Embed Size (px)
Citation preview

“Is het gebruik van cannabis een risicofactor voor schizofrenie?
Biologische grondslagen en klinische implicaties”
Ruud van Winkel Rebecca Kuepper
Maastricht University
Bunnik Symposium 8 maart 2013
Disclosure Ruud van Winkel
•Speaker fees received from: AstraZeneca, Eli Lilly, Lundbeck
•Positions held on Advisory Boards: None
•Grants and sponsoring: AstraZeneca, Eli Lilly, Janssen-Cilag

Disclosure Rebecca Kuepper
• Speaker fees received from: Lundbeck
• Positions held on Advisory Boards: none
• Grants and sponsoring: none

Moore et al, Lancet
2007
OR 1.41

Moore et al, Lancet 2007 OR 2.09

PSYCHOSIS

t0 t1
Psychotic sym ptom sPsychotic sym ptom s
t3t2
Psychotic sym ptom sPsychotic sym ptom s
German EDSP study (Early Developmental Stages of Psychopathology) Lieb et al., 2000; Wittchen et al., 1998
Kuepper et al., BMJ 2012
Does cannabis cause
persistence?

Het is bewezen, cannabis is een causale factor in de ontwikkeling van psychose.

Individuals differ in sensitivity
Genetic (e.g. familial
liability) and non-genetic
factors

time
response ‘Sensitization’
-severe -enduring
van Winkel et al, Schizophrenia Bulletin, 2008
Collip et al, Schizophrenia Bulletin, 2008

NEMESIS
Association between trauma and later cannabis use:
OR = 1.57 (1.33-1.86), p < 0.001 Konings et al., Psych Med, 2012

Causality over the life course
Phenotype
Early causes Late causes
Vulnerability Neuroendocrine
Behavioural deviance
Cognitive set
Developmental programming

Decoster et al, 2012

0 250 500 750 N(risk variants)
Frequency in
population

0 250 500 750 N(risk variants)
Frequency in
population

Distribution of psychotic symptoms in the general population?
85% no symptoms
14% symptoms
5% true psychotic symptoms
1% schizophrenia

Number of
genetic risk
variants
Psychosis
expression

Number of
genetic risk
variants
Psychosis
expression
“Liability-threshold model”

Liability
Psychosis
expression

Liability
Psychosis
expression

Parents, n=919
Siblings, n=1057 Patients, n=1120 Controls, n=590
Genetic Risk and Outcome in Psychosis Study
(GROUP)

Parents, n=919
Siblings, n=1057 Patients, n=1120 Controls, n=590
Genetic Risk and Outcome in Psychosis Study
(GROUP)

Cross-sib, cross-trait: no evidence for rGE

Caspi et al, 2005
COMT Val158Met

Decoster et al, Curr Pharm Des, 2012
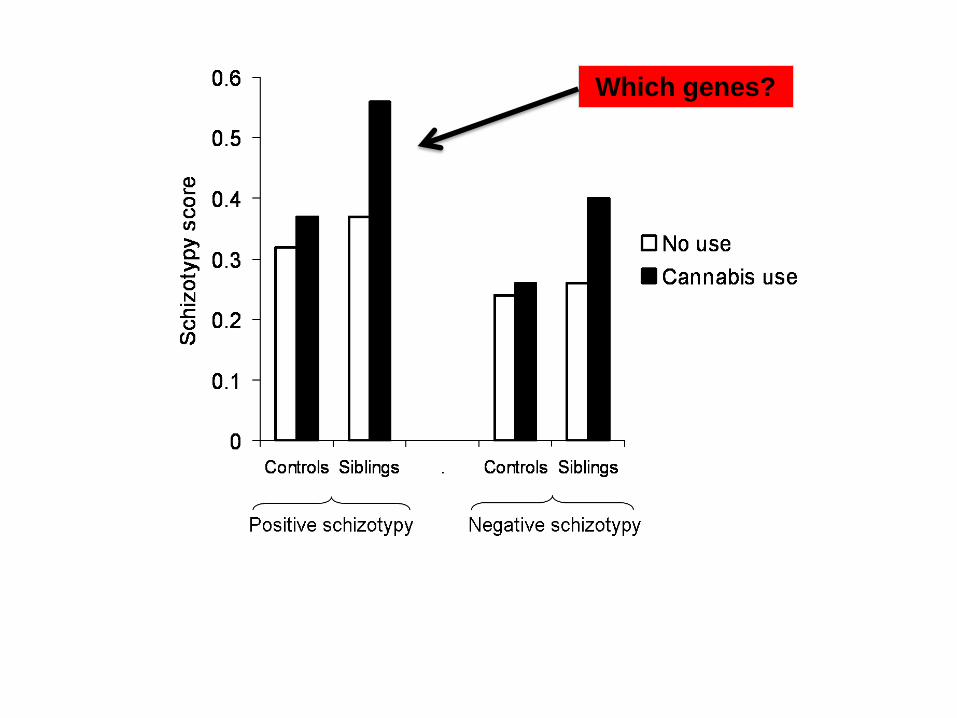
Which genes?

Association with schizophrenia: RGS4, NRG1, DTNBP1, PIP5K2A, G72/DAOA, DISC1, HT2A, AKT1,
LRRTM1, FGF2, FGFR1, GPM6A, PRODH, GRM3, GABRA6, GAD1,
NOS1, RGS2, ROBO1, CHRM3, TBX1
Important for dopaminergic neurotransmission COMT, ANKK1, DRD1, DRD2, DRD3, SLC6A3, PPP1R1B, SLC18A2
Directly related to cannabinoid signaling CNR1
Responsivity to environmental stress ADRA2C, FKBP5
Adaptive neuronal survival BDNF, P2RX7, NPY, NQO1, GST-1, GST-2
Epigenetic regulation of environmental influences MTHFR, MTR, MTRR, DNMT3B, EHMT1, EHMT2, PRDM2
van Winkel et al, Arch Gen Psychiatry, 2011

van Winkel, R. et al. Arch Gen Psychiatry 2011
Significant SNP x Cannabis Interactions (at P<.05) in 740 Unaffected Siblings

van Winkel, R. et al. Arch Gen Psychiatry 2011.
Siblings
Patients

Di Forti, Biol Psychiatry 2012

RRR
P= .13
AKT1 follow-up: case-only analysis of the UPC Catholic
University Leuven sample N=533
van Winkel & GROUP, submitted

time
response ‘Sensitization’
-severe -enduring
van Winkel et al, Schizophrenia Bulletin, 2008
Collip et al, Schizophrenia Bulletin, 2008
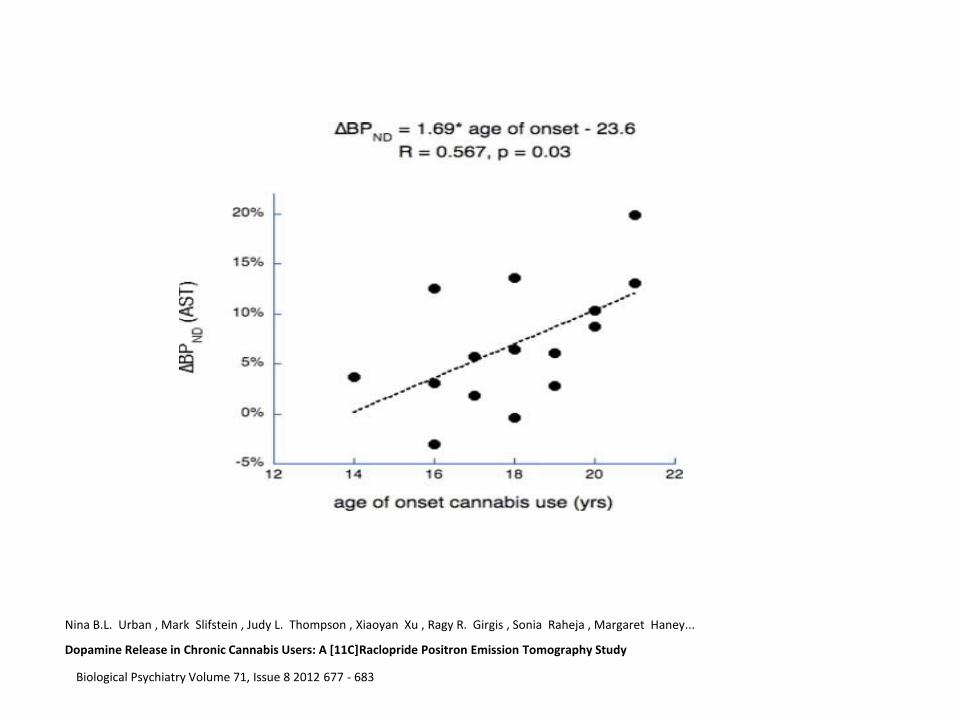
Nina B.L. Urban , Mark Slifstein , Judy L. Thompson , Xiaoyan Xu , Ragy R. Girgis , Sonia Raheja , Margaret Haney...
Dopamine Release in Chronic Cannabis Users: A [11C]Raclopride Positron Emission Tomography Study
Biological Psychiatry Volume 71, Issue 8 2012 677 - 683

Figure 1. Total striatal [11C]-raelopride BPND values for volunteers with a history of cannabis
use compared to control volunteers.
Stokes P R et al. J Psychopharmacol 2011;26:144-149
Copyright © by British Association for Psychopharmacology

D2
dopamine
AKT1
D2
dopamine
AKT1
dopaminesignaal
CB1

Percentages of voxels with significant (sig. threshold of t > 2.4) THC-induced ligand displacement

0
10
20
30
40
Patients Population
% cannabis
users
Why do patients with schizophrenia use cannabis??
e.g. Mueser et al., Schiz Bull, 1992; Regier et al., JAMA, 1990

Acute effecten
Hal
luci
nat
ies
Stem
min
g “Ik voel me opgewekt...”
“Ik hoor stemmen...”
Henquet et al., British Journal of Psychiatry, 2010
Sub-acuut
Acuut
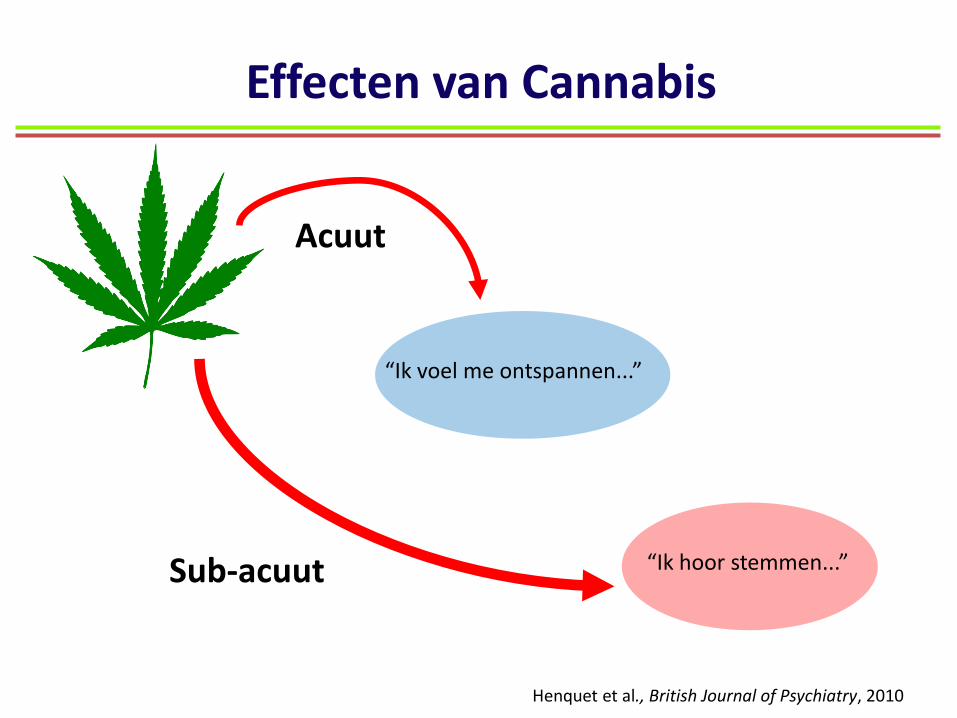
Effecten van Cannabis
“Ik voel me ontspannen...”
“Ik hoor stemmen...”
Henquet et al., British Journal of Psychiatry, 2010

Patienten zijn verhoogd gevoelig voor cannabis
0
0,05
0,1
0,15
0,2
0,25
0,3
E
ffe
ct
Siz
e
(TH
C)
Controles
Patienten
Henquet et al., British Journal of Psychiatry, 2010

Acute reacties als voorspeller
0
20
40
60
No treatment Other psychoticdisorder
Bipolar Sz spectrumdisorder
% o
f case
s a
t fo
llo
w-u
p
Baseline cannabis psychosis
n = 535 incident cases
3-5 year follow-up
Arendt at al., British Journal of Psychiatry, 2005

But Are There Changes in
Schizophrenia Incidence?

Incidence Schizophrenia South-East London, 1965-1997
1
1,2
1,4
1,6
1,8
2
2,2
1965 1997
Rela
tive I
ncid
en
ce
Boydell, van Os, et al., British Journal of Psychiatry, 2003

Incidence Changes?
• Sensitivity of assessment • DSM-IV definitions
• Other risk factors

Minder angst / stress
Meer stemmen
Stress
Als ik drink Ben ik meer relaxed word ik leuk gevonden Als ik cannabis gebruik Ben ik minder angstig Heb ik minder last van stemmen

Behandeling:
• Cognitieve gedragstherapie ?
• Motiverende gespreksvoering ?
• Terugvalpreventie ?
Verwachtingen van gebruik
X

• Adapted from substance use field (Miller and Rollnick, 2001)
• Substance use is not identified by the therapist as being problematic
• Emphasis on helping client to identify the consequences of their substance use (positive or negative)
MOTIVATIONAL INTERVIEWING

Ik weet het niet. Ik zou
wel willen stoppen met
blowen, maar ik denk dat ik
het erg zal gaan missen.
Ja.
Nee, het brengt me niets.
Maar het helpt me wel met mijn
angstige gevoelens. Het
kalmeert me.
Ja. Ik durf dan nog
steeds niet goed naar
buiten, maar voel me
thuis wel rustiger.

Ja, ik wil wel graag
stoppen, maar ik ben
bang dat ik niet zonder
kan.
Ik voelde me minder
achterdochtig toen ik niet
gebruikte. Maar nu ben ik
soms zo paranoide dat ik
moet blowen om te
kunnen slapen. Maar dan
als ik ‘s ochtends wakker
wordt….

The ‘spirit’ of Motivational Interviewing Motivational Interviewing can be described as forming a partnership with the client or patient, within which one’s style is quiet, accepting, attentive, respectfully curious, and directive rather than overtly persuasive. Motivation to change is elicited.
“It’s dancing; not wrestling.” (Jeff Allison)
MOTIVATIONAL INTERVIEWING

M.I. and Motivation
“ M.I. is more than a set of techniques for doing counselling. It is a way of being with clients.”
“ Lack of motivation is not a fault for which to blame your clients: It’s a challenge for your therapeutic skills”
Miller & Rollnick, 1991

Barrowclough et al., Am J Psychiatry, 2001:
• N = 36 patient-caregiver (parents/partners) pairs
• Gender: majority patients were male
• Mean age: 31.1 years
• Mean illness duration: 8.4 years
• Study design: • Randomized to either TAU or integrated therapy (CBT +
MI, family intervention)
• Baseline to 12 months follow-up
EVIDENCE SO FAR…

PRIMARY OUTCOME: GAF score
46
48
50
52
54
56
58
60
62
0m 9m 12m 18m
CBT
N=15
Control
N=14
Global Assessment Functioning at 0, 9, 12, and 18 month p = 0.001
Barrowclough et al., Am J Psychiatry, 2001

Positive symptoms
12
13
14
15
16
17
18
0m 9m 12m 18m
CBT
N=15
Control
N=14
Mean PANSS positive score at 0, 9, 12, and 18 month p > 0.5, n.s
Barrowclough et al., Am J Psychiatry, 2001

10
11
12
13
14
15
16
17
0m 9m 12m 18m
CBT
N=15
Control
N=14
Negative symptoms
Mean PANSS negative score at 0, 9, 12, and 18 month p = 0.028
Barrowclough et al., Am J Psychiatry, 2001

28
29
30
31
32
33
34
0m 9m 12m 18m
CBT
N=15
Control
N=14
Mean PANSS general score at 0, 9, 12, and 18 month p > 0.05, n.s.
General symptoms
Barrowclough et al., Am J Psychiatry, 2001

A first conclusion…
CBT + MI superior to TAU
Treatment needs to be extended or boosters delivered
Barrowclough et al., Am J Psychiatry, 2001

Het is van groot belang om cannabis gebruik onder patiënten met
psychose te behandelen, omdat dit een positief effect heeft op het
ziekteverloop en de klinische outcome significant verbetert.

Further evidence?
Barrowclough et al., BMJ, 2010
N = 327 patients with psychosis and comorbid substance use

Dr. Rebecca Küpper (Maastricht University)
Dr. Monique Konings (GGzEindhoven)
Drs. Maurice Smits (Mondriaan)
Dr. Cécile Henquet (Mondriaan)
Prof. dr. Inez Germeys (Maastricht University)
Prof. dr. Jim van Os (Maastricht University)
Maastrichtse Behandelstudie naar de effecten van M.I. in combinatie met CGT

Study Design
Behandelfase: 24 sessies van 45-60 min over 40 weken (eerste fase MI, tweede fase in combinatie met CGT)
2 booster sessies 5 en 10 weken na afronding van de behandeling
Assessment (incl. GAF, PANSS, BPRS, craving): Meting 1: baseline
Meting 2 en 3: na 12 en na 24 behandelsessies
Meting 4 en 5: 6 maanden na afronding en 12 maanden na afronding
Deelnemers: Patiënten met dubbel diagnose psychose en cannabis gebruik
Gerandomiseerd naar MI+CGT versus TAU (treatment as usual)

Preliminary Results
0
10
20
30
40
50
60
1 2 3 4 5
MI+CBT
TAU
GAF
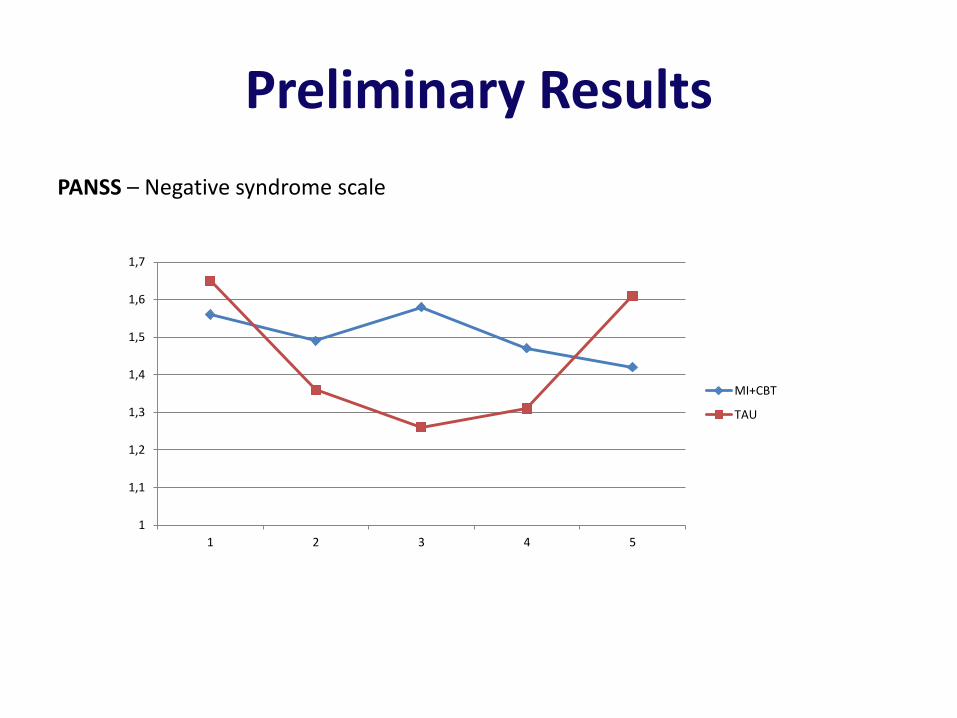
Preliminary Results
PANSS – Negative syndrome scale
1
1,1
1,2
1,3
1,4
1,5
1,6
1,7
1 2 3 4 5
MI+CBT
TAU

1
1,1
1,2
1,3
1,4
1,5
1,6
1,7
1,8
1,9
1 2 3 4 5
MI+CBT
TAU
Preliminary Results
PANSS – Positive syndrome scale

Results: Frequency & amount of cannabis use
Craving for cannabis
No difference in GAF
Psychological Medicine, 2012

A second conclusion…
CBT + MI + family intervention superior to TAU
But: effects rather on substance use, and not on clinical or functional outcome variables

Cannabis gebruik is schadelijk voor de mentale gezondheid,
ongeacht iemands leeftijd of andere risicofactoren. Daarom is het
ook sterk aan te raden om het gebruik van cannabis in de hele
populatie te verminderen.

Thank you for your attention!
Ruud van Winkel, PhD [email protected] Rebecca Kuepper, PhD [email protected]
Maastricht University, Department Psychiatry & Psychology, School for
Mental Health and Neuroscience (MHeNS), Maastricht, The
Netherlands
![af1277 factsheet roken en schizofrenie · 2019-02-07 · Mensen die lijden aan schizofrenie sterven gemiddeld 12-15 jaar jonger dan de algemene bevolking [4]. Schizofrenie veroorzaakt](https://img.pdfslide.net/doc/110x75/5e305bf5eac078442e74cb54/af1277-factsheet-roken-en-schizofrenie-2019-02-07-mensen-die-lijden-aan-schizofrenie.jpg)





























