multi‐variate analysis revealed that low
group stage (I ‐ II) disease, minor salivary sites, lack of skull base
invasion, and primary disease were associated with a statistically
significant improvement in cause‐specific survival. The 6‐year
actuarial local‐regional control rate was 59 %. Multi‐variate
analysis revealed size 4 cm or smaller, lack of base of skull
invasion, prior surgical resection, and no previous radiotherapy to
have a statistically significant improved local‐regional control.
Patients without evidence of gross residual disease had a 100 %
6‐year actuarial local‐regional control. The 6‐year actuarial
freedom from metastasis rate was 64 %. Factors associated with
decreased development of systemic metastases included negative
lymph nodes at the time of treatment and lack of base of skull
involvement. The 6‐year actuarial rate of development of grade 3
or 4 long‐term toxicity (using the Radiation Therapy Oncology
Group and European Organization for Research on the Treatment
of Cancer criteria) was 10 %. No patient experienced grade 5
toxic effects. The authors concluded that NBT is an effective
treatment for patients with salivary gland neoplasms who have
gross residual disease and achieves excellent local‐regional
control in patients without evidence of gross disease.
Other Types of Cancer:
Russell et al (1994) evaluated the effectiveness of fast neutron
radiation therapy in treatment of locally advanced carcinomas of
the prostate (n = 178). Median follow‐up was 68 months (range
of 40 to 86 months). The 5‐year actuarial clinical local‐regional
failure rate was significantly better for neutron‐treated patients
than photon‐treated patients (11 % versus 32 %). When findings
of routine post‐treatment prostate biopsies were incorporated,
the resulting "histological" local‐regional tumor failure rates were
13 % for the neutron‐treated group versus 32 % for the photon‐
treated group (p = 0.01). Moreover, actuarial survival and cause‐
specific survival rates were statistically indistinguishable for the 2
patient cohorts, with 32 % of the neutron‐treated patient deaths
and 41 % of the photon‐treated patient deaths caused by
prostate cancer. Prostate specific antigen values were elevated in

45 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
17 % of neutron‐treated patients and 45 % of photon‐treated
patients at 5 years (p < 0.001). Severe late complications of
treatment were higher for the neutron‐treated patients (11 %
versus 3 %), and were inversely correlated with the degree of
neutron beam shaping available at the participating institutions.
The authors concluded that high energy fast neutron
radiotherapy is safe and effective when adequate beam delivery
systems and collimation are available, and it is significantly
superior to external beam photon radiotherapy in the local‐
regional treatment of large prostate tumors.
In a review on the use of fast neutron radiation for the treatment
of prostatic adenocarcinomas, Lindsley et al (1998) stated that the
Radiation Therapy Oncology Group performed a multi‐
institutional randomized trial comparing mixed beam (neutron
plus photon) irradiation to conventional photon irradiation for the
treatment of locally advanced prostate cancer. A subsequent
randomized trial by the Neutron Therapy Collaborative Working
Group compared pure neutron irradiation to standard photon
irradiation. Both studies reported significant improvement in
loco‐regional control with neutron irradiation compared to
conventional photon irradiation in the treatment of locally
advanced prostate carcinoma. To date, only the mixed beam
study has demonstrated a significant survival benefit. Future
analysis of the larger Neutron Therapy Collaborative Working
Group trial at the 10‐year follow‐up should confirm whether or
not improved loco‐regional control translates into a survival
advantage.
Lindsley et al (1996) noted that a phase III clinical study
comparing NBT to photon radiotherapy for inoperable regional
non‐small cell lung cancer showed no overall improvement in
survival. However, a statistically significant improvement in
survival was observed in the subset of patients with squamous
cell histology. Engenhart‐Cabillic and colleagues (1998) discussed
the use of NBT in the management of locally advanced non‐
resectable primary or recurrent rectal cancer. They noted that
the value of radiation therapy in managing such patients is being
appreciated, although up to 40 % of the treated patients have no
symptomatic response. The authors also stated that over
46 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
350 patients were entered in studies comparing NBT alone and
mixed‐beam treatments. At present, no therapeutic gain for
long‐lasting survival has been achieved. However, local control
and pain improvement seems to be better with NBT than with
photon therapy. There is insufficient evidence regarding the
effectiveness of NBT for rectal and lung cancers.
Strander et al (2003) stated that there is some evidence that
adjuvant radiation therapy in combination with conservative
surgery improves the local control rate in the treatment of STS of
extremities and trunk in patients with negative, marginal or
minimal microscopic positive surgical margins. A local control
rate of 90 % has been achieved. Improvement is obtained with
radiation therapy added in the case of intralesional surgery, but
the local control rate is somewhat lower. More studies are
needed on this issue. For STS in other anatomical sites,
retroperitoneum, head and neck, breast and uterus, there is only
weak indication of a benefit for the local control rate, with the use
of adjuvant radiation therapy. There is still insufficient data to
establish that pre‐operative radiotherapy is favorable compared
to post‐operative radiotherapy for local control in patients
presenting primarily with large tumors. One small study has
shown a possible survival benefit for pre‐operative radiotherapy.
There is fairly good evidence to suggest that the pre‐operative
setting results in more wound complications. There is no
randomized study comparing external beam radiotherapy and
brachytherapy. The data suggested that external beam
radiotherapy and low‐dose rate brachytherapy result in
comparable local control for high‐grade tumors. Some patients
with low‐grade STS benefit from external beam radiotherapy in
terms of local control. Brachytherapy with low‐dose rate for low‐
grade tumors seems to be of no benefit, but data are sparse. The
available data are inconclusive concerning the effect of intra‐
operative high‐dose rate radiotherapy for retroperitoneal STS.
Further studies are needed. Neutron radiotherapy might be
beneficial for patients with low‐grade and intermediate‐grade
tumors considered inoperable and for those operated with
intralesional margins. More severe adverse effects for NBT have
been reported.
47 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Murray (2004) noted that the commonest STS of the upper
extremity are the epithelioid sarcoma, synovial cell sarcoma, and
malignant fibrous histiocytoma. Limb salvage surgery is the
treatment of choice for STS to preserve upper extremity
function. Following wide tumor resection, adjuvant therapies
such as chemotherapy, external beam radiation therapy, and
brachytherapy may lessen local recurrence rates, but their effect
on overall survival remains unclear.
A review by Hassen‐Khodja and Lance (2003) stated that the
efficacy of NBT is well‐established only for the treatment of
inoperable or unresectable salivary gland tumors, regardless of
their degree of malignancy or stage of progression, and for the
treatment of large residual tumors after surgical resection. The
authors also examined the data on the effectiveness of for NBT in
the treatment of malignant prostate tumors, STS and central
nervous system tumors. However, these data are insufficient to
rule on its therapeutic efficacy.
An assessment of the evidence for neutron beam radiotherapy
prepared by the Australia and New Zealand Horizon Scanning
Network (Purins et al, 2007) found that NBT is a promising
technology. The assessment cautioned, however, that "[t]he
studies identified in this prioritising summary were not of high
quality and, as such, the conclusions must be taken as preliminary
in nature."
In a phase I study, Kankaanranta and colleagues (2011) examined
the safety of BNCT in the treatment of malignant gliomas that
progress after surgery and conventional external beam radiation
therapy. Adult patients who had histologically confirmed
malignant glioma that had progressed after surgery and external
beam radiotherapy were included in this study, provided that
greater than 6 months had elapsed from the last date of radiation
therapy. The first 10 patients received a fixed dose, 290 mg/kg, of
l‐boronophenylalanine‐fructose (l‐BPA‐F) as a 2‐hour infusion
before neutron irradiation, and the remaining patients were
treated with escalating doses of l‐BPA‐F, either 350 mg/kg, 400
mg/kg, or 450 mg/kg, using 3 patients on each dose level.
Adverse effects were assessed using National Cancer Institute
48 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Common Toxicity Criteria version 2.0. A total of 22 patients
entered the study. Twenty subjects had glioblastoma, and 2
patients had anaplastic astrocytoma, and the median cumulative
dose of prior external beam radiotherapy was 59.4 Gy. The
maximally tolerated l‐BPA‐F dose was reached at the 450 mg/kg
level, where 4 of 6 patients treated had a grade 3 adverse event.
Patients who were given more than 290 mg/kg of l‐BPA‐F
received a higher estimated average planning target volume dose
than those who received 290 mg/kg (median of 36 versus 31 Gy
[W, i.e., a weighted dose]; p = 0.018). The median survival time
following BNCT was 7 months. The authors concluded that BNCT
administered with an l‐BPA‐F dose of up to 400 mg/kg as a 2‐hour
infusion is feasible in the treatment of malignant gliomas that
recur after conventional radiation therapy.
Ghost Cell Odontogenic Carcinoma:
Martos‐Fernandez et al (2014) noted that ghost cell odontogenic
carcinoma is a rare condition characterized by ameloblastic‐like
islands of epithelial cells with aberrant keratinitation in the form
of ghost cell with varying amounts of dysplastic dentina. These
investigators reported a case of a 70‐year old woman with a rapid
onset of painful swelling right maxillary tumor. Magnetic
resonance showed a huge tumor dependent on the right half of
the right hard palate with invasion of the pterygoid process and
focally to the second branch of the trigeminal. Radiological stage
was T4N0. The patient underwent a right subtotal maxillectomy
with clear margins. Adjuvant radiotherapy was given. The patient
was free of residual or recurrent disease 12 months after
surgery. The tumor was 3.9 cm in diameter. It was spongy and
whitish gray. Microscopically the tumor was arranged in nets and
trabeculae, occasionally forming palisade. Tumoral cells had clear
cytoplasm with vesicular nuclei. There was atipia and mitosi with
vascular and peri‐neural invasion. The excised tumor was
diagnosed as a GCOC. The authors concluded that ghost cell
carcinoma is a rare odontogenic carcinoma. Its course is
unpredictable, ranging from locally invasive tumors of slow
growth to highly aggressive and infiltrative ones. Wide surgical
excision with clean margins is the treatment of choice although
its combination with post‐operative radiation therapy, with or
49 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
without chemotherapy, remains controversial. This was a single‐
case study, and it’s unclear whether NBT was used as adjuvant
radiotherapy. Moreover the authors stated that post‐operative
radiation therapy, with or without chemotherapy, remains
controversial.
Li et al (2014) stated that the diagnosis of ameloblastic carcinoma
is often difficult and the optimal treatment methods remain
controversial. The current study retrospectively investigated the
optimal diagnosis and treatment methods of 12 ameloblastic
carcinoma patients at the West China Hospital of Stomatology,
Sichuan University (Chengdu, China), and 20 patients selected
from the PubMed database, were reviewed. The clinical features,
diagnosis and outcome of the different treatments were
evaluated. Ameloblastic carcinoma occurred in 12 out of a total
of 538 ameloblastoma patients; the majority were of the primary
type. Of the 538 ameloblastoma patients, 294 were males, 244
were females with a male to female ratio of 1.2:1. The
predilection age is 20 to 30 years, which accounts for 40 % of the
total. In total, 461 cases were in the mandible and 77 were
located in the maxilla. The cure rate of the primary type and the
recurrence rate of the secondary type tumors were higher in the
patients from the West China Hospital of Stomatology compared
with those reported in the literature. In particular, a case with a
long‐term survival of 30 years was presented, which was
considered to be relatively rare. The evolution of the clinical
course has experienced 3 stages: Ameloblastoma (1978) followed
by metastatic ameloblastoma (2000) and finally ameloblastic
carcinoma (2008). To avoid recurrence, wide local excision with
post‐operative radiation therapy was required. While novel
therapeutic regimens should also be considered as appropriate,
including carbon ion therapy and Gamma Knife stereotactic
radiosurgery. However, controlled studies with larger groups of
patients are required to increase the accuracy of results. This
study did not mention ghost cell odontogenic carcinoma and NBT.
Furthermore, reviews on “Ghost cell odontogenic carcinoma”
(Martos‐Fernandez et al, 2014; Ahmed et al, 2015) do not
mention NBT as a therapeutic option.
50 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
CPT Codes / HCPCS Codes / ICD‐10 Codes
Informa'tion in the [brackets] below has been added for clarifica'tion
purposes. Codes requiring a 7th character are represented by "+":
Proton Beam Radiotherapy (PBRT):
CPT codes covered if selection criteria are met:
77520 Proton treatment delivery; simple, without
compensation
77522 simple, with compensation
77523 intermediate
77525 complex
Other CPT codes related to the CPB:
61796 Stereotactic radiosurgery (particle beam, gamma ray
or linear accelerator); 1 simple cranial lesion
+61797 each additional cranial lesion, simple (List separately
in addition to code for primary procedure)
61798 1 complex cranial lesion
+61799 each additional cranial lesion, complex (List
separately in addition to code for primary procedure)
63620 Stereotactic radiosurgery (particle beam, gamma ray,
or linear accelerator); 1 spinal lesion
+63621 each additional spinal lesion, complex (List
separately in addition to code for primary procedure)
77432 Stereotactic radiation treatment management of
cranial lesion(s) (complete course of treatment
consisting of 1 session)
Other HCPCS codes related to the CPB:
S8030 Scleral application of tantalum ring(s) for localization
of lesions for proton beam therapy
ICD‐10 codes covered if selection criteria are met for adults:
C41.0 Malignant neoplasm of bones of skull and face
[Chordomas or chondrosarcomas arising at the base of
the skull or cervical spine without distant metastases]
51 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
C41.2 Malignant neoplasm of vertebral column [Chordomas
or chondrosarcomas arising at the base of the skull or
cervical spine without distant metastases]
C69.30 ‐
C69.32
Malignant neoplasm of choroid
C69.40 ‐ Malignant neoplasm of ciliary body [confined to globe
C69.42 ‐ not distant metastases]
C75.1 Malignant neoplasm of pituitary gland and
craniopharyngeal duct
C75.2 Malignant neoplasm of craniopharyngeal duct
D33.4 Benign neoplasm of spinal cord [Chordomas or
chondrosarcomas arising at the base of the skull or
cervical spine without distant metastases]
D43.0 ‐ Neoplasm of uncertain behavior of brain and spinal
D43.2, D43.4 cord [Chordomas or chondrosarcomas arising at the
base of the skull or cervical spine without distant
metastases]
ICD‐10 codes not covered for indications listed in the CPB for adults
(not all‐inclusive):
C01 ‐ C02.9 Malignant neoplasm of tongue [squamous cell
carcinoma]
C06.9 Malignant neoplasm of mouth, unspecified [Malignant
neoplasm of minor salivary gland, unspecified site]
C07 ‐ C08.9 Malignant neoplasm of major salivary glands
C09.0 ‐
C09.9
Malignant neoplasm of tonsil
C11.0 ‐
C11.9
Malignant neoplasm of nasopharynx [adenoid cystic
carcinoma] [nasopharngeal carcinoma]
C14.0 ‐
C14.8
Malignant neoplasm of other and ill‐defined sites
within the lip, oral cavity, and pharynx
C15.3 ‐
C15.9
Malignant neoplasm of esophagus
C17.0 ‐
C17.9
Malignant neoplasm of small intestine
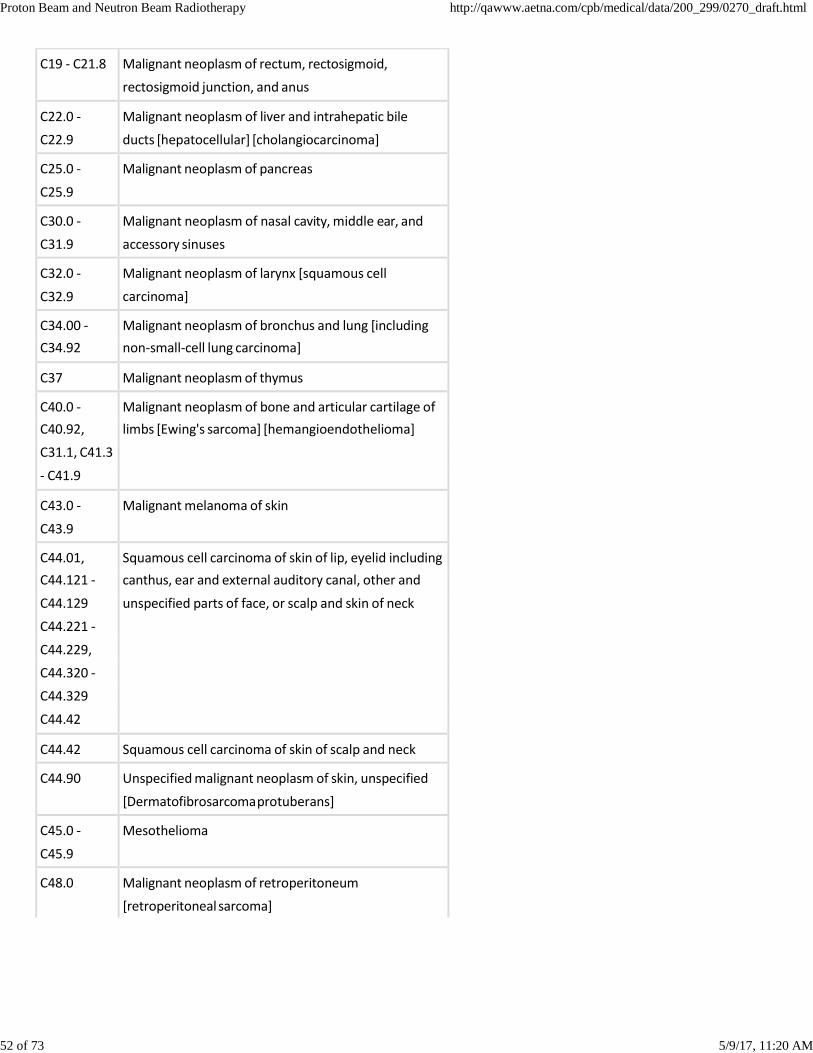
52 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
C19 ‐ C21.8 Malignant neoplasm of rectum, rectosigmoid,
rectosigmoid junction, and anus
C22.0 ‐
C22.9
Malignant neoplasm of liver and intrahepatic bile
ducts [hepatocellular] [cholangiocarcinoma]
C25.0 ‐
C25.9
Malignant neoplasm of pancreas
C30.0 ‐
C31.9
Malignant neoplasm of nasal cavity, middle ear, and
accessory sinuses
C32.0 ‐
C32.9
Malignant neoplasm of larynx [squamous cell
carcinoma]
C34.00 ‐ Malignant neoplasm of bronchus and lung [including
C34.92 non‐small‐cell lung carcinoma]
C37 Malignant neoplasm of thymus
C40.0 ‐ Malignant neoplasm of bone and articular cartilage of
C40.92, limbs [Ewing's sarcoma] [hemangioendothelioma]
C31.1, C41.3
‐ C41.9
C43.0 ‐
C43.9
Malignant melanoma of skin
C44.01, Squamous cell carcinoma of skin of lip, eyelid including
C44.121 ‐ canthus, ear and external auditory canal, other and
C44.129 unspecified parts of face, or scalp and skin of neck
C44.221 ‐
C44.229,
C44.320 ‐
C44.329
C44.42
C44.42 Squamous cell carcinoma of skin of scalp and neck
C44.90 Unspecified malignant neoplasm of skin, unspecified
[Dermatofibrosarcoma protuberans]
C45.0 ‐
C45.9
Mesothelioma
C48.0 Malignant neoplasm of retroperitoneum
[retroperitoneal sarcoma]
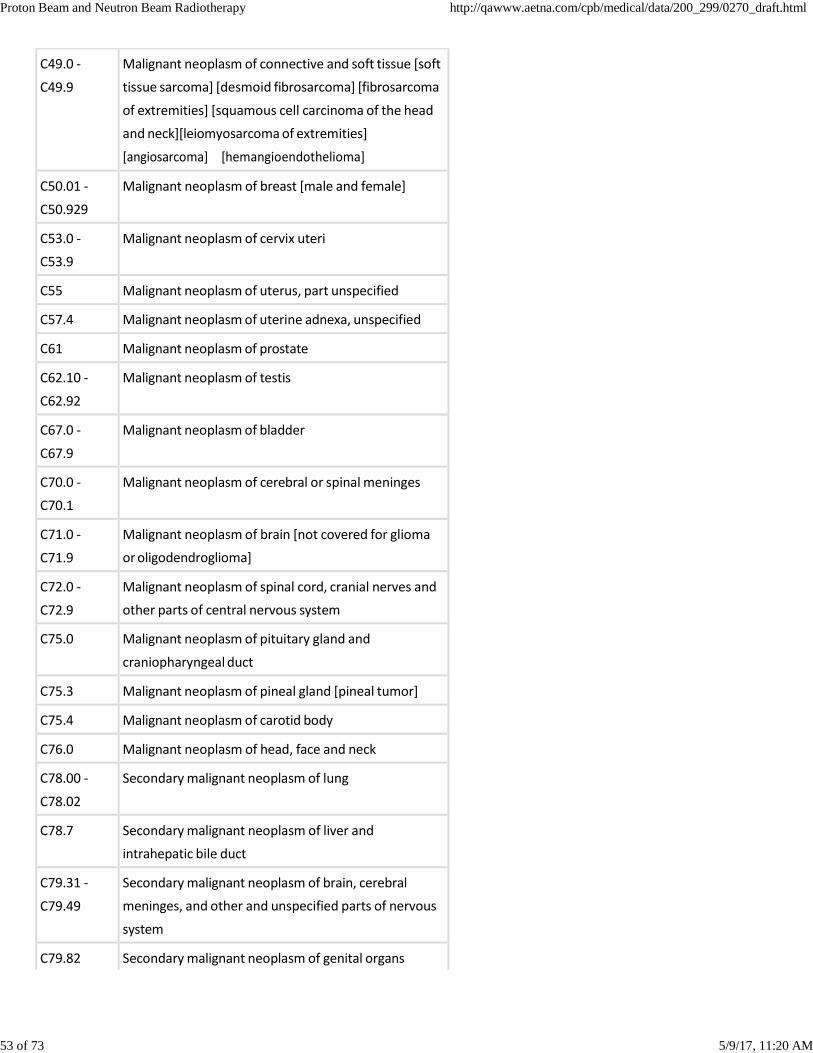
53 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
C49.0 ‐
C49.9
Malignant neoplasm of connective and soft tissue [soft
tissue sarcoma] [desmoid fibrosarcoma] [fibrosarcoma
of extremities] [squamous cell carcinoma of the head
and neck][leiomyosarcoma of extremities]
[angiosarcoma] [hemangioendothelioma]
C50.01 ‐
C50.929
Malignant neoplasm of breast [male and female]
C53.0 ‐
C53.9
Malignant neoplasm of cervix uteri
C55 Malignant neoplasm of uterus, part unspecified
C57.4 Malignant neoplasm of uterine adnexa, unspecified
C61 Malignant neoplasm of prostate
C62.10 ‐
C62.92
Malignant neoplasm of testis
C67.0 ‐
C67.9
Malignant neoplasm of bladder
C70.0 ‐
C70.1
Malignant neoplasm of cerebral or spinal meninges
C71.0 ‐
C71.9
Malignant neoplasm of brain [not covered for glioma
or oligodendroglioma]
C72.0 ‐
C72.9
Malignant neoplasm of spinal cord, cranial nerves and
other parts of central nervous system
C75.0 Malignant neoplasm of pituitary gland and
craniopharyngeal duct
C75.3 Malignant neoplasm of pineal gland [pineal tumor]
C75.4 Malignant neoplasm of carotid body
C76.0 Malignant neoplasm of head, face and neck
C78.00 ‐
C78.02
Secondary malignant neoplasm of lung
C78.7 Secondary malignant neoplasm of liver and
intrahepatic bile duct
C79.31 ‐
C79.49
Secondary malignant neoplasm of brain, cerebral
meninges, and other and unspecified parts of nervous
system
C79.82 Secondary malignant neoplasm of genital organs
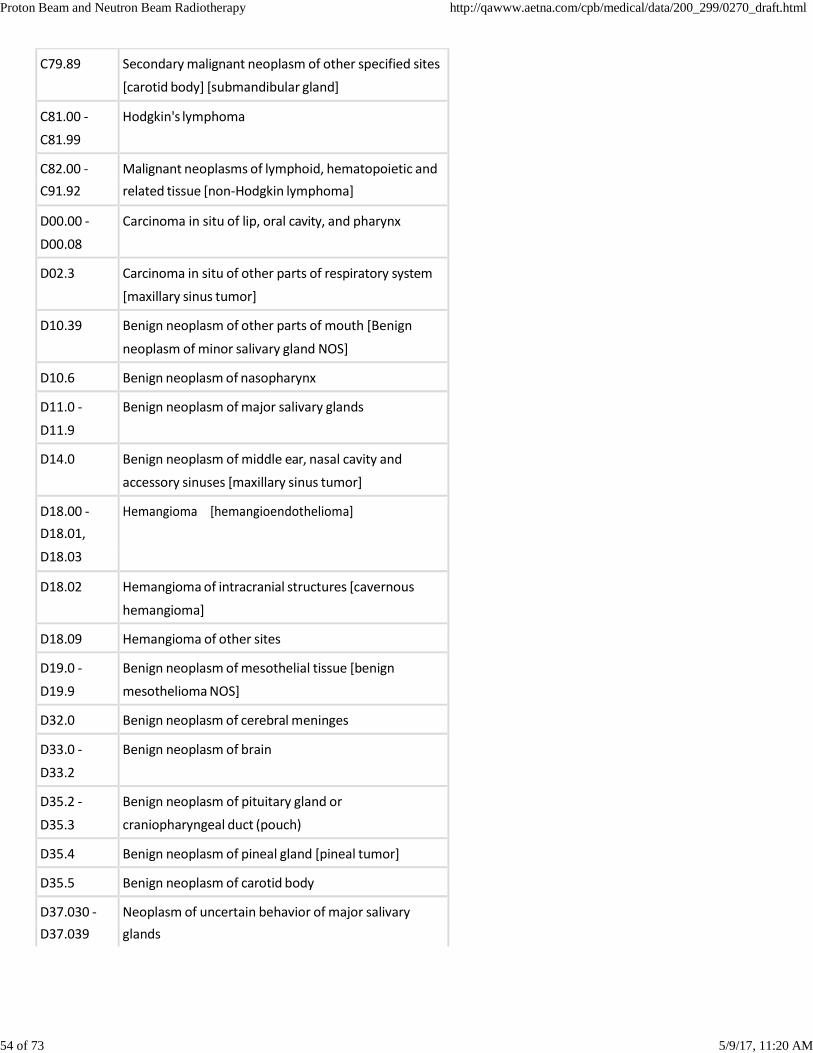
54 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
C79.89 Secondary malignant neoplasm of other specified sites
[carotid body] [submandibular gland]
C81.00 ‐
C81.99
Hodgkin's lymphoma
C82.00 ‐ Malignant neoplasms of lymphoid, hematopoietic and
C91.92 related tissue [non‐Hodgkin lymphoma]
D00.00 ‐
D00.08
Carcinoma in situ of lip, oral cavity, and pharynx
D02.3 Carcinoma in situ of other parts of respiratory system
[maxillary sinus tumor]
D10.39 Benign neoplasm of other parts of mouth [Benign
neoplasm of minor salivary gland NOS]
D10.6 Benign neoplasm of nasopharynx
D11.0 ‐
D11.9
Benign neoplasm of major salivary glands
D14.0 Benign neoplasm of middle ear, nasal cavity and
accessory sinuses [maxillary sinus tumor]
D18.00 ‐ Hemangioma [hemangioendothelioma]
D18.01,
D18.03
D18.02 Hemangioma of intracranial structures [cavernous
hemangioma]
D18.09 Hemangioma of other sites
D19.0 ‐
D19.9
Benign neoplasm of mesothelial tissue [benign
mesothelioma NOS]
D32.0 Benign neoplasm of cerebral meninges
D33.0 ‐
D33.2
Benign neoplasm of brain
D35.2 ‐
D35.3
Benign neoplasm of pituitary gland or
craniopharyngeal duct (pouch)
D35.4 Benign neoplasm of pineal gland [pineal tumor]
D35.5 Benign neoplasm of carotid body
D37.030 ‐ Neoplasm of uncertain behavior of major salivary
D37.039 glands
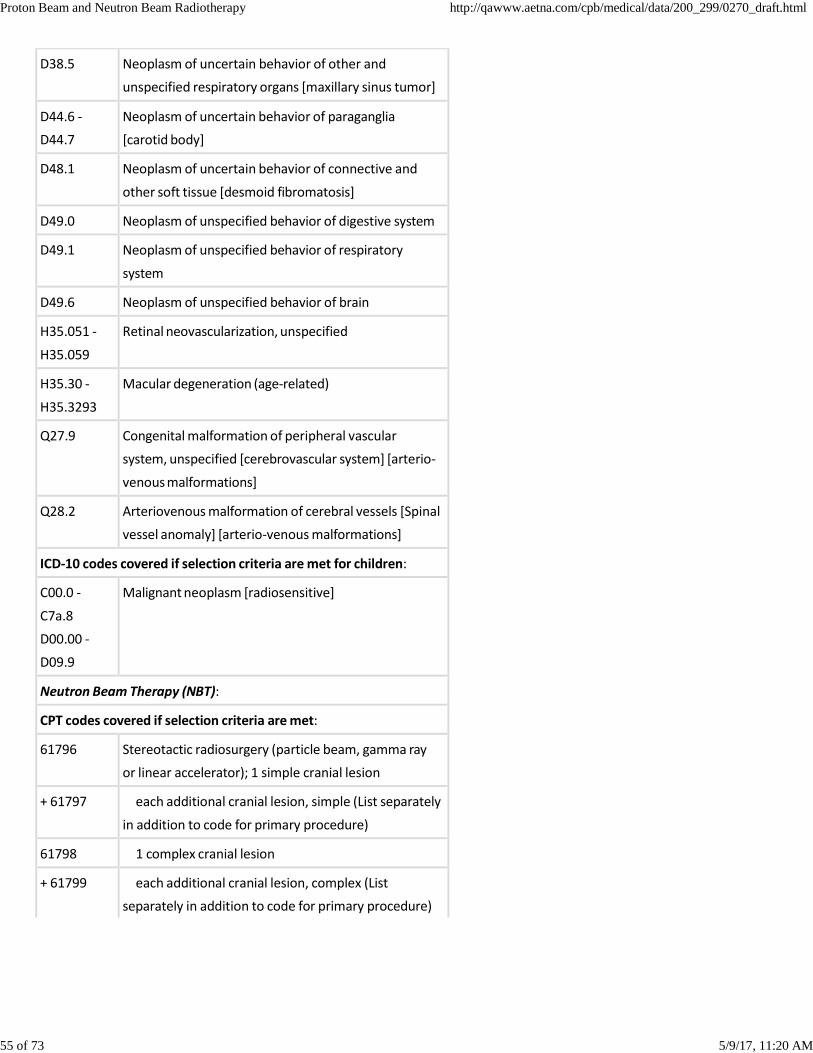
55 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
D38.5 Neoplasm of uncertain behavior of other and
unspecified respiratory organs [maxillary sinus tumor]
D44.6 ‐
D44.7
Neoplasm of uncertain behavior of paraganglia
[carotid body]
D48.1 Neoplasm of uncertain behavior of connective and
other soft tissue [desmoid fibromatosis]
D49.0 Neoplasm of unspecified behavior of digestive system
D49.1 Neoplasm of unspecified behavior of respiratory
system
D49.6 Neoplasm of unspecified behavior of brain
H35.051 ‐
H35.059
Retinal neovascularization, unspecified
H35.30 ‐
H35.3293
Macular degeneration (age‐related)
Q27.9 Congenital malformation of peripheral vascular
system, unspecified [cerebrovascular system] [arterio‐
venous malformations]
Q28.2 Arteriovenous malformation of cerebral vessels [Spinal
vessel anomaly] [arterio‐venous malformations]
ICD‐10 codes covered if selection criteria are met for children:
C00.0 ‐
C7a.8
D00.00 ‐
D09.9
Malignant neoplasm [radiosensitive]
Neutron Beam Therapy (NBT):
CPT codes covered if selection criteria are met:
61796 Stereotactic radiosurgery (particle beam, gamma ray
or linear accelerator); 1 simple cranial lesion
+ 61797 each additional cranial lesion, simple (List separately
in addition to code for primary procedure)
61798 1 complex cranial lesion
+ 61799 each additional cranial lesion, complex (List
separately in addition to code for primary procedure)
56 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
77422 High energy neutron radiation treatment delivery;
single treatment area using a single port or parallel‐
opposed ports with no blocks or simple blocking
77423 1 or more isocenter(s) with coplanar or non‐
coplanar geometry with blocking and/or wedge,
and/or compensator(s)
ICD‐10 codes covered if selection criteria are met:
C07 ‐ C08.9 Malignant neoplasm of major salivary glands [locally
advanced, unresectable, or inoperable]
ICD‐10 codes not covered for indications listed in the CPB (not
all‐inclusive):
C00.0 ‐
C06.9
C09.0 ‐
C80.2
Malignant neoplasms [other than salivary gland]
[includes ghost cell odontogenic carcinoma]
The above policy is based on the following references:
Proton Beam Therapy:
1. Matsuzaki Y, Osuga T, Saito Y, et al. A new, effective, and
safe therapeutic option using proton irradiation for
hepatocellular carcinoma. Gastroenterology.
1994;106(4):1032‐1041.
2. Shipley WU, Verhey LJ, Munzenrider JE. Advanced prostate
cancer: The results of a randomized comparative trial of
high dose irradiation boosting with conformal protons
compared with conventional dose irradiation using protons
alone. Int J Radio Oncol Biol Phys. 1995;32:3‐12.
3. Raju MR. Proton radiobiology, radiosurgery and
radiotherapy. Int J Radiat Biol. 1995;67:237‐259.
4. Levin VA, Gutin PH, Leibel S. Neoplasms of the central
nervous system. In: Cancer: Principles and Practice of
Oncology. VT DeVita, S Hellman, AS Rosenberg, eds.
Philadelphia, PA: JB Lippincott; 1993: 1723‐1724.
5. Nahum AE, Dearnaley DP, Steel GG. Prospects for proton
beam radiotherapy. Eur J Canc. 1994;30A:1577‐1583.
57 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
6. Hanks GE. A question filled future for dose escalation in
prostate cancer. In J Radiation Oncol Biol Phys.
1995;32:267‐269.
7. Suit H, Urie M. Proton beams in radiation therapy. J Natl
Cancer Inst. 1992;84:155‐164.
8. Rossi CJ Jr, Slater JD, Reyes‐Molyneux N, et al. Particle beam
radiation therapy in prostate cancer: Is there an advantage?
Semin Radiat Oncol. 1998;8(2):115‐123.
9. Zelefsky MJ, Leibel SA, Kutcher GJ, Fuks Z. Three‐
dimensional conformal radiotherapy and dose escalation:
Where do we stand? Semin Radiat Oncol. 1998;8(2):107‐
114.
10. Fleurette F. Charvet‐Protat S. Proton and neutron radiation
in cancer treatment: Clinical and economic outcomes.
French National Agency for Medical Evaluation (ANDEM).
Bull Cancer Radiother. 1996;83(Suppl):223s‐227s.
11. Rossi CJ. Conformal proton beam therapy of prostate
cancer – update on the Loma Linda University medical
center experience. Strahlenther Onkol. 1999;175(Suppl
2):82‐84.
12. Yonemoto LT, Slater JD, Rossi CJ Jr, et al. Combined proton
and photon conformal radiation therapy for local advanced
carcinoma of the prostate: Preliminary results of a phase
I/II study. Int J Radiat Oncol Bio Phys. 1997;37(1):21‐29.
13. Slater JD, Yonemoto LT, Rossi CJ Jr, et al. Conformal proton
therapy for prostate carcinoma. Int J Radiat Oncol Bio Phys.
1998;42(2):229‐304.
14. Krengli M, Liebsch NJ, Hug EB, et al. Review of current
protocols for proton therapy in USA. Tumori.
1998;84(2):209‐216.
15. Hart KB, Porter AT. A rational approach to the treatment of
prostate cancer with radiation therapy: Lessons for the
future. Semin Oncol. 1997;24(6):745‐755.
16. Carroll PR, Presti JC Jr, Small E, et al. Focal therapy for
prostate cancer 1996: Maximizing outcome. Urology.
1997;49(3A Suppl):84‐94.
17. Habrand JL, Schlienger P, Schwartz L, et al. Clinical
applications of proton therapy. Experiences and ongoing
studies. Radiat Environ Biophys. 1995;34(1):41‐44.
18. Tsuji H, Inada T, Maruhashi A, et al. Clinical results of
58 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
fractionated proton therapy. Int J Radiat Oncol Bio Phys.
1993;25(1):49‐60.
19. Bush DA, Slater JD, Bonnet R, et al. Proton‐beam
radiotherapy for early‐stage lung cancer. Chest.
1999;116(5):1313‐1319.
20. Habrand JL, Mammar H, Ferrand R, et al. Proton beam
therapy (PT) in the management of CNS tumors in
childhood. Strahlenther Onkol. 1999;175 Suppl 2:91‐94.
21. Hug EB, Slater JD. Proton radiation therapy for chordomas
and chondrosarcomas of the skull base. Neurosurg Clin N
Am. 2000;11(4):627‐638.
22. Krisch EB, Koprowski CD. Deciding on radiation therapy for
prostate cancer: The physician's perspective. Semin Urol
Oncol. 2000;18(3):214‐225.
23. Gragoudas ES, Lane AM, Regan S, et al. A randomized
controlled trial of varying radiation doses in the treatment
of choroidal melanoma. Arch Ophthalmol.
2000;118(6):773‐778.
24. Munzenrider JE. Uveal Melanomas. Conservation
treatment. Hematol Oncol Clin North Am.
2001;15(2):389‐402.
25. Bonnet RB, Bush D, Cheek GA, et al. Effects of proton and
combined proton/photon beam radiation on pulmonary
function in patients with resectable but medically
inoperable non‐small cell lung cancer. Chest.
2001;120(6):1803‐1810.
26. Noel G, Habrand JL, Jauffret E, et al. Radiation therapy for
chordoma and chondrosarcoma of the skull base and the
cervical spine. Prognostic factors and patterns of failure.
Strahlenther Onkol. 2003;179(4):241‐248.
27. Egger E, Zografos L, Schalenbourg A, et al. Eye retention
after proton beam radiotherapy for uveal melanoma. Int J
Radiat Oncol Biol Phys. 2003;55(4):867‐880.
28. Noel G, Habrand JL, Helfre S, et al. Proton beam therapy in
the management of central nervous system tumors in
childhood: The preliminary experience of the Centre de
Protontherapie d'Orsay. Med Pediatr Oncol.
2003;40(5):309‐315.
29. Robertson DM. Changing concepts in the management of
choroidal melanoma. Am J Ophthalmol.
59 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
2003;136(1):161‐170.
30. Li W, Gragoudas ES, Egan KM. Tumor basal area and
metastatic death after proton beam irradiation for
choroidal melanoma. Arch Ophthalmol.
2003;121(1):68‐72.
31. Ciulla TA, Danis RP, Klein SB, et al. Proton therapy for
exudative age‐related macular degeneration: A
randomized, sham‐controlled clinical trial. Am J
Ophthalmol. 2002;134(6):905‐906.
32. Spatola C, Privitera G, Raffaele L, et al. Clinical application
of proton beams in the treatment of uveal melanoma: The
first therapies carried out in Italy and preliminary results
(CATANA Project). Tumori. 2003;89(5):502‐509.
33. Kagei K, Tokuuye K, Okumura T, et al. Long‐term results of
proton beam therapy for carcinoma of the uterine cervix.
Int J Radiat Oncol Biol Phys. 2003;55(5):1265‐1271.
34. Silander H, Pellettieri L, Enblad P, et al. Fractionated,
stereotactic proton beam treatment of cerebral
arteriovenous malformations. Acta Neurol Scand.
2004;109(2):85‐90.
35. Sivagnanavel V, Evans JR, Ockrim Z, Chong V. Radiotherapy
for neovascular age‐related macular degeneration.
Cochrane Database Syst Rev. 2004;(3):CD004004.
36. Bush DA, Hillebrand DJ, Slater JM, Slater JD. High‐dose
proton beam radiotherapy of hepatocellular carcinoma:
Preliminary results of a phase II trial. Gastroenterology.
2004;127(5 Suppl 1):S189‐S193.
37. Zietman AL, DeSilvio ML, Slater JD, et al. Comparison of
conventional‐dose vs high‐dose conformal radiation
therapy in clinically localized adenocarcinoma of the
prostate: A randomized controlled trial. JAMA.
2005;294(10):1233‐1239.
38. Kawashima M, Furuse J, Nishio T, et al. Phase II study of
radiotherapy employing proton beam for hepatocellular
carcinoma. J Clin Oncol. 2005;23(9):1839‐1846.
39. Nihei K, Ogino T, Ishikura S, et al. Phase II feasibility study of
high‐dose radiotherapy for prostate cancer using proton
boost therapy: First clinical trial of proton beam therapy for
prostate cancer in Japan. Jpn J Clin Oncol. 2005;35(12):745‐
752.
60 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
40. Al‐Shahi R, Warlow CP. Interventions for treating brain
arteriovenous malformations in adults. Cochrane Database
Syst Rev. 2006;(1):CD003436.
41. Nihei K, Ogino T, Ishikura S, Nishimura H. High‐dose proton
beam therapy for Stage I non‐small‐cell lung cancer. Int J
Radiat Oncol Biol Phys. 2006;65(1):107‐111.
42. Fitzek MM, Linggood RM, Adams J, Munzenrider JE.
Combined proton and photon irradiation for
craniopharyngioma: Long‐term results of the early cohort
of patients treated at Harvard Cyclotron Laboratory and
Massachusetts General Hospital. Int J Radiat Oncol Biol
Phys. 2006;64(5):1348‐1354.
43. Kozak KR, Smith BL, Adams J, et al. Accelerated partial‐
breast irradiation using proton beams: Initial clinical
experience. Int J Radiat Oncol Biol Phys.
2006;66(3):691‐698.
44. Adelaide Health Technology Assessment on behalf of
National Horizon Scanning Unit (HealthPACT and MSAC).
Proton beam therapy for cancer therapy. Horizon Scanning
Prioritising Summary ‐ Volume 13. Adelaide, SA;
HealthPACT and MSAC; 2006.
45. Konski A, Speier W, Hanlon A, et al. Is proton beam therapy
cost effective in the treatment of adenocarcinoma of the
prostate? J Clin Oncol. 2007;25(24):3603‐3608.
46. Almefty K, Pravdenkova S, Colli BO, et al. Chordoma and
chondrosarcoma: Similar, but quite different, skull base
tumors. Cancer. 2007;110(11):2457‐2467.
47. Hata M, Tokuuye K, Kagei K, et al. Hypofractionated high‐
dose proton beam therapy for stage I non‐small‐cell lung
cancer: Preliminary results of a phase I/II clinical study. Int
J Radiat Oncol Biol Phys. 2007;68(3):786‐793.
48. Nishimura H, Ogino T, Kawashima M, et al. Proton‐beam
therapy for olfactory neuroblastoma. Int J Radiat Oncol Biol
Phys. 2007;68(3):758‐762.
49. Vargas C, Fryer A, Mahajan C, et al. Dose‐volume
comparison of proton therapy and intensity‐modulated
radiotherapy for prostate cancer. Int J Radiat Oncol Biol
Phys. 2008;70(3):744‐751.
50. Bush DA, Slater JD, Garberoglio C, et al. A technique of
partial breast irradiation utilizing proton beam
61 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
radiotherapy: Comparison with conformal x‐ray therapy.
Cancer J. 2007;13(2):114‐118.
51. Konski A, Speier W, Hanlon A, et al. Is proton beam therapy
cost effective in the treatment of adenocarcinoma of the
prostate? J Clin Oncol. 2007;25:3565–3566.
52. Australian Safety and Efficacy Register of New Interventional
Procedures ‐ Surgical (ASERNIP‐S). Proton
beam therapy for the treatment of uveal melanoma.
Horizon Scanning Report. Stepney, SA: Australian Safety and
Efficacy Register of New Interventional Procedures ‐Surgical
(ASERNIP‐S); 2007.
53. Australian Safety and Efficacy Register of New
Interventional Procedures ‐ Surgical (ASERNIP‐S). Proton
beam therapy for the treatment of neoplasms involving (or
adjacent to) cranial structures. Horizon Scannint
Report. Stepney, SA: Australian Safety and Efficacy Register
of New Interventional Procedures ‐Surgical (ASERNIP‐S);
2007.
54. Wilt TJ, Shamliyan T, Taylor B, et al. Comparative
effectiveness of therapies for clinically localized prostate
cancer. Comparative Effectiveness Review No. 13. Rockville,
MD: Agency for Healthcare Research and Quality (AHRQ);
2008.
55. Wilt TJ, MacDonald R, Rutks I, et al. Systematic review:
Comparative effectiveness of therapies for clinically
localized prostate cancer. Ann Intern Med.
2008;148:435‐448.
56. Institute for Clinical and Economic Review (ICER).
Brachytherapy and proton beam therapy for treatment of
clinically localized, low‐risk prostate cancer. Final Appraisal
Document. Boston, MA: ICER; December 22, 2008.
57. Nguyen PL, Trofimov A, Zietman AL. et al. Proton‐beam vs
intensity‐modulated radiation therapy. Which is best for
treating prostate cancer? Oncology (Williston Park).
2008;22(7):748‐754; discussion 754, 757.
58. Efstathiou JA, Trofimov AV, Zietman AL. Life, liberty, and the
pursuit of protons: An evidence‐based review of the role of
particle therapy in the treatment of prostate cancer. Cancer
J. 2009;15(4):312‐318.
59. Hall EJ. Intensity‐modulated radiation therapy, protons, and
62 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
the risk of second cancers. Int J Radiat Oncol Biol Phys.
2006;65(1):1‐7.
60. Yock TI, Tarbell NJ. Technology insight: Proton beam
radiotherapy for treatment in pediatric brain tumors. Nat
Clin Pract Oncol. 2004;1(2):97‐103.
61. Wilson VC, McDonough J, Tochner Z. Proton beam
irradiation in pediatric oncology: An overview. J Pediatr
Hematol Oncol. 2005;27(8):444‐448.
62. Schulz RJ, Kagan AR. Should proton‐beam therapy be
widely adopted? Int J Radiat Oncol Biol Phys.
2008;72(5):1307‐1310.
63. Lodge M, Pijls‐Johannesma M, Stirk L, et al. A systematic
literature review of the clinical and cost‐effectiveness of
hadron therapy in cancer. Radiother Oncol.
2007;83(2):110‐122.
64. Olsen DR, Bruland OS, Frykholm G, et al. Proton therapy—A
systematic review of clinical effectiveness. Radiother Oncol.
2007;83:123–132.
65. Coen JJ, Zietman AL. Proton radiation for localized prostate
cancer. Nat Rev Urol. 2009;6(6):324‐330.
66. Merchant TE. Proton beam therapy in pediatric oncology.
Cancer J. 2009;15(4):298‐305.
67. Brada M, Pijls‐Johannesma M, De Ruysscher D. Proton
therapy in clinical practice: Current clinical evidence. J Clin
Oncol. 2007;25:965–970.
68. Brada M, Pijls‐Johannesma M, De Ruysscher D. Current
clinical evidence for proton therapy. Cancer J.
2009;15(4):319‐324.
69. Macdonald OK, Kruse JJ, Miller JM, et al. Proton beam
radiotherapy versus three‐dimensional conformal
stereotactic body radiotherapy in primary peripheral,
early‐stage non‐small‐cell lung carcinoma: A comparative
dosimetric analysis. Int J Radiat Oncol Biol Phys.
2009;75(3):950‐958.
70. Terasawa T, Dvorak T, Ip S, et al. Systematic review:
Charged‐particle radiation therapy for cancer. Ann Intern
Med. 2009;151(8):556‐565.
71. Ollendorf DA, Hayes J, McMahon P, et al.
Brachytherapy/proton beam therapy for clinically localized,
low‐risk prostate cancer. Boston, MA: Institute for Clinical
63 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
and Economic Review (ICER); 2008.
72. Trikalinos TA, Terasawa T, Ip S, Raman G, Lau J. Particle
Beam Radiation Therapies for Cancer. Technical Brief No. 1.
(Prepared by Tufts Medical Center Evidence‐based Practice
Center under Contract No. HHSA‐290‐07‐10055.) Rockville,
MD: Agency for Healthcare Research and Quality;
revised November 2009.
73. Samson DJ, Ratko TA, Rothenberg BM, et al. Comparative
effectiveness and safety of radiation therapy treatments for
head and neck cancer. Comparative Effectiveness Review
No. 20. Prepared by the Blue Cross Blue Shield Association
Technology Evaluation Center and Evidence‐based Practice
Center under Contract No. 290‐02‐0026 for the Agency for
Healthcare Research and Quality. AHRQ Publication No. 10‐
EHC014‐EF. Rockville, MD: AHRQ; May 2010.
74. Flynn K. Brief overview: Reviews of proton beam therapy
for cancer. Boston, MA: Veterans Health Administration
Technology Assessment Program (VATAP); April 2010.
75. Mizumoto M, Sugahara S, Nakayama H, et al. Clinical results
of proton‐beam therapy for locoregionally advanced
esophageal cancer. Strahlenther Onkol. 2010;186(9):482‐
488.
76. Bassim MK, Berliner KI, Fisher LM, et al. Radiation therapy
for the treatment of vestibular schwannoma: A critical
evaluation of the state of the literature. Otol Neurotol.
2010;31(4):567‐573.
77. Ligtenberg G, Staal PC, Kleijnen S. Indications for proton
therapy (part 1): Intraocular
tumours; Chordomas/chondrosarcomas; Paediatric
tumours. Report. CVZ Publication No. 287. Diemen, The
Netherlands: CVZ; March 23, 2010.
78. Ligtenberg G, Staal PC, et al. Indications for proton therapy
(part 2): Proton therapy for model‐based indications
(head/neck tumours, breast cancer, lung cancer and
prostate cancer) and for other indications. Report
[summary]. CVZ Publication No. 304. Diemen, The
Netherlands: CVZ; August 22, 2011.
79. Lance JM. La protontherapie. [Proton therapy]. Informative
Note. Montreal, QC: Agence d'evaluation des technologies
et des modes d'intervention en sante (AETMIS); 2010.
64 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
80. BlueCross BlueShield Association (BCBSA), Technology
Evaluation Center (TEC). Proton beam therapy for
non‐small‐cell lung cancer. TEC Assessment Report.
Chicago, IL BCBSA; 2010;25(7).
81. BlueCross BlueShield Association (BCBSA), Technology
Evaluation Center (TEC). Proton beam therapy for prostrate
cancer. TEC Assessment Program. Chicago, IL: BCBSA;
2011;25(10).
82. NCCN Clinical Practice Guidelines in Oncology. Esophageal
and esophagogastric junction cancers (Excluding the
proximal 5 cm of the stomach). Version 1.2011. Available
at: http://www.nccn.org/professionals/physician_gls
/pdf/esophageal.pdf (http://www.nccn.org/professionals
/physician_gls/pdf/esophageal.pdf). Accessed March 24,
2011.
83. Bush DA, Kayali Z, Grove R, Slater JD. The safety and efficacy
of high‐dose proton beam radiotherapy for hepatocellular
carcinoma: A phase 2 prospective trial. Cancer.
2011;117(13):3053‐3059.
84. Allen A, Pawlicki T, Bonilla L, et al; Evaluation
Subcommittee of ASTRO’s Emerging Technologies
Committee. An evaluation of proton beam therapy. Fairfax,
VA: American Society for Radiation Oncology (ASTRO);
October 2009.
85. Welsh J, Amini A, Likhacheva A, et al. Update: Modern
approaches to the treatment of localized esophageal
cancer. Curr Oncol Rep. 2011a;13(3):157‐167.
86. Welsh J, Gomez D, Palmer MB, et al. Intensity‐modulated
proton therapy further reduces normal tissue exposure
during definitive therapy for locally advanced distal
esophageal tumors: A dosimetric study. Int J Radiat Oncol
Biol Phys. 2011b;81(5):1336‐1342.
87. Mizumoto M, Sugahara S, Okumura T, et al.
Hyperfractionated concomitant boost proton beam therapy
for esophageal carcinoma. Int J Radiat Oncol Biol Phys.
2011;81(4):e601‐e606.
88. Hong TS, Ryan DP, Blaszkowsky LS, et al. Phase I study of
preoperative short‐course chemoradiation with proton
beam therapy and capecitabine for resectable pancreatic
ductal adenocarcinoma of the head. Int J Radiat Oncol Biol
65 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Phys. 2011;79(1):151‐157.
89. Ryan DP, Mamon H. Management of locally advanced and
borderline resectable exocrine pancreatic cancer. UpToDate
[online serial. Waltham, MA: UpToDate; reviewed January
2012.
90. Fernandez‐del Castillo C, Jimenez RE, Steer ML. Surgery in
the treatment of exocrine pancreatic cancer and prognosis.
UpToDate [online serial]. Waltham, MA: UpToDate;
reviewed January 2012.
91. Salgia R. Clinical presentation and management of
thymoma and thymic carcinoma. UpToDate [online serial].
Waltham, MA: UpToDate; reviewed January 2012.
92. Allen AM, Pawlicki T, Dong L, et al. An evidence based
review of proton beam therapy: The report of ASTRO's
emerging technology committee. Radiother Oncol.
2012;103(1):8‐11.
93. Hocht S, Wachtlin J, Bechrakis NE, et al. Proton or photon
irradiation for hemangiomas of the choroid? A
retrospective comparison. Int J Radiat Oncol Biol Phys.
2006;66(2):345‐351.
94. Levy‐Gabriel C, Rouic LL, Plancher C, et al. Long‐term results
of low‐dose proton beam therapy for circumscribed
choroidal hemangiomas. Retina. 2009;29(2):170‐175.
95. Chan RV, Yonekawa Y, Lane AM, et al. Proton beam
irradiation using a light‐field technique for the treatment of
choroidal hemangiomas. Ophthalmologica.
2010;224(4):209‐216.
96. Sheets NC, Goldin GH, Meyer AM, et al. Intensity‐
modulated radiation therapy, proton therapy, or conformal
radiation therapy and morbidity and disease control in
localized prostate cancer. JAMA. 2012;307(15):1611‐1620.
97. BlueCross BlueShield Association. Proton beam therapy for
non‐small‐cell lung cancer. BCBS Technology Evaluation
Center. September 2012. Available at:
http://www.bcbs.com/blueresources/tec/vols/25/proton‐
beam‐therapy‐for.html. Accessed January 10, 2013.
98. Allen AM, Pawlicki T, Dong L, et al. An evidence based
review of proton beam therapy: The report of ASTRO's
emerging technology committee. Radiother Oncol.
2012;103(1):8‐11.
66 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
99. Laurie SA. Malignant salivary gland tumors: Treatment of
recurrent and metastatic disease. Last reviewed
December2012. UpToDate Inc. Waltham, MA.
100. Koch WM, Machtay M. Treatment of early (stage I and II)
head and neck cancer: The larynx. Last reviewed December
2012. UpToDate Inc. Waltham, MA.
101. BrocksteinBE, Stenson KM, Sher DJ. Treatment of
locoregionally advanced (stage III and IV) head and neck
cancer: The larynx and hypopharynx. Last reviewed
December 2012. UpToDate Inc. Waltham, MA.
102. Efstathiou JA, Paly JJ, Lu HM, et al. Adjuvant radiation
therapy for early stage seminoma: Proton versus photon
planning comparison and modeling of second cancer risk.
Radiother Oncol. 2012;103(1):12‐17.
103. Beard CJ. Treatment of stage I seminoma. Last reviewed
December 2012. UpToDate Inc. Waltham, MA.
104. Beard CJ, Oh WK. Treatment of stage II seminoma. Last
reviewed December 2012. UpToDate Inc. Waltham, MA.
105. Finger PT. Choroidal hemangioma. Eye Cancer Network:
New York, NY. 2013. Available at:
http://www.eyecancer.com/patient
/condition.aspx?nid=61&category=choroidal+tumors&
condition=choroidal+hemangioma
(http://www.eyecancer.com/patient
/condition.aspx?nid=61&category=choroidal+tumors&
condition=choroidal+hemangioma). Accessed January 30,
2013.
106. American Society for Radiation Oncology (ASTRO). Use of
proton beam for prostate cancer. ASTRO Position
Statement. Alexandria, VA: ASTRO: February 2013.
107. Eckel F, Brunner T, Jelic S; ESMO Guidelines Working Group.
Biliary cancer: ESMO Clinical Practice Guidelines for
diagnosis, treatment and follow‐up. Ann Oncol.
2011;22(Suppl 6):vi40‐vi44.
108. Meyer RM, Gospodarowicz MK, Connors JM, et al; NCIC
Clinical Trials Group; Eastern Cooperative Oncology Group.
ABVD alone versus radiation‐based therapy in limited‐stage
Hodgkin's lymphoma. N Engl J Med. 2012;366(5):399‐408.
109. National Comprehensive Cancer Network. Clinical practice
guideline: Head and neck cancers (Version 2.2013). NCCN:
67 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Fort Washington, PA. Available at: http://www.nccn.org
/professionals/physician_gls/pdf/head‐and‐neck.pdf
(http://www.nccn.org/professionals/physician_gls
/pdf/head‐and‐neck.pdf). Accessed February 3, 2014.
110. Proton Therapy Guideline Working Group, Guideline
Advisory Group. Proton beam radiation therapy. Edmonton
(AB): Alberta Health Services, Cancer Care; March 2013.
(Clinical practice guideline; no. RT‐002). Available at:
http://www.guideline.gov/content.aspx?id=45375&
search=proton+beam+radiotherapy
(http://www.guideline.gov/content.aspx?id=45375&
search=proton+beam+radiotherapy). Accessed February 3,
2014.
111. Shridhar R, Almhanna K, Meredith KL, et al. Radiation
therapy and esophageal cancer. Cancer Control.
2013;20(2):97‐110.
112. National Comprehensive Cancer Network. Clinical practice
guideline: Hepatobiliary cancers (Version 2.2013). NCCN:
Fort Washington, PA. Available at: http://www.nccn.org
/professionals/physician_gls/pdf/hepatobiliary.pdf
(http://www.nccn.org/professionals/physician_gls
/pdf/hepatobiliary.pdf). Accessed February 3, 2014.
113. National Comprehensive Cancer Network. Clinical practice
guideline: Dermatofibrosarcoma protuberans (Version
1.2014). NCCN: Fort Washington, PA. Available at:
http://www.nccn.org/professionals/physician_gls
/pdf/dfsp.pdf (http://www.nccn.org/professionals
/physician_gls/pdf/dfsp.pdf). Accessed February 3, 2014.
114. Li J, Recinos PF, Orr BA, et al. Papillary tumor of the pineal
region in a 15‐month‐old boy. J Neurosurg Pediatr.
2011;7(5):534‐538.
115. Amsbaugh MJ, Grosshans DR, McAleer MF, et al. Proton
therapy for spinal ependymomas: Planning, acute toxicities,
and preliminary outcomes. Int J Radiat Oncol Biol Phys.
2012;83(5):1419‐1424.
116. Clivio A, Kluge A, Cozzi L, et al. Intensity modulated proton
beam radiation for brachytherapy in patients with cervical
carcinoma. Int J Radiat Oncol Biol Phys. 2013;87(5):897‐
903.
117. Plastaras JP, Berman AT, Freedman GM. Special cases for
68 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
proton beam radiotherapy: Re‐irradiation, lymphoma, and
breast cancer. Semin Oncol. 2014;41(6):807‐819.
118. Plaxe SC, Mundt AJ. Approach to adjuvant treatment of
endometrial cancer. UpToDate Inc., Waltham, MA. Last
reviewed December 2014.
119. Campos SM, Cohn DE. Treatment of recurrent or metastatic
endometrial cancer. UpToDate Inc., Waltham, MA. Last
reviewed December 2014.
120. National Comprehensive Cancer Network. Clinical practice
guideline: Uterine cancer. Version 1.2015. NCCN: Fort
Washington, PA.
121. McDonald MW, Beitler JJ, Busse PM, et al; Expert Panel on
Radiation Oncology‐Head & Neck Cancer. ACR
Appropriateness Criteria® retreatment of recurrent head
and neck cancer after prior definitive radiation [online
publication]. Reston (VA): American College of Radiology
(ACR); 2014. Available at: http://www.guideline.gov
/content.aspx?id=48302&
search=Proton+beam+AND+ependymoma
(http://www.guideline.gov/content.aspx?id=48302&
search=Proton+beam+AND+ependymoma). Accessed
January 30, 2015
122. Mitin T, Zietman AL. Promise and pitfalls of heavy‐particle
therapy. J Clin Oncol. 2014;32(26):2855‐2863.
123. Kieran MW. Ependymoma. UpToDate Inc., Waltham, MA.
Last reviewed December 2014.
124. Greenberger BA, Pulsifer MB, Ebb DH, et al. Clinical
outcomes and late endocrine, neurocognitive, and visual
profiles of proton radiation for pediatric low‐grade gliomas.
Int J Radiat Oncol Biol Phys. 2014;89(5):1060‐1068.
125. Moschovi M, Chrousos GP. Pineal gland masses. UpToDate
Inc., Waltham, MA. Last reviewed December 2014.
126. van den Bent M. Management of anaplastic
oligodendroglial tumors. UpToDate Inc., Waltham, MA. Last
reviewed December 2014.
127. Mendenhall NP, Hoppe BS, Nichols RC, et al. Five‐year
outcomes from 3 prospective trials of image‐guided proton
therapy for prostate cancer. Int J Radiat Oncol Biol Phys.
2014;88(3):596‐602.
128. Ratko TA, Douglas GW, de Souza JA, et al. Radiotherapy
69 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
treatments for head and neck cancer update. Comparative
Effectiveness Review No. 144. Rockville, MD: Agency for
Healthcare Research and Quality (AHRQ); 2014
129. National Comprehensive Cancer Network. Clinical practice
guideline: Prostate cancer. Version 1.2015. NCCN: Fort
Washington, PA.
130. Drolet BA, Trenor CC 3rd, Brandao LR, et al. Consensus‐
derived practice standards plan for complicated Kaposiform
hemangioendothelioma. J Pediatr. 2013;163(1):285‐291.
131. Cao W, Lim G, Liao L, et al. Proton energy optimization and
reduction for intensity‐modulated proton therapy. Phys
Med Biol. 2014;59(21):6341‐6354.
132. Pan HY, Jiang S, Sutton J, et al. Early experience with
intensity modulated proton therapy for lung‐intact
mesothelioma: A case series. Pract Radiat Oncol.
2015;5(4):e345‐353.
133. Kelly KJ, Yoon SS, Kuk D, et al. Comparison of perioperative
radiation therapy and surgery versus surgery alone in 204
patients with primary retroperitoneal sarcoma: A
retrospective 2‐institution study. Ann Surg.
2015;262(1):156‐162.
134. Ahmed SK, Watanabe M, deMello DE, Daniels TB. Pediatric
metastatic odontogenic ghost cell carcinoma: A multimodal
treatment approach. Rare Tumors. 2015;7(2):5855.
135. Ravi V, Patel SR. Desmoid tumors: Systemic therapy.
UpToDate Inc., Waltham, MA. Last reviewed January 2016.
136. Ravi V, Patel SR, Raut CP, DeLaney TF. Desmoid tumors:
Epidemiology, risk factors, molecular pathogenesis, clinical
presentation, diagnosis, and local therapy. UpToDate Inc.,
Waltham, MA. Last reviewed January 2016.
137. Admas D, Frieden IJ. Tufted angioma, kaposiform
hemangioendothelioma, and the Kasabach‐Merritt
phenomenon. UpToDate Inc., Waltham, MA. Last reviewed
January 2016.
138. Lydiatt WM, Quivey JM. Salivary gland tumors: Treatment
of locoregional disease. UpToDate Inc., Waltham, MA. Last
reviewed January 2016.
139. Falkson CB, Vella ET, Yu E, et al. Radiotherapy With Curative
Intent in Patients With Early‐stage, Medically Inoperable,
Non‐Small‐cell Lung Cancer: A Systematic Review. Clin Lung
70 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Cancer. 2016 Oct 27. [Epub ahead of print]
140. Park J, Park Y, Lee SU, et al. Differential dosimetric benefit
of proton beam therapy over intensity modulated
radiotherapy for a variety of targets in patients with
intracranial germ cell tumors. Radiat Oncol. 2015;10:135.
141. Patel AV, Lane AM, Morrison MA, et al. Visual outcomes
after proton beam irradiation for choroidal melanomas
involving the fovea. Ophthalmology. 2016;123(2):369‐377
142. Gilligan TD, Kantoff PW. Diagnosis and treatment of
relapsed and refractory testicular germ cell tumors.
UpToDate Inc., Waltham, MA. Last reviewed December
2016.
143. Ravi V, Patel SR, Raut CP, DeLaney TF. Desmoid tumors:
Epidemiology, risk factors, molecular pathogenesis, clinical
presentation, diagnosis, and local therapy. UpToDate Inc.,
Waltham, MA. Last reviewed December 2016.
144. Ravi V, Patel SR. Desmoid tumors: Systemic therapy.
UpToDate Inc., Waltham, MA. Last reviewed December
2016.
145. Rajkumar SV. Overview of the management of multiple
myeloma. UpToDate Inc., Waltham, MA. Last reviewed
December 2016a.
146. Rajkumar SV. Treatment of relapsed or refractory multiple
myeloma. UpToDate Inc., Waltham, MA. Last reviewed
December 2016b.
147. Romesser PB, Cahlon O, Scher ED, et al. Proton beam
reirradiation for recurrent head and neck cancer: Multi‐
institutional report on feasibility and early outcomes. Int J
Radiat Oncol Biol Phys. 2016;95(1):386‐395.
148. McDonald MW, Zolali‐Meybodi O, Lehnert SJ, et al.
Reirradiation of recurrent and second primary head and
neck cancer with proton therapy. Int J Radiat Oncol Biol
Phys. 2016;96(4):808‐819.
149. National Comprehensive Cancer Network. Clinical practice
guideline: Head and neck cancers. Version 2.2016. NCCN:
Fort Washington, PA .
150. National Comprehensive Cancer Network. Clinical practice
guideline: Multiple myeloma. Version 3.2017. NCCN: Fort
Washington, PA .
151. Vogel J, Berman AT, Lin L, et al. Prospective study of proton
71 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
beam radiation therapy for adjuvant and definitive
treatment of thymoma and thymic carcinoma: Early
response and toxicity assessment. Radiother Oncol.
2016;118(3):504‐509.
152. Parikh RR, Rhome R, Hug E, et al. Adjuvant proton beam
therapy in the management of thymoma: A dosimetric
comparison and acute toxicities. Clin Lung Cancer.
2016;17(5):362‐366.
153. National Comprehensive Cancer Network. Clinical practice
guideline: Thymomas and thymic carcinomas. Ve rsion
3.2016. NCCN: Fort Washington, PA .
154. Canadian Agency for Drugs and Technologies in Health
(CADTH). Proton beam therapy versus photon radiotherapy
for adult and pediatric oncology patients: A review of the
clinical and cost‐effectiveness. Rapid Response Report:
Summary with Critical Appraisal. Ottawa, ON: CADTH; May
20, 2016.
Neutron Beam Therapy:
1. Laramore GE, Krall JM, Griffin TW, et al. Neutron versus
photon irradiation for unresectable salivary gland tumors:
Final report of an RTOG‐MRC randomized clinical trial.
Radiation Therapy Oncology Group. Medical Research
Council. Int J Radiat Oncol Biol Phys. 1993;27(2):235‐240.
2. Russell KJ, Caplan RJ, Laramore GE, et al. Photon versus fast
neutron external beam radiotherapy in the treatment of
locally advanced prostate cancer: Results of a randomized
prospective trial. Int J Radiat Oncol Biol Phys.
1994;28(1):47‐54.
3. Lindsley KL, Cho P, Stelzer KJ, et al. Clinical trials of neutron
radiotherapy in the United States. Bull Cancer Radiother.
1996;83 Suppl:78s‐86s.
4. Krull A, Schwarz R, Brackrock S, et al. Neutron therapy in
malignant salivary gland tumors: Results at European
centers. Recent Results Cancer Res. 1998;150:88‐99
5. Engenhart‐Cabillic R, Debus J, Prott FJ, et al. Use of neutron
therapy in the management of locally advanced
nonresectable primary or recurrent rectal cancer. Recent
Results Cancer Res. 1998;150:113‐124.

72 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
6. Lindsley KL, Cho P, Stelzer KJ, et al. Fast neutrons in
prostatic adenocarcinomas: Worldwide clinical experience.
Recent Results Cancer Res. 1998;150:125‐136.
7. Prott FJ, Micke O, Haverkamp U, et al. Results of fast
neutron therapy of adenoid cystic carcinoma of the salivary
glands. Anticancer Res. 2000;20(5C):3743‐3749.
8. Huber PE, Debus J, Latz D, et al. Radiotherapy for advanced
adenoid cystic carcinoma: Neutrons, photons or mixed
beam? Radiother Oncol. 2001;59(2):161‐167
9. Chou RH, Wilder RB, Wong MS, Forster KM. Recent
advances in radiotherapy for head and neck cancers. Ear
Nose Throat J. 2001;80(10):704‐707, 711‐714, 716 passim
10. Eng TY, Thomas CR, Herman TS. Primary radiation therapy
for localized prostate cancer. Urol Oncol. 2002;7(6):239‐257
11. Airoldi M, Cortesina G, Giordano C, et al. Update and
perspectives on non‐surgical treatment of salivary gland
malignancies. Acta Otorhinolaryngol Ital.
2003;23(5):368‐376.
12. Strander H, Turesson I, Cavallin‐Stahl E. A systematic
overview of radiation therapy effects in soft tissue
sarcomas. Acta Oncol. 2003;42(5‐6):516‐531.
13. Douglas JG, Koh WJ, Austin‐Seymour M, Laramore GE.
Treatment of salivary gland neoplasms with fast neutron
radiotherapy. Arch Otolaryngol Head Neck Surg.
2003;129(9):944‐948.
14. Hassen‐Khodja R, Lance JR. The efficacy of neutron therapy
in the treatment of malignant salivary gland tumors.
Summary. Technology brief prepared for Agence
d’évaluation des technologies et des modes d’intervention
en santé (AETMIS). AETMIS 03‐04. Montreal, QC: AETMIS;
November 2003. Available at:
http://www.aetmis.gouv.qc.ca/
(http://www.aetmis.gouv.qc.ca/). Accessed September 23,
2004.
15. Day TA, Deveikis J, Gillespie MB, et al. Salivary gland
neoplasms. Curr Treat Options Oncol. 2004;5(1):11‐26.
16. Murray PM. Soft tissue sarcoma of the upper extremity.
Hand Clin. 2004;20(3):325‐333, vii.
17. Purins A, Mundy L, Hiller J. Boron neutron capture therapy
for cancer treatment. Horizon Scanning Prioritising

73 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Summary. Adelaide, SA: Adelaide Health Technology
Assessment (AHTA); October 2007.
18. Kankaanranta L, Seppälä T, Koivunoro H, et al. l‐
boronophenylalanine‐mediated boron neutron capture
therapy for malignant glioma progressing after external
beam radiation therapy: A phase I study. Int J Radiat Oncol
Biol Phys. 2011;80(2):369‐376.
19. National Comprehensive Cancer Network. Clinical practice
guideline: Dermatofibrosarcoma protuberans (Version
1.2014). NCCN: Fort Washington, PA. Available at:
http://www.nccn.org/professionals/physician_gls
/pdf/dfsp.pdf (http://www.nccn.org/professionals
/physician_gls/pdf/dfsp.pdf). Accessed February 3, 2014.
20. Martos‐Fernandez M, Alberola‐Ferranti M, Hueto‐Madrid
JA et al. Ghost cell odontogenic carcinoma: A rare case
report and review of literature. J Clin Exp Dent.
2014;6(5):e602‐e606.
21. Li J, Du H, Li P, et al. Ameloblastic carcinoma: An analysis of
12 cases with a review of the literature. Oncol Lett.
2014;8(2):914‐920. Available at:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4081393/
(http://www.ncbi.nlm.nih.gov/pmc/articles
/PMC4081393/).
22. Martos‐Fernandez M, Alberola‐Ferranti M, Hueto‐Madrid
JA, Bescos‐Atfn C. Ghost cell odontogenic carcinoma: A rare
case report and review of literature. J Clin Exp Dent.
2014;6(5):e602‐e606.
74 of 73 5/9/17, 11:20 AM
Proton Beam and Neutron Beam Radiotherapy http://qawww.aetna.com/cpb/medical/data/200_299/0270_draft.html
Copyright Aetna Inc. All rights reserved. Clinical Policy Bulletins are developed by Aetna to assist in administering plan
benefits and constitute neither offers of coverage nor medical advice. This Clinical Policy Bulletin contains only a
partial, general description of plan or program benefits and does not constitute a contract. Aetna does not provide
health care services and, therefore, cannot guarantee any results or outcomes. Participating providers are
independent contractors in private practice and are neither employees nor agents of Aetna or its affiliates. Treating
providers are solely responsible for medical advice and treatment of members. This Clinical Policy Bulletin may be
updated and therefore is subject to change.
Copyright © 2001‐2017 Aetna Inc.
AETNA BETTER HEALTH® OF PENNSYLVANIA
Amendment to Aetna Clinical Policy Bulletin Number: 0270 - Proton Beam and
Neutron Beam Radiotherapy
There are no amendments for Medicaid.
www.aetnabetterhealth.com/pennsylvania revised 05/12/2017