-
7/29/2019 Rigid Endoscopic Evaluation of Conventional
Adenoidectomy
1/6
Rigid endoscopic evaluation of conventional
curettage adenoidectomy
D REGMI, N N MATHUR, M BHATTARAI
Department of Otolaryngology and Head and Neck Surgery, B P
Koirala Institute of Health Sciences, Dharan, Nepal
AbstractObjectives: To evaluate the results of conventional
adenoidectomy, using rigid endoscopy of the nasopharynx, and
to establish the role of such evaluation in facilitating
complete adenoid removal via the curettage technique.
Design: Descriptive rigid endoscopic evaluation of the
nasopharynx before and after adenoid curettage, and
following subsequent endoscopy-assisted adenoidectomy.
Setting: Tertiary referral centre.
Patients: Forty-one consecutive children with symptomatic
adenoid hypertrophy scheduled to undergo
adenoidectomy.
Results: Rigid endoscopic evaluation indicated that conventional
curettage, used alone, failed to completely
remove adenoid tissue from the superomedial choanae and anterior
vault in all cases; incomplete removal was
also seen in other parts of the choanae (in 67.2 per cent of
patients), the eustachian tube opening (63 per cent),
the nasopharyngeal roof (61.78 per cent) and the fossa of
Rosenmuller (61 per cent). Subsequent rigid
endoscopy-assisted adenoidectomy successfully removed the
residual adenoid tissue from all nasopharyngeal
sites, except the eustachian tube opening in two cases.
Conclusion: Conventional curettage adenoidectomy misses a
substantial amount of adenoid tissue. Rigid
endoscopy-assisted adenoidectomy improves this result by
enabling localisation of any residual adenoid tissue.
Key words: Adenoidectomy; Endoscopy; Otorhinolaryngologic
Surgical Procedures
IntroductionAdenoidectomy is a commonly performed procedure
inthe field of otolaryngology. It has traditionally beenconducted
using the curettage method. This is a rela-tively blind technique
which risks nasopharyngealinjury and incomplete adenoid removal;
indeed, it has
been found to completely remove adenoid vegetationsin less than
30 per cent of cases.1
In 1992, Beckeret al. reported the use of endoscopy-assisted
adenoidectomy.2 This technique uses a 0, 30,70 and 120 rigid nasal
endoscope of 2.7 or 4 mmdiameter. It has the advantages of improved
visualisa-tion and magnification, rigidity, superior
haemostasis,reduction of unnecessary trauma, complete removalof
adenoid tissue, and improved safety. Endoscopy-assisted
adenoidectomy is generally perceived to bemore effective in
clearing adenoid tissue, comparedwith the conventional curettage
method, but this hasnot been objectively assessed.
Therefore, we undertook a descriptive, cross-sectional study
evaluating the nasopharynx of 41consecutive paediatric
adenoidectomy cases, using a
0, 30 and 70, rigid, 4 mm endoscope. The study
aimed (1) to evaluate the role of such endoscopy inassessing the
adenoids before and after traditional cur-ettage adenoidectomy; (2)
to assess the effectiveness ofcurettage adenoidectomy performed
alone; and (3) toevaluate the possible role of such endoscopy in
improv-ing the results of curettage adenoidectomy.
Materials and methodsWe included in the study 41 paediatric
patients under-going adenoidectomy with or without other
surgical
procedures (e.g. tonsillectomy or ventilation tube inser-tion),
whose parents were willing to give informedconsent. We excluded
patients with contraindicationsfor adenoidectomy, and those in whom
the rigid naso-
pharyngeal endoscope could not be navigated up to
thenasopharynx.
Ethical approval was obtained from our institutionsethical
committee.
All patients underwent clinical history-taking, andwere assessed
pre-operatively using relevant, noninva-sive investigations such as
pure tone audiometry, impe-dance audiometry and X-ray (using a soft
tissue, lateral
neck view with open mouth and neck extension).
Accepted for publication 2 June 2010 First published online 18
October 2010
The Journal of Laryngology & Otology (2011), 125, 5358. MAIN
ARTICLE JLO (1984) Limited, 2010
doi:10.1017/S0022215110002100
-
7/29/2019 Rigid Endoscopic Evaluation of Conventional
Adenoidectomy
2/6
The nasal cavity was decongested with cottonsoaked in 0.05 per
cent oxymetazoline.
The nasopharynx was inspected via the nasal cavityusing a 0, 30
and 70 rigid endoscope (Karl Storz,Tuttlingen, Germany) to assess
the extent of adenoidtissue (this was the first endoscopy). The
operating
surgeon was kept unaware of the findings.Surgery was performed
under general anaesthesia
with orotracheal intubation, with the patient placed inRoses
position. A BoyleDavis mouth gag of appro-
priate size was inserted. A small French rubber catheterwas
inserted through the nostril and brought outthrough the mouth, and
the ends were clinched for
palatal retraction.3 The operating surgeon assessed thesize and
extent of the adenoid with the index fingerof the dominant hand.
The adenoids were removed
by conventional curettage. Small tags of lymphoidtissue retained
after curettage were removed with
punch forceps. Pressure haemostasis was achieved bypacking the
area with sterile cotton gauze packssoaked in adrenaline (1:100
000), for three minutesunless contraindicated. If adrenaline was
contraindi-cated, sterile gauze packs soaked with saline onlywere
used.
4
Thereafter, the patients nasal cavity and nasophar-ynx were
again examined endoscopically, by thesame endoscopist as
previously, to determine the com-
pleteness of adenoid tissue removal at different sites(this was
the second endoscopy). If remnant adenoidtissue was seen, it was
removed under endoscopiccontrol, and the final result again
assessed endoscopi-cally (this was the third endoscopy).
Following curettage and endoscopy-assisted adenoi-dectomy, the
volume of adenoid tissue removed wasmeasured using the displacement
method (utilising a25 ml measuring cylinder).
ResultsPatients mean age standard deviation (SD) was8.83 2.77
years; most were aged seven to 12 years.The male to female ratio
was 1.56:1. The mostcommon symptom was snoring (97.6 per cent),
fol-lowed by nasal obstruction. Mouth-breathing was
seen in 85.5 per cent cases, and a sore throat in 80.5per cent
(Table I).
All the patients had enlarged adenoids on X-ray (softtissue,
lateral neck view).
The most common surgical procedure conductedwas
adenotonsillectomy (n= 32), followed by adeno-
tonsillectomy with ventilation tube insertion (n= 6).Isolated
adenoidectomy was performed in only onecase.
In seven cases, both choanae were completelyblocked by adenoid
tissue, preventing passage of the4 mm rigid endoscope. In the
remaining cases (n=
34), the nasopharynx could be easily accessed with a0, 30 and
70, 4 mm, rigid endoscope, and theadenoid tissue extent at various
nasopharyngeal sitescould be studied satisfactorily.
Before curettage, adenoid tissue was found to bepresent in all
cases in the nasopharyngeal roof and
superomedial choanae. Adenoid tissue was alsopresent in the
anterior vault (in 91.6 per cent ofpatients), other parts of the
choanae (84.15 per cent),the fossa of Rosenmuller (77.95 per cent)
and the eusta-chian tube opening (76.45 per cent).
The second endoscopy could be easily performed inall cases.
Excellent haemostasis was achieved in all
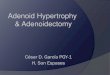
patients. In all cases, the curettage technique failed
tocompletely remove adenoid tissue from the superome-dial choanae
and the anterior vault. Other sites ofincomplete removal were (in
descending order of fre-quency) other parts of the choanae (in 67.2
per centof patients), the eustachian tube opening (63 percent), the
nasopharyngeal roof (61.78 per cent) andthe fossa of Rosenmuller
(61 per cent) (Figure 1).The curettage method was most successful
in removing
adenoid tissue from the nasopharyngeal roof; even so,38.2 per
cent of patients had incomplete removal at thissite. Thus, further,
endoscopy-guided clearance wasnecessary in all cases to ensure
complete removal ofadenoid tissue. Data on the success of curettage
adenoi-dectomy are presented in Table II.
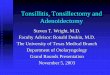
Endoscopy-assisted adenoidectomy successfullyremoved the
residual adenoid tissue from all nasophar-yngeal sites, except for
the eustachian tube opening in
two cases (Figure 2). Thus, the success rate for com-plete
adenoid remnant removal from the eustachiantube opening, under
endoscopic guidance, was 89.4
per cent. For all other nasopharyngeal sites, a 100 percent
success rate was achieved. Data on the successof endoscopy-assisted
adenoidectomy are presentedin Table III.
The mean volume SD of adenoid tissue removedusing conventional
curettage was 1.74 0.77 ml(range 0.503). In addition,
endoscopy-assisted ade-noidectomy removed a mean volume SD of
0.91
0.34 ml (range 0.52). Thus, if endoscopy-assisted
adenoidectomy had not been performed, 34.3 percent of the total
adenoid tissue volume would havebeen retained (this equates to 52.3
per cent of theadenoid tissue volume removed by curettage).
TABLE I
PATIENTS CLINICAL FEATURES
Clinical feature Patients
% n
Snoring 97.1 40Nasal obstruction 95.1 39Mouth-breathing 85.6
35Sore throat 80.5 33Sleep apnoea 29.3 12Ear ache 24.4 10Hearing
loss 22 9
Nasal discharge 19.5 8Ear discharge 9.8 4Voice change 4.9
2Epistaxis 0 0
D REGMI, N N MATHUR, M BHATTARAI54
-
7/29/2019 Rigid Endoscopic Evaluation of Conventional
Adenoidectomy
3/6
The mean time SD required to perform the first,pre-operative
endoscopy was 3.56 1.58 minutes(range 110), while that for the
second, post-curettageendoscopy was 8.82 2.15 minutes (range
212).
Intra-operative complications were noted in twopatients, in the
form of transient tachycardia while
packing with adrenaline-soaked gauze, immediatelyafter curettage
adenoidectomy. This resolved uponremoval of the pack.
One patient developed a reactionary haemorrhagefrom the
tonsillar bed six hours post-operatively; this
was managed successfully with bipolar cautery undergeneral
anaesthesia.
The patients mean SD hospital stay was 3.76
0.487 days (range 35).
DiscussionThe objective of adenoidectomy is to remove
thehypertrophic adenoid tissue that causes nasal airwayobstruction
and pathological restriction of nasalairflow. Dissatisfaction with
the safety and adequacyof clearance of conventional curettage
adenoidectomyhas led to the development of alternative
techniques,made possible by developments in fibre-optics
andendoscopic instrumentation.57
The main disadvantage of curettage is that it is a rela-tively
blind technique that may lacerate the choanaeand torus tubarius and
graze the nasopharyngealmucosa; it may also merely skim the adenoid
bulk,leaving behind obstructing tissue particularly at
theeustachian tube openings and intranasal protrusions
and high in the nasopharynx.8
A popular alternativeto conventional curettage is
endoscopy-assisted ade-noidectomy the second method employed in
ourstudy.
Our study was designed to assess the success of con-ventional
curettage adenoidectomy versus endoscopy-assisted adenoidectomy in
removing adenoid tissuefrom different nasopharyngeal sites. We also
aimedto assess the possible role of rigid endoscopic evalu-ation in
improving the success of conventional curet-tage adenoidectomy.
The first, pre-operative endoscopy could not be con-
ducted in two patients due to bilateral inferior
turbinatehypertrophy; these patients were thus excluded fromthe
study. In the remaining cases (n= 41), theadenoid tissue was easily
assessable prior to curettage,
FIG. 1
Site of residual adenoid tissue (AT) following conventional
curettage. L = left; R= right; Cho= other parts of choana; ETO =
eustachian tubeopening; FOR= fossa of Rosenmuller; SMC=
superomedial choana; AV= anterior vault
TABLE II
PATIENT RESULTS FOR CURETTAGE ADENOIDECTOMY
AT site N1 N2 AT
present atEnd-1 (n)
AT
present atEnd-2 (n)
Complete
AT removal(%)
No Yes
L Cho 34 34 27 9 18 33.3R Cho 34 34 28 9 19 32.1L ETO 34 34 22 3
19 13.6R ETO 34 34 27 5 22 18.5L FOR 34 34 25 6 19 24R FOR 34 34 28
7 21 25
NP roof 34 34 34 13 21 38.2L & R SMC 24 24 24 0 24 0L &
R AV 24 24 22 0 22 0
AT= adenoid tissue; N1= first endoscopy; N2= second endo-scopy;
End-1=pre-operative endoscopy; End-2=post-curettage
endoscopy; L= left; R= right; Cho= other parts of choanae;ETO=
eustachian tube opening; FOR= fossa of Rosenmuller;
NP= nasopharyngeal; SMC= superomedial choanae; AV=anterior
vault
ENDOSCOPIC EVALUATION OF CURETTAGE ADENOIDECTOMY 55
-
7/29/2019 Rigid Endoscopic Evaluation of Conventional
Adenoidectomy
4/6
using a 0, 30 and 70, 4 mm, Hopkins rod rigidendoscope. The
anterior vault and the superomedial
portion of the choanae were assessed with a 70Hopkins rod rigid
endoscope and a posterior rhino-scopy mirror.
Pre-operatively, adenoid tissue was invariably foundat the
nasopharyngeal roof, followed by the fossa ofRosenmuller (on the
left in 73.5 per cent of patientsand on the right in 82.4 per cent)
and the eustachiantube opening (64.7 per cent on the left and 79.4
percent on the right). We searched the literature butcould not
locate any similar studies performed toassess the nasopharyngeal
extent of adenoid tissue,
prior to performing curettage. In our study, the
adenoid tissue observed in the eustachian tube open-ings and
nasopharyngeal vault correlated well withour patients symptoms of
ear ache and snoring,respectively. We expect that the anatomical
extent ofadenoid hypertrophy would affect its
clinicalsymptomatology.
Following curettage adenoidectomy, we used cottongauze packs
soaked in 1:100 000 adrenaline to pack the
nasopharynx for three minutes, to achieve haemostasis.Adrenaline
packs were not contraindicated in any ofour cases. Patients were
closely monitored for adrena-line side effects. We encountered
transient tachycardiain two cases, which settled after removing the
naso-
pharyngeal pack.Excellent peri-operative haemostasis was
achieved
in all patients. We did not encounter any
immediatepost-operative haemorrhage; this is consistent withthe
results of Teppo et al.9 However, one patient (2.4
per cent) developed a reactionary haemorrhage fromthe right
tonsillar bed six hours post-operatively; this
was managed successfully with bipolar cautery undergeneral
anaesthesia. A prospective study has shownthat the incidence of
reactionary haemorrhage is 28
per cent.10 Return to theatre for haemostasis wasrequired in
0.5% and 2%.1113 Thus, our complicationrate was within acceptable
limits.
In the present study, a second nasopharyngealendoscopy was
conducted following curettage adenoi-dectomy, and we noted that the
extent of superomedialchoanae and anterior vault adenoid tissue
wasunchanged from its pre-operative state (as viewed at
the first endoscopy). Other sites harbouring retained
adenoid tissue included (in descending order offrequency) other
parts of the choanae (in 67.2 percent of patients), the eustachian
tube opening(63 per cent), the nasopharyngeal roof (61.78 per
FIG. 2
Site of residual adenoid tissue (AT) following
endoscopy-assisted adenoidectomy. L= left; R= right; Cho= other
parts of choana;ETO= eustachian tube opening; FOR= fossa of
Rosenmuller; SMC= superomedial choana; AV= anterior vault
TABLE III
PATIENT RESULTS FOR ENDOSCOPY-ASSISTEDADENOIDECTOMY
AT site N1 N2 AT
present atEnd-2 (n)
AT
present atEnd-3 (n)
Complete
AT removal(%)
Yes No
L Cho 34 34 18 18 0 100R Cho 34 34 19 19 0 100L ETO 34 34 19 17
2 89.4R ETO 34 34 22 22 0 100L FOR 34 34 19 19 0 100R FOR 34 34 21
21 0 100
NP roof 34 34 21 21 0 100L & R SMC 24 24 24 24 0 100L &
R AV 24 24 22 22 0 100
AT= adenoid tissue; N1= first endoscopy; N2= second endo-scopy;
End-2=post-curettage endoscopy; End-3=post endo-
scopy-assisted adenoidectomy endoscopy; Cho= other parts
ofchoanae; ETO= eustachian tube opening; FOR= fossa ofRosenmuller;
NP= nasopharyngeal; SMC= superomedialchoanae; AV= anterior
vault
D REGMI, N N MATHUR, M BHATTARAI56
-
7/29/2019 Rigid Endoscopic Evaluation of Conventional
Adenoidectomy
5/6
cent) and the fossa of Rosenmuller (61 per cent).
Thus,conventional curettage had not cleared the adenoid
tissuecompletely in even a single case. These observationswould
have not been possible had we not conducted asecond endoscopy after
the curettage procedure. Hence,the second objective of our study
was fulfilled.
Although we assessed all cases with a 70 rigidendoscope and a
posterior mirror, we found the super-omedial choanae and anterior
vault could only be eval-uated with a 0 and 30 endoscope, with
regards to theextent of adenoid tissue. In addition, these two
areaswere the most inaccessible sites for conventional curet-tage
removal of adenoid tissue.
In the present study, conventional curettage adenoi-dectomy
successfully removed adenoid tissue fromother parts of the choanae,
the eustachian tubeopening and the fossa of Rosenmuller areas in
33, 16and 24.5 per cent of patients, respectively. By compari-
son, Bross-Soriano et al. studied 150 patients with anabsolute
indication for adenoidectomy, in order toevaluate the efficacy of
conventional adenoidectomy,using intra-operative endoscopic
inspection of thenasopharynx, and to evaluate the need for
endoscopy-guided revision surgery.
1They found residual
adenoid tissue in 107 cases, 45.3 per cent of whichinvolved the
pharyngeal part of the eustachian tubes.Our study findings indicate
a higher prevalence ofresidual adenoid tissue across a greater
range of naso-
pharyngeal sites, following curettage adenoidectomy.Although not
used in the present study, we believe
that adenoid tissue in the superomedial choanae andanterior
vault can also be effectively dealt with usinga microdebrider or
suction diathermy.
In the present study, endoscopy-assisted clearanceachieved
complete adenoid removal in all but twocases. In these two
patients, a small tag of adenoidtissue could not be removed from
the eustachian tubeopening; this would have required very
tightlycurved, small Blakesley or Takahashi forceps, whichwere
unavailable.
Huang et al. treated 15 patients with symptomaticadenoid
hypertrophy, using combined conventionaland endoscopic
adenoidectomy (any residual adenoid
tissue was completely removed during an endoscopicrevision
procedure).6 They concluded that (1) this
procedure could completely remove large amounts ofadenoid tissue
without prolonging the operativetime, and (2) the endoscope
provided a clear, directview that enabled the surgeon to remove
adenoidtissue accurately, to evaluate and stop bleeding
effec-tively, and to avoid unnecessary trauma. Thus, theseauthors
believed that a combined approach employing
both conventional and endoscopic adenoidectomywas an effective
and safe method for managingenlarged adenoids.
Kulak conducted a similar study of 125 adenoidect-omy cases, in
which complete removal of adenoidtissue was achieved using an
endoscopy-assistedmethod.14
In the present study, the first, pre-operative endo-scopy took
3.56 minutes on average. Curettage adenoi-dectomy took an average
of 9.2 minutes, while thesecond, post-curettage endoscopy took an
average of8.82 minutes. In comparison, in Cannon and col-leagues
series of 130 endoscopy-assisted adenoidect-
omy cases, revision endoscopy was performed toclear residual
adenoid tissue following curettage andtook less than 5
minutes.15
In the present study, the mean volume SD ofadenoid tissue
removed via conventional curettagewas 1.74 0.77 ml (range 0.503),
while thatremoved via endoscopy-assisted adenoidectomy was0.91 0.34
ml (range 0.52). Thus, failure to under-take endoscopy-assisted
adenoidectomy would haveresulted in retention of 34.3 per cent of
the total pre-operative adenoid tissue volume (equating to 52.3
percent of the adenoid volume removed by curettage).
The use of an endoscope during
adenoidectomy gives the surgeon a clear,
direct view, facilitating precise and complete
adenoid tissue removal, effective haemostasis,
and avoidance of unnecessary trauma
Endoscopy-assisted adenoidectomy allows
better adenoid tissue clearance, compared
with conventional curettage adenoidectomy,
by enabling localisation of residual adenoid
tissue especially in the superomedial choanae
and anterior vault
Conventional curettage adenoidectomy may
achieve the desired clinical results in patients
with adenoid hypertrophy; however,
endoscopic evaluation indicates that it fails to
completely remove adenoid tissue
All our patients were discharged on the third post-oper-ative
day, giving a mean hospital stay SD of 3.76
0.487 days (range 35).The slightly older age of our patient
group could
be attributed to parents waiting longer before
seeking health care for their child, due to differingattitudes
to health care compared with other parts ofthe world.
ConclusionThe use of an endoscope gives surgeons a clear,
directview of the nasopharynx, enabling them to removeadenoid
tissue precisely and completely, to control
bleeding effectively, and to avoid unnecessary
trauma.Endoscopy-assisted adenoidectomy improves the
results of conventional curettage adenoidectomy byenabling
accurate localisation of residual adenoid
tissue, especially in the superomedial choanae andanterior vault
areas.Conventional curettage adenoidectomy may achieve
the desired result in patients with adenoid hypertrophy;
ENDOSCOPIC EVALUATION OF CURETTAGE ADENOIDECTOMY 57
-
7/29/2019 Rigid Endoscopic Evaluation of Conventional
Adenoidectomy
6/6
however, endoscopic evaluation reveals that it fails toachieve
complete adenoid removal and hence is lesssatisfactory than
endoscopy-assisted adenoidectomy.Further research is needed to
establish whether anato-mically complete adenoid removal leads to
real clinical
benefit for patients.
References
1 Bross-Soriano D, Schimelmitz-Idi J, Arrieta-Gmez JR.Endoscopic
adenoidectomy; use or abuse of the technology?Cir Cir
2004;72:1519
2 Eiji Y, Lawrence M. Nasal endoscopy, video rhinoscopy
anddocumentation. In: Ananda VK, Panje WR, eds. Practical
Endoscopic Sinus Surgery, 1st edn. New York:
McGraw-Hill,1993
3 Gabalski EC, Mattucci KF, Setzen M, Moleski P.
Ambulatorytonsillectomy and adenoidectomy. Laryngoscope
1996;106:7780
4 Wang DY, Bernheim N, Kaufman L, Clement P. Assessment
ofadenoid size in children by fiberoptic examination.
ClinOtolaryngol Allied Sci 1997;22:1727
5 Parsons DS. Rhinologic uses of powered instrumentation in
chil-
dren beyond sinus surgery. Otolaryngol Clin North Am
1996;29:10514
6 Huang HM, Chao MC, Chen YL, Hsiao HR. A combinedmethod of
conventional and endoscopic adenoidectomy.
Laryngoscope 1998;108:110467 Yanagisawa E, Weaver EM. Endoscopic
adenoidectomy with
the microdebrider. Ear Nose Throat J 1997;76:7248 Koltai PJ,
Kalathia AS, Stanislaw P, Heras HA. Power-assisted
adenoidectomy. Arch Otolaryngol Head Neck Surg 1997;123:6858
9 Paradise JL. Tonsillectomy and adenoidectomy. In: BluestoneCD,
Stool SF, Alper CM, Arjmand EM, Casselbrant ML,Dohar JE, Yellon RF,
eds. Pediatric Otolaryngology, 4th edn.Philadelphia: Saunders,
2002
10 Drake-Lee A, Stokes M. A prospective study of length of stay
of150 children following tonsillectomy and/or adenoidectomy.Clin
Otolaryngol 1998;23:4915
11 Guida R, Muttucci K. Tonsillectomy and adenoidectomy: an
in-
patient or out-patient procedure? Laryngoscope 1990;100:4913
12 Leighton S, Rowe-Jones J, Knight J. Day case
adenoidectomy.Clin Otolaryngol 1993;18:21519
13 Marshall J, Sheppard I, Narula A. A prospective study of
daycase adenoidectomy. Clin Otolaryngol1995;20:1646
14 Uar C. Endoscopic adenoidectomy. Kulak Burun Bogaz IhtisDerg
2008;18:668
15 Cannon CR, Replogle WH, Schenk MP. Endoscopic
assistedadenoidectomy. Otolaryngol Head Neck Surg 1999;121:7404
Address for correspondence:Dr N N Mathur,Professor,Department of
ENT and Head Neck Surgery,
Vardhman Mahavir Medical College and Safdarjung Hospital,New
Delhi 110029,India
E-mail: [email protected]
Dr N N Mathur takes responsibility for the integrity ofthe
content of the paperCompeting interests: None declared
D REGMI, N N MATHUR, M BHATTARAI58