Embed Size (px)
DESCRIPTION
RSPT 1060. MODULE C – Applied Physics Lesson #1 - Mechanics. OBJECTIVES. At the end of this module, the student should be able to… define the terms and abbreviations used in the module. draw & explain the equation of motion. - PowerPoint PPT Presentation
Citation preview

RSPT 1060
MODULE C – Applied Physics
Lesson #1 - Mechanics

OBJECTIVES• At the end of this module, the
student should be able to…• define the terms and abbreviations
used in the module.• draw & explain the equation of
motion.• list the forces that oppose lung
inflation & cause the work of breathing.
• list the different types of compliance, their normal values & equations.

OBJECTIVES
• At the end of this module, the student should be able to…• differentiate between compliance &
elastance.• list some pulmonary disorders that
could change compliance.• explain the relationship between
pressure, surface tension & radius.• explain how LaPlace’s Law relates to
surface tension.

OBJECTIVES• At the end of this module, the student
should be able to…• explain the purpose of surfactant.• list the different types of resistance,
their normal values and equations.• explain how Poiseuille’s Law relates
to resistance.• list some pulmonary diseases that
will alters resistance.• explain what the equal pressure
point is.

Ventilation vs. Respiration
• Ventilation: The bulk movement of gas in and out of the lung.
• Respiration: The exchange of gas (specifically oxygen and carbon dioxide) at the cellular level.• Internal Respiration: The exchange of
gas between a peripheral capillary and a cell of the body.
• External Respiration: the exchange of gas across the alveolar-capillary membrane.

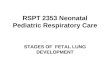
EQUATION OF MOTION
STRETCH
FRICTION
Flow ResistanceCompliance
Volume Inflate toPressure

Equation of Motion
Mechanical positive
pressure to inflate
Resistance (gas flow)
Compliance (volume)
Muscle negativ
e pressur
e to inflate

Contraction
Thorax-Diaphragm Pump
Pressure
Ventilator-Pump
PMUS
Mechanical Ventilator vs. Spontaneous Breathing

Inflation pressure• Spontaneous Breathing
• Contraction of muscles generates a negative pressure in lungs & gas is pulled into lungs.
• Work done by patient.
• Mechanical Ventilator• Positive pressure builds in the ventilator
circuit & gas is pushed into the lungs.• Work done by machine.

WORK OF BREATHING• FORCES OPPOSING INFLATION
• Elastic (stretch)• Physical tendency of an object to resist
stretching
• Non-elastic (friction)• Occurs only when gas and the system is
moving

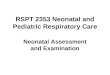
Work of Breathing
Compliance Resistance
Elastic Work
(Stretch)
Non-elastic Work
(Friction)
65% 35%
Lungs & Chest Wall Tissue & Airway
(20%)(80%
)Lungs
Ribs
Diaphragm
Abd. organs
Airways
Gas flow
Surfactant
Tissue
Lungs
Pleura
Skeletal
Muscular
Skin

COMPLIANCE• ELASTIC OPPOSITION TO INFLATION
• Elastic and collagen fibers found in lung parenchyma give the lungs elasticity.
• Inflation - occurs as a result of forcibly stretching lung fibers during inspiration. (work)
• Deflation or exhalation is normally passive.
• The resting position of the lung is deflation.

Compliance• Pressure-Volume loop
Vol
Pressure
Low compliance
Normal Compliance
High Compliance

Compliance• Pressure-Volume loop
Vol
Pressure
Low volume (opening)
Normal volume (filling)
High volume (over-inflated)

EXPERIMENT• Balloon
• Initial inflation – easy or difficult?
• Normal inflation – easy or difficult?
• Over inflation – easy or difficult?

Compliance• Compliance: Distensibility of the lung
• Elastance: Property of resisting deformation or desire to return to original shape
ElastanceCompliance
1

Comparison
Example: Tennis ball vs. Balloon
• Tennis ball • High elastance & low compliance
• High resistance to change in shape• Low ability to stretch
• Balloon• Low elastance & high compliance
• Low resistance to change in shape• High ability to stretch

Comparison
Normal lung vs. Emphysema vs. Pneumonia
• Normal lung • Normal elastance & Normal compliance
• Returns to original shape easily• Easily filled
• Emphysema• Low elastance & high compliance
• Does not return to original shape easily (floppy)• Easily stretched until air-trapping occurs
• Pneumonia• High elastance and low compliance
• Readily returns to collapsed state• Very difficult to inflate

Compliance
Compliance =▲Volume (liters)
▲Pressurepl (cmH2O)=
Total Compliance is composed of:Lung ComplianceChest Wall Compliance

Lung Compliance
Disease states that cause a change in lung compliance?
• Decrease• Fibrosis• Adult Respiratory Distress Syndrome• Pulmonary Edema
• Increase• Emphysema

Lung Compliance• How will a patient with decreased
lung compliance breathe?
• Rapid• Shallow

Experiment• Wrap belt tightly around chest.
• Breathe slow & deep• Breath rapid & shallow
• Which feels better?

Chest Wall Compliance• “Stiffness” of chest wall
• When thorax is intact, its resting level is FRC
• With disruption to chest wall – lung collapse and chest wall expands (open pneumothorax)
• Force of movement of chest wall is opposite that of lung • Chest Wall has tendency to expand (pull
out)• Lung has tendency to collapse (pull in)• At rest – they balance (FRC)

Chest Wall Compliance• Disease states that cause a change in
chest wall compliance?
• Decrease• Chest trauma• Chest burns• Kyphosis• Scoliosis• Chest wall deformity

Total Compliance• Normal Lung compliance = 0.2 L/cmH2O
• Normal Chest wall compliance = 0.2 L/cmH2O
• Normal Total compliance = 0.1 L/cmH2O
• Why is total less than the individual compliances?• Lungs at rest = collapse• Chest wall at rest = expansion• They are working in opposite directions

Calculation of Total Compliance
• Clinically we measure Dynamic and Static Lung Compliance
CDYNTidal Volume {Vt} (liters)
Peak Pressure – PEEP (cmH2O)=
CSTAT
Tidal Volume {Vt} (liters)
Plateau Pressure – PEEP (cmH2O)
=
With air movemen
t
No air movemen
t
NOTE: PEEP stands for Positive End Expiratory Pressure. It is the BASELINE or starting pressure.

Calculations
• Normal compliance = 0.1 Liter/cmH2O
Volume = 0.5 liters = 0.1 L/cmH2O
Pressure 5 cmH2O

Calculations
• Low compliance = 0.05 Liter/cmH2O
Volume = 0.5 liters = 0.05 L/cmH2O
Pressure 10 cmH2O
Stiffer lung needs more inflation pressure.

Calculations
• High compliance = 0.17 Liter/cmH2O
Volume = 0.5 liters = 0. 17 L/cmH2O
Pressure 3 cmH2O
Floppier lung needs less inflation pressure.

SURFACE TENSION
• The alveoli are like bubbles lined with fluid and filled with air.
• Surface tension is the attractive force exerted by like molecules at the liquid’s surface.
• Surface tension forces cause the bubble to collapse.

The Force of Surface Tension in a drop of liquid. Cohesive force (arrows) attracts molecules inside the drop to one another. Cohesion can pull the outermost molecules inward only, creating a centrally directed force that tends to contract the liquid into a sphere.

Two bubbles of different sizes with the same surface tension.
Bubble A, with the smaller radius, has the greater inward or deflating pressure and is more prone to collapse than the larger bubble B.
Because the two bubbles are connected, bubble A would tend to deflate and empty into bubble B.
Conversely, because of bubble A's greater surface tension, it would be harder to inflate than bubble B.
LaPlace’s Law

Calculation of Surface Tension
• LaPlace’s formula:
Pressure in a bubble
=4ST
r
ST = surface tension If surface tension increases, the pressure to inflate the bubble increases.
R = radiusIf the radius decreases, the pressure to open the alveoli increases.
P
P


Surfactant
• Alveoli are lined with a surface-tension lowering agent (surfactant) produced by alveolar type II cells.
• Surfactant has a low attractive force exerted by its molecules.
• Surfactant helps stabilize the alveoli so they do not collapse completely on each exhalation.
• Destruction of surfactant will significantly decrease compliance and increase the work of breathing.

Surface Tension
• Disorders altering or destroying surfactant:• Prematurity• Adult respiratory Distress Syndrome• Oxygen toxicity



RESISTANCE
• INELASTIC OPPOSITION TO INFLATION
• Occurs only when the system is in motion and air is moving. (friction)
• Tissue Viscous Resistance• Airway Resistance

Tissue Resistance
• Tissue Viscous Resistance (20%)
• Things that increase tissue resistance:• Obesity• Fibrosis• Abdominal distention

Airway Resistance
• Airway Resistance (80%)• Mainly in upper airway• Only 20% in small airways (less than 2
mm)
• Things that increase airway resistance:• High gas flow• Turbulent gas flow• Narrow airway• Long airway• Viscous gases

Poiseuille’s law
Pressure = ŋ 8 l V
╥r4
ŋ = gas viscosity l = tube length
V = gas flow r = tube radius
Pressure increases with increased tube length and gas viscosity.
Pressure increases with decreased radius

Poiseuille’s law
• Reducing the radius of a tube by ½ requires an increase in pressure 16 fold to maintain the same speed of gas flow through the tube.Pressure = 1 cmH2O Pressure = 16
cmH2O

Poiseuille’s law
•Egan:•Rule of Thumb – page 215
•Mini Clini – page 215

Airway Size• If a smaller radius causes increased
resistance then why is resistance less in the smaller airways?• More cross section• Slower flow• Laminar flow
• Large airways have less cross section & higher more turbulent flows thus more resistance.

Increased resistance
Decreased resistance

Calculation of Airway Resistance
RAW
Pressure (cmH2O)
Flow (Liters/min.)
= X 60

Calculations
• Normal Resistance = 0.5 – 2.5 cmH2O/L/sec
Pressure = 10cmH2O = 2 cmH2O/L/sec
Flow 5 L/sec

Calculations
• Increased Resistance = 4 cmH2O/L/sec
Pressure = 20 cmH2O = 4 cmH2O/L/sec
Flow 5 L/sec
Narrower airways require more
pressure.

Resistance
• Diseases that cause an increase in airway resistance• Asthma• Emphysema• Excessive sputum production• Tumors
• Things that decrease airway resistance• Bronchodilators• Anti-inflammatory agents

Resistance• How will a patient with increased
airway resistance breathe?
• Slow• Deep

Experiment• Breathe through a straw or coffee
stirrer
• Breathe slow & deep• Breath rapid & shallow
• Which feels better?

EQUAL PRESSURE POINT• See Egan page 217 – Figure 9-9
• Point where the pressure within the airway is equal to the pressure outside the airway.
• The airway will collapse downstream from the EPP.


EPP• Airway caliber is determined by:
• Anatomical support from cartilage and traction by tissues
• Pressure differences across their walls• Inside pressure > outside = open• Inside pressure < outside = collapse
• During forced exhalation, outside pleural pressure can become higher than inside airway pressure and airways collapses.

EPP & Emphysema
• Low compliance found in emphysema results in less recoil pressure and less pressure inside the airway.
• Airways collapse sooner and more gas is trapped as EPP moves upstream toward smaller airways. (increased resistance)
• Encourage slow deep inspiration and slow exhalation through pursed lips.

Air Trapping
FIG 28-3, page 609

Assignments
• READ: Egan• Chapter 6 Surface tension - pgs. 99-
100• Chapter 10 Mechanics of Ventilation -
pgs. 216-224
• Do Sibberson Math Book Chapter 13• First – Third sample sets• Practice exercises pgs. 160 – 171
• Look to objectives