Embed Size (px)
Citation preview

Mimics and chameleons ofoptic neuritis
Dinushi Weerasinghe,1,2 Christian Lueck1,2
1Department of Neurology,The Canberra Hospital,Canberra, Australian CapitalTerritory, Australia2Australian National UniversityMedical School, Canberra,Australia
Correspondence toDr Christian Lueck, Departmentof Neurology, The CanberraHospital, P.O. Box 11,Woden ACT 2606, Australia;[email protected]
Accepted 22 November 2015Published Online First13 January 2016
To cite: Weerasinghe D,Lueck C. Pract Neurol2016;16:96–110.
ABSTRACTOptic neuritis is a common problem and mostneurologists are familiar with it. Recent studieshave suggested that it can be overdiagnosed in asmany as 10% of cases. The major reasons for thisrelate to confusion regarding terminology andlack of familiarity with common mimics. Thisarticle covers typical ‘idiopathic’ demyelinatingoptic neuropathy (IDON) and several possiblevariations in the way it can present (chameleons).We then discuss several conditions that can mimicIDON, including neuromyelitis optica, sarcoidosis,chronic relapsing inflammatory optic neuropathy,anterior ischaemic optic neuropathy, infectious/parainfectious optic neuropathy, neuroretinitis,Leber’s hereditary optic neuropathy, and some‘ocular’ mimics including autoimmune retinopathyand central serous choroidoretinopathy.
INTRODUCTIONOptic neuritis is familiar to all neurolo-gists. It is quite common: in Westerncountries the annual incidence is around5/100 000 population.1 2 Neurologistsare generally conversant with its implica-tions in terms of multiple sclerosis (MS).The problem is that it can be overdiag-nosed. A recent study found that 10% ofpatients referred to a dedicated opticneuritis clinic had other diagnoses.3
Conversely, it can present in someunusual ways that may cause confusion.Accurate diagnosis is important to
ensure patients receive appropriate treat-ment and prognostic information.Evidence from the optic neuritis treat-ment trial suggests that corticosteroidsmake little difference to the eventualoutcome of the optic neuritis associatedwith MS.2 However, this does not applyto many of the other causes of opticneuritis that may well require corticoster-oid (or other) therapy.4
Space does not allow discussion of allpossible differential diagnoses. Instead,we first discuss variations in presentation
that might cause confusion (‘chame-leons’). We then discuss a selection ofalternative diagnoses (‘mimics’) that areclinically important because their man-agement is very different. We finish witha summary to provide suggestions onpatient management in this difficult area.
Idiopathic demyelinating optic neuritisFirst, a note about terminology. ‘Opticneuritis’ simply means inflammation ofthe optic nerve and, strictly speaking,covers all inflammatory causes. We willuse the term ‘idiopathic demyelinatingoptic neuritis’ (IDON) to denote the con-dition which neurologists recognise asassociated with MS but which can also beseen as a clinically isolated syndrome.i
IDON is the presenting symptom inabout 25% of cases of MS and occurs atsome point in 70% of all patients withMS.2 5 In spite of recent developments inimaging technology, the diagnosis remainsa clinical one. It is, strictly speaking, a diag-nosis of exclusion and is a retrospectivediagnosis that cannot be made at the timeof presentation. MRI and optical coherencetomography provide diagnostic support,assist with prognosis and exclude mimics,but they do not make the diagnosis itself.6
In its broadest sense, the differentialdiagnosis of IDON is enormous (box 1).However, most of the conditions in box 1are unlikely to cause confusion inday-to-day neurological practice. We willconfine ourselves to discussing potentialmimics (highlighted in dark red) that wethink could cause confusion in a generalneurology clinic. But first, the chameleons.
iOf course, if ‘IDON’ occurs in a patient with adiagnosis of MS the adjective ‘idiopathic’ is notreally appropriate. Nevertheless, it is difficult tofind a label for the optic neuritis that occurs eitheras an isolated entity or as a feature of establishedMS, even though these entities are considered to bethe same. It is hoped that the reader will bear withour use of ‘IDON’.
REVIEW
96 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

Box 1 Potential mimics of ‘optic neuritis’
Many of these conditions are very unlikely to be confused with idiopathic demyelinating optic neuritis (IDON) as their presenta-tion will be atypical (eg, too slow), or there will be other, disease-specific, clinical features present. Nevertheless, the conditionshave the potential to cause apparently isolated involvement of the optic nerve(s) which could result in diagnostic difficulty. Thelist has been compiled from a number of published sources.3 32 67 68 Highlighted items in dark red are discussed in detail in thetext.
Inherited▸ Leber’s hereditary optic neuropathy▸ Other inherited optic atrophies (eg, OPA1, OPA3, Wolfram/DIDMOAD)
InfectiousDirect involvement of optic nerve or involvement of adjacent structures (eg, sinusitis, orbital cellulitis or meningitis)▸ Viral (adenoviruses, cytomegalovirus, Coxsackie, dengue, enteroviruses, Epstein-Barr virus, hepatitis A & B, HIV type 1,
Herpes simplex virus 1 and 2, influenza B, measles, mumps, rubella, rubeola, Varicella zoster virus, HHV, HTLV1, WestNile virus)
▸ Rickettsial (Mediterranean spotted fever, typhus, scrub typhus)▸ Bacterial (Bacillus anthracis, Bartonella henselae, β-haemolytic streptococci, Bordatella pertussis, Borrelia burdorferi,
brucellosis, Coxiella burneti, Treponema pallidum, Mycobacterium tuberculosis, Mycoplasma pneumoniae, Neisseriameningitidis/any cause of bacterial meningitis, Salmonella typhi, Tropheryma whipplei)
▸ Invasive fungal disease (aspergillus, candida, coccidioides, cryptococcus, mucor)▸ Parasites (angylostrongyliasis, cysticercosis, toxocara, toxoplasma, intraocular nematode infection)
Inflammatory/reactive/autoimmune▸ Inflammatory demyelinating optic neuropathy/multiple sclerosis▸ Neuromyelitis optica spectrum disorders (anti-NMO, anti-MOG antibodies)▸ Autoimmune optic neuropathy (systemic lupus erythematosus, inflammatory bowel disease, rheumatoid disease,
coeliac disease, Sjögren’s syndrome, mixed connective tissue disease, scleroderma, Churg-Strauss syndrome, granulo-matosis with polyangiitis (Wegener’s), polyarteritis nodosa)
▸ Sarcoidosis▸ Behçet’s disease▸ Paraneoplastic (small cell lung cancer, anti-CRMP-5 antibodies)▸ Acute disseminated encephalomyelitis▸ Chronic relapsing inflammatory optic neuropathy▸ Postinfectious/postvaccination▸ Orbital pseudotumour (Tolosa-Hunt syndrome)▸ Posterior scleritis▸ Optic perineuritis▸ Neuroretinitis▸ Acute zonal outer occult retinopathy, acute idiopathic blind spot enlargement, multiple evanescent white dot syndrome
and related chorioretinal disorders▸ Autoimmune retinopathies (including cancer-associated and melanoma-associated retinopathy)
Vascular/arteritic/ischaemic▸ Anterior ischaemic optic neuropathy:
○ Arteritic (giant cell arteritis, polyarteritis nodosa)○ Non-arteritic
▸ Posterior ischaemic optic neuropathy▸ Malignant hypertension▸ Pituitary apoplexy▸ Radiation optic neuropathy▸ Retinal vasospasm▸ Susac’s syndrome▸ Diabetic papillopathy
Toxic/nutritional▸ B12 deficiency▸ Folate deficiency▸ Copper deficiency
REVIEW
Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254 97
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

CHAMELEONSClinical features of typical IDONAccurate diagnosis relies on a thorough history.Likewise, general and neurological examinations arecritical, including careful examination of the ocularfundus (with pupillary dilatation if necessary). An MRscan of the brain and orbits is useful in most cases toexclude other diagnoses and assist with prognosis. Asabove, however, the diagnosis of IDON is clinical andcan only be made retrospectively. When first seen, it isappropriate to make a tentative diagnosis of IDON ifa patient displays all the typical features of IDON(box 2). However, the patient must be followed up toensure that there is improvement and that no atypicalfeatures have developed. If any atypical featuresappear, the clinician must consider alternative diagno-ses (with appropriate investigation).A typical case of IDON7 8 (box 2) presents with
subacute onset of unilateral visual loss preceded bydull pain around or behind the eye. The pain isusually not distressing but is often worsened by eyemovement. The extent of visual loss is variable, butthe nadir is generally reached within a few days fromonset. Patients typically report disturbed colourvision, visual blurring, reduction in acuity or frank
visual loss. About three quarters of patients arefemale.8 Spontaneous visual recovery is almost univer-sal, typically starting within 4 weeks of symptomonset. The prognosis is usually very good, regardlessof treatment.2 9
▸ Tobacco/alcohol amblyopia▸ Implant (cobalt)▸ Methanol, ethylene glycol, solvents, lead▸ Drugs (eg, ethambutol, isoniazid, amiodarone, linezolid, etc)▸ Bariatric surgery
Compressive optic neuropathy/malignancy▸ Thyroid eye disease▸ Aneurysm▸ Orbital myositis▸ Mucocele▸ Paget’s disease, fibrous dysplasia, thalassaemia▸ Optic nerve sheath meningioma▸ Optic nerve glioma▸ Orbital tumour (primary or secondary)▸ Intracranial tumour (pituitary, craniopharyngioma)▸ Tuberculoma▸ Leukaemia/lymphoma▸ Retinoblastoma
Miscellaneous▸ Central serous chorioretinopathy▸ Other ophthalmic disorder (uveitis, other maculopathies, refractive error, optic disc drusen, glaucoma, cone/rod
dystrophy)▸ Traumatic optic neuropathy▸ Acute papilloedema▸ Bee and wasp stings▸ Functional
DIDMOAD, diabetes insipidus, diabetes mellitus, optic atrophy and deafness; HHV, human herpes virus; HTLV, human Tcell lymphotropic virus; MOG, myelin oligodendrocyte glycoprotein; NMO, neuromyelitis optica; OPA1, OPA3, optic atrophygenes.
Box 2 Typical features of idiopathic demyelinatingoptic neuritis
▸ Pain around the eye, usually worse on eye movementand starting before or with visual loss
▸ Unilateral visual loss developing over hours to a fewdays, ranging in severity from loss of colour vision,through blurring of vision, loss of central vision tocomplete visual loss
▸ Reduction of colour vision, visual acuity, contrastsensitivity
▸ Loss of visual field▸ Relative afferent pupillary defect▸ Normal fundus, apart from optic disc swelling in a
third of cases▸ Evidence of visual improvement by 4 weeks from
onset.
REVIEW
98 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

Examination at presentation typically finds reducedvisual acuity and/or contrast sensitivity in the affectedeye, reduced colour vision, loss of visual field and arelative afferent pupillary defect. The optic disc isnormal in two-thirds of cases, but there may be discswelling.8
A few additional features can still be regarded as‘typical’, including:▸ A history of MS (33% of cases).8
▸ Phosphenes/photopsias (flashes of light), often provokedby eye movement (30% of cases).8
▸ Optic disc swelling (36% of cases).8
▸ Mild posterior uveitis or periphlebitis (up to 6% ofcases).8
▸ Several additional symptoms in the recovery phase,9 forexample:– Uhthoff ’s phenomenon (transient deterioration of
vision with heat or exercise).– Pullfrich’s phenomenon (disturbance in perception of
depth of moving objects).
Variation in painAbout 10% of patients have no pain at all.7 9 If thereis pain, it is usually mild, but 12% of patients havesuch severe pain that it wakes them from sleep. Thepain can be continuous or intermittent and is usuallyexacerbated by eye movement. A minority of patientshas intermittent pain unrelated to eye movements.8
Loss of vision may coincide with pain onset or bedelayed by a few hours to days.
Variation in disease courseDeterioration in visual loss rarely continues beyond7–10 days. Ongoing deterioration after 2 weeksshould prompt consideration of another diagnosis.10
Recovery should begin by the 4th week but may con-tinue for up to a year.11
Variation in visual acuity, colour vision and visual field lossVisual acuity at presentation can range from betterthan 6/6 (10%) to no light perception (3%) with mostpatients having an acuity between 6/7.5 and 6/60.8
Visual acuity (as measured by a standard Snellenchart) measures high-contrast visual discrimination.However, in IDON low-contrast visual acuity is moreaffected than high-contrast acuity so contrast sensitiv-ity may be abnormal even when the Snellen acuity isnormal. Contrast sensitivity is easily tested using aPelli-Robson chart or low-contrast Sloan letter chart.In the optic neuritis treatment trial, 97% of patientshad abnormal contrast sensitivity even though only88% had impaired visual acuity on standard clinicaltesting and contrast sensitivity was impaired in 88%of patients with normal visual acuity.12 Overall, abnor-mal contrast sensitivity was the most sensitive test ofvisual dysfunction.12 It is worth considering measur-ing contrast sensitivity in all patients with suspectedIDON.
Colour vision is affected in almost all patients to avarying degree, even in those who still have a normalvisual acuity.13 During the acute phase of optic neur-itis, blue/yellow defects are the most common. Atrecovery, red/green defects are more common.13
The pattern of visual field loss is very variable. Atpresentation, two-thirds of patients have diffuse visualfield loss, predominantly central or affecting theentire visual field. However, a third have a localiseddefect that can take several forms (eg, paracentral,hemianopic, arcuate or altitudinal).14 15 Hence, thepattern of loss does not distinguish IDON from otherconditions.15 Interestingly, with careful assessment thefellow (ie, ‘uninvolved’) eye at presentation has minorvisual field abnormalities in 75% of clinically unilat-eral cases.15
Variation in ocular examinationOcular examination is typically normal in IDON.However, there may be optic disc swelling (papilli-tis) if the optic nerve inflammation is anterior.Patients with retrobulbar IDON are over twice aslikely to go on to develop MS than patients withpapillitis.16 Perivenous sheathing, if present, increasesthe future risk of MS.17 Very occasionally, there area few peripapillary haemorrhages, retinal exudatesand/or cells in the vitreous8 but finding these, orany other abnormality, on funduscopy shouldprompt a search for another underlying cause (seebelow). Optic disc pallor typically develops overseveral weeks; its presence at presentation impliespre-existing disease.
Variation in pupil responsesA relative afferent pupillary defect (RAPD) occurs inthe affected eye provided the involvement is unilat-eral, or unequal if both eyes are involved. An RAPD iscommon to all optic neuropathies irrespective ofcause and simply reflects differential input to thecentral mechanisms that control pupil size: if botheyes are equally affected, there is no RAPD. Bilateral,symmetrical, optic nerve involvement does occur inIDON but strongly suggests another cause.
Variation in MRI findingsAbnormalities in brain MRI have relatively little influ-ence on the diagnosis of IDON compared with theirimplications for prognosis. Patients with neuromyelitisoptica (NMO) are more likely than patients withIDON to have a normal brain MRI scan at presenta-tion,18 but the absolute number of patients withNMO is sufficiently small that the scan does notreally influence diagnosis (which remains clinical, asabove). Prognosis is a very different matter: a patientpresenting with IDON whose MRI is entirely normalat baseline has a 25% chance of going on to developMS over the next 15 years.16 Increasing numbers oflesions on the baseline MRI are associated with
REVIEW
Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254 99
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

progressively increasing risk of developing MS at15 years: 78% with three or more lesions.16
The optic nerve may appear normal or abnormal onMRI at baseline. In IDON, abnormalities are typicallyfocal, confined to one segment, and more likely to beanterior.19 Long lesions, posterior lesions and lesionsinvolving the optic chiasm or tract should prompt asearch for an alternative diagnosis.18 19
A comment on cerebrospinal fluid findingsLumbar puncture is relatively rarely performed now-adays in patients with typical IDON as it is not neces-sary for diagnosis and adds little to MRI forprognosis. A mild lymphocytic pleocytosis of up to 30cells/mm3 develops in about a third of patients.20
Similarly, oligoclonal bands restricted to the cerebro-spinal fluid (CSF) occur in 30–70% of patients: theirpresence significantly correlates with the presence ofabnormalities on brain MRI scans. Unadjusted for theMRI, finding oligoclonal bands slightly increases therisk of developing MS at 2 years but this becomes non-significant after adjustment for MRI abnormalities.20
MIMICSBox 1 shows the large number of conditions that canaffect the optic nerve and so, in theory, be confusedwith IDON. However, distinguishing most of thesefrom IDON is often not difficult because the clinicalpresentation is not that of typical IDON (box 2).Many patients with other diagnoses have systemic fea-tures that prompt consideration of alternative diagno-ses. For example, a strong family history of visual lossor finding bilateral optic disc pallor should suggest aninherited disorder. A recent history of infectiousillness raises the possibility of an infectious or postin-fectious cause, and there are often clues to the pres-ence of a toxic or metabolic cause in the history.Similarly, imaging is likely to detect most structural,that is, compressive, abnormalities. As a result, mostof these conditions do not generally present aproblem to neurologists and we will not discuss themfurther.It is more useful to consider those conditions that
have a reasonable chance of being misdiagnosed asIDON in day-to-day neurological practice. Box 1highlights the conditions that we feel merit discussion.
Neuromyelitis optica spectrum disordersNMO is much less common than MS (perhaps 1% ofoptic neuritis is due to NMO)3 but their pathophysi-ology is significantly different.21 Unlike MS, NMOrequires immunosuppressive therapy. Also, treatingpatients with NMO with β-interferon may increasethe relapse rate.22 The question therefore arises as towhich patients should be screened by testing forserum antiaquaporin antibodies.Clinical features offer little help. There is no signifi-
cant difference in pain or the incidence of papillitis.19
Patients with NMO are, however, more likely to havebilateral optic neuritis at presentation and to presentwith worse visual acuities.18 There is a suggestion thatthere is greater thinning of the retinal nerve fibrelayer in NMO on optical coherence tomography butthis difference does not separate the conditions clinic-ally at the time of presentation.23 24
MRI is more helpful. MRI of the brain is much lesslikely to be abnormal in NMO-related optic neuritisthan in IDON18 and there are significant differenceson MRI of the optic nerve: NMO lesions tend to belongitudinally extensive (>17.6 mm) and to involve atleast three optic nerve segments, whereas IDON/MSlesions tend to be focal in one segment and typicallyoccur anteriorly.25 An enhancing lesion of >40 mm inlength is much more likely to be associated withNMO than with IDON and/or MS.19 The opticchiasm and tract can be affected in NMO but are notgenerally affected in MS.18
Antibodies to myelin oligodendrocyte glycoprotein(MOG) have recently been identified in patients withNMO-spectrum disorder who are antiaquaporin anti-body negative.26 27 Anti-MOG positive patients typic-ally present with bilateral optic neuritis and have apropensity to relapse. Pain at onset is not uncommon,as is a history of prodromal infection. Transverse mye-litis is rare. Most patients have abnormal optic nerves(often longitudinally extensive) on T2-weighted MRIscans, but chiasmal and optic tract involvement israre. Oligoclonal bands are not present. The conditionis usually corticosteroid-responsive and sometimescorticosteroid-dependent.26 27 This condition has abetter prognosis than NMO.
Comment: Patients presenting with optic neuritisshould be tested for antiaquaporin antibodies if thebrain MRI is atypical for MS, the onset was bilateralor severe, the optic neuritis was recurrent, recoverywas poor, or there was evidence of coexisting auto-immune disease.28 This also applies to patients whohave extensive and/or more posterior disease of theiroptic nerves on MRI. It is appropriate to test a patientwith bilateral onset of optic neuritis for anti-MOGantibodies.
SarcoidosisOcular involvement in sarcoidosis is relativelycommon (20%) but anterior visual pathway involve-ment occurs in only 1–5%.29 Nevertheless, opticnerve involvement is a common presentation of neu-rosarcoidosis.30 31 It is relatively straightforward todiagnose sarcoid optic neuropathy if the patient isalready known to have sarcoidosis. However, manycases of sarcoid optic neuropathy occurring in theabsence of known sarcoidosis are mislabelled asIDON.29 31
Sarcoid optic neuropathy presents at a mean age of40 years (range 25–75 years) and is more common inwomen. Only 25% are unilateral but two-thirds of
REVIEW
100 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

patients have an afferent pupillary defect. Ocular painoccurs in about 10% and a similar number describephotopsias. Visual loss may be subacute, sometimesevolving over several months. Visual acuity at presen-tation ranges from 6/7.5 to no light perception, butacuities of 6/18 or worse are common. Colour visionis frequently impaired and, like IDON, there aremany possible different patterns of visual field loss.Over 50% have optic disc pallor at presentation, butseveral other abnormalities are common includingdisc swelling, periphlebitis and granuloma; only 10%have truly normal fundi.29 31 32
Patients may have evidence of anterior uveitis orother features of sarcoidosis (eg, lacrimal glandenlargement), but this is by no means the rule.29
Investigation with serum ACE, chest X-ray, galliumscan, lumbar puncture and MR scanning generallyyields the diagnosis; optic nerve biopsy is a last resort.Optic nerve enhancement along its entire length, withenhancement of the meninges or other cranial nerves,strongly suggests sarcoidosis.29 31 Patients mayrespond to corticosteroids, but often relapse on cessa-tion and many patients deteriorate to acuities of 6/60or worse.30
Comment: Unlike IDON, sarcoid optic neuropathyrequires immunosuppressive treatment.4 31 Clinicalexperience suggests that the long-term outcomeimproves with early and aggressive treatment, so it isimportant to detect these patients. This is relativelystraightforward if the patient already has a diagnosisof sarcoidosis. If not, pointers that might suggest itare racial origin, bilateral optic nerve involvement,relatively slow speed of onset, more severe visual loss,abnormalities on fundal examination and extensiveinvolvement of the optic nerve(s) (or other centralnervous system abnormalities) on MRI.
Chronic relapsing inflammatory optic neuropathyThis is rare33 34 but it is important that clinicians areaware of its existence as the management is very dif-ferent from that of IDON.ii
The mean age of onset is 36 years (range 14–69years).34 Patients often develop loss of vision to 6/60or worse. Pain at onset is typical but not universal; ifpresent, the pain is often more severe than the painin IDON. Unilateral onset is the norm but both eyesare usually affected ultimately. Optic disc swelling atpresentation is common. Importantly, there is usuallya dramatic response to high-dose corticosteroidsfollowed by a relapse a few days to a few weeksafter the end of treatment. Relapses are usually
corticosteroid-sensitive, but they continue to recur sopatients end up on low-dose maintenance therapy.33
The final visual acuity is, overall, worse than that ofIDON, and there is a strong suggestion that earlier,more aggressive treatment with corticosteroids gives abetter outcome.32 34
Investigation typically finds normal brain imagingbut the optic nerves are abnormal on MRI, withincreased T2 signal and contrast enhancement.Oligoclonal bands are not present in CSF and tests forother causes of optic neuritis, including anti-NMOantibodies, are negative.34 35
Comment: Unlike IDON, this condition is verycorticosteroid-responsive and the ultimate visual acuityat outcome may depend upon early and aggressivetreatment. Unfortunately, it can only be diagnosedafter there is a relapse following corticosteroid with-drawal. More severe pain and visual loss at onsetsuggest that the diagnosis might ultimately be chronicrelapsing inflammatory optic neuropathy. Such patientsshould be treated with high-dose corticosteroids withclose follow-up after stopping treatment. One reportdescribed recovery of vision to 6/6 following cortico-steroid therapy after 4 years of being registered blind.4
Anterior ischaemic optic neuropathyThis involves infarction of nerve fibres in the regionof the optic disc through interruption in the bloodsupply from small vessels, typically the short ciliaryarteries. It may be non-arteritic or associated with vas-culitis, most commonly giant cell arteritis.36
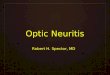
Non-arteritic anterior ischaemic optic neuropathy(NA-AION) usually presents (often on awakening) assudden, painless visual loss in one eye associated withswelling of the optic disc, though the vision may con-tinue to worsen for the first few days. It typicallyoccurs in patients with small, crowded optic discswith a small physiological cup: the unaffected felloweye may show these features, known as a ‘disc at risk’(figure 1). Visual acuity varies from normal to noperception of light, but most patients have acuities of6/60 or better. Visual fields may show arcuate scotoma,altitudinal field loss or global field loss. Disc swellingresolves over 2–3 months, often leaving residual discpallor. Visual acuity may improve with time but mostpatients are left with residual visual impairment.In addition to a crowded optic disc, risk factors for
NA-AION include hypertension, diabetes mellitus,smoking, other vascular disease, and obstructive sleepapnoea. Hypercoagulability is a rare association, andsome medications are implicated, including amiodar-one, vasoconstrictors and phosphodiesterase-5 inhibi-tors. The fellow eye becomes affected in 12–15% overthe next 5 years. There is no specific treatment but itis essential to exclude the possibility of arteritic anter-ior ischaemic optic neuropathy (A-AION).
iiSome authors refer to another entity termed ‘relapsinginflammatory optic neuropathy’. In our view, this is unhelpful as itis purely descriptive and potentially implies an independentpathophysiological entity. Relapses can occur in many of theconditions in table 1.
REVIEW
Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254 101
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

A-AION occurs most commonly in the context ofgiant cell arteritis. Most patients have typical clinicalfeatures, but about 25% do not (so-called ‘occult’giant cell arteritis).36 Like NA-AION, there is typicallysudden onset of painless monocular visual loss,though this is preceded by transient visual loss overthe previous week or two in up to 10% of patients.Serum C reactive protein and/or erythrocyte sedimen-tation rate are elevated in 97% of biopsy-provencases. Untreated, the other eye becomes involved in50% of cases within days to weeks, meaning that thisis a medical emergency requiring accurate diagnosisand treatment with high-dose corticosteroids.Apart from the clinical features of giant cell arteritis
listed above, pointers to the possibility of A-AIONinclude previous transient visual loss, the lack of adisc-at-risk in the fellow eye, pallor of the swollendisc (figure 2), profound visual loss, an elevated plate-let count and delayed choroidal perfusion and/orischaemia on a fluorescein angiogram.
Comment: This is a very important differential diag-nosis of optic neuritis. Though non-arteritic AION(NA-AION) most commonly occurs in patients overthe age of 50 years, it can occur in younger patientswhen it is commonly mislabelled as IDON. Detecting‘occult’ giant cell arteritis (ie, NA-AION) can also bedifficult. Either of these misdiagnoses has importantimplications. The key ‘red flags’ that suggest that thisis not IDON are lack of pain, sudden onset, pale opticdisc swelling, a disc-at-risk in the fellow eye, and lackof improvement with time. Most neurologists areaware of the significance of giant cell arteritis, butmany are unaware of the prevalence of ‘occult’ giantcell arteritis. It is important to maintain a high indexof suspicion at all times.
Infectious/parainfectious optic neuropathyMany infectious organisms can affect the optic nerve,either directly or as a parainfectious phenomenon.
Parainfectious optic neuropathy is much morecommon and can arise from either immunologicallymediated demyelination of the optic nerve or, alterna-tively, from inflammation of the vasculature at theoptic disc (ie, neuroretinitis, see below).The list of possible organisms is enormous (box 1).
Most often, the clinician is alerted to a possible para-infectious cause because the patient presents with pro-dromal systemic symptoms. However, this prodromeis not always that obvious and clinicians must have aparticularly high index of suspicion in patients whoare diabetic, immunosuppressed, or in those whocome from (or are living in) developing countries.Parainfectious optic neuritis typically follows theprimary illness within 1–3 weeks. A viral cause ismuch more common than a bacterial one and itoccurs more commonly in children. Bilateral involve-ment is frequent and the illness may affect other partsof the nervous system (eg, cerebellitis or meningo-encephalitis). Optic disc swelling can occur. In somecases optic disc swelling occurs without either demon-strable functional impairment of the optic nerve orraised intracranial pressure—this is known as opticperineuritis (or perioptic neuritis).37 The time courseof parainfectious optic neuritis is typically similar tothat of IDON and the prognosis is usually good.38
If possible, the causative organism should be identi-fied as the patient may require specific treatment (eg,HIV, mycoplasma, syphilis or tuberculosis).Unfortunately, it is not always possible to identifythe causal organism; the search must be guided by theclinical context. A detailed discussion is beyond thescope of this article and the interested reader isreferred elsewhere.39
Figure 1 Small, crowded optic disc (‘disc-at-risk’). Note thelack of optic cup.
Figure 2 Pallid disc swelling in a 79-year-old man presentingwith severe left visual loss, no other symptoms apart fromweight loss over 6 months, and normal serum C reactive proteinand erythrocyte sedimentation rate (occult giant cell arteritis).
REVIEW
102 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

Direct infection of the optic nerve can occur byextension from adjacent meningitis or orbital disease.This situation is not always obvious clinically butpatient outcome may be critically influenced by earlyconsideration of unusual organisms. This particularlyapplies to fungal disease, which is frequently fatalunless patients start appropriate treatment veryearly.40 Fungi should always be considered in patientswho are diabetic or immunosuppressed who developmeningitis or disease in their nasal sinuses/orbits.There are case reports of patients who presented withisolated optic nerve involvement from aspergillus41 ormucor42 before orbital disease appeared. Such patientshave been treated with corticosteroids for ‘optic neur-itis’ before the diagnosis became obvious.41
Comment: This is a very difficult area without abso-lute guidelines. It is not appropriate to screen everypatient for an underlying infectious aetiology but it isimportant not to miss one if it exists. Clues to the factthat infection needs to be considered are a recent‘infectious’ illness, known diabetes mellitus orimmunosuppression, local disease of the orbit, nasalsinuses or meninges, or continued deterioration invision. Imaging (particularly with MRI) may showoptic nerve thickening or other clues to the fact thatthis is not IDON, but this is not always the case in theearly stages.
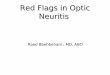
NeuroretinitisIn neuroretinitis, lipid-rich fluid leaks from inflamedblood vessels at the optic disc into the surroundingretina.43 The fluid accumulates and leads to depositsunder the retina in a radial (star) pattern because ofthe anatomy of the outer plexiform layer. Visual lossis predominantly due to maculopathy rather thanoptic nerve dysfunction. Neuroretinitis is classifiedinto three broad categories: (1) idiopathic, (2) asso-ciated with infection (most commonly cat-scratchfever due to Bartonella henselae but there are reportsof many other causative organisms32), and (3) inflam-matory but non-infectious (eg, sarcoidosis or polyar-teritis nodosa).44
Patients usually present with unilateral, painless,subacute visual loss over several days. Over half have arecent history of upper respiratory tract infection orflu-like illness. Visual acuity varies between normaland light perception only but the acuity is generallybetween 6/18 and 6/60. Visual fields typically show acentral or centrocaecal scotoma. There may or maynot be a RAPD.In the earliest stages, the only funduscopy abnor-
mality is a swollen optic disc, possibly with peripapil-lary haemorrhage. There may be peripapillary serousretinal detachment and macular thickening but theseare much more obvious on optical coherence tomog-raphy. The typical star pattern of exudates (figure 3)take 9–12 days to appear, by which time the disc is
usually less swollen. The exudates resolve after severalmonths sometimes leaving residual pigmentationaround the macula. The disc swelling typically settlesafter 2–3 months but there may be mild residual opticatrophy. The prognosis is good: 90% of patientsregain vision of 6/12 or better, but a small number donot recover well, possibly due to vasculitic infarcts atthe optic disc.Neuroretinitis is not associated with MS though
there are reports of it in patients with MS. High-dosecorticosteroids may be a treatment of choice for idio-pathic neuroretinitis but patients with an infectiouscause need appropriate antibiotics.44
Comment: Neuroretinitis in the early stages mayresemble papillitis due to IDON. A history of preced-ing symptoms of infectious illness, the absence ofpain, and subretinal oedema around the disc shouldraise suspicion, though subretinal oedema may onlybe visible on optical coherence tomography. Thetypical macular star may not appear for 2 weeks afteronset so it is important to review the patient early toensure that this diagnosis is not missed.There are other causes of a macular star combined
with disc swelling, the most important being hyper-tensive retinopathy (box 3). The combination mayoccur in other conditions such as diabetic papillopa-thy, anterior ischaemic optic neuropathy, and evenpapilloedema, but the clinical features should serve toseparate out these conditions.
Leber’s hereditary optic neuropathyLeber’s hereditary optic neuropathy (LHON) iscaused by mutations of mitochondrial DNA, the threemost common mutations being at 11770, 3460 and14484. It is maternally inherited but, for reasons thatare still not clear, manifests much more commonly inmen. Symptom onset is usually at age 15–35 years,(range 2–87 years).45 A typical presentation is with
Figure 3 Postviral neuroretinitis showing macular star.
REVIEW
Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254 103
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

painless, subacute loss of central vision, usually to6/60 or worse, with relatively little recovery. This isfollowed by similar involvement of the other eye,usually within 2–3 months, leaving the patient func-tionally blind. At the time of visual loss, the optic discappears swollen with peripapillary telangiectasia butusually without leakage on a fluorescein angiogram.Most cases, paradoxically, have no RAPD.45 The opticdiscs eventually become atrophic and pale.From a clinical perspective, up to 20% of patients
with LHON report ocular pain or pain on eye move-ment, and some even describe Uhthoff ’s phenom-enon.46 Patients (particularly those with the 14484mutation45) may significantly improve after manymonths so it is easy to see how these patients can bemisdiagnosed as having optic neuritis47 (box 4).To complicate matters, LHON and MS coexist 50
times more frequently than expected by chance48 andpatients with LHON, particularly women, may havebrain MRI appearances indistinguishable from MS.49
Indeed, patients with LHON may develop clinical fea-tures typical of relapsing remitting MS.46 48
Comment: Even though it is rare, it is worth remem-bering LHON as a possible differential diagnosis inpatients presenting with optic neuritis, particularly inmen and especially if there is minimal RAPD or ifthere has been bilateral sequential visual loss. Taking adetailed family history may help, as may fluoresceinangiography if this can be done at the time of visualloss.
‘Ocular’ mimicsSome patients have a retinal disorder that can mas-querade as IDON. This is particularly likely if theretina appears normal, or almost normal. Neurologistsmust be aware that these conditions exist and if
necessary seek help from an ophthalmologist orneuro-ophthalmologist. It is also worth bearing inmind that primary macular disorders can occasionallybe missed (even by ophthalmologists!) and referred tothe neurology clinic in error.
Acute zonal occult outer retinopathy and relatedconditionsMany neurologists are unfamiliar with these rare con-ditions. Acute zonal occult outer retinopathy is anidiopathic condition characterised by focal degener-ation of photoreceptors.50 51 There are several otherchorioretinal diseases with visual loss of uncertainorigin, including multiple evanescent white dot
Figure 4 (A) Gross optic disc swelling in a patient’s left eyeshowing partial macular star (arrows). (B) Optical coherencetomogram showing subretinal fluid at the left macula. (C)Optical coherence tomogram of the normal right macula.
Box 3 Hypertensive retinopathy
A 47-year-old man presented with sudden onset of pain-less visual loss in his left eye. His visual acuity was 6/24and funduscopy demonstrated a swollen optic disc withhaemorrhages and a macular star. There was submacularfluid on his optical coherence tomography (figure 4). Hisblood pressure was 220/130 mm Hg. He ultimatelyrequired five antihypertensive agents to bring his bloodpressure under control.
Comment: This case had a number of features that wereunusual for idiopathic demyelinating optic neuritis(IDON)—the unilateral visual loss was sudden and pain-less and, of course, the blood pressure was grossly ele-vated. It is important to remember to measure theblood pressure in patients presenting with visual loss.Also, this case is a good reminder that not all macularstars are due to neuroretinitis.
REVIEW
104 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

syndrome, acute idiopathic blind spot enlargement,acute macular neuroretinopathy, punctuate inner chor-oidopathy, multifocal choroiditis and acute macularneuroretinopathy.Patients with acute zonal occult outer retinopathy
typically present with a scotoma, usually with photo-psias, and may have involvement of central vision.Three quarters of patients are female and the averageage is 37 (13–86) years. There may be photophobiaand/or difficulty with night vision. One or both eyesmay be affected. Visual acuities range from 6/6 to 6/60. At least 20% have a RAPD. Visual fields typicallyshow blind spot enlargement, often with a centralscotoma, but there may be other visual field defects.Fundal examination is normal in 75% of cases butmay show patches of atrophy of the retinal pigmentepithelium or pigment clumping with time.51 52
About a fifth of patients have a history of immune-mediated inflammatory systemic disease (particularlythyroid disease).Electroretinography (ERG) is abnormal in 99% of
cases.52 Detailed ophthalmic investigation shows atypical pattern of abnormalities in areas of involvedretina. Optical coherence tomography shows a diffuseloss of photoreceptors, often sparing the fovea, withabnormalities on autofluorescence and, subsequently,fluorescein angiography.51 Visual loss typically dete-riorates for a few months but stabilises by 6 months.A quarter of patients experience subsequent improve-ment but there is no established treatment.52
There is a strong suspicion that multiple evanescentwhite dot syndrome may be the result of a viral infec-tion, as many patients have a prior ‘flu-like’ illness butits cause remains unknown. Patients are typicallyyoung (mean age 28 years) and the vast majority arefemale. Patients present with acute unilateral visualloss; visual acuity is typically reduced to 6/12 to 6/60with patchy visual field loss. Fundal examinationshows numerous white lesions in the retina (‘dots’ and‘spots’, 100–200 mm in diameter) (figure 5),53 whichevolve over time. There may also be venous sheathingand/or cells in the posterior vitreous. Patients mayhave a RAPD. Fluorescein angiography shows typicalabnormalities. Recovery generally occurs over2–4 months: visual outcome is typically good butsubtle abnormalities of the retinal pigment epitheliumremain.54
Acute idiopathic blind spot enlargement can oftenbe misdiagnosed as IDON.55 Like acute zonal occultouter retinopathy, patients are often younger womenwho report loss of vision that may be quite sudden inonset. Over half have positive visual phenomena.55 56
Mild reduction in visual acuity is typical and
Box 4 Leber’s hereditary optic neuropathy
A 38-year-old male bus driver was referred with possiblebilateral optic neuritis. He complained of a 2-monthhistory of painless decline in vision in both eyes. Hesmoked and drank heavily. On examination, the visualacuity in both eyes was 6/60 and he had bilateral centralscotomata. His pupil responses were normal. His opticdiscs and optical coherence tomography were normal.Blood tests for B12, autoimmune and inflammatory dis-eases, fundus fluorescein angiography, lumbar punctureand MR brain were normal.Further questioning revealed an uncle who had had
‘optic neuritis’ that had recovered slowly following intra-venous methylprednisolone. Our patient proved positivefor the 14484 T>C Leber’s mutation. Subsequent familyhistory tracing identified several other affected malerelatives.
Comment: This case had several unusual features makingidiopathic demyelinating optic neuritis (IDON) unlikely—it was painless, of relatively slow onset, and was bilat-eral. The 14484 mutation of Leber’s can be associatedwith recovery and clearly caused confusion in thepatient’s uncle whose recovery was erroneously attribu-ted to corticosteroid therapy.
Figure 5 Multiple evanescent white dot syndrome. Leftfundus of young woman with visual blurring following upperrespiratory tract infection. (A) Fundus photograph showingmultiple white ‘spots’. (B) Early fluorescein angiogram showinghyperfluorescence of the spots.
REVIEW
Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254 105
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

disturbances of colour vision and afferent pupillarydefects may also occur. Visual field testing shows vari-able, and often considerable, enlargement of the blindspot (involving 12–55° of vision).56 About half ofpatients have a RAPD56 and about half have a slightswelling of the optic disc (but never to a degree toexplain the extent of blind spot enlargement). Theremay be several other minor retinal abnormalities(including white dots). Full-field ERG is typicallynormal but focal ERG may show nasal parafovealabnormalities.55 57 Visual field loss does not improvein most patients, but the photopsias diminish withtime.55
Comment: Neurologists should consider these condi-tions if a patient presents with painless visual losswith marked photopsias. Although an enlarged blindspot is more typical of these conditions, a centralscotoma and a RAPD are not uncommon and so theycan be confused with IDON. Unlike IDON, however,the visual loss is usually painless and continues to pro-gress rather than improving by the fourth week. Itsformal diagnosis almost certainly requires referral toan ophthalmology service for specialised ophthalmictests and retinal electrophysiology.
Autoimmune retinopathyThese conditions are extremely rare. Though both eyesare usually involved, the condition can be monocular58
and, in this situation, misdiagnosis as optic neuritis iswell reported.59 There are three main autoimmuneconditions that can affect the retina. These are cancer-associated retinopathy,60 melanoma-associated retinop-athy61 and non-neoplastic autoimmune retinopathy 59
(most patients with autoimmune retinopathy).59 62
Patients often have a personal or family history ofother autoimmune conditions. Autoimmune retinop-athy may also develop as a complication of other oph-thalmic conditions such as retinitis pigmentosa.Most patients with autoimmune retinopathy
develop sudden onset of photopsias followed by othersymptoms, depending on the type of photoreceptorinvolved. Features associated with cone dysfunctionare photosensitivity, abnormal visual acuity, colourvision abnormalities, central scotomas and abnormalcone-mediated ERG. Features associated with rod dys-function are night blindness, prolonged dark adapta-tion, peripheral or ring scotomas and abnormalrod-mediated ERG.61 Vision loss typically progressesover several months: patients may have impairedcentral vision and contrast sensitivity. Ocular examin-ation usually shows no evidence of inflammation (atleast initially) but ERG is very abnormal. With time,the retina can become depigmented with vascularattenuation.Antibodies to at least 16 proteins have been
described but the most common antigens are the23-kDa photoreceptor protein, recoverin and
α-enolase.61 62 Patients with melanoma-associated ret-inopathy typically have antibodies to bipolar cells onindirect immunofluorescent histology.61
Cancer-associated retinopathy is most commonlyassociated with small cell carcinoma of the lung, butcan develop in gynaecological, breast, endocrine,colonic and other malignancies. Melanoma-associatedretinopathy most commonly occurs in patients withan established diagnosis of melanoma, but both condi-tions may develop before diagnosis of the underlyingmalignancy. Importantly, patients with all types ofautoimmune retinopathy can respond to immunosup-pression and a good recovery is more likely if treat-ment is started early.62
Comment: As above, these conditions are rare andneurologists are relatively unlikely to see them.However, because early treatment is effective, it isimportant that neurologists are aware of these condi-tions so that they are can refer patients onwards forfurther investigation and management. Red flagsinclude a known diagnosis of malignancy and, import-antly, positive visual symptoms and other symptomsof photoreceptor dysfunction.
Central serous chorioretinopathyCentral serous chorioretinopathy is relatively common(incidence 10/100 000 population) and ophthalmolo-gists are very familiar with it. Patients develop a cir-cumscribed retinal detachment at the posterior pole,
Figure 6 Central serous retinopathy. Left fundus of youngman presenting with central visual distortion andmetamorphopsia. (A) Fundus photograph showing localisedretinal detachment at posterior pole. (B) Optical coherencetomogram showing retinal detachment with fluid belowmacula.
REVIEW
106 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

typically involving the macula. The cause is unknown,but active choroidal leakage on indocyanine greenangiography suggests the choroid is the site of theprimary pathology.63 It is strongly associated withincreased serum levels of glucocorticoids (usually dueto the use of systemic corticosteroids) and is alsomore common during pregnancy, following severepsychosocial stressors, and in people with ‘type A’ per-sonalities. It is much more common in men and has apeak age of onset of 40–45 years, though it can occurin children.63 64
Patients typically present with a unilateral centralscotoma, often associated with distortion of vision,particularly metamorphopsia and/or micropsia, dys-chromatopsia and reduced contrast sensitivity. Visualacuity ranges from 6/6 to 6/60. In the acute stages,there is a circumscribed area of retinal detachmentaround the macula (figure 6). With time, the retinalpigment epithelium shows abnormal pigmentationwhich is associated with worsening acuity. There isincreased autofluorescence at the site of the detach-ment and fluorescein angiography shows focal leakage
Table 1 Red flags suggesting consideration of diagnoses other than idiopathic demyelinating optic neuritis (IDON), with particularreference to conditions discussed in the text
‘Red flag’ Consider
History
Background, or ongoing, systemic or neurological disease that mightbe relevant
See box 1
Patient born, raised or living in a ‘non-Western’ country Infectious/parainfectious optic neuritis, sarcoidosis, NMO
Diabetes mellitus or immunosuppression Infectious/parainfectious optic neuritis
Known orbital/nasal sinus disease Infectious optic neuritis (note, fungi)
Autoimmune disease NMO
Cancer/melanoma Autoimmune retinopathy
Preceding infectious illness Parainfectious optic neuritis, neuroretinitis
Features of giant cell arteritis A-AION
Strong family history of visual disturbance LHON, DOA
Visual symptoms at onset
Sudden onset of visual loss AION
Bilateral simultaneous involvement Parainfectious optic neuritis, NMO, anti-MOG
Slow speed of onset Sarcoidosis, malignancy
Lack of pain at onset AION, neuroretinitis, LHON, AZOOR, AIBSE, MEWDS, autoimmune retinopathy
Severe pain at onset or pain persisting for >2 weeks CRION
Severe visual loss NMO, CRION, sarcoidosis
Marked phosphenes or photopsias AZOOR, AIBSE, autoimmune inflammatory
Visual distortion (micropsia, metamorphopsia) CSC
Examination findings
Local disease of orbit or nasal sinuses Infectious optic neuritis (N.B. fungi)
Lack of afferent pupillary defect LHON, CSC
Severe disc swelling, peripapillary haemorrhages, retinal exudates Sarcoidosis
Pale optic disc swelling A-AION
Disc-at-risk in fellow eye NA-AION
Macular star Neuroretinitis, hypertensive retinopathy
Ocular inflammation or retinal abnormalities Sarcoidosis, AZOOR, MEWDS
Optic disc pallor at presentation DOA, sarcoidosis
Findings on initial investigation
Raised inflammatory markers or platelet count A-AION
Extensive or posterior abnormalities of the optic nerve on MRI NMO, anti-MOG, sarcoidosis
Follow-up
Bilateral sequential involvement LHON, CRION, NMO, sarcoidosis
Lack of improvement or ongoing deterioration at 4 weeks Box 1 consider compressive or infectious cause sarcoidosis, NMO, AZOOR
Deterioration in vision after withdrawal of corticosteroids CRION, sarcoidosis
AION, anterior ischaemic optic neuropathy; A-AION, arteritic anterior ischaemic optic neuropathy; AIBSE, acute idiopathic blind spot enlargement; AZOOR,acute zonal occult outer retinopathy; CRION, chronic relapsing inflammatory optic neuropathy; CSC, central serous choroidoretinopathy; DOA, dominantoptic atrophy; LHON, Leber’s hereditary optic neuropathy; MEWDS, multiple evanescent white dot syndrome; MOG, myelin oligodendrocyte glycoprotein;NA-AION, non-arteritic anterior ischaemic optic neuropathy; NMO, neuromyelitis optica.
REVIEW
Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254 107
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

in the retinal pigment epithelium and subretinal accu-mulation of the dye. Optical coherence tomographyclearly shows the subretinal fluid, but also showsthickening of the choroid in affected and unaffectedeyes. The condition is usually self-limiting, resolvingspontaneously in 2–3 months. There are several sug-gested treatments but no standard management otherthan stopping any corticosteroid treatment.63–66
Comment: Ophthalmologists normally manage centralserous chorioretinopathy. Occasionally, however, thepredominant central visual loss may prompt referralto a neurologist, particularly if the fundus has notbeen examined or if the retinal detachment is subtle(this is becoming less likely with the advent of opticalcoherence tomography). Unlike IDON, patients oftencomplain of visual distortion in the form of micropsiaor metamorphopsia because the photoreceptors aredeformed. An RAPD is unlikely and its absenceshould prompt an examination of the fundus and areferral to (or back to) an ophthalmologist. Grantedthat corticosteroids are used in the treatment of manyneurological conditions including IDON and otherneuropathies, it is important that neurologists arefamiliar with this condition.
CONCLUSIONMost neurologists will correctly diagnose most casesof optic neuritis but may have difficulty in perhaps10% of cases.3 We believe that there are two under-lying issues contributing to this. The first relates tosemantics, that is, confusion in terminology: not all‘optic neuritis’ is the optic neuritis that is associatedwith MS (IDON). Second, there are many conditionsthat mimic IDON and can cause confusion. Table 1
lists a number of ‘red flags’ which should promptreconsideration of a diagnosis of IDON.
Acknowledgements The authors thank Associate ProfessorsClare Fraser (figure 1) and Justin O'Day (figure 6) andProfessor John Crompton (figures 3–6) for the photographs.John Crompton also provided helpful feedback on themanuscript.
Contributors DWand CL wrote the article jointly.
Competing interests None declared.
Provenance and peer review Not commissioned; externallypeer reviewed. This paper was reviewed by Mark Lawden,Leicester, UK.
REFERENCES1 Rodriguez M, Siva A, Cross SA, et al. Optic neuritis:
a population-based study in Olmsted County, Minnesota.Neurology 1995;45:244–50.
2 Atkins EJ, Biousse V, Newman NJ. Optic neuritis. SeminNeurol 2007;3:211–19.
3 Horwitz H, Friis T, Modvig S, et al. Differential diagnoses toMS: experiences from an optic neuritis clinic. J Neurol2014;261:98–105.
4 Wong SH, Cleary G, Storoni M, et al. ‘Blindness cured!’:long-standing visual loss responding to corticosteroids. PractNeurol 2013;13:245–8.
5 Toosy AT, Miller DH. Optic neuritis. Lancet 2014;13:83–99.6 Balcer LJ. Optic neuritis. New Eng J Med 2006;354:1273–80.7 Beck RW, Cleary PA, Anderson MM, et al., the Optic Neuritis
Study Group. A randomized, controlled trial of corticosteroidsin the treatment of acute optic neuritis. New Eng J Med1992;326:581–8.
8 [No authors listed]. The clinical profile of optic neuritis:experience of the optic neuritis treatment trial. Optic NeuritisStudy Group. Arch Ophthalmol 1991;109:1673–8.
9 Hickman SJ, Dalton CM, Miller DH, et al. Management ofacute optic neuritis. Lancet 2002;360;1953–62.
10 Foroozan R, Buono LM, Savino PJ, et al. Acute demyelinatingoptic neuritis. Curr Opin Ophthalmol 2002;13:375–80.
11 Beck RW, Cleary PA, Optic neuritis treatment trial; one-yearfollow-up results. Arch Ophthalmol 1993;111:773–5.
12 Trobe JD, Beck RW, Moke PS, et al. Contrast sensitivity andother vision tests in the optic neuritis treatment trial.Am J Ophthalmol 1996;121:547–53.
13 Katz B. The dyschromatopsia of optic neuritis: a descriptiveanalysis of data from the optic neuritis treatment trial. TransAm Ophthalmol Soc 1995;93:685–708.
14 Keltner JL Johnson CA, Spurr JO, et al., Baseline visual fieldprofile of optic neuritis: the experience of the optic neuritistreatment trial. Optic Neuritis Study Group. Arch Ophthalmol1993;111:231–4.
15 Keltner JL, Johnson CA, Cello KE, et al. for the Optic NeuritisStudy Group. Visual field profile of optic neuritis: a finalfollow-up report from the optic neuritis treatment trial frombaseline through 15 years. Arch Ophthalmol 2010;128:330–7.
16 The Optic Neuritis Study Group. Multiple sclerosis risk afteroptic neuritis; final optic neuritis treatment trial follow-up.Arch Neurol 2008;65:727–32.
17 Lightman S, McDonald WI, Bird AC, et al. Retinal venoussheathing in optic neuritis; its significance for the pathogenesisof multiple sclerosis. Brain 1987;110:405–14.
Key points
▸ ‘Typical’ idiopathic demyelinating optic neuritis is aclinical diagnosis and a diagnosis of exclusion andmisdiagnoses occur in up to 10%; the clinician mustbe wary of features that suggest possible alternativediagnoses.
▸ Careful history and examination are essential, includ-ing examination of the ocular fundi (with pupillarydilatation if necessary).
▸ The major role of MRI is to exclude other diagnosesand to assist with prognostication, not to make thediagnosis.
▸ Common conditions that may cause confusion in aneurological clinic include neuromyelitis optica,sarcoidosis, chronic relapsing inflammatory opticneuropathy, anterior ischaemic optic neuropathy,infectious/parainfectious optic neuropathy, neuroreti-nitis, Leber’s hereditary optic neuropathy and several‘ocular’ mimics.
REVIEW
108 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

18 Lim YM, Pyun SY, Lim HT, et al. First-ever optic neuritis:distinguishing subsequent neuromyelitis optica from multiplesclerosis. Neurol Sci 2014;35:781–3.
19 Pula JH, Kattah JC, Keung B, et al. Longitudinally extensiveoptic neuritis in neuromyelitis optica spectrum disorder.J Neurol Sci 2014;345:209–12.
20 Rolak LA, Beck RW, Paty DW, et al. for the Optic NeuritisStudy Group. Cerebrospinal fluid in acute optic neuritis:experience of the optic neuritis treatment trial. Neurology1996;46:368–72.
21 Levin MH, Bennett JL, Verkman AS. Optic neuritis inneuromyelitis optica. Prog Ret Eye Res 2013;36:159–71.
22 Shimizu J, Hatanaka Y, Hasegawa M, et al. IFNβ-1b mayseverely exacerbate Japanese optic-spinal MS in neuromyelitisoptica spectrum. Neurology 2010;75:1423–7.
23 Lange AP, Sadjadi R, Zhu F, et al. Spectral-domain opticalcoherence tomography of retinal nerve fiber layer thickness inNMO patients. J Neuro-Ophthalmolol 2013;33:213–19.
24 Bennett JL, de Seze J, Lana-Peixoto M, et al., GJCF-ICC&BR.Neuromyelitis optica and multiple sclerosis: seeing differencethrough optical coherence tomography. Mult Scler2015;21:678–88.
25 Mealy MA, Whetstone A, Orman G, et al. Longitudinallyextensive optic neuritis as an MRI biomarker distinguishesneuromyelitis optica from multiple sclerosis. J Neurol Sci2015;355:59–63.
26 Ramanathan S, Reddel SW, Henderson A, et al. Antibodies tomyelin oligodendrocyte glycoprotein in bilateral and recurrentoptic neuritis. Neurol Neuroimmunol Neuroinflamm 2014;1:e40;
27 Nakajima H, Motomura M, Tanaka K, et al. Antibodies tomyelin oligodendrocyte glycoprotein in idiopathic opticneuritis. BMJ Open 2015;5:e007766.
28 Galetta SL, Cornblath WT. Should most patients with opticneuritis be tested for neuromyelitis optica antibodies andshould this affect their treatment? J Neuro-Ophthalmol2010;30:376–9.
29 Frohman LP, Guirgis M, Turbin RE, et al. Sarcoidosis of theanterior visual pathway: 24 new cases. J Neuro-Ophthalmol2003;23:190–7.
30 Zajicek JP, Scolding NJ, Foster O, et al. Central nervous systemsarcoidosis—diagnosis and management. Q J Med1999;92:103–17.
31 Terushkin V, Stern BJ, Judson MA, et al. Neurosarcoidosis:presentations and management. Neurologist 2010;16:2–15.
32 Kidd D. Inflammatory optic neuropathies not associated withmultiple sclerosis. In: Kidd DP, Newman NJ, Biousse V, eds.Neuro-ophthalmology. Philadelphia: Butterworth-Heinemann,2008:153–90.
33 Kidd D, Burton B, Plant GT, et al. Chronic relapsinginflammatory optic neuropathy (CRION). Brain2003;126:276–84.
34 Petzold A, Pittock S, Lennon V, et al. Neuromyelitis optica-IgG(aquaporin-4) autoantibodies in immune mediated opticneuritis. J Neurol Neurosurg Psychiatry 2010;81:109–11.
35 Petzold A, Plant GT. Chronic relapsing inflammatory opticneuropathy: a systematic review of 122 cases reported.J Neurol 2014;261:17–26.
36 Biousse V, Newman NJ. Ischemic optic neuropathies. New EngJ Med 2015;372:2428–36.
37 Purvin V, Kawasaki A, Jacobson DM. Optic perineuritis:clinical and radiographic features. Arch Ophthalmol2001;119:1299–306.
38 Rappoport D, Goldenberg-Cohen N, Luckman J, et al.Parainfectious optic neuritis: manifestations in children vs.adults. J Neuro-Ophthalmol 2014;34:122–9.
39 Miller NR, Newman NJ, Biousse V, et al., eds. Wash & Hoyt’sclinical neuro-ophthalmology. 6th edn, Vol 3. Philadelphia:Lippincott Williams & Wilkins, 2005.
40 Thurtell MJ, Chiu ALS, Goold LA, et al. neuro-ophthalmologyof invasive fungal sinusitis: 14 consecutive patients and a reviewof the literature. Clin Exp Ophthalmol 2013;41:567–76.
41 Matsuo T, Notohara K, Yamadori I. Aspergillosis causingbilateral optic neuritis and later orbital apex syndrome. Jpn JOphthalmol 2005;49:423–33.
42 Alsuhaibani AH, Al-Thubaiti G, Al Badr FB. Optic nervethickening and infarction as the first evidence of orbitalinvolvement with mucormycosis. Middle East Afr J Ophthalmol2012;19:340–2.
43 Gass JDM. Diseases of the optic nerve that may simulatemacular disease. Trans Am Acad Ophthalmol Otolaryngol1977;83:766–9.
44 Purvin V, Sundaram S, Kawasaki A. Neuroretinitis: review ofthe literature and new observations. J Neuro-Ophthalmol2011;31:58–68.
45 Fraser JA, Biousse V, Newman NJ. The neuro-ophthalmologyof mitochondrial disease. Surv Ophthalmol 2010;55:299–334.
46 Riordan-Eva P, Sanders MD, Govan GG, et al. The clinicalfeatures of Leber’s hereditary optic neuropathy defined by thepresence of a pathogenic mitochondrial mutation. Brain1995;118:319–37.
47 Hsu TK, Wang AG, Yen MY, et al. Leber’s hereditary opticneuropathy masquerading as optic neuritis with spontaneousvisual recovery. Clin Exp Optom 2014;97:84–6.
48 Palace J. Multiple sclerosis associated with Leber’s hereditaryoptic neuropathy. J Neurol Sci 2009;286:24–7.
49 Matthews L, Enzinger C, Fazekas F, et al., on behalf of theMAGNIMS project. MRI in Leber’s hereditary opticneuropathy: the relationship to multiple sclerosis. J NeurolNeurosurg Psychiatry 2015;86:537–42.
50 Gass JD. Acute zonal occult outer retinopathy. J ClinNeuroophthalmol 1993;13:79–97.
51 Mrejen S, Khan S, Gallego-Pinazo R, et al. Acute zonal occultouter retinopathy: a classification based on multimodalimaging. JAMA Ophthalmol 2014;132:1089–98.
52 Monson DM, Smith JR. Acute zonal occult outer retinopathy.Surv Ophthalmol 2011;56:23–35.
53 Gross NE, Yannuzzi LA, Freund B, et al. Multiple evanescentwhite dot syndrome. Arch Ophthalmol 2006;124:493–500.
54 Jampol LM, Sieving PA, Pugh D, et al. Multiple evanescentwhite dot syndrome; 1. Clinical findings. Arch Ophthalmol1984;102:671–4.
55 Volpe NJ, Rizzo JF, Lessell S. Acute idiopathic blind spotenlargement syndrome; a review of 27 new cases. ArchOphthalmol 2001;119:59–63.
56 Watzke RC, Shults WT. Clinical features and natural history ofthe acute idiopathic enlarged blind spot syndrome.Ophthalmology 2002;109:1326–35.
57 Fletcher WA, Imes RK, Goodman D, et al. Acute idiopathicblind spot enlargement. Arch Ophthalmol 1988;106:44–9.
58 Almeida DRP, Chin EK, Niles P, et al. Unilateral manifestationof autoimmune retinopathy. Can J Ophthalmol 2014;49:e85–7.
59 Mizener JB, Kimura AE, Adamus G, et al. Autoimmuneretinopathy in the absence of cancer. Am J Ophthalmol1997;123:607–18.
REVIEW
Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254 109
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from

60 Thirkill CE, FitzGerald P, Sergott RC, et al. Cancer-associatedretinopathy (CAR syndrome) with antibodies reacting withretinal, optic-nerve, and cancer cells. New Eng J Med1989;321:1589–94.
61 Keltner JL, Thirkill CE, Yip PT. Clinical and immunologiccharacteristics of melanoma-associated retinopathy syndrome:eleven new cases and a review of 51 previously publishedcases. J Neuro-Ophthalmol 2001;21:173–87.
62 Heckenlively JR, Ferreyra HA. Autoimmune retinopathy:a review and summary. Semin Immunopathol 2008;30:127–34.
63 Quin G, Liew G, Ho IV, et al. Diagnosis and interventions forcentral serous chorioretinopathy: review and update. Clin ExpOphthalmol 2013;41:187–200.
64 Liegl R, Ulbig MW. Central serous chorioretinopathy.Ophthalmologica 2014;232:65–76.
65 Wang M, Munch IC, Hasler PW, et al. Central serouschorioretinopathy. Acta Ophthalmol 2008;86:126–45.
66 Liew G, Quin G, Gillies M, et al. Central serouschorioretinopathy: a review of epidemiology andpathophysiology. Clin Exp Ophthalmol 2013;41:201–14.
67 Atkins EJ, Newman NJ, Biousse V. Lesions of the opticnerve. In: Kennard C, Leigh RJ, eds. Handbook ofclinical neurology: neuro-ophthalmology. Amsterdam: Elsevier,2011:159–84.
68 Petzold A, Plant GT. Diagnosis and classification ofautoimmune optic neuropathy. Autoimmunity Rev2014;13:539–45.
REVIEW
110 Weerasinghe D, Lueck C. Pract Neurol 2016;16:96–110. doi:10.1136/practneurol-2015-001254
on Septem
ber 9, 2020 by guest. Protected by copyright.
http://pn.bmj.com
/P
ract Neurol: first published as 10.1136/practneurol-2015-001254 on 13 January 2016. D
ownloaded from