Embed Size (px)
Citation preview
Role of surgery for tracheal stenosis
and tumors
Paul De Leyn, MD, PhD
Chairman Department of Thoracic Surgery
University Hospitals Leuven
Belgium
C. Dooms, Department of pneumology
A. Neyrinck, Anesthesiology
M. Boada, Resident Thoracic Surgery
G. Deneffe †, Department of Thoracic surgery
Eindejaarsmeeting 4-6 december 2015
In memoriam Prof. G. Deneffe
• Chairman lung surgery
1994-2000
P. De Leyn, H. Decaluwé, D. Van Raemdonck,
C. Dooms, J. Yserbyt, G. Verleden, R. Vos
P. Delaere, V. Vanderpoorten
J. Vranckx
C. Deboeck, M. Proesmans
R. Hermans
Department of Thoracic Surgery
Department of Pneumology
Department of Otorhinology
Department of Plastic Surgery
Department of Pediatrics
Department of Radiology
Multidisciplinary Tracheal Workgroup
• Benign postintubation and tracheostomy
stenosis
– Surgical technique
– Literature results
– UZ Leuven results
• Idiopathic laryngotracheal stenosis
• Surgery for tracheal tumors
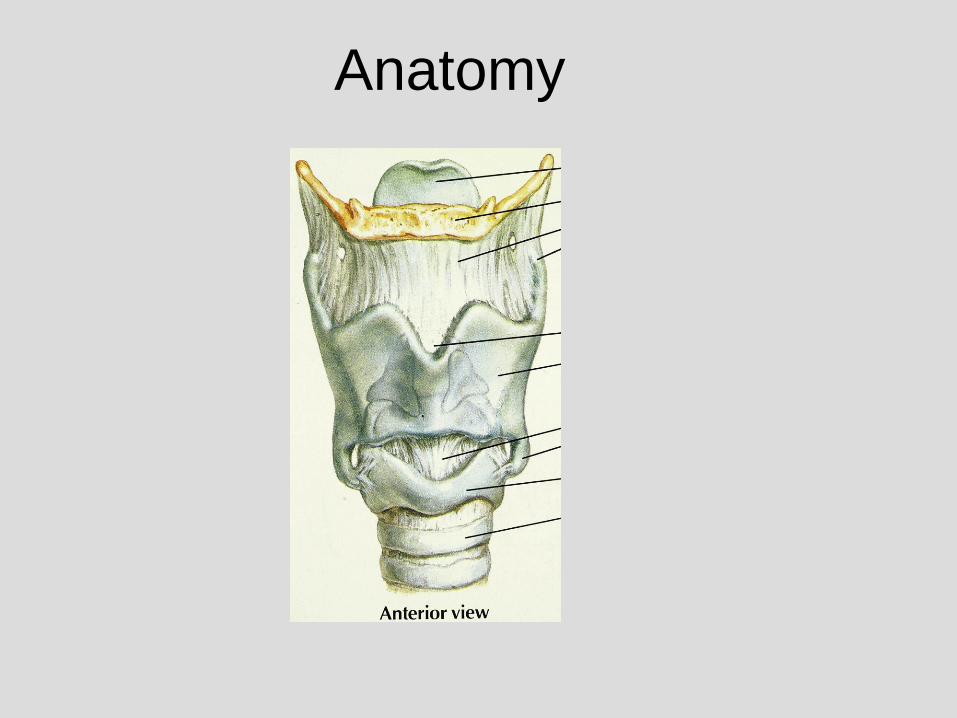
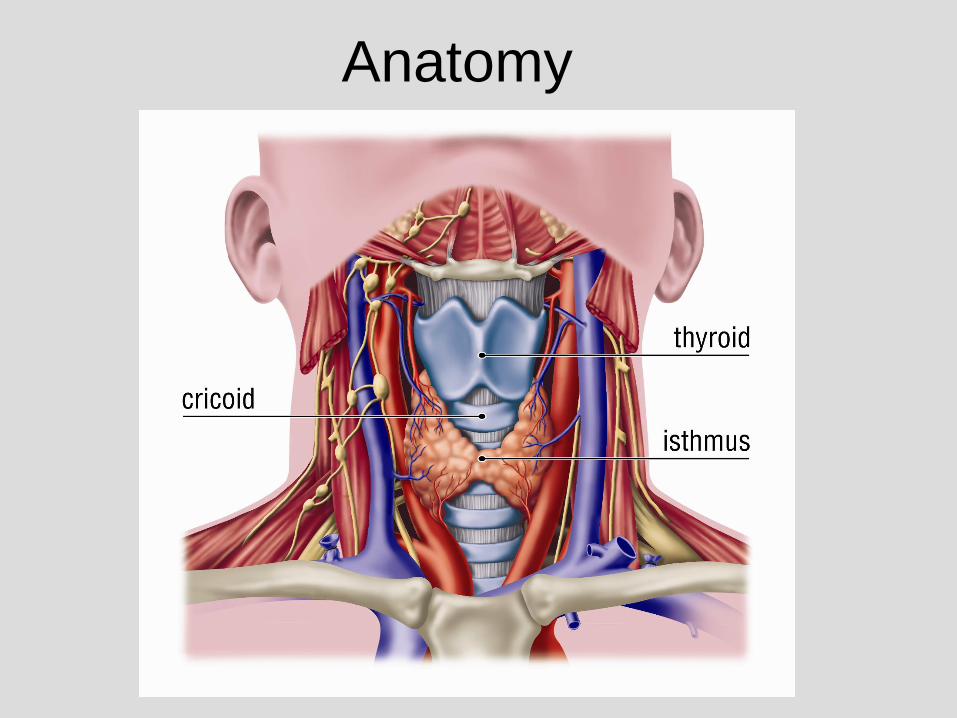
Anatomy
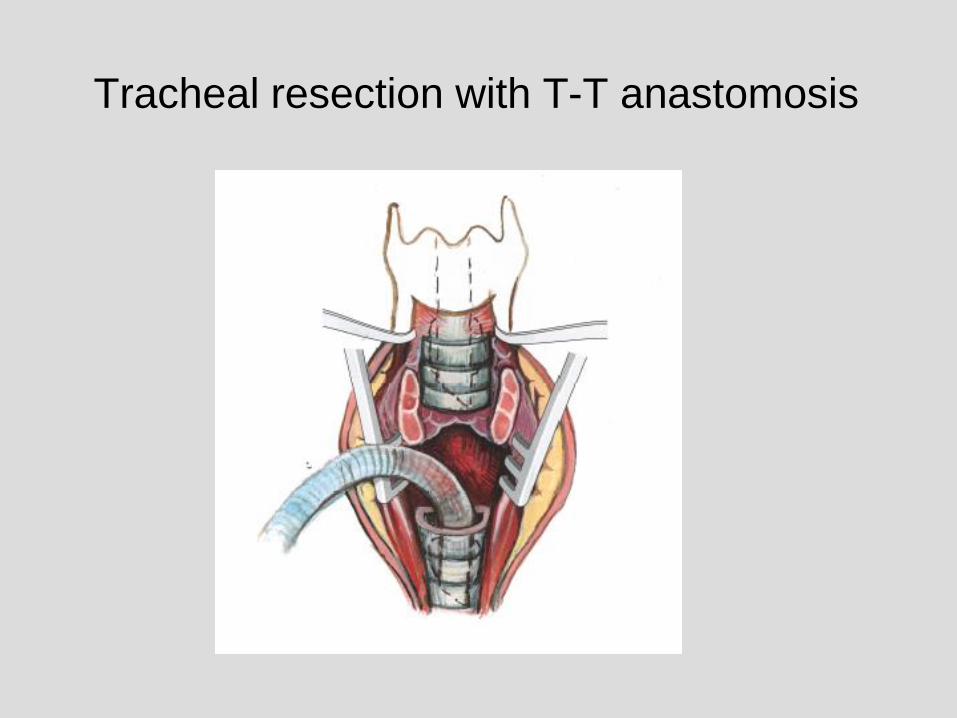
Tracheal resection with T-T anastomosis
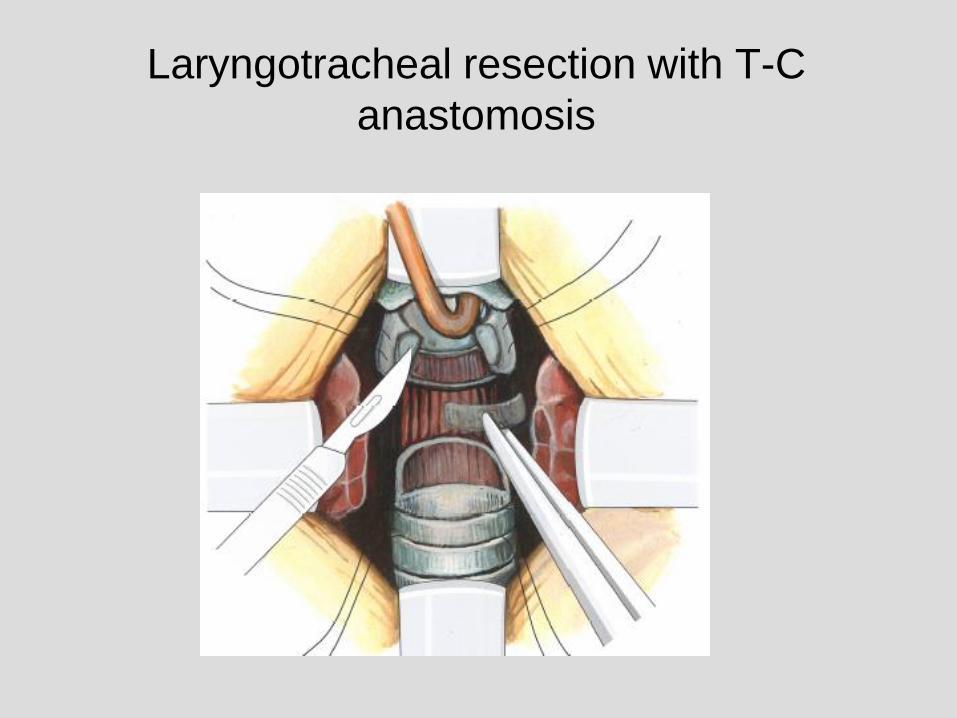
Laryngotracheal resection with T-C
anastomosis
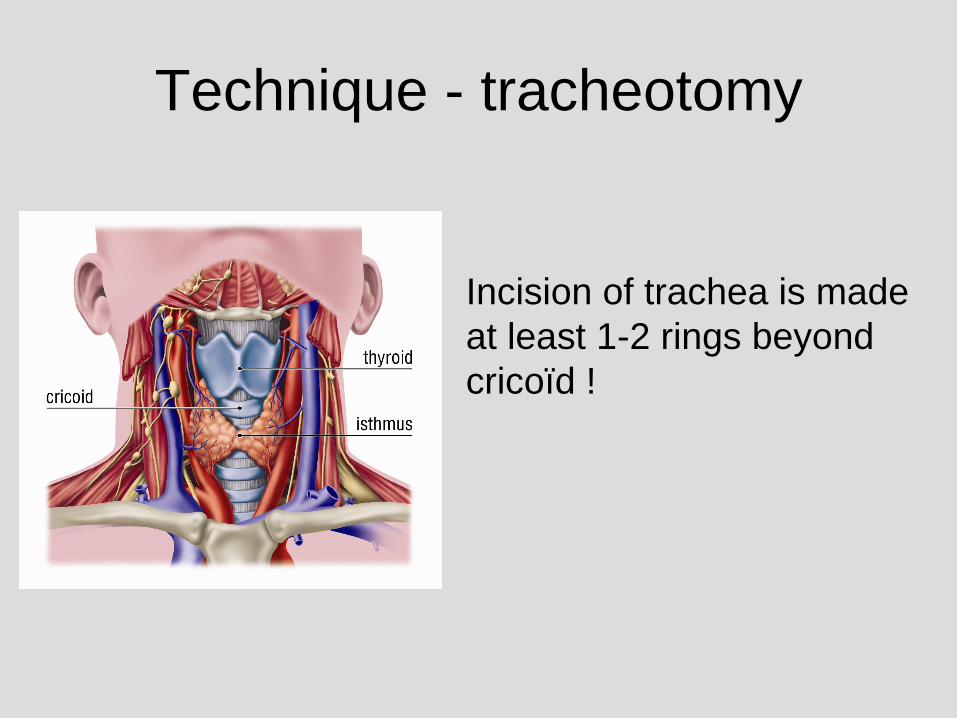
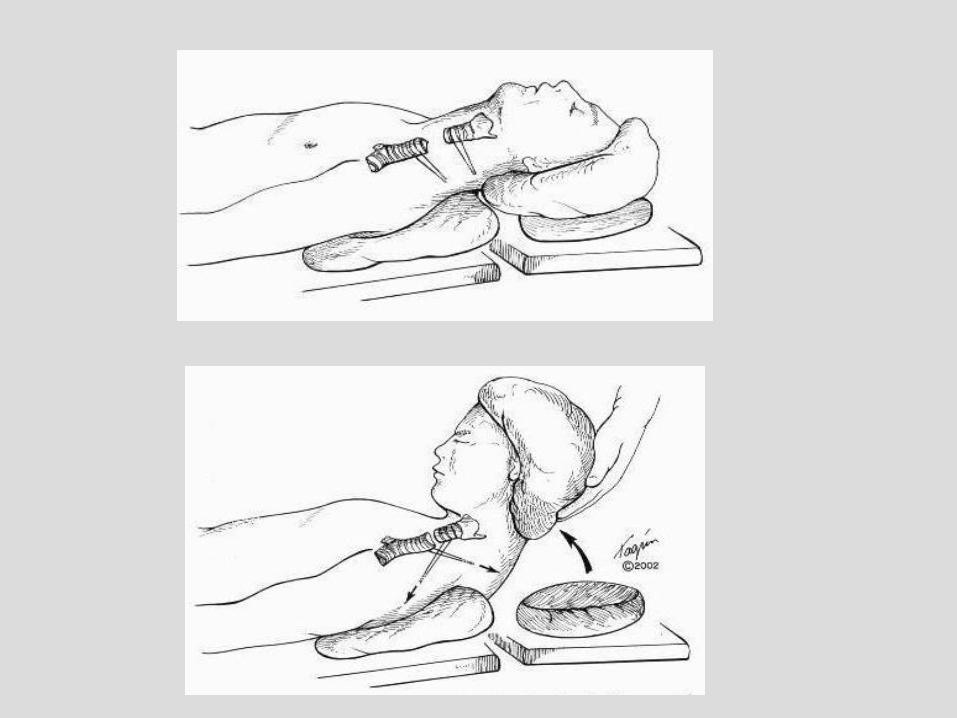
Technique - tracheotomy
Incision of trachea is made
at least 1-2 rings beyond
cricoïd !
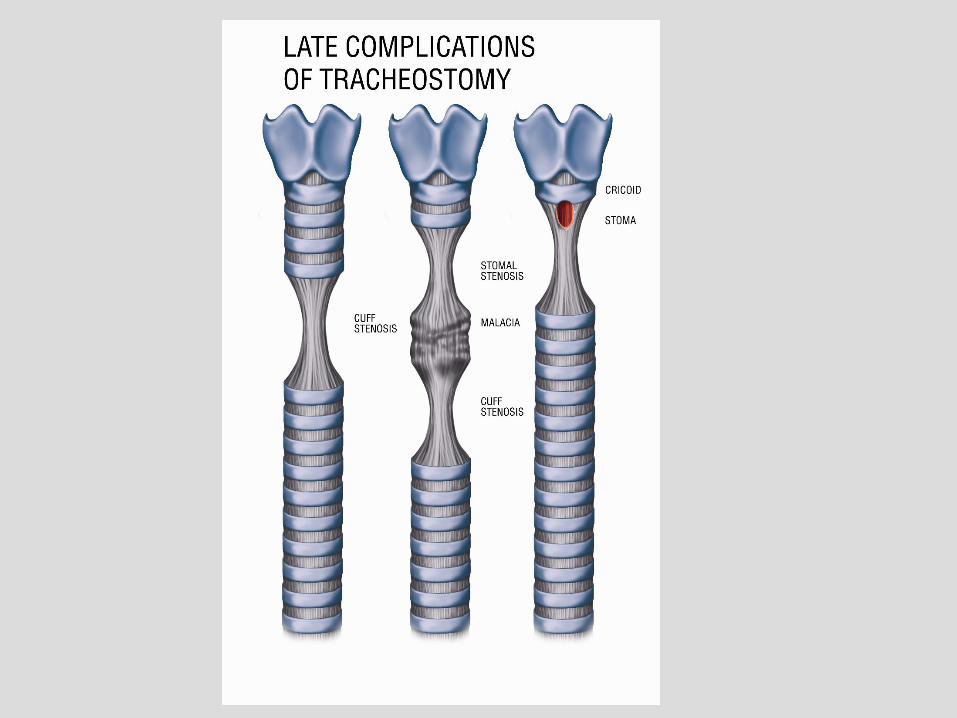
Benign stenosis
• Bronchoscopy : length of stenosis.
Indication for surgery!!
• CT scan (sagittal plane) : distance from
posterior cricoid plate
• If stent : removal, bronchoscopy and CT
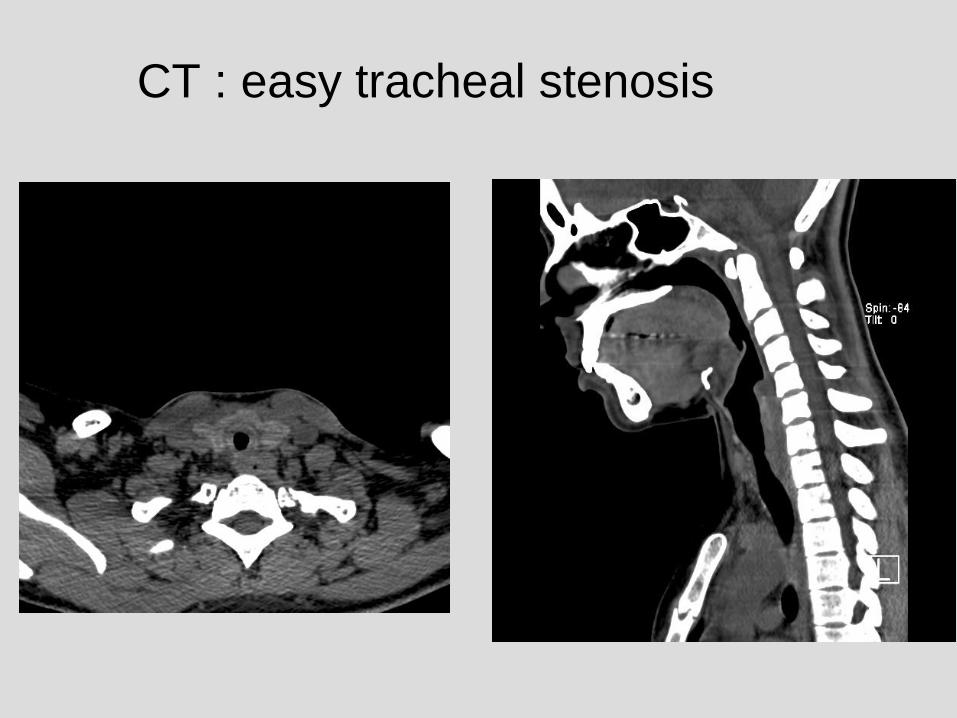
CT : easy tracheal stenosis
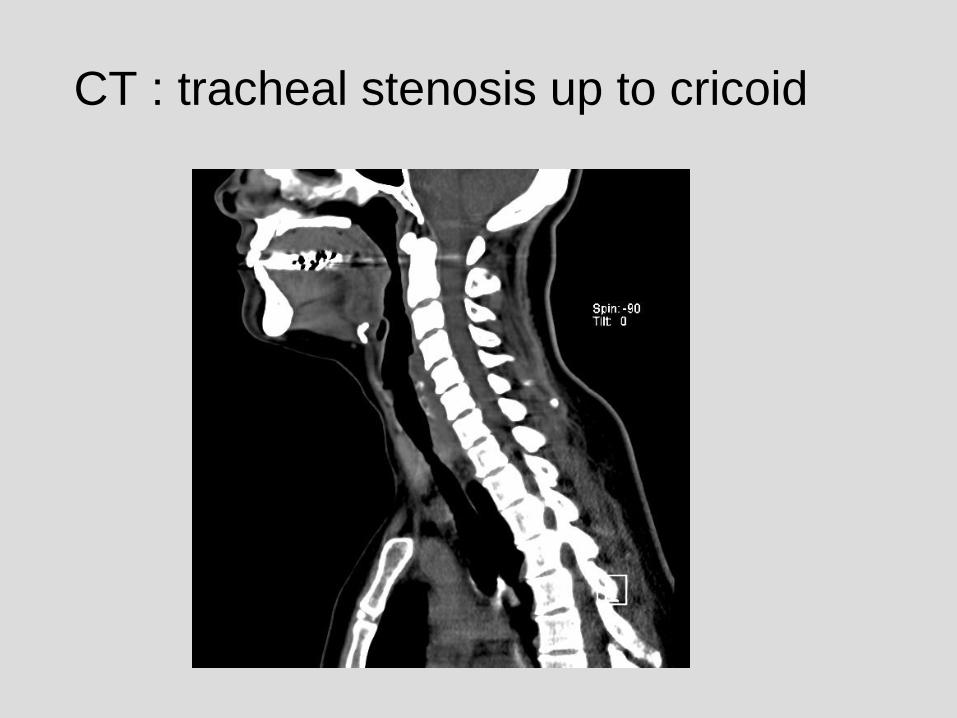
CT : tracheal stenosis up to cricoid
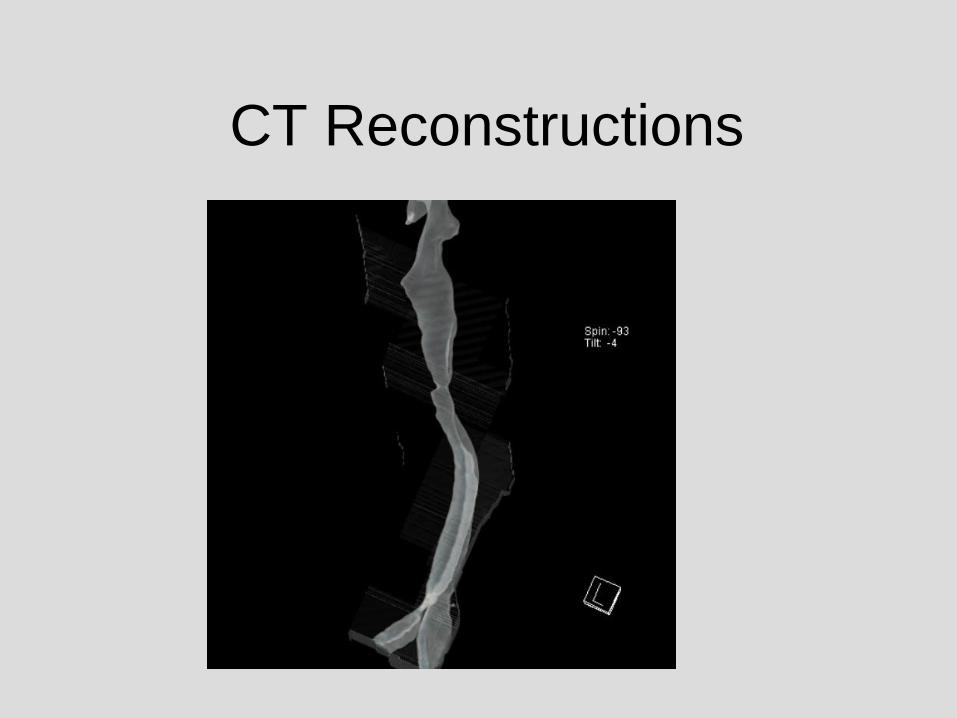
CT Reconstructions
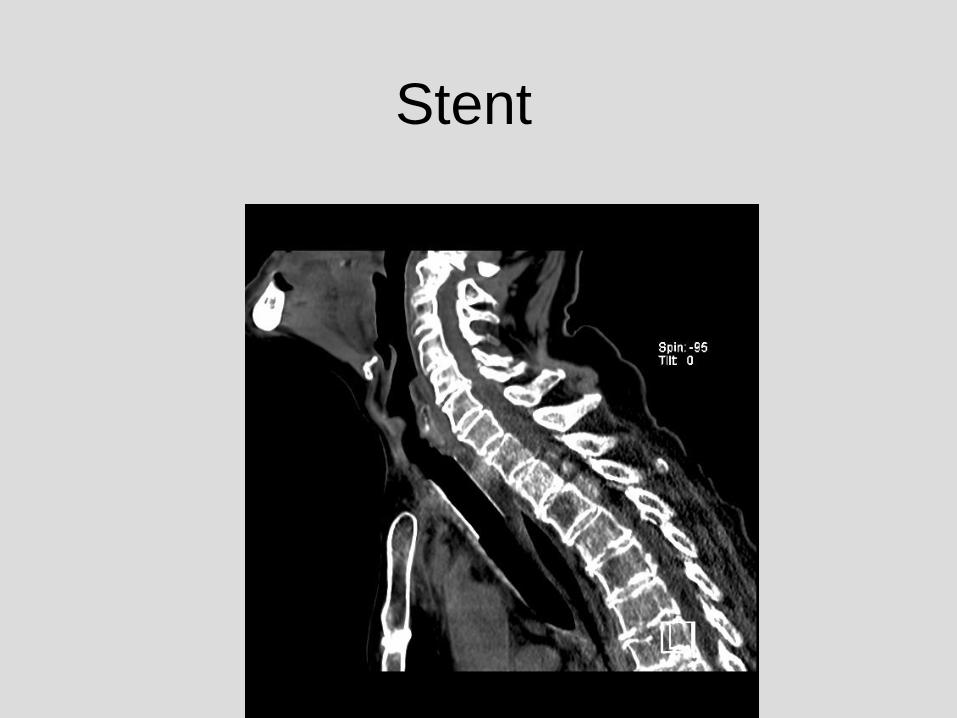
Stent
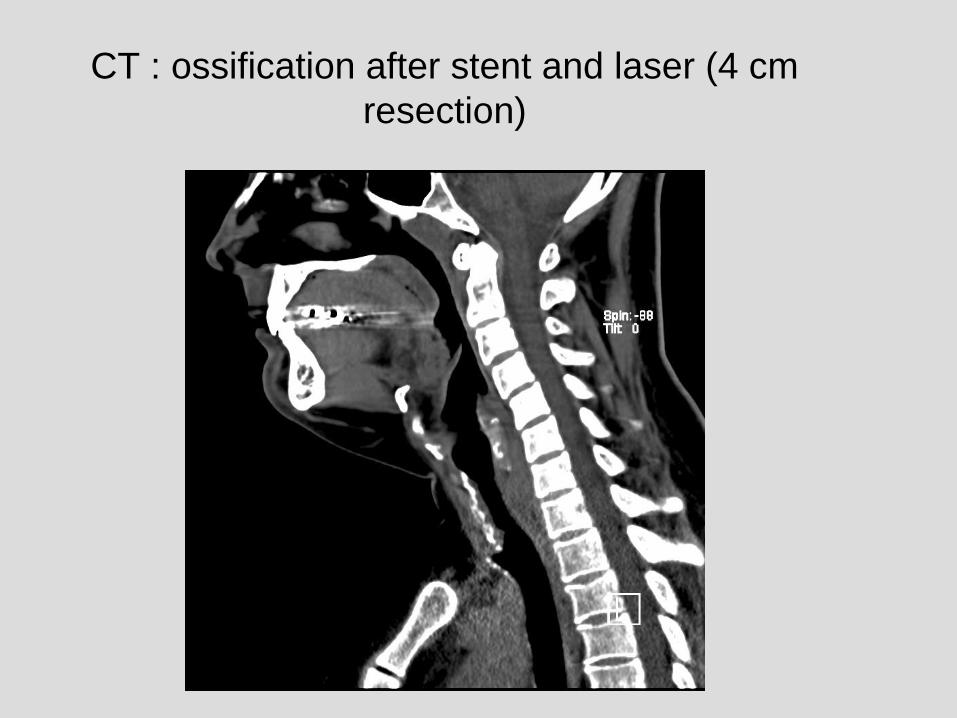
CT : ossification after stent and laser (4 cm
resection)
Technique
• Experience of anesthesiologist!
• Endotracheal intubation
• Laryngeal mask is a good alternative
• IV anesthesia (since several periods of
apnea for performing )anastomosis

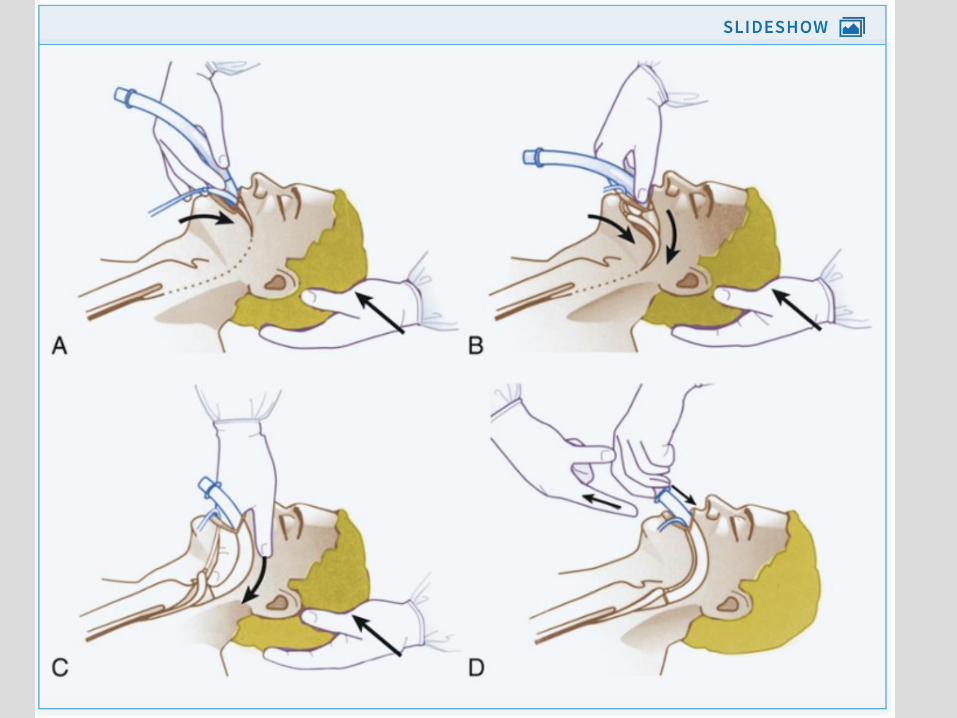
Classical laryngeal mask
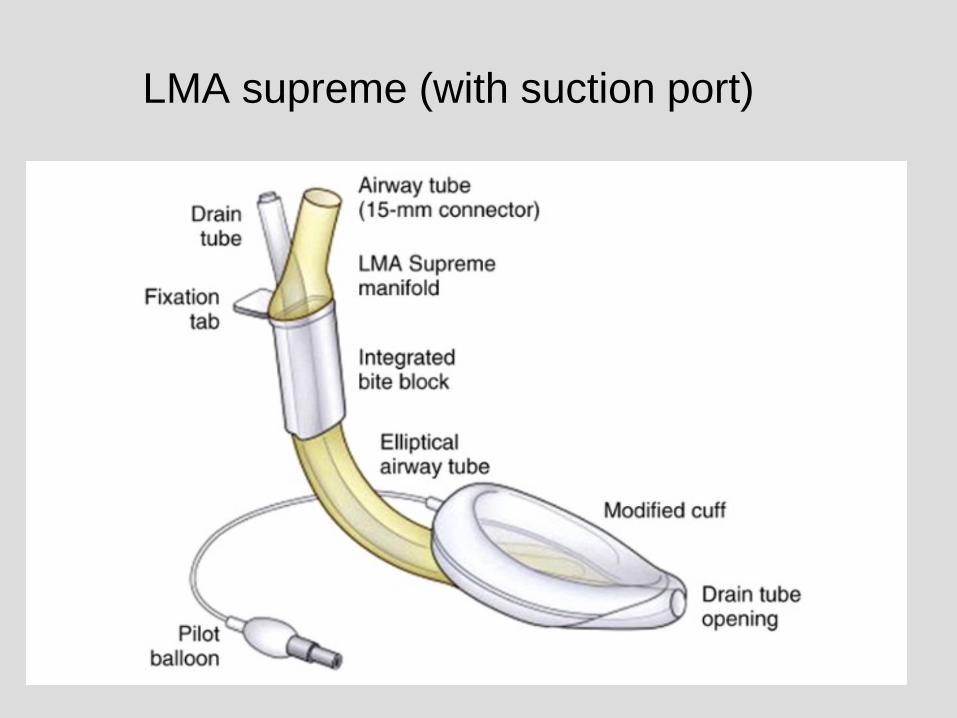
LMA supreme (with suction port)
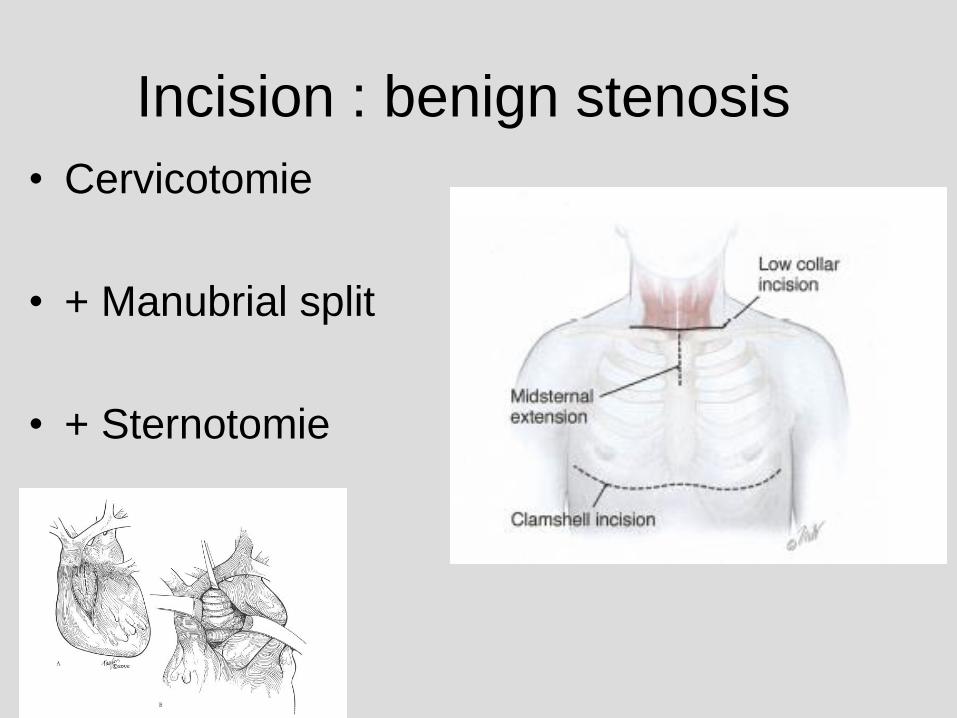
Incision : benign stenosis
• Cervicotomie
• + Manubrial split
• + Sternotomie
Anatomy
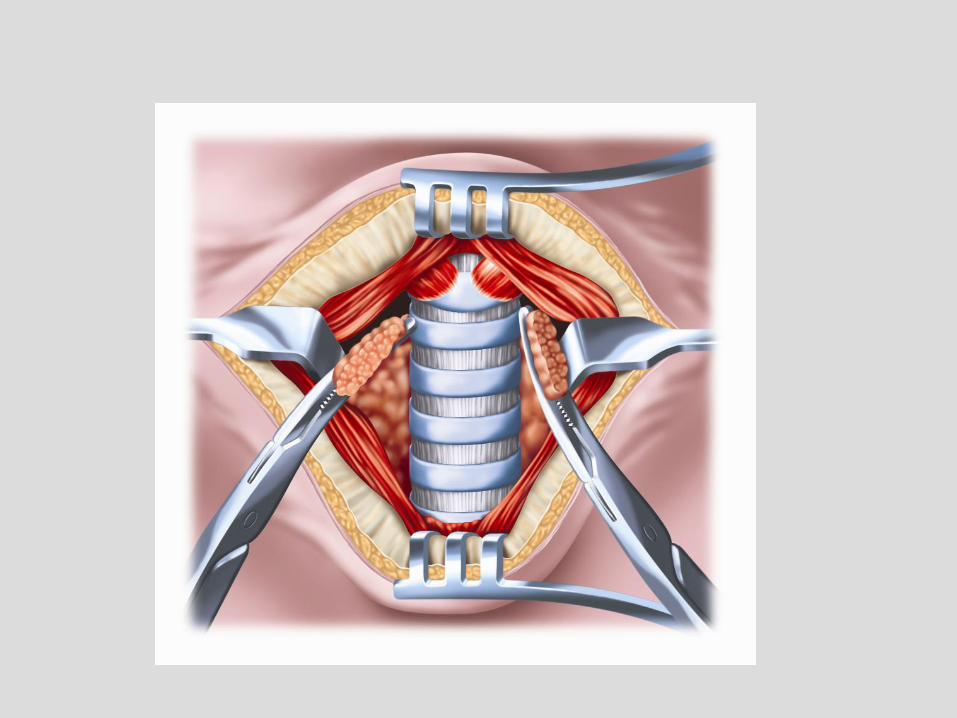
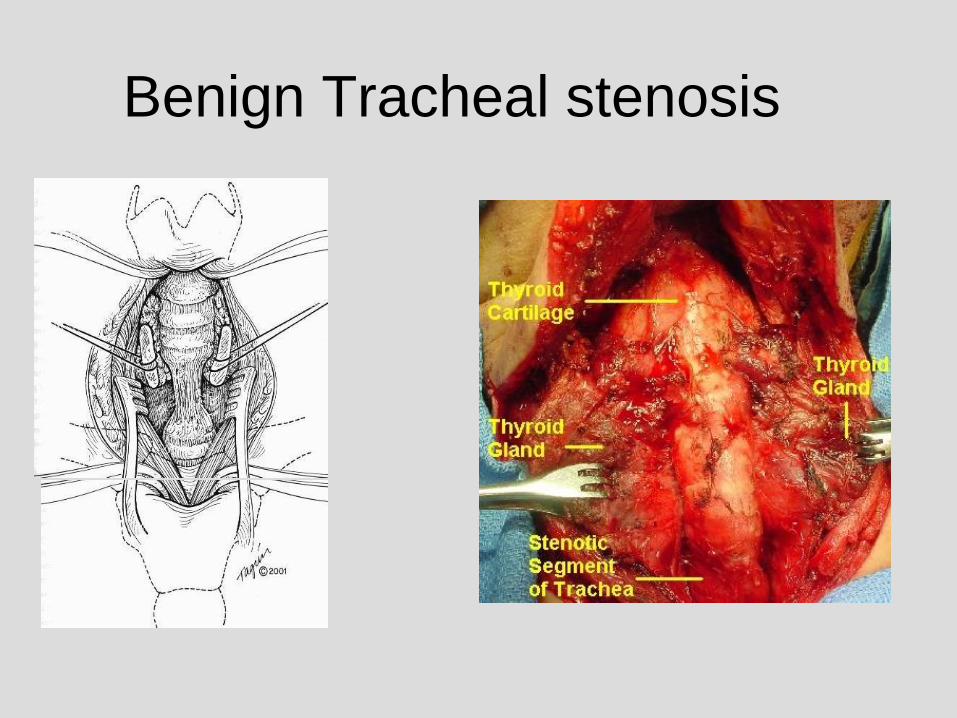
Benign Tracheal stenosis
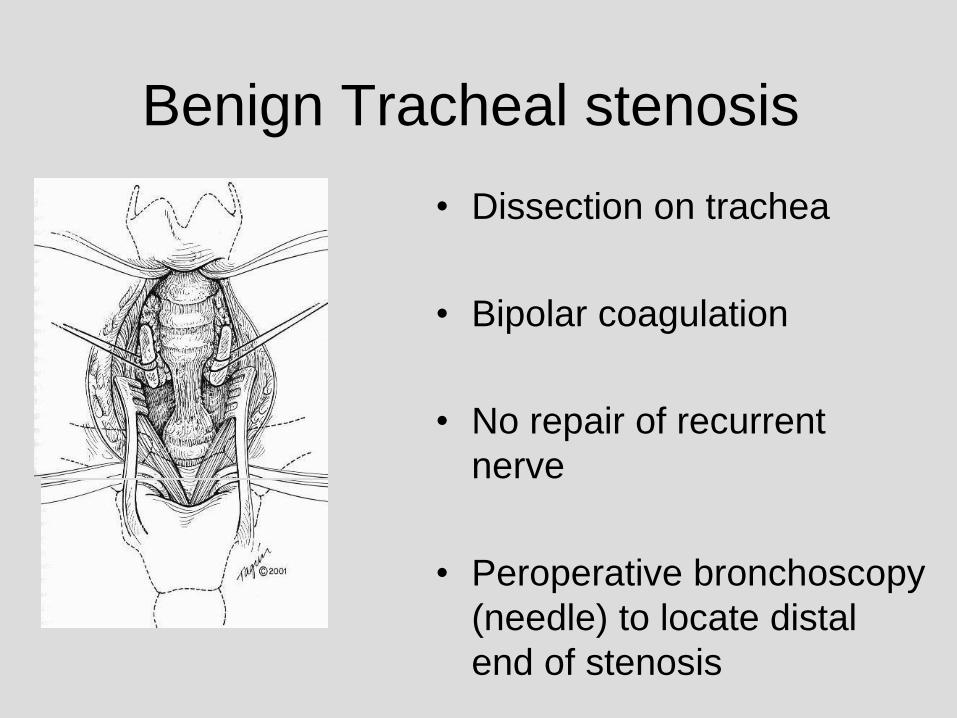
Benign Tracheal stenosis
• Dissection on trachea
• Bipolar coagulation
• No repair of recurrent
nerve
• Peroperative bronchoscopy
(needle) to locate distal
end of stenosis
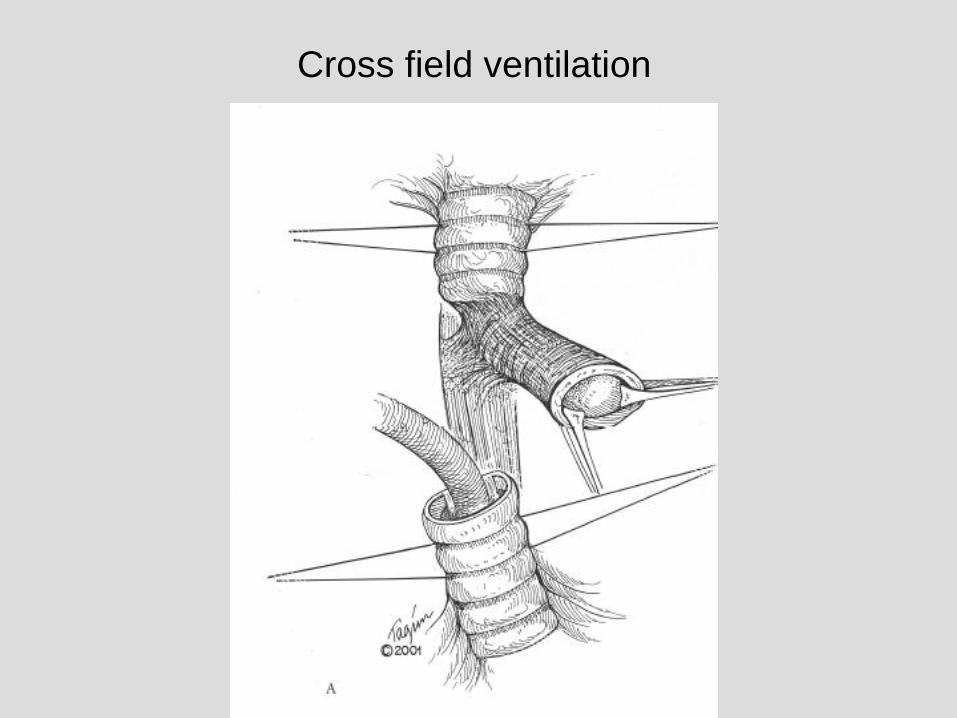
Cross field ventilation
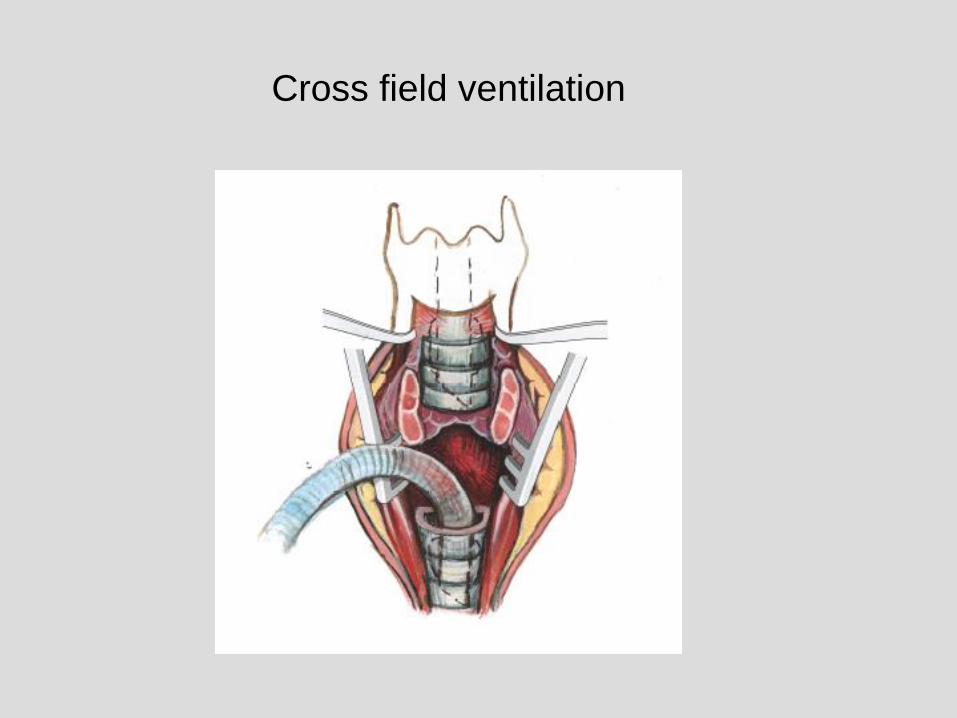
Cross field ventilation
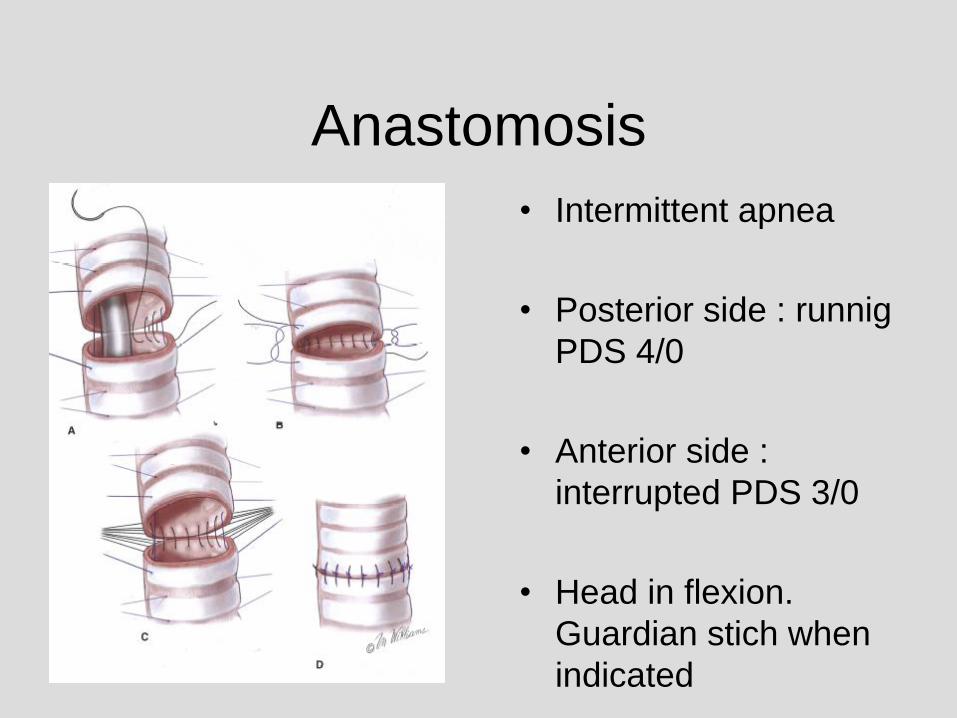
Anastomosis
• Intermittent apnea
• Posterior side : runnig
PDS 4/0
• Anterior side :
interrupted PDS 3/0
• Head in flexion.
Guardian stich when
indicated
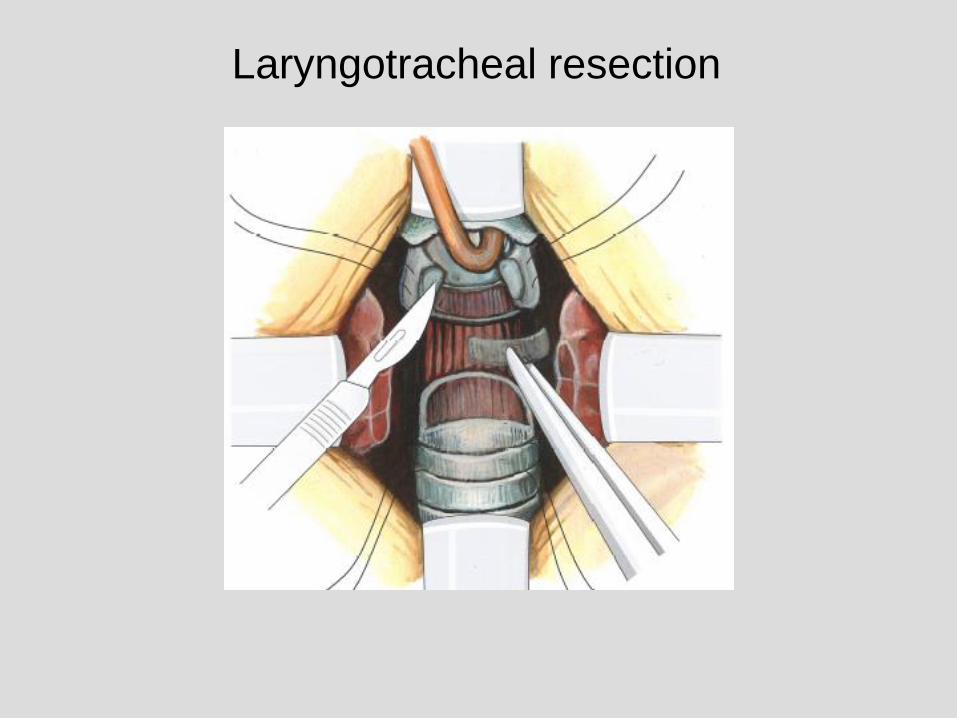
Laryngotracheal resection
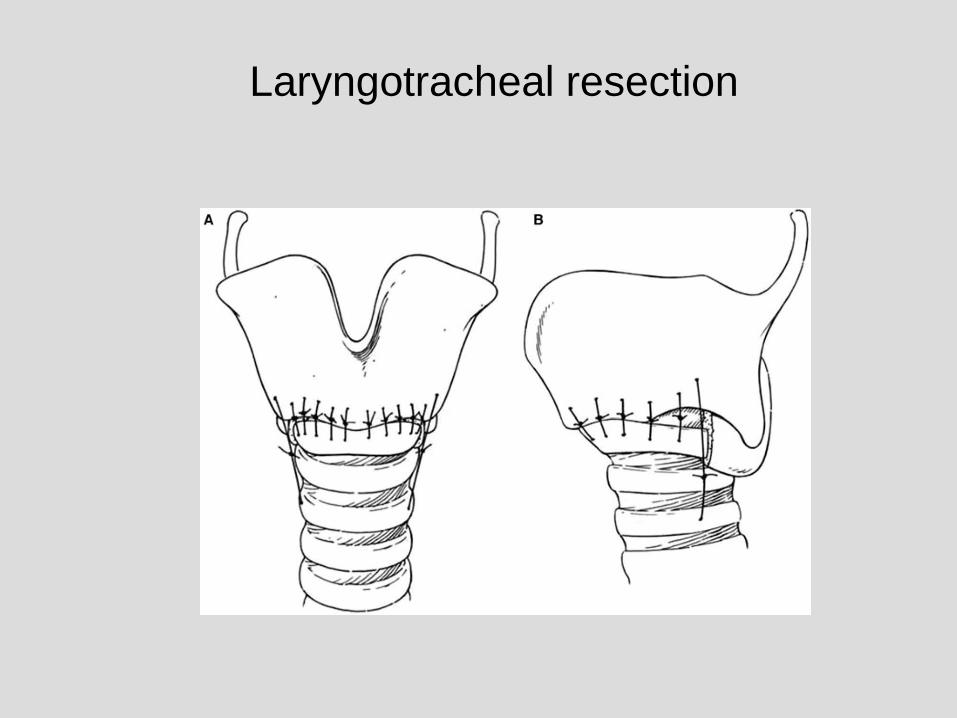
Laryngotracheal resection
Benign tracheal and laryngotracheal
stenosis : surgical treatment and results
• Retrospective series 65 patients
• Cervical approach in 60, cervical split 4, sternotomy : 1
• 70% tracheal resections and 30% laryngotracheal
resections
Rea et al, Europ J Cardiothorac Surg 2002
Benign tracheal and laryngotracheal
stenosis : surgical treatment and results
• Postoperative mortality : 1(1,5%)
• Major complications : 8(12,3%)– Anastomotic dehiscence : 4
– Vocal cord paralysis : 2
– Deglutition problems : 1
– Restenosis : 1
• Minor complications : 15 (23%)– Temporary vocal cord dysfunction : 8
– Superficial wound infection 5
– Anastomotic granulation tissue 2
Rea et al, Europ J Cardiothorac Surg 2002
Predictors for postoperative complications
after tracheal resection
• Retrospective analysis 94 patients (patients with
idiopathic laryngotracheal resections were excluded
• Complications more common in laryngotracheal
resections and lenght of resection is important
Bibas et al, Ann Thorac Surg 2014
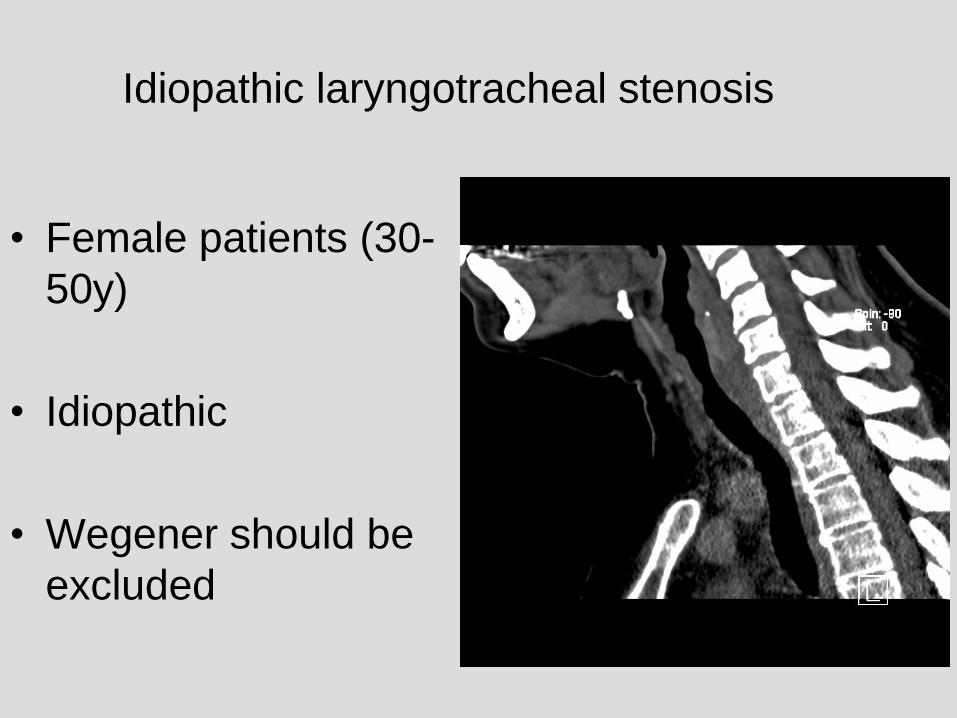
Idiopathic laryngotracheal stenosis
• Female patients (30-
50y)
• Idiopathic
• Wegener should be
excluded
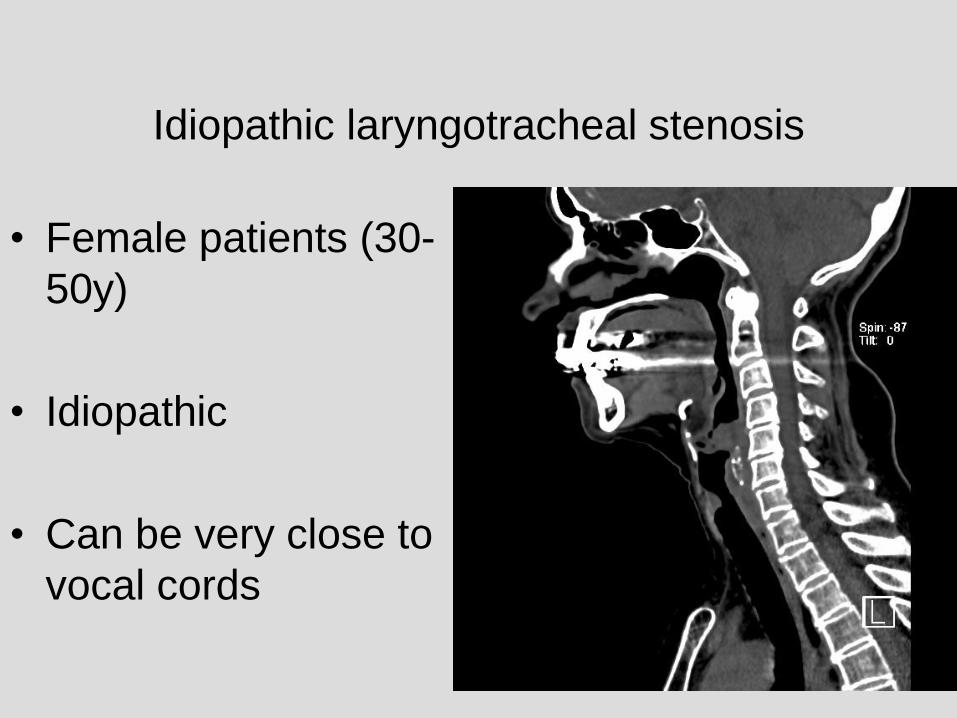
Idiopathic laryngotracheal stenosis
• Female patients (30-
50y)
• Idiopathic
• Can be very close to
vocal cords
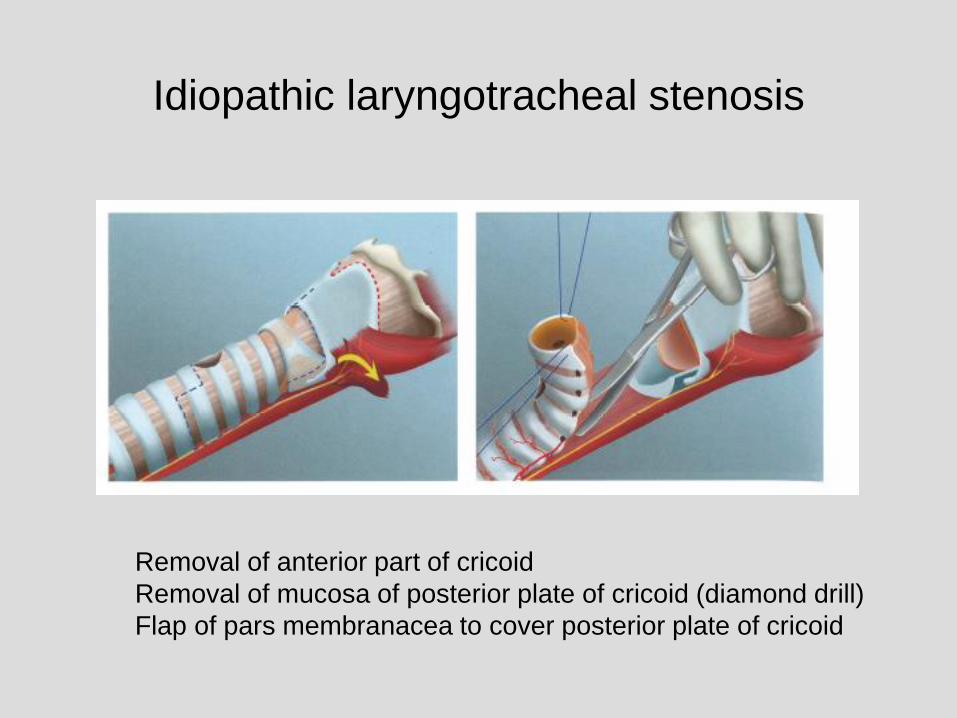
Idiopathic laryngotracheal stenosis
Removal of anterior part of cricoid
Removal of mucosa of posterior plate of cricoid (diamond drill)
Flap of pars membranacea to cover posterior plate of cricoid
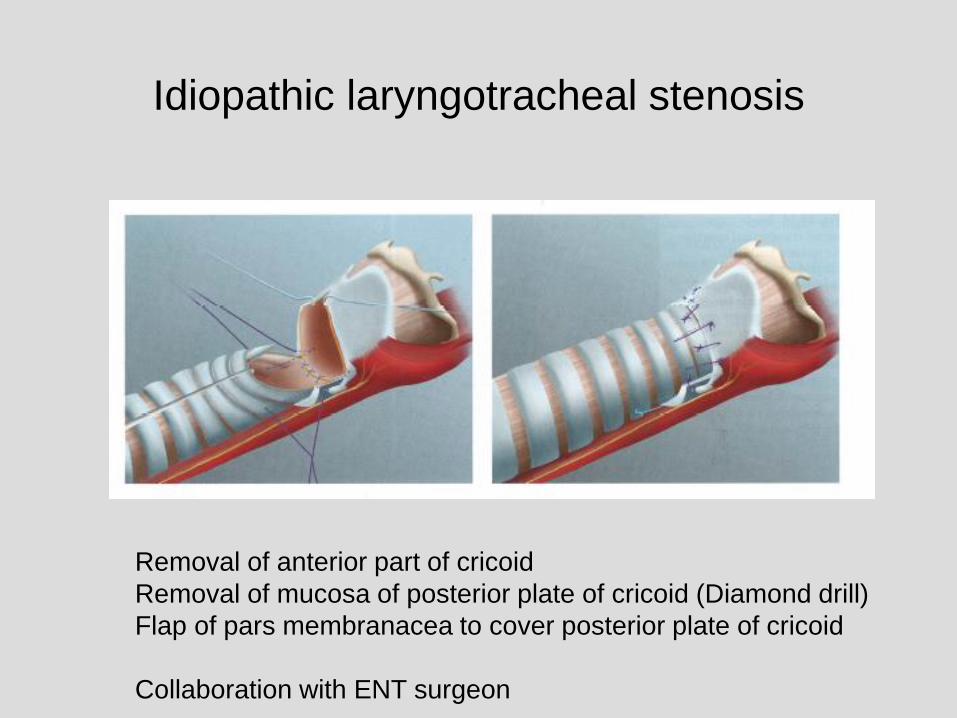
Idiopathic laryngotracheal stenosis
Removal of anterior part of cricoid
Removal of mucosa of posterior plate of cricoid (Diamond drill)
Flap of pars membranacea to cover posterior plate of cricoid
Collaboration with ENT surgeon
Primary tumours of the
trachea
• Rare
• Epidemiological studies (USA,
Netherlands)
– Annual incidence 1-2%/miljon inhabitants
Primary tumours of the
trachea : pathology
• Malignant : 90%– Squamous cell carcinoma : 35% (50% in
epidemiological series)
– Adenoid Cystic carcinoma : 35%
– Carcinoids: 10%
– Lymphoma 3%
– Non-squamous cell carcinoma 3%
– Sarcoma 3%
• Benign : 10%
Primary tumours of the
trachea : diagnosis
• Bronchoscopy
• CT scan
• In some cases mediastinoscopy (just
before resection)
Tracheal surgery Leuven
1994 – april 2014
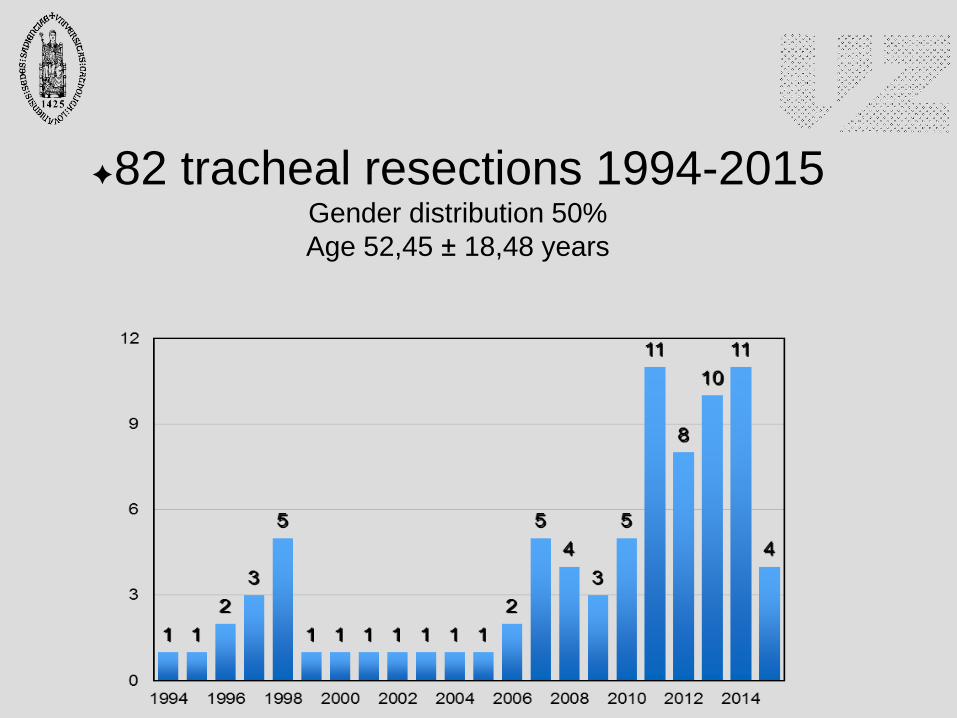
✦82 tracheal resections 1994-2015 Gender distribution 50%
Age 52,45 ± 18,48 years
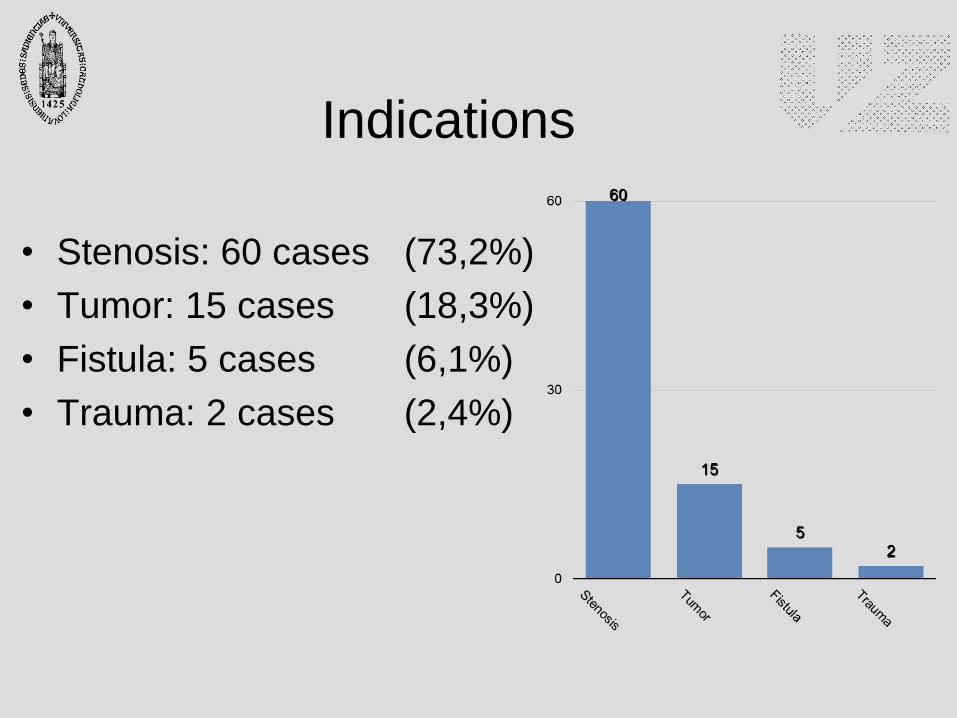
Indications
• Stenosis: 60 cases (73,2%)
• Tumor: 15 cases (18,3%)
• Fistula: 5 cases (6,1%)
• Trauma: 2 cases (2,4%)
Tracheal resection for stenosis
• Postintubation: 50 cases
• Idiopathic: 9 cases
• Compression: 1 case
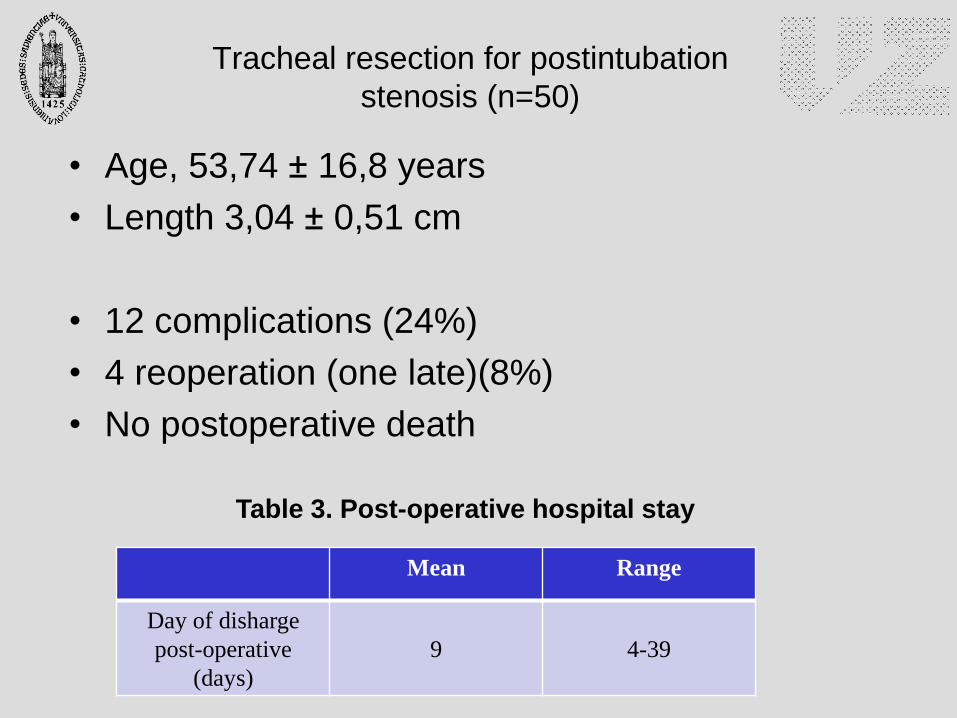
Tracheal resection for postintubation
stenosis (n=50)
• Age, 53,74 ± 16,8 years
• Length 3,04 ± 0,51 cm
• 12 complications (24%)
• 4 reoperation (one late)(8%)
• No postoperative death
Mean Range
Day of disharge
post-operative
(days)
9 4-39
Table 3. Post-operative hospital stay
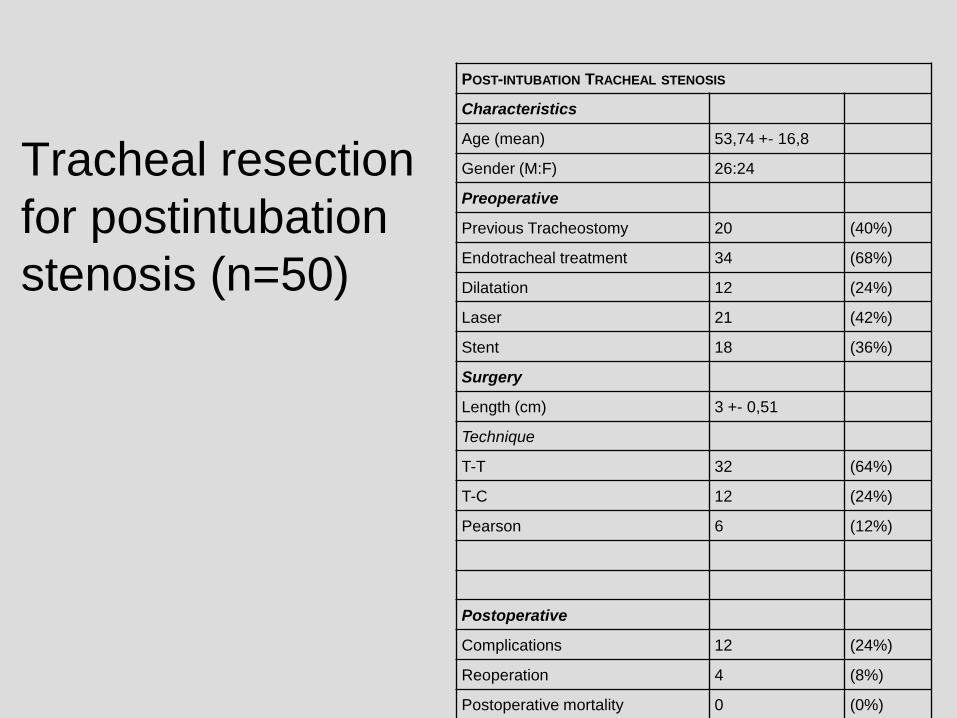
Tracheal resection
for postintubation
stenosis (n=50)
POST-INTUBATION TRACHEAL STENOSIS
Characteristics
Age (mean) 53,74 +- 16,8
Gender (M:F) 26:24
Preoperative
Previous Tracheostomy 20 (40%)
Endotracheal treatment 34 (68%)
Dilatation 12 (24%)
Laser 21 (42%)
Stent 18 (36%)
Surgery
Length (cm) 3 +- 0,51
Technique
T-T 32 (64%)
T-C 12 (24%)
Pearson 6 (12%)
Postoperative
Complications 12 (24%)
Reoperation 4 (8%)
Postoperative mortality 0 (0%)
• 30 (60%) patients had previous tracheostomy
• 34 (68%) had previous endobronchial intervention
– Stent 21 (42%), Laser 18 (36%), Dilatation 12 (24%)
– Single 19 (38%), Double 13 (26%), Triple 2 (4%)
Tracheal resection for postintubation
stenosis (n=50)
Tracheal resection for postintubation
stenosis (n=50)Approach:
• 43 (86%) cervicotomy, 5 (10%) partial sternotomy, 2
(4%) sternotomy
Technique:
• 32 (64%) Tracheal-Tracheal
• 12 (24%) Tracheal-Cricoid
• 6 (12%) Pearson
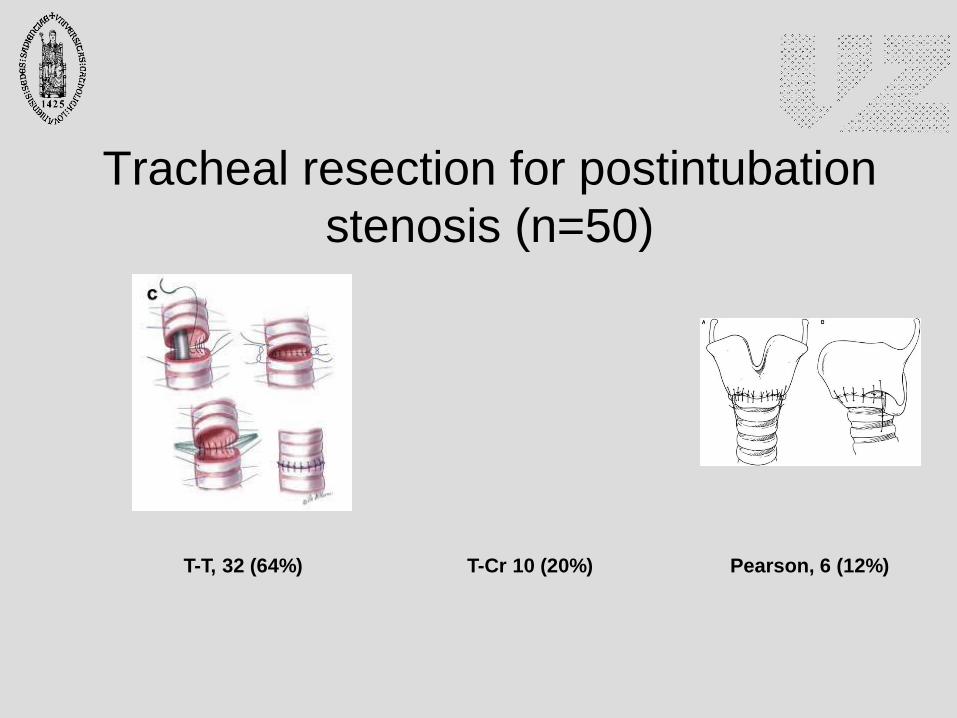
T-T, 32 (64%) Pearson, 6 (12%)T-Cr 10 (20%)
Tracheal resection for postintubation
stenosis (n=50)
Tracheal resection for postintubation
stenosis (n=50)
12 patients had complications
24% of all surgeries
4 patients needed a reoperation
3 for tracheostomy (1 permanent)
1 Posterior plate enlargement (after 2 years)
No hospital mortality
Tracheal resection for postintubation stenosis
(n=50). Complications in 12 patients
• Tracheostomies : 3– subglottic stenosis 85 y
– laryngeal oedema (removed 6 weeks)
– anterior dehiscence (removed after 6 weeks)
• Dehiscence : 2– Tracheostomy
– No treatment : discharged d 10
• Reintubation : 2
Tracheal resection for postintubation stenosis
(n=50). Complications in 12 patients
• Stenosis : 2– Tracheostomy
– Posterior enlargement (after 2 years)
• Wound infection: 2
• ARDS : 1
• Pneumonia : 1
• Other (minor) : 2
Tracheal resection for tumor
• Primary tracheal tumor, 11
• Infiltration , 2
• Metastases, 1
• Recurrence, 1
Squamous, 2
Adenoid Cystic, 5
Sarcoma, 1
Leiomioma, 1
Carcinoid, 1
Clear cell, 1
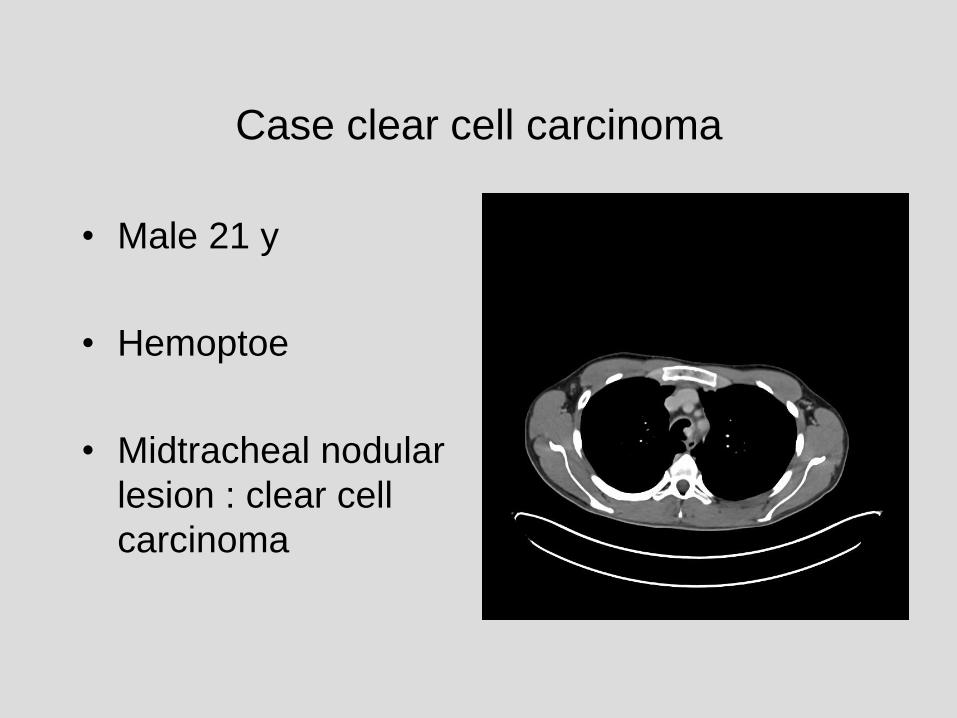
Case clear cell carcinoma
• Male 21 y
• Hemoptoe
• Midtracheal nodular
lesion : clear cell
carcinoma
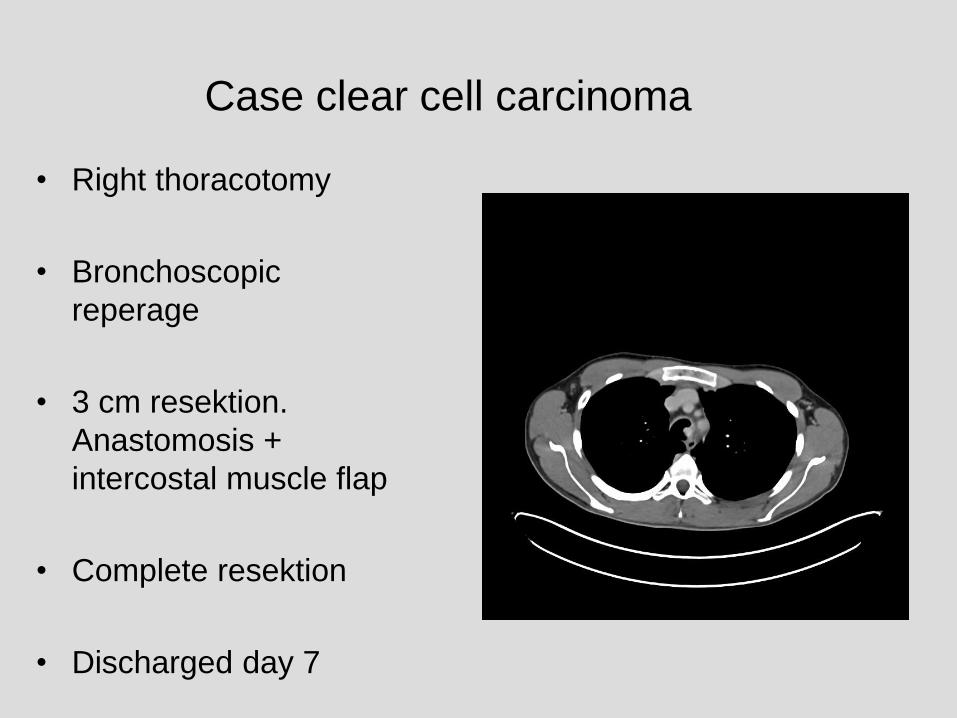
Case clear cell carcinoma
• Right thoracotomy
• Bronchoscopic
reperage
• 3 cm resektion.
Anastomosis +
intercostal muscle flap
• Complete resektion
• Discharged day 7
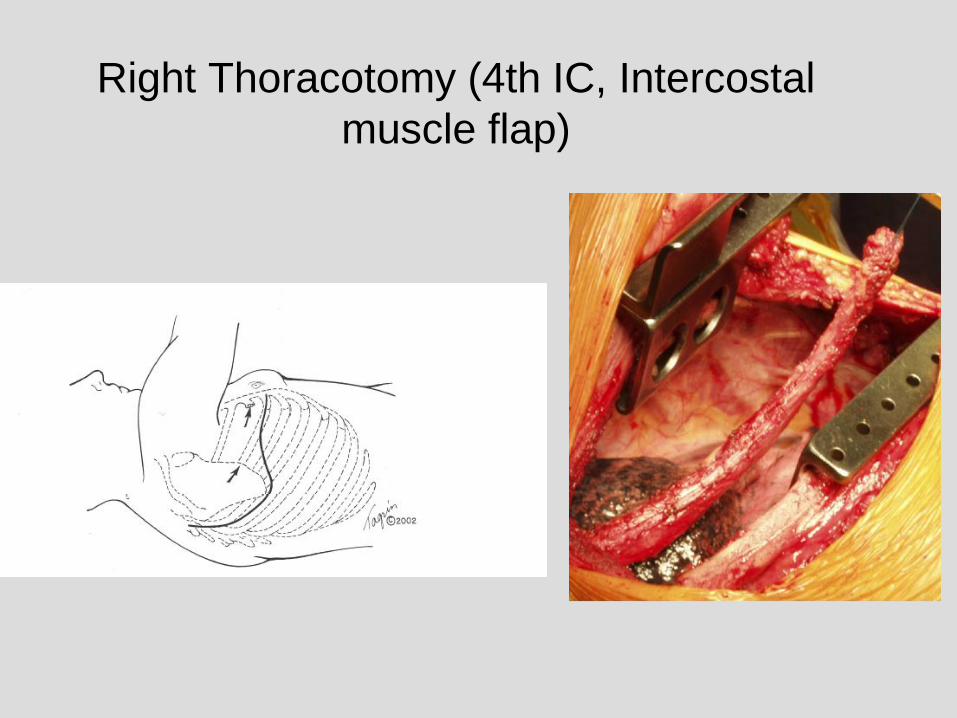
Right Thoracotomy (4th IC, Intercostal
muscle flap)
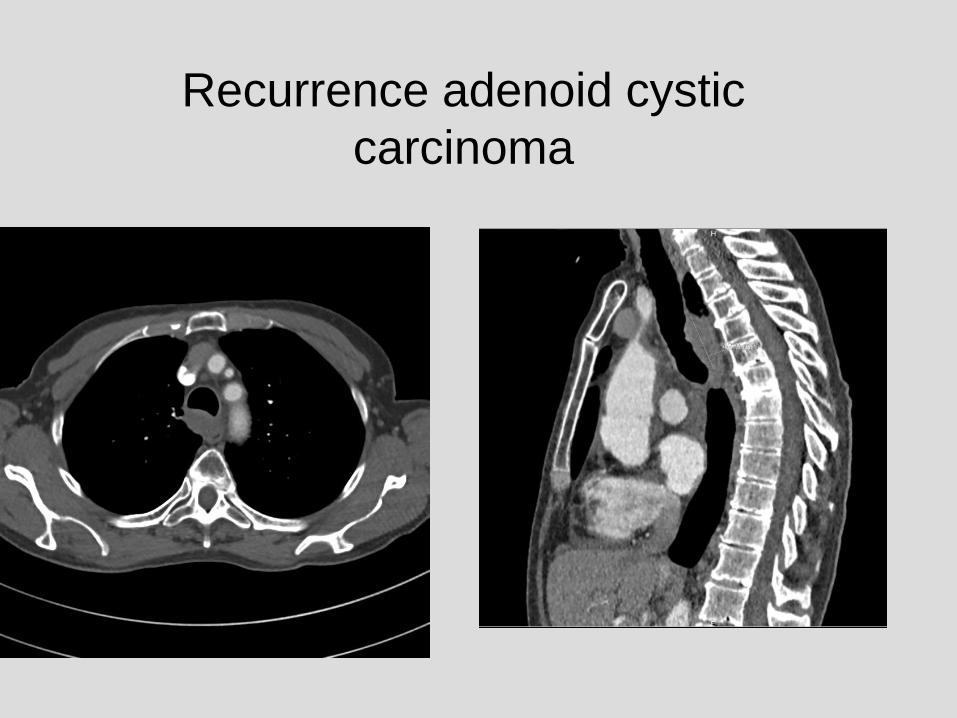
Recurrence adenoid cystic
carcinoma
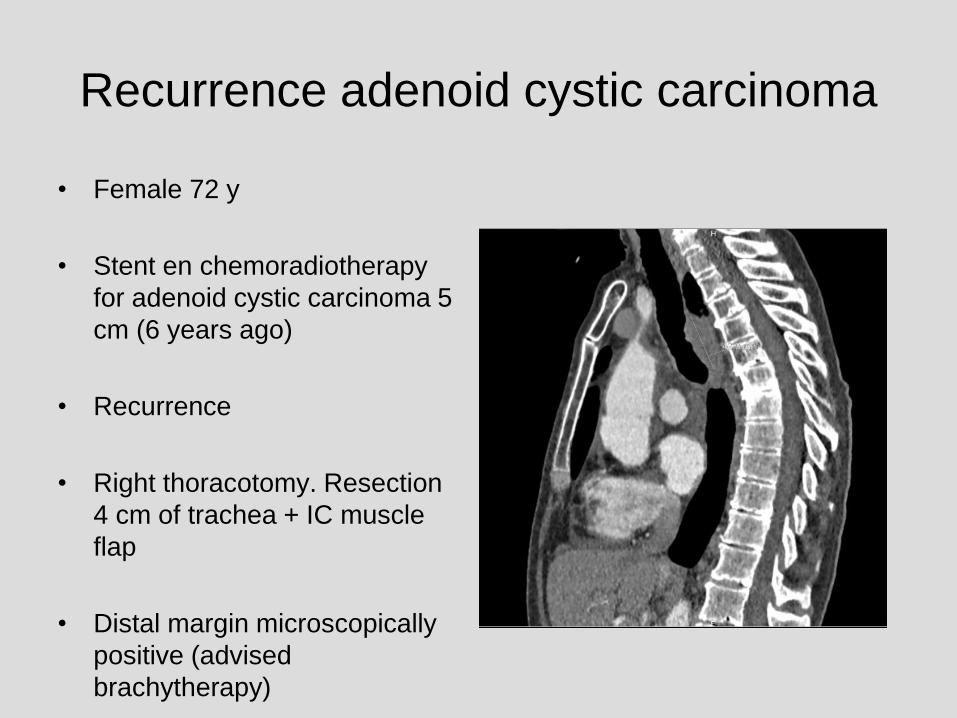
Recurrence adenoid cystic carcinoma
• Female 72 y
• Stent en chemoradiotherapy
for adenoid cystic carcinoma 5
cm (6 years ago)
• Recurrence
• Right thoracotomy. Resection
4 cm of trachea + IC muscle
flap
• Distal margin microscopically
positive (advised
brachytherapy)

Bronchoscopy 7 days
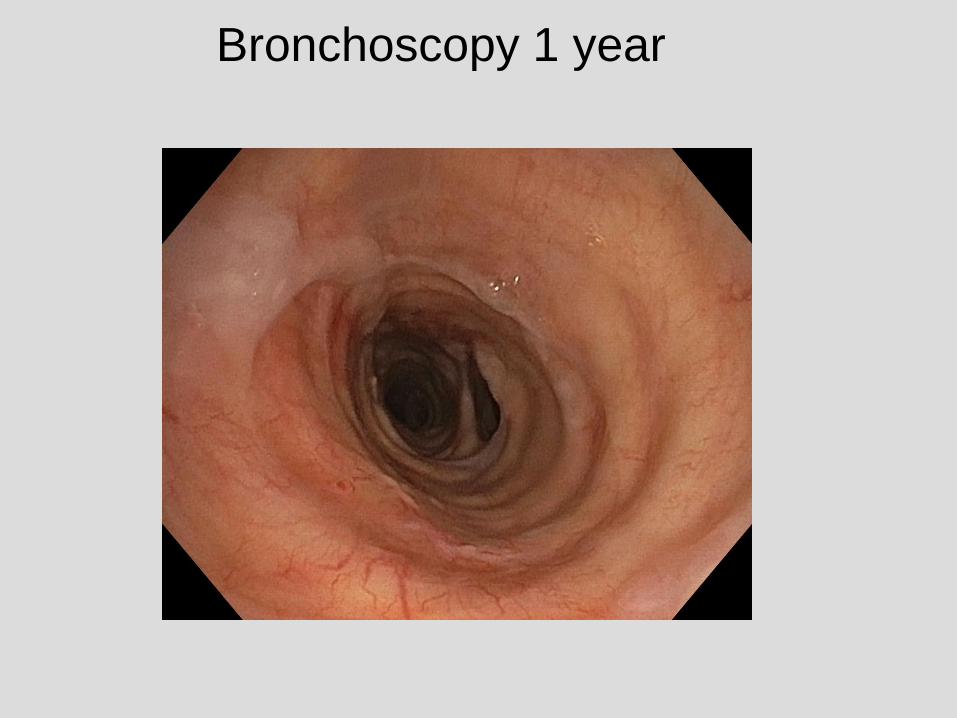
Bronchoscopy 1 year
Conclusion
• Multidisciplinary approach!
• Tracheal surgery requires meticulous
surgical technique
• Good results with surgery for benign
stenosis
• Idiopathic laryngotracheal stenosis and
tracheal tumors : rare and complex
disease


![Primary tracheal schwannoma a review of a rare entity ......include benign, intermediate, and malignant tumors [1]. Neurogenic tumors of the tracheobronchial tree are ex-tremely rare](https://img.pdfslide.net/doc/110x75/60f7b75799a3976448468c79/primary-tracheal-schwannoma-a-review-of-a-rare-entity-include-benign-intermediate.jpg)
![Percutaneous tracheostomy: An evaluation of the damage to ...€¦ · percutaneous tracheostomy and it was suggested that this had a role in tracheal stenosis [9]. Unlike that study,](https://img.pdfslide.net/doc/110x75/6064a8a5ab105d08385c7a95/percutaneous-tracheostomy-an-evaluation-of-the-damage-to-percutaneous-tracheostomy.jpg)