Embed Size (px)
Citation preview

Review of Drug InterferenceWith Urine Glucose Tests
MICHAEL D. ROTBLATT, PharmD, AND MARY ANNE KODA-KIMBLE, PharmD
Many drugs have been reported to interfere with copper-reduction or glucose oxidase tests used tomeasure urine glucose. However, only a few drugs or drug classes have been well documented toclinically interfere with these tests. The interfering drugs include ascorbic acid, P-lactam antibiotics(e.g., cephalosporins and penicillins), levodopa, and salicylates. Several other drugs may also interferewith certain urine glucose tests, but the interactions are poorly documented. These drugs include chloralhydrate, hyaluronidase, nalidixic acid, nitrofurantoin, p-aminosalicylic acid, phenazopyridine, probe-necid, and X-ray contrast media. Drugs or their metabolites that are strong reducing substances producefalse-positive results by the copper-reduction method and false-negative results by the glucose oxidasemethod. The p-lactam antibiotics interfere with copper-reduction tests by producing copper compoundsof various colors that confuse interpretation of test results. Tables are provided that summarize the druginterferences discussed. Diabetes Care 10:103-10, 1987
Self-monitoring of blood glucose (SMBG) is the mon-itoring method of choice for diabetic patients. How-ever, many diabetic patients still rely on urineglucose testing for routine self-monitoring. Diabe-
tologists and other health-care providers should have a listavailable of the many drugs that have been reported to in-terfere with these urine tests. Although several lists or reviewshave been published that provide a variety of information topractitioners and their diabetic patients (1-12), most of theselists are poorly researched, reference secondary sources ofinformation, or do not include data from current investiga-tions. Reference to secondary literature sources has inappro-priately implicated several drugs on the basis of anecdotalreports of obscure, antiquated, or unknown origin.
We have evaluated the primary literature that describespotential drug interference with the urine glucose tests. Drugsthat have been reported to interfere with urine glucose testsbut are currently unavailable in the United States [i.e., ace-tanilide, aminopyrine, trimetozine, Mercuhydrin, metaxa-lone, and phenacetin (1)] have been excluded from thisreview. Although several drugs interfere with urine glucosetests, many drugs have been reported to interfere with thesetests based on evidence that we believe is inadequate or
inappropriate. Because urine glucose test results are onlysemiquantitative, varying by one color block is within ac-ceptable accuracy (13). This should be noted when authorsof single-case reports or small studies describe positive ornegative reactions that vary only slightly from the expectedresult. We review the literature on drug interference withurine glucose tests and present an easy-to-use reference forpractical clinical use. In general, appropriately designed stud-ies and clinically relevant literature are discussed in depth.Other material is cited but discussed only briefly.
MECHANISM FOR DRUG INTERFERENCE WITH URINEGLUCOSE TESTS
Copper-reduction tests {Clinitest). Drugs or drug metabolitesthat have similar reducing properties to glucose react withcopper-reduction tests by reducing cupric sulfate (a blue toblue-green substance) to cuprous oxide (a yellow to red-orange substance) (2,14).* In many instances, drug inter-ference has only been documented with the Benedict's test,which is now rarely used and may be more sensitive thanClinitest to interference with reducing agents (3,14). Littleevidence justifies extrapolating drug interference with the
*CuSO4 (blue to blue-green) + reducing substance Cu2O (yellow to red) + oxidized substance
DIABETES CARE, VOL. 10 NO. 1, JANUARY-FEBRUARY 1987 103
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022

DRUG INTERFERENCE WITH URINE GLUCOSE TESTS/M. D. ROTBLATT AND M. A. KODA-KIMBLE
Benedict's test to drug interference with Clinitest. Therefore,we limit most of our discussion concerning copper-reductiontests to Clinitest, but we include a summary of the reporteddrug interference with Benedict's test in Table 3.
Certain drugs can also interfere with interpretation of thecopper-reduction test by reacting with cupric sulfate to formother colored copper compounds, e.g., copper sulfides. Thesereactions may be reported in the literature as uninterpretable,false positive, or false negative, depending on the ultimatecolor produced.
Glucose oxidase tests (Clinistix, Diastix, KetO'Diastix, Chem-strips Ug and Ugk, and Tes-Tape). The color changes in thesetests are initiated by a series of chemical reactions, beginningwith glucose oxidase converting glucose to D-glucuronic acidand hydrogen peroxide. In the presence of peroxidase, hy-drogen peroxide then oxidizes a chromogen to produce aparticular color change. The chromogen system varies witheach of the commercial products as follows (2,14,15). *
Strong reducing agents inhibit the glucose oxidase tests toproduce false-negative results. These reducing agents preventor diminish oxidation of the chromogen, the reaction thatforms the basis of the color change in the test strip or pad(14-16). Thus, reducing agents can produce false-negativeglucose oxidase test results and, as described above, false-positive Clinitest results.
Drugs or chemicals may also interfere with glucose oxidasetests by inhibiting the glucose oxidase or peroxidase enzymes.For example, sodium fluoride is an inhibitor of peroxidaseand in 1-2 mg/ml concentration can inhibit a reaction inurine containing 1-2% glucose (17,18).
There are no reports of false-positive glucose oxidase re-actions due to drugs. However, cleansing residues in urinecontainers have caused positive glucose oxidase results. Suchcleansing agents include hydrogen peroxide and sodium hy-pochlorite (bleach) (19).
DRUGS
Drugs reported to interfere with urine glucose tests are dividedinto three groups. Group A represents drugs for which in-terference is well documented, group B represents drugs forwhich interference is poorly documented, and group C rep-resents drugs that do not interfere with the urine glucosetests.
Group A DrugsAscorbic acid {vitamin C). Based on the available data, as-corbic acid supplementation can inhibit glucose oxidase testresults (18,20-30). Oral administration of ascorbic acid (atleast ^ 9 g/day) does not appear to affect Clinitest readings,but intravenous administration may potentially produce false-positive results.
Many investigators have studied the effects of ascorbic acidon glucose oxidase tests by spiking urine samples with varyingaliquots of glucose and ascorbic acid. Although the concen-trations of ascorbic acid required to inhibit the glucose ox-idase reaction varied with each study, most investigatorsfound that 50-100 mg/dl of ascorbic acid was required toinhibit the reaction in urine samples containing 0.25% glu-cose. Urine samples containing higher concentrations of glu-cose required higher concentrations of ascorbic acid to inhibitthe reaction.
Several case reports suggest that ascorbic acid may alsointerfere with copper-reduction tests; however, most of thesereports are anecdotal or difficult to interpret (3,23,25). Inone early investigation, 500 and 1000 mg of ascorbic acidadministered intravenously to an unstated number of subjectsproduced positive Benedict's test results in most of the pa-tients (22). In contrast, three recent well-designed clinicalstudies have demonstrated that large oral doses of ascorbicacid have no effect on Clinitest results (27,29). In each study,adult nondiabetic subjects received 3—9 g/day of ascorbicacid for at least 3 days before testing. Only 2 of 2035 urinetests from 146 subjects were positive for glucose in traceamounts. The conflicting results between the latter studiesand the older reports may be due to a difference in sensitivitybetween Benedict's test and Clinitest or to a difference inurinary recovery from intravenous versus oral administration.
fi'Lactam antibiotics. Both in vitro and in vivo studies con-firm that the P-lactam antibiotics (penicillins, cephalospo-rins, monobactams, and carbapenems) interfere with theinterpretation of Clinitest results but do not interfere withthe interpretation of glucose oxidase test results (31-33).Unlike other drugs that produce false-positive reactions withcopper-reduction tests, the p-lactam antibiotics appear tohave no reducing properties. It has been postulated that thevigorous boiling that occurs during the Clinitest reactionbreaks the (B-lactam ring to release free sulfur. The sulfurreacts with copper ions from the test to create insoluble
'All testsP-L>glucose + O2 - ^
Chromogen systemsglucuronic acid + H2O2
Clinistix
Diastix
Chemstrips
Tes-Tape
H2O2 + reduced o-tolidine (pink) peroxidase oxidized o-tolidine (blue)
H2O2 + 2KI """l^ > I2 + 2KOH (dark brown)
Ug H2O2 + reduced tetramethylbenzidine —v"°^x > oxidized tetramethylbenzidine (orange to brown)
H2O2 + reduced o-tolidine (pink) —pe"""dasc > oxidized o-tolidine (blue)
oxidized o-tolidine (blue) h tartrazine dve (yellowt
A Site of potential drug interference.
pale green to deep blue
104 DIABETES CARE, VOL. 10 NO. 1, JANUARY-FEBRUARY 1987
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022

DRUG INTERFERENCE WITH URINE GLUCOSE TESTS/M. D. ROTBLATT AND M. A. KODA-KIMBLE
TABLE 1Cephalosporin and penicillin antibiotics that have been studied
Cephalosporin andcephalosporin-likeantibiotics
Penicillins
Drugs
cefaclor (Ceclor)cefadroxil (Duricef, Ultracef)cefamandole (Mandol)cefazolin (Ancef, Kefzol)cefonicid (Monocid)cefoperazone (Cefobid)ceforanide (Precef)cefotaxime (Claforan)cefoxitin (Mefoxin)ceftazidime (Fortaz, Tazidime)ceftizoxime (Cefizox)ceftriaxone (Rocephin)cephapirin (Cefadyl)cephradine (Velosef, Anspor)cephalothin (Keflin)moxalactam (Moxam)ampicillinazlocillin (Azlin)carbenecillinmezlocillin (Mezlin)penicillin Gpiperacillin (Pipracil)ticarcillin (Ticar)
Refs.
3232
32,353432
36,3732
32,35,3732,3534,37
37373834
36,39,4032,35
3136,37
3136,3731,4136,37
37
colored compounds, e.g., copper sulfide (black) or cuproussulfide (gray, blue, or black). These compounds, combinedwith cupric sulfate (blue) or cuprous oxide (yellow to red),create colors that may not match the color chart providedwith the test (34).
Moxalactam, a cephalosporin-like antibiotic that is tech-nically an oxa-(3-lactam, contains an oxygen rather than asulfate ring system. Because moxalactam cannot release freesulfur, it is one of the only P-lactam antibiotics that doesnot interfere with the Clinitest reaction (32).
Some of the fJ-lactam antibiotics also produce consistentfalse-positive or even false-negative reactions with Clinitest,depending on the drug or glucose concentration in the urine.Clinitest readings rarely vary more than one color block,which is within the acceptable accuracy range for the urineglucose tests. However, the occurrence of uninterpretablemeasurements, especially with the cephalosporins, suggeststhat Clinitest cannot be relied on when the patient is re-ceiving a p-lactam antibiotic.
1. Cephalosporins. Most cephalosporin and cephalospo-rin-like antibiotics currently available in the United Stateshave been studied (Table 1; 32,34-40). Several investigatorshave demonstrated that these cephalosporins consistentlyproduce false-positive Clinitest results (32,34-36). This re-action is drug-concentration dependent and is more likely tooccur after administering large drug doses (32,34,36,37).Urine containing higher concentrations of glucose (>1%) isless likely to be affected by the cephalosporins.
More important, cephalosporins also produce unpredict-able color changes in urine tested with Clinitest. Colors thathave been reported as brown, black, or green are either
uninterpretable or mistakenly interpreted as the green-brown color that occurs after a pass-through phenomenon(34,37,39,40). Only moxalactam does not interfere with theClinitest reaction (32).
2. Penicillins. Many penicillin antibiotics have also beenstudied (Table 1; 31,36,37,41). Several investigators havereported that penicillins may cause false decreases as well asfalse increases in urine glucose concentrations measured bythe Clinitest copper-reduction test (31,36,37). These effectsare drug- and glucose-concentration dependent. High con-centrations of a penicillin can produce false-positive resultswhen no glucose is present in the urine and false-negativeresults when urine contains significant amounts of glucose.Both increased and decreased readings may occur in urinewith small or intermediate glucose concentrations (0.5%),but falsely decreased readings occur most consistently at lowerpenicillin concentrations.
The mechanism proposed for the false-positive readings issimilar to that previously discussed for the |3-lactam anti-biotics in general. Vigorous boiling of the Clinitest reagentbreaks the penicillin thiazolidine ring, releasing a free sulfurmolecule that reacts with copper ions. Because all penicillinderivatives possess this ring structure, probably all will in-terfere with the urine glucose test similarly.
The false low readings produced by penicillin are moredifficult to explain. MacCara and Parker (31) have proposedthat the combination of glucose and penicillin produces ahigh specific gravity in the urine. Like high concentrationsof protein, this may prolong the exothermic reaction to pro-duce falsely decreased glucose readings.
3. Monobactams. The monobactam antibiotic, aztreo-nam (still investigational), reacts with Clinitest similarly toother P-lactam antibiotics (37). In the absence of glucose,high concentrations of aztreonam react with Clinitest to forma black color. When glucose is present, aztreonam may causethe reading to be falsely low (1% is read as 0.75%).
4. Carbapenems. Imipenem is the first drug of a new classof carbapenem (3-lactam antibiotics. It is combined with ci-lastatin, a dehydropeptidase inhibitor used to prevent en-zymatic degradation of imipenem in the renal tubules.Tartaglione and Flint (33) demonstrated in an in vitro studythat low urine concentrations of imipenem-cilastatin pro-duced false low-glucose results measured with the Clinitestmethod. However, high urinary drug concentrations did notinterfere with the urine test. As with other p-lactam anti-biotics, the glucose oxidase tests are not affected.
Levodopa. Levodopa appears to have a dose-related effecton urine glucose tests (18,42-44). In a study of 12 patientstaking 0.75-3.0 g/day of levodopa for Parkinson's syndrome,false-positive (trace) urine glucose test results were obtainedwith Clinitest in 6 of 25 urine samples (24%). False-negativeClinistix readings were also observed in the same 6 urinesamples spiked with 1% glucose. Similar readings were ob-served in 13 of 17 urine samples (76%) from patients taking3.5-5.0 g/day of levodopa. DOPAC (3,4-dihydroxyphe-nylacetic acid), a metabolite with strong reducing properties,is responsible for levodopa's effect on urine glucose testing(18,42).
DIABETES CARE, VOL. 10 NO. 1, JANUARY-FEBRUARY 1987 105
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022

DRUG INTERFERENCE WITH URINE GLUCOSE TESTS/M. D. ROTBLATT AND M. A. KODA-KIMBLE
It might be anticipated that Sinemet, a combination oflevodopa and the decarboxylase inhibitor carbidopa, wouldnot affect urine glucose testing. Patients require ~75% lesslevodopa in this combination than they would with levodopaadministered alone. In fact, carbidopa inhibits the decar-boxylation of levodopa to dopamine, substantially reducingthe urinary excretion of DOPAC (45). Until this is clinicallysubstantiated, however, urine glucose tests should not beconsidered reliable for patients taking levodopa in any form.
Salicylates. Large, chronic doses of aspirin and other sa-licylates may inhibit glucose oxidase reactions and producefalse-positive Clinitest results. The substance responsible forthis interference appears to be gentisic acid, a minor hy-droxylated metabolite of most salicylates that acts as a re-ducing agent (18).
In a study by Feldman et al. (18), urine samples frompatients taking various doses of aspirin were spiked to a glu-cose concentration of 1%. The Clinistix glucose oxidase re-action was inhibited in 5 of 10 urine samples (50%) frompatients receiving 2.4-2.7 g/day of aspirin. The same re-action was also inhibited in 5 of 7 urine samples (71%) frompatients receiving 3.6-5.4 g/day of aspirin. Most urine sam-ples that inhibited the glucose oxidase test also producedfalse-positive results for glucose when tested by the Clinitestcopper-reduction method.
Small, single doses of aspirin or salicylate equivalents prob-ably do not interfere with urine glucose tests because suchdoses produce low concentrations (<1%) of gentisic acid inthe urine. With larger doses, however, two of the five met-abolic pathways for salicylic acid become saturated, signifi-cantly increasing the proportion metabolized to gentisic acid(46).
All of the salicylates that are available in the UnitedStates, with two exceptions noted below, are converted invivo to salicylic acid, an aspirin metabolite that is furthermetabolized to gentisic acid. These salicylates can be ex-pected to interfere with urine glucose tests when administeredin large or chronic doses (Table 2). However, diflunisal (Do-lobid) or salicylamide (Uromide) probably does not interferewith urine glucose tests at any dose, because neither agentis metabolized to salicylic or gentisic acid.
Group B DrugsThe primary literature supporting claims that group B drugsinterfere with urine glucose tests is limited. Some of thedocumentation is available only from secondary informationsources or from manufacturers' statements, without a primarysource. However, until more primary literature can be eval-uated or there is evidence to the contrary, we recommendthat diabetic patients verify the test results or use alternativetesting methods during therapy with the drugs discussed be-low.
Chloral hydrate, hyaluronidase, nitrofurantoin, and probene-cid. For many years, these four drugs have been included inlists of drugs that cause false-positive copper-reduction urineglucose tests (3). The leading manufacturers of chloral hy-drate and probenecid have included information to this effectin their package inserts (47,48). However, personal com-
TABLE 2Salicylates expected to interfere with urine glucose tests in large or chronicdoses
Aspirin (e.g., Ascriptin, Bufferin, Ecotrin, Empirin, Alka-Seltzer)Choline magnesium trisalicylate (Trilisate)Choline salicylate (Arthropan)Magnesium salicylate (e.g., Doan's Pills)Salicylsalicylic acid (e.g., Salsalate, Disalcid)Sodium salicylate (e.g., Uracel 5)Sodium thiosalicylate (various)
munication with manufacturers of these four products and asearch of the medical literature has failed to document anyprimary literature for these alleged interactions.
Nalidixic acid and p-aminosalicylic acid (PAS). Limited re-ports have associated nalidixic acid (49-51) and PAS (52,53)with interference of copper-reduction tests such as the Ben-edict's test. Some of these reports are subjective and notclinically relevant. Ciprofloxacin, an investigational quin-olone antibiotic related to nalidixic acid, does not interferewith Clinitest or glucose oxidase tests (33). However, enoughevidence exists to recommend that patients should avoid orat least verify Clinitest readings during therapy with eithernalidixic acid or PAS.
Phenazopyridine. Phenazopyridine (Pyridium) is a yellowazo dye used as a urinary tract analgesic. Naumann (54) testedurine samples for glucose from an unstated number of subjectsreceiving phenazopyridine in a dose of 200 mg three timesdaily. No interference was demonstrated with Clinitest; how-ever, reactions to Tes-Tape, Clinistix, and Combistix weredelayed, yielding false-negative results.
X-ray contrast media, intravenous. Iodinated radiopaqueagents, used to visualize various organ systems on X-ray ex-amination, are excreted primarily unchanged in the urine.Most of these agents have a half-life of <2 h. Althoughconflicting reports exist (55,56), the best study suggests thatdiatrizoate sodium (Hypaque) and similar radiopaque agentsmay interact with both the Clinitest and glucose oxidase teststo create a characteristic greenish-black color. This color issimilar to that seen in the reaction with urine containinghomogentisic acid from patients with alkaptonuria (57). Theinvestigators hypothesized that diatrizoate, which is struc-turally somewhat similar to homogentisic acid, may interferewith urine glucose test results in a similar manner. Althoughmore evidence is needed to document this reaction, we rec-ommend that patients not rely on urine glucose test resultsfor 24 h after the injection of an intravenous X-ray contrastagent.
Group C DrugsThese drugs can be further categorized into three separategroups. The first subgroup includes drugs that have been welldocumented not to interfere with the urine glucose tests.Many of these drugs were initially thought to interfere basedon isolated case reports or poorly designed studies and maystill be included in existing lists. These drugs include theaminoglycoside antibiotics (amikacin, gentamicin, tobra-
106 DIABETES CARE, VOL. 10.NO. 1, JANUARY-FEBRUARY 1987
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022
DRUG INTERFERENCE WITH URINE GLUCOSE TESTS/M. D. ROTBLATT AND M. A. KODA-KIMBLE
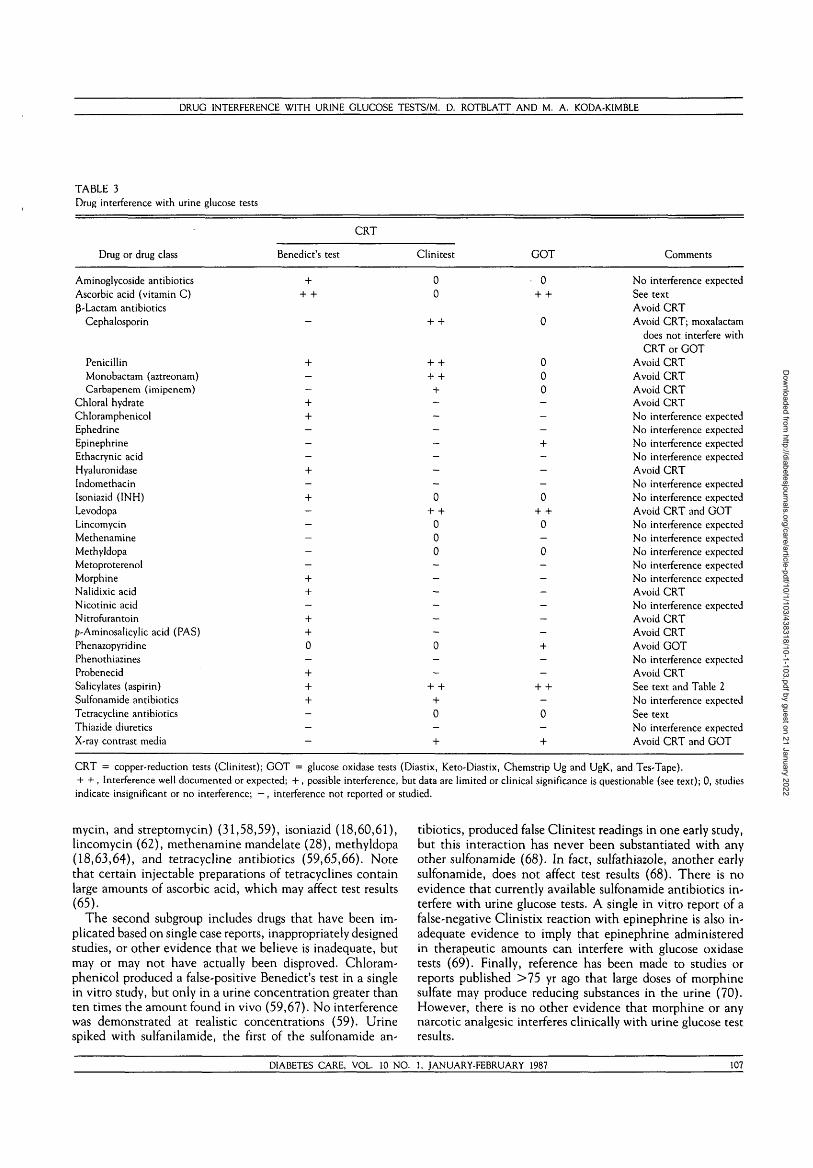
TABLE 3Drug interference with urine glucose tests
CRT
Drug or drug class
Aminoglycoside antibioticsAscorbic acid (vitamin C)B-Lactam antibiotics
Cephalosporin
PenicillinMonobactam (aztreonam)Carbapenem (imipenem)
Chloral hydrateChloramphenicolEphedrineEpinephrineEthacrynic acidHyaluronidaseIndomethacinIsoniazid (INH)LevodopaLincomycinMethenamineMethyldopaMetoproterenolMorphineNalidixic acidNicotinic acidNitrofurantoinp-Aminosalicylic acid (PAS)PhenazopyridinePhenothiazinesProbenecidSalicylates (aspirin)Sulfonamide antibioticsTetracycline antibioticsThiazide diureticsX-ray contrast media
Benedict's test
++ +
—
+
--++---+-+-----++-++0-
+++---
Clinitest
00
+ +
+ +
+ ++-------0
+ +000------0--
+ ++0-
+
GOT Comments
No interference expectedSee textAvoid CRTAvoid CRT; moxalactam
does not interfere withCRT or GOT
Avoid CRTAvoid CRTAvoid CRTAvoid CRTNo interference expectedNo interference expectedNo interference expectedNo interference expectedAvoid CRTNo interference expectedNo interference expectedAvoid CRT and GOTNo interference expectedNo interference expectedNo interference expectedNo interference expectedNo interference expectedAvoid CRTNo interference expectedAvoid CRTAvoid CRTAvoid GOTNo interference expectedAvoid CRTSee text and Table 2No interference expectedSee textNo interference expectedAvoid CRT and GOT
CRT = copper-reduction tests (Clinitest); GOT = glucose oxidase tests (Diastix, Keto-Diastix, Chemstrip Ug and UgK, and Tes-Tape).+ + , Interference well documented or expected; + , possible interference, but data are limited or clinical significance is questionable (see text); 0, studiesindicate insignificant or no interference; —, interference not reported or studied.
mycin, and streptomycin) (31,58,59), isoniazid (18,60,61),lincomycin (62), methenamine mandelate (28), methyldopa(18,63,64), and tetracycline antibiotics (59,65,66). Notethat certain injectable preparations of tetracyclines containlarge amounts of ascorbic acid, which may affect test results(65).
The second subgroup includes drugs that have been im-plicated based on single case reports, inappropriately designedstudies, or other evidence that we believe is inadequate, butmay or may not have actually been disproved. Chloram-phenicol produced a false-positive Benedict's test in a singlein vitro study, but only in a urine concentration greater thanten times the amount found in vivo (59,67). No interferencewas demonstrated at realistic concentrations (59). Urinespiked with sulfanilamide, the first of the sulfonamide an-
tibiotics, produced false Clinitest readings in one early study,but this interaction has never been substantiated with anyother sulfonamide (68). In fact, sulfathiazole, another earlysulfonamide, does not affect test results (68). There is noevidence that currently available sulfonamide antibiotics in-terfere with urine glucose tests. A single in vitro report of afalse-negative Clinistix reaction with epinephrine is also in-adequate evidence to imply that epinephrine administeredin therapeutic amounts can interfere with glucose oxidasetests (69). Finally, reference has been made to studies orreports published >75 yr ago that large doses of morphinesulfate may produce reducing substances in the urine (70).However, there is no other evidence that morphine or anynarcotic analgesic interferes clinically with urine glucose testresults.
DIABETES CARE, VOL. 10 NO. 1, JANUARY-FEBRUARY 1987 107
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022

DRUG INTERFERENCE WITH URINE GLUCOSE TESTS/M. D. ROTBLATT AND M. A. KODA-KIMBLE
The third subgroup includes drugs that may induce truehyperglycemia and glucosuria. These have been included inseveral lists of drugs that interfere with urine testing, whichhas caused some confusion in the literature (2,5,6). Althoughhyperglycemia and glucosuria may be a pharmacologic sideeffect of some of these drugs, to our knowledge there is noevidence that the following drugs produce false urine glucosetest results: indomethacin, ephedrine, ethacrynic acid, me-taproterenol, nicotinic acid, phenothiazines, and thiazidediuretics.
DISCUSSION
Anumber of drugs and drug classes have been re-ported to interfere with urine glucose tests, butonly a few of these interactions have been studiedextensively. We were surprised to find little data
in the literature to document even those drugs "well known"to interfere with urine glucose tests. Many group B druginteractions are based on limited or unavailable documen-tation. We recommend that patients use alternative glucosetesting methods when available for this group of drugs. Manydrugs have also been implicated based on results of olderreports that used test materials no longer in use. These con-tinue to be included on lists even though their interferencewith current test materials has been disproved. We havesummarized our review in Tables 3 and 4, which can be usedas a quick reference.
Falsely increased or decreased urine test results are unlikely
to be a problem for most diabetic patients who use urine teststo qualitatively monitor the presence or absence of glucosein the urine. Nevertheless, for other diabetic patients, drugalteration of test results may lead to a false sense of alarm orsecurity. Drug interference of any magnitude is particularlysignificant for diabetic patients who continue to use urineglucose results to make adjustments in insulin dose.
Some drugs interfere with only one type of urine glucosetest (either copper reduction or glucose oxidase). If a patientmust test urine for glucose while receiving one of these drugs,an alternative type of urine test will be available. For ex-ample, cephalosporins and penicillins (group A drugs) in-terfere only with copper-reduction tests, and therefore aglucose oxidase test may be used. If switching from one typeof test to another is difficult or disadvantageous, and theinterference is poorly documented (a group B drug is in-volved), the patient or clinician can verify the reliability ofthe test by using both test types soon after drug therapy isinitiated. For example, a diabetic woman who has been usingClinitest is initiated on probenecid, a group B drug, whichmay interfere with the Clinitest copper-reduction test. Iden-tical samples of her urine can be tested for glucose with bothClinitest and a glucose oxidase test 2 or 3 days after proben-ecid therapy has begun (at least 3—4 drug half-lives). If thetest results are similar, Clinitest should be reliable. Mostgroup B drugs have only been reported to interfere withcopper-reduction tests; nevertheless, they should be sus-pected to interfere with glucose oxidase tests unless provenotherwise (Tables 3 and 4).
TABLE 4Classes of drugs that interfere with urine glucose tests
Group A:drugs that interfere
with urine glucose tests
Ascorbic acidp-Lactam antibiotics'
CephalosporinsPenicillinsMonobactams (aztreonam)
Carbapenems (imipenem)
LevodopaSalicylates
Affected test
C, GOTC
C, GOTC, GOT
Group B:drugs that may interferewith urine glucose tests
Chloral hydrateHyaluronidaseNalidixic acidNitrofurantoinp-Aminosalicylic acidPhenazopyridineProbenecidX-ray contrast media
Affected tests
CCCCCGOTCC, GOT
Group C:drugs that do not interfere
with urine glucose tests
Aminoglycoside antibioticsCh loramphen ico 1CiprofloxacinEphedrineEpinephrineEthacrynic acidIndomethacinIsoniazid (INH)LincomycinMethenamineMethyldopaMetaproterenolMorphineNicotinic acidPhenothiazinesSulfonamide antibioticsTetracycline antibiotics!Thiazide diuretics
In general, drugs cause false-positive reactions with Clinitest (C) and false-negative reactions with glucose oxidase tests (GOT). GOTs include Diastix,Keto-Diastix, Chemstrip Ug/Ugk, and Tes-Tape.'False-positive, false-negative, and uninterpretable results have been reported. Moxalactam does not interfere with urine glucose tests.tSome injectable preparations of tetracycline contain large amounts of ascorbic acid.
108 DIABETES CARE, VOL. 10 NO. 1, JANUARY-FEBRUARY 1987
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022

DRUG INTERFERENCE WITH URINE GLUCOSE TESTS/M. D. ROTBLATT AND M. A. KODA-KIMBLE
If the drug interferes with both types of tests, the availableoptions for patients who require glucose monitoring duringdrug therapy include Tes-Tape, which may be read accuratelyat the wet-dry border, and SMBG. Tes-Tape acts as a min-iature chromatography system that separates the interferingdrug from the chromagen (18). However, because Tes-Tapeis one of the least quantitative of the urine test systems, weadvocate the use of SMBG whenever possible.
Drugs and drug metabolites excreted by the kidney usuallyachieve much higher concentrations in the urine than inblood or serum. Blood glucose testing should therefore beconsiderably less susceptible to drug interference than urineglucose testing. However, a recent well-designed investiga-tion of in vitro drug interference with several SMBG systemsdocumented falsely decreased blood glucose results due toascorbic acid, aspirin (but not gentisic acid), and acetami-nophen (71). Clinically important decreases of >20% com-pared with control values were observed at moderate to highdrug concentrations. SMBG systems depend on a glucoseoxidase reaction and further oxidation of a chromogen, sim-ilar to the urine glucose oxidase systems. Although additionalstudies are needed to confirm these observations, some drugsthat inhibit urine glucose oxidase test results may also affectSMBG systems. SMBG results should also be interpreted withcaution.
CONCLUSION
Drugs that have been well documented to interfere with atleast one type of currently available urine glucose test (groupA) include ascorbic acid, P-lactam antibiotics (e.g., ceph-alosporins and penicillins), levodopa,'and salicylates. Drugsfor which there is poor documentation for interference withthe urine glucose tests, but which must be suspected untilthere is evidence to the contrary (group B), include chloralhydrate, hyaluronidase, nalidixic acid, nitrofurantoin, PAS,phenazopyridine, probenecid, and X-ray contrast media.Drugs that have been well documented not to interfere withthe urine tests, or for which insufficient evidence exists tosuspect that a clinically significant interference will occur(group C), include aminoglycoside antibiotics, chloram-phenicol, ciprofloxacin, ephedrine, epinephrine, ethacrynicacid, indomethacin, isoniazid, lincomycin, methenamine,methyldopa, metaproterenol, morphine, nicotinic acid, phe-nothiazines, sulfonamide antibiotics, oral tetracycline anti-biotics, and thiazide diuretics.
From the Department of Pharmacy, Stanford University Hos-pital, Stanford and the Division of Clinical Pharmacy, School ofPharmacy, University of California at San Francisco, San Fran-cisco, California.
Address reprint requests and correspondence to Mary AnneKoda-Kimble, PharmD, Division of Clinical Pharmacy, C-152,University of California, San Francisco, CA 94143-0622.
REFERENCES
1. Hansten PD: Urine glucose: drugs which may interfere withurine glucose determinations. In Drug Interactions. 4th ed. Phil-adelphia, PA, Lea & Febiger, 1979, p. 449-55
2. Soliman KFA, Davis D, Wallace P: Nonprescription diagnosticproducts for the diabetic patient. Contemp Pharm Pract 3:215—27, 1980
3. Cook MH, Free AH, Giordano AS: The accuracy of urinesugar tests. Am J Med Technol 19:283-90, 1953
4. Wirth WA, Thompson RL: The effects of various conditionsand substances on the results of laboratory procedures. Am ]Clin Pathol 43:579-90, 1965
5. Young PS, Pestaner LC, Gibberman V: Effects of drugs onclinical laboratory tests. Clin Chem 21:1—432D, 1975
6. Elking MP, Kabat HF: Drug-induced modifications of laboratorytest values. Am J Hosp Pharm 25:485-519, 1968
7. Lubran M: The effects of drugs on laboratory values. Med ClinN Am 53:211-22, 1969
8. Henry RJ, Cannon DC, Winkelman JW (Eds.): Clinical Chem-istry. 2nded. Hagerstown, MD, Harper &. Row, 1974, p. 1294-99
9. Nelson CJ: A guide to glucose testing systems. Drug Intel! ClinPharm 8:422-29, 1974
10. Constantino NV, Kabat HF: Drug-induced modifications oflaboratory test values—revised 1973. Am J Hosp Pharm 30:24-71, 1973
11. Factors Affecting Urine Chemistry Tests. Elkhart, IN, Ames Di-vision, Miles, 1982
12. Lipman AG: Drugs that interfere with urine glucose tests. Mod-em Med 46:195-96, 1978
13. Clinitest Reagent Tablets Package Insert. Elkhart, IN, Ames Di-vision, Miles, 1979
14. Modem Urine Chemistry. Elkhart, IN, Ames Division, Miles,1982, p. 43-47
15. Urinalysis With Chemstrip. Indianapolis, IN, Bio-Dynamics,1983
16. Feldman JM, Lebovitz FL: Tests for glucosuria: an analysis offactors that cause misleading results. Diabetes 22:115-21, 1973
17. Onstad J, Hancock D, Wolf PL: Inhibitory effect of fluorideon glucose tests with glucose oxidase strips, d in Chem 21:8,1975
18. Feldman JM, Kelley WN, Lebovitz HE: Inhibition of glucoseoxidase paper tests by reducing metabolites. Diabetes 19:337-43, 1970
19. Caraway WT: Chemical and diagnostic specificity of laboratorytests. Am J Clin Pathol 37:445-64, 1962
20. O'Gorman P, Griffiths PD, Bloxam HR: Ascorbic acid inhi-bition of the glucose-oxidase test for glycosuria. Br Med 7 1:603-606, 1960
21. Gifford H, Bergerman J: Falsely negative enzyme paper testsfor urinary glucose. JAMA 178:423-24, 1961
22. Mithoefer JC, Vilter CF: Glycosuria simulated by the admin-istration of ascorbic acid: its occurrence and differentiation(Abstract). J Lab Clin Med 33:1471, 1948
23. Mayson JD, Schumaker O, Nakamura RM: False-negative testsfor urinary glucose in the presence of ascorbic acid. Am J ClinPathol 58:297-99, 1972
24. Davison JM, Cheyne GA: False-negative tests for glycosuria(Letter). Lancet 1:1321-22, 1973
25. Brandt R, Guyer KE, Banks WL Jr: Urinary glucose and vitaminC. Am] Clin Pathol 68:592-94, 1977
26. Nakamura RM, Reilly EB, Fujita K, Brown J, Kunitake GM:False-negative reactions and sensitivity in the urine glucoseoxidase test. Diabetes 14:224-25, 1965
27. Nahata MC, McLeod DC: Noneffect of oral urinary copperascorbic acid on reduction glucose test. Diabetes Care 1:34-35,1978
DIABETES CARE, VOL. 10 NO. 1, JANUARY-FEBRUARY 1987 109
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022

DRUG INTERFERENCE WITH URINE GLUCOSE TESTS/M. D. ROTBLATT AND M. A. KODA-KIMBLE
28. Nahata MC, McLeod DC: Lack of effect of ascorbic acid,hippuric acid, and methenamine (urinary formaldehyde) onthe copper-reduction glucose test in geriatric patients. J AmGeriatr Soc 28:230-33, 1980
29. Smith D, Young WW: Effect of large-dose ascorbic acid on thetwo-drop Clinitest determination. Am J Hosp Pharm 34:1347-49, 1977
30. Free HM, Free AH: Influence of ascorbic acid on urinary glu-cose tests (Abstract). Clin Chem 19:662, 1973
31. MacCara ME, Parker WA: In vitro effect of penicillins andaminoglycosides on commonly used tests for glycosuria. Am JHosp Pharm 38:1340-45, 1981
32. Kowalsky SF, Wishnoff FG: Evaluation of potential interactionof new cephalosporins with Clinitest. Am J Hosp Pharm39:1499-501, 1982
33. Tartaglione TA, Flint NB: Effect of imipenem-cilastatin andciprofloxacin on tests for glycosuria. Am J Hosp Pharm 42:602-605, 1985
34. MacCara ME, Angaran DM: Cephalosporin-Clinitest inter-action: comparison of cephalothin, cefazolin and cephradine.Am] Hosp Pharm 35:1064-67, 1978
35. McManus MC, Barriere SL: Interaction between newer ceph-alosporins and Clinitest, Diastix and Tes-Tape. Am J HospPharm 40:1544-45, 1983
36. McCue JD, Gal P, Pearson RC: Interference of new penicillinsand cephalosporins with urine glucose monitoring tests. Dia-betes Care 6:504-505, 1983
37. LeBel M, Paone RP, Lewis GP: Effect of ten new P-lactamantibiotics on urine glucose test methods. Drug Intell Clin Pharm18:617-20, 1984
38. Haas JD, Raebel MA: Cephapirin interference with urine-glu-cose testing systems. Am) Hosp Pharm 41:1186-87, 1984
39. Kostis J, Bergen SS: Usual color reaction in glycosuria testingduring cephalothin administration (Letter). JAMA 196:125,1966
40. Morrill J, Davis LJ, Burris DM: Interference with urinary glu-cose determination by cephalothin (Letter). JAMA 230:822-23, 1974
41. Whipple RL, Bloom WL: The occurrence of false-positivetests for albumin and glucose in the urine during the courseof massive penicillin therapy. J Lab Clin Med 36:635-39,1950
42. Feldman JM, Lebovitz HE: Levodopa and tests for urinary glu-cose (Letter). N Engl} Med 283:1053-54, 1970
43. Cotzias GC, Van Woert MH, Schiffer LM: Aromatic aminoacids and modification of Parkinsonism. N EnglJ Med 276:374-79, 1967
44. Cawein MJ, Williamson MA, Ebenezer C, Hewins JP: Lev-odopa and tests for ketonuria. N Engl J Med 283:659,1970
45. McEvoy GK (Ed.): American Hospital Formulary Service DrugInformation. Bethesda, MD, Am. Soc. Hosp. Pharm., 1984,p. 1592
46. Levy G: Clinical pharmacokinetics of aspirin. Pediatrics 62(Suppl.):867-72, 1978
47. hJoctec Package Insert. Princeton, NJ, Squibb, 198448. Benemid Package Insert. Rahway, NJ, Merck, Sharp & Dohme,
197849. Islam MA, Streedhavan T: Convulsions, hyperglycemia and
glycosuria from overdose of nalidixic acid. JAMA 192:1100—101, 1965
50. Klumpp TG: Nalidixic acid . . . false-positive glycosuria andhyperglycemia (Letter). JAMA 193:746, 1965
51. Ronald AR, Turck M, Petersdorf RF: A critical evaluation ofnalidixic acid in urinary-tract infections. N Engl ] Med275:1081-89, 1966
52. Phillips RW: The superiority of enzyme impregnated paper fordetermining glycosuria in patients receiving antituberculosisdrug therapy. Dis Chest 36:160-63, 1959
53. Iuchi I, Shibita S: A new method for the examination of mel-lituria. Clin C/xim Acta 5:42-47, 1960
54. Naumann HN: Prevention of pyridium interference in urinal-ysis by dithionate reduction or butanol extraction. Am J ClinPathol 48:337-41, 1967
55. Nelson JC, Krueger GG, Wilcox RB, Thompson WP: Effectof radio-contrast media on the measurement of adrenal ste-roids in the urine (Letter). J Clin Endocrinol Metab 28:1515-17,1968
56. Hurt R: The effect of radiographic contrast media on urinalysis.Am J Med Tech 26:122-24, I960
57. Lee S, Schoen I: Black-copper reduction reaction simulatingalkaptonuria occurrence after intravenous urography. N Engl JMed 275:266-67, 1966
58. Neuberg HW: Streptomycin as a cause of false-positive Ben-edict reaction for glycosuria. Am J Clm Pathol 24:245-46, 1954
59. Lippman RW: Effect of antibiotic agents on tests for proteinand reducing sugar in the urine. Am J Clin Pathol 22:186-88,1952
60. Luntz GRWN, Smith SG: Effect of isoniazid on carbohydratemetabolism in controls and diabetics. BrMed] 1:296-99, 1953
61. Self TH, Wester VL: Noneffect of isoniazid on urine glucosetests. Diabetes Care 3:44-45, 1980
62. Panzer JD: Lincomycin therapy and urinary glucose tests (Let-ter). JAMA 210:349, 1969
63. Bowers CB, Self TH: Noneffect of methyldopa on urine glucosetests. Diabetes Care 1:36, 1978
64. Ives TJ, Pevonka P, Andresen BD, Yost RL: Effect of meth-yldopa on urine glucose test methods. AmJ Hosp Pharm 3 7:683-87, 1980
65. Kristensen KAB: I.V. Tetracycline and "dip stick" urine tests(Letter). N Engl J Med 283:660, 1970
66. Wester VL, Self TH: Noneffect of oral tetracycline on urineglucose determination by the copper reduction method. Dia-betes Care 3:567, 1980
67. Kucers A, Bennett NMcK: The Use of Antibiotics. 3rd ed. Phil-adelphia, PA, Lippincott, 1979, p. 431-32
68. Todd WR, Dodson MC, Trainer JB, McKee J: Sulfa drug in-terference in sugar determinations. Arch Biochem 4:337-41,1944
69. Naganna B, Rajamma M, Vasucera RK: On the failure of en-zyme paper strips to detect glucose in certain abnormal urines.CUnChimActa 17:219-21, 1967
70. Sollman T: A Manual of Pharmacology and Its Application toTherapeutics and Toxicology. 7th ed. Philadelphia, PA, Saun-ders, 1948, p. 293
71. Rice GK, Gait KA: In vitro drug interference with home bloodglucose measurement systems. AmJ Hosp Pharm 42:2202-207,1985
no DIABETES CARE, VOL. 10 NO. 1, JANUARY-FEBRUARY 1987
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/10/1/103/438318/10-1-103.pdf by guest on 21 January 2022





























