Embed Size (px)
Citation preview

ROLE OF MRI VERSUS ULTRASOUND IN THE
ASSESSMENT OF PLACENTAL ABNORMALITIES AND
DISEASES
2015
Background & Aim of Work1
The placenta is often overlooked in the routineevaluation of a normal gestation, receiving attentiononly when an abnormality is detected
Although uncommon, abnormalities of theplacenta are important to recognize owing to thepotential for maternal and fetal morbidity andmortality
Background1
Placental abnormalities and diseases include:1. Abnormal location (Placenta previa)2. Abnormal implantation (PAD)3. Degenerative and vascular abnormalities (Vasa
previa, placental abruption, hematomas,placental bed infarction)
4. Abnormal placental thickness/size (volume)5. Abnormal placental shapes (normal variants)6. Placental calcifications7. Placental tumors (GTD, nontrophoblastic
placental tumors, metastases, cystic lesions)8. Placenta in multiple gestations
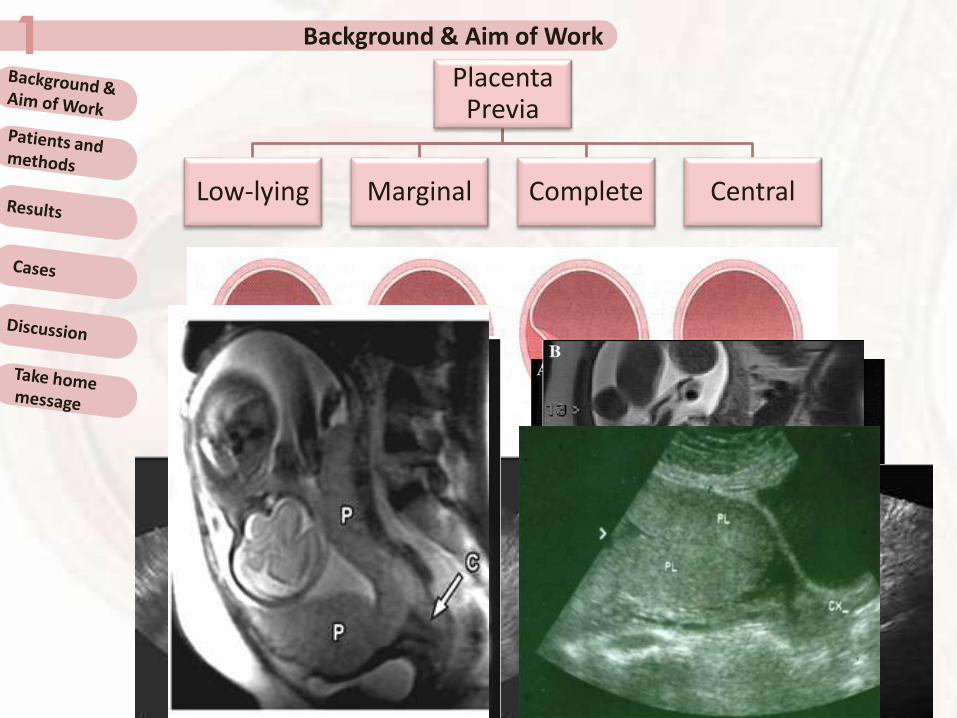
Background & Aim of Work1Placenta
Previa
Low-lying Marginal Complete Central

Background & Aim of Work1
PLACENTAL INVASION
Background & Aim of Work1
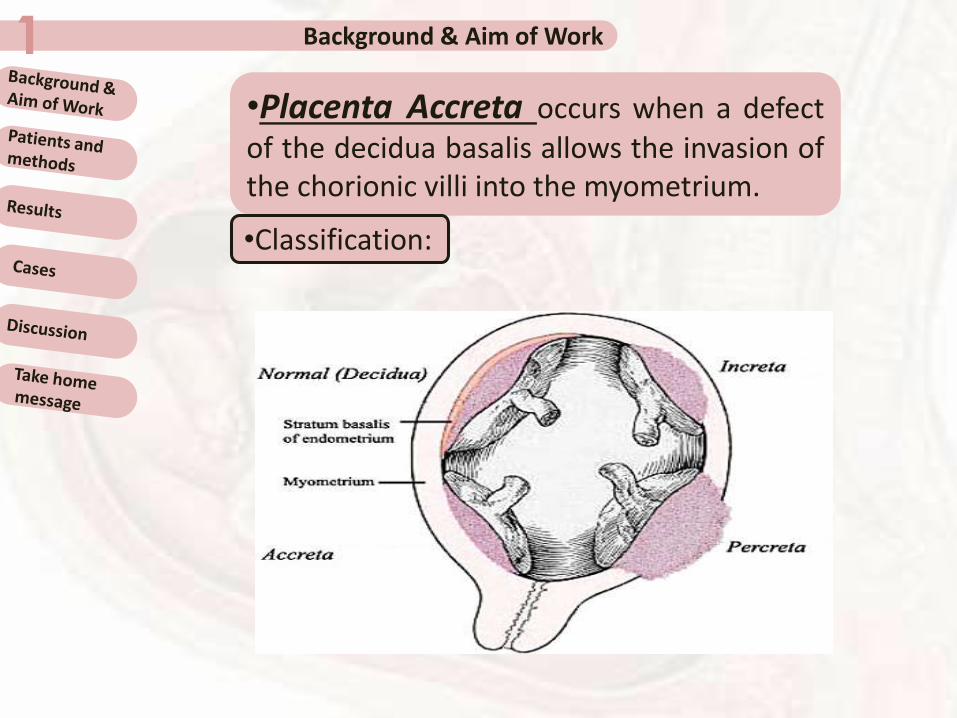
•Placenta Accreta occurs when a defectof the decidua basalis allows the invasion ofthe chorionic villi into the myometrium.
•Classification:
Background & Aim of Work1
Risk Factors for PA
Placenta Previa
Catastrophic intrapartum
heamorrhage
Previous CS
Background & Aim of Work1
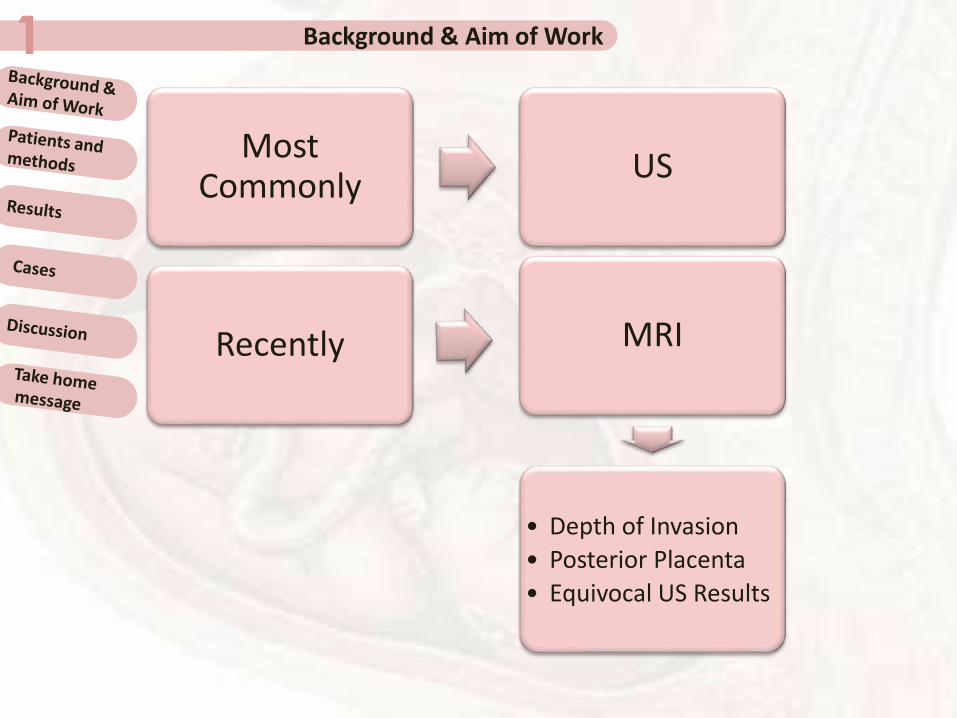
Most Commonly
US
Recently MRI
• Depth of Invasion
• Posterior Placenta
• Equivocal US Results
Background & Aim of Work1 US
Gray scale B-mode Transabdominal USColor Doppler US
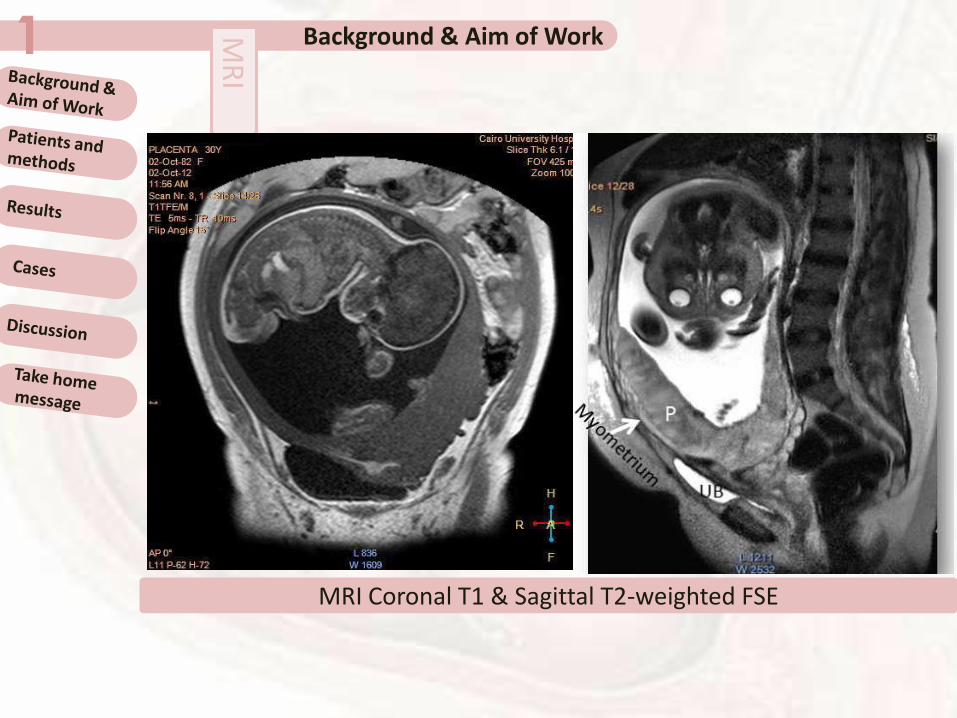
Background & Aim of Work1 MR
I
MRI Coronal T1 & Sagittal T2-weighted FSE

Background & Aim of Work1Placenta previa findings that are considered suggestive of accreta/percreta on US :
1. Loss of the retroplacental hypoechoic clear zone
2. Loss of the bladder wall-uterine interface
3. Presence of placental lacunae (vascular spaces)
4. Presence of hypervascularity of the interface between the uterine serosa and the bladder wall on color Doppler imaging

Background & Aim of Work1Placenta previa findings that are considered suggestive of accreta/percreta on MRI :
1. Uterine bulging2. Heterogeneous signal intensity within
the placenta3. Dark intraplacental bands on T2-WI4. Focal interruptions in the myometrial
wall5. Direct visualization of the invasion of
pelvic structures by placental tissue

Background & Aim of Work1
GESTATIONAL TROPHOBLASTIC DISEASE
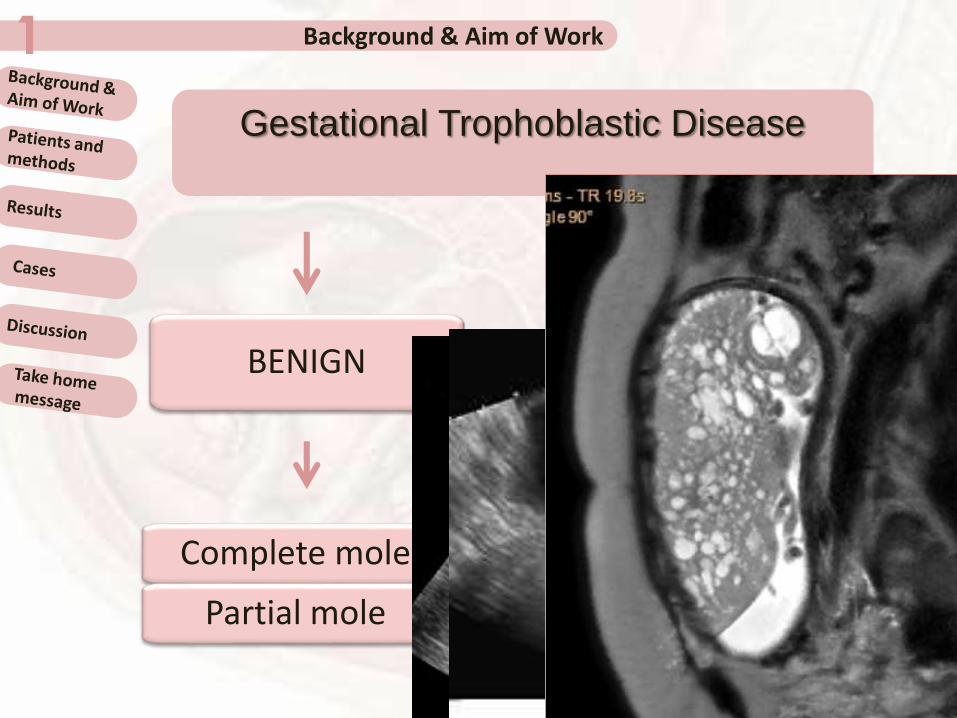
Background & Aim of Work1
Gestational Trophoblastic Disease
BENIGN
Complete mole
Partial mole
MALIGNANT
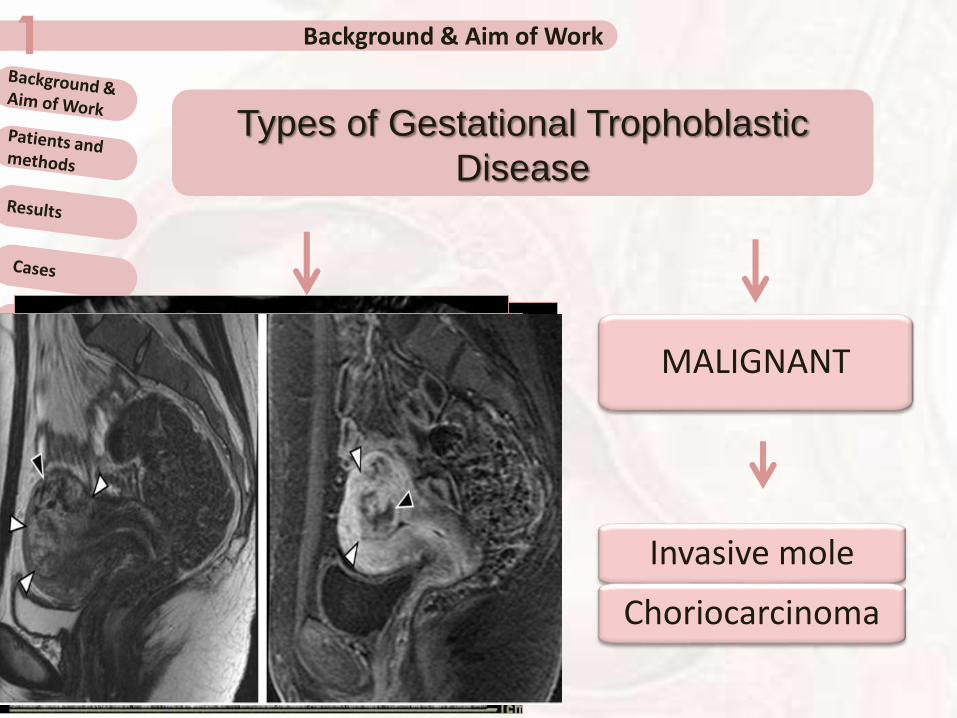
Background & Aim of Work1
Types of Gestational Trophoblastic
Disease
BENIGN
Complete mole
Partial mole
MALIGNANT
Invasive mole
Choriocarcinoma
Background & Aim of Work1
PLACENTAL ABRUPTION & HEMATOMA

PLACENTAL ABRUPTION & HEMATOMA1
ACUTESUBACUTE3-14 days
Hyper to isoechoic
Hypoechoic anechoic
Poor sonographic detection:1. Echotexture of acute hemorrhage is very similar to that of the adjacent placenta
2. Abnormally thick and heterogeneous placenta is only present in large acute clots
3. Subacute clots may not be visualized because blood dissects out and drains through the cervix
SUBACUTE>14 days
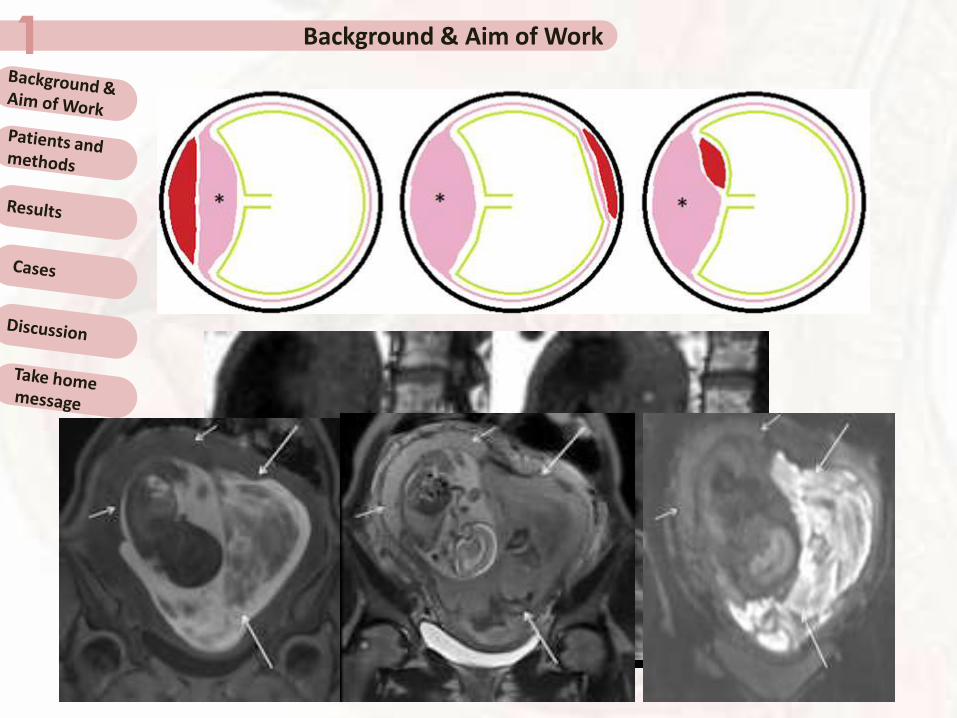
Placental abruption is a condition in which the placenta
peels away from the uterine wall partially or almost
completely before delivery. It is mainly a clinical
diagnosis and is only seen on ultrasound when
associated with a haematoma or increasedheterogeneous placental thickness
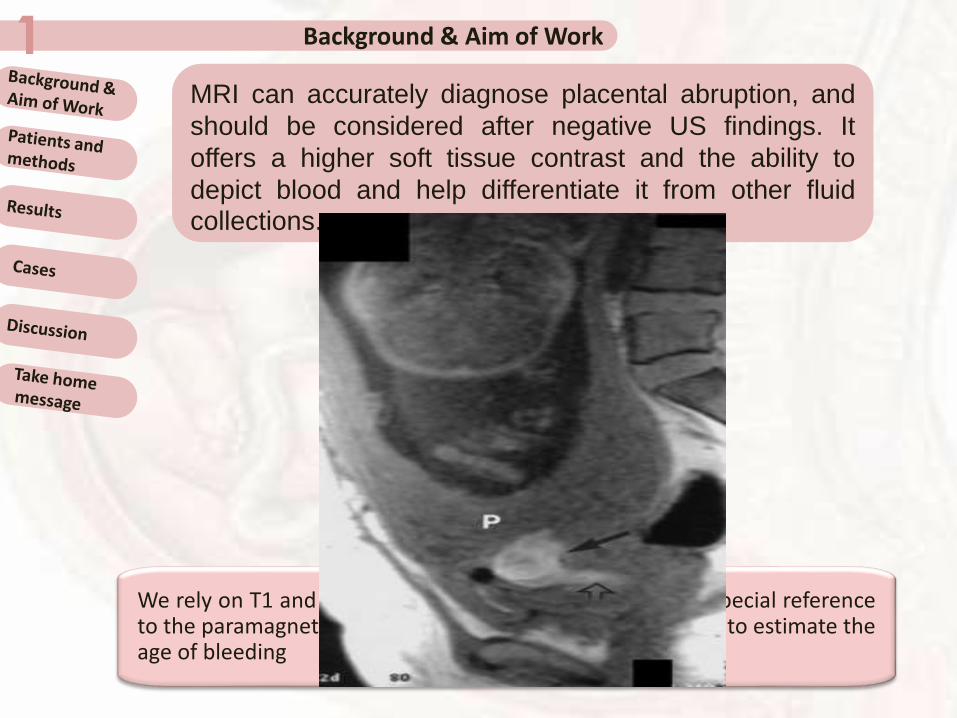
Background & Aim of Work1MRI can accurately diagnose placental abruption, and
should be considered after negative US findings. It
offers a higher soft tissue contrast and the ability to
depict blood and help differentiate it from other fluidcollections.
We rely on T1 and T2WIs for tissue characterization, with special referenceto the paramagnetic effects of methemoglobin, it is possible to estimate theage of bleeding
Background & Aim of Work1
Background & Aim of Work1
The aim of this work was to high lightenthe role of (MRI) in detecting placentalabnormalities and diseasesSoha Talaat Hamed *, Ahmed Mahmood H* * , Lamia Muhammed Bassam **radiology department ,** obstetric & gynecology department
Patients and methods2
Fifty pregnant females with placentalabnormalities and diseases had beenevaluated; we divided them into 3 groups:Group I: (40/50) Abnormal placental locationand/or implantation (one ectopic pregnancy onCS scar with decidual invasion and 39 placentaprevia at high risk of coexisting PAD)Group II: (8/50) Gestational trophoblasticdiseaseGroup III: (2/50) Placental hematoma andabruption
Patients and methods2
Ultrasound examination was performed using:
•LOGIQ 7 PRO, GE (General Electric Medical System)
Transabdominal approachfor all cases using 5 MHzsector transducerTransvaginal and/ortranslabial approach using7-8 MHz endoluminaltransducer
Patients and methods2
Pelvic MRI was performed for all cases using a1.5-T (Gyroscan Intera, Philips medicalsystems, Netherland)
Protocol of scanning for group I and group III:1. T2WI FSE (axial, sagittal and coronal planes)2. T1WI SE (axial, sagittal and coronal planes)3. B-FFE (sagittal and coronal planes)
Protocol of scanning for group II:1. T2WI FSE (axial, sagittal and coronal planes)2. T1WI SE (axial, sagittal and coronal planes)3. T1WI SE post contrast (axial, sagittal and
coronal planes)

Results3
80%(40/50)
16%
(8/50)
4%
(2/50)
Placental abnormalities & diseases
Abnormal placental location and/or implantation
Gestational trophoblastic diseases
Placental hematoma and abruption
Results3
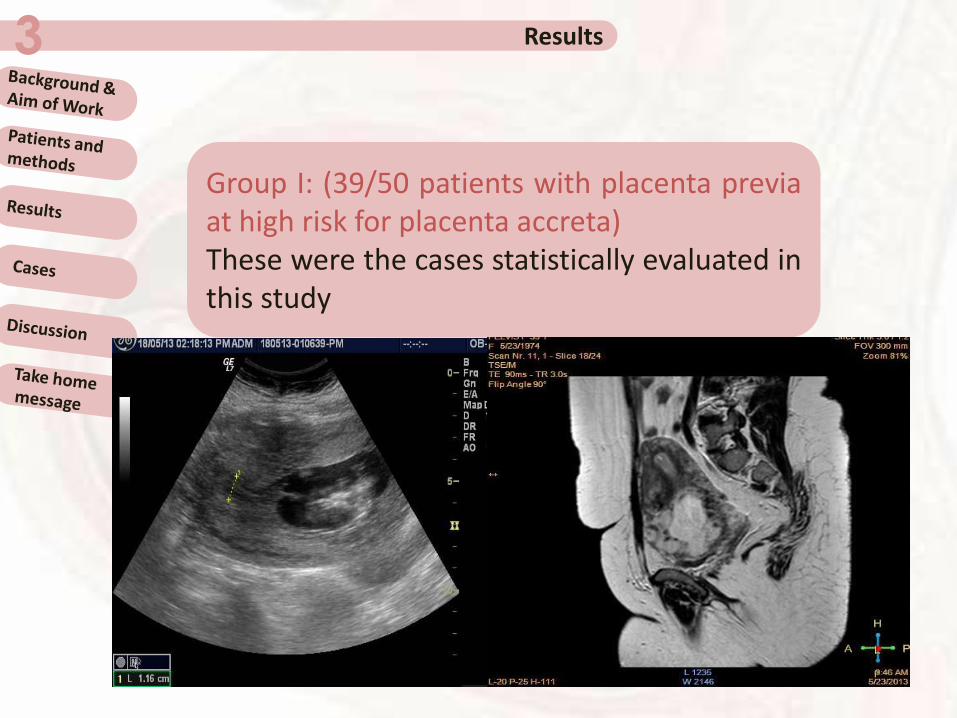
Group I: (39/50 patients with placenta previaat high risk for placenta accreta)These were the cases statistically evaluated inthis study
Results3
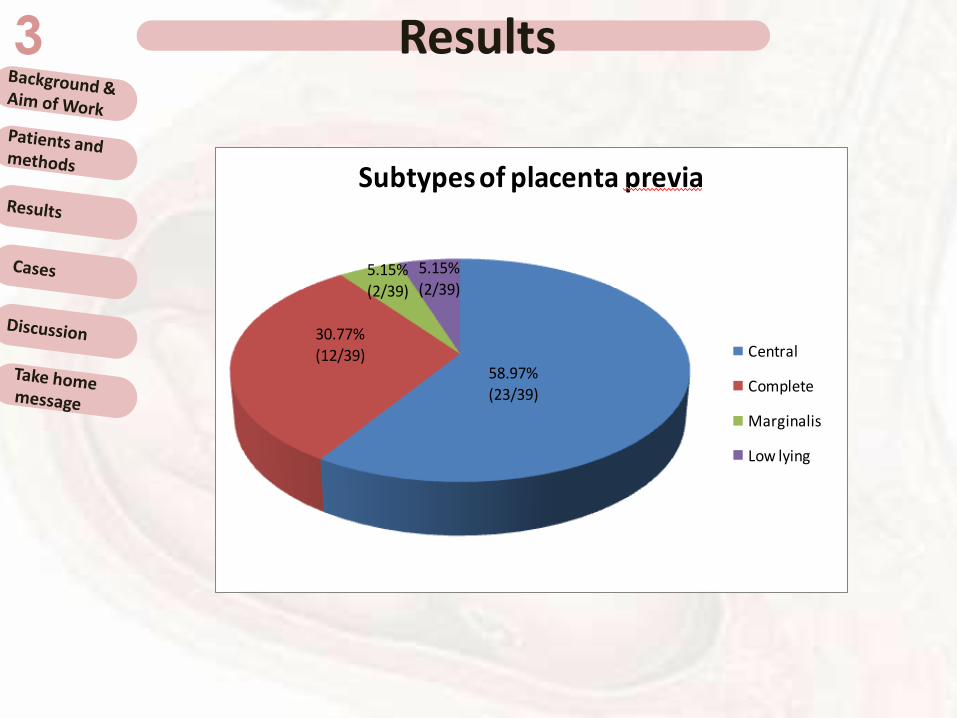
58.97%
(23/39)
30.77%
(12/39)
5.15%(2/39)
5.15%
(2/39)
Subtypes of placenta previa
Central
Complete
Marginalis
Low lying
Results3
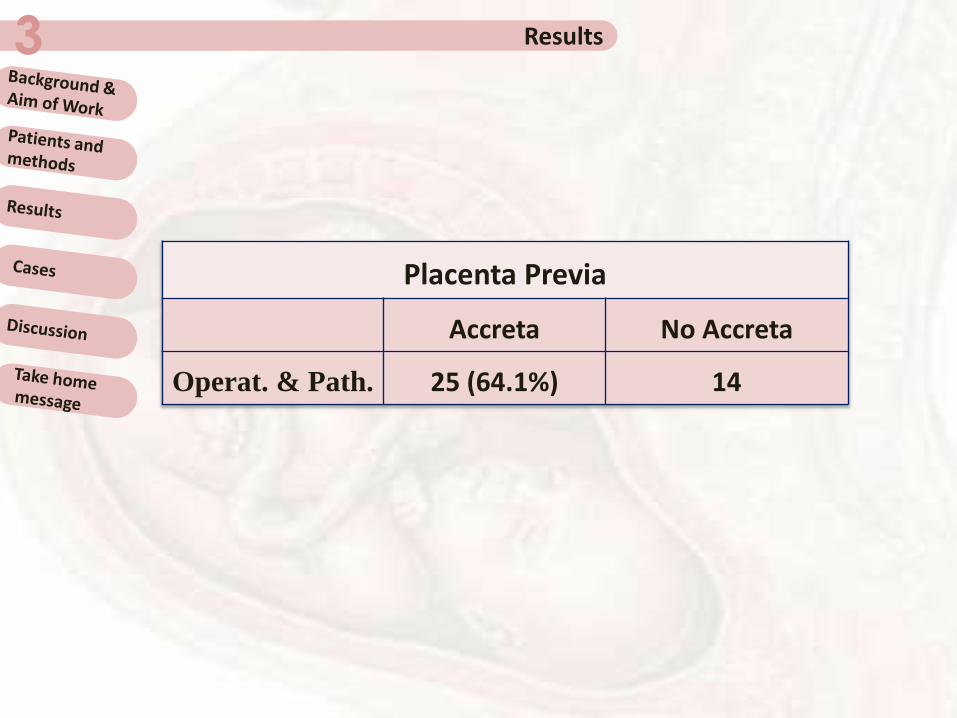
Placenta Previa
Accreta No Accreta
Operat. & Path. 25 (64.1%) 14

Results3
36%(9/25)
36%(9/25)
28%(7/25)
Types of placental invasion
Accreta
Percreta
Increta

Results3
Sensitivity, Specificity, PPV and NPV of US diagnostic criteria
Item Sensitivity Specificity (+)ve PV (-)ve PV Accuracy
Loss of retroplacental
clear space68.00 85.71 89.47 60.00 74.36
Loss of bladder uterine
interface24.00 100.00 100.00 42.42 51.28
Vascular lacunae 56.00 92.86 93.33 54.17 69.23
Increased vascularity
on Ut.-bladder
interface
24.00 92.86 85.71 40.62 48.72
Dec. Myometrial
Thickness48.00 92.86 92.31 50.00 64.10

Results3
Sensitivity, specificity, PPV and NPV of MRI diagnostic criteria
Items Sensitivity Specificity (+)ve PV (-)ve PV Accuracy
Heterogeneous
placenta intensity80.00 78.57 86.96 68.75 79.49
Dark intraplacental
bands on T272.00 92.86 94.74 65.00 79.49
Focal interruption in
myometrial wall64.00 92.86 94.12 59.09 74.36
Uterine bulging 48.00 100.00 100.00 51.85 66.67
Direct visualization of
invasion of pelvic
structures
24.00 100.00 100.00 42.42 51.28
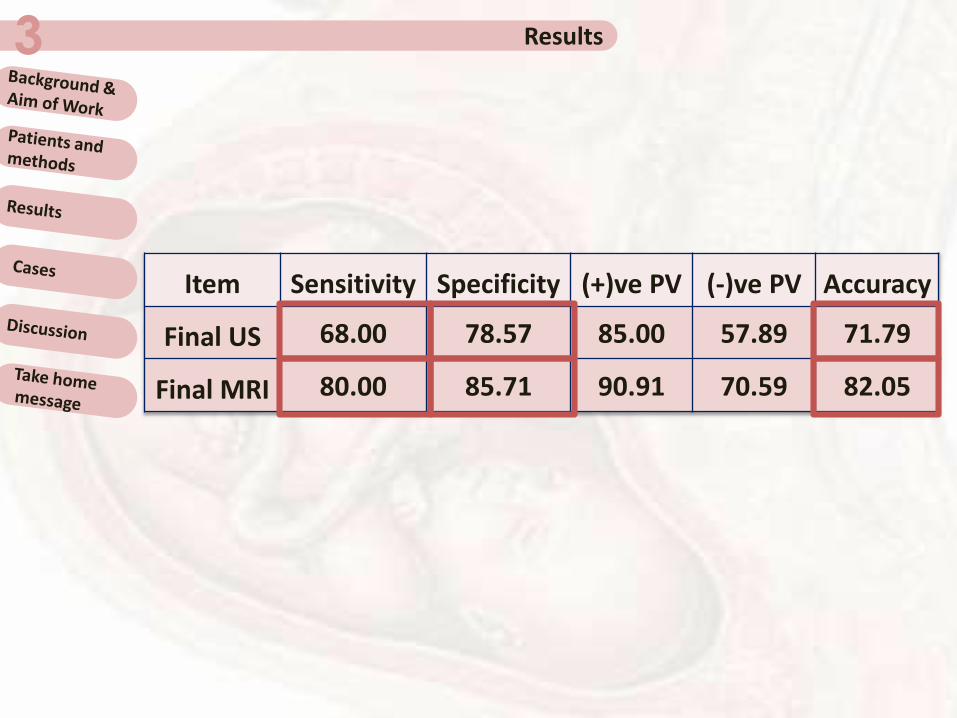
Results3
Item Sensitivity Specificity (+)ve PV (-)ve PV Accuracy
Final US 68.00 78.57 85.00 57.89 71.79
Final MRI 80.00 85.71 90.91 70.59 82.05
Results3
Group I: (1/50 case of ectopic pregnancy on CS scarwith decidual invasion)That case was diagnosed by both modalitieshowever, decidual invasion was suggested by MRIGroup II: (8/50 cases GTD)1/8 was misdiagnosed by US as vesicular molehowever MRI revealed the myometrial invasion inthat choriocarcinoma/invasive mole caseGroup III: (2/50 cases hematoma/abruption)1/2 was suspected to by a placental mass by US,however MRI by its high sensitivity and specificity todetect different ages of blood helped to correctlydiagnose hematoma and abruption
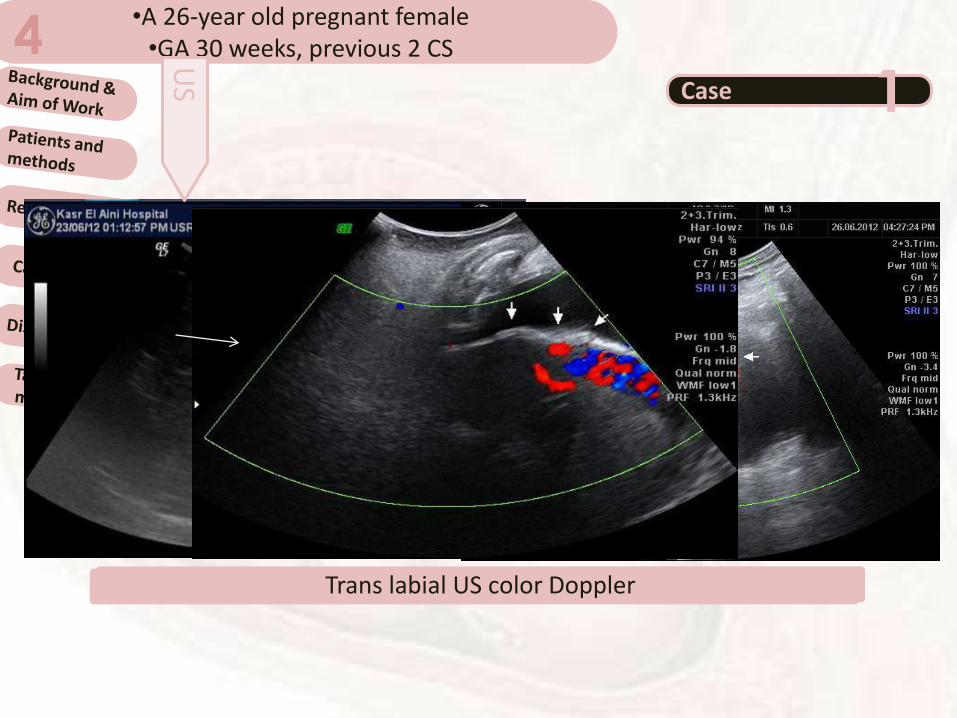
•A 26-year old pregnant female •GA 30 weeks, previous 2 CS 4
Case 1
Trans abdominal US gray scale and color Doppler
US
Trans labial US color Doppler
Cases4Case 1
Sagittal and Coronal T2WI FSE
MR
I
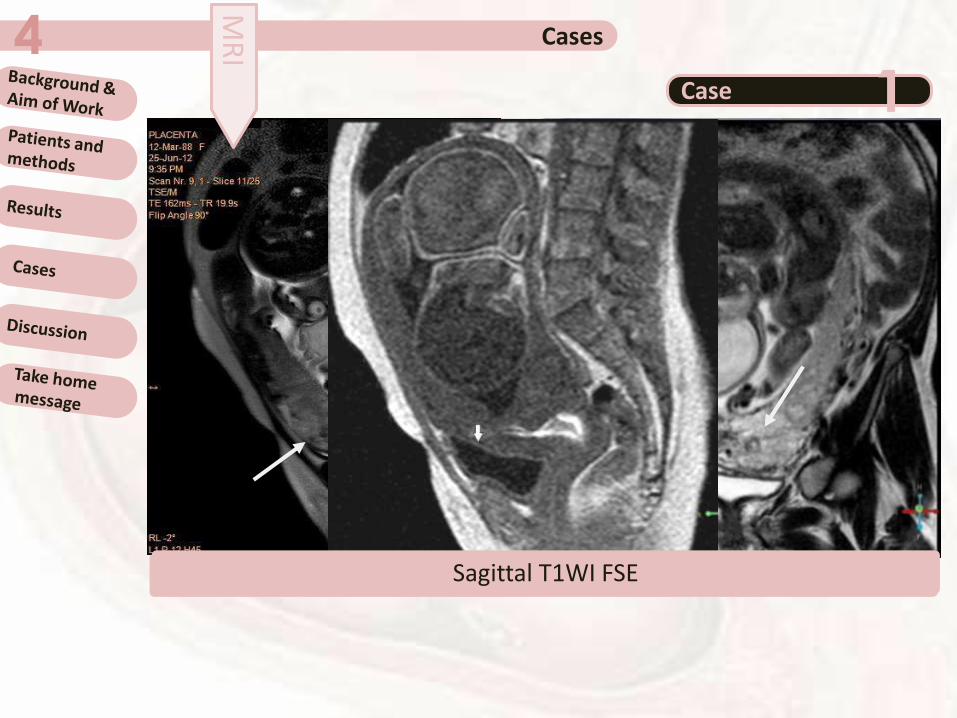
Sagittal T1WI FSE
Cases4Case 1
Placenta Increta & hysterectomy was done
Operative & Pathological Findings
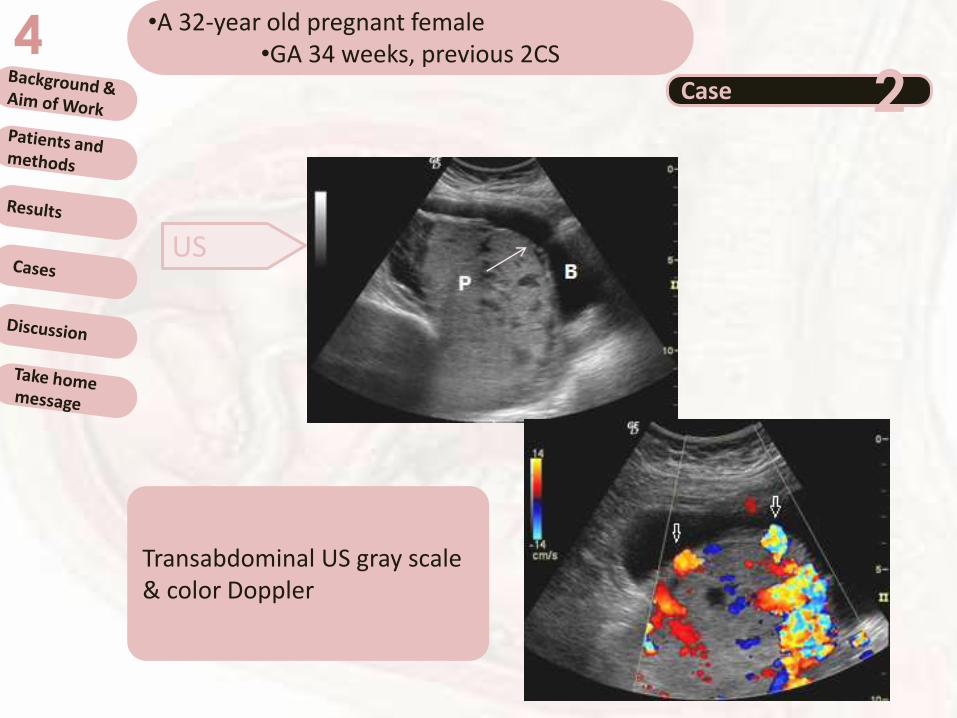
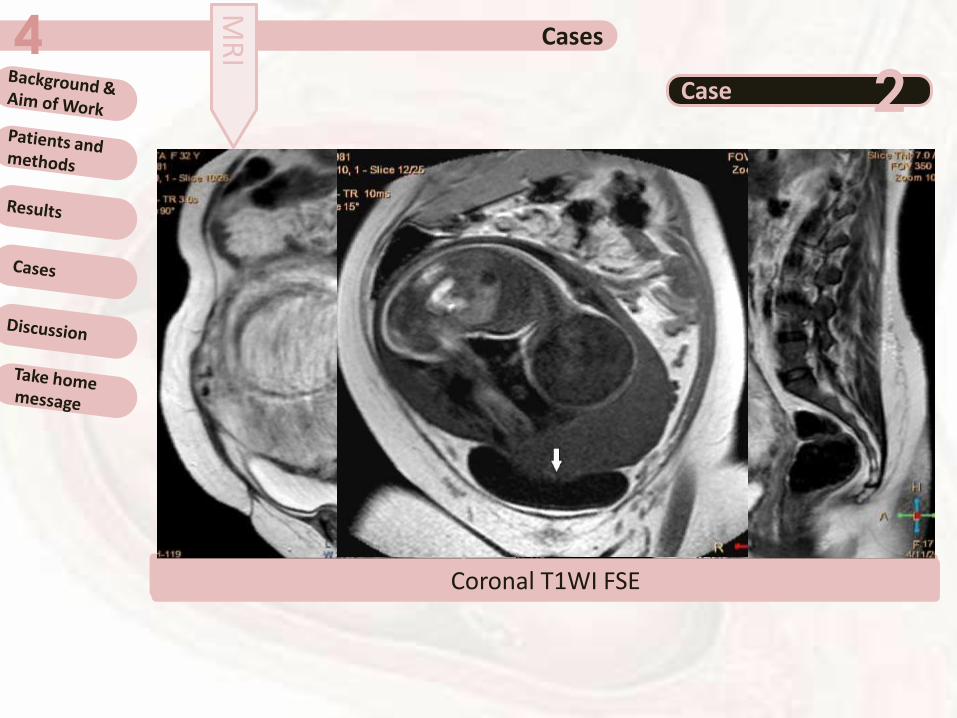
•A 32-year old pregnant female•GA 34 weeks, previous 2CS 4
Case 2
US
Transabdominal US gray scale & color Doppler
Cases4Case 2
MR
I
Sagittal T2WI FSECoronal T1WI FSE
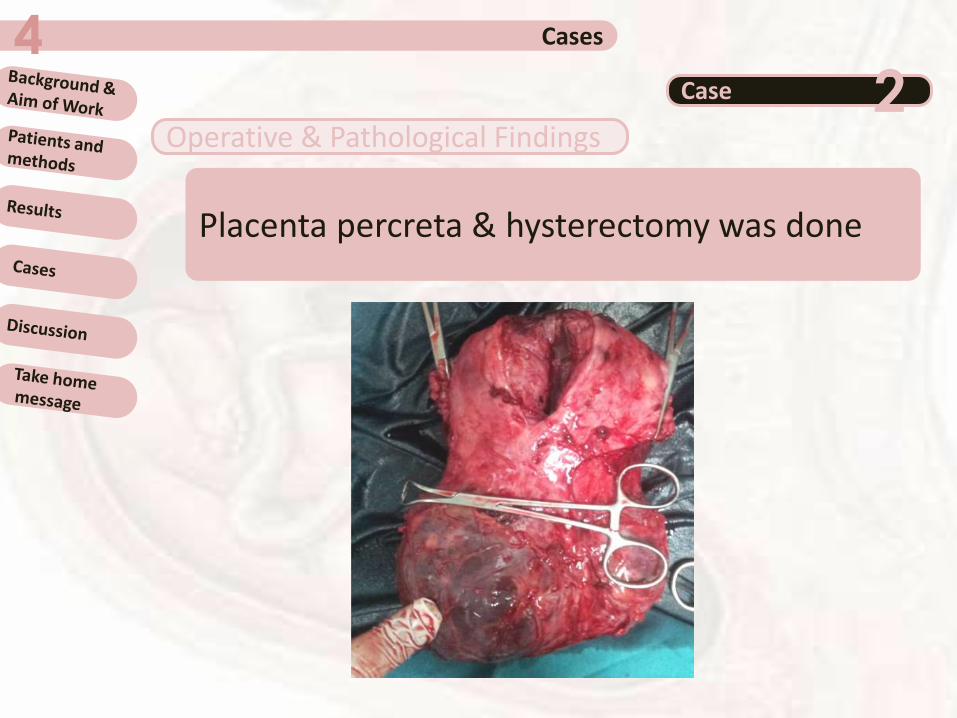
Cases4Case 2
Placenta percreta & hysterectomy was done
Operative & Pathological Findings
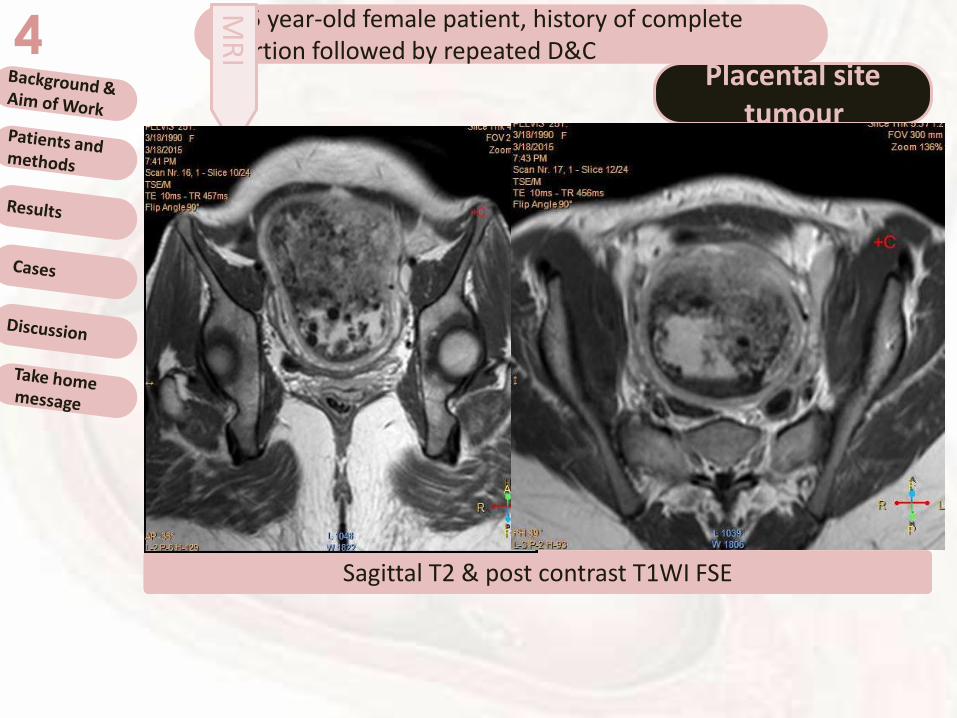
A 25 year-old female patient, history of complete abortion followed by repeated D&C4
Placental site tumour
MR
I
Sagittal T2 and T1WI FSESagittal T2 & post contrast T1WI FSE
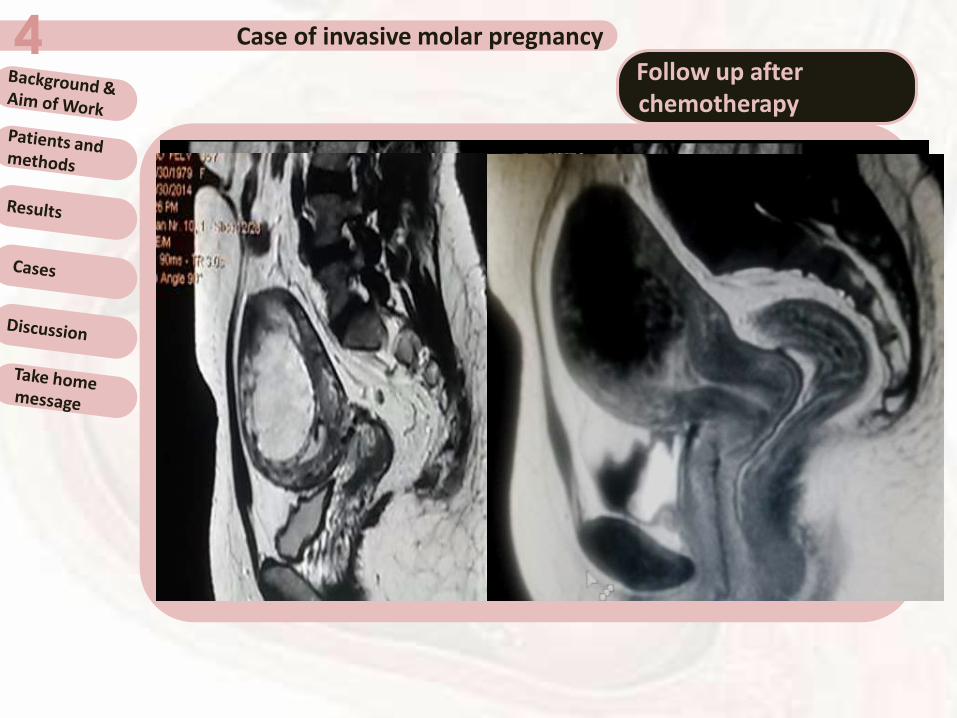
Case of invasive molar pregnancy 4Follow up after chemotherapy
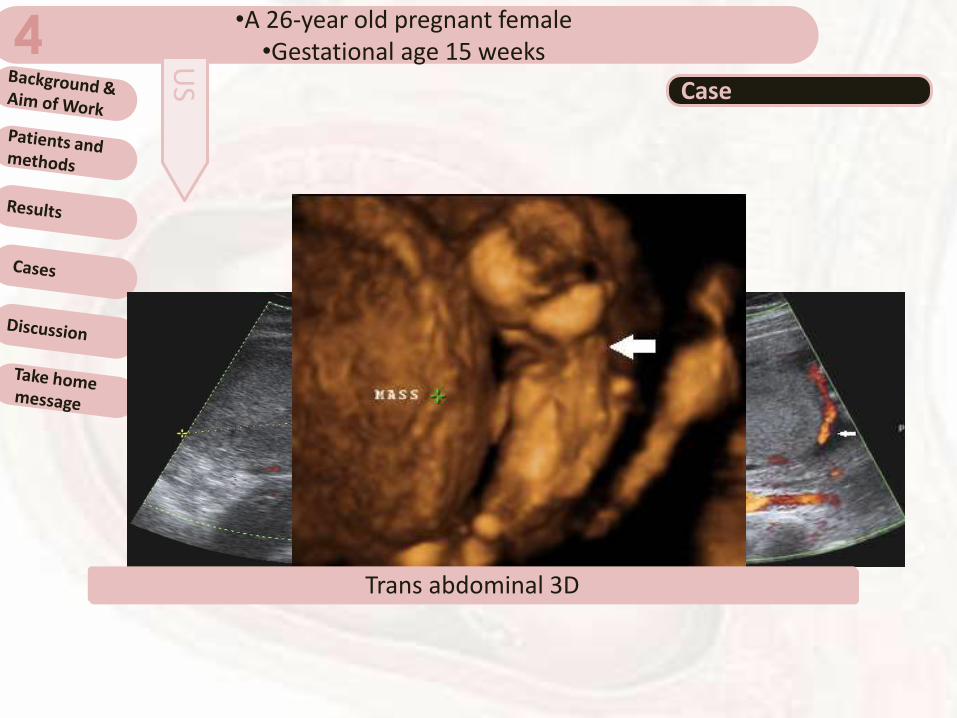
•A 26-year old pregnant female•Gestational age 15 weeks 4
Case
Trans abdominal color DopplerTrans abdominal 3D
US
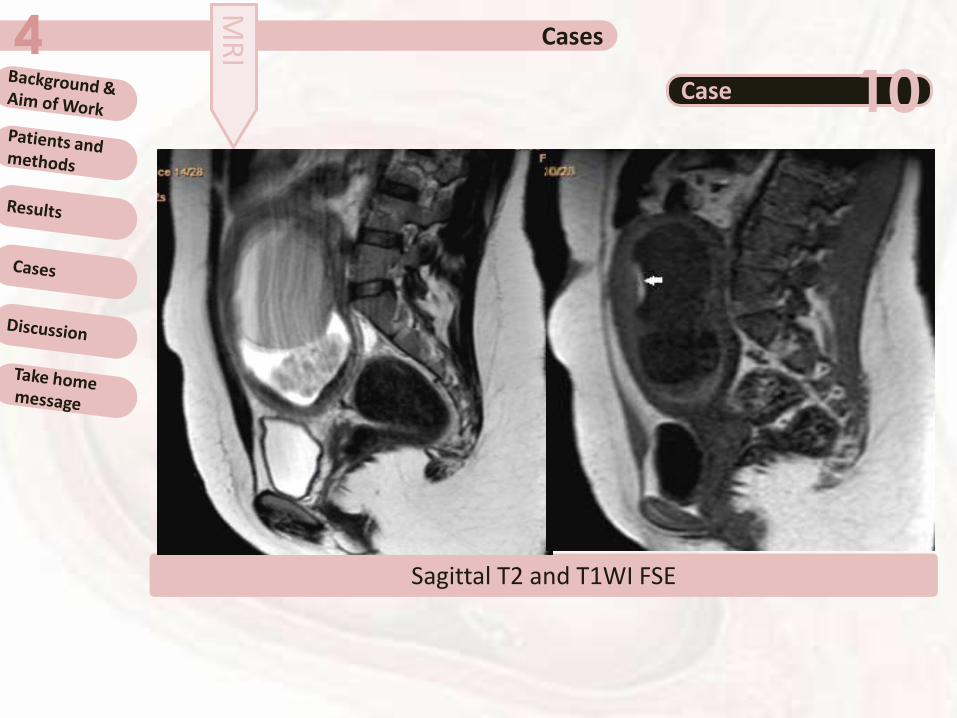
Cases4Case 10
Sagittal T2 and T1WI FSE
MR
I

Discussion5Some studies concluded that MRI is anexcellent tool for staging and topographicevaluation of PAD, while others stated that MRIis less reliable in differentiating betweendifferent degrees of placental invasion,especially between accreta vera and increta.
Among the true positive cases, USunderestimated 2 cases of percreta andoverestimated 1 case, on the other hand MRIunderestimated 2 cases. Both modalities failedto diagnose 1 case of percreta posteriorly.
Masselli et al, 2008Varghese et al, 2013
Discussion5
Matching between US and MRI findings tookplace in 78.57% (11/14) of the negative casesand in 68% (17/25) of the positive cases ofinvasion.
When US and MRI diagnosis is not matching, itis probably better to consider that the moreaggressive findings are correct.
Take home message6
•MRI hand in hand with US is important for theaccurate diagnosis of placental abnormalities anddiseases especially the invasive placental processes(GTD and placenta previa/accreta).•Co-operation of both modalities may provide morediagnostic information.
US remains the first imaging modality of evaluation ofthe placenta.

Thanks



























![Chapter 11 [blood abnormalities n diseases]](https://img.pdfslide.net/doc/110x75/5477db1fb4af9f7a0f8b45fd/chapter-11-blood-abnormalities-n-diseases.jpg)

