Embed Size (px)
Citation preview

REVIEW OF CLINICAL ANATOMY & PHYSIOLOGY OF
THE ORBIT
Dr. Ayesha Abdullah 12.09.2012

LEARNING OUTCOME
By the end of this lecture the students would be able to;
“correlate the structural organization of the orbit with its functions and clinical significance”

ANATOMY OF THE ORBIT
• The orbital cavities are …………

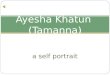
Adult orbital dimensions
Entrance height 35 mm
Entrance width 40 mm
Medial wall length / depth
45 mm
Volume 30 cc
Distance from the back of the globe to the optic foramen
18 mm
45mm
45mm
35mm

SALIENT ANATOMICAL FEATURES
• 7 bones• 4 walls• 4 margins• 4 important openings• 6 contents• 5 important relationships

v

MZSFELP
Bones &
walls

IMPORTANT OPENINGS OF THE ORBIT

Which orbit ?

IMPORTANT OPENINGS OF THE ORBIT Optic Foramen• Where?• size?• what passes through?• Clinical significance?Superior orbital fissure• Where? • What passes through? • What is annulus of Zinn?• Clinical significance?Inferior orbital fissure: • Where?• What passes through?• Clinical significance?

Openings of the orbit
Nasolacrimal canal • Where? • What passes through? • Clinical significance
Inferior orbital foramen• Where?• What passes through• Clinical significance?


Orbital walls Roof• Frontal bone and sphenoid lesser wing• Lacrimal gland, trochlea • Superior orbital notch • BrainFloor• Zygomatic, maxilla and palatine bones. • weak part • Infraorbital groove & canal for the
infraorbital nerve • Maxillary sinus.

Medial Wall• lacrimal, maxillary, ethmoid &
sphenoid• Thinnest wall• Lamina papyrecea• It separates the orbit from the nasal
cavity, the ethmoidal and the sphenoidal sinuses
Lateral Wall• Zygomatic & Sphenoid (greater wing) • Stronger wall• It separates the orbit from the
(temporal fossa) and the brain

Roof

Medial wall
Floor

IMPORTANT RELATIONS OF THE ORBIT
1. Brain : Orbit is closely related to the brain in relation to its roof and lateral wall.
2. Para nasal sinuses: Orbit is intimately connected to the paranasal sinuses.
– Maxillaly sinus via the floor. – Ethmoidal and sphenoidal sinus via the medial
wall. – Frontal sinus at the roof. – Any infection can easily spread to the orbit from
the sinuses. 3. Nasal cavity: Nasal cavity is related to the
orbit at its medial or inner wall & through the nasolacrimal duct
4. Cavernous sinus via the veins of the orbit5. Pterygopalatine fossa via the inferior
orbital fissure

Orbit as seen from above


CONTENTS OF THE ORBIT
1. Eyeball & the optic nerve2. Muscles – To move the eyeball. 3. Nerves –
– To move the muscles ( III, IV, VI). – To carry different sensations ( V)– parasympathetic innervation ( accommodation, pupillary
constriction & lacrimal gland stimulation– Sympathetic innervation ( pupillary dilatation,
vasoconstriction, smooth muscles of the eye lids & hidrosis)4. Blood vessels ( branches of ophthalmic artery, superior &
inferior ophthalmic veins) 5. Fat & orbital fascia – For padding purposes &for smooth
movements 6. Most of the Lacrimal Apparatus ( lacrimal gland & part of
the tear drainage system)



Lacrimal gland and the view of the orbit from
the roof



Orbital fascia
• Periorbita• Orbital septum• Tenon’s capsule• Fascial spaces
intraconal extraconalsubtenon
subperiosteal

Intraconal
extraconal
subtenon
subperiosteal

Extraconal space
Intraconal space
Subperiosteal space


VIEWS : AXIAL VIEWS
RADIOGRAPHIC ANATOMY OF THE ORBIT

CORONAL VIEW

SAGITTAL VIEW



AXIAL CT SCAN



Summary
• Orbit is the protective casing for the delicate visual apparatus - the eyeball
• It is made up of 7 bones, has 4 margins, 4 walls/ boundaries, 4 important openings , 5 important relations & 6 contents
• Infection can spread to the brain from the orbit directly or through the venous drainage
• Trauma mostly damages the medial wall & the floor ( the weakest parts give way)
• The symptomotology of orbital diseases is reflective of its clinical anatomy

References
• American Academy of Ophthalmology.Orbit, eyelids & lacrimal system. American Academy of Ophthalmology; 1997-98
• Jack J Kanski. Clinical ophthalmology a systematic approach. 5th ed;2003:557-89
• Parsons’ diseases of the eye. Diseases of the adnexa-diseases of the orbit. 19th ed. 2004; 505-524
• Remington LA. Clinical Anatomy of the visual system. Bones of the skull & orbit. 1998; 123-35