Embed Size (px)
Citation preview

Safety and Efficacy of a Leadless Pacemaker: Results from the LEADLESS II clinical trial
Vivek Y. Reddy, MD, T. Jared Bunch, MD, Daniel J. Cantillon, MD, Rahul Doshi, MD, N.A. Mark Estes, MD, Derek V. Exner, MD, Paul Friedman, MD, Gery Tomassoni, MD, John Ip, MD,
Kenneth Plunkitt, MD
Icahn School of Medicine at Mount Sinai, New York, NY, Intermountain Medical Center Heart Institute, Salt Lake City, UT, Cleveland Clinic, Cleveland, OH, USC University Hospital, Los Angeles, CA, Tufts
University, Boston, MA, Libin Cardiovascular Institute of Alberta, Calgary, Canada, Mayo Clinic, Rochester, MN, Central Baptist Hospital, Lexington, KY, Sparrow Research, Lansing, MI, Naples
Community Hospital, Naples, FL.
• COI: St Jude Medical Inc – Grant support & Consultant• I will be discussing the use of non-FDA approved devices
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
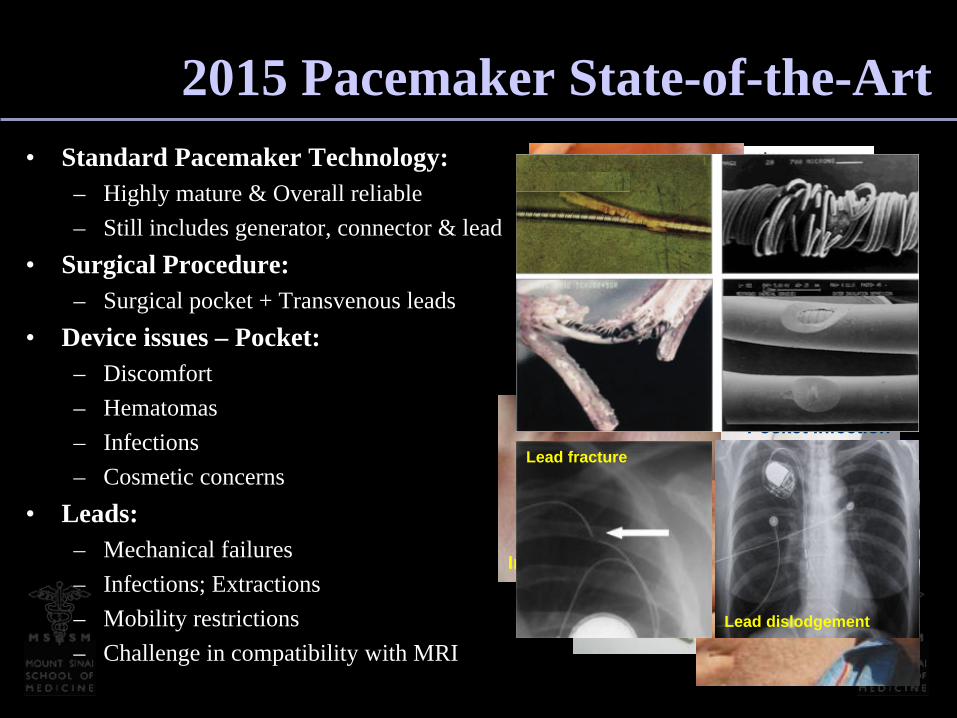
2015 Pacemaker State-of-the-Art• Standard Pacemaker Technology:
– Highly mature & Overall reliable– Still includes generator, connector & lead
• Surgical Procedure: – Surgical pocket + Transvenous leads
• Device issues – Pocket:– Discomfort– Hematomas– Infections– Cosmetic concerns
• Leads:– Mechanical failures– Infections; Extractions– Mobility restrictions– Challenge in compatibility with MRI
Hematoma
Pocket Infection
Infection Erosion
Lead dislodgement
Lead fracture
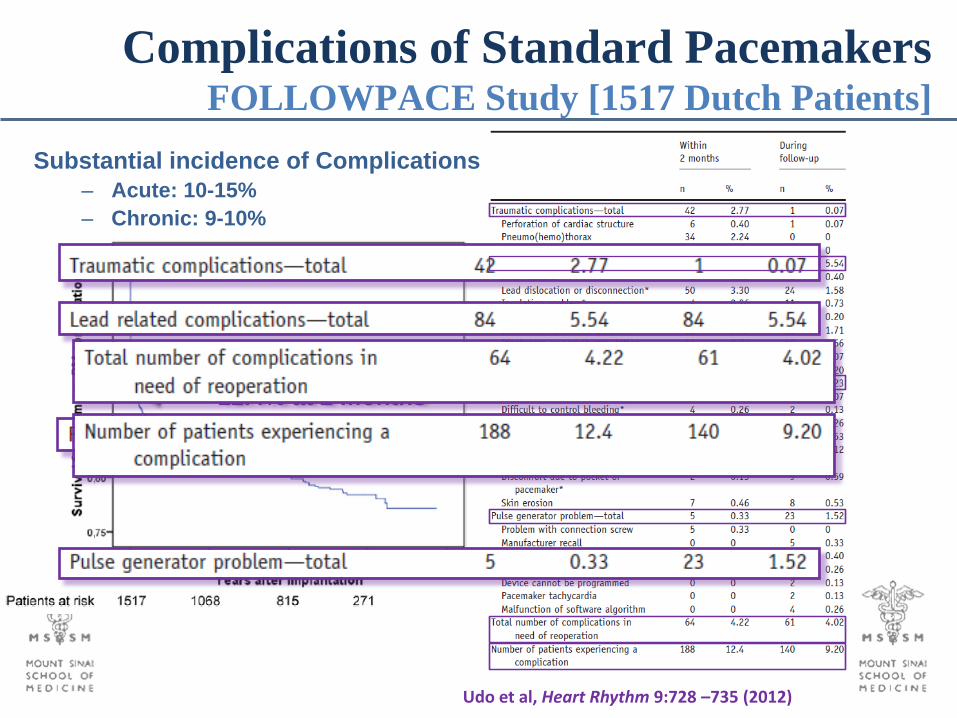
Complications of Standard PacemakersFOLLOWPACE Study [1517 Dutch Patients]
Udo et al, Heart Rhythm 9:728 –735 (2012)
12.4% at 2 months
Substantial incidence of Complications– Acute: 10-15%– Chronic: 9-10%
cc

Can we Avoid both Surgery & the Lead?A Fully Self-Contained Pacemaker
Spickler et al, J.Electrocardiology, 3:325 (1970)

Proprietary and Confidential6
• Percutaneous femoral vein delivery- 18F introducer /steerable catheter- <30 minute skin-to-skin procedure
• Self-contained device in ventricle - No lead or surgical pocket- Inherently MRI compatible
• Conventional Features-Temperature-Based Rate Response- >10-yr battery life- Hysteresis- Magnet Mode
• Flexible replacement options- Catheter-based retrieval- Place additional leadless pacemakers- Revert to conventional pacing lead
Today’s Leadless Pacemaker SystemThe Nanostim Device

Leadless Pacemaker SystemImplantation Procedure

Leadless Pacemaker CaseDevice Implanted

First-in-Man Study of Leadless PacingLEADLESS: A 3-Center, 33-Patient Study
Reddy VY / Knops R / Neuzil P Circulation 129:1466 (2014Ritter P, Eur Heart J doi:10.1093/eurheartj/ehv214
Leadless II Clinical TrialOverview
• Prospective, multicenter, non-randomized, FDA IDE study• Objective:
– To evaluate the clinical safety and efficacy of non-surgical implantation of the leadless cardiac pacemaker (LCP) system in patients who are indicated for VVI(R) pacemaker.
• Primary Endpoints:– Safety: Freedom from Serious Adverse Device Effects (SADEs) at 6
months– Efficacy: Acceptable pacing capture threshold (≤2.0 V at 0.4 msec) and
a therapeutically acceptable sensing amplitude (R wave ≥5.0 mV, or a value equal to or greater than the value at implantation) through 6 mo.
• 56 Centers in the US, Canada and Australia– 100 Operators– Of which, only one had prior experience with leadless pacing

Eligible subjects will meet all of the following: • Subject must have an indication as per guidelines:
– Chronic AF with 2 or 3° AV or bifascicular BBB block, including slow ventricular rates associated with AF 55.9%
– NSR with 2 or 3° AV or BBB block and a low level of physical activity or short expected lifespan 8.7%
– Sinus bradycardia with infrequent pauses or unexplained syncope with EP findings 35.4%
• Subject ≥18 years of age; and • Subject has life expectancy of at least one year; and • Subject is not enrolled in another clinical investigation; and • Subject is willing to comply with clinical investigation procedures and agrees to return
for all required follow-up visits, tests, and exams; and • Subject has been informed of the nature of the study, agrees to its provisions and has
provided written informed consent, approved by the IRB; and • Subject is not pregnant and does not plan to get pregnant during the course of the study
Leadless II Clinical TrialInclusion Criteria

Subjects will be excluded if they meet any of the following: • Subject has pacemaker syndrome, has retrograde VA conduction or suffers a drop in
arterial blood pressure with the onset of ventricular pacing; or • Subject is allergic or hypersensitive to <1 mg of dexamethasone sodium phosphate; or • Subject has a mechanical tricuspid valve prosthesis; or • Subject has a pre-existing pulmonary arterial (PA) hypertension (PA systolic pressure
exceeds 40 mmHg or RV systolic pressure (RVSP) as estimated by echo exceeds 40 mmHg), or significant physiologically-impairing lung disease (have severe pulmonary disease producing frequent hospitalizations for respiratory distress or requiring continuous home oxygen); or
• Subject has a pre-existing pacing or defibrillation leads; or • Subject has current implantation of either conventional or subcutaneous implantable
cardioverter defibrillator (ICD) or cardiac resynchronization therapy (CRT); or • Subject has an implanted vena cava filter; or • Subject has evidence of thrombosis in one of the veins used for access during the
procedure; or • Subject had recent cardiovascular or peripheral vascular surgery within 30 days of
enrollment; or• Subject has an implanted leadless cardiac pacemaker.
Leadless II Clinical TrialExclusion Criteria
• Pre-specified Primary Efficacy and Safety endpoints were analyzed in the first 300 patients, followed for 6 months…occurred in June 2015 (Primary Cohort)– Performance goal for the primary efficacy endpoint = 85%– Performance goal for the primary safety endpoint = 86%
• All analyses were conducted with the use of exact confidence intervals for binomial proportions.
• The primary efficacy end point was assessed in the– Intention-to-treat (ITT) population (All in whom implantation was
attempted)– Patients with successful implant
• The primary safety end point was assessed in the ITT population• Additional outcomes were assessed in all 526 patients who were
enrolled as of June 2015 (the Total Cohort)• All adverse events were adjudicated by an independent CEC
Leadless II Clinical TrialMethodology

Leadless II Clinical Trial Patient Flow
Informed Consent
Enrollment
Implant Successful?
No
Yes
Pre-Discharge
2-Week Post Implant Visit
Follow Patient for 30 days, then
withdraw
6-Week Post Implant Visit
3-Month Post Implant Visit
6-Month Post Implant Visit
Every 6 months post implant until study
completion
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
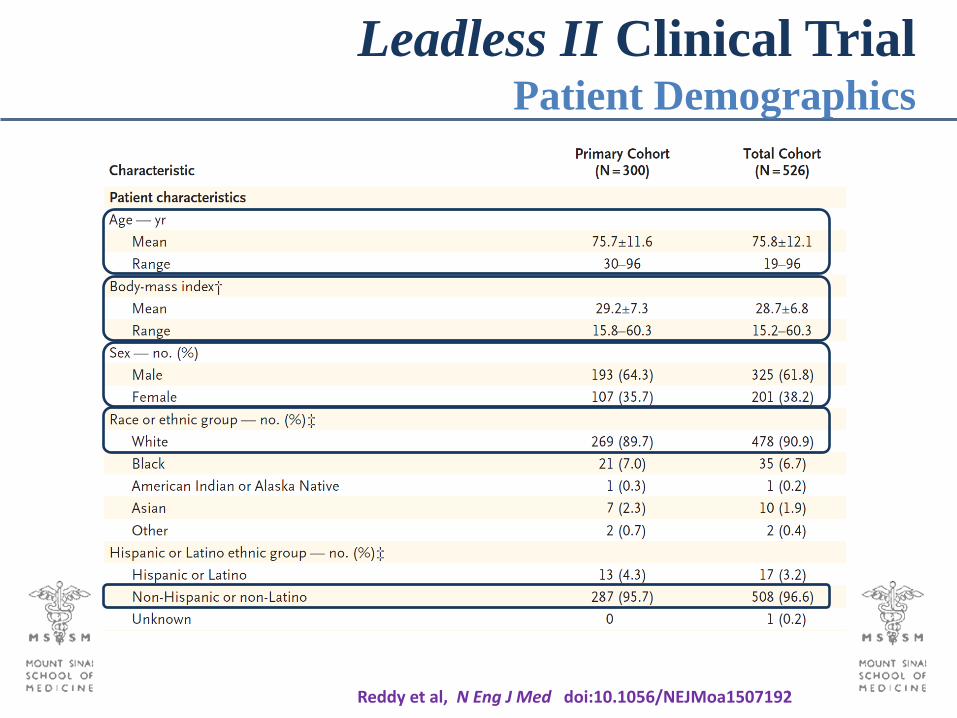
Leadless II Clinical Trial Patient Demographics
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
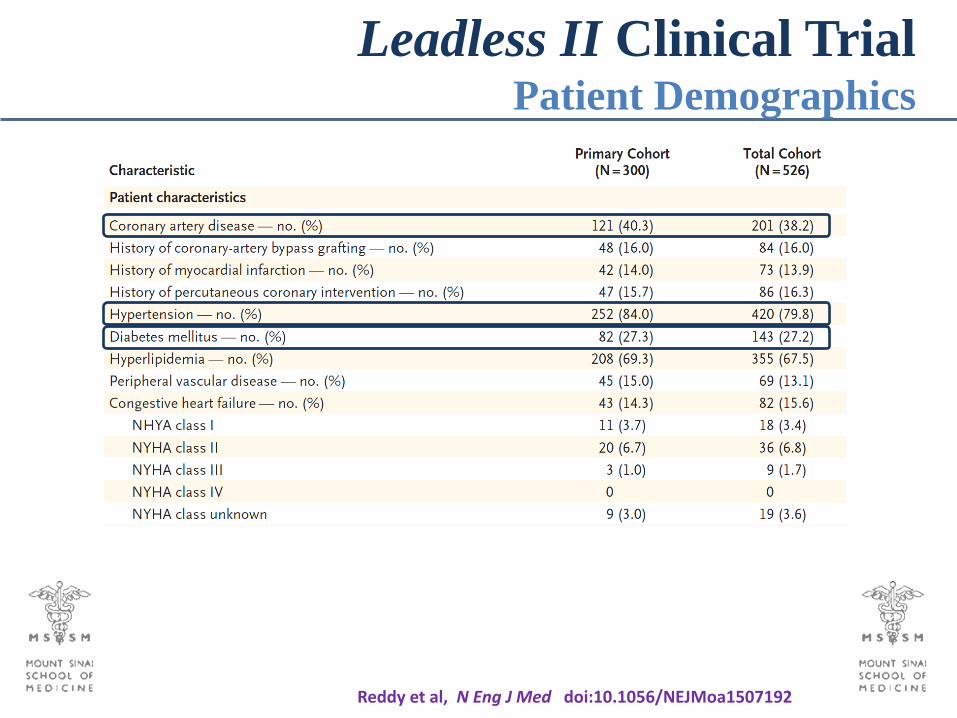
Leadless II Clinical Trial Patient Demographics
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192

Leadless II Clinical Trial Patient Demographics
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192

Leadless II Clinical Trial Procedural Characteristics
Successful Implantation 96.3% 95.8%
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192

• Safety (Intent-to-Treat Analysis)– 280 of the 300 patients achieved endpoint (93.3%; 95% CI = 89.9 to 95.9)– This exceeded the performance goal of 86% (P<0.001)
• Efficacy (Intent-to-Treat Analysis)– 270 of the 300 patients achieved endpoint (90.0%; 95% CI = 86.0 to 93.2)– This exceeded the performance goal of 85% (P = 0.007)
• Efficacy (Successful implants)– 289 patients with successful device implant– 270 of the 289 patients achieved endpoint (93.4%; 95% CI = 89.9 to 96.0) – This exceeded the performance goal of 85% (P <0.001)
Thus, all endpoints were achieved
Leadless II Clinical TrialPrimary Endpoints
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
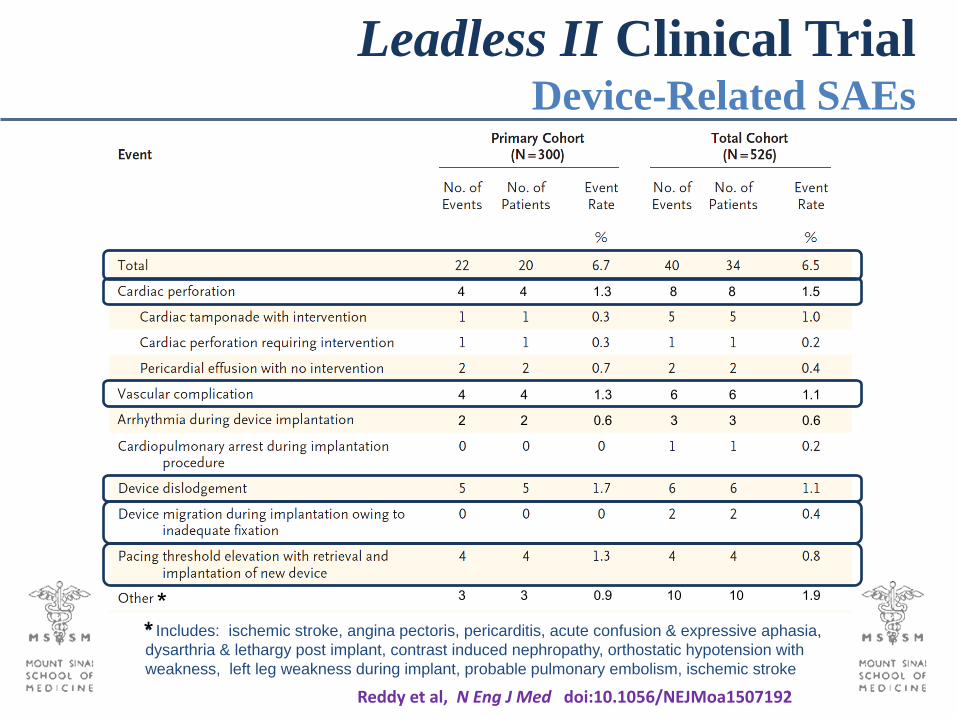
Leadless II Clinical Trial Device-Related SAEs
4 4 1.3 6 6 1.1
2 2 0.6 3 3 0.6
3 3 0.9 10 10 1.9
4 4 1.3 8 8 1.5
* Includes: ischemic stroke, angina pectoris, pericarditis, acute confusion & expressive aphasia, dysarthria & lethargy post implant, contrast induced nephropathy, orthostatic hypotension with weakness, left leg weakness during implant, probable pulmonary embolism, ischemic stroke
**
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
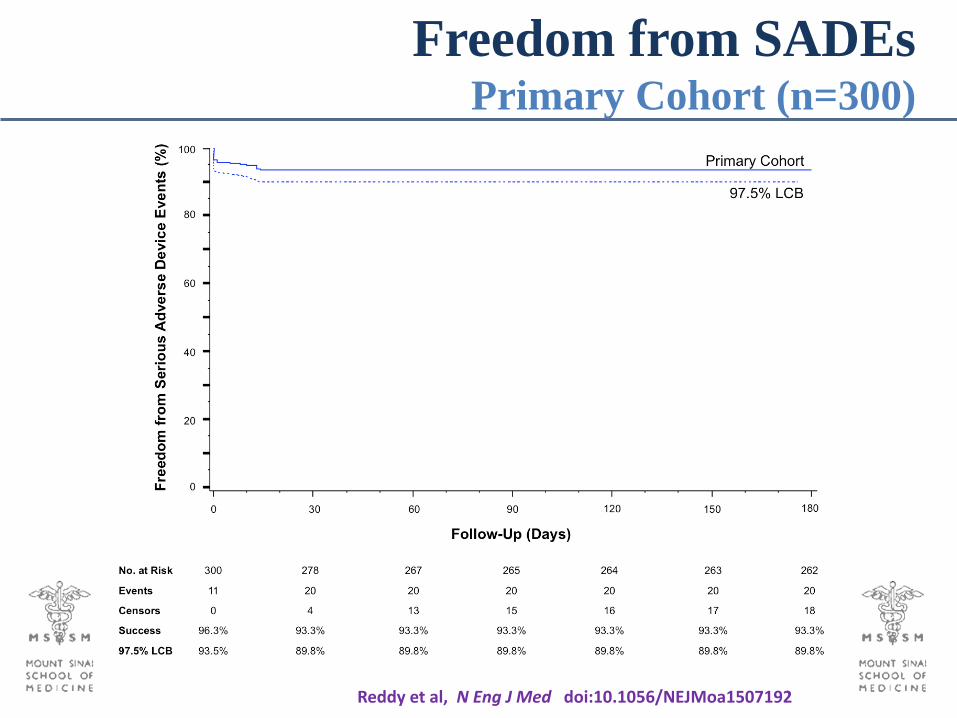
Freedom from SADEsPrimary Cohort (n=300)
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
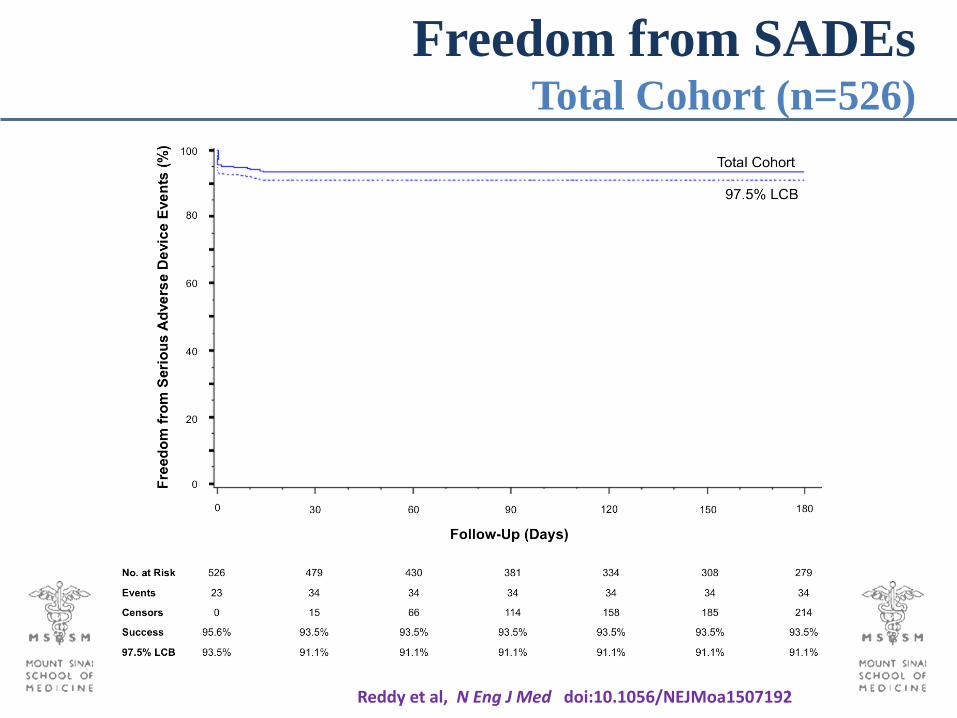
Freedom from SADEsTotal Cohort (n=526)
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
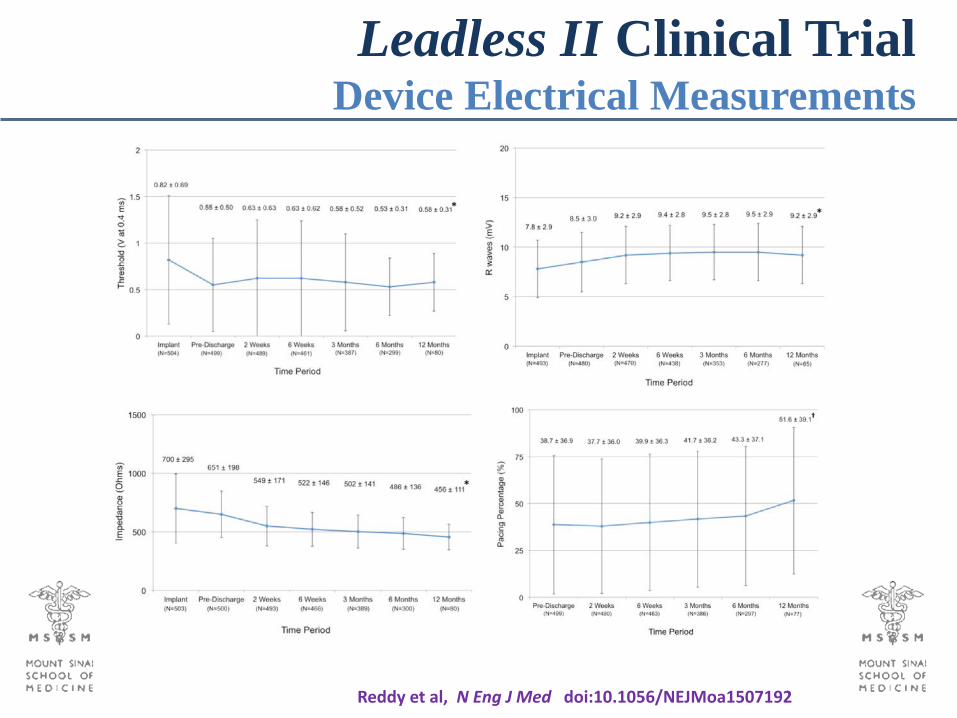
Leadless II Clinical Trial Device Electrical Measurements
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
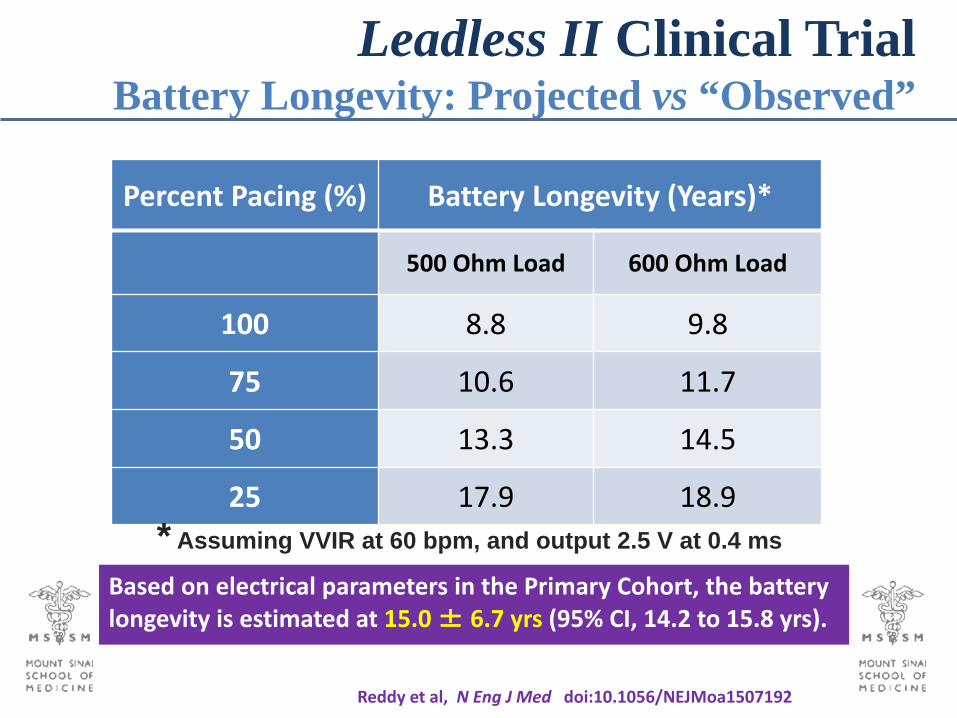
Leadless II Clinical Trial Battery Longevity: Projected vs “Observed”
Reddy et al, N Eng J Med doi:10.1056/NEJMoa1507192
Based on electrical parameters in the Primary Cohort, the battery longevity is estimated at 15.0 ± 6.7 yrs (95% CI, 14.2 to 15.8 yrs).
Percent Pacing (%) Battery Longevity (Years)*
500 Ohm Load 600 Ohm Load
100 8.8 9.8
75 10.6 11.7
50 13.3 14.5
25 17.9 18.9* Assuming VVIR at 60 bpm, and output 2.5 V at 0.4 ms

• Retrieval of 7 implanted devices 100% success without complications• Time from implant: 160 ± 180 days (Range = 1 to 413 days)• Reasons for retrieval
Elevated Pacing Thresholds = 4 pts Worsening CHF = 2 pts Elective Explantation = 1 pt
• Retrieval is an important capability in the intermediate timeframe
Leadless II Clinical TrialRetrieveability of Chronically-Implanted Devices
• The observed safety and efficacy of the Leadless Pacemaker supports its use as an alternative to standard pacemakers in patients requiring single-chamber ventricular pacing.
• The device was successfully implanted in ~96% of patients.
• The trial met the pre-specified Safety and Efficacy endpoints Complication rate in line with that seen with conventional pacemakers Complication rate likely to improve with operator experience ( Rem: 99 of 100 operators had never implanted a leadless device )
• The device was shown to be retrievable in a group of patients who needed a replacement
• The estimated device longevity (15.0 ± 6.7 yrs) is encouraging
Leadless II Clinical TrialConclusions

An Observational study (not Randomized) Mean Follow-Up of only 6 months How to manage device after battery depletion?
o Possible to retrieve after ~1 year, but what about 5, 10, 15 yrs?o Retrieval vs Abandonment
Limited device diagnostics (eg, no electrogram data) Large venous sheath (18Fr)
o Now increasingly common used for cardiology procedureso Low observed rate of hematomas
Single‐chamber (RV) pacing onlyo Device-to-device communication is in development …
Leadless II Clinical TrialLimitations

Future of Leadless PacemakersPotentiated by Device-to-Device Communication
Dual-Chamber PacemakerSingle-Chamber PacemakerCardiac Resynchronization Leadless Pacemaker + Subcutaneous ICD
Miller MA / Neuzil P / Dukkipati SR / Reddy VY J Am Coll Cardiol 66:1180 (2015)
CRT-D

















![Leadless Cardiac Pacemaker as a Novel Intervention ... · called the Leadless Cardiac Pacemaker (LCP) [3,4]. There are two main types of Leadless Cardiac Pacemaker: the multicomponent](https://img.pdfslide.net/doc/110x75/5f0bfd557e708231d433367a/leadless-cardiac-pacemaker-as-a-novel-intervention-called-the-leadless-cardiac.jpg)












