Embed Size (px)
Citation preview

ROENTGEN DIAGNOSIS OF DIAPHRAGMATIC HERNIA
ARTHUR S. UNGER, M.D. AND M. H. POPPEL, M.D.
Director of Department of Radiology, Associate RoentgenoIogist, Gouverneur Sydenham and Gouverneur HospitaI; Adjunct Roentgenologist,
Hospitals, New York Sydenham Hospital; Assistant in Roentgenology, CoIIege of Medicine,
New York University
NEW YORK CITY
INTRODUCTION
W E are presenting this subject be- cause of the need for a detaiIed roentgenographic outline of differ-
entiaI diagnostic aids which may be of assistance in the earIy cIinica1 diagnosis of the many cases of diaphragmatic hernia that we beIieve escape recognition in the ordinary routine Roentgen examindtion.
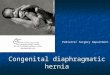
I. Thoracic stomach associated with a short esophagus. (Fig. 3.) This is not a true diaphragmatic hernia because the stomach
CLASSIFICATION
Diaphragmatic hernias may be divided into two types: congenita1 and acquired. GeneraIIy speaking, a diaphragmatic hernia is to be regarded as congenital unti1 proved to be acquired.
The congenita1 type may be sub-divided into :
I. The form which is due to the com- pIete absence of one haIf of the diaphragm. (Fig. I.)
2. The form which is due to a partia1 defect in the muscuIature of one Ieaf of the diaphragm. (Fig. 2.)
3. The form which is due to a congenita1 eniargement of one or more of the dia- phragmatic hiati.
The acquired type may be sub-divided into :
I. The form which is produced by a reIaxation of the various hiatuses of the diaphragm. This type is usuaIIy secondary to an increased intra-abdomina1 pressure.
2. The form which is produced as a resuIt of trauma.
There are two conditions which are so cIoseIy reIated to diaphragmatic hernia, especiaIIy in the differentia1 diagnosis, that we have deemed it important to add them as a coroIIary in the cIass&cation. They are:
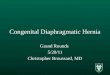
FIG. I. Complete absence of the Ieft diaphragm with colon and stomach in the chest.
has never been a part of the abdomina1 cavity, and has therefore never herniated. Because of the short esophagus, the stomach has developed in the thorax and must obviousIy remain there.
2. Eventration of the diaphragm, with or without an associated megaIo-coIon.
(Fig. 4.)

252 American hrd 0f surgery Unger & Poppel, Diaphragmatic Hernia NOVEMBER. I
CLINICAL INVESTIGATION Iess, there are certain symptoms and sig
We have carefuIIy reviewed the symp- in the cIinica1 picture which are suggesti 3ms and signs that a11 our cases presented of the diagnosis whenever they are preset
937
ins
ive
nt.
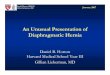
FIG. 2. PartiaI defect in the Ieft diaphragm with the cardiac end of the stomach in the chest.
before Roentgen investigation was insti- tuted. From this study we have concIuded
FIG. 3. Short curved esophagus associated with thoracic stomach. (Courtesy Dr. Heirnan.)
We have found it suitabIe to make a com- posite Iisting of a11 the simiIar cases in our
FIG. 4. Eventration of the left diaphragm.
that there is no cIinica1 syndrome charac- teristic of diaphragmatic hernia. Neverthe-
FIG. 5. Herniation of the cardiac end of the stomach into the left chest through a defect in the Ieft diaphragm.
series and to present these suggestive symptoms and signs in the foIlowing ab-

~~~ sERIEs voL. XXXVIII, No. 1 Unger &LPoppeI, Diaphragmatic Hernia A m&can JOULE 0f surgery 253
stract groups, in order to avoid a Iong
discussion of the individual cases.
I. Any unusuaI marked epigastric dis-
ROENTGEN INVESTIGATION. PART I
Roentgen Technique. CarefuI and thor- ough roentgenoIogic study wiI1 aIways
FIG. 6. A large gastric herniation in a woman of 60.
comfort in a pregnant patient should stimuIate search for an enIarged esophagea1 hiatus and for the herniating viscus.
2. Any gurgling, spIashing, rumbIing or other noises in the chest of a patient, shouId be investigated aIong these lines, especiaIIy if they are exaggerated in the knee-chest position.
3. Any deIay in the onset of respiration in a new-born together with dispIacement of the heart, other respiratory diff&Ities and a persistent cyanosis might be due to a congenita1 hernia.
4. Any secondary anemia, associated with atypica1, equivoca1 or evanescent physica signs in the base of the left chest shouId be investigated with the possibiIity that they may be due to a diaphragmatic hernia or one of the reIated conditions.
FIG. 7. Concentric shadows containing gas in the part of the left chest in a pregnant patient. Barium enema examination proved them to be coIon.
enabIe the examiner to demonstrate dia- phragmatic hernia or any of its reIated conditions, but on the other hand, it wiI1 invariabIy be overIooked unIess it is actuaIIy searched for.
The Roentgen technique shouId incIude the foIIowing : preIiminary ff uoroscopy of the chest during inspiration and expira- tion. This wiI1 visuaIize the extent of the Iung compression and the function therein. If a herniation is present we may see gas and fluid IeveIs. This observation is espe- ciaIIy important if the herniation is strangu- Iated and no barium is abIe to enter the lumen of the invoIved portion.
There shouId be aIso incIuded a compIete ff uoroscopic and Roentgen examination of the esophagus, stomach and smaII intes- tines, empIoying manua1 manipuIation of the abdomen with or without compression. If negative, a barium enema examination of the coIon must be made. It is some- times necessary to have the patient cough or strain in order to demonstrate the lesion.

254 American hrd 0f surgery Unger & PoppeI, Diaphragmatic Hernia NOVEMBER, ,937
CarefuI posturing in the supine, TrendeI- organs in their respective normaI positions, enburg, IateraI recumbent and IateraI up- it wiI1 be necessary to suppIement the right positions is very essentia1 and should usua1 examination with either an intra-
FIG. 8~. Defect in the Ieft diaphragm through which the coton is herniating.
not be negIected in the routine study, as it is onIy in these positions that many of the herniations are demonstrated roentgeno- graphicaIIy. The IateraI views wiI1 show the antero-posterior distribution of both haIves of the diaphragm, simpIyfying the differ- entiation between hernia and eventration. This view is aIso vaIuabIe in demonstrating the absence of one Ieaf of the diaphragm. It must be borne in mind that the greater the degree of eventration the greater wiI1 the muscle of the diaphragm be thinned out, and consequentIy the more diffIcuIt to visuaIize. If a hernia is suspected and a11 the hoIIow abdomina1 organs are in their norma positions, it might be we11 to con- sider a soIid viscus, such as the Iiver, spIeen or kidney, to be the offender. If a flat abdomina1 Mm does not visuaIize these
FIG. 8~. Same case as 8~. Appendix in the Ieft chest.
venous injection of a smaI1 amount of thorotrast for the visuaIization of the Iiver and spIeen, or with a retrograde pyeIo- graphic study using one of the urographic contrast media in a greater concentration than is ordinariIy used, for the purpose of demonstrating whether the position of the kidney is norma or ectopic.
ROENTGEN INVESTIGATION. PART II
Roentgen observations necessary for diagnosis.
The Roentgen examination must demon- strate the foIIowing if an earIy ‘and accurate diagnosis is to be established:
Type and Site of Herniation. It may not aIways be possibIe to demonstrate the type or the site of the herniation. Whenever possibIe the observation should be incIuded

~~~ sBRIEs voL. XXXVIII, No. 1 Unger & Poppei, Diaphragmatic Hernia A merican Journal 0f surgery 255
in the report as it aids the surgeon in mak- case associated with thoracic stomach, ing his decision for the operative approach. the stomach or duodenum may use this
Contents of the Herniation. AImost a11 means of entering the abdomen.
FIG. 9. Demonstration of gastric rugae above the Ieft diaphragm.
the abdomina1 organs except the rectum, urinary bIadder and uterus have been found in the herniation.
FIG. IO. Herniation of the cardiac end of the stomach with a secondary proved maIignancy in the her-
Reducibility of the Herniation. It must niated portion. There is a titling defect with dis-
be determined whether the herniation is tortion of the rugae. (Courtesy Dr. Stone.)
fixed or whether it can be reduced. It may Diaphragms. We must study the struc- be possibIe to fiI1 the herniation with ture, reIative positions, shape, contour barium if there is a stranguIation at the and movements of the diaphragms in neck of the herniation. NevertheIess, the order to determine their presence or diagnosis may be suggested by the con- absence, or the possibiIity of an eventra- centric ectopic shadows containing gas and tion or other defect. fluid IeveIs situated above the diaphragm. Costa-phrenic Spaces. We must deter-
Length of the Esophagus. This observa- mine the size, shape and iIIumination of tion is very important, as it expIains why these spaces, in order to ruIe out the the stomach is in the thorax when the presence therein of any dispIaced viscera. esophagus is short. This aIso enabIes the Associated Pathology. It is necessary to surgeon to avoid interference in the short demonstrate any associated pathoIogy in esophagus type of case. addition to the presence of a diaphragmatic
Size of the Esophageal Hiatus. It must hernia or a reIated condition. The foIIow- be demonstrated whether the hiatus is ing conditions may be found associated: norma or whether it is congenitaIIy or I. EsophageaI uIceration. The esoph- otherwise enIarged. If the enlargement is agea rugae are examined after the method acquired, it shouId be shown whether it is of Berg as practised by HoImes and Schat- due to a pregnancy or to some other intra- ski in this country. If the result is not abdomina1 increase in pressure. It is aIso satisfactory such as in the cases where important to know what passes the hiatus there are shaIIow erosions instead of because in the short esophagus type of uIcerations, the examiner shouId seek the

236 A merican ~~~~~~~ or surgery Unger & Popped, Diaphragmatic Hernia NOVEMBER, rye,
FIG. IIA. Herniation through an enIarged FIG. I IB. Same case as I IA. DuodenaI uIcer seen esophagea1 hiatus. in relief.
FIG. 12~. Large carcinoma in the sigmoid with Iarge bowe1 obstruction.
FIG. 12~. Same case as 12~. SmaII bowel obstruc- tion secondary to the sigmoid carcinoma.

NEW SERIES VOL. XXXVIII, No. 2 Unger & PoppeI, Diaphragmatic Hernia A m&can Journal of Surgery 257
aid of esophagoscopy. Manges and CIerf were abIe to observe eight cases in such a way.
sigmoid mahgnancy which had perforated into a Ioop of iIeum and as a resuIt there had been produced both smaI1 and Iarge
FIG. I zc. Same case as I 2~. Herniation of the cardiac end into the Ieft chest as a result of the increased intra-abdominal pressure.
2. Gastric malignancy. We have en- countered a case where the cardiac portion of the stomach which was herniated into the Ieft chest, presented a Iarge fiIIing defect with distortion of the rugae, both characteristic of maIignancy. Both condi- tions are visuaIized on the iIIustration. Later the findings were confirmed by operation. We believe that the association was mereIy a coincidence and not reIated to each other etioIogicaIIy.
3. DuodenaI uIcer. In this instance the uIcer was responsibIe for the symptoms and was consequentIy deserving of the treatment rather than the herniation which was the accidenta finding.
4. Large bowel mahgnancy. We have encountered a case where the cardiac portion of the stomach was herniated into the Ieft chest, through a defect in the Ieft diaphragm as a resuIt of a tremendous increase in the intra-abdomina1 pressure. This increased pressure was produced by a
FIG. 13. Encysted pIeural fluid resembling stomach in the chest.
boweIobstruction. In the roentgen routine of the gastro-intestina1 examination the gastric herniation was found before the associated pathoIogy in the smaI1 and Iarge intestine.
5. Inffammation, as for exampIe in the appendix. It is very important to know the position of the appendix on account of the possibiIity of the occurrence of an acute appendicitis. In one of our cases, the appendix was visuaIized in the Ieft chest. This information wiI1 aid in accurate diagnosis and provide the surgeon with sufficient data to enabIe him to make a proper incision.
6. Secondary Iung changes. The Iung wiI1 be compressed and ateIectatic in proportion to the size of the herniation. It is very important to know the extent of the Iung damage, and to avoid any erroneous interpretation of this change.
ROENTGEN INVESTIGATION. PART III
Special Roentgen Features. The foI- Iowing Roentgen signs are especiaIIy sug-

258 A merican ~~~~~~~ or surgery Unger & PoppeI, Diaphragmatic Hernia NOVEMBER, 193,
gestive of the diagnosis and when present and have demonstrated that the Roentgen shouId stimuIate further study. examination offers the onIy concIusive
I. The persistent absence of the stomach pre-operative proof of its existence.
FIG. 14. A loop of coIon between the right diaphragm and the upper border of the liver, resembhng a diaphragmatic hernia cIinicaIIy.
gas bubbIe (magenbIase) is very suggestive of the presence of a diaphragmatic hernia, especiaIIy so if cardiospasm has been ruled out.
2. The presence of inspiratory eIevation of one side of the diaphragm (paradoxica1 movement) is suggestive of an eventration of the diaphragm, especiaIIy so if there is aIs present a megaIocoIon.
3. The Roentgen visuaIization of any concentric shadows resembIing stomach or intestine-with or without gas or fIuid IeveIs, situated above the diaphragm, is suspicious of the diagnosis, especiaIIy so if the heart is dispIaced toward the opposite side.
4. Any apparent benign stenosis in the Iower part of the esophagus shouId be investigated with the possibiIity of its being the esophago-gastric junction in a case of a congenitaIIy short esophagus.
CONCLUSIONS
We have stressed the importance of the earIy recognition of diaphragmatic hernia,
It is hoped that the discussion herein presented wiI1 in the future enable the cIinician and the roentgenoIogist to detect diaphragmatic hernia and its reIated condi- tions more readiIy than in the past, thereby providing a causa1 reIationship to a group of variabIe symptoms and signs which have heretofore gone unexpIained for Iong periods of time.
AccordingIy, we wouId Iike to stress that there must be cIose cooperation between the cIinician and the roentgenoIo- gist if accurate and earIy diagnoses are to be made.
REFERENCES
I. MANGES, W. F. and CLERF, L. H. Congenital AnomaIies of the G.I. Tract. Am. J. Roentgenol. ti Radium Tberapy., 33: 5; 650-668.
2. UNGER, ARTHUR S. and POPPEL, M. H. Diaphrag
matic Hernia. Am. J. Roentgenol. CY Radium
Therapy., 37: 4; 472-478. 3. UNGER, ARTHUR S. and SPEISER, M. D. Congenital
Diaphragmatic Hernia. Am. J. Roentgenol. u Radium Tberapy.. 15: 135-143.