Embed Size (px)
Citation preview

Role of Etericoxib in Chronic Pain Management “ Balance Efficacy and Safety”
dr. Alif Noeriyanto Rahman, Sp.OT, FIPM, FIPP, CIPS
Secretary General PERDINI
Educational Program Coordinator PRECURSOR FK UNPAD
Head DOPIC Sentra Medika Cisalak Depok

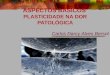
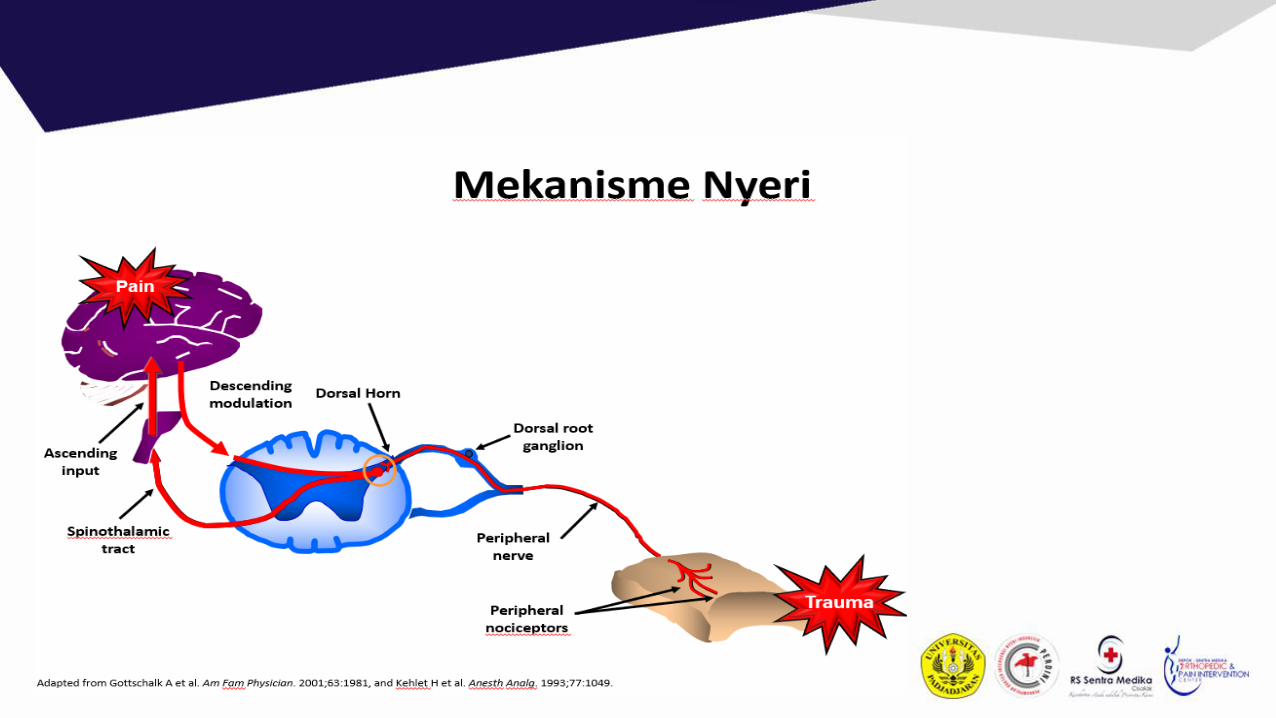
Time-based classification of pain
• Acute: short-term; usually due to nociception (tissue damage); resolves with healing.
• In back pain, Acute = < 4 wks
Sub-acute = 4-12 weeks
Chronic = > 12 weeks
• Chronic pain: pain lasting > 3-6 months
• Persisting pain (NHMRC: acute pain guidelines)
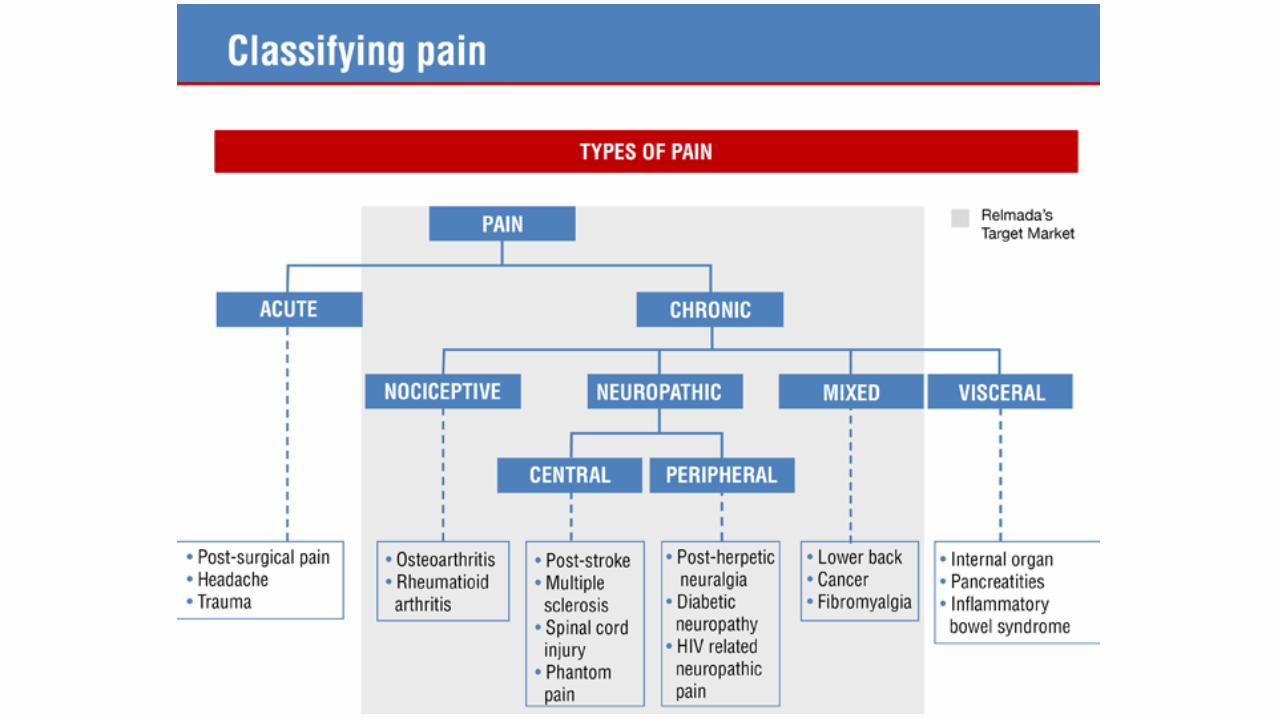
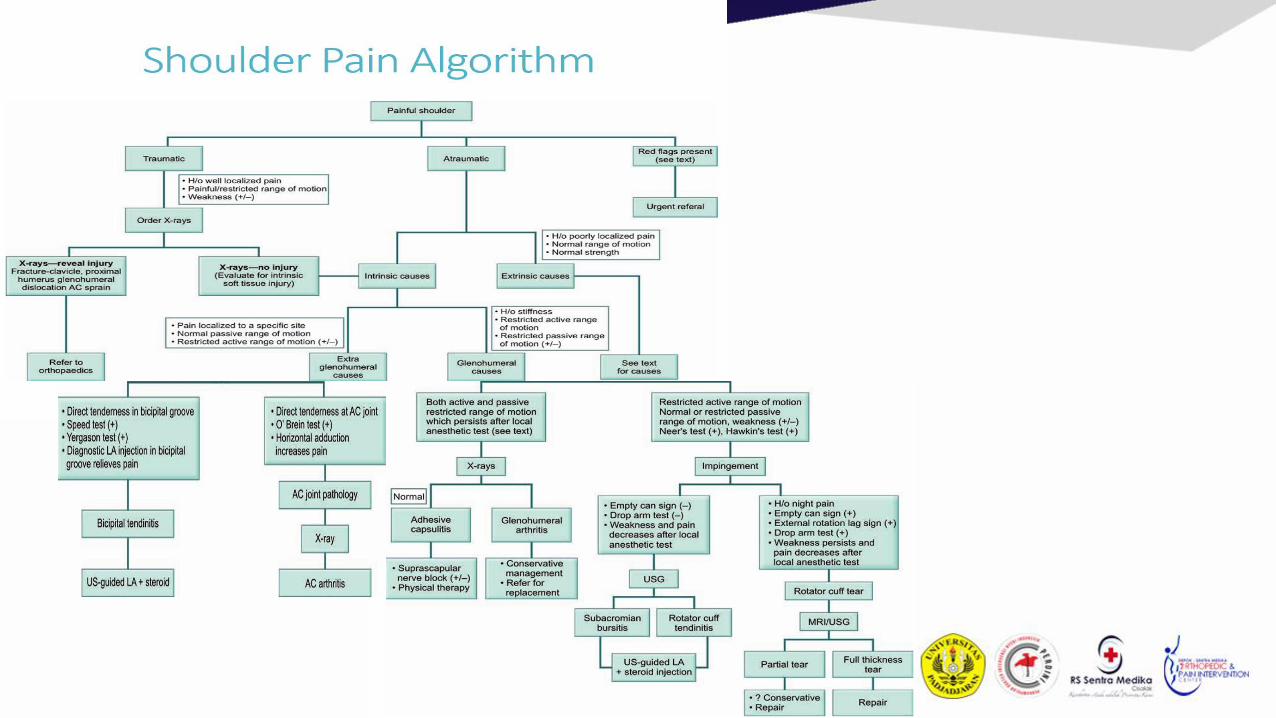
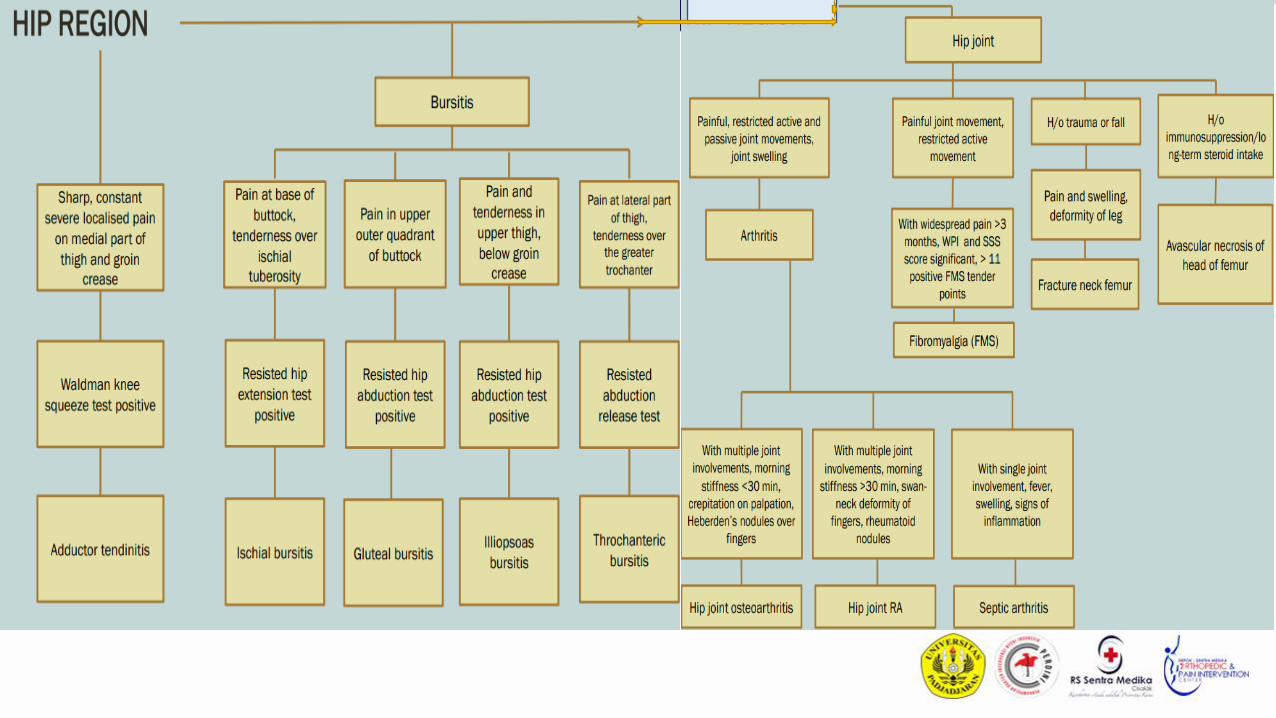
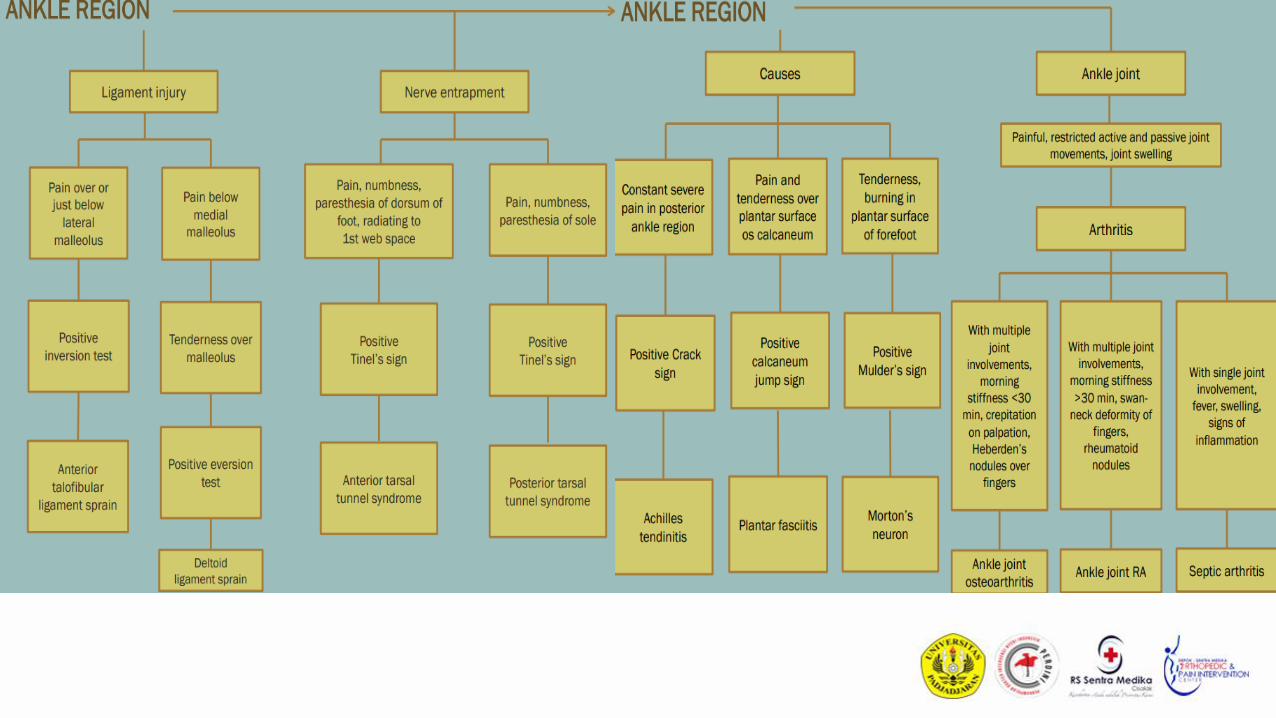
Soft tissues- tendinitis
- bursitis
- myofascial pain
- nerve entrapment
Bone
Non/mild Inflammation
Monoarthritis Polyarthritis
Non Articular
Osteoarthritis•Gout
•Trauma
•Septic
• RA
• SLE
• AS
• PsA
• Reiter’s
Musculoskeletal Pain
Articular
Inflammation
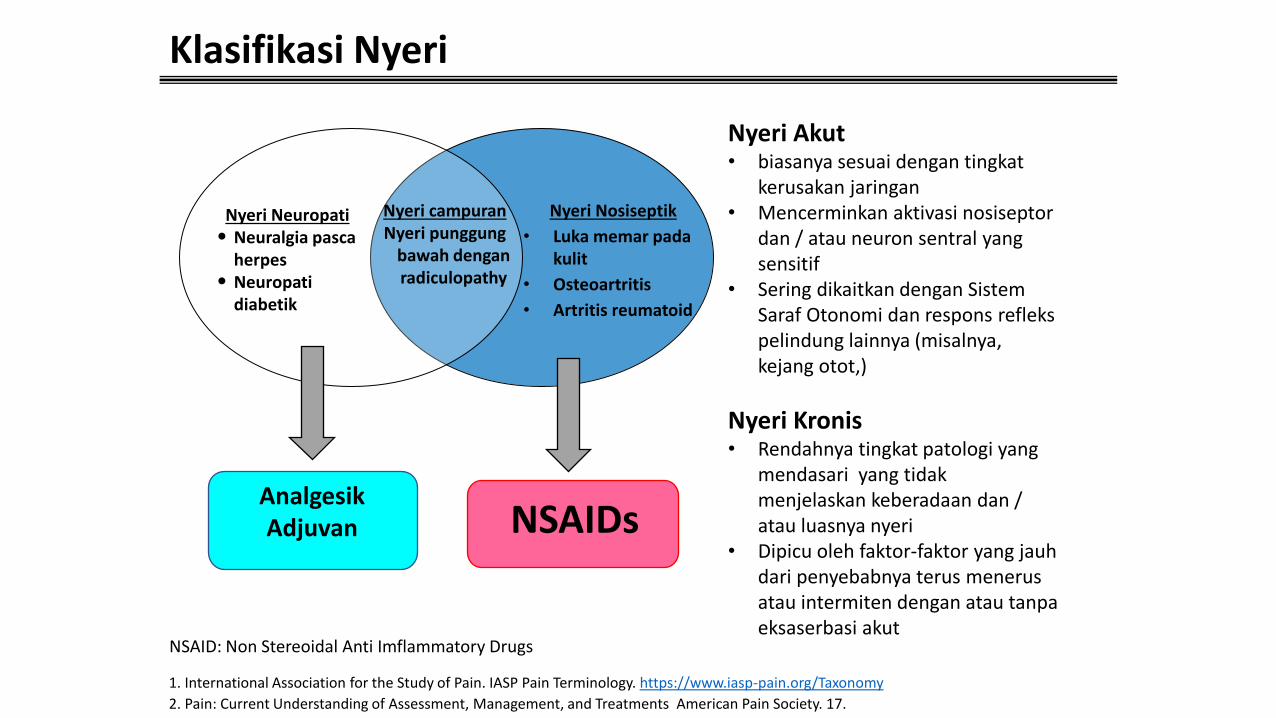
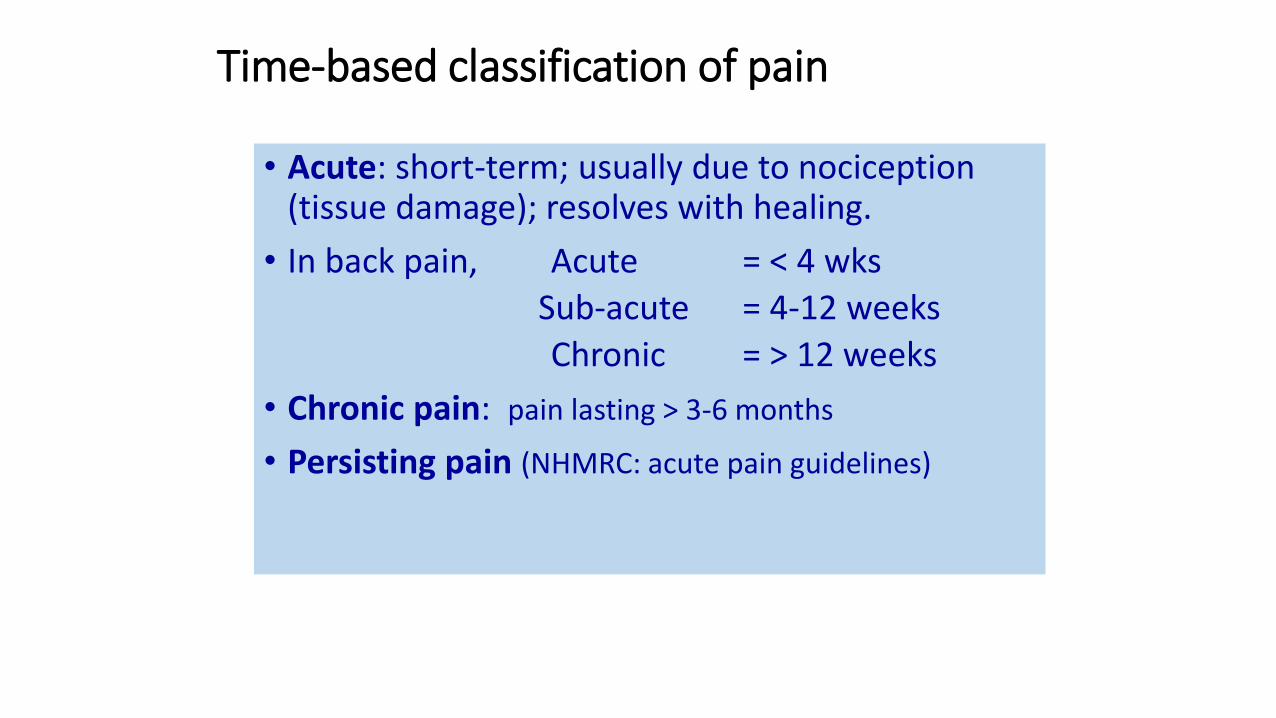
Klasifikasi Nyeri
1. International Association for the Study of Pain. IASP Pain Terminology. https://www.iasp-pain.org/Taxonomy
2. Pain: Current Understanding of Assessment, Management, and Treatments American Pain Society. 17.
NSAIDsAnalgesikAdjuvan
Nyeri campuranNyeri punggung
bawah denganradiculopathy
Nyeri Neuropati• Neuralgia pasca
herpes• Neuropati
diabetik
Nyeri Nosiseptik
• Luka memar pada kulit
• Osteoartritis
• Artritis reumatoid
Nyeri Akut• biasanya sesuai dengan tingkat
kerusakan jaringan• Mencerminkan aktivasi nosiseptor
dan / atau neuron sentral yang sensitif
• Sering dikaitkan dengan SistemSaraf Otonomi dan respons reflekspelindung lainnya (misalnya, kejang otot,)
Nyeri Kronis• Rendahnya tingkat patologi yang
mendasari yang tidakmenjelaskan keberadaan dan / atau luasnya nyeri
• Dipicu oleh faktor-faktor yang jauhdari penyebabnya terus menerusatau intermiten dengan atau tanpaeksaserbasi akut
NSAID: Non Stereoidal Anti Imflammatory Drugs
Fine PG, et al. J Support Oncol. 2004;2(suppl 4):5-22.
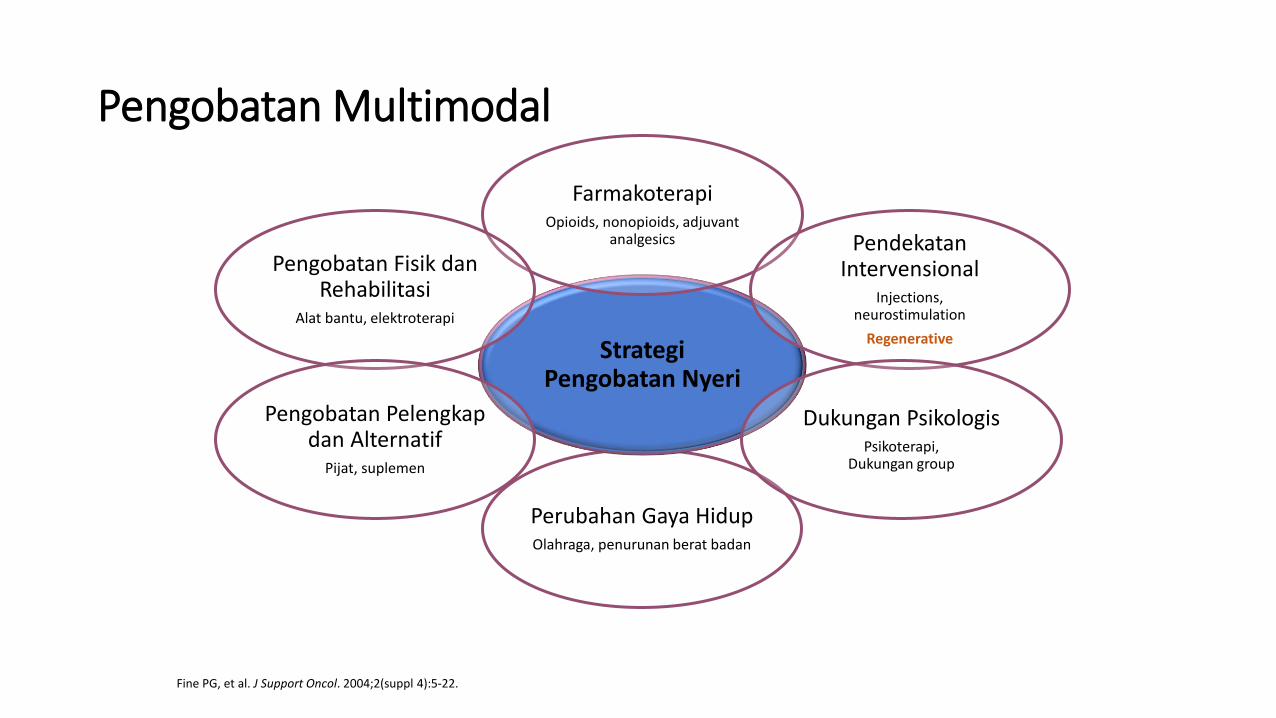
Pengobatan Multimodal
Perubahan Gaya HidupOlahraga, penurunan berat badan
StrategiPengobatan Nyeri
FarmakoterapiOpioids, nonopioids, adjuvant
analgesics PendekatanIntervensional
Injections, neurostimulation
Regenerative
Pengobatan Fisik danRehabilitasi
Alat bantu, elektroterapi
Dukungan PsikologisPsikoterapi,
Dukungan group
Pengobatan Pelengkapdan Alternatif
Pijat, suplemen
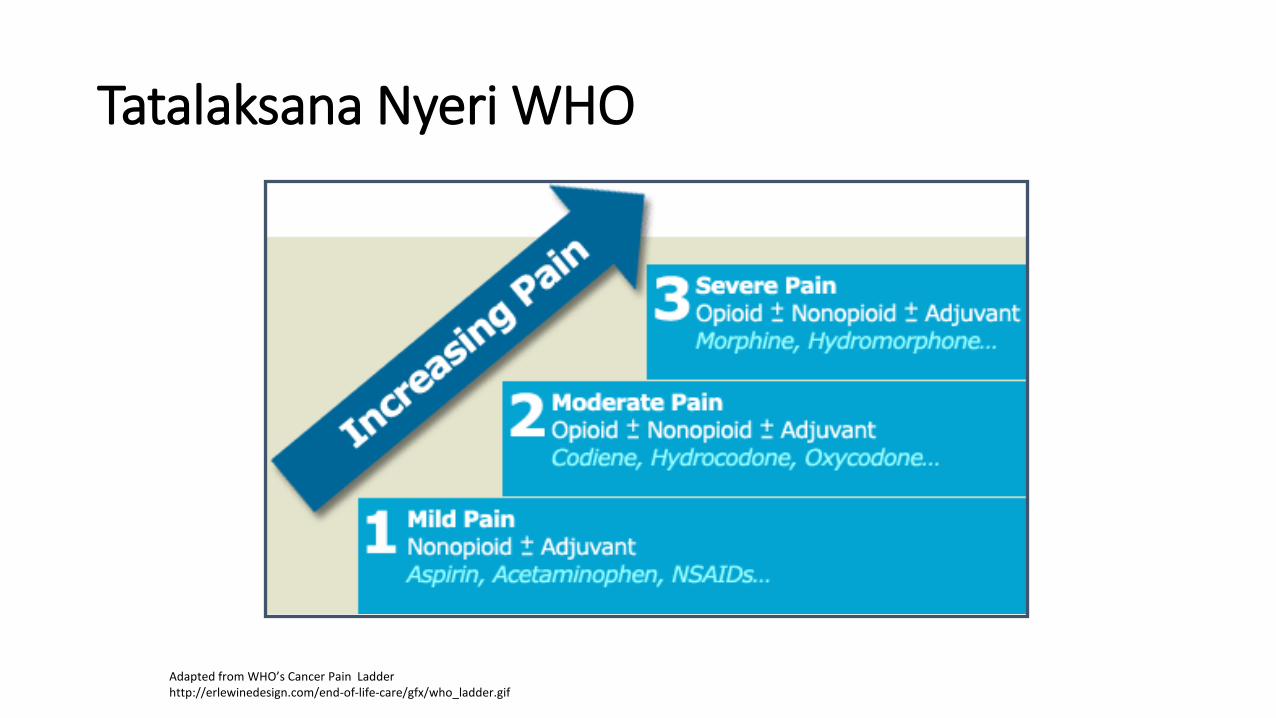
Tatalaksana Nyeri WHO
Adapted from WHO’s Cancer Pain Ladderhttp://erlewinedesign.com/end-of-life-care/gfx/who_ladder.gif
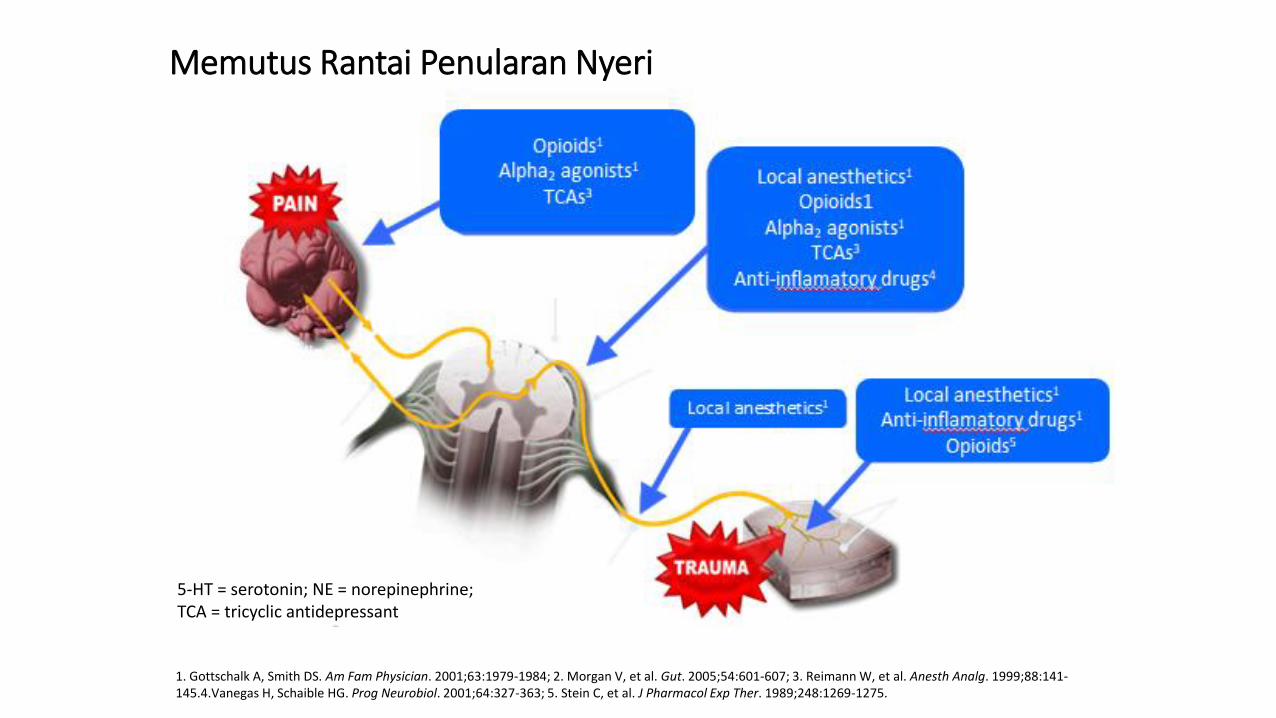
1. Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-1984; 2. Morgan V, et al. Gut. 2005;54:601-607; 3. Reimann W, et al. Anesth Analg. 1999;88:141-145.4.Vanegas H, Schaible HG. Prog Neurobiol. 2001;64:327-363; 5. Stein C, et al. J Pharmacol Exp Ther. 1989;248:1269-1275.
Memutus Rantai Penularan Nyeri
5-HT = serotonin; NE = norepinephrine; TCA = tricyclic antidepressant
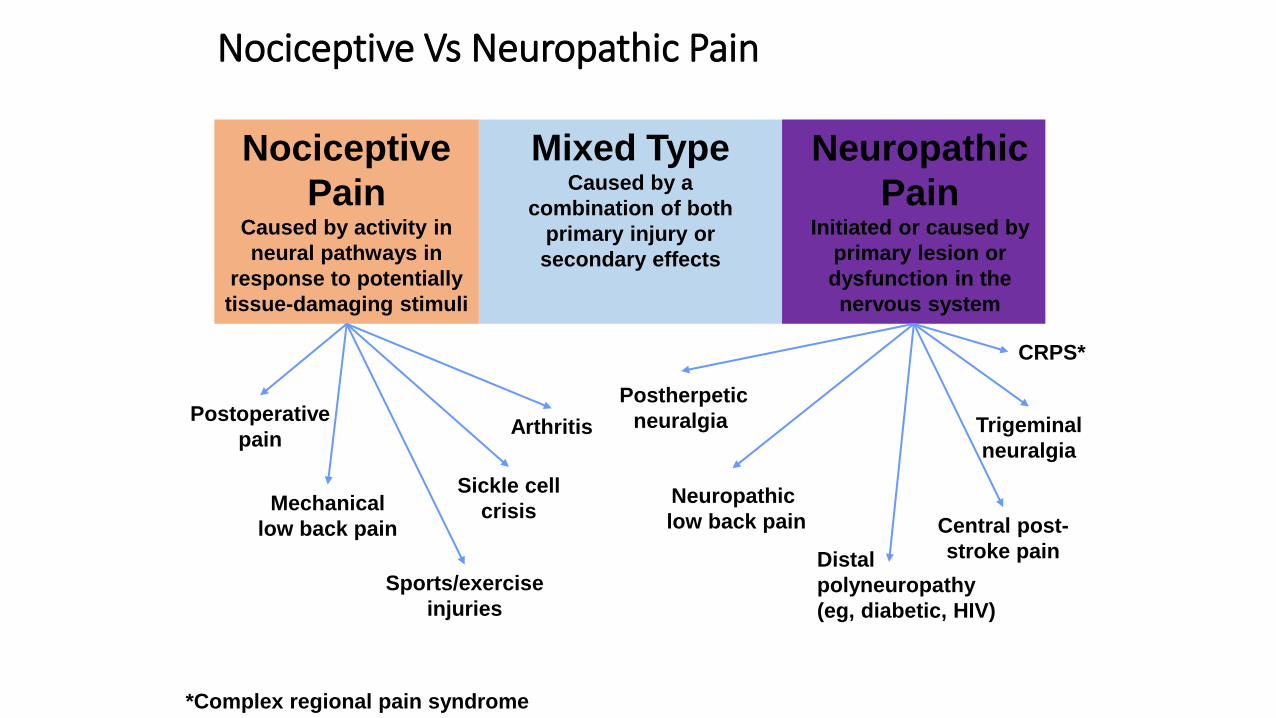
Nociceptive Vs Neuropathic Pain
Mixed TypeCaused by a
combination of both
primary injury or
secondary effects
Nociceptive
PainCaused by activity in
neural pathways in
response to potentially
tissue-damaging stimuli
Neuropathic
PainInitiated or caused by
primary lesion or
dysfunction in the
nervous system
Postoperative
pain
Mechanical
low back pain
Sickle cell
crisis
Arthritis
Postherpetic
neuralgia
Neuropathic
low back pain
CRPS*
Sports/exercise
injuries
*Complex regional pain syndrome
Central post-
stroke pain
Trigeminal
neuralgia
Distal
polyneuropathy
(eg, diabetic, HIV)
What is the “Best Way” to manage pain?
• FIRST, DO NO HARMTherefore, the “best way” is a BALANCE
Patient Safety
Effective Analgesic
Modalities
LandMark and Image Guided Injection• Research about accuracy of needle placement in MSK injecion
• 1948-2000 : 17 studies
• 2000-2010 : 92 studies
• Visualization and palpation of anatomical landMark
The Way Of Thinking




Powerful Efficacy of Etoricoxib in Pain Management
26
THE POWER STUDYEtoricoxib improves pain, function and quality of life:
result of a real-world effectiveness trialH. Y. LIN, et al., International Journal of Rheumatic
Disease, 2010
Study The POWER
• Suatu multicenter, prospective, open-label, single arm, selama 4 minggupada pasien OA.
• Pasien OA yang memakai NSAID atau analgesik lain dialihkan langsung keetoricoxib 60 mg sekali sehari selama 4 minggu tanpa “Wash out” sebelumnya..
• Tujuan utama : Untuk mendemonstrasikan efektivitas etoricoxib dalammanajemen pasien OA dengan kontrol nyeri suboptimal setelahmenggunakan terapi standar (NSAID, Cox-2, acetaminophen, dll) → diukurberdasarkan proporsi pasien dengan respons yang signifikan secara klinis(pengurangan VAS nyeri ≥30%) setelah studi pengobatan obat selama 4 minggu.
H. Y. LIN, et al., International Journal of Rheumatic Disease, 2010
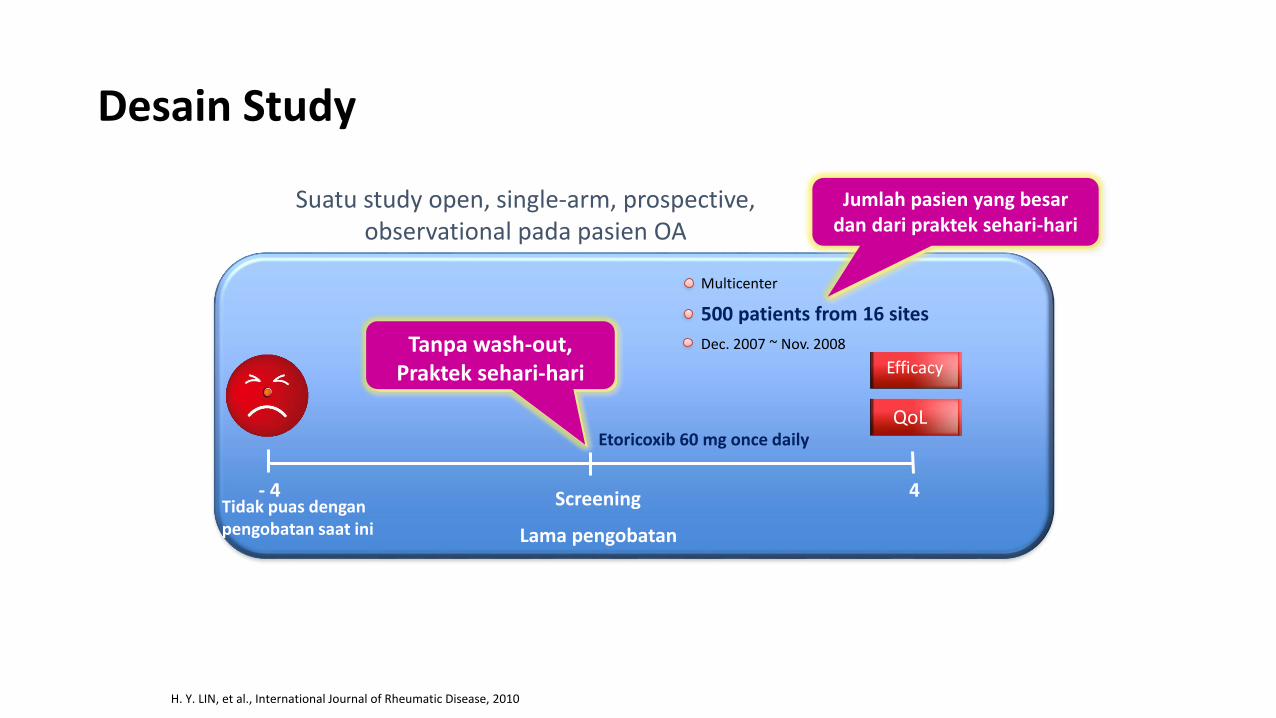
Suatu study open, single-arm, prospective, observational pada pasien OA
Tidak puas denganpengobatan saat ini
Etoricoxib 60 mg once daily
Screening 4
Lama pengobatan
- 4
Multicenter
500 patients from 16 sites
Dec. 2007 ~ Nov. 2008
Efficacy
QoL
Tanpa wash-out,Praktek sehari-hari
Jumlah pasien yang besardan dari praktek sehari-hari
Desain Study
H. Y. LIN, et al., International Journal of Rheumatic Disease, 2010
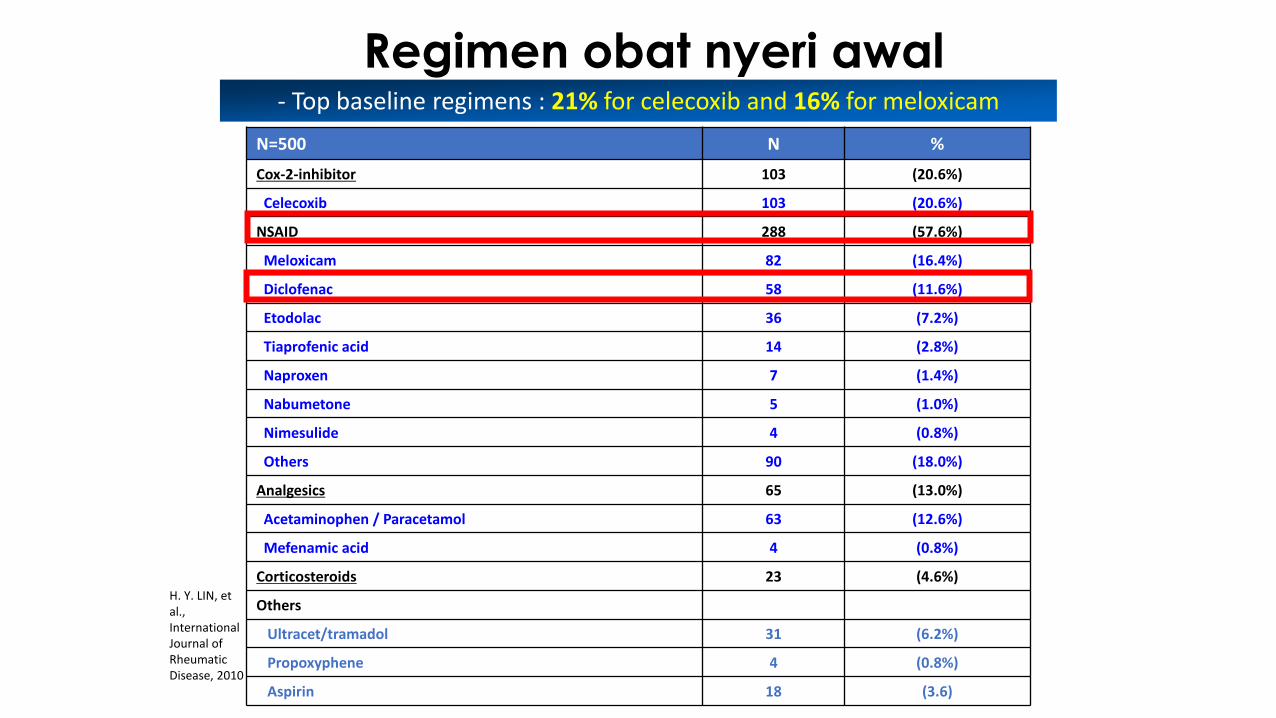
Regimen obat nyeri awal
N=500 N %
Cox-2-inhibitor 103 (20.6%)
Celecoxib 103 (20.6%)
NSAID 288 (57.6%)
Meloxicam 82 (16.4%)
Diclofenac 58 (11.6%)
Etodolac 36 (7.2%)
Tiaprofenic acid 14 (2.8%)
Naproxen 7 (1.4%)
Nabumetone 5 (1.0%)
Nimesulide 4 (0.8%)
Others 90 (18.0%)
Analgesics 65 (13.0%)
Acetaminophen / Paracetamol 63 (12.6%)
Mefenamic acid 4 (0.8%)
Corticosteroids 23 (4.6%)
Others
Ultracet/tramadol 31 (6.2%)
Propoxyphene 4 (0.8%)
Aspirin 18 (3.6)
- Top baseline regimens : 21% for celecoxib and 16% for meloxicam
H. Y. LIN, et al., International Journal of Rheumatic Disease, 2010
70.00%
60.00%
50.00%
40.00%
30.00%
20.00%
10.00%
0.00%
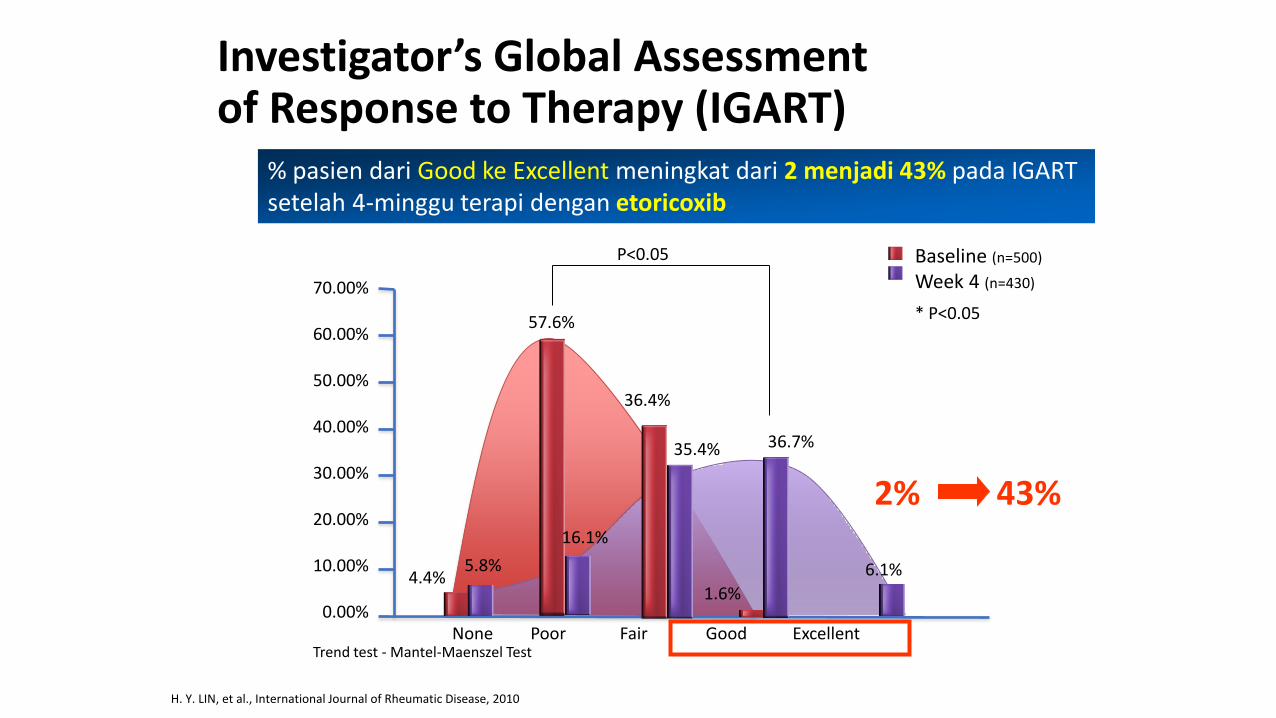
4.4%
None Poor Fair Good Excellent
Baseline (n=500)
Week 4 (n=430)
* P<0.05
5.8%
57.6%
16.1%
36.4%
35.4%
1.6%
36.7%
6.1%
Trend test - Mantel-Maenszel Test
2% 43%
P<0.05
% pasien dari Good ke Excellent meningkat dari 2 menjadi 43% pada IGARTsetelah 4-minggu terapi dengan etoricoxib
Investigator’s Global Assessment of Response to Therapy (IGART)
H. Y. LIN, et al., International Journal of Rheumatic Disease, 2010
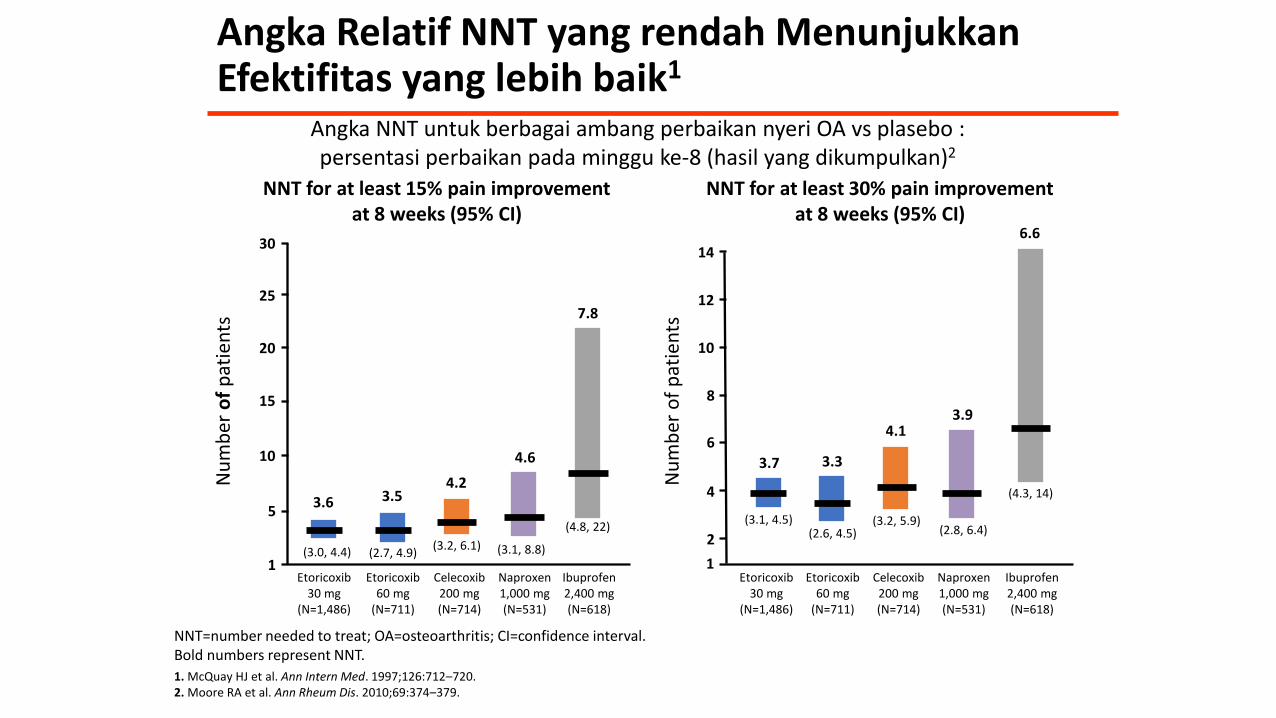
Angka Relatif NNT yang rendah MenunjukkanEfektifitas yang lebih baik1
NNT=number needed to treat; OA=osteoarthritis; CI=confidence interval.Bold numbers represent NNT.
1. McQuay HJ et al. Ann Intern Med. 1997;126:712–720.2. Moore RA et al. Ann Rheum Dis. 2010;69:374–379.
Angka NNT untuk berbagai ambang perbaikan nyeri OA vs plasebo :persentasi perbaikan pada minggu ke-8 (hasil yang dikumpulkan)2
Etoricoxib30 mg
(N=1,486)
Etoricoxib60 mg
(N=711)
Celecoxib200 mg(N=714)
Naproxen1,000 mg(N=531)
Ibuprofen2,400 mg(N=618)
Etoricoxib30 mg
(N=1,486)
Etoricoxib60 mg
(N=711)
Celecoxib200 mg(N=714)
Naproxen1,000 mg(N=531)
Ibuprofen2,400 mg(N=618)
(3.2, 6.1)(3.0, 4.4) (2.7, 4.9) (3.1, 8.8)
(4.8, 22) (3.2, 5.9)(3.1, 4.5)(2.6, 4.5) (2.8, 6.4)
(4.3, 14)
1
5
10
15
20
25
3014
2
4
6
8
10
1
12
3.6 3.54.2
4.6
7.8
6.6
3.94.1
3.7 3.3
Nu
mb
ero
f p
atie
nts
Nu
mb
er o
f p
atie
nts
NNT for at least 15% pain improvementat 8 weeks (95% CI)
NNT for at least 30% pain improvementat 8 weeks (95% CI)
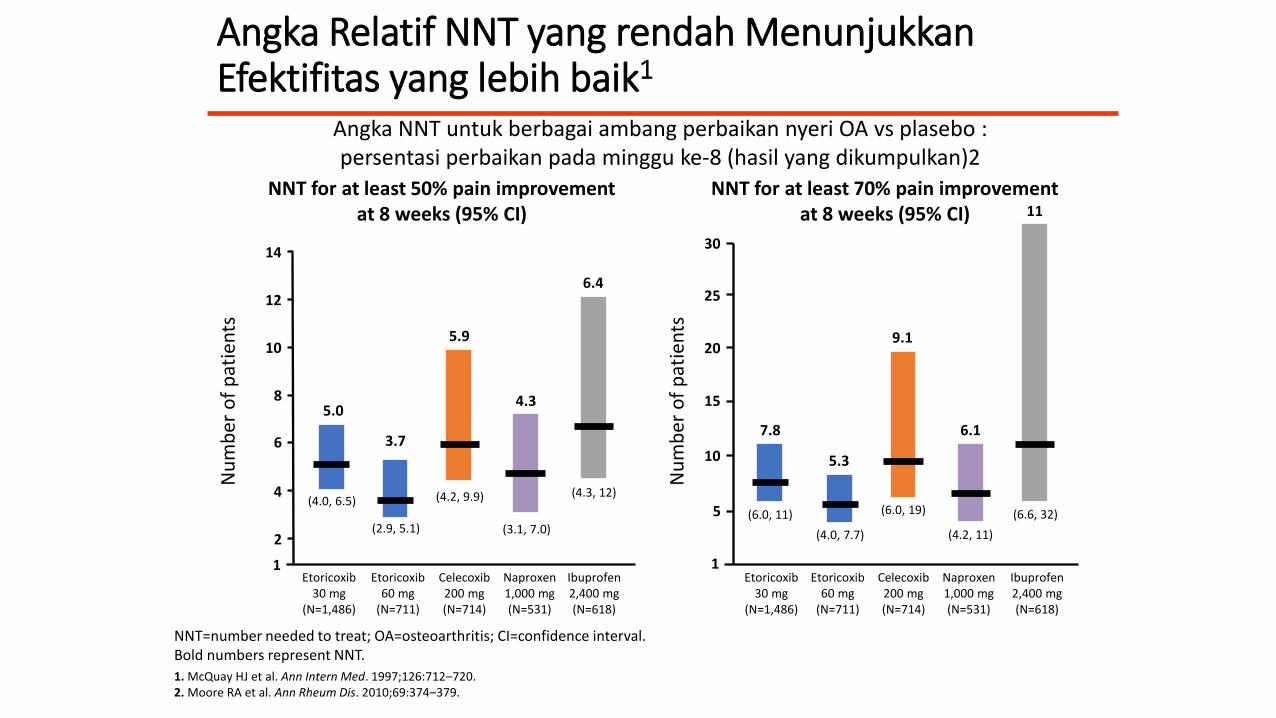
Angka Relatif NNT yang rendah MenunjukkanEfektifitas yang lebih baik1
(6.0, 19)(6.0, 11)
(4.0, 7.7) (4.2, 11)
(6.6, 32)
(4.2, 9.9)(4.0, 6.5)
(2.9, 5.1) (3.1, 7.0)
(4.3, 12)
7.8
5.3
9.1
6.1
11
6.4
4.3
5.9
5.0
3.7
Angka NNT untuk berbagai ambang perbaikan nyeri OA vs plasebo :persentasi perbaikan pada minggu ke-8 (hasil yang dikumpulkan)2
NNT for at least 50% pain improvementat 8 weeks (95% CI)
NNT for at least 70% pain improvementat 8 weeks (95% CI)
Nu
mb
er o
f p
atie
nts
Nu
mb
er o
f p
atie
nts
Etoricoxib30 mg
(N=1,486)
Etoricoxib60 mg
(N=711)
Celecoxib200 mg(N=714)
Naproxen1,000 mg(N=531)
Ibuprofen2,400 mg(N=618)
Etoricoxib30 mg
(N=1,486)
Etoricoxib60 mg
(N=711)
Celecoxib200 mg(N=714)
Naproxen1,000 mg(N=531)
Ibuprofen2,400 mg(N=618)
1 1
5
10
15
20
25
3014
2
4
6
8
10
12
NNT=number needed to treat; OA=osteoarthritis; CI=confidence interval.Bold numbers represent NNT.
1. McQuay HJ et al. Ann Intern Med. 1997;126:712–720.2. Moore RA et al. Ann Rheum Dis. 2010;69:374–379.
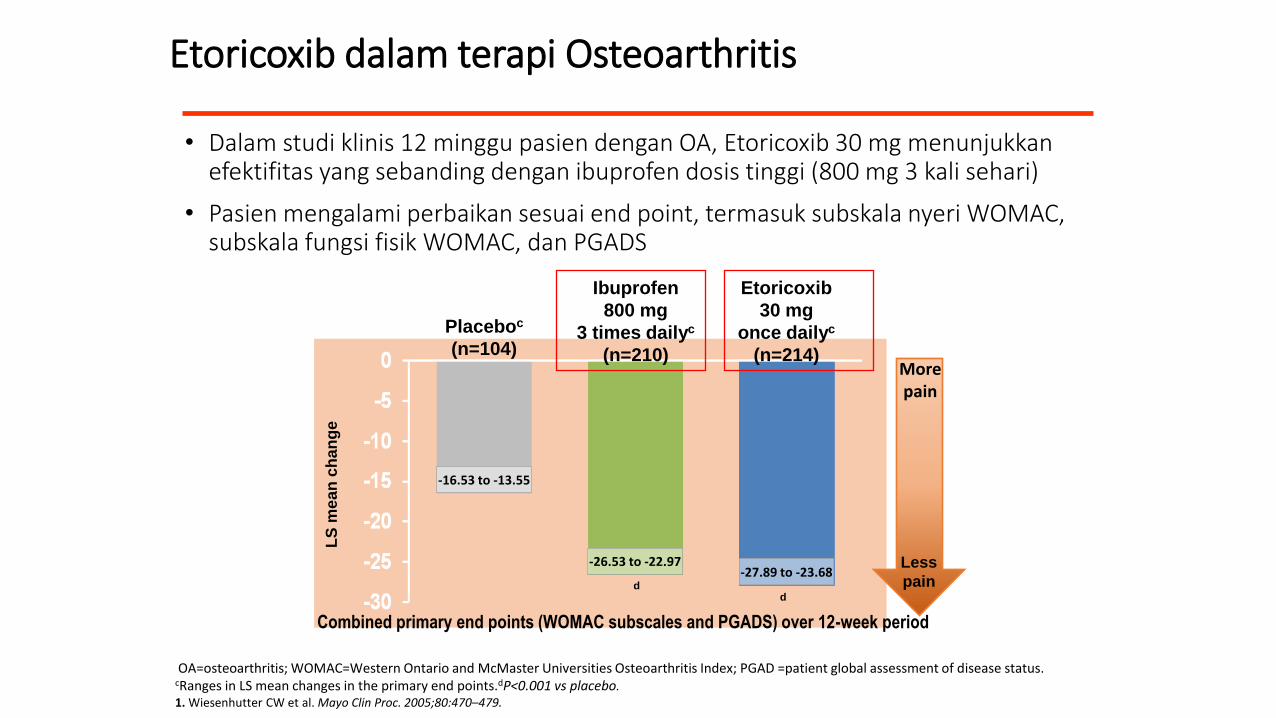
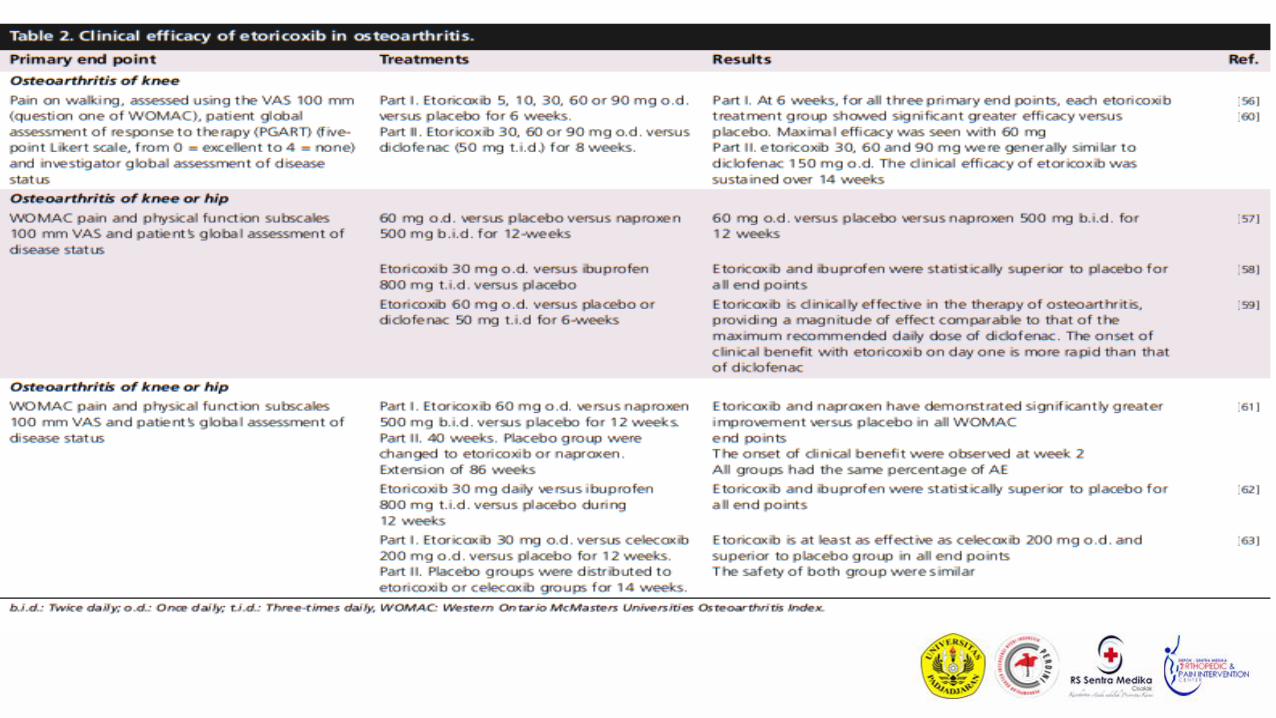
• Dalam studi klinis 12 minggu pasien dengan OA, Etoricoxib 30 mg menunjukkanefektifitas yang sebanding dengan ibuprofen dosis tinggi (800 mg 3 kali sehari)
• Pasien mengalami perbaikan sesuai end point, termasuk subskala nyeri WOMAC, subskala fungsi fisik WOMAC, dan PGADS
Etoricoxib dalam terapi Osteoarthritis
Placeboc
(n=104)
Ibuprofen
800 mg
3 times dailyc
(n=210)
Etoricoxib
30 mg
once dailyc
(n=214)
-16.53 to -13.55
-26.53 to -22.97-27.89 to -23.68
LS
me
an
ch
an
ge
dd
Morepain
Less
pain
Combined primary end points (WOMAC subscales and PGADS) over 12-week period
OA=osteoarthritis; WOMAC=Western Ontario and McMaster Universities Osteoarthritis Index; PGAD =patient global assessment of disease status.cRanges in LS mean changes in the primary end points.dP<0.001 vs placebo.1. Wiesenhutter CW et al. Mayo Clin Proc. 2005;80:470–479.
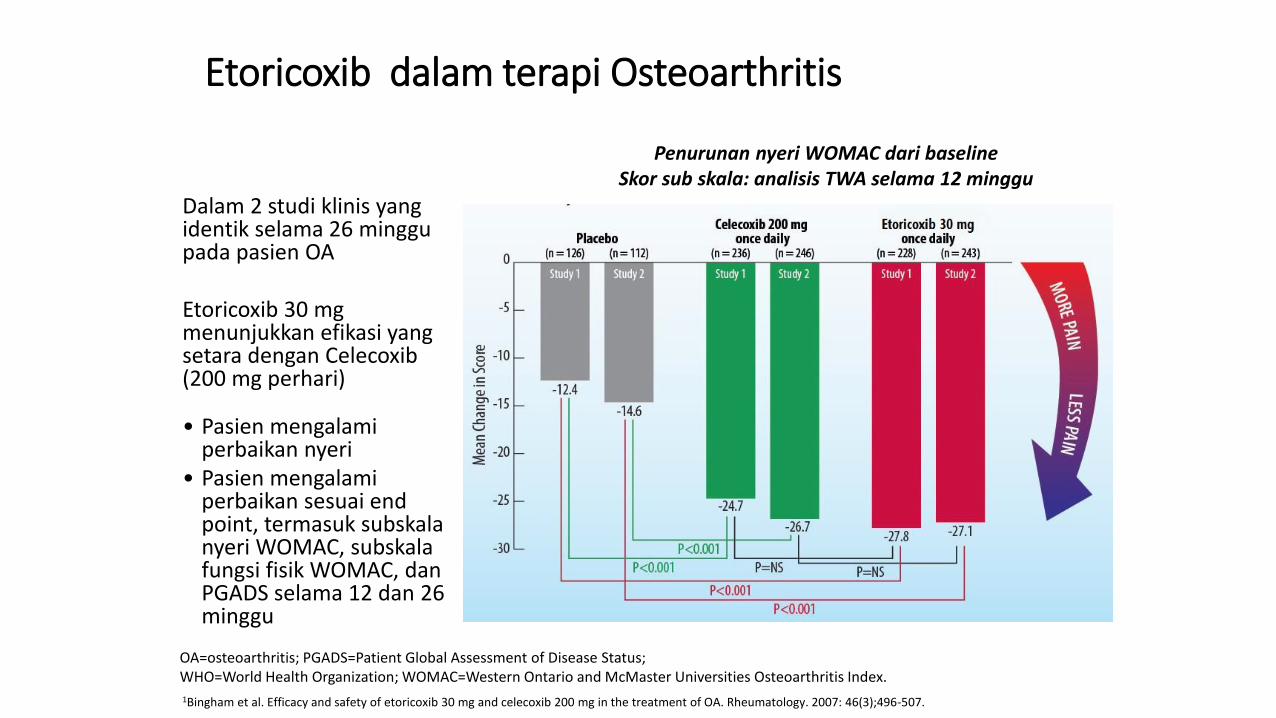
Dalam 2 studi klinis yang identik selama 26 minggupada pasien OA
Etoricoxib 30 mg menunjukkan efikasi yang setara dengan Celecoxib(200 mg perhari)
• Pasien mengalamiperbaikan nyeri
• Pasien mengalamiperbaikan sesuai end point, termasuk subskalanyeri WOMAC, subskalafungsi fisik WOMAC, danPGADS selama 12 dan 26 minggu
In a Study of Patients with Osteoarthritis
Penurunan nyeri WOMAC dari baselineSkor sub skala: analisis TWA selama 12 minggu
1Bingham et al. Efficacy and safety of etoricoxib 30 mg and celecoxib 200 mg in the treatment of OA. Rheumatology. 2007: 46(3);496-507.
Etoricoxib dalam terapi Osteoarthritis
OA=osteoarthritis; PGADS=Patient Global Assessment of Disease Status;WHO=World Health Organization; WOMAC=Western Ontario and McMaster Universities Osteoarthritis Index.
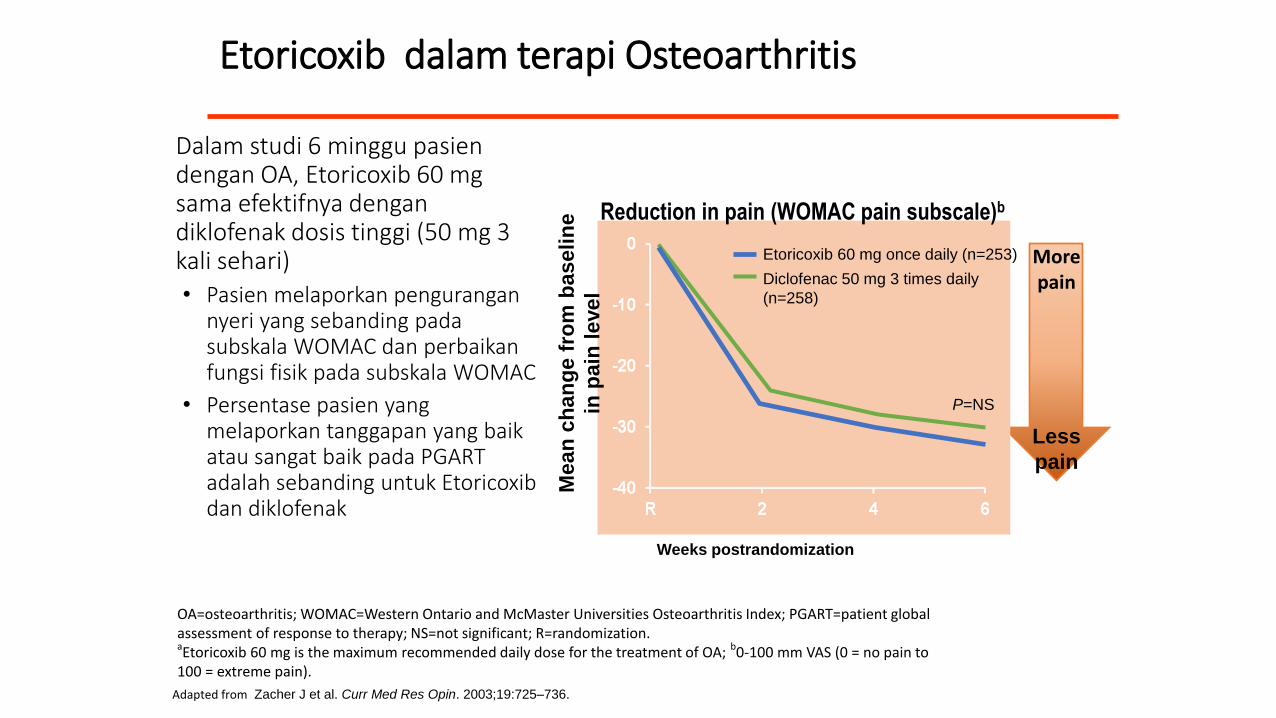
Dalam studi 6 minggu pasiendengan OA, Etoricoxib 60 mg sama efektifnya dengandiklofenak dosis tinggi (50 mg 3 kali sehari)• Pasien melaporkan pengurangan
nyeri yang sebanding padasubskala WOMAC dan perbaikanfungsi fisik pada subskala WOMAC
• Persentase pasien yang melaporkan tanggapan yang baikatau sangat baik pada PGART adalah sebanding untuk Etoricoxibdan diklofenak
Etoricoxib dalam terapi Osteoarthritis
Adapted from Zacher J et al. Curr Med Res Opin. 2003;19:725–736.
Weeks postrandomization
Morepain
Less
pain
Mea
n c
ha
ng
e f
rom
bas
elin
e
in p
ain
level
Diclofenac 50 mg 3 times daily
(n=258)
Etoricoxib 60 mg once daily (n=253)
P=NS
Reduction in pain (WOMAC pain subscale)b
OA=osteoarthritis; WOMAC=Western Ontario and McMaster Universities Osteoarthritis Index; PGART=patient global assessment of response to therapy; NS=not significant; R=randomization.aEtoricoxib 60 mg is the maximum recommended daily dose for the treatment of OA; b0-100 mm VAS (0 = no pain to 100 = extreme pain).
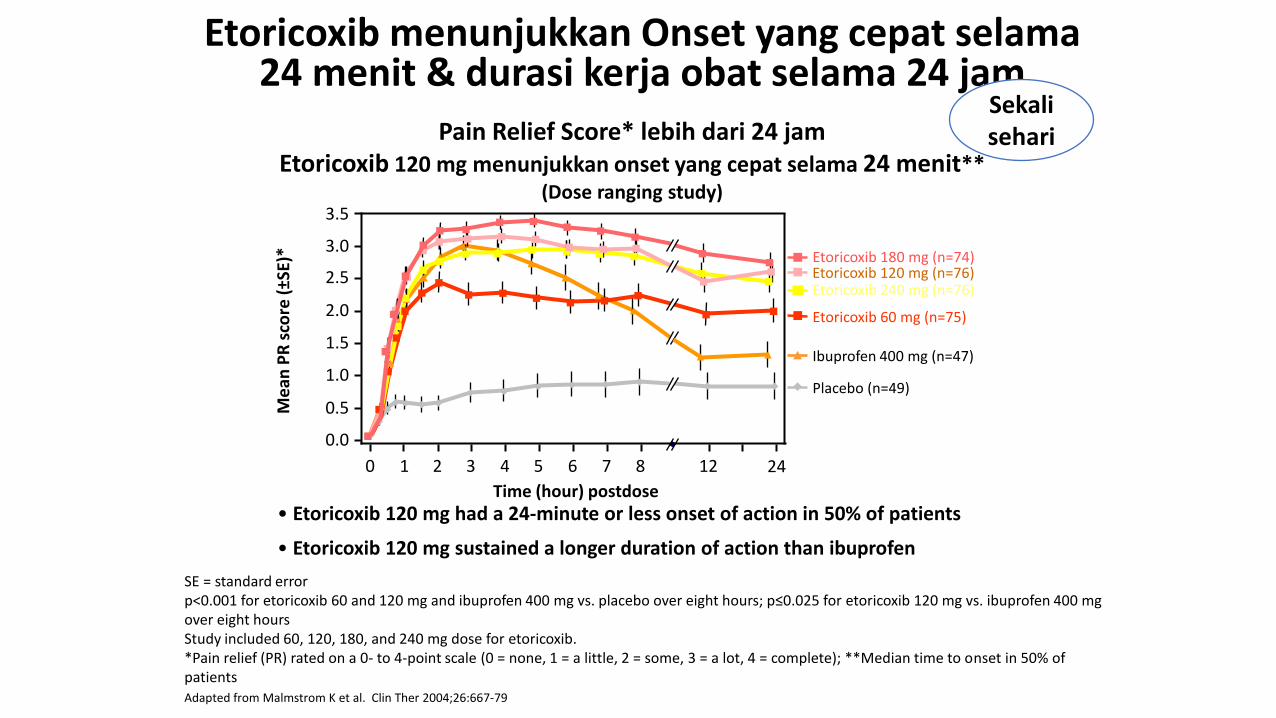
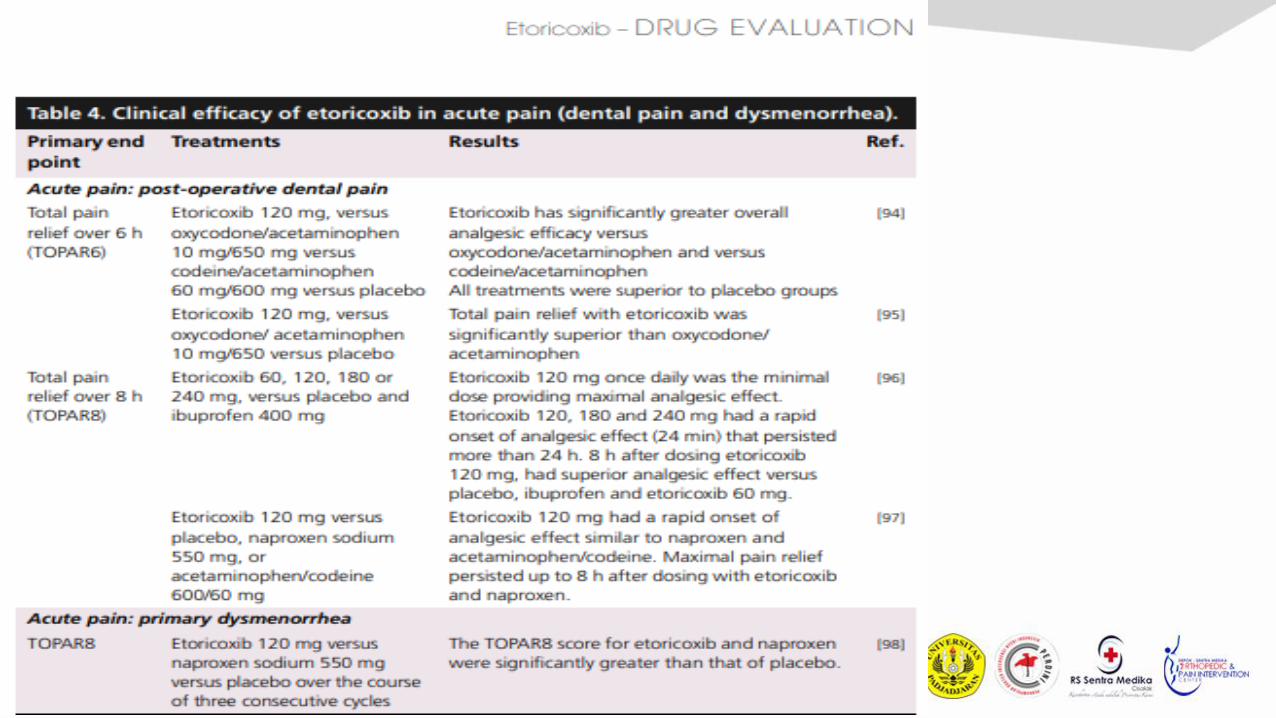
• Etoricoxib 120 mg had a 24-minute or less onset of action in 50% of patients
• Etoricoxib 120 mg sustained a longer duration of action than ibuprofen
Pain Relief Score* lebih dari 24 jamEtoricoxib 120 mg menunjukkan onset yang cepat selama 24 menit**
(Dose ranging study)
Me
an P
R s
core
(±S
E)*
Time (hour) postdose
Placebo (n=49)
Ibuprofen 400 mg (n=47)
Etoricoxib 60 mg (n=75)
Etoricoxib 240 mg (n=76)
Etoricoxib 180 mg (n=74)Etoricoxib 120 mg (n=76)
543210 6 7 8 12 24
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Etoricoxib menunjukkan Onset yang cepat selama24 menit & durasi kerja obat selama 24 jam
SE = standard errorp<0.001 for etoricoxib 60 and 120 mg and ibuprofen 400 mg vs. placebo over eight hours; p≤0.025 for etoricoxib 120 mg vs. ibuprofen 400 mg over eight hoursStudy included 60, 120, 180, and 240 mg dose for etoricoxib.*Pain relief (PR) rated on a 0- to 4-point scale (0 = none, 1 = a little, 2 = some, 3 = a lot, 4 = complete); **Median time to onset in 50% of patientsAdapted from Malmstrom K et al. Clin Ther 2004;26:667-79
Sekalisehari
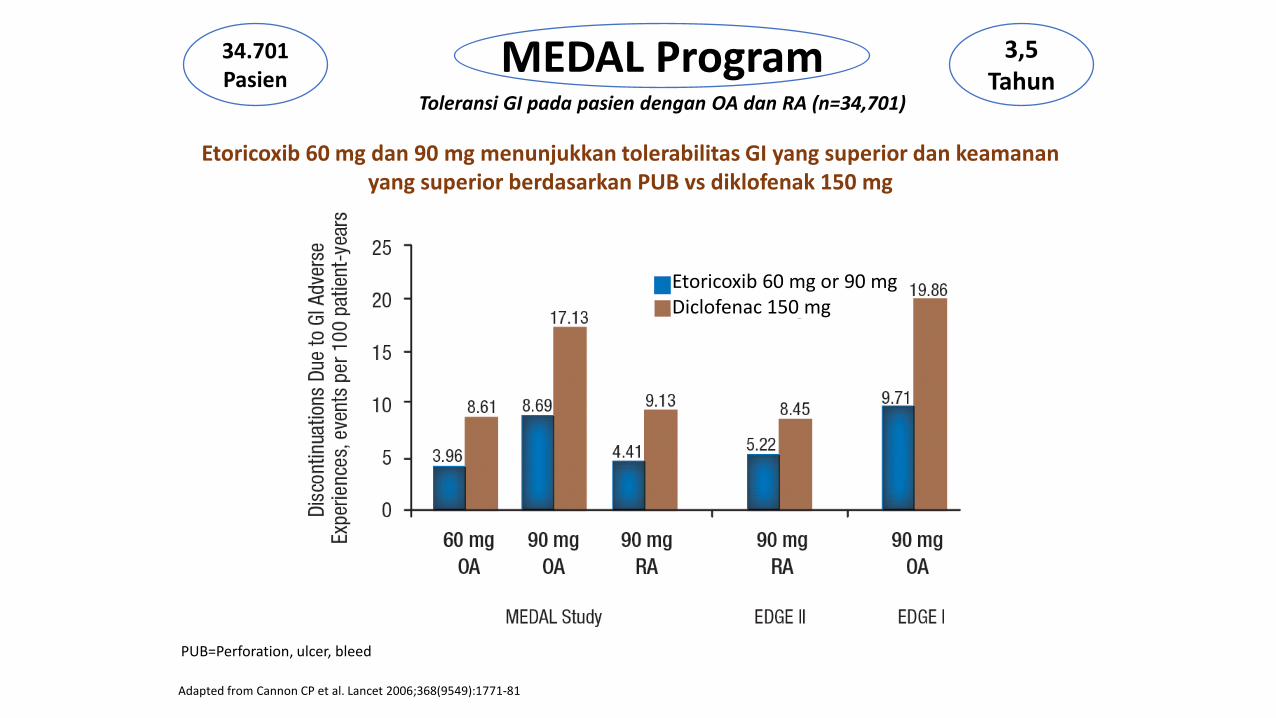
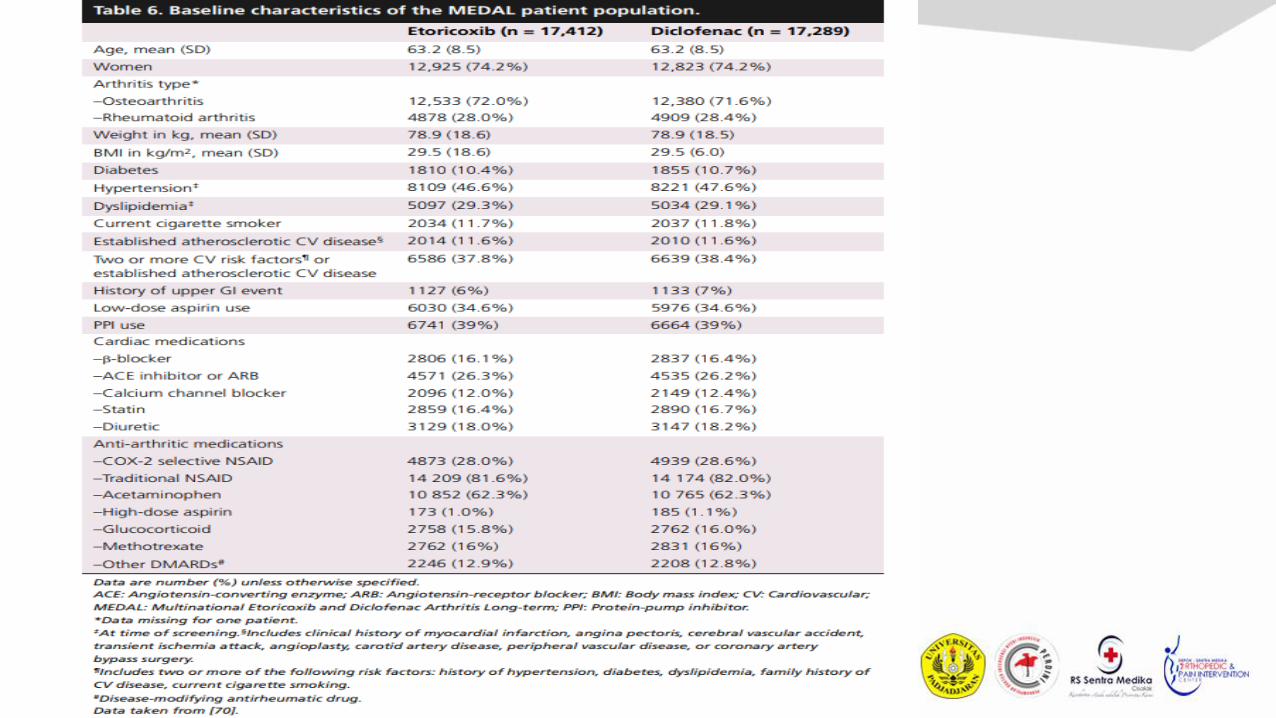
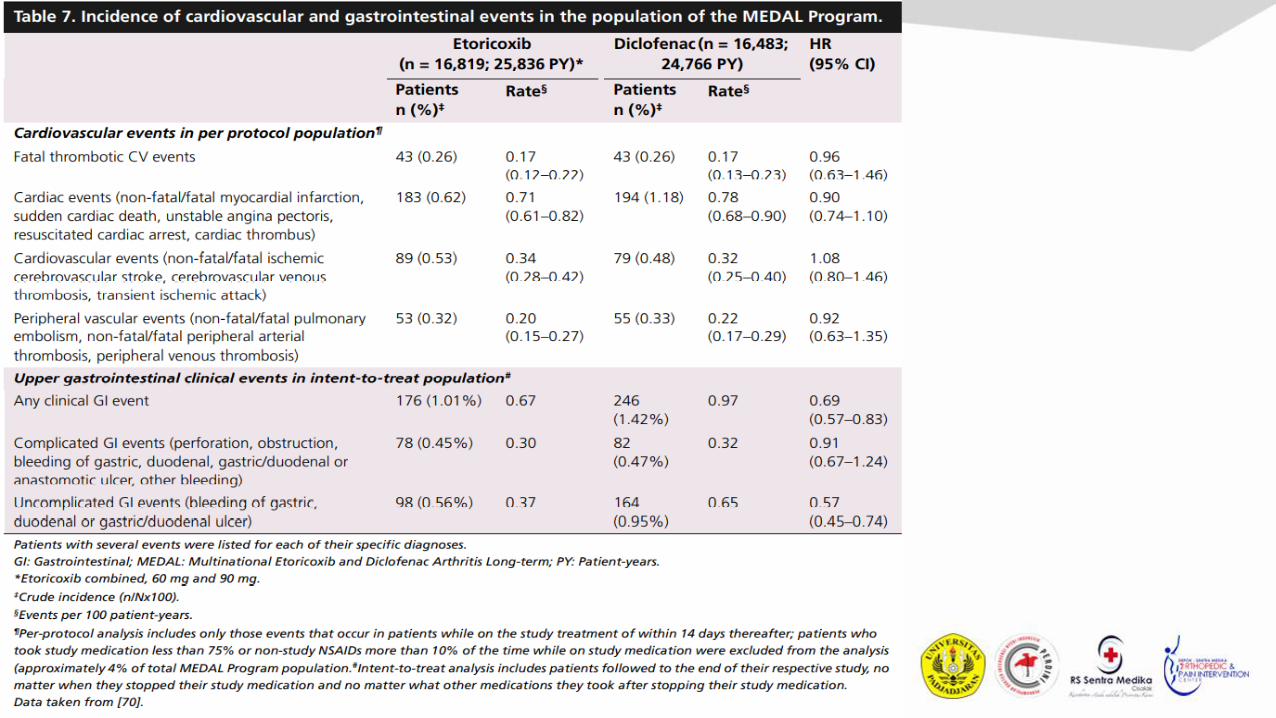
Etoricoxib 60 mg dan 90 mg menunjukkan tolerabilitas GI yang superior dan keamananyang superior berdasarkan PUB vs diklofenak 150 mg
MEDAL Program Toleransi GI pada pasien dengan OA dan RA (n=34,701)
34.701 Pasien
3,5 Tahun
Adapted from Cannon CP et al. Lancet 2006;368(9549):1771-81
PUB=Perforation, ulcer, bleed
Etoricoxib 60 mg or 90 mgDiclofenac 150 mg
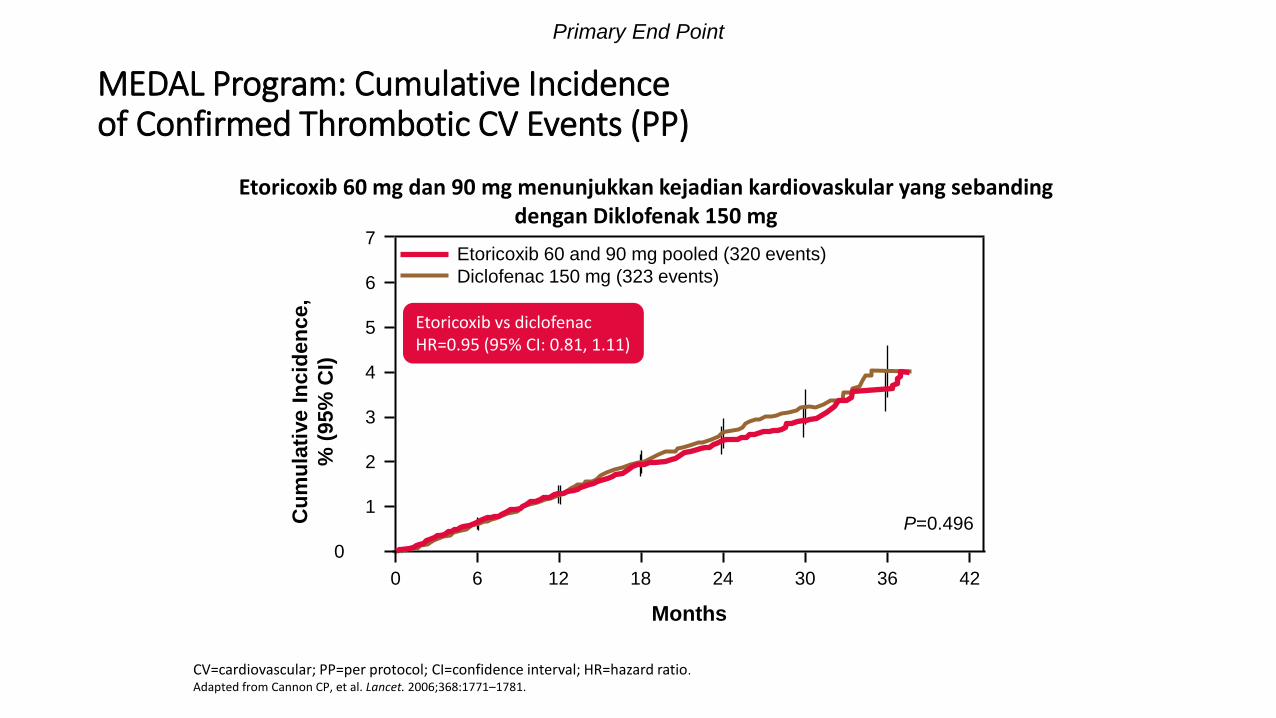
MEDAL Program: Cumulative Incidence of Confirmed Thrombotic CV Events (PP)
CV=cardiovascular; PP=per protocol; CI=confidence interval; HR=hazard ratio.
Adapted from Cannon CP, et al. Lancet. 2006;368:1771–1781.
Cu
mu
lati
ve I
ncid
en
ce,
% (
95%
CI)
Months
0 6 4224
Etoricoxib 60 and 90 mg pooled (320 events)
Diclofenac 150 mg (323 events)
7
0
12 18 30 36
6
5
4
3
2
1
Etoricoxib vs diclofenacHR=0.95 (95% CI: 0.81, 1.11)
P=0.496
Primary End Point
Etoricoxib 60 mg dan 90 mg menunjukkan kejadian kardiovaskular yang sebandingdengan Diklofenak 150 mg
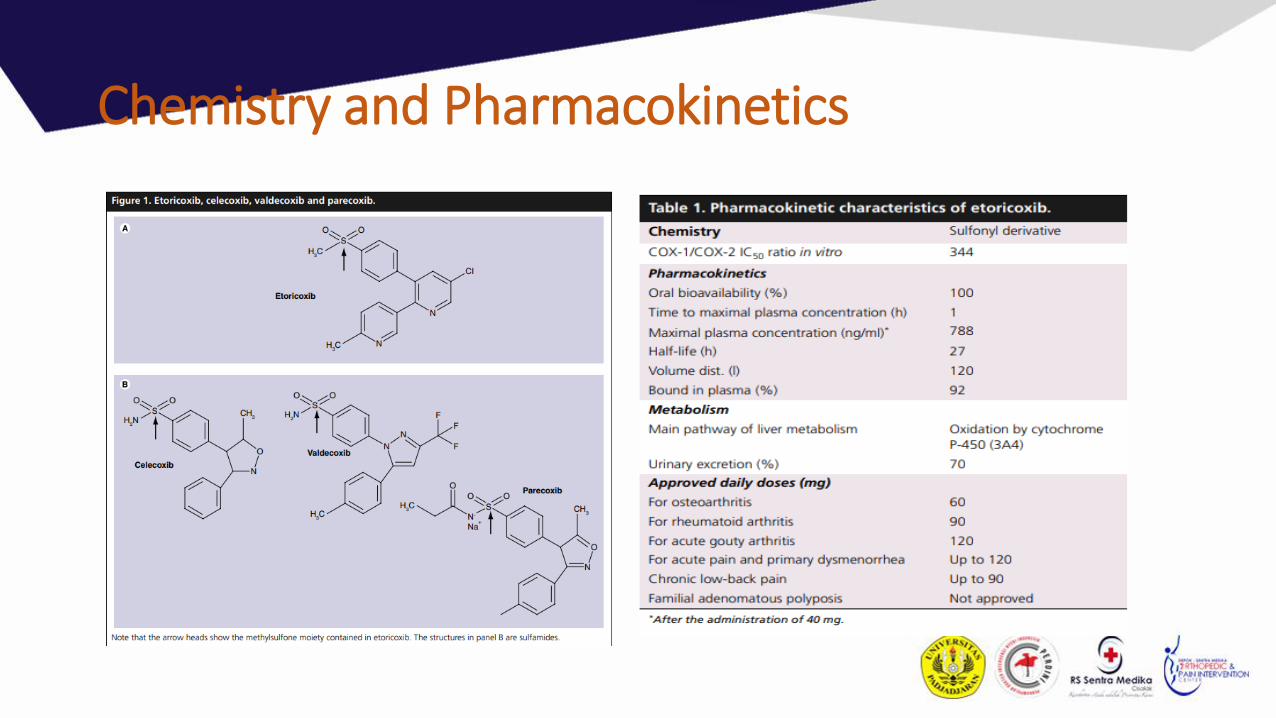
Chemistry and Pharmacokinetics

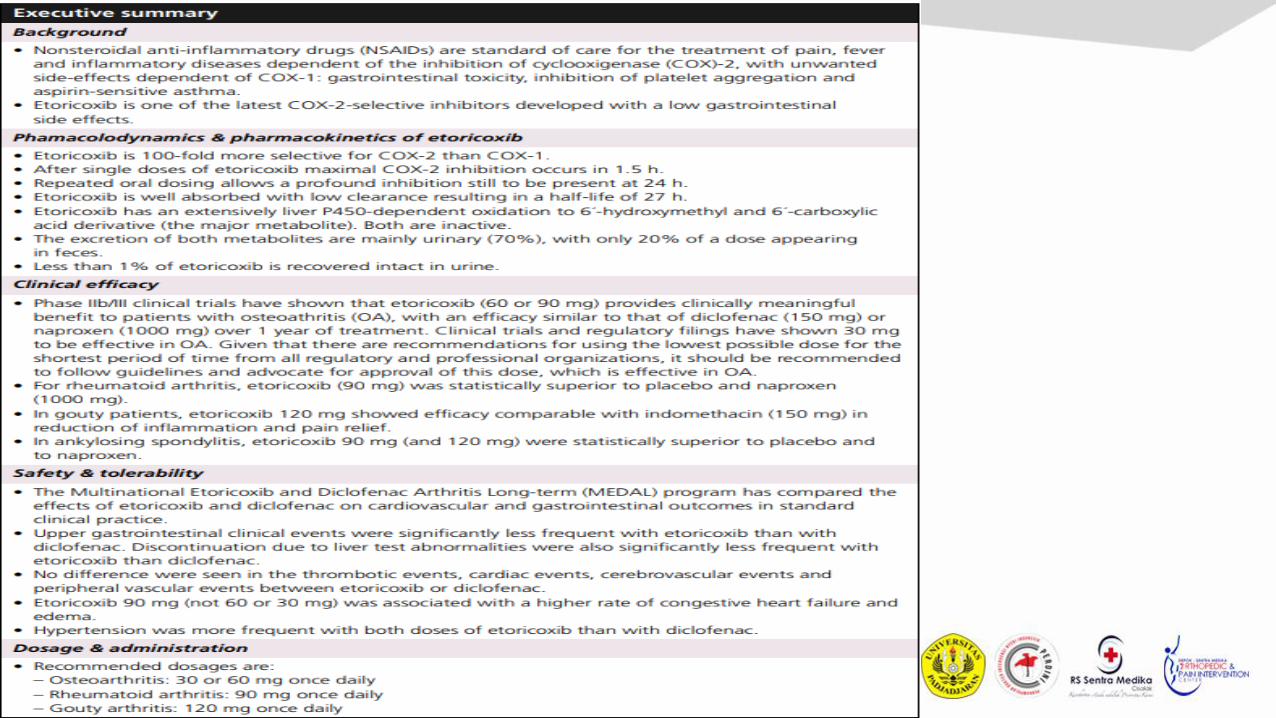
Kesimpulan
• Dalam kehidupan sehari-hari, 54% pasien OA dengangejala OA lutut mengalami pereda nyeri yang tidakadekuat (IPR) yang memengaruhi kualitas hidup..
• COXIB efektif untuk meredakan nyeri dan peradangan
• Perlu dipertimbangkan keseimbangan antaraefektifitas dan keamanan NSAID→ Etoricoxib adalahinhibitor COX2 dengan khasiat & keamanan yang telah terbukti
• Etericoxib bias digunakan pada kasus kronis dan penggunaan jangka Panjang dengan tettapmemperhatikan balance dan safety


TERIMA KASIH